masters of surgery thesis - minerva access
TRANSCRIPT

Masters of Surgery thesis
Thesis title
Procurement-related liver injury: an analysis of the incidence, risk factors and
consequences at the Victorian Liver Transplant Unit.
Author
James Clement Chrysogonus Walcott
ORCID ID: 0000-0002-0976-8089
Degree
Submitted for assessment of total fulfilment of a Masters in Surgery degree, Melbourne
University, Austin campus (CRICOS Code: 006666J)
Submitted February 2020
Principle Supervisor:
Christopher Christophi
Co-Supervisors:
Michael Fink
Vijayaragavan Muralidharan
2
Table of contents
Acknowledgements 3 Declaration 4 Abstract 5 Introduction 6 Systematic review 8 Figure 1. PRISMA flow diagram 9 Table 1. Summary of studies describing PRLI from systematic review 10 Patterns of PRLI 11 Table 2. Summary of patterns of PRLI, their risk factors and consequences 11 Risk factors for PRLI 13 Consequences of PRLI 17 Rationale for study 21 Hypotheses 23 Methods 24 Figure 2. Example of Organ Retrieval Report Form 27 Results 28 Table 3. Donor and surgery characteristics 29 Table 4. Variant hepatic anatomy and liver injuries 30 Table 5. Associations with PRLI - univariate analysis 32 Table 6a. Multivariate analysis 33 Table 6b. Univariate subgroup analysis 33 Table 7. Surgical outcome and expected impact of PRLI vs survival 34 Table 8. Complications compared by presence of PRLI and subgroup 35 Figure 3. Patient survival compared by injury 36 Figure 4. Graft survival compared by injury 36 Figure 5. Graft survival compared by type of injury 37 Figure 6. Graft survival compared by surgical “outcome” of injury at transplant 37 Figure 7. Graft survival compared by expected “impact” of injury 38 Discussion 39 Conclusion 44 References 45

3
Acknowledgements
This thesis could not have been completed without the knowledge, patience, help and
dedication of my supervisors. Their belief and commitment have allowed me to bear fruit.
I also acknowledge the support from my partner Evan and from my family.
Finally, I must acknowledge Paganini and Hildegard whose unwavering love and loyalty have
helped me to get through.
4
Declaration
I James Clement Chrysogonus Walcott, the author of this thesis submitted for assessment
towards a Masters in Surgery at Melbourne University make the following declarations:
1. I declare the entire content of this thesis represents original work performed by
myself under the supervision of the above-mentioned supervisors
2. I declare that this thesis does not exceed the word limit of 50,000 words –
comprising a total of 11,259 words excluding declaration, acknowledgements,
contents and bibliographies
James Clement Chrysogonus Walcott
17 February 2020

5
Abstract
Introduction
Liver transplantation is an established treatment for liver failure, and its success relies on the
quality of the donated organ. A systematic review on the topic of procurement-related liver
injury (PRLI) showed that studies on PRLI are few, with widely variable methodologies and
results, and may not apply to modern day practice. This is the first Australian study examining
risk factors and consequences of PRLI.
Method
The Victorian Liver Transplant database was examined for PRLI from deceased liver donors
from 2010 to 2017. Information regarding the donor, surgery and subsequent transplantation
was obtained. PRLI details were retrieved from the “organ retrieval report form” (ORRF). Risk
factors and complications for PRLI were obtained and analyzed.
Results
420 transplants were included in this study. There were 46 injuries in 45 livers equating to an
injury rate of 10.7%. Aberrant anatomy increased the risk of PRLI (OR 3.68 CI 1.84 – 7.35,
p<0.001). Surgeon experience of less than 172 cases increased the risk of PRLI (OR 5.96, CI
1.29 – 27.51, p=0.02). On subgroup analysis aberrant anatomy increased the risk of vascular
injury and lower surgeon experience increased the risk of parenchymal injury. There was no
difference in patient or graft survival for injured grafts with the exception of reduced graft
survival at 3 months for injuries requiring repair or modification (78.6% vs. 93.3%, p=0.028).
Complication rates were the same in the presence of PRLI.
Conclusion
This study shows that PRLI is common, and that aberrant anatomy and surgeon inexperience
increase the risk of injury. Similar outcomes for transplantation despite the presence of PRLI
indicate that injuries are being appropriately managed in the Australian setting.

6
Introduction
Liver transplantation is the only effective treatment for end-stage liver disease and fulminant
liver failure. It also has a well-established role in the treatment of liver malignancies such as
hepatocellular carcinoma and for metabolic disorders [1]. In Australia and New Zealand, more
than 300 patients undergo liver transplantation each year [2]. In the last five years a total of
90 people died while waiting for a liver transplant (4.5% of patients activated on the waiting
list), highlighting the limited availability of suitable donor organs [2]. Deceased organ donors
remain the predominant source of liver donation in Australia, the majority of which are brain
dead donors [2]. Living-donor liver donation represents a very small number of liver donors,
totalling 1.6% of transplanted livers in the last 5 years in Australia and New Zealand [2].
The success of transplantation is dependent on multiple factors, including the quality of the
donated organ and the organ retrieval process. Donor related factors include the donor’s age,
comorbidities, pre-existing liver parenchymal disease, mode of death and pre-operative
management of the organ donor [3]. For liver transplantation, the “donor risk index” (DRI)
describes multiple independently significant characteristics that increase the risk of graft
failure and is used to calculate a predictive score for graft failure [4]. The factors that comprise
the DRI include age, race, height, cause of death, donation after circulatory death (DCD), and
split or reduced grafts. Additionally, in this study two transplant factors; cold ischaemic time
and sharing outside a local donor area, were identified to independently contribute to risk of
graft failure. Injury to the liver during the procurement process for transplantation is a well-
recognised issue that may impact on the subsequent transplantation, however this is not
featured in the DRI by Feng et al [4]. Fortunately, the rate of discard owing to PRLI is relatively
low at approximately 1-3 per 1000 retrievals in large registry analyses [5, 6]. Nonetheless,
several studies have shown increased rates of complications due to PRLI. In particular
bleeding complications requiring operative intervention have been associated with
parenchymal injuries [7] and arterial injuries have been associated with increased rates of
hepatic artery thrombosis [8, 9].
PRLI became increasingly recognised as in issue late last century when shipment of grafts
between geographical locations became more commonplace and a subsequent separation

7
between procurement and implanting teams ensued [10]. Lerut described “major” vascular
and parenchymal injuries in 23% of 39 imported livers over a two-year period in the early
1990s compared with 0.7% injuries in locally procured grafts in the same period [10]. This lead
to the development of feedback forms such that transplanting surgeons could document
technical issues related to the graft that could be relayed to the procurement team and
archived for quality assurance, research and educational purposes. Since then several case
series have described quite variable rates of PRLI, from 4-34% [5, 6, 9, 11-14], with registry
studies estimating the rate of PRLI from 1.8 – 14% [5, 6]. Nijkamp et al. [9] described the
highest PRLI rate of 34% in a series of 241 liver transplants although the majority of these
injuries were not “clinically relevant”.
The technique of organ retrieval has been described since the 1960s starting with single-organ
deceased donor renal procurement [15, 16]. Multi-organ abdominal procurements and
combined chest and abdominal procurements were described in the 1980s [17, 18]. The
abdominal multi-organ procurement technique was standardized by Starzl in the mid to late
1980s [19, 20], and currently, formal training programs in multivisceral organ procurement
are available world-wide.
DCD livers are considered marginal grafts owing to an increased risk of graft failure and
patient death compared with donation after brain death (DBD), however their utility is
balanced against the scarcity of donor liver supply [21]. The majority of morbidity associated
with DCD liver transplantation is attributed to the period of warm ischaemia in DCD organ
procurement and the sensitivity of the liver to ischaemic injury, in particular the development
of ischaemic cholangiopathy and non-anastomotic biliary strictures. Minimising warm-
ischaemia time through systematic management of the DCD donor has been shown to
improve outcomes for DCD liver transplants. In particular, withdrawal within the operating
theatre improves graft survival and premortem administration of heparin has been shown to
reduce the rate of primary graft non-function [22].
PRLI is a potentially avoidable problem that can affect the outcome of subsequent
transplantation. This subject has been most extensively studied regarding renal procurement,
however studies on PRLI are much more limited. Understanding the nature of PRLI, their risk

8
factors and impact, is relevant to understanding how they can be prevented and what
consequences can be anticipated if they occur.
Systematic review
A search of Pubmed, the Transplant Library and the Cochrane Library was performed for
journal publications concerning liver procurement and specifically liver injury during
procurement. A search using a combination of MeSH headings: “liver transplant”, “tissue and
organ procurement” and “wounds and injuries” with keywords: “procurement injury”,
“procurement related injury”, “retrieval associated graft injury”, “parenchymal injury”,
“parenchymal liver injury” and “vascular injury” returned 184 potential publications (see Fig
1; PRISMA flow diagram). A further three publications were sourced from bibliographic
searching of relevant articles resulting in 187 potentially relevant publications. Titles and
abstracts were screened to include publications relevant to PRLI within a series of liver
procurements or liver transplants from deceased donors. Articles not related to liver
procurement, injury to organs other than liver during procurement, individual cases of liver
injury, series from living donors, abstracts from conference proceedings, animal studies, or
non-English publications were excluded, leading to 21 full-text articles that were examined.
Of these, ten publications were identified that specifically investigated PRLI [5-14]. These are
summarized in Table 1.

9
Figure 1. PRISMA flow diagram
Records identified through database searching
(n=184)
Additional records identified through bibliography reviews
(n=3)
Abstracts screened (n=187) Records excluded based on
abstract (n=166)
Full-text articles assessed for eligibility
(n=21) Full-text articles excluded (n=11)
Studies included in review (n=10)

10
Table 1. Summary of studies describing PRLI from systematic review
Reference Country Study design Number of livers
Injuries (%) Parenchymal injuries (%)
Vascular injuries (%)
Biliary injuries (%)
Comments
Ausania 2013 [5] UK Registry analysis 7,146 1,001 (14) 838 (12) 163 (2.3) 0 (0) Compared DBD to DCD injury rates, found capsular injuries increased in DCD
Taber 2016 [6] USA Registry analysis 4,396 80 (1.8) NS NS NS Prospectively collected registry data comparing different organ procurement organisations
Ausania 2012 [8] UK Retrospective cohort
844 NS NS 14 (1.7)* NS Study specifically investigated injured accessory RHA, and found an increased risk of HAT (14.3% vs 2.9%, p=0.01)
Soliman 2000 [7] Austria Retrospective cohort
572 NS 23 (4.0)** NS NS Only parenchymal injuries described according to an injury grading system
Nijkamp 2006 [9] Netherlands Retrospective cohort
241 82 (34) 50 (21) 40 (17) 6 (2.5) Only 6.6% of injuries were “clinically relevant”
Boteon 2019 [11]
UK Retrospective cohort
236 64 (27) 37 (16) 27 (11) NS Cohort of only DCD livers, found PRLI in high-risk groups had a negative impact on graft survival
Lerut 1994 [10] Belgium Retrospective audit 180 10 (5.6) NS NS NS Found a large number of injuries in imported grafts compared with local grafts
Jung 2015 [14] Korea Retrospective cohort
165 13 (7.9) 7 (4.2) 6 (3.6) 0 (0) Single surgeon experience of warm dissection technique
De Boer 2017 [12]
Netherlands Prospective observational
133 36 (27) NS NS NS Higher injury rate in DCD group
Fernandez 2007 [13]
Germany Retrospective cohort
102 9 (8.8) 1 (1.0) 8 (7.8) NS
NS: not specified, DBD: donation after brain death, DCD: donation after circulatory death, RHA: right hepatic artery, *only injuries to accessory RHA included, **only parenchymal injuries included

11
Patterns of PRLI
Donor liver injuries can be broadly divided into three categories: parenchymal, vascular and
biliary. These are summarised in Table 2.
Parenchymal injury
Parenchymal injuries are the most common injuries encountered during organ procurement
ranging from 1-21%. These are subcategorised into capsular tears, parenchymal lacerations
and subcapsular haematomas [5, 7, 9, 11, 13, 14]. In a capsular tear, the laceration is confined
solely to the Glissonian capsule and is frequently the result of traction on the liver where it is
fixed to its peritoneal attachments or adhesions. This is commonly seen on the right lobe of
the liver adjacent the attachment of the right triangular ligament. A parenchymal laceration
is deeper than a capsular tear and involves the underlying parenchyma as its name implies.
These are seen in the case of more severe traction injuries or when the parenchyma is
inadvertently cut with surgical instruments during abdominal entry or mobilisation of the
liver. Haematomas are the result of blunt force to the liver due to handling or traction. They
may coexist with tears or lacerations.
Table 2. Summary of patterns of PRLI, their risk factors and consequences
Injury type Parenchymal Vascular Biliary
Subtype
Laceration
Capsular tear
Haematoma
Arterial
Portal
Caval
High division
Inadvertent ligation
Stripping of bile duct
Risk factor DCD procurement Aberrant anatomy None identified
Consequence Bleeding HAT Bile leak
AS
DCD – donation after circulatory death, HAT – hepatic artery thrombosis, AS – anastomotic stricture
12
Nijkamp et al. [9] reported the highest incidence of parenchymal injuries at 21%, of which the
majority were capsular tears. Soliman et al. [7] found a 4% rate of parenchymal injuries and
graded them from Grade I – VI, according to a modified organ injury scale similar to that used
for trauma assessment [23]. The highest grade of injury encountered in their study was Grade
IIIb, representing a parenchymal laceration of greater than 3 cm depth but involving less than
25% of an hepatic lobe.
DCD procurement has been shown to increase the risk of parenchymal injury (see below) [5,
12]. Adhesions from previous abdominal surgery are also considered a risk factor for
parenchymal injuries especially for lacerations encountered on abdominal entry where the
liver is adherent to the scar of a previous laparotomy. However as far as the author is aware,
this has not been validated in the context of a study.
Vascular injury
Vascular injuries may be arterial, portal or caval in nature. They occur in 2.3 – 17% of donor
organs [5, 8, 9, 11, 13, 14]. Arterial injuries are the commonest of the vascular injuries and
have the greatest clinical significance. Nijkamp et al. [9] identified vascular injuries in 17% of
transplanted livers which included arterial (12%), caval (3%) and portal venous (2%) injuries.
Boteon [11] found a vascular injury rate of 11% in a series of DCD livers. These were
significantly higher than the rate of vascular injuries documented by Fernandez et al. (8%),
Jung et al (3.6%) and Ausania et al. (2.3%) [5, 13, 14]. Arterial injuries can be repaired in most
cases either primarily or reconstructed using branches of the arterial patch attached to the
donor liver such as anastomosing the donor gastroduodenal artery to a replaced right hepatic
artery. In some cases, additional vessels (such as donor iliac vessels or recipient saphenous
vein) or synthetic conduits may be required. The complexity of the reconstruction increases
as the number of arterial anastomoses and required level of magnification increases.
Aberrant arterial anatomy is the main known risk factor for arterial injury, and has been
demonstrated to increase the risk of arterial injury from 9.5% to 26.8%, p=0.002 [9].
Venous injuries occur in less than 5% of transplants and include injury to the portal vein and
its branches, hepatic veins and their tributaries or the inferior vena cava [5, 9, 11, 14]. A short
supra-hepatic inferior vena cava divided at the confluence of the hepatic veins is often the

13
consequence of combined liver and heart retrieval where the division of the cava is in favour
of the cardiac procurement, leaving a hepatic segment of cava that may be unsuitable for
anastomosis. Portal venous and caval injuries can be repaired primarily or by the use of
various patches or interposition grafts. Successful techniques for reconstruction of caval
injuries have been described in case reports with minimal long-term consequences [24, 25].
Biliary injury
Biliary injuries are the least common of procurement related liver injuries and are
encountered in 2% of transplants in the Nijkamp study [9] The most common biliary injuries
include high division of the bile duct affecting the biliary anastomosis, and stripping of the
bile duct which could potentially result in ischaemia to that duct. Other biliary injuries include
injury to the common hepatic duct or its branches, or inadvertent ligation or transection of
extrahepatic biliary variations. Previous surgery such as cholecystectomy or variant biliary
anatomy are thought to increase the risk of biliary injury, however this has not been
demonstrated in the context of a study.
Risk factors for PRLI
Donor related factors
There is limited evidence demonstrating specific donor-related risk factors for PRLI. Aberrant
arterial anatomy was shown to increase the risk of arterial injury from 9.5% to 26.8%
(p=0.002) in a series of 241 liver transplants [9]. Donor age, gender and BMI were not found
to have any association with PRLI in two studies [9, 12]. This contrasts with studies regarding
kidney procurement where increasing age [26], male gender and increasing BMI [27] have
been positively associated with procurement related injury to the kidney.
Multiple organ donation
Liver procurement in combination with other organs is routine practice, however care must
be taken that each individual organ’s needs are met during the process. Liver may be procured
in combination with kidneys, pancreas, intestines, heart and lung.

14
Liver procured in combination with kidney appears to be safe for both organs, and possibly
beneficial to the outcome of the kidney donation. Several large retrospective studies have
demonstrated that renal graft survival is improved when the kidneys were procured in
combination with other organs [28-30]. This is perhaps better explained that multivisceral
donors have better quality kidneys than kidney-only donors, however the finding that kidney
injury is less likely to occur when it is procured in combination with liver and other organs at
least demonstrates safety for combined procurement. In addition, kidney injuries have been
shown to be least likely to occur when procured by a liver retrieval team compared with a
kidney-only retrieval team suggesting an element of surgical experience to be relevant [28].
Pancreas and intestinal retrieval present significant challenges when performed with liver
retrieval owing to sharing of blood supply [31], however there are several case series
demonstrating safety in combined liver, pancreas and intestinal procurements [32-34].
Special care is required in the case of an aberrant right hepatic artery arising from the superior
mesenteric artery when liver and pancreas are procured in combination. This can be dealt
with by dividing the aberrant right hepatic artery outside of the pancreas and anastomosing
it to a branch of the common hepatic artery (usually the gastroduodenal artery) leaving the
intact superior mesenteric artery for transplantation with the pancreas.
In combined liver and heart procurement, the suprahepatic cava is at risk of being transected
too short in favour of the heart. Several case studies describe repairing such injuries [24, 25],
Good communication between thoracic and abdominal procurement teams is essential in
avoiding such injuries, and downward traction on the liver when the right atrium is being
separated from the cava may help to preserve length in the suprahepatic cava.
Cold versus warm phase dissection and “en bloc” dissection
Historically with the advent of heart beating deceased organ donation, the majority of the
dissection for organ procurement was performed while the heart was beating, i.e. during the
“warm phase” [19, 35]. A rapid retrieval technique with early cold perfusion followed by
dissection and recovery during the cold (or pulseless) phase was utilized for unstable donors
[20, 36] and a shift to cold phase dissection ensued in various centres. Proponents for cold
phase dissection cite evidence that the technique is quicker, may have fewer reported

15
injuries, “improves collegiality” between operating staff and can be performed by less
experienced surgeons [37-39]. Proponents for warm phase dissection argue the technique is
not substantially longer, there are less surgical cues in the pulseless setting, and that injury
rates are acceptable [14]. Ultimately, it appears to be surgeon and institutional preference,
as well as the clinical situation, that dictate the most appropriate technique.
“En bloc” organ retrieval describes the technique whereby more than one organ is procured
from the donor and the organs are subsequently dissected and separated on the back table.
This technique is especially relevant for combined pancreas and liver procurement. In a
retrospective study of 32 patients comparing en bloc retrieval to extensive warm phase
dissection, recipients of en bloc retrieved livers had better early liver function as measured by
liver biochemistry, and shorter in-hospital stay. Long-term liver graft function was equivalent,
as was pancreas function [40]. Similarly, a series of 81 consecutive en bloc “total abdominal
eviscerations” (TAE) compared with a matched cohort of traditional dissection concluded that
the TAE had a lower rate of liver graft primary non-function and a lower requirement for fresh
frozen plasma [41]. Kidney function was similar in the TAE and non-TAE groups, and 9 whole
pancreata were successfully transplanted using this technique.
While the above evidence demonstrates advantages for the transplanted liver for cold phase
dissection and en bloc retrieval in the context of non-randomised studies, there are no studies
comparing PRLI rates for those techniques and no convincing evidence of superiority of such
techniques.
DCD versus DBD organ retrieval
An increasing number of liver procurements from DCD donors are being performed in an
effort to expand the donor pool. For kidney procurement, DCD recovery has been shown to
have a higher rate of organ injury and a higher discard rate related to organ injury [27]. In a
registry analysis of 7,146 procured livers in the UK, DCD procurement was associated with an
increased rate of capsular injuries (15.6% vs 11.4%, p = 0.002). There was no increase in the
rate of arterial, portal venous or caval injuries associated with DCD procurement in this study,
nor was there an increase in discard owing to PRLI with DCD procurement [5]. A higher rate
of non-utilisation of DCD recovered livers compared with DBD recovered livers was

16
demonstrated but attributed to steatosis rather than injury. In a Dutch prospective study of
133 procured livers, DCD donation was the only risk factor associated with PRLI, conferring
an odds ratio of 2.316 (95% CI 1.063-5.045, p=0.034) compared with DBD donation [12]. Long-
term studies on graft and patient survival in DCD liver transplantation demonstrate inferior
results compared with DBD donors [42], including higher rates of primary non-function [43]
and non-anastomotic biliary strictures [44]. However, the contribution of PRLI to long-term
outcome in DCD liver transplantation is not well defined, and there were no studies identified
that examined the effect of PRLI on graft and overall survival for DCD procured livers. In spite
of a higher rate of organ injury and poorer outcomes associated with DCD liver donation, this
remains an important resource of organs to an expanding requirement for donor livers.
Surgeon experience and geographical location
Surgeon experience has not been definitively shown to increase the risk of PRLI during
procurement [9]. It has however been shown to have an impact on procurement-related
injury in several studies for kidney [12, 26] and pancreas [12, 45]. Wigmore et al. [26] reported
a higher rate of injury in kidneys procured by renal retrieval teams compared with liver
retrieval teams when procuring both liver and kidneys (21.2% vs 16.8%, p<0.001), and that
centres that did greater than 50 retrievals per year had a lower rate of kidney injury. Lam et
al. [45] showed that professional certification for abdominal retrieval in the Netherlands via
an online teaching program, followed by multiple choice exam and a two-day practical
masterclass led to an increase in pancreatic organ quality and allografts accepted for
transplantation. In a Dutch series examining liver, pancreas and kidney retrieval, high volume
centres had reduced rates of organ injury for kidneys and pancreas retrievals, however no
difference was found for liver retrievals [12].
Geographical location appears to be relevant as a risk factor for organ injury and may be a
surrogate marker for surgeon experience in liver retrieval. Nijkamp et al. [9] examined their
series of 241 liver transplants in the Netherlands according to the geographical location from
which the organ was retrieved and the local teams that were responsible for that location.
The cohort was divided into two national regions nominated as national region 1 and 2 (which
had separate procurement teams responsible for each region), and a separate group for
organs imported from other countries which were procured by a retrieval team local to the

17
donor. They found that national region 1 had a lower rate of injury than national region 2 and
imported organs (23% vs 46% and 42%, respectively, p = 0.003). There was a lower injury rate
when the procuring surgeon was a liver transplant surgeon compared to a non-liver
transplant surgeon, but this did not achieve statistical significance (28% vs 38%, p=0.186) [9].
Taber et al. [6] showed in a prospective series of 5,401 deceased donors for all organs from
36 separate organ procurement organizations (OPOs) that higher volume OPOs (>147.5
donors per year) had a lower rate of “class 3” injuries (rendering the organ non-
transplantable). Lerut et al. [10] found a much higher rate of PRLI in imported liver grafts
(23.1%) compared with locally retrieved livers (0.7%) in a Belgian series of 180 liver
transplants over a 2-year period and advocated for a feedback system to address this issue.
More recently in the UK Boteon et al. [11] demonstrated that geographical location increased
the risk of PRLI in DCD livers with a lower injury rate in their local retrieval centre compared
with others (18% vs. 32%, p=0.02). While variations in geographical location appear to impact
on the frequency of injury rates in liver procurement, more data are needed to explain the
reasons for this, including variations in surgical technique, logistics and level of experience.
Consequences of PRLI
Organ discard
Non-utilisation of donor livers owing to PRLI is fortunately a rare occurrence ranging from 1-
3 per 1,000 donors in large multi-centre studies [5, 6]. The main reasons attributed to discard
following procurement-related injuries are vascular injuries that defy reconstruction or
severe parenchymal injuries precluding transplantation.
Haemorrhagic complications
Bleeding following liver transplantation may sometimes be managed conservatively or via
radiological and percutaneous techniques, but most often requires re-laparotomy. Nijkamp
et al. [9] demonstrated haemorrhagic complications to occur in 10.8% of liver transplantation.
In the presence of parenchymal injury, they found an 18% incidence of haemorrhagic
complications compared with 9% in livers without parenchymal injury however, this was not
statistically significant (p=0.06). Lerut et al. [10] showed major capsular injuries in 5 of 39

18
imported grafts (12.8%) all of which suffered from haemorrhagic complications resulting in
one re-transplantation and one death. Soliman et al. [7] described various techniques for
controlling bleeding due to parenchymal injuries. These included suturing, fibrin glue,
hemostyptics, mesh wrapping and mesh packing. There were seven re-operations for
bleeding, equivalent to a 30% re-operation rate in the presence of a parenchymal injury. The
re-operation rate for transplants without a parenchymal injury was not described in the study.
An increased injury grade was found to be associated with an increased requirement for re-
operation for haemorrhage. Seven out of 17 transplants with Grade II or III injuries required
further laparotomy for control of haemorrhage while none out of six transplants with a Grade
I injury required re-operation (p=0.04). Donor organs with higher grades of parenchymal
injuries also showed an increasing trend towards longer operating times during
transplantation but this did not reach statistical significance (7 +/-1 hours for Grade II and III
injuries vs 5 +/-1 hours for Grade I injures; p=0.06). Parenchymal injury did not impact on
overall or graft survival in this study.
It appears that parenchymal injury rarely prevents utilization of donor organs. In a study of
4,396 procured livers in the USA, there were two (0.05%) donor livers not transplanted owing
to parenchymal injury [6]. Similarly, a study of 102 procured livers in Germany identified one
(1%) case of liver discard due to parenchymal injury [13].
Vascular complications and hepatic artery thrombosis
Vascular complications include arterial, portal venous and hepatic venous complications.
Vascular complications may be divided into stenosis, thrombosis, dissection or aneurysmal
transformation of the vessel. Stenosis occurs when the vessel appears to narrow but flow
beyond the stenosis is maintained. By contrast vascular thrombosis describes complete
occlusion to flow of the vessel.
Hepatic artery thrombosis (HAT) is the most commonly described vascular complication
following liver transplant. HAT affects less than 5% of liver transplants, however it is
associated with a high rate of graft loss [46]. In a systematic review of 21,822 liver transplants
involving 843 cases of early (defined as within 2 months of transplantation) hepatic artery
thrombosis, Bekker et al. [46] found that hepatic artery thrombosis was associated with a

19
53% incidence of graft loss and 33% incidence of mortality in the postoperative period. Risk
factors for early hepatic artery thrombosis included paediatric transplantation, CMV
donor/recipient mismatch, re-transplantation, use of conduits and primary sclerosing
cholangitis. Low volume transplant centres were also found to have a higher rate of early
hepatic artery thrombosis.
Nijkamp et al. [9] showed that the presence of arterial injury in the donor liver correlated with
an increased incidence of hepatic artery thrombosis compared with recipients where there
was no arterial injury (23% vs 4%, p = 0.001). A study looking specifically at the consequence
of injury to aberrant right accessory arteries in a series of 844 liver transplants divided their
cohort into three groups: A) normal anatomy and single arterial anastomosis (n=654), B) right
accessory hepatic artery requiring reconstruction (n=63) and C) right accessory hepatic artery
with injury during procurement requiring reconstruction (n=14) [8]. In this study, the
incidence of hepatic artery thrombosis was 2.9% in group A, 6.4% in group B, and 14% in
group C (p = 0.01). Following transplantation of a graft with a reconstructed accessory right
hepatic artery, those requiring reconstruction because of injury to the accessory right hepatic
artery had worse 3-month patient (82% vs 98%, p = 0.02) and graft (62% vs 88 %, p = 0.01)
survival [8]. The incidence of biliary complications at three months was not significantly
different between the three groups.
The consequences of venous injuries requiring repair include portal or caval stenosis or
thrombosis which may lead to portal hypertension, venous outflow obstruction or graft loss.
Organ discard due to vascular injury is also uncommon. Taber et al., in their study of 4,396
procured livers, found only three (0.07%) donor organs not transplanted due to venous injury
[6].
Biliary complications
Biliary complications following liver transplantation include bile leaks, biliary anastomotic
strictures, non-anastomotic biliary strictures (NAS), mucocoeles, calculus formation and
haemobilia [47]. Procurement-related biliary injuries such as high division or stripping of the
bile duct are uncommon, but may lead to subsequent anastomotic biliary strictures or
necessitate the formation of a hepaticojejunostomy [9].

20
NAS are thought to be related to ischaemic cholangiopathy but are most likely multifactorial.
Hepatic artery thrombosis is a well-recognized cause of NAS and thus hepatic arterial injury
during procurement may indirectly lead to NAS [47, 48]. However other factors have been
shown to impact on the development of NAS, which can be subdivided into early and late
onset NAS with different aetiologies [49]. In a series of 397 liver transplants, primary
sclerosing cholangitis (PSC) was identified as a primary risk factor for NAS. When excluding
PSC patients, early NAS (<1 year) were associated with perioperative variables such as high
MELD score, increasing donor age and identical ABO status of donor and recipient. By
contrast, late NAS (>1 year) were associated with immunological variables [49]. PRLI was not
analysed in this study.
The contribution of biliary injury to subsequent biliary complications has little mention in the
literature and is difficult to quantify given the significant number biliary complications that
arise due to other causes. The causes of biliary complications are multifactorial including
technical issues (such as the type of reconstruction or presence of T-tube), perfusion-related
factors (such as overall perfusion quality or ischaemic injury due to prolonged ischaemia
times), HAT and DCD versus DBD procurement [47]. Overall the contribution of procurement
related biliary injury to biliary complications is likely to be very low.
Graft survival
There are few studies that examined graft survival rates with respect to PRLI, with only three
studies identified in this review each of which demonstrated no difference in survival
between injured and non-injured donor livers [9, 12, 14]. Nijkamp et al. [9] reported no
difference in 12-month graft survival rates in the presence of parenchymal (78% vs. 82%,
p=0.597) or arterial injuries (87% vs. 80%, p=0.398). Similarly, De Boer et al. [12] showed no
difference in 12-month graft survival rates comparing injured and non-injured livers (85.3%
vs 83.2%, p=0.740). In their series of warm-phase procured organs, Jung et al. [14] reported
no difference in graft survival at one or three years between injured and non-injured grafts
(83% and 78.7% vs. 83.3% and 83.3%, respectively, p=0.73). Boteon et al. [11] showed in DCD
liver transplants with a high or futile UK-DCD risk score, that PRLI increased the risk of graft

21
loss (OR 2.731, CI 1.452-162.274, p = 0.02), however this effect was not seen in the group with
a low UK-DCD risk score (OR 1.45, CI 0.490-4.293, p = 0.5) [11].
Rationale for study
This review represents the combined data of eight studies describing the issue of PRLI. Whilst
the methodology of obtaining and examining the available evidence we believe is sound and
reproducible, the heterogenous nature of the studies in terms of their design, geography,
method of data collection and time period of the study limits the ability to draw significant
conclusions from this review. Nonetheless there are a few points that one can take away from
this.
Firstly, PRLI is common. Admittedly there is a wide range of reported incidences of PRLI, from
1.4% in a large prospective registry analysis from the USA to 34% in a small retrospective
series from Europe. This raises questions on the definition of PRLI and how injuries are
recorded and data compiled to produce the studies that were examined. Whilst all the studies
examined in this review described a method for reporting injuries (usually a feedback form)
that formed the basis for the data collection, it is unclear exactly how the quality of those
forms is maintained. It is certainly possible that underreporting of injuries occurs, particularly
if the injuries might be considered of little consequence. Additionally, there may be instances
where significant injuries may not be reported if, for example, the procuring surgeon has
repaired the injury and the transplanting surgeon is satisfied with the repair and there exists
a culture where a relaxed attitude to organ injury that may limit the threshold for reporting.
On the other hand, it is also possible for over-reporting of injuries to occur. For instance, a
feedback form may be more likely to be completed in the case where an injury has occurred
compared to if no injury occurs. If no feedback form is completed, then these non-injured
cases may be excluded from a series leading to a reduction in the number of total cases
studied, but by consequence leading to a falsely elevated perceived injury rate.
Secondly, PRLI is likely to have an impact on the subsequent transplant. Whilst this may not
be true for all injuries, vascular injuries and large parenchymal injuries appear to have an
increased risk of complications. Interestingly, the majority of studies that reported on patient

22
and graft survival did not demonstrate any significant difference between transplants with or
without PRLI. The exception being specifically for high-risk DCD livers, where PRLI appears to
increase the risk of graft loss. Overall this is a reassuring finding, and suggests that when PRLI
do occur and in spite of an increased rate of complications, the graft survival is generally
unaffected by the presence of PRLI. Indeed, the success of transplantation is multifactorial
and perhaps there are other more important factors impacting on graft survival that outweigh
the impact due to PRLI.
Thirdly, risk factors for PRLI have been identified. Aberrant anatomy and DCD procurement
were identified as risk factors, and this observation in itself has value in identifying ways to
prevent PRLI – such as pre-donation imaging to identify aberrant vascular anatomy, or
appropriate dissection techniques to evaluate such anatomy. However, it was surprising that
factors related to the donor (e.g. age or BMI), or surgeon experience were not confidently
identified as risk factors for PRLI, even though they have been identified as risk factors for
injury in renal and pancreatic procurement. Again, this potentially relates to quality and
availability of data. Whilst the smaller retrospective studies showed non-significant trends
towards risk factors for PRLI, the larger registry studies lacked the detailed data to
demonstrate such relationships.
The majority of studies included in this review derive from countries within the
Eurotransplant network while the two large registry studies were from the UK and USA. Whilst
the author is satisfied that this represents the available literature on the topic, admittedly,
this has implications for applying the results externally and should be interpreted as such. In
addition, half of the studies included in this review are more than ten years old. With this in
mind, and accepting that liver injuries are common and consequential, then there is a real
need for further contemporary and well executed studies where data is collected in a
prospective and intentional manner to better characterise PRLI and how to best prevent and
manage it.

23
Hypotheses
1. PRLI is a common and relevant issue in liver transplantation.
2. PRLI has an impact on the outcome of subsequent transplantation.
3. There are potentially modifiable risk factors for PRLI that may be used as a target to
prevent injury and to improve the success of transplantation.

24
Methods
The Victorian Liver Transplant Unit database was searched for all deceased liver donors
offered for transplantation of a whole liver in Victoria from 01 January 2010 to 31 December
2017, including donor offers from interstate and New Zealand. Donors were included if they
resulted in a whole liver transplantation in the Victorian Liver Transplant Unit, which performs
liver transplantation at the Austin and Royal Children’s Hospitals in Melbourne. Adult and
paediatric recipients were included in the study. The database was separately examined for
donors where the whole liver was declined owing to surgical damage during procurement.
Donors were subsequently included in the study if an accompanying organ retrieval report
form (ORRF) was available and were excluded if not. Split and reduced donor livers were
excluded. Whole donor livers exported from Victoria for transplantation interstate or New
Zealand were also excluded.
Information regarding donor demographics, comorbidities, ethnicity, cause of death,
referring hospital, logistical arrangements, concomitant procurement of other organs, time
of surgery and retrieval team were sought from the database. Mode of donation via DBD or
DCD pathway was obtained. Donor hospitals were classified as from metropolitan Melbourne,
regional Victoria or Tasmania or from Interstate/New Zealand. Retrieval teams were classified
as Victorian or non-Victorian. “In hours” operating for the donor surgery was defined as
starting at or after 6:00 am and finishing prior to 6:00 pm.
The Victorian Liver Transplant Unit employs a number of consultant surgeons trained in
retrieval surgery who perform the majority of retrieval operations. Fellows (with a General
Surgery Fellowship qualification) and registrars (training towards a General Surgery
Fellowship qualification) may be trained to perform retrieval operations during their
appointment to the unit and may perform the retrieval operations as the primary surgeon
either with a consultant assisting or (for fellows) independently as their experience
progresses. For the purposes of this study, surgeon experience was defined in two ways – by
“experience” and “level”. Surgeon “experience” was calculated as the number of donor
operations recorded on the database by the senior-most surgeon present prior to the index
surgery, regardless of who was the primary surgeon. Surgeon “level” was defined as the level
25
of seniority of the primary surgeon (Consultant, Fellow or Registrar) as recorded in the
database regardless of the number of previous donor operations performed or level of the
assistant surgeon. This aimed to distinguish between experience of the most senior surgeon
present and experience of the primary surgeon.
PRLI was defined as an iatrogenic and macroscopic injury to the parenchyma, vasculature or
biliary system of the donor liver that occurred during the organ retrieval process as a
consequence of the surgery or the surgical technique. The definition did not include
microscopic or biochemical injuries such as those related to ischaemia or perfusion
techniques. Information regarding injuries to the donor liver were sought from the ORRF and
the operation notes from the transplant. ORRFs have sections to be filled out by both the
procurement surgeon and the transplanting surgeon. The procuring surgeon’s section
describes the quality of the liver, any aberrant anatomy or surgical damage. The transplanting
surgeon’s section includes any issues or injuries not identified by the procuring surgeon.
When an injury is identified it is graded according to the “outcome” of how the injury was
managed by the transplanting surgeon, and the anticipated “impact” of the injury. Outcome
at transplantation was documented on a scale of 1-4 as follows: 1: Transplanted without
modification or repair, 2: Transplanted after modification or repair, 3: Discarded unrelated to
the injury, 4: Discarded due to the injury. Impact of injury was documented on a scale from
1-4 as follows: 1: No impact, 2: Possible significant impact, 3: Probable significant impact, 4:
Definite significant impact. An example of a completed ORRF form is included in figure 2.
Complications including bleeding, hepatic arterial thrombosis (HAT), bile leak, development
of anastomotic or non-anastomotic biliary strictures were obtained from the Victorian Liver
Transplant Unit database and from the Austin Surgical Audit Program. These databases are
updated prospectively and are each reviewed at a weekly consultant-led unit meetings.
Bleeding was defined as requiring an intervention for post-operative haemorrhage (such as
laparotomy or radiological intervention), or where a haematoma was discovered on imaging
but managed conservatively. HAT was defined as complete occlusion of flow on imaging of
the common hepatic artery, hepatic artery proper, or the right or left hepatic arteries. Both
early (<3 months) and late HAT were included in the definition. Bile leaks were defined as
perioperative leaks and leaks that occurred after transcystic biliary tube removal. However,

26
since the occurrence of perioperative leaks was so rare (occurring in one case), for statistical
purposes these were grouped together.
Statistical analysis was performed using SPSS version 24. Continuous variables were analysed
using Mann-Whitney U Test and categorical variables using Chi-square and Fisher exact tests.
Receiver operating characteristic (ROC) curves and Youden J statistic were used to calculate
points of discrimination for continuous variables that may predict risk of PRLI. Variables with
P value <0.10 on univariate analysis were then assessed for independent significance using
multivariate logistic regression. Survival was calculated using Kaplan-Meier curves and
compared using log-rank. Ethics approval was obtained from the Australian Red Cross Blood
service (Ref: 22052018) and the Austin Health Human Research Ethics Committee (Ref:
LNR/18/Austin/144).

27
Figure 2. Example of Organ Retrieval Report Form

28
Results
Donor characteristics
There was a total of 639 offers of donor livers accepted for whole liver transplantation in
Victoria from 1 January 2010 to 31 December 2017. During this period there was a single case
(0.16%) of an accepted offer being declined during the procurement owing to PRLI from an
interstate donor and a non-Victorian retrieval team. Unfortunately, neither an ORRF form or
operation notes were able to be retrieved and the case was subsequently excluded from
further analysis. Other reasons for declining the liver at procurement were for steatosis or
cirrhosis (101), DCD not progressing within timeframe (16), poor perfusion (10), malignancy
(4), other donor issues (19), logistical issues (3) and not recorded (17). The remaining 468
donors resulted in whole liver transplants in Victoria of which there was a total of 420
accompanying ORRF forms (90% return rate) which were included for analysis. Donor
characteristics are shown in table 3. There were 34 DCD donors that resulted in liver
transplantation over the study period, equivalent to 8.1% of whole liver donors. Thirty-six
donors (8.6%) resulted in whole liver paediatric transplantation. Donor cause of death was by
stroke in 49%. Trauma, hypoxia and other causes accounted for 12%, 13% and 25%,
respectively.
Donor surgery logistics and surgeon experience
The majority of donor livers were from metropolitan Melbourne, accounting for 285 donors
(68%). Ninety donor livers (21%) were from regional Victoria or Tasmania, with the remaining
45 donor livers (11%) imported from interstate Australia (other than Tasmania) or New
Zealand. The Austin retrieval team performed 378 (90%) liver retrievals, with the majority
(73%) being performed “in hours”. A charter flight was required in 67 retrievals (17%). The
mean duration of procurement surgery was 3 hours 16 minutes (S.D. 2 hours 0 minutes). Liver
was procured in combination with kidneys (94%), pancreas (47%), and intestine (1.3%). A
thoracic procurement team was present in 47% of cases. The mean number of cases for
surgeon experience was 181. Consultants were the primary operators in the majority of
procedures, accounting for 68%. Fellows and registrars accounted for 22% and 11% of primary
operators respectively. These are shown in table 3.

29
Table 3. Donor and surgery characteristics
Characteristic Mean or number (n=420)
SD or per cent Characteristic Mean or number (n=420)
SD or per cent
Age (years) 44 18 Donor location Gender Metropolitan 285 68% Male 231 55% Regional Victoria + Tasmania 90 21% Female 188 45% Interstate + New Zealand 24 11% Height (cm) 169 15 Retrieval team
Weight (kg) 74 18 Victorian team 378 90% BMI (kg/m2) 26 5 Non-Victorian team 42 10% Smoker Charter flight used 67 16% Current 221 55% Performed in hours 244 73% Non-smoker 141 35% Duration of surgery (hours/mins) 3h 16m 2h 0m Ex-smoker 38 10% Combined procurement Diabetic 25 6.1% Kidney retrieved 354 94% DCD 34 8.1% Pancreas retrieved 177 47% Ethnicity Intestine retrieved 5 1.3% Caucasian 276 86% Thoracic procurement 199 47% Asian 31 10% Surgeon experience (cases) 181 114 Pacific Islander 8 2.5% Primary surgeon level
South American 3 0.9% Registrar 41 11% Aboriginal / TSI 2 0.6% Fellow 81 22% Cause of death Consultant 254 68% Stroke 206 49% Anoxia 56 13% Trauma 52 25% Other 106 25%
BMI: body mass index, DCD: donation after circulatory death, TSI: Torres Strait Islander

30
Anatomical variation
Of the 420 donor livers, aberrant anatomy was described in 105 cases (25%) With the
exception of one case describing two hepatic veins, all referred to variations in arterial
anatomy. The difference between accessory and replaced arterial anatomy was not
distinguishable on the ORRF or the operation report and was therefore described as
“aberrant”. The frequencies of aberrant anatomy are shown in table 4.
Injuries
There were 46 injuries documented in 45 donor livers, representing an injury rate of 10.7%.
Of these, there were 23 parenchymal injuries, 22 vascular injuries and one biliary injury,
including one case where both a vascular and biliary injury occurred in the same donor liver.
These are shown in table 4.
Table 4. Variant hepatic anatomy and liver injuries
*Other anomalies included three instances where the common hepatic artery arose from the superior mesenteric
artery, two instances where the coeliac and superior mesenteric arteries had a common origin from the aorta,
and a single case of two hepatic veins. **Denotes one liver with a combined vascular and biliary injury
Anatomical Variation Frequency Percentage
Left only aberrant hepatic artery 49 11.7%
Right only aberrant hepatic artery 32 7.6%
Right and left aberrant arteries 18 4.3%
Other anomalies * 6 1.4%
Total 105 25%
Injury Type Number Percentage
Parenchymal 23 5.5%
Vascular 22 5.2%
Biliary 1 0.2%
Total injured livers 45** 10.7%
31
Risk factors for PRLI
Donor age, gender, weight, height and BMI were not found to be associated with presence of
PRLI (see table 5). No significant association was found between PRLI and a donor history of
smoking, diabetes or cause of death. Logistical factors such as geographical location of donor,
retrieval team, usage of charter flights or out-of-hours surgery had no impact on the risk of
PRLI. DCD retrieval had a higher incidence of PRLI than DBD retrieval, however this was not
statistically significant (17.6% vs. 9.8%, p= 0.131). There was no increased or decreased risk
of PRLI when the liver was procured in combination with kidney, pancreas, intestine or when
a thoracic procurement team was present.
Presence of anatomical variation was found to significantly increase the risk of iatrogenic PRLI
(21% vs. 7%, p<0.001). Increased surgeon experience was found to decrease the risk of PRLI.
A ROC analysis of surgeon experience compared with injury resulted in an AUC (area under
curve) of 0.610, p=0.023. The Youden index was found to be 171.5 cases. Thus, surgeon
experience was dichotomised into a “low-volume” group of less than 172 cases, and a “high-
volume” group of greater than or equal to 172 cases. The low-volume group had a significantly
increased risk of PRLI compared with the high-volume group (15% vs. 5%, OR 3.511, p < 0.01).
When comparing the level of primary surgeon, registrars were found to have a higher rate of
PRLI compared to consultants and fellows, but this did not achieve significance.
A multivariate logistic regression analysis was performed for all variables with p <0.10.
Anatomical variation and surgeon experience as defined by category of volume remained
significant (see table 6a). A univariate subgroup analysis of injury type (vascular or
parenchymal) was performed for the two categories that were significant on multivariate
analysis - anatomical variation and surgeon experience. Anatomical variation was found to
increase the risk of vascular injury but not parenchymal injury. For surgical experience,
parenchymal injury was found to be at increased risk, but not vascular injury (see table 6b).

32
Table 5. Associations with PRLI - univariate analysis
BMI: body mass index, DCD: donation after circulatory death, DBD: donation after brain death, VIC: Victoria, TAS:
Tasmania, NZ: New Zealand, Ref: reference variable, * mean +/-SD, or number (%).
Variable With injury * No injury * Odds ratio Confidence interval p
Age (years) 41 +/-18 45 +/-18 0.990 0.973-1.007 0.23 Gender Male 23 (10%) 208 (90%) 0.839 0.452-1.559 0.58 Female 22 (12%) 166 (88%) Ref. - - Height (cm) 169 +/-16 169 +/-14 0.999 0.978 – 1.020 0.90 Weight (kg) 78 +/-21 74 +/-18 1.013 0.995 – 1.030 0.16 BMI (kg/m2) 27.1 +/-6 25.7 +/-5 1.051 0.992 – 1.113 0.09 Smoking status Current 24 (11%) 197 (89%) 0.969 0.512 – 1.940 0.99 Ex-smoker 4 (11%) 34 (89%) 0.887 0.288 – 2.930 0.89 Non-smoker 16 (11%) 125 (89%) Ref. - - Diabetes Present 1 (4%) 24 (96%) 0.323 0.043 – 2.446 0.27 Not present 44 (11%) 341 (89%) Ref. - - Ethnicity Caucasian 31 (11%) 245 (89%) 0.801 0.313 – 2.049 0.64 Non-Caucasian 6 (14%) 38 (86%) Ref. - - Cause of death Stroke 20 (10%) 186 (90%) 1.900 0.544 – 6.639 0.32 Anoxia 3 (5%) 53 (95%) Ref - - Trauma 7 (14%) 45 (86%) 1.392 0.585 – 3.308 0.45 Other 15 (14%) 91 (86%) 2.748 0.671 – 11.252 0.16 Withdrawal pathway DCD procurement 6 (18%) 28 (82%) 1.907 0.743 – 4.890 0.18 DBD procurement 39 (10%) 347 (90%) Ref. - - Paediatric donor Paediatric donor 3 (9%) 29 (91%) 0.852 0.249 – 2.919 0.80 Adult donor 42 (11%) 346 (89%) Ref. - - Anatomical variation Present 22 (21%) 83 (79%) 3.365 1.786 – 6.339 <0.001 Absent 23 (7%) 292 (93%) Ref - - Combined renal 38 (11%) 316 (89%) 1.323 0.299 – 5.847 0.71 Combined pancreas 21 (12%) 156 (88%) 1.289 0.669 – 2.486 0.45 Combined thoracic 24 (12%) 175 (88%) 1.306 0.703 – 2.427 0.40 Charter flight used 6 (9%) 61 (91%) 0.774 0.313 – 1.911 0.58 Surgery time of day In hours 27 (11%) 218 (89%) 1.306 0.571 – 2.991 0.53 Out of hours 8 (9%) 84 (91%) 0.774 0.313 – 1.911 0.59 Duration of surgery 3h17m 3h16m 1.000 1.000 – 1.000 0.98 Donor hospital Metropolitan Melbourne 31 (11%) 254 (89%) Ref. - - Regional VIC + TAS 9 (10%) 81 (90%) 0.910 0.416 – 1.992 0.81 Interstate / NZ 5 (11%) 40 (89%) 1.024 0.376 – 2.789 0.96 Retrieval team Victorian team 40 (11%) 338 (89%) 0.876 0.326 – 2.356 0.79 Non-Victorian team 5 (12%) 37 (88%) Ref. - - Surgeon experience (cases) 142 +/-99 186 +/-115 0.996 0.993 – 1.000 0.03 Surgeon experience Low volume <172 32 (15%) 180 (85%) 3.511 1.572 – 7.843 <0.01 High volume ≥172 8 (5%) 158 (95%) Ref. - - Primary surgeon level Registrar 8 (20%) 33 (80%) 2.323 0.964 – 5.598 0.06 Fellow 8 (10%) 73 (90%) 1.050 0.452 – 2.438 0.90 Consultant 24 (9%) 230 (91%) Ref. - -

33
Table 6a. Multivariate analysis
Univariate factor Injury with variable
Injury without variable Odds ratio Confidence
interval p
Anatomical variation 22 (21%) 23 (7%) 3.68 1.84 – 7.35 <0.001
Surgeon experience
(<172 cases) 32 (15%) 8 (5%) 5.96 1.28 – 27.51 0.02
Registrar 8 (20%) 32 (11%) 1.80 0.72 – 4.49 0.21
Table 6b. Univariate subgroup analysis
Donor or logistic variable
Injury with variable
Injury without variable Odds ratio Confidence
interval p
Anatomical variation 22 (21%) 23 (7%) - - -
Vascular injury 12 (11%) 9 (3%) 4.80 1.99 – 11.60 <0.001
Parenchymal injury 9 (9%) 14 (4%) 2.02 0.85 – 4.80 0.11
Surgeon experience
(<172 cases) 32 (15%) 8 (5%) - - -
Vascular injury 13 (6%) 7 (4%) 1.48 0.58 – 3.81 0.41
Parenchymal injury 19 (9%) 1 (0.6%) 16.24 2.15 – 122.64 <0.01
Surgical “outcome” and expected “impact” of PRLI
Of the 45 injured livers, surgical “outcome” was classed as level 1 (transplanted without need
for modification or repair) in 31 injuries (69%) and level 2 (transplanted after modification or
repair) in 14 (31%). Vascular injuries were more likely to be level 2 than parenchymal injuries
(59% vs. 4.3%, p<0.001). Injuries with level 2 outcome had a decreased graft survival at 3
months, however graft survival at 1 month and 12 months were not statistically different (see
table 7). Of the level 2 surgical “outcomes” there were three cases of early graft loss that
contributed to the decreased survival at 3 months. Two had injured accessory right hepatic
arteries – one developed hepatic artery thrombosis and was retransplanted, and the other

34
developed septic complications to which they succumbed. The third recipient had an injured
accessory left hepatic artery but was retransplanted due to an incidental neuroendocrine
tumour identified in the graft which was unrelated to the injury.
Expected “impact” was level 1 (no impact) in 27 (60%) and level 2 (possible significant impact)
in 18 (40%). There were no cases of PRLI that were described at higher levels (probable and
definite significant impact). Vascular injuries were more likely to be described as level 2 than
parenchymal injuries (77.3% vs 4.3%, P<0.001). There was no significant difference based on
degree of impact on graft survival at 1, 3 or 12 months (see table 7).
Table 7. Surgical outcome and expected impact of PRLI vs survival
Survival parameter No injury n=375
Organ transplanted without need for
repair or modification
n=31
Organ transplanted after repair or modification
n=14
p
1-month graft survival 94.4% 100.0% 85.7% 0.142
3-month graft survival 93.3% 100.0% 78.6% 0.028
12-month graft survival 86.7% 90.3% 78.6% 0.562
Survival parameter No injury n=376
No expected impact n=27
Possible significant impact n=17
p
1-month graft survival 94.4% 100.0% 88.9% 0.26
3-month graft survival 93.3% 100.0% 83.3% 0.09
12-month graft survival 86.7% 88.9% 83.3% 0.866
35
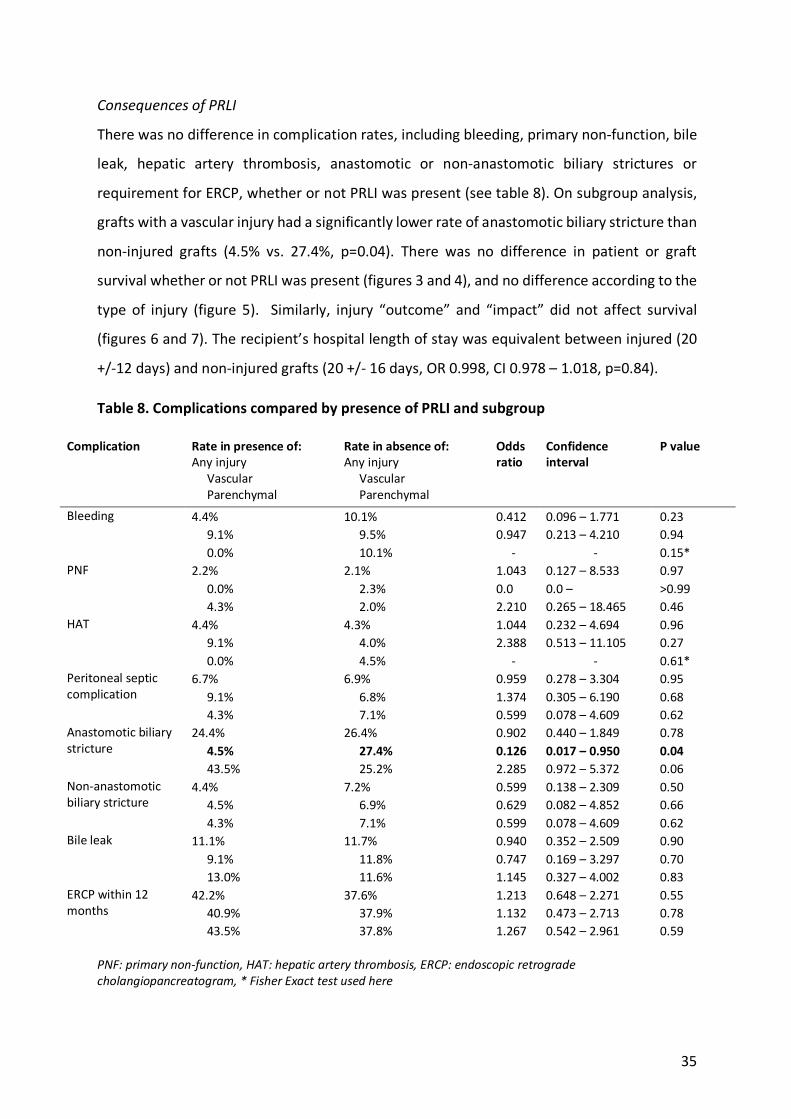
Consequences of PRLI
There was no difference in complication rates, including bleeding, primary non-function, bile
leak, hepatic artery thrombosis, anastomotic or non-anastomotic biliary strictures or
requirement for ERCP, whether or not PRLI was present (see table 8). On subgroup analysis,
grafts with a vascular injury had a significantly lower rate of anastomotic biliary stricture than
non-injured grafts (4.5% vs. 27.4%, p=0.04). There was no difference in patient or graft
survival whether or not PRLI was present (figures 3 and 4), and no difference according to the
type of injury (figure 5). Similarly, injury “outcome” and “impact” did not affect survival
(figures 6 and 7). The recipient’s hospital length of stay was equivalent between injured (20
+/-12 days) and non-injured grafts (20 +/- 16 days, OR 0.998, CI 0.978 – 1.018, p=0.84).
Table 8. Complications compared by presence of PRLI and subgroup
Complication Rate in presence of: Any injury Vascular Parenchymal
Rate in absence of: Any injury Vascular Parenchymal
Odds ratio
Confidence interval
P value
Bleeding 4.4% 10.1% 0.412 0.096 – 1.771 0.23 9.1% 9.5% 0.947 0.213 – 4.210 0.94 0.0% 10.1% - - 0.15*
PNF 2.2% 2.1% 1.043 0.127 – 8.533 0.97 0.0% 2.3% 0.0 0.0 – >0.99 4.3% 2.0% 2.210 0.265 – 18.465 0.46
HAT 4.4% 4.3% 1.044 0.232 – 4.694 0.96 9.1% 4.0% 2.388 0.513 – 11.105 0.27 0.0% 4.5% - - 0.61*
Peritoneal septic complication
6.7% 6.9% 0.959 0.278 – 3.304 0.95 9.1% 6.8% 1.374 0.305 – 6.190 0.68 4.3% 7.1% 0.599 0.078 – 4.609 0.62
Anastomotic biliary stricture
24.4% 26.4% 0.902 0.440 – 1.849 0.78 4.5% 27.4% 0.126 0.017 – 0.950 0.04 43.5% 25.2% 2.285 0.972 – 5.372 0.06
Non-anastomotic biliary stricture
4.4% 7.2% 0.599 0.138 – 2.309 0.50 4.5% 6.9% 0.629 0.082 – 4.852 0.66 4.3% 7.1% 0.599 0.078 – 4.609 0.62
Bile leak 11.1% 11.7% 0.940 0.352 – 2.509 0.90 9.1% 11.8% 0.747 0.169 – 3.297 0.70 13.0% 11.6% 1.145 0.327 – 4.002 0.83
ERCP within 12 months
42.2% 37.6% 1.213 0.648 – 2.271 0.55 40.9% 37.9% 1.132 0.473 – 2.713 0.78 43.5% 37.8% 1.267 0.542 – 2.961 0.59
PNF: primary non-function, HAT: hepatic artery thrombosis, ERCP: endoscopic retrograde
cholangiopancreatogram, * Fisher Exact test used here

36
Figure 3. Patient survival compared by injury
Figure 4. Graft survival compared by injury

37
Figure 5. Graft survival compared by type of injury
Figure 6. Graft survival compared by surgical “outcome” of injury at transplant

38
Figure 7. Graft survival compared by expected “impact” of injury

39
Discussion
The objective of this study was to describe the epidemiology of PRLI as experienced at the
Victorian Liver Transplant Unit, identify risk factors for PRLI and to recognise any impact that
may be attributed to PRLI. This is to our knowledge the most detailed analysis on the topic of
PRLI. This study examining a cohort of 420 whole-liver transplants over eight years
demonstrates that PRLI is a relatively common phenomenon, occurring in just over one in ten
transplants. This is consistent with the reported incidence of PRLI in the literature which
ranges from 1.8 – 34%.
The incidence of PRLI is potentially subject to issues of under-reporting and to a lesser extent,
over-reporting. Under-reporting can occur either as a deliberate event when recognised or
non-deliberate if unrecognised. The reasons for deliberately not reporting an injury would be
if it were deemed non-significant, such as a small capsular injury that required no treatment,
or in the case of a significant injury which requires repair or modification, there may be a
motivation to conceal the injury. As the ORRF form is completed by two surgeons (the
procuring surgeon and the transplanting surgeon), it is more difficult to conceal a significant
injury and given there is no specific disincentive (financial or other) to report injuries, we feel
that under-reporting for significant injuries is not likely to be an important issue in our study.
Over-reporting of injuries is also worth consideration. In this study, 60% of injuries were
considered to be of “no impact” to the transplantation, and 69% were transplanted without
need for repair or modification. These categories are assigned by the transplanting surgeon
after transplantation has occurred, however the injuries can be documented by either of the
procuring surgeon and the transplanting surgeon. The transplanting surgeon is better suited
for describing the severity of the PRLI, as it can be best assessed at completion of the
operation. The procuring surgeon does not have this insight at the completion of the
procurement operation and may describe issues to alert the transplanting surgeon which may
eventually turn out not to be significant. Thus, while less experienced surgeons may be more
inclined to over-report non-significant issues, it is also possible that with more experience,
procurement surgeons may be less likely to document injuries that he or she considers to be
insignificant. This raises the question as to the definition of PRLI that requires reporting, and
at what point the threshold needs to be reached in order to call something an injury. Another
possible mechanism for over-reporting may be attributed an artificially high proportion of

40
ORRF forms completed due to the presence of PRLI. A transplanting surgeon is potentially
more likely to complete an ORRF if an injury has occurred, and therefore if ORRF forms from
non-injured grafts are not completed there is a reduction in the total number of completed
forms (or the denominator), leading to an apparent increase in the rate of reported PRLI. In
this study there was a 90% completion rate for ORRFs. If all of the missing forms were from
transplants where there was no PRLI, then the incidence of PRLI would drop from 10.7% to
9.6% in this study, which is unlikely to be of significance.
Aberrant anatomy and surgeon experience were identified as risk factors for PRLI in this
study. Donor age, gender, height, weight, BMI, race, smoking status or history of diabetes did
not affect the risk of PRLI. This is consistent with previous studies which have failed to identify
risk factors related to the donor. Equally, surgical factors such as procurement in combination
with other abdominal or thoracic organs, or logistic factors such as time of day, duration of
surgery, import status or geographical location were not associated with PRLI.
Aberrant vascular anatomy was identified as a strong risk factor for PRLI and on subgroup
analysis this was significant for vascular injury. Clearly this is an expected result. Of note, these
injuries were more likely to be found significant in terms of the surgical “outcome” and
expected “impact” of the injury. Identification of aberrant anatomy is part of the surgical
technique during procurement surgery. Given the majority of vascular injuries occur in the
presence of aberrant anatomy, strategies to prevent PRLI should be considered. Better
training and awareness of aberrant anatomy could potentially reduce the number of vascular
injuries; however, surgeon experience was not identified as a risk factor for vascular injury in
this study. Preoperative liver angiography by cross-sectional imaging is not routinely
employed for the assessment of whole-liver donors, however it may be performed for other
reasons related to the hospital admission of the donor. The question as to whether
preoperative liver angiography reduces the risk of vascular injury in the presence of aberrant
vascular anatomy is beyond the scope of this study. However, it would be worth considering
the routine use of CT angiography to help alert the surgeon toward the presence of aberrant
anatomy, although the benefit of such would need to be balanced against the risk of causing
contrast nephropathy in donor kidneys.

41
Surgeon experience was also identified as a risk factor for PRLI. This is the first instance as far
as the author is aware, in which a study has demonstrated a relationship between surgeon
experience and risk of PRLI. In this study, experience was measured in two ways. Firstly, by
directly measuring the number of procedures performed by the most senior surgeon present
at the operation prior to the operation in question and secondly by the “level” or qualification
of the primary operating surgeon. Both methods demonstrated a higher rate of PRLI with
lesser experience, however statistical significance was achieved only by the number of
procedures performed by the most senior surgeon present, after dichotomising into a high
experience and a low experience group. This is relevant in that it appears that the overall
experience of the surgical team is more relevant than the level of experience of the primary
surgeon and implies safety in training junior surgeons, so long as a suitably experienced
surgeon is present at the procurement. This then leads to the question as to how much
experience is required before a surgeon performs liver procurement without supervision. It
was interesting to note that the cut-off calculated between “low” and “high” levels of
experience at which point that rate of injuries dropped significantly, was in itself quite high at
172 procedures. Of course, this result does not imply that surgeons need to acquire 172
procedures before they are deemed proficient. Whilst the calculation of surgical learning
curves for procurement surgery was beyond the initial scope proposed in this study, that
would be a valuable question to be addressed in future studies.
Whilst surgeon experience was a relevant risk factor for PRLI, it was relevant only for
parenchymal injuries. These were more likely to score lower with regards to the surgical
“outcome” and expected “impact” of the injury. It is unclear why less significant injuries are
more likely to occur with less experience, and more significant injuries are not affected by
experience. One possible explanation is that avoidance of significant injuries is addressed
early in the training, and that the presence of minor injuries reduces as the technique is
mastered. Alternatively, as discussed earlier, it is possible that less experienced surgeons may
be more inclined to document minor issues than more experienced surgeons.
DCD procurement was found to have a higher rate of PRLI than DBD procurement in this
study, however the difference was not statistically significant. This is in contrast to the study
by Ausania et al. [5] which showed a significantly higher rate of parenchymal injuries in the

42
DCD group. The study by Ausania et al. has 7,000 procured livers compared with 420 in the
current study, which is the most likely explanation for this point of difference. Other possible
explanations for why this study did not demonstrate a difference between DBD and DCD
retrieval include: 1. In DCD the cannulation occurs remotely from the liver and then the
removal of the liver is essentially the same as a DBD, 2. DCDs are less likely to be pancreas
donors, reducing the complexity, 3. (related to 2) the SMA and CA can be procured en bloc
with the liver ensuring that an aberrant hepatic artery is not transected. Of note, the study
by Ausania et al. did not show any increased rate of organ discard attributed to the PRLI, nor
did it demonstrate that PRLI in the context of DCD retrieval had an impact on the subsequent
transplant in addition to the effects attributed to warm ischaemia.
Consequences of PRLI were measured in two ways in this study – according to rates of
complications and according to survival curves. Broadly speaking, the available literature has
not reported any differences for graft survival or patient survival with respect to PRLI and this
was replicated in this study. Furthermore, we found no difference in survival with respect to
the type of injury (vascular vs parenchymal) or the magnitude of the injury as described by
the expected “impact”. On the other hand, we observed a difference in graft survival at 3
months between injuries that required “repair or modification” compared with either no
injury, or injuries transplanted without repair or modification, and that two out of the three
graft losses were attributed to the injury. Of note, the difference in survival did not persist at
the 12-month mark, and reviewing the corresponding Kaplan-Meier survival curves, it
appears that after an early drop-off in graft survival in the group requiring “repair or
modification”, survival after 12 months was similar. Thus, it is possible to argue on the basis
of these results that significant PRLI influences early graft survival, but not long-term graft
survival.
This study showed no difference in the overall rates of complications in the presence of PRLI.
Similarly, no difference was observed for bleeding, PNF, HAT, peritoneal infections, biliary
strictures, bile leaks or the requirement for post transplantation ERCP. This is a reassuring
finding and implies that when injuries occur, they are managed in an appropriate way such
that an increase in complication rates is not observed. The exception to these results was
observed in the subgroup analysis of vascular injuries which were associated with a

43
significantly lower rate of anastomotic biliary strictures (4.5% in the presence of a vascular
injury vs 27.4% in its absence, p = 0.04). This is an unexpected finding, and it is difficult to
explain why vascular injury would be protective against anastomotic biliary strictures.
Vascular injuries were observed to be more frequent in the presence of aberrant anatomy,
and it is possible that aberrant anatomy may be associated with biliary anatomy that is more
favourable to a successful biliary anastomosis. However, noting the relatively weak p-value,
we believe this finding is more likely related to chance.
In this study, there was no significant difference in HAT despite the presence or absence of
injury. This contrasts with the studies by Nijkamp et al. [9] and Ausania et al. in their 2012
study [8] which demonstrated a higher risk of HAT in the presence of vascular injury. We did
note an increased rate of HAT in the presence of vascular injury (9.1% vs 4.0%, p = 0.27)
however this did not reach statistical significance. It is noted that Ausania et al. had roughly
twice the number of liver transplants in their series [8] compared with the current study, and
this may explain the difference in HAT rates and survival that were observed. Alternatively,
vascular reconstruction in response to injury in the current cohort may be sufficient to
prevent the occurrence of HAT.

44
Conclusion
This study demonstrates the occurrence of PRLI to be relatively common at approximately
11% of procurements which is consistent with the reported literature. Aberrant vascular
anatomy and surgeon experience were both found to impact on risk of PRLI. Other donor
factors and logistical factors related to the procurement process were not found to affect the
risk of injury. PRLI overall did not impact on patient or graft survival or on the incidence of
complications. However, in injuries that required repair or modification, a reduced early graft
survival at 3 months post transplantation was observed. This difference was no longer
significant after 12 months.

45
References
1. Fox, A.N. and R.S. Brown, Jr., Is the patient a candidate for liver transplantation? Clin Liver Dis, 2012. 16(2): p. 435-48.
2. ANZLT Registry 29th Report, S.V. Lynch and G.A. Balderson, Editors. 2017, Australia and New Zealand Liver Transplant Registry: Brisbane, QLD, Australia.
3. Brockmann, J.G., et al., Retrieval of abdominal organs for transplantation. Br J Surg, 2006. 93(2): p. 133-46.
4. Feng, S., et al., Characteristics associated with liver graft failure: the concept of a donor
risk index. Am J Transplant, 2006. 6(4): p. 783-90.
5. Ausania, F., et al., Liver damage during organ donor procurement in donation after
circulatory death compared with donation after brain death. Br J Surg, 2013. 100(3): p. 381-6.
6. Taber, T.E., et al., Deceased donor organ procurement injuries in the United States. World J Transplant, 2016. 6(2): p. 423-8.
7. Soliman, T., et al., Parenchymal liver injury in orthotopic liver transplantation. Transplantation, 2000. 69(10): p. 2079-2084.
8. Ausania, F., et al., Clinical impact of right accessory hepatic artery injury in deceased
donor livers. J Hepatobiliary Pancreat Sci, 2012. 19(6): p. 656-60.
9. Nijkamp, D.M., et al., Surgical injuries of postmortem donor livers: incidence and
impact on outcome after adult liver transplantation. Liver Transpl, 2006. 12(9): p. 1365-70.
10. Lerut, J., et al., Technical problems in shipped hepatic allografts: the UCL experience. Transpl Int, 1994. 7(4): p. 297-301.
11. Boteon, A., et al., Retrieval Practice or Overall Donor and Recipient Risk: What Impacts
on Outcomes After Donation After Circulatory Death Liver Transplantation in the
United Kingdom? Liver Transpl, 2019. 25(4): p. 545-558.
12. de Boer, J.D., et al., Abdominal organ procurement in the Netherlands - an analysis of
quality and clinical impact. Transpl Int, 2017. 30(3): p. 288-294.
13. Fernandez, E.D., et al., Technical complications in organ procurement. Transplant Proc, 2007. 39(10): p. 2975-6.
14. Jung, D.H., et al., Safety and usefulness of warm dissection technique during liver graft
retrieval from deceased donors. Transplant Proc, 2015. 47(3): p. 576-9.
15. Ackermann, J.R. and M.E. Snell, Cadaveric renal transplantation: a technique for donor
kidney removal. Br J Urol, 1968. 40(5): p. 515-21.
16. Alexandre, G.P., Organ procurement. Proc Eur Dial Transplant Assoc, 1973. 10(0): p. 31-56.
17. Shaw, B.W., Jr., et al., Techniques for combined procurement of hearts and kidneys
with satisfactory early function of renal allografts. Surg Gynecol Obstet, 1983. 157(3): p. 261-4.

46
18. Wright, F.H., et al., Combined retrieval of liver and pancreas grafts: alternatives for
organ procurement. Transplant Proc, 1989. 21(3): p. 3522.
19. Starzl, T.E., et al., A flexible procedure for multiple cadaveric organ procurement. Surg Gynecol Obstet, 1984. 158(3): p. 223-30.
20. Starzl, T.E., et al., An improved technique for multiple organ harvesting. Surg Gynecol Obstet, 1987. 165(4): p. 343-8.
21. Callaghan, C.J., et al., Outcomes of transplantation of livers from donation after
circulatory death donors in the UK: a cohort study. BMJ Open, 2013. 3(9): p. e003287.
22. Cao, Y., et al., Donation After Circulatory Death for Liver Transplantation: A Meta-
Analysis on the Location of Life Support Withdrawal Affecting Outcomes. Transplantation, 2016. 100(7): p. 1513-24.
23. Moore, E.E., et al., Organ injury scaling: spleen, liver, and kidney. J Trauma, 1989. 29(12): p. 1664-6.
24. di Francesco, F., et al., Reconstruction of the suprahepatic cuff injured during
multiorgan procurement using the infrahepatic vena cava of the liver allograft. Liver Transpl, 2007. 13(10): p. 1468-9.
25. Nicolini, D., et al., Technical solutions for venous outflow reconstruction in damaged
liver grafts during procurement: case reports. Transplant Proc, 2008. 40(6): p. 1941-3.
26. Wigmore, S.J., et al., Kidney damage during organ retrieval: data from UK National
Transplant Database. Kidney Advisory Group. Lancet, 1999. 354(9185): p. 1143-6.
27. Ausania, F., et al., Kidney damage during organ recovery in donation after circulatory
death donors: data from UK National Transplant Database. Am J Transplant, 2012. 12(4): p. 932-6.
28. Peters, T.G. and W.K. Vaughn, Organs for transplantation: analysis of 27,000 cadaveric
donor organs. South Med J, 1990. 83(8): p. 889-92.
29. Smits, J.M., et al., The outcome of kidney grafts from multiorgan donors and kidney
only donors. Transplantation, 1996. 62(6): p. 767-71.
30. Vaughn, W.K., T.G. Peters, and E.K. Spees, Multiple organ procurement is not
detrimental to cadaveric kidney allograft function and survival. Transplant Proc, 1988. 20(5): p. 835-8.
31. Bunzendahl, H., et al., Combination harvesting procedure for liver and whole pancreas. Transpl Int, 1988. 1(2): p. 99-102.
32. Boggi, U., et al., A simplified technique for the en bloc procurement of abdominal
organs that is suitable for pancreas and small-bowel transplantation. Surgery, 2004. 135(6): p. 629-41.
33. Dunn, D.L., et al., Evidence that combined procurement of pancreas and liver grafts
does not affect transplant outcome. Transplantation, 1991. 51(1): p. 150-7.
34. Sterioff, S., et al., Pancreaticoduodenal allograft procurement in combination with
liver allograft procurement. Transplant Proc, 1989. 21(1 Pt 3): p. 2767-8.
35. Rosenthal, J.T., et al., Principles of multiple organ procurement from cadaver donors. Ann Surg, 1983. 198(5): p. 617-21.

47
36. Nghiem, D.D., Rapid exenteration for multiorgan harvesting: a new technique for the
unstable donor. Transplant Proc, 1996. 28(1): p. 256-7.
37. Belli, L.S., et al., Kidney and liver initial graft function under different procurement
techniques. Transplant Proc, 1989. 21(1 Pt 2): p. 1209-10.
38. Huber, O., et al., [1 year of multiple organ procurement using the Starzl technic of rapid
cooling: personal results]. Helv Chir Acta, 1989. 55(5): p. 623-8.
39. Margreiter, R., et al., Multiple organ procurement--a simple and safe procedure. Transplant Proc, 1991. 23(5): p. 2307-8.
40. Imagawa, D.K., et al., Rapid en bloc technique for pancreas-liver procurement.
Improved early liver function. Transplantation, 1996. 61(11): p. 1605-9.
41. Nakazato, P.Z., et al., Total abdominal evisceration: an en bloc technique for
abdominal organ harvesting. Surgery, 1992. 111(1): p. 37-47.
42. Reich, D.J. and J.C. Hong, Current status of donation after cardiac death liver
transplantation. Curr Opin Organ Transplant, 2010. 15(3): p. 316-21.
43. Busuttil, R.W. and K. Tanaka, The utility of marginal donors in liver transplantation. Liver Transpl, 2003. 9(7): p. 651-63.
44. Dubbeld, J., et al., Similar liver transplantation survival with selected cardiac death
donors and brain death donors. Br J Surg, 2010. 97(5): p. 744-53.
45. Lam, H.D., et al., Professionalization of surgical abdominal organ recovery leading to
an increase in pancreatic allografts accepted for transplantation in the Netherlands: a
serial analysis. Transpl Int, 2017. 30(2): p. 117-123.
46. Bekker, J., S. Ploem, and K.P. de Jong, Early hepatic artery thrombosis after liver
transplantation: a systematic review of the incidence, outcome and risk factors. Am J Transplant, 2009. 9(4): p. 746-57.
47. Gastaca, M., Biliary complications after orthotopic liver transplantation: a review of
incidence and risk factors. Transplant Proc, 2012. 44(6): p. 1545-9.
48. Ferraz-Neto, B.H., et al., Correlation between graft arterial anatomy and biliary
complications after liver transplantation. Transplant Proc, 2007. 39(8): p. 2514-5.
49. Howell, J.A., et al., Early-onset versus late-onset nonanastomotic biliary strictures post
liver transplantation: risk factors reflect different pathogenesis. Transpl Int, 2012. 25(7): p. 765-75.

Minerva Access is the Institutional Repository of The University of Melbourne
Author/s:
Walcott, James Clement Chrysogonus
Title:
Procurement-related liver injury: an analysis of the incidence, risk factors and consequences
at the Victorian Liver Transplant Unit
Date:
2020
Persistent Link:
http://hdl.handle.net/11343/241934
File Description:
Final thesis file
Terms and Conditions:
Terms and Conditions: Copyright in works deposited in Minerva Access is retained by the
copyright owner. The work may not be altered without permission from the copyright owner.
Readers may only download, print and save electronic copies of whole works for their own
personal non-commercial use. Any use that exceeds these limits requires permission from
the copyright owner. Attribution is essential when quoting or paraphrasing from these works.