maternal perinatal mental health how can we help? kareena private hospital professional education...
TRANSCRIPT

Maternal Perinatal Mental HealthHow can we help?
Kareena Private Hospital
Professional Education Evening
23rd June 2008
Dr Ian HarrisonVisiting Perinatal Psychiatrist,
Karitane Residential Unit, Carramar
drianharrison.com.au

Our 3 Domains of Influence
BIOLOGICAL
The mother
and baby’s
Physical
development
and well
being

Our 3 Domains of Influence
BIOLOGICAL PSYCHOLOGICAL
The mother
and baby’s
Physical
development
and well
being
the mother’s
Psychological
health (and the
father’s as
well)
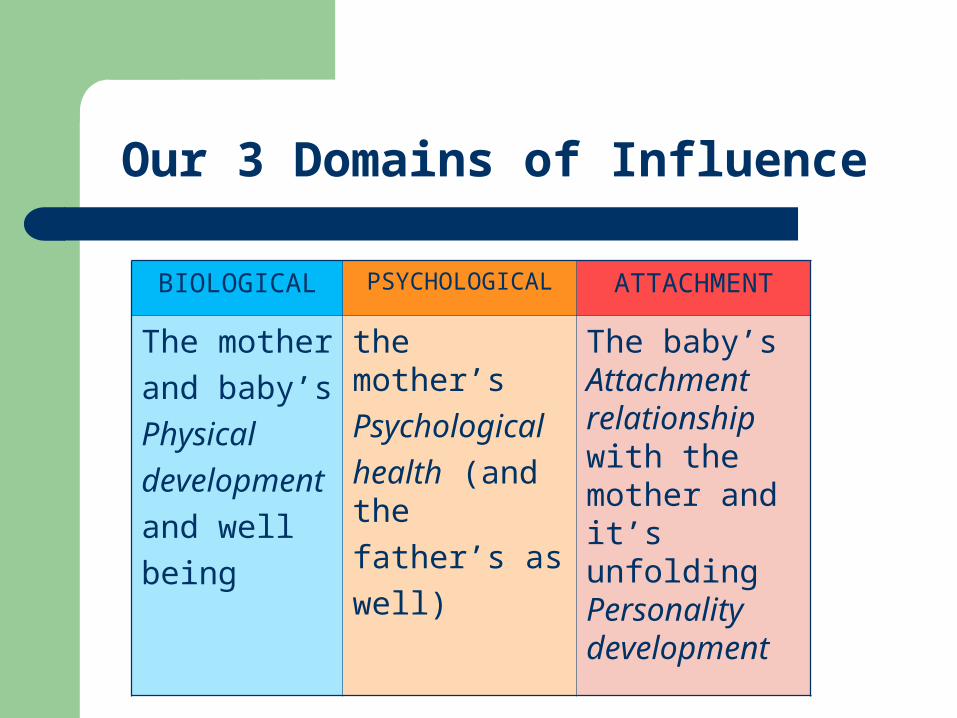
Our 3 Domains of Influence
BIOLOGICAL PSYCHOLOGICAL ATTACHMENT
The mother
and baby’s
Physical
development
and well
being
the mother’s
Psychological
health (and the
father’s as
well)
The baby’s Attachment relationship with the mother and it’s unfolding Personality development
A Mother’s Attachment Relationship With Her Baby
…begins well before birth. …begins before conception …begins in her relationship with her own
mother.

Motherhood as a Developmental Crisis
A developmental crisis:
Has potential for growth or regression
Is she/he: having a baby? becoming a mother/father? developing the personality of a new person?

What Prepares a Mother for this New Task?
best predictor of a good attachment relationship is a good experience and a good relationship with their own mother, as a baby (herself) ….and as a child ….and now as an adult

Adjustment to Motherhood (and Fatherhood)
We want to know: 1.What will heighten the crisis for this
mother? 2. What strengths does she bring to the
process? 3. In what way can we facilitate the process?
i.e. What do we bring?

We are Psychological and Attachment Midwives
Develop a collaborative approach. It is helpful to be upfront about our focus. “Is there anything that might get in the way of
you having a good experience, good outcome, successful transition, etc to motherhood and bonding with your new baby?”

Routine Antenatal Psychosocial Screening & History Taking
The Important Questions to Ask 1. Have you had any difficulties with anxiety or
depression in the past? 2. How were things for you when you were a
baby? 3. How much support to do you have socially
and from your partner to help you with this baby?
4. How are you going emotionally?

The Safe Start Model
Lack of social or emotional support availability of practical and emotional support
Recent Major Stressors (in the last 12 months) changes or losses e.g. financial stressors, migration issues, someone close dying etc
Low self-esteem including low self- confidence, high anxiety and perfectionistic traits
The Safe Start Model
History of anxiety, depression or other mental health problems, substance abuse
Couple relationship problems or dysfunction Adverse childhood experiences Domestic Violence

Use of the Edinburgh Postnatal Depression Scale
use it early, use it serially, use it as a springboard for discussion.
How has your mood been? (Might be good today – false negative)
How is your bonding with the baby?

The Four P’s of Maternal (Paternal) Maladjustment
Protective Perpetuating Precipitating Predisposing
Bio
Psycho
Social
Prior to pregnancy and/or During pregnancy
Maternal age <18 , >35 Low socio economic status Lack of partner or other social support Drug or alcohol problems, including heavy smoking Recent bereavement Infertility or other obstetric difficulties Previous termination, miscarriages, still birth, neonatal
deaths SIDS Pregnancy not wanted Late or poor attendance for antenatal care
: Caring for the Family’s Future by Barnett, Fowler, and Glossop 2004.

Prior to pregnancy and/or During pregnancy
Bleeding, hypertension, admission to hospital Past psychological problems or family history of
mental illness Severe premenstrual syndrome Anxious, perfectionistic personality Problems in relationship with partner, Domestic violence Poor relationship with mother Developmental disability Adverse childhood experiences e.g. physical or
sexual abuse or neglect : Caring for the Family’s Future by Barnett, Fowler, and Glossop 2004.

At Delivery (in addition to any of the previous risks)
No partner No partner or support person in attendance Unsupportive person in attendance Any complication in the mother or in the baby Labour and delivery not going to plan Premature or post mature baby Negative feelings regarding the baby
: Caring for the Family’s Future by Barnett, Fowler, and Glossop 2004.

After the birth (in addition to any of the previous)
Multiple birth Premature sick baby Abnormal appearance of the baby Not the expected baby Severe baby “blues”, “pinks” Breastfeeding problems Unsettled baby
: Caring for the Family’s Future by Barnett, Fowler, and Glossop 2004.

Most potent risk factors for postnatal depression
Any previous psychological disorder Anxious conscientious (perfectionistic) personality Problematic relationship with partner (poor
communication through to criticism and hostility through to domestic abuse)
Recent or otherwise significant bereavement or other loss
History of physical or emotional or sexual abuse Recent migration, non-English speaking Aboriginal Torres Strait Islander background
: Caring for the Family’s Future by Barnett, Fowler, and Glossop 2004.

Always assess Strengths and Goals
Vulnerability and strength is always a fluid dynamic.
One is never at the extremes but always oscillating somewhere between the two.
Look for exceptions to the problem What would tell you that the problem was no
longer present?

Aim for Prevention & Look for Reversibility
Low incidence
Low reversibility
High Incidence
High Reversibility
“Others” who can still get into difficulty

Some Recent Trends
Increased age of women having a baby Increased chance of having a past history of
depression or anxietyIncreased treatment of depression generally
means more women presenting taking an antidepressant
Increased detection via antenatal screening Increased research and concern re the effects of
depression on babies/toddlersIncreased use of atypicals antipsychotics and
mood stabilisers and herbals (St John’s Wort)

Prenatal Maternal Psychiatric Illness
Effects on Mother and foetus poor compliance with obstetric/medical care poor maternal health/nutrition abuse of alcohol and cigarettes abuse of other substances including over the
counter remedies suicidality, self-harm, recklessness
– reduced care of other children– marital disturbance

What about the direct effects of maternal psychiatric illness on the foetus?
These are potential effects on the foetus via changes in maternal blood chemistry, hormones, catecholamines, immune function etc,
What happens to the foetus in untreated maternal psychiatric illness??
What are the long term consequences of untreated maternal psychiatric illness (eg depression) for offspring into childhood, adolescence, etc
Potential Direct Effects of Maternal Depression/Anxiety/Stress.
Effects on foetus– changes in the HPA axis especially with
anxiety disorders– lower birth weight– prematurity– “behavioural teratogenicity” (experiments
in pregnant rats)

What has been shown?
Deleterious effect on obstetric outcome and later infant development.
Severe Stress and Depression may:– impede foetal growth– smaller head circumference– increased rate of preterm delivery and other
complications– long term behavioural problems eg aggression in
boys

Effects of Antidepressants on Foetus.
Miscarriage possible slight increase Malformations ? Increase VSD Intra-uterine deaths no increase Low birth weight slight increase Prematurity slight increase Withdrawal syndromes can occur Behavioural sequelae as yet unknown

Clinical Problem: Minimising Exposure.
We focus on the issue of exposure. There are 2 exposures:
1. What will the foetus/baby be exposed to in terms of medication? (in utero & breastfeeding)
2. What will the foetus/baby be exposed to in terms of maternal psychiatric illness? (in utero & breastfeeding)

Clinical Problem: Minimising Exposure
The foetus/baby will be exposed to something. “There is no such thing as non-exposure.” Z. Stowe.
The foetus/baby will be exposed to medication or psychiatric illness or both.
Our role is to help the mother and her partner decide which path of exposure is best for them.

The Risk/Benefit Ratio
The risks associated with medication are fairly fixed even if some of them are as yet unknown.
The risks associated with maternal psychiatric illness varies enormously for each individual.
Hence we ask, “What is the risk-benefit ratio for this woman, given her current symptom pattern or what has happened in her previous episodes of illness?”

“Happy Milk” vs. “Sad Milk”
Milk may be pure but unhappy Milk may be impure but happy At the beginning of feed infant takes in only
the milk. Soon the baby takes in a milk-and-mother
“combo” By the end of the feed the baby takes in only
the mother.
Psychotherapeutic Management
Supportive psychotherapy builds good will with the woman who is, for the time being, opposed to medication.
Avoid the dichotomy, “Well if you don’t want to take medication, I can’t help you”. – or “…. I don’t want to see you.”
Always keep the “door open”.

Case 1
Woman who is pregnant and presents with a Major Depression and doesn’t wish to take antidepressants.
She will counter any attempt to reassure her about their safety with, “I don’t even take a Panadol if I have a headache”.
“It’s the one thing I can do for my baby”.

Case 2
A mother of 2 older children and h/o severe major depression, rang to say that she had just become pregnant and could she stop her Zoloft.
This was agreed and we met 3 weeks later. At which time she was OK. Further appointment made for 4 weeks later.
3 weeks later her husband rang to say she was very depressed. Seen the next day and immediately hospitalised due to severe suicidality.

Case 2
This woman’s husband and mother in law are angry that she is depressed.
They don’t believe in the illness. They say to her, “Look what you’re doing to
the family!” They want a “guarantee” that the baby won’t
be affected by the antidepressant medications.

Case 3
Woman with first pregnancy and previous history of major depression, taking Prozac.
By 24 weeks pregnancy she is becoming increasingly depressed and suicidal.
Wants to walk in front of a bus. Psychiatrist refuses to increase the medication for fears of its effects on foetus. GP eventually overrides the decision. Medication is increased.
Woman’s mental state improves markedly.

Case 4
A woman with chronic Major Depression and Anorexia Nervosa is pregnant with second baby.
Dose of antidepressant is kept at same level as for first child. Outcome: chronically depressed and often intoxicated throughout pregnancy.
Second child has developmental delay, ?cause. 3rd baby, dose increased up to double previous
doses. Mother is less depressed in pregnancy. Baby is “perfect” and dev. normal, now 8 yrs.

Postnatal Maternal Psychiatric Illness
Effects on Mother and baby. deficits in mother-infant attachment Neuro-behavioural sequelae increased failure to breastfeed separations at home, possible psychiatric
hospitalisation abuse, neglect, self harm, recklessness rarely, suicidality/infanticide

Case 5
Woman with first baby aged 16 weeks. Baby and mother resident at Karitane.
Mo. not relating at all to baby. “Cut-off”. Staff express fears for safety of mother and baby.
Commenced on Zoloft and attempted hospitalisation with diagnosis of severe postnatal depression.
Followed up for next 8 months. Attachment relationship with baby appears to be good.

Maternal Psychiatric Illness Further Effects
Effects on Family and Environment reduced care of other children emotional neglect of other children marital disturbance occupational deterioration reduced social network Etc, etc

Case 6
Mother of 2 children. History of recurrent major depression. Continues to resist suggestions regarding medications. Remains depressed.
Eldest son, aged 4, is probably not getting enough attention. Father supports mother’s punitive and ineffective disciplinary techniques to do with time out in room. The boy is alternatively terrorised and aggressive and indulged by mother’s “guilt”.
An improvement in mother’s mood would be part of the solution.

Protect me Comfort me Delight in me Organize my feelings
Circle of SecurityCircle of SecurityParent Attending to the Child’s Needs
I need you to
Support My Exploration
Welcome My Coming To You
I need you to
Watch over me Help me Enjoy with me
I need you to
I need you to
© 2000 - Cooper, Hoffman, Marvin & Powell
explorationexploration
attachmentattachment
There Is Nothing Special About Birth!
Birth is only ever a compromise. Mahler and the “12 month-pregnancy” Winnicott and “Primary Maternal
Preoccupation.” Bruce Perry’s “Somatosensory Bath”

THE END
Thank You and Good Luck!