mass medical care with scarce resources: the essentials
TRANSCRIPT
Mass Medical Care With Scarce
Resources: The Essentials
Tools and Models for Planning and Preparedness
Public Health Emergency Preparedness Research
Includes Chapter onInfluenza Pandemic Preparedness

Mass Medical Care With Scarce Resources: The Essentials
Editors
Sally J. Phillips, R.N., Ph.D. Public Health Emergency Preparedness Research Program Agency for Healthcare Research and Quality
RADM Ann Knebel, R.N., D.N.Sc., FAAN Office of Preparedness and Emergency Operations Office of the Assistant Secretary for Preparedness and Response
Kelly J. Johnson, M.P.H. Public Health Emergency Preparedness Research Program Agency for Healthcare Research and Quality U.S. Department of Health and Human Services
AHRQ Pub. No. 09-0016 September 2009

The authors of this report are responsible for its content. No statement in the report should be construed as an official position of the Agency for Healthcare Research and Quality (AHRQ), the Office of the Assistant Secretary for Preparedness and Response, or the U.S. Department of Health and Human Services.
This document is in the public domain and may be used and reprinted without permission except those copyrighted materials noted, for which further reproduction is prohibited without the express permission of copyright holders.
This report is based on the 2007 AHRQ publication Mass Medical Care With Scarce Resources: A Community Planning Guide, developed with collaboration and funding from the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Preparedness and Response through an AHRQ contract to Health Systems Research, Inc., an Altarum company (Contract No. 290-04-0010).
Suggested Citation
Phillips SJ, Knebel A, Johnson K, eds. Mass Medical Care With Scarce Resources: The Essentials. AHRQ Publication No. 09-0016. Rockville, MD: Agency for Healthcare Research and Quality: 2009.
ii
iii
AcknowledgmentsAuthors of the Original Mass Medical Care With Scarce Resources
Mass Medical Care With Scarce Resources: The Essentials is a condensation of the Mass Medical Care With Scarce Resources: A Community Planning Guide, published by AHRQ in 2007 (AHRQ Pub. No. 07-0001). We remain indebted to the expert teams who authored chapters of the original report.
Ethical Considerations
Mark Roberts, Ph.D. Professor of Economy Department of Health Policy Management Harvard University
Evan G. DeRenzo, Ph.D. Bioethicis Center for Ethics Washington Hospital Center
Assessing the Legal Environment
James G. Hodge, Jr., J.D., LL.M. Associate Professor, Johns Hopkins University Bloomberg School of Public Health Executive Director, Center for Law and the Public’s Health Georgetown and Johns Hopkins Universities
Prehospital Care
Edward Gabriel, M.P.A., AEMT-P Director of Crisis Management The Walt Disney Corporation
George Foltin, M.D. Associate Professor of Pediatrics and Emergency Medicine Center for Pediatric Emergency Medicine Bellevue Hospital
Paul Maniscalco, M.P.A., EMT-P Assistant Professor/Chief Researcher Homeland Security Policy Institute The George Washington University
Richard Serino, EMT-P Chief Boston Emergency Medical Service
Hospital/Acute Care
John L. Hick, M.D., Team Lead Assistant Professor Emergency Department Hennepin County Medical Center
Gabor Kelen, M.D. Director, Office of Critical Event Preparedness and
Response (CEPAR) Professor and Chair, Director of Research Department of Emergency Medicine The Johns Hopkins University
Daniel O’Laughlin, M.D. Assistant Professor of Emergency Medicine University of Minnesota/Abbott Northwestern Hospital
Lewis Rubinson, M.D., Ph.D. Health Officer Division of Pulmonary and Critical Care Medicine Deschutes County Health Department Bend Memorial Clinic
Richard Waldhorn, M.D. Distinguished Scholar Center for Biosecurity University of Pittsburgh Medical Center
Dennis P. Whalen Executive Deputy Commissioner New York State Department of Health Empire State Plaza
Alternative Care Sites
Stephen Cantrill, M.D., Team Lead Associate Director Department of Emergency Medicine Denver Health Medical Center
Carl Bonnett, M.D. Emergency Medical Services Fellow Department of Emergency Medicine Denver Health Medical Center
Dan Hanfling, M.D., FACEP DirectorEmergency Management and Disaster Medicine Inova Health System
iv
Peter Pons, M.D. (Also in Prehospital Care) Professor of Emergency Medicine Department of Surgery University of Colorado Health Sciences Center Senior Technical Physician, Emergency Department Denver Health Medical Center
Palliative Care
Marianne Matzo, Ph.D., APRN, B.C., FAAN Professor and Frances E. and Earl Ziegler Chair in Palliative Care Palliative Care Nursing University of Oklahoma College of Nursing University of Oklahoma Health Sciences Center
Anne M. Wilkinson, M.S., Ph.D. Senior Social/Behavioral Scientist Palliative Care Policy Center RAND Corporation
Maria Gatto, M.A., APRN Director of Palliative Care Bon Secours Health System
Joanne Lynn, M.D., M.A., M.S. Senior Natural Scientist RAND Corporation
The bibliography and resources from the original Mass Medical Care With Scarce Resources have been updated for this guide. Many of the authors above contributed to this update. We also appreciate the valuable input from the following:
Rachel E. Kaul, L.C.S.W., C.T.S. Senior Public Health Analyst U.S. Department of Health and Human Services Office of the Secretary Office of the Assistant Secretary for Preparedness and Response
Sherline Lee, M.P.H.U.S. Department of Health and Human Services Centers for Disease Control and Prevention Division of Healthcare Quality Promotion
Gamunu Wijetunge U.S. Department of Transportation National Highway Traffic Safety Administration Office of Emergency Medical Services

v
Contents
1. Community-Wide Planning.....…………….....………………………………………………....1
2. Ethical Considerations..................................................................................................................5
3. Assessing the Legal Environment..............................................................................................7
4. Prehospital Care.......................................................................................................................15
5. Hospital/Acute Care.................................................................................................................21
6. Alternative Care Sites ..............................................................................................................29
7. Palliative Care..........................................................................................................................35
8. Influenza Pandemic Preparedness............................................................................................41
Bibliography.................................................................................................................................57

1. Community-Wide Planning
Key Questions
What is a mass casualty event?
What are the two types of mass casualty events?
What are the basic steps planners must take to prepare for a mass casualty event?
In the event of a catastrophic public health or terrorism-related event, such as an influenza pandemic or the detonation of a nuclear device, the needs of tens of thousands of victims may overwhelm the resources of a community’s health care system. Indeed, if the event incapacitates health care workers, damages facilities, or destroys supplies, the capacity of the health care system to respond may be severely compromised. If other communities are faced with similar demands (as would be the case in an influenza pandemic or a nuclear detonation, for example), the arrival of additional health care resources, including assistance from the Federal Government, likely would be significantly delayed. Additional resources may not arrive at all.
In this dire scenario, referred to as a mass casualty event (MCE), if the health care system is to remain functioning and save as many lives as possible, it will be necessary to allocate scarce resources in ways that are different from normal circumstances but are appropriate for the situation. For the purposes of this report, scarce resources broadly include physical items (e.g., medical supplies, drugs, beds, equipment), services (e.g., medical treatments, nursing care, palliative care), and health care personnel (e.g., physicians, nurses, laboratory technicians, other essential workers in health care settings).
In general, MCEs can be organized into two categories: those that result in a sudden impact and those that result in a developing impact.
The “sudden-impact” MCE includes events such as detonation of bombs, airplane or train crashes, and natural disasters such as earthquakes. This category is characterized by many casualties at the outset of the event that generally taper off. In some cases there may be a second wave of casualties because of depleted resources or such factors as exposure to natural elements, unclean water, and contagious diseases. In this category of MCE, planners need to consider that the event may destroy essential infrastructure, requiring a mass migration of survivors.
The “developing-impact” MCE features events such as a mass exposure to anthrax or smallpox or an influenza pandemic. The number of people affected by the event increases gradually to a catastrophic number. In this category, the number of cases may decline due to treatment and prophylactic efforts, for example, only to increase as a result of additional waves of the disease. A “developing-impact” MCE necessitates a more sustained response, since the impact is felt over a much longer period than that of the “sudden-impact” MCE.
1

Levels of preparedness differ for the two types of MCEs. The “sudden-impact” MCE is unpredictable and requires immediate response in terms of the need to triage and temporize until the necessary resources arrive. In a “developing” MCE, such as an influenza pandemic, the impact is considered more predictable, and preparedness efforts most likely will mitigate its impact.
In the event of an MCE, whether “sudden impact” or “developing impact”, community planners will face the challenge of allocating scarce resources quickly enough to prevent undue illness and death. To prepare, planners need to take several steps.
Be proactive. Planners should anticipate to the degree possible the types of health care needs and resource shortfalls that will occur and identify policy and operational adjustments that will be needed in response.
Build and maintain relationships. Planners should forge partnerships, memoranda of understanding, interhospital agreements, and other relationships with key stakeholders from:
� The health care system, emergency management system, State and local public health systems, local emergency responders, emergency medical services, home health care, and other medical providers;
� volunteer agencies; and
� other public and private partners at State, local, Tribal, regional, and Federal levels.
These relationships need to clearly define the roles, responsibilities, capabilities, oversight, communications, logistics, and response resources each partner will contribute in an MCE. All partners must have a common vision for how they will function during a disaster. Multiagency coordination provides a mechanism for cooperative coordination of activities, resources, and policies across multiple agencies and jurisdictions. The involvement of senior leadership from all response agencies is essential.
Devise, model, and exercise MCE response plans. Stakeholders should understand and practice the processes that responders and health facilities will use to request resources from each other, supply vendors, special stockpiles, and emergency management contacts. Plans should be modified and refined continually based on input from response partners, lessons learned from exercises, and changing conditions. Modeling responses to a catastrophic MCE may take the form of tabletop exercises, actual but smaller events, or computer simulations. Such modeling efforts should begin by using small numbers of casualties as a starting point and then use rising victim number scalability models; i.e., plan for 100 casualties, then 1,000, then 10,000, and then 100,000. Possible useful models include:
� The Large Scale Emergency Response (LaSER) Program at New York University, which includes computer modeling of large-scale events, risk communication, legal aspects, workforce support, and community-based response issues.
� The Hospital Surge Model and Mass Evacuation Transportation Model, developed through collaboration between the U.S. Department of Health and Human Services (HHS) Agency for Healthcare Research and Quality (AHRQ) and the Office of the Assistant Secretary for Preparedness and Response (ASPR). The Surge Model estimates the amount of hospital resources needed to treat casualties of major disasters and the Evacuation Transportation model estimates the time required to evacuate patients from health care facilities.
2

Resources
Information on the LaSER program is available at http://www.nyu.edu/ccpr/laser/planc.html.
The Hospital Surge Model is available at http://www.ahrq.gov/prep/hospsurgemodel/.
The Mass Evacuation Transportation Model is available at
http://www.ahrq.gov/prep/massevac/.
Establish clear channels of communication. The State, rather than local jurisdictions, should assume responsibility for overall risk communication management. This includes information provided to hospitals, health care systems, providers, or the public via telephone, the Internet, media campaigns, 9-1-1 dispatchers, established community health call centers (poison centers, nurse advice lines, public health hotlines), and other communications mechanisms.
A Joint Information Center (JIC) should be established as well as other ways to link communications at the local, jurisdictional, and State levels to establish mechanisms for media message development. The JIC serves to gather incident data, analyze public perceptions, and provide the public or targeted audiences with accurate and comprehensive incident and response information. Communication strategies must be established and practiced ahead of time and can include risk communication, regular media releases, and press conferences.
ResourceA description of a virtual joint information center, The Virtual Joint Information Center: A Technological Tool for Emergency Communication, is available at http://www.cdc.gov/about/pah/pages/pahbestPractices2.htm.
Establish clear public messages. The public will need information on the status of the MCE and information that can help them make appropriate decisions about their own and their family’s health care. Messages can tell community members how to protect themselves and others, when it is safe to stay home, how to provide the best possible care at home, where to go for particular services, and when to call 9-1-1 or go to the emergency room. This information will help address the strain on health system resources and, in the case of infectious diseases, slow the spread of disease, while engaging the public in the allocation of scarce resources.
Clarify the process for leadership and coordination. It is critical to identify leaders, alternates, and the decisionmaking process for resource allocation and policy guidance.
Emphasize prevention. In MCEs such as an influenza pandemic, prevention of transmission is critical to minimizing the burden of disease.
Identify existing national and State tools, protocols, and processes for phases of the MCE.Many products and resources have been developed to help plan for catastrophic events. Numerous examples of these are presented in this report.
Consider the financial implications of responding to an MCE and the potential need to enact administrative or policy changes to facilitate reimbursement and recordkeeping. It is important to take into account any funding from HHS’s Centers for Disease Control and
3
Prevention’s Public Health Emergency Preparedness Cooperative Agreement Program and HHS’s ASPR Hospital Preparedness Cooperative Agreement Program.
Consider vulnerable populations. Explicit planning must occur at all levels for vulnerable populations including infants, children, frail elderly people, pregnant women, people with disabilities, people with mental illness, and those with chronic medical conditions (e.g., cardiac, dialysis, HIV, and oncology patients).
Develop robust security plans. Security is especially important in the case of a large-scale MCE because of the chaos such an event engenders. Having a uniformed presence (e.g., hospital security personnel, off-duty police officers, National Guard members, volunteers) helps maintain order, as do clear identification tags; visiting rules; and procedures for accessing supplies, service sites, and patients.
4
2. Ethical Considerations
Key Questions What ethical challenges do planners face in preparing for a mass casualty event?
How can planners employ a systematic approach to making ethical decisions as they prepare for a mass casualty event?
Ethical issues are critical in shaping and implementing any community’s disaster response planning. Who do we protect, and to what level of safety? Disaster preparedness planning almost inevitably has to be concerned with providing some minimum level of protection to all. How do we set budgets and priorities? Who do we evacuate first? Ethical choices must be made clear during the planning process so that on-the-spot decisions will be consistent with those choices.
Transparency also serves the goal of accountability. Citizens have a right to know what decisions public institutions make on their behalf--especially in those life-or-death choices that a disaster can require. Transparency opens the process to public feedback. This can help professionals ensure that their plans reflect community values and concerns.
Understanding of what is meant by rights and fairness is necessary. Planners must define these principles to gain community commitment to any disaster response plan. The public will support difficult choices if they know about and are committed to them beforehand and if they have input into the process.
Collaborative involvement of elected officials from all levels of government with local planners and citizens groups also is necessary. Direct citizen participation also should have a role in planning, including opportunities for discussion among a cross-section of community leaders.
In desperate situations, resources will indeed be overwhelmed. Preparedness activities will always be in competition with other priorities and it is impossible to be 100% prepared, but the better the plan, the easier it will be to carry out that plan when adverse events do occur. In that sense, disaster planners need to defend both their own interests and those of their communities through the planning process.
Deciding how and why to divert resources from one sector of the community to others should rest on predictions of what will produce the best outcome for the most people and on considerations of how resource distribution will work to ensure that Federal, State, and local governments meet their obligations. A balance must be struck between utilitarian (the greatest good for the greatest number) and duty-based (respect for all human beings) planning assumptions.
5

Ethics Analysis Algorithm: Applying a Systematic Approach to Sorting Through Ethical Disagreements
Debate about which ethical principles and theories to apply and how to prioritize them in a specific situation has been going on for millennia. As noted, there are no simple, formulaic schemes for such choices. There are, however, ways of thinking about ethical principles and theories that can help preparedness planners devise strategies for emergency response. These involve a systematic approach to applying basic ethical principles and theories to any particular situation. One can create an ethics algorithm that, if consistently applied to planning for any particular kind of emergency, can at least provide reasonable confidence that ethical issues raised by an emergency were well-considered. The ethics algorithm might be constructed as follows:
1. Who are all the possibly interested parties? Think broadly -- include not only persons and categories of persons but institutions, organizations, professions, and/or communities.
2. What is the full range of duties and obligations of each potentially interested party, or at least the primarily interested parties? Think of parties as not only individuals but also institutions and groups.
3. How might various duties and obligations of each of the various parties clash or conflict?
4. What might be short-term and long-term consequences, both good and bad, of each possible course of action? How confident are you of your predictive accuracy?
5. What ethical principles are at stake? (Possible ethical principles include respect for persons, beneficence, nonmalfeasance, justice, truth telling, liberty, opportunity, and reciprocity.) Which ones are in tension?
a. After enumerating the list of principles at stake, work to specify them; refine the meaning of each principle involved. Work to bring broad abstractions down to the level of the specific situation under discussion.
b. Make explicit the strategy for use of the principles. For example, for the situation at hand, must all the involved principles be upheld or is the strategy to balance the principles? If a balancing strategy is being applied, make explicit which values/ethical considerations are being balanced against which other values/ethical considerations.
6. What might be the intentions of the various players? Evaluate the praiseworthiness or lack thereof, of the motives of the people, organizations, and/or institutions involved.
7. What appears to be the full range of the possible courses of action?
8. Weed out those possible courses of action that do not appear to be justifiable based on potentially bad consequences, inability to meet duties and obligations, and/or the ethical soundness, or lack thereof, of intentions.
9. With the remaining possible courses of action, make explicit the justifications for taking each. Then vigorously scrutinize whether or not those justifications are ethically robust.
The sequence in which 2 through 6 above is conducted may not appear to be of major importance. It is necessary, however, to be able to claim convincingly that all points have been thoughtfully considered and deliberated, with all discussions and decisions fully documented.
Evan G. DeRenzo, Ph.D., Center for Ethics, Washington Hospital Center, Washington, DC.
6
3. Assessing the Legal Environment
Key Questions What are the principal types of emergency declarations?
What are the basic legal issues that emergency planners must consider?
Can normal licensing requirements for volunteer health personnel be circumvented during an emergency?
What legal protections are there for health care workers and volunteer health personnel during an emergency?
Laws at all levels of government are a critical part of emergency responses and allocation decisions involving scarce resources in MCEs. Constitutional provisions, statutes, administrative regulations, cases, compacts, mutual aid agreements, and public health or emergency management policies or plans are all relevant to assessing the legal environment in declared emergencies.
Please note that the information in this report and this section does not provide specific legal advice. Legal advice on these issues is necessarily fact-specific and varies depending on State or local laws and specific circumstances. Community planners are encouraged to work closely with their State Attorney General offices or local counsel to identify specific legal issues and solutions before and during MCEs.
By their nature, MCEs will typically result in the invocation of state of emergency declarations at multiple levels of government (Federal, Tribal, State and local). Emergency declarations essentially change the legal environment to facilitate emergency responses.1 State and local public health agencies (and their public and private sector partners) may assume a number of extraordinary public health powers.2 Governmental emergencies, however, vary depending often on the type of emergency declared and the level of government making the declaration.3 As discussed below, major types of emergency declarations include public health emergencies, general emergencies, and disasters.
Public health emergencies. Some States or local governments may declare a public health emergency.4 Once a state of public health emergency has been declared, State and local public health agencies (and their public and private sector partners) may be given a number of extraordinary public health powers.5 These include the ability to waive State professional licensing and certification requirements for volunteer health professionals (VHPs) participating in emergency response efforts,6 liability protections for medical personnel,7 and expedited procedures to acquire essential supplies and personnel.8
General emergencies and disasters. Every State and many local governments have developed a legal structure for declaring a general emergency or disaster and related emergency management functions. A state of emergency or disaster typically may be declared in response to any natural or manmade event or occurrence that threatens the public’s health or safety. Thus, an official such as a Governor, State health commissioner, local mayor, county commissioner can declare an emergency, depending on the laws in the jurisdiction.9
7
Dual declarations. Some States allow for the dual declaration of public health emergencies and general emergencies, which can lead to legislative confusion and duplication of efforts.10
Dual declarations present two major problems: the flow of specific powers and protections from emergency declarations vary depending on the type of declaration, and responsibility and authority for emergency responses may become convoluted when differing State or local agencies are charged with coordinating responses.11
Federal declarations. The Federal Government also has the power to declare an emergency or disaster. These powers operate independently or in conjunction with State and local emergency response efforts.12 The President may authorize emergency assistance “to save lives and to protect property and public health and safety, or to lessen or avert the threat of a catastrophe in any part of the United States” at the request of a State Governor or when the emergency is primarily a Federal responsibility.13 Depending on whether the event is an emergency or a major disaster, the Federal Government has differing powers.14 For example, Federal disaster assistance is only available on the request of the State Governor for major disasters, including natural catastrophes, fires, floods, or explosions, for which “effective response is beyond the capabilities of the State and the affected local governments….”15
In addition, the HHS Secretary is authorized to declare a public health emergency.16 This declaration authorizes a host of Federal actions. At any time, the HHS Secretary may deploy members of the Public Health Service or intermittent disaster response personnel to support States in responding to public health emergencies.
Balancing Individual and Communal Interests While emergency laws can help planners make decisions about scarce resources, other legal requirements also may affect these decisions. Constitutional principles may limit government actions. For example, allocation decisions that (1) are based on discrimination against race, ethnicity, national origin, religion, or sex, for example, (2) lack meaningful justification, or (3) deny individuals an opportunity to be heard may violate constitutional principles of equal protection and due process or civil rights statutes. Legal action may be brought to stop the enforcement of these decisions even during emergencies.
Disability laws, such as the Americans With Disabilities Act17 or State or local equivalents, may require protections for people with disabilities during emergencies. Some States and localities bar discrimination under much broader human rights laws.18
State and local governments legally may require the prioritization of their own workforce over the general population concerning specific medical interventions to ensure government stability and continued efforts to protect the public’s health. Similar decisions by health care entities to protect their essential personnel when resources are scarce also may be legally supportable.19
Federal or State agencies may prescribe specific laws or guidance on prioritization of vulnerable populations. These types of legal actions demonstrate how laws can help allocation decisions, but also how they may interfere with local decisions of community health planners.
8
Suspension of Existing Legal Requirements
Statutes allowing suspensions of existing provisions of law (except constitutional norms) exist in most Federal, State, and local emergency laws.20 Their use during an emergency can affect allocation decisions profoundly.
Interjurisdictional Legal Coordination
Emergency responses may require moving people and property between jurisdictions efficiently. Difficult legal questions arise that require coordination of activities and resources across local, State, and Federal boundaries.21 Interjurisdictional coordination may arise between similar jurisdictions (e.g., between adjacent counties) or different jurisdictions (e.g., between local or tribal and/or State and Federal governments).22
Formal mutual aid agreements between States (e.g., the Emergency Management Assistance Compact [EMAC23]), local governments (e.g., Illinois Public Health Mutual Aid System Agreement24), and foreign countries (e.g., International Emergency Management Assistance Compact between several New England States and Canadian provinces25) help with exchanges of resources in real time during emergencies.
Medical Licensure Reciprocity
During MCEs involving Federal or State declarations of emergency, the potential for significant losses of health care personnel coupled with hundreds or thousands of new patients presents an immediate need for additional trained health care providers.26 These providers may come from facilities both in and out of State.
In nonemergencies, licensed non-Federal practitioners in one State cannot practice medicine or public health services in another State without waivers of State licensure requirements or other conditions (e.g., Good Samaritan provisions).27 Federal health care providers need only to be licensed in one State to perform their official duties in any State.28
States have created several legal approaches to circumvent normal licensing requirements for VHPs during emergencies. These provisions allow these volunteers to practice during an emergency as if they were licensed in the jurisdiction, subject to restrictions on the scope of practice set forth by the State or a political subdivision.29 Licensure reciprocity provisions must be clearly communicated during emergencies to ensure that VHPs can participate in emergency response.
Patient family members, neighbors, or others in the community also may be needed to provide palliative or other medical care or offer essential support for medical personnel. While a State-based declaration of an emergency typically does not authorize individuals without medical training to provide systematic medical care of patients, their supervised participation in the care of relatives or companions is essential. Just as in nonemergencies, such activities are legally warranted in many cases. Individuals lacking medical training also may provide key support services to patients, provided that they do not actually treat them. Screening patients through the administration of basic services by nonmedical personnel is legally permissible in emergencies; diagnosing patients, deciding their treatment, or prescribing their medications is likely not.
9
Liability and Other Protections for Health Care Workers and Volunteers The uncertainties of emergency legal environments, the need to work within standards appropriate to the situation,30 and the unpredictability of harms to some patients (especially during emergencies) raise liability fears among health care workers and VHPs attempting to provide health services via medical triage. Immunity from civil liability for harms to patients may be available through legal sources,31 including:
� Governmental sovereign immunity (if the worker or volunteer is a government employee or agent);
� Federal and State volunteer protection acts;32
� States’ Good Samaritan Acts;33
� State emergency health powers statutes34; and
� Mutual aid compacts such as (EMAC).35 For example, State officers or employees providing aid via EMAC during emergencies are protected from civil liability as agents of the requesting State so long as they act in good faith and without “willful misconduct, gross negligence, or recklessness.”36
Fewer liability protections exist for the entities (e.g., private hospitals, medical clinics) that respond to emergencies.37 The Federal Volunteer Protection Act of 1997, for example, provides immunity for volunteers of nonprofit entities but not for the entities themselves.38 Some State laws mimic this approach; additional state legislative reforms are in development.39 Currently, however, hospitals and other health care entities may be subject to potential liability during an emergency, even if their employees or VHPs are protected.40 The Uniform Emergency Volunteer Health Practitioners Act (UEVHPA), which has been enacted in several States (including Arkansas, Colorado, Indiana, Kentucky, New Mexico, Tennessee, and Utah), provides some liability protections for entities coordinating or hosting VHPs.41
Resource Further information on the Uniform Emergency Volunteer Health Practitioners Act is available at http://www.uevhpa.org/DesktopDefault.aspx.
Liability concerns may also arise concerning injuries to health care workers or VHPs. Under some circumstances, government or the private sector may compensate these individuals for injuries (physical or mental) incurred in responding to the emergency. Workers are often protected from these harms through workers’ compensation programs that cover individuals injured or killed at work42, even during emergencies.43
VHPs, however, are not typically classifiable as employees and so do not benefit automatically from worker’s compensation plans. VHPs deployed as Federal or State agents may be covered by governmental workers compensation plans. VHPs deployed through EMAC are automatically eligible for State workers compensation benefits. Some States, such as Michigan, have legally extended their workers compensation programs to registered VHPs providing services in the State during an emergency.44 Some employers have worked out contractual agreements with their workers’ compensation carriers to continue to cover employees who volunteer to respond to an emergency outside their jobs.
10
Making Allocation Decisions in Real Time: Legal Triage Community health planners must align with their local legal community to clarify
emergency legal issues in their jurisdictions. Addressing legal issues that underlie the allocation of scarce resources is an essential part of emergency plans. Planners should begin with a series of legal questions that have been answered in prior emergencies. Does local government have sufficient home rule to declare an emergency? If so, under what authority? What types of emergencies can be declared? What powers flow from the declaration? What nonemergency legal provisions may be suspended? What emergency provisions directly affect the allocation of scarce resources? Who is legally responsible for making critical decisions at the State or local level? How much authority will a particular entity have to make critical choices? When can the government challenge that entity’s decisions? When is that entity, its employees, or its volunteers legally accountable for these decisions?
Resource
Local Government Public Health Emergency Legal Preparedness and Response, developed by the Centers for Law and the Public’s Health: A Collaborative at Johns Hopkins and Georgetown Universities, provides useful checklist on local government public health emergency legal preparedness and response. Available at http://www.publichealthlaw.net/Projects/EmergencyPrep.php.45
Legal practitioners must be prepared to prioritize relevant legal issues in real time. Legaltriage refers to efforts of these practitioners to construct a favorable legal environment during emergencies through a prioritization of issues and solutions that help public health responses and allocation decisions.46 Community health planners should partner with members of the local legal community who are prepared during emergencies to:
� Identify legal issues that may help or hinder allocation decisions as they arise;
� Monitor changing legal norms during emergencies;
� Communicate with lawmakers and policy officials in government and the private sector;
� Develop innovative, responsive legal solutions to reported barriers to allocation decisions;
� Explain legal conclusions through tailored communications to planners and affected individuals; and
� Revisit regularly the utility of legal guidance related to allocation decisions.47
Endnotes
1 Hodge, JG, Anderson, ED. Principles and practice of legal triage during public health emergencies. NYU Ann. Surv. Am. L. 2008; 64(2): 249-291. 2 Gostin LO, Sapsin JW, Teret SP, Burris S, Mair JS, Hodge JG Jr, Vernick JS. The Model State Emergency Health Powers Act: planning for and response to bioterrorism and naturally occurring infectious diseases. JAMA. 2002;288:622.
11
3 Hodge, JG, Garcia, A, Anderson, ED, Kaufman, T. Emergency legal preparedness for hospitals and health care personnel. Disaster Medicine and Public Health Preparedness 2009; 3:Suppl 1: S37-S44. 4 Center for Law and the Public’s Health. Model State Emergency Health Powers Act (MSEHPA) art. V-VI 2001. Available at: http://www.publichealthlaw.net/MSEHPA/MSEHPA2.pdf. Accessed April 15, 2006. 5 Gostin LO, Sapsin JW, Teret SP, Burris S, Mair JS, Hodge JG Jr, Vernick JS. The Model State Emergency Health Powers Act: planning for and response to bioterrorism and naturally occurring infectious diseases. JAMA. 2002;288:622. 6 Center for Law and the Public’s Health. Model State Emergency Health Powers Act. § 608 (2001). Available at: http://www.publichealthlaw.net/MSEHPA/MSEHPA2.pdf. Accessed April 15, 2006. 7 Ibid. § 804 (2001).8 Ibid. §§ 505-507 (2001).9 Hodge JG Jr, Gable LA, Calves S. The legal framework for meeting surge capacity through the use of volunteer health professionals during public health emergencies and other disasters. Journal of Contemporary Health Law and Policy. 2006;22:5-71.10 Ibid. 2006:25-26. 11 Ibid. 12 Hodge, JG, Anderson, ED. Principles and practice of legal triage during public health emergencies. NYU Ann. Surv. Am. L. 2008; 64(2): 249-291 13 The Robert T. Stafford Disaster Relief and Emergency Assistance Act, 42 U.S.C. §§ 5122(1), 5191 (2002). 14 Ibid. §§ 5120-5206 (2002). 15 Ibid. §§ 5170, 5191 (2002) (requiring that, prior to requesting Federal assistance from the President, the State Governor must utilize State resources to respond to the emergency, including the activation of the State emergency management plan). 16 Public Health Security and Bioterrorism Preparedness and Response Act of 2002, 42 U.S.C. § 247d. 2003. 17 The Americans with Disabilities Act of 1990. Pub. L. No. 101-336. 18 The New York “Human Rights Law,” New York Executive Law Art. 15 §290 et seq. 19 Hodge JG Jr. Bioterrorism law and policy: critical choices in public health. Journal of Law, Medicine & Ethics. 2002;30:254-255.20 Hodge, JG, Anderson, ED. Principles and practice of legal triage during public health emergencies. NYU Ann. Surv. Am. L.2008; 64(2): 249-291. 21 Center for Law and the Public’s Health. Public health emergency legal preparedness checklist on interjurisdictional legal coordination. Available at http://www.publichealthlaw.net/Resources/BTlaw.htm (2004). 22 Hodge, JG, Anderson, ED Principles and practice of legal triage during public health emergencies. NYU Ann. Surv. Am. L.2008; 64(2): 249-291. 23 Emergency Management Assistance Compact (EMAC), Pub. L. No. 104-321. 24 Intergovernmental Mutual Aid Agreement for the establishment of the Illinois Public Health Mutual Aid System. Available at: http://www.idph.state.il.us/local/mutualaidagree_9.30.04.pdf. Accessed November 27, 2006. 25 Fox P. Cross-border assistance in emergencies: the New England/eastern Canadian model. New England Journal of International Contemporary Law. 2004;11:75. 26 Hodge JG Jr. Legal issues concerning volunteer health professionals and the hurricane-related emergencies in the Gulf Coast region. Public Health Report. 2006;121:205-207. 27 Department of Health and Human Services, Assistant Secretary for Preparedness and Response, Emergency system for advance registration of volunteer health professionals (ESAR-VHP) – legal and regulatory issues. 2008:(Draft report – September 2008). 28 Ibid. 29 Hodge, JG Jr. Legal issues concerning volunteer health professionals and the hurricane-related emergencies in the Gulf Coast region. Public Health Rep. 2006;121:205-207. 30 Agency for Healthcare Research and Quality. Altered Standards of Care in Mass Casualty Events., AHRQ Publication No. 05-0043. April 2005. Available at: http://www.ahrq.gov/research/altstand/. Accessed November 27, 2007. 31 Department of Health and Human Services, Assistant Secretary for Preparedness and Response, Emergency system for advance registration of volunteer health professionals (ESAR-VHP) – legal and regulatory issues. 2008:(Draft report – September 2008).32 Federal Volunteer Protection Act of 1997. Pub. L. No. 105-19, § 4, 111 Stat. 218, 219 (1997), 42 U.S.C. § 14503 (2000); Ala. Code. § 6-5-336(d)(1) (LexisNexis 2005); Miss. Code Ann. § 95-9-1(3) (LexisNexis 1972).
12
33 Department of Health and Human Services, Assistant Secretary for Preparedness and Response, Emergency system for advance registration of volunteer health professionals (ESAR-VHP) – legal and regulatory issues. 2008:(Draft report – September 2008).34 Ibid. 35 Emergency Management Assistance Compact (EMAC), Pub. L. No. 104-321. 36 Emergency Management Assistance Compact (EMAC), Pub. L. No. 104-321, art. VI, 100 Stat. at 3880. 37 Matthews G. Expanding Emergency Liability Protection within Existing State Laws: The Work Around Approach. Available at: http://nciph.sph.unc.edu/law/tampa_report2.pdf. Accessed October 1, 2008. 38 The Volunteer Protection Act, 42 U.S.C. 14503(c). 39 Matthews G. Expanding Emergency Liability Protection within Existing State Laws: The Work Around Approach. Available at: http://nciph.sph.unc.edu/law/tampa_report2.pdf. Accessed October 1, 2008. 40 Hodge JG Jr, Calves S, Gable LA, Meltzer E, Kraner S. Risk management in the wake of hurricanes and other disasters: Hospital civil liability arising from the use of volunteer health professionals during emergencies. Michigan State University Journal of Medicine and Law. In press. 41 Hodge, JG, Pepe RP, Henning, WH. Voluntarism in the wake of Hurricane Katrina: The Uniform Emergency Volunteer Health Practitioners Act. Disaster Medicine and Public Health Preparedness 2007; 1:1: 44-50.. 42 Hodge JG Jr. The intersection of Federal health information privacy and State administrative law: the protection of individual health data and worker’s compensation. Administrative Law Review. 1999;51:117-144. 43 Department of Health and Human Services, Assistant Secretary for Preparedness and Response, Emergency system for advance registration of volunteer health professionals (ESAR-VHP) – legal and regulatory issues. 2008:(Draft report – September 2008). 44 M.C.L. §§ 418.161(g), 30.411 Sec. 11(1)(b)-(c). 45 Center for Law and the Public’s Health. Checklist on local government public health emergency legal preparedness and response. Available at: http://www.publichealthlaw.net/Projects/EmergencyPrep.php. Accessed September 17, 2009. 46 Hodge, JG, Garcia, A, Anderson, ED, Kaufman, T. Emergency legal preparedness for hospitals and health care personnel. Disaster Medicine and Public Health Preparedness 2009; 3:Suppl 1: S37-S44. 47 Hodge, JG, Anderson, ED. Principles and practice of legal triage during public health emergencies. NYU Ann. Surv. Am. L. 2008; 64(2): 249-291.
13

4. Prehospital Care
Key Questions How can planners maximize the availability of emergency medical services personnel?
How can transport be coordinated and transport capability be maximized?
How can patients be triaged most efficiently?
How can home care be incorporated into emergency planning?
In the event of a catastrophic MCE, it is Emergency Medical Services (EMS) that will be called on to provide first-responder rescue, assessment, care, and transportation to the health care delivery system. EMS in the United States is provided through highly varied organizations. Nearly half of all EMS are delivered through local fire departments. Others fall under municipal or county governments, police departments, health departments, or private companies (e.g., hospital-based, for-profit ambulance services) or are volunteer-based.48 The variability of EMS response systems and the differences in EMS preparedness training, guidelines, and response capacity pose significant coordination and communications challenges for EMS planners.
Recommendations for Planners
Planners should take several actions prior to an MCE to help maximize the response capacity of prehospital EMS services. Those actions include the following:
Forge partnerships at all levels. As with all aspects of preparedness, the need to coordinate and allocate scarce prehospital resources in an MCE requires the development, implementation, exercising, and refinement of partnerships between Federal, State, and local government response agencies, as well as between public and private entities.
Improve communication and coordination. Planners must develop integrated and interoperable communications and data systems, with backup strategies and procedures that can link EMS agencies to hospitals, trauma centers, public safety departments, emergency management offices, and public health agencies. In addition, EMS systems must be familiar with the Federal response capability, such as the provisions of the Homeland Security Presidential Directive/HSPD-5, the National Disaster Medical System (NDMS), Disaster Medical Assistance Teams, the Incident Command System (ICS), Occupational Safety and Health Administration (OSHA) personal protective equipment guidelines, and OSHA Hazardous Materials Operations regulations. This awareness will reduce the risk that requests for resources will be misdirected. EMS personnel should be trained in the National Response Framework to learn about its incident command and its tenets for supporting operational requirements. Ideally, EMS systems should be centralized through established ICS channels.
Improve EMS Education. The National Highway Traffic Safety Administration (NHTSA) together with the Health Resources and Services Administration and other members of the Federal Interagency Committee on EMS are involved in ongoing efforts to improve the EMS education system and to provide leadership and coordination of comprehensive, evidence-based and data driven emergency medical services and 9-1-1 systems. NHTSA is supporting
implementation of the EMS Education Agenda for the Future: A Systems Approach, and has published the National EMS Scope of Practice Model and the National EMS Education Standards.
ResourcesEMS Education Agenda for the Future: A Systems Approach is available at http://www.nhtsa.gov/people/injury/ems/EdAgenda/final/index.html.
National Emergency Medical Services Scope of Practice Model is available at http://www.nhtsa.dot.gov/portal/site/nhtsa/menuitem.2a0771e91315babbbf30811060008a0c/.
National Emergency Medical Services Education Standards are available at http://www.nhtsa.gov/staticfiles/DOT/NHTSA/ems/811077a.pdf.
The National EMS Information System (NEMSIS) is an effort to improve the uniformity of EMS data nationally. NEMSIS includes linkages between State and local EMS data systems, as well as a National EMS Database to be housed at NHTSA. More information on NEMSIS is available at www.nemsis.org.
EMS Pandemic Influenza Guidelines for Statewide Adoption and Preparing for Pandemic Influenza: Recommendations for Protocol Development for 9-1-1 Personnel and Public Safety Answering Points (PSAPs) are available online under the “Pandemic News” section at http://www.ems.gov.
Continually modify and refine plans. Planning should include concrete implementation steps with training and exercise goals for each step. Each component of the response should be taught, exercised, evaluated, modified, and tested again. Exercises should simulate actual casualties, as well as management of the “worried well”--individuals calling for EMS resources who actually do not need them. Exercises should include response partners from public, private, community, and governmental and nongovernmental agencies. This iterative process allows for continuous modifications and improvements to plans, policies, and procedures.
Provide leadership. Leadership training should be provided for mid- and upper-level EMS supervisory staff members to ensure that in case of major illness, injuries, or deaths, there will be individuals who can take on the role of EMS medical director or leadership. A staff member or members should be designated in advance who can adjust standard operating procedures and the scope of practice of EMS personnel to accommodate the needs of the situation.
Approaches to the Allocation of Scarce Resources In the case of an MCE, there likely will be scarcities of emergency medical technicians (EMT), transport capacity, and destinations for patient treatment. As a result, plans should be in place for coordinating and maximizing the use of available staff members and resources. These plans should be tested and refined prior to the MCE. Legal and ethical advisors should be included in planning discussions. Allocation of scarce resources should include the following:
Make sure as many EMS personnel as possible are available through use of modified or extended shifts, deployment of no more than two providers per vehicle, and use of one-person response vehicles for “patient evaluation” prior to dispatch of transport resources. Staff members also may be shifted so that non- EMTs can serve as drivers; fire, police, or volunteer EMTs can provide assistance during transport; and other medical personnel (e.g., physicians,
16
nurses, nurse’s aides) can help staff casualty treatment sites to permit EMS personnel to provide transport services. “Just-in-time” programs that train nonmedical volunteers to provide basic medical care such as applying direct pressure for hemorrhage control also should be developed.
Make best use of available EMS personnel. Some medical protocols may be suspended to allow greater efficiency and flexibility in patient management. EMS personnel may be used in nontraditional settings (e.g., alternative care sites (ACSs), hospitals, pharmaceutical distribution centers) for field triage, treatment, or transport. Their scope of practice may be extended to provide vaccinations or medications or to deliver nontraditional medical care at the scene.
Maximize transport capability. Public and private ambulance services should be coordinated and steps should be taken to ensure that they do not self-dispatch to MCEs. Paramedic-initiated alternative transportation (e.g., buses, taxis, privately owned vehicles) also should be used. Mutual aid agreements should be in place to deploy available transportation assets, staff members, and staging locations. Transportation assets should be loaded to full capacity and patients taken to the closest appropriate hospital or care site. Air transport should be used to take patients to distant facilities (unless the incident presents contamination risks). Noncritical calls should be batched by geographic area. Bypass, diversion, or closure rules can be suspended to best distribute patients and to avoid overloading any one hospital.
Use the Community Emergency Response Team (CERT). The CERT program trains people in basic disaster response skills, such as fire safety, light search and rescue, team organization, and disaster medical operations. CERT members can assist others following an event when professional responders are not immediately available.
Resource
Information about CERT is available at http://www.citizencorps.gov/cert/about.shtm.
Screen calls and dispatch efficiently. Call screening strategies should be in place to determine the level of urgency required to respond to calls. Response strategies involving multiple responders (e.g., engine company, ambulance, law enforcement) used in standard EMS response should be avoided. Prearrival instructions should be scripted and tailored to the incident with formal recommendations on use of alternative transport and ACSs.
Provide personal protection for personnel. Universal precautions should be used for every patient encounter, if possible. To reduce the number of responders exposed to pathogens or chemicals, specialized protections should be used to the extent possible and adjusted to the nature of the incident (e.g., distribution of antibiotics, vaccines, or antidotes to staff and family members). In the case of chemical incidents, decontamination needs must be evaluated and addressed before transportation to preserve transport capability. Similarly, security personnel should be assigned to protect EMS response operations, logistics centers, and stockpile depots.
Triage and evaluate patients efficiently. Specific triage systems should be in place before an incident, and personnel should be trained and exercised in their use. Simple triage methods include rapid separation of critical patients from noncritical patients (i.e., “Everyone who can walk should get on this bus.”). The overarching principle for triage is “to do the most good for the most people.”
17

There are three basic types of triage. Primary triage is the first triage of patients into the medical system (possibly occurring prehospital), at which point patients are assigned an acuity level based on the severity of their illness/disease. Secondary triage is the reevaluation of the patient’s condition after initial medical care.49 This may occur at the hospital following EMS interventions or after initial interventions in the emergency department. Tertiary triage is the reevaluation of the patients’ response to treatment after further interventions. This continues for the duration of the patient’s hospital stay. Historically, triage has involved four levels of priority for traumatic injuries:
� Green--delayed treatment--patient has minor injuries or illness that should not pose a threat to life or limb.
� Yellow--intermediate--patient has injuries or illness that may result in death or disability but pose no immediate threat to life or limb.
� Red--critical--patient has injuries or illness that will result in death within the hour unless interventions occur.
� Black--expectant or deceased--patient is expected to die because of severity of illness or injuries or has died. Comfort measures, including pharmacologic treatment, should be provided as available.
An experienced health care provider, such as the EMS Medical Director or designee, should be involved in any decision to classify a patient as “black” during a disaster. Although such patients may be designated as low priorities for transport, they should have access to palliative care (e.g., analgesia, sedation, physical and behavioral care) to the extent possible under the circumstances. Expectant patients should be reassessed regularly for comfort, improvements in their situation, or in case resources become available unexpectedly.
Coordinate destination choices. A centralized coordination of patient transport should be in place for minimal hospital overloading and best use of other available resources, such as primary care providers, ACSs, medical evaluation centers, or triage centers.
The vast majority of victims of an MCE may end up being most appropriately managed at home, either because their illness or injury is not severe enough to warrant institutionalized care or because, given scarce resources, inpatient treatment may be considered futile or wasteful.
Use local, regional, State, and national information services systems that provide updates of hospital bed status and capabilities to inform EMS about destination choices and to help coordinate patient distribution.
Establish casualty treatment areas on or near the disaster site or at ACSs (depending on the nature of the incident) to address the volume of casualties, provide triage, assess transport, and serve as treatment sites. Home health care should be used according to predetermined triage protocols to prevent unnecessary use of EMS transport and hospital resources.
ResourceHome Health Care During an Influenza Pandemic, available at http://www.flu.gov/professional/hospital/homehealth.html.
18
Incorporating Home Health Care Into Emergency Planning: Issues to Consider
Register patients being cared for in the home setting with a local emergency management agency and the public health department to ensure access to relevant information.
Ensure adequate stock of routine chronic care medications.
Ensure adequate stock of basic first aid supplies, including bandages, antipyretic medications (e.g., acetaminophen, ibuprofen), oral electrolyte solutions, and thermometers.
Ensure that backup utility support is in place if warranted (particularly for those patients requiring electricity for medical devices).
Establish a “sick room” in the home for managing ill household members, particularly in the event of a transmissible infectious disease.
In caring for patients with advanced symptoms who are too sick for hospital care, coordinate symptom palliation with a home care team coordinated by local public health authorities.
Ensure the availability of a bedside commode or bedpan.
48 Institute of Medicine, Committee on the Future of Emergency Care in the United States Health System. EmergencyMedical Services: At the Crossroads. Washington: National Academies Press; 2006. 49 Saffle JR, Gibran N, and Jordan M. Defining the ratio of outcomes to resources for triage of burn patients in mass casualties. Journal of Burn Care & Rehabilitation. November/December 2005;26(6): 478-482.
19

5. Hospital/Acute Care
Key Questions What is the National Incident Management System and what are its components?
What guidance should be included in a plan for allocating scarce resources?
How can staff and space capacity be increased during an emergency?
What factors should be included in patient assessments when resources are scarce?
In the event of an MCE, decisions and policies regarding resource allocation in hospitals will have to be developed in advance at multiple levels, ranging from the State to local communities and institutions. Hospitals should be able to follow guidance and decision support tools available through a clearinghouse to make resource allocation decisions (e.g., who should receive mechanical ventilation). Even with the support of these tools or policies, however, it is the hospital that will have to take on the role of implementing them. To plan for addressing hospital and acute care needs following an MCE, hospitals and their partners need to prepare.
Developing an Integrated Incident Management System Hospitals must have in place a system of coordination with other local hospitals, public health departments, incident commands, public safety, and EMS systems to provide care. Integrated incident management is critical to preparing for an MCE and must be developed prior to any catastrophic event.50
The ICS has been adopted as the National Incident Management System, a national training curriculum for public and private sector users that can be applied to multihazard and planned event situations.
Resource
Information on the National Incident Management System training curriculum is available at http://www.fema.gov/emergency/nims/NIMSTrainingCourses.shtm.
An Institute of Medicine report on hospital-based emergency care recommends that coordination and incident management require the following components:51
� The establishment of hospital coalitions, compacts, and mutual aid agreements to create a common platform for planning and response. This may be facilitated by the use of an existing program, such as the Hospital Incident Command System (HICS). HICS is a nationally recognized approach to disaster management (see box below).
� The establishment of a jurisdictional Emergency Operations Center. Hospitals should be familiar with its local office of emergency preparedness and know how it is represented there.
21
� The designation of a particular hospital or local public health agency as a “trusted source” to serve as the hospital’s resource and policy gateway within the region during a major multijurisdictional event.
The Hospital Incident Command System The Hospital Incident Command System (HICS) was developed in California to provide an emergency management system for hospitals for use during a medical disaster. The system helps coordinate emergency response between hospitals and other emergency responders and is based on a clear chain of management, clearly defined responsibilities, prioritized response checklists, clear reporting channels for documentation and accountability, and a common nomenclature. HICS is compliant with the National Incident Management System. More information on HICS is available at http://www.hicscenter.org/pages/index.php.
The Incident Command Section provides overall coordination of the response and is the central communications point.
The Operations Section conducts tactical medical operations to carry out the incident action plan. Activities will include basic medical services, behavioral/mental health support, ancillary medical services, and preventive medicine.
The Planning Section prepares and documents the Incident Action Plan (IAP) by collecting and evaluating information, maintaining resource status and documentation for incident records.
The Logistics Section provides support, resources, and other services, including personnel, needed to meet operational objectives.
Finance and Administration is responsible for time-recording, procurement, accounting, and cost analysis.
Developing a Planning Framework for Allocating Scarce Resources The planning framework should be transparent and shared with key stakeholders in the
health department, attorney general’s office, and governor’s office and with the community, both in advance of and during an MCE. The framework should establish ways to:
� Define or project the resource shortfalls and the impact on clinical care.
� Request additional resources, facilitate the transfer of patients out of the affected area, or facilitate alternative strategies for patient care (e.g., alternative care sites, home care).
� Develop and disseminate supportive policy and clinical guidance (e.g., triage and treatment recommendations, decision tools)--ideally ones that have been nationally sanctioned or federally approved and disseminated. Clinical guidance or decision aids should reflect any available Federal guidance and ideally be flexible enough to allow hospital and clinician discretion in making resource allocation decisions, as deemed medically justified.
� Provide guidance for liability relief for providers.
� Provide guidance on the equitable management and allocation of scarce resources.
22

� Integrate response strategies and tactics across facilities and agencies at the local, regional, State, and Federal levels (see Figure 1). The six-tier construct depicts public health and medical asset management levels during response to mass casualty or mass effect incidents. The tiers range from individual health care organizations or other healthcare assets and their integration into a local healthcare coalition to coordination of Federal assistance. Each tier must be managed internally to integrate externally with other tiers.
Source: Barbera JA, Macintyre AG. Medical Surge Capacity and Capability Handbook. Prepared for the U.S. Department of Health and Human Services by CNA Corporation under contract. September 2007). Accessed July 21, 2009 at http://www.hhs.gov/disasters/discussion/planners/mscc/chapter1/1.2.html.
Coordinating Community and Regional Response Planning for Hospital/Acute Care The State health department has the overall responsibility for projecting health resource needs in the event of a major health-related emergency and for allocating scarce resources to meet those needs. Some States have intrastate regional coalitions (clearinghouse hospitals, regional coordinating hospitals) that can help the State health department in managing resource allocation in their area. This arrangement allows for plans to consolidate supplies, epidemiological data, medical response, communications, and command and control. These
23
intrastate regional coalitions, where they exist, should be incorporated into regional Multi-Agency Coordination (MAC) planning and response.
Interstate agreements and cooperation help promote sharing of assets across State lines. This level of interstate cooperation is difficult to achieve but is one of the most important ways to maximize resource allocation.
Increasing System Capacity In advance of an MCE, hospitals should establish a preference list of supplemental
providers to expand staff capacity. These providers might include:
� State Emergency Systems for Advanced Registration of Volunteer Healthcare Professionals (ESAR-VHP). Local hospital staff, clinic staff, and health professional volunteers registered with an ESAR-VHP have had their credentials verified.
� The Medical Reserve Corps (MRC). Local MRC units of volunteers may include medical and public health professionals, such as physicians, nurses, pharmacists, dentists, veterinarians, epidemiologists, and paramedics.
� Federal public health and medical teams. (e.g., National Disaster Medical System, Public Health Service).
� Trainees.
� Patient family members.
� Military members.
� CERTs.
� Lay volunteers.
Resources
More information on MRC and ESAR-VHP is available at http://www.medicalreservecorps.gov.
Policies should be in place in advance for credentialing staff members and managing deployment of nonhospital personnel in the hospital. A plan also should be in place for managing volunteers.
An important staffing issue in the context of MCE planning is the concern that a significant proportion of health care providers will fail to report to work if they perceive possible harm to themselves or their family members. Some States have provisions to delicense or otherwise sanction providers who do not report for duty during a declared disaster. Nevertheless, there are real concerns for providers about duty to family and child care issues that may not be solved easily.
Careful determination of priority groups and essential personnel, facilitation of child care, providing adequate personal protective equipment, and providing housing apart from family for workers who request it, all can help ensure that health care workers are willing and able to work (and work safely) during a disaster.
24

Applying Short-Term Strategies
Short-term strategies may be applied to increase healthcare facility capacity in cases in which resource shortages can be expected to be resolved relatively quickly (within hours or days). These strategies usually do not require a systematic assessment of the standard of care being provided.
Planners can increase space capacity by:
� Employing rapid discharge of emergency department and other outpatients who can continue their care at home safely.
� Employing rapid discharge of inpatients who can safely continue their care at home or at alternate facilities if they are available.
� Canceling elective surgeries and procedures, with reassignment of surgical staff members and space. The definition of “elective” may vary with the severity and duration of the situation and requires daily review; a surgery to remove a neoplasm, for example, may be elective for 24 hours but not for weeks.
� Reducing the usual use of imaging, laboratory testing, and other ancillary services.
� Expanding critical care capacity by placing select ventilated patients on monitored or step-down beds; using pulse oximetry (with high/low rate alarms) in lieu of cardiac monitors; or relying on ventilator alarms (which should alert for disconnect, high pressure, and apnea) for ventilated patients, with spot oximetry checks.
� Converting single rooms to double rooms or double rooms to triple rooms if possible.
� Designating wards or areas of the facility that can be converted to negative pressure or isolated from the rest of the ventilation system for cohorting contagious patients; or use of these areas to cohort health care providers caring for contagious patients to minimize disease transmission.
� Using cots and beds in flat space areas (e.g., classrooms, gymnasiums, lobbies) within the hospital for noncritical patient care.
� Transferring patients to other institutions in and out of the State.
� Facilitating home-based care for patients in cooperation with public health and home care agencies.
� Establishing mobile or temporary evaluation and treatment facilities in the community. These locations also may be used to screen patients with mild symptoms when medications are available and must be taken early in the course of illness to be effective.
Planners can expand staff capacity by:
� Calling in staff members.
� Changing staff scheduling (e.g., duration of shifts, staffing ratios, staff assignments).
� Requesting supplemental staff members.
� Sharing small numbers of specialized staff members (e.g., burn nurses, pediatric critical care staff members) with hospitals in need.
25

� Activating memoranda of understanding (MOU) with regional and distant hospitals, health systems, or State disaster medical assistance teams. Planners can increase access to supplies by activating MOUs with commercial companies.
If these strategies are not sufficient to meet the demands of the incident and no immediate relief is available, then an evaluation of the level of care being provided must be conducted. Surge strategies should be reviewed and revised based on available resources.
Applying the Spectrum of Adaptation: From Administrative to Clinical Change
In the case of a long-term resource shortage, strategies for meeting the demands of an MCE can be classified along a spectrum that includes two categories of changes: administrative adaptations and clinical adaptations.
Administrative adaptations are designed to increase provider availability for patient care. Though their effect on clinical care should be minimal, it must be recognized that changes in shift length or staffing patterns will increase the risk for complications such as infections.
Administrative changes generally can be implemented with minimal discussion, but they require planning. Examples of administrative changes may include the following:
� Changes to reduce provider documentation, billing and coding, registration, and other administrative policy burdens. These changes should be discussed in advance with the State and Federal agencies that oversee public health insurance programs and with private payers.
� Cancellation of elective procedures.
� Reassignment of qualified administrative nursing staff members to clinical roles or use of nonhospital staff members, potentially including family members, to provide basic patient care.
� Adoption of Continuity of Operations (COOP) strategies in each department as needed to cope with the impact of the event. A good COOP plan details the critical functions and staffing within each department and lists ways for these functions to be carried out when the staff or infrastructure is inadequate to carry on daily operations.
Clinical adaptations represent the allocation of scarce resources or services based on preestablished ethical principles as discussed earlier. Examples of clinical adaptations include the following:
� Triage of patients who would otherwise be treated as inpatients to home care, acute care sites, or other alternative care sites.
� Assignment of limited resources (e.g., ventilators, radiographs, laboratory testing) to those most expected to benefit.
� Provision of specialty care (e.g., burn or intensive care) by nonspecialty trained staff members (ideally with supervision by trained staff members).
The hospital should be able to follow State guidance regarding clinical triage decisions. If no guidance exists, the hospital will need a plan for bringing together the appropriate personnel who can make the critical decisions and reevaluate the situation during each planning cycle
26
(e.g., each shift per day). When there is little advance evidence to guide allocation decisions (for example, not knowing how different age groups of patients in an influenza pandemic respond to mechanical ventilation), good clinical judgment by experienced clinicians will be the final common denominator to justify resource allocation decisions. The decisionmaking process should be shared openly with staff members, patients, and the public and should be as consistent as possible across facilities.
There are no clear trip points to indicate when the shift from reactive, mostly administrative changes to proactive, clinical changes must occur. Situational awareness by the Incident Commander and Planning Section Chief can help anticipate or recognize resource bottlenecks that may require intervention.
Allocating Scarce Hospital Resources
Patient assessment. When resources are scarce, at a minimum patient assessment should include the following factors:
� Patient’s need for the resource.
� Potential to return to the baseline state.
� Overall acute resource needs of the patient.
� Health and prognosis related to an underlying disease or diseases.
� Event-specific or injury-specific prognostic factors.
If there is no differentiation in criteria between patients, then resources should be allocated on a first-come, first-served basis.
Patient triage. The four levels of priority for triage discussed earlier—green, yellow, red, and black—can be used in assigning patient acuity levels. An experienced health care provider should be involved in any decision to classify a patient as “black” during a disaster.
Addressing Select Operational Considerations
In addition to allocating scarce resources, an MCE will require that hospitals address many operational considerations, including security and mass mortuary.
Security. A patient surge that results in scarce resources may increase the potential for violence against health care facilities and providers. Hospitals should work with their community law enforcement agencies and hospital security staff to develop a security assessment and vulnerability analysis and a plan for increasing hospital security during a widespread disaster. This plan should prioritize hospital assets for protection and rely, when possible, on physical and technological solutions rather than human solutions.
Security measures that hospitals may wish to consider in an MCE include:
� Increased security personnel.
� Increased monitoring of hospital premises and surroundings.
� A lockdown plan that can be rapidly implemented (including campus buildings that may be used in nontraditional capacities as part of the facility response plan).
27

� Single or few designated entrances.
� Limiting visitors to one or none per patient.
� Metal detectors and security screening at entry points.
� Increased law enforcement presence (mutual aid agreements must be in place ahead of an event. Hospitals could consider using uniformed peace officers or National Guard personnel).
� Equipping and training hospital security personnel with nonlethal methods of behavioral control with appropriate policies and oversight (e.g., batons or pepper spray).
� Other deterrents at entrances (e.g., canine officers, increased uniformed security).
Mass Mortuary. Hospitals should understand the community plan for management of the deceased. In some cases, hospital responsibilities for record-keeping and reporting will change in a disaster. Temporary facility morgue facilities may be required, and regional processing sites may be needed.
Provisions should be made for appropriate solutions to barriers presented by culturally based funeral and burial practices. Every effort should be made to plan for adjusting standards of care as appropriate to the situation, to advise and involve the public and faith-based communities in these decisions, and to ensure as little disruption as possible to cultural practices and that the maximum level of dignity is afforded the deceased and their families.
Endnotes
50 Barbera J, Macintyre A. Medical and Health Incident Management System: A Comprehensive Functional System Description for Mass Casualty Medical and Health Incident Management. Washington: George Washington University Institute for Crisis, Disaster, and Risk Management; December 2002. Available at: www.gwu.edu/~icdrm. Accessed May 20, 2009. 51 Institute of Medicine. Hospital-based Emergency Care: At the Breaking Point. Washington: National Academies Press, 2006.
28

6. Alternative Care Sites
Key Questions What are the three most important issues to consider in establishing an alternative care site?
How do planners go about defining the role of an alternative care site?
How do planners choose an alternative care site?
What are the staffing options for alternative care sites?
To respond effectively to an MCE, community planners from municipal agencies, including public safety, public health, and emergency management must plan how ACSs will operate. The decision to open an ACS will be made in collaboration, as applicable, among:
� Local, Tribal, and regional emergency planners;
� Hospitals, outpatient clinics, multispecialty group offices and home care agencies;
� Health care workers responsible for operating the facility;
� County and State health officials; and
� Any other institutions that will participate in staffing or logistical support of the ACS.
Planners need to identify the logistical support necessary for establishing an ACS. A mechanism must exist for triage of patients, so patient needs are matched with resources. Planners must delineate the specific medical functions and treatment objectives that the ACS facility would need to accomplish. The facility may serve as:
� A primary triage point, providing primary victim care and helping decide which patients require hospitalization, which can be managed at home, which might need observational care and minimal interventions available at the ACS, which require palliative care, which also might be available at an ACS. Such a facility might be reasonably expected to cohort patients who have been exposed to certain infectious agents but do not need more than observation and minimal, if any, medical intervention.
� A community-focused ambulatory care clinic that serves as a point of distribution for medications, vaccinations, or other medical interventions that must be delivered to a wide population.
� A low-acuity patient care site to permit the offloading of stable patients from hospitals to increase their surge capacity or a primary site for the care of stable low-acuity patients.
Much of the information here also applies when a locale is supporting a Federal Medical Station (FMS). FMSs are deployed with logistical implementation teams by CDC’s Division of the Strategic National Stockpile and provide medical surge capacity (equipment, material, pharmaceuticals) to communities overwhelmed by mass casualties.
29

Ownership, Command, and Control The most important issues in the successful establishment of an ACS are ownership, command, and control of the ACS. These issues should be decided at a local or regional (as opposed to institutional) level and must involve the identification of those individuals with the authority to decide whether, when, and where an ACS should be opened and with the authority to operate the site. The administrative structure for operation of an ACS should follow HICS concepts.
An ACS should operate from a “concept of operations” document that defines its role in advance. The ACS also should be integrated into the local CDC Health Alert Network (HAN), which is designed to ensure that each community has rapid access to health information and professional personnel.
Resource
More information on CDC’s Health Alert Network is available at: http://www2a.cdc.gov/han/Index.asp.
Selecting the Site An ACS will likely be located in a building of convenience or shelter of opportunity. Each will have advantages and disadvantages. Possible ACSs include:
� Adult detention facilities.
� Aircraft hangers.
� Churches or schools.
� Community centers, recreation centers or meeting halls.
� Convalescent care centers.
� Fairgrounds.
� Hotels or motels.
� Government buildings, military facilities, or National Guard armories.
� Same-day surgical centers or clinics.
� Shuttered hospitals.
� Sports facilities (including stadiums).
� Trailers or tents (military or other).
Tentative sites are best identified in advance, and the mechanism of approval for use as an ACS should be investigated. As a rule, permission to use municipal buildings is easier to obtain, and it is easier to obtain MOUs to use existing staff members. Although site selection is usually a local function, State partners should be asked early in the planning process whether potential shelters or ACSs have been designated at a State or regional level. If the ACS must supply ambulatory patient care, it may help if it is located near a victim shelter to support victims with chronic medical needs.
30
A key decision point in care delivery at an ACS is whether the ACS will be able to provide oxygen and respiratory therapy, particularly mechanical ventilation. Sustaining oxygen delivery systems in an ACS setting is complex and can be expensive. The exception to this may be the use of nursing homes and long-term care facilities, given their existing medical gas supply.
AHRQ and ASPR are currently updating the ACS Selection Tool, which is designed to use in advance of a public health emergency to develop and maintain a list of potential ACSs. The new Disaster Alternate Care Facility Selection Tool was in press at the time of this report’s publication. To check on availability, go to http://www.ahrq.gov/prep/.
Another useful tool from AHRQ is Reopening Shuttered Hospitals to Expand Surge Capacity. Although this tool focuses specifically on assessing shuttered hospitals, much of the information is valuable for assessment of any site.
Resource
Reopening Shuttered Hospitals to Expand Surge Capacity is available at http://www.ahrq.gov/research/shuttered/.
Arranging for Supplies and Equipment Routine supply chains will be stressed or not operational during an MCE of any magnitude or duration. Although the degree of need for certain supplies may be event specific (e.g., increased need for masks during a pandemic), the need for many basic supplies can be accurately forecasted. This is especially true for basic durable medical equipment (cots, IV poles, wheelchairs, etc.). Certain supplies have a limited shelf life and therefore will require product rotation or replacement. Supplies may be stored as portable caches, which can be transported to the ACS. Caches can vary from a bare minimum cache (Level I) for institutional augmentation to a very complete cache (Level III) as defined by the Soldier and Biological Chemical Command. Caches of supplies should be stored in modular units supporting 50–100 patients, allowing an ACS to be set up in stages.
As noted above, supplying supplemental oxygen to patients in an ACS poses a complex challenge. The three major mechanisms of supply are compressed cylinders, oxygen concentrators, and liquid oxygen. Each of the three mechanisms has advantages and disadvantages. At least two and possibly all three will be necessary.
Wheelchairs, walkers, and canes will also be needed in an ACS. Local or regional resources are not likely to be sufficient to deal with this requirement.
Expensive diagnostic and monitoring equipment (e.g., portable x-ray machines, ultrasounds, cardiac monitors) may be beyond the scope of an ACS. Advances in point-of-care clinical laboratory testing, however, may allow some basic laboratory tests to be performed at an ACS.
The Hospital Surge Model (see page 3) can help with determining resources needed for specific scenarios.
Securing Pharmaceuticals
Pharmaceuticals require environmental storage, stock rotation, and legal control. In certain
31
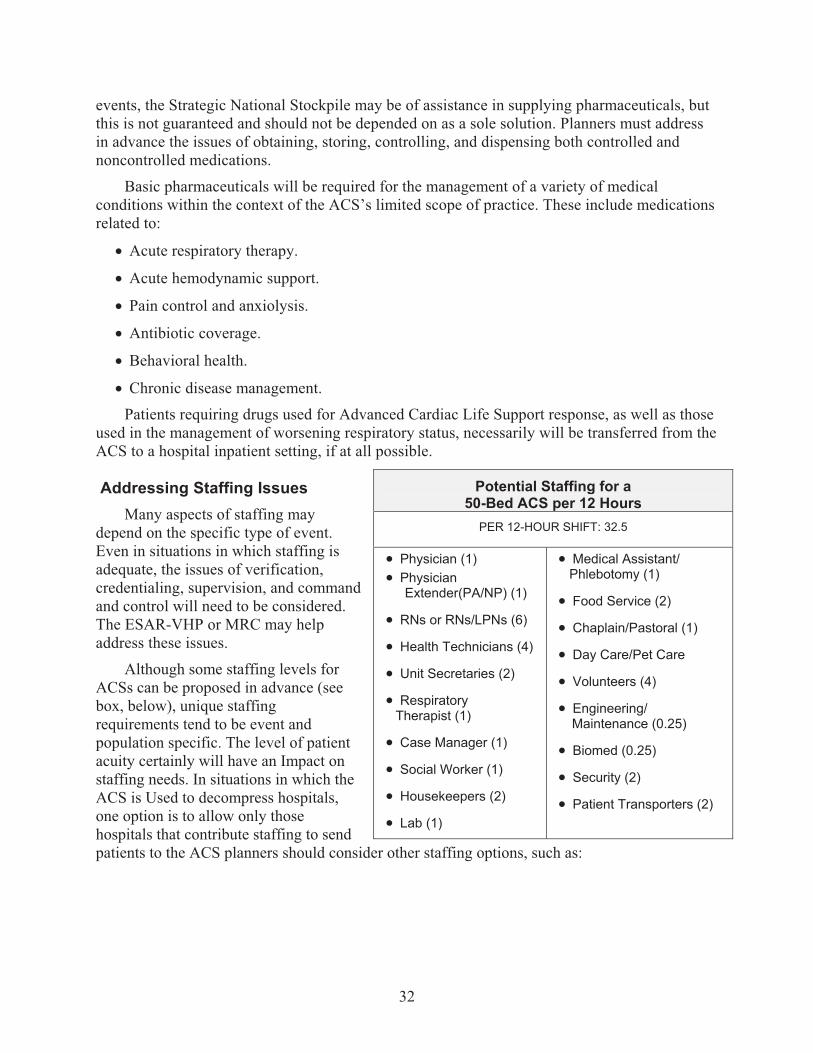
events, the Strategic National Stockpile may be of assistance in supplying pharmaceuticals, but this is not guaranteed and should not be depended on as a sole solution. Planners must address in advance the issues of obtaining, storing, controlling, and dispensing both controlled and noncontrolled medications.
Basic pharmaceuticals will be required for the management of a variety of medical conditions within the context of the ACS’s limited scope of practice. These include medications related to:
� Acute respiratory therapy.
� Acute hemodynamic support.
� Pain control and anxiolysis.
� Antibiotic coverage.
� Behavioral health.
� Chronic disease management.
Patients requiring drugs used for Advanced Cardiac Life Support response, as well as those used in the management of worsening respiratory status, necessarily will be transferred from the ACS to a hospital inpatient setting, if at all possible.
Addressing Staffing Issues Many aspects of staffing may depend on the specific type of event. Even in situations in which staffing is adequate, the issues of verification, credentialing, supervision, and command and control will need to be considered. The ESAR-VHP or MRC may help address these issues.
Although some staffing levels for ACSs can be proposed in advance (see box, below), unique staffing requirements tend to be event and population specific. The level of patient acuity certainly will have an Impact on staffing needs. In situations in which the ACS is Used to decompress hospitals, one option is to allow only those hospitals that contribute staffing to send patients to the ACS planners should consider other staffing options, such as:
Potential Staffing for a50-Bed ACS per 12 Hours
PER 12-HOUR SHIFT: 32.5
� Physician (1) � Physician
Extender(PA/NP) (1)
� RNs or RNs/LPNs (6)
� Health Technicians (4)
� Unit Secretaries (2)
� Respiratory Therapist (1)
� Case Manager (1)
� Social Worker (1)
� Housekeepers (2)
� Lab (1)
� Medical Assistant/ Phlebotomy (1)
� Food Service (2)
� Chaplain/Pastoral (1)
� Day Care/Pet Care
� Volunteers (4)
� Engineering/ Maintenance (0.25)
� Biomed (0.25)
� Security (2)
� Patient Transporters (2)
32
� Regional hospital alliances, which can designate in advance a small number of key staff members, including pharmacists, laboratory workers (to be responsible for the point-of-care testing), respiratory therapists, and administrators to help support ACS operations.
� A single hospital, which can adopt an ACS and in so doing may be able to provide staffing for an entire ACS.
� The faith-based community and community health workers, which also can be viable sources of volunteers.
� Academic medical centers, which can be sources of teams of health care workers with centers outside of the local geographic area in advance of an event
� Administrative staff from large, geographically diverse health care systems, who also can help meet staff needs.
Planners need to establish guidelines and protocols in advance for the care and management of patients treated in an ACS. These guidelines should help to minimize the difficulties inherent in bringing a new team of health care professionals together for the first time.
Other potential issues include:
� Advance negotiation of overtime contracts in cases where municipal-owned buildings are to be used as ACSs with municipal workers providing support staffing.
� Identification of staff members, patients, and their family members, which will require a name badge system that can be as simple as stick-on name tags or as complicated as a site-generated photo.
� Housing provisions for the staff.
Arranging Operational Support
Actual operation of an ACS will require a host of support services, including food services, sanitary services, infrastructure maintenance, and security. Although some of these needs will be driven by the nature of the event, much planning can and should be done in advance to assure that these support services will be delivered.
Documentation of Care
Only modest patient care documentation can be expected at an ACS. Electronic medical records are not likely to be available or practicable. Rather, simple paper-based charting will be required. Forms for patient records (including nursing notes and flow sheets), patient tracking and discharge planning should be prepared in advance. Forms should be in adequate supply, along with clipboards and pens.
Security Issues
As with hospital systems, ACS planners must develop robust security plans.
33
Rules and Policies for Operation
Rules of behavior for patients, caregivers, and visitors are necessary for the smooth operation of the ACS. ACS planning should include establishment of such a set of rules, as well as operating procedures. Operating procedures should address incident command, staffing, criteria for admission, discharge and transfer, clinical roles and responsibilities, infection control, pharmacy and medication control, security, supplies, finances, documentation, staff housing, housekeeping, food services, and areas unique to the event.
Development of an Exit StrategyCriteria for disengaging the ACS should be established as part of the planning process. The
actual decision to close the facility should be made in concert with local emergency managers and local or State health officials.
Exercising the ACS Plans for a regional ACS can be fully vetted only through exercises. Ideally, these exercises
should include the ACS as a stand-alone facility and use the ACS support components in cooperation with other entities such as health care systems and Federal assets such as FMS and DMAT.
34
7. Palliative Care
Key Questions What is palliative care?
How should palliative care be managed during a mass casualty event?
What steps can planners take to recruit and train palliative care providers in advance of a mass casualty event?
The World Health Organization defines palliative care as “an approach which improves the quality of life of patients and their families facing life-threatening illness, through the prevention, assessment, and treatment of pain and other physical, psychosocial, and spiritual problems.” Those who may not be expected to survive following a catastrophic MCE may include:
� Those who are expected to die over the course of weeks (e.g., those with radiation exposure).
� The already existing palliative care population (e.g., those already enrolled in hospice or receiving palliative care in acute care settings).
� Vulnerable patients (e.g., patients with advanced illness in long-term care facilities) whose situation will be worsened due to scarcities associated with the event.
� Patients who are triaged as a result of scarce resources.
While it is important to understand what palliative care is, it is also important to specify what it is not. Palliative care is not abandonment of the patient or reduction or elimination of treatment. Rather, it involves active treatment for symptom management and support to address the comfort of the patients and their families. The aggressive and appropriate treatment of pain and other symptoms is not euthanasia, nor does it hasten death. The application of palliative care principles in an MCE would include:
� Recognizing that initial prognostication may change if additional resources become available or if the situation deteriorates.
� Honoring the humanity of the dying and those who serve them (whether loved ones, professionals, or strangers) by providing comfort and social, psychological, and spiritual support.
Making Triage and Treatment Decisions
In the interest of maximizing good outcomes for as many patients as possible and, at the very least, providing palliative care to all who need it, treatment decisions will have to balance utilitarian notions with other ethical values, with medical effectiveness as a key determinant. Priority access to scarce resources may be given to those with the greatest potential for survival.
35

Thus, services to those expected to die soon will fall more heavily on people who do not have substantial prior health experience and expertise. Recommended actions include:
� Integrating knowledgeable professionals and organizations (e.g., geriatricians, palliative care clinicians, long-term care providers and organizations, home health providers, hospice providers) into local, tribal, State, and regional disaster preparedness to fully incorporate palliative care into State and local disaster planning/training guidelines, protocols, and activities.
� Including pediatric-specific palliative care issues in all plans, and developing guidelines for treating them. Failure to do so will hamper the ability of health care workers to move children into palliative care.
� Basing planning on lessons learned from previous disasters (including war).
� Establishing practical measures of success in palliative care services in MCEs.
� Conducting gap analyses and tabletop exercises on how to integrate palliative care services into preparedness systems.
� Encouraging attention to palliative care in all four phases of emergency management (mitigation, preparedness, response, recovery) and in all relevant settings (prehospital, acute care/hospital, and ACS).
Casualties will be triaged at the site of the incident. Some patients will be deemed likely to die during the catastrophe and therefore will be triaged not to receive (or not to continue to receive) life-supporting treatment. For these casualties, death will be expected within a short period.
This reality poses substantial challenges for all involved, including the recognition that some people who might survive under other circumstances now will die. Given the usual focus of rescue in manageable disaster events, most patients, families, and emergency responders are likely to resist this designation and attempt to save all, potentially exacerbating an already overwhelmed medical care system. Thus, ACSs and providers need to be identified and used for this population during catastrophic MCEs. Recommended actions include:
� Building smooth links with supportive service organizations and personnel (e.g., home health, long-term care settings, hospice, and palliative care providers) for those expected to die.
� Working with first responder personnel and local and regional disaster response planners (e.g., EMS, fire, police, departments of public health, community health clinics, local and regional governmental entities) to develop clear guidelines and protocols to address the following issues :
o Triage.
o ACSs for palliative care.
o Who delivers treatment and support (e.g., spiritual, psychological) and how.
o What levels of care are to be delivered in what settings and by whom.
o Training of providers for the provision of appropriate palliative care at all treatment sites.
36
o Lines of authority and the clear identification of responsible personnel.
o Identification of location and use of stockpiles, supplies, and personal protective equipment.
o Building strong support for triage and standards of care to respond to dire circumstances or scarce resources by redefining public expectations and training of palliative care and other health professionals. Actions would include:
o Establishing psychological and ethical support for front-line responders.
o Establishing flexible methods of response for revising triage decisions and treatment when affected persons are doing better than expected.
o Expecting anxiety and strong emotions and have security and appropriate medications available.
o Establishing guidelines and protocols for “just-in-time” training and palliative service delivery from secondary providers at all treatment sites.
Arranging for Medical Supplies and Equipment
Supply arrangements must be identified as part of the community planning effort not only to ensure that all potential palliative care supply sources are included, but to prevent too many organizations from unknowingly relying on the same suppliers. Mutual aid agreements should be made ahead of time with community agencies, other health care providers, and backup suppliers to ensure that resource needs for palliative care service delivery can be met. To ensure supplies and equipment are available:
� Stockpile palliative care medications in each community for disaster response, including injectable morphine, dihydromorphone, and haloperidol, subcutaneous butterfly needles, dressings, antipyretics, steroids, and diuretics.
� Plan for the needs of patients who are chronically dependent on dialysis, ventilators, or the supplies such as dressings, splints, syringes and oral droppers, incontinence supplies, beds or cushioned surfaces, and personal protective devices.
Long-term care facilities, inpatient hospice settings, or home nursing care offices are possibilities for storage sites. Controlled substances in lockboxes are probably most naturally kept at nursing homes, where systems for storage of these drugs are already in place. Another option would be designated pharmacies. The effectiveness of these two options obviously would depend on their proximity to the disaster scene.
Training Training in palliative care may include:
� Building on existing training models to incorporate palliative care services training. Training in palliative care must occur prior to an MCE and will involve many layers of education and practice.
� Cross-training personnel from other areas of expertise as well as other areas of the country to provide aid. In addition, lay persons can be recruited to serve (e.g., bus drivers, mail deliverers, anyone from the community who is willing to attend the training). Education
37
and training should be competency based, with programming specific to the individual’s role in emergency response.
� Incorporating palliative care training for first responders as part of disaster and MCE planning.
� Training all first responders to use oral and injectable morphine to manage pain and symptoms until licensed personnel are available. How to locate and access the medication should be part of training. Ensure that all first responders are familiar with the basics of psychosocial counseling for peer-to-peer and provider/patient support.
� Developing and implementing competency-based evaluation and measurement.
� Providing personal protection and individual response training that first responders ordinarily receive to lay or professional individuals designated as responsible for providing palliative care.
Recruiting Professional Providers and Volunteers
With planning, a community can develop a reasonable reserve capacity for providing palliative care during an MCE. Local palliative assistance teams can be recruited from a variety of practice settings (e.g., hospices, hospitals, long-term care) and disciplines (e.g., physicians, nurses, social workers, chaplains). These teams can be developed locally with sponsorship from groups such as senior centers, churches and synagogues, hospices, long-term care providers, nurses’ organizations, senior citizens’ organizations (e.g., AARP, the National Hospice and Palliative Care Organization, the American Academy of Hospice and Palliative Medicine, and local hospitals and palliative care programs.
Planners should consider incorporating these teams under the MRC and the Community Response Team (CERT) for deployment depending on the nature and scope of an incident. Planners also should consider extending the credentialing of palliative care disaster volunteers into the existing disaster response Federal/State and local legal/insurance systems in order to expand community capacity through such mechanisms as the ESAR-VHP. These rapid response teams would supplement, not replace, local palliative care services.
Arranging Mental Health and Spiritual Care Services Psychological and spiritual counseling and support should be made available to those not
expected to survive and their families.
Local mental health care providers, such as psychologists, chaplains, and health care providers, are a vital resource. A number of behavioral, psychological, and spiritual response plans have been developed and can serve as the basis for the planning and delivery of these services in an MCE (see box below).
Support will be needed by response providers as well. As the volume of patients triaged to palliative care expands, so will the strain of providing mass palliative care. These individuals also will need to have periodic emotional and psychological relief (e.g., by having them rotate to teams that are doing other types of work, such as delivering food); this is important for the welfare and morale of the provider corps as a whole.
38
Resources
Mental Health All-Hazards Disaster Planning Guidance is available from the Center for Mental Health Services, Substance Abuse and Mental Health Services Administration (SAMHSA) at http://mentalhealth.samhsa.gov/publications/allpubs/SMA03-3829/default.asp.
Mental Health Response to Mass Violence and Terrorism is available from the Center for Mental Health Services, SAMHSA at http://mentalhealth.samhsa.gov/publications/allpubs/SMA-3959/default.asp.
Preparing for the Psychological Consequences of Terrorism: A Public Health Strategy. Is available from the Institute of Medicine at http://www.iom.edu/CMS/3775/3895/11573.aspx.
Psychological First Aid: Field Operations Guide, Available from the National Child Traumatic Stress Network and National Center for PTSD at http://ncptsd.va.gov/ncmain/ncdocs/manuals/nc_manual_psyfirstaid.html.
Disaster Mental Health for Responders: Key Principles, Issues and Questions is available from theCenters for Disease Control and Prevention at http://www.bt.cdc.gov/mentalhealth/responders.asp.
Managing the Dead
A number of behavioral, psychological, and spiritual response plans can serve as the basis for the planning and delivery of these services in an MCE. For example, Disaster Mortuary Operational Response Teams (DMORTs) are composed of private citizens, each with a particular expertise. DMORTs work under the guidance of local authorities, providing technical assistance for body recovery and assisting with identification of remains. Recommendations include:
� Pay attention to and be respectful of religious beliefs and approaches to body management.
� Do all that is possible to document the identity of the dead and the disposition of the body, for the benefit of the survivors. After a disaster, the identification and disposal of human remains are typically handled by the local community. The remains typically pose no immediate health risk in a natural disaster but may pose considerable risk in an epidemic.
� Address issues such as the supply of body bags and refrigerator trucks, ways to catalog bodies, and cremation with local funeral directors prior to an MCE. Include DMORTs, funeral directors, and medical examiners in disaster planning and drills.
Resource
Information about Disaster Mortuary Operational Response Teams is available at http://www.dmort.org/.
39

8. Influenza Pandemic PreparednessOverview This chapter applies information from the previous chapters to preparing for a specific mass casualty event--an influenza pandemic.
An influenza pandemic is a “developing impact” mass casualty event (MCE). It occurs in many areas simultaneously. Indeed, a pandemic affects a large part of the population across the world and across all age groups, including the health care and emergency response workforce. Large numbers of patients may quickly overwhelm hospitals and emergency departments and necessitate the allocation of scarce resources.
The National Strategy for Pandemic Influenza Implementation Plan puts the bulk of the planning and coordination responsibility on States and localities rather than the Federal Government. Because many communities may be simultaneously affected, State and local health authorities and community planners represent the front lines of pandemic preparedness response planning efforts.
Resources
The Department of Health and Human Services Pandemic Influenza Plan is available at www.flu.gov.
The National Governors Association Primer for Governors and Senior State Officials is available at www.nga.org.
CDC Pandemic Influenza information for Health Professionals is available at http://www.cdc.gov/flu/pandemic/healthprofessional.htm .
World Health Organization materials on influenza preparedness are available at http://www.who.int/csr/disease/avian_influenza.
State health planning information from The Association of State and Territorial Health Officials is available at http://www.astho.org/Programs/Infectious-Disease/H1N1/.
For planners incorporating home health care as part of their ACS strategies, Interim Guidance for H1N1 Flu (Swine Flu): Taking Care of a Sick Person in Your Home is available at http://www.cdc.gov/h1n1flu/guidance_homecare.htm.
Planners should create their pandemic preparedness plans now, practice and exercise the plans, and revise them when necessary. Effective and coordinated risk communication, domestically and internationally, before and during a pandemic, is essential to help the public understand the rationale for recommended actions and accept the prioritization of scarce resources.
Communications activities include identification of credible spokespersons at all levels of government to communicate informative and timely messages Available communications tools (see box) should be used to develop messages to address the issues, including the uses of scarce
41

resources and caring for the sick at home. Communities should identify which resources will be needed and which processes and systems should be put in place and prepare their plans now.
ResourceRisk communications training guides are available at www.pandemicflu.gov/rcommunication.
Background
All influenza viruses are capable of mutating. When a novel strain of virus gains the capacity to spread in humans, an influenza pandemic may ensue.
We have experience with pandemics. Over the course of the last century, the world witnessed three pandemics: the “Spanish influenza” of 1918, which resulted in a worldwide death toll of more than 50 million; the “Asian influenza” in 1957, which resulted in 1-to-2 million deaths worldwide; and the “Hong Kong influenza” in 1968, with 700,000 deaths worldwide.
With novel viruses, people have little or no immune protection, so most are susceptible. The supply of antiviral drugs may be inadequate and the development of a vaccine may take a long time. Moreover, as with any public health emergency, shortages of supplies, equipment, and hospital beds are possible.
Potential shortages of ventilators could be particularly problematic. Hospitals may not have an adequate supply of reserve ventilators to treat patients suffering from acute respiratory failure. The Centers for Disease Control and Prevention (CDC) has a limited reserve supply of thousands of mechanical ventilators in the Strategic National Stockpile that may deployed at the time of a pandemic to alleviate some of the shortfall. The American Association for Respiratory Care (AARC) has issued a set of guidelines and recommendations on ventilator capacity.
A pandemic may result in school closings and increased worker absenteeism as employees remain at home because of their own illness or that of a family member.
ResourceAARC Guidelines for Acquisition of Ventilators to Meet Demand for Pandemic Flu and Mass Casualty is available at http://www.aarc.org/resources/mass_casualty/index.asp.
Concepts, Strategies, and Actions for Planners
The following sections detail concepts, strategies, and actions that planners need to incorporate into their preparedness planning for pre-pandemic, early pandemic response, and widespread pandemic response periods of a hypothetical pandemic. Concepts and actions for prehospital, hospital, alternative care site (ACS), and palliative care sectors are highlighted.
In a flu pandemic, planners should emphasize the importance of the home as a “safe haven” and consider the use of primary care vans to provide services so that people may remain in their homes. At the same time, planners need to recognize the vital role of primary care providers in deciding which patients may remain at home and which patients need to go to the hospital.
42

Primary care providers may be the first medical personnel contacted, and the ambulatory care system will be critical in keeping hospitals from being overwhelmed.
Many concepts provided here will need to be tailored to the resources and systems in each locality, region, or State. This chapter aims to provide community planners with options to consider. Further pandemic influenza planning resources are listed in this and previous chapters.
PRE-PANDEMIC PERIOD: GENERAL COORDINATION AND PLANNING ISSUES
Most advance planning for a pandemic should take place in the pre-pandemic period. An overview of issues and activities that community planners need to consider is listed below.Command Structure
� Determine the trigger for emergency health powers provision (see discussion of legal issues in Chapter IV of this guide).
� Discuss with hospital associations and local and State public health officials when the trigger would be pulled and who would make that decision.
� Develop continuity of government and leadership protocols in the event that senior leadership becomes incapacitated or dies.
� Conduct regional exercises that are inclusive, use realistic scenarios, involve all responders, and embrace participation from agencies that are often not included.
� Include local and State political representatives, using education and exercises to get them involved, committed, and supportive.
� Consider special needs populations and children in all planning scenarios. Communications
� Begin a public communication campaign. Focus the messaging campaign on managing expectations; and providing updates on the community plan for pandemic response, including community care sites. This communications campaign should be a joint effort by hospitals, hospital partners, and public health departments.
� Emphasize prevention. Inform and educate the public about influenza. Provide advice and information on prevention and interventions to reduce virus transmission so that if and when the virus arrives, the public is knowledgeable about reducing the spread.
PREHOSPITAL: PRE-PANDEMIC PERIOD � Maintain standard precautions for every patient encounter.
� Preplan community staging locations—predesignated sites that could be opened in advance for alternative care and EMS staging.
ResourceAn Emergency Medical Service and Medical Transport Checklist is available at http://www.flu.gov/professional/hospital/emgncymedical.html.
43
� Locate surge transport assets in advance.
� Arrange mutual aid agreements for acquiring and using specialized assets by meeting with local and regional transportation authorities or businesses and agreeing by memorandum of understanding (MOU) on available assets (e.g., buses and other transport, staff augmentation), deployment, and staging locations. The MOU could be enhanced further by the development of a pre-event contractual agreement between the government and these institutions.
� Evaluate triage models such as JUMPSTART Pediatric Mass Casualty Incident Triage Tool and Sacco Triage Method.
� Develop and publicize call centers to minimize load on hospitals and clinics.
PREHOSPITAL: EARLY PANDEMIC RESPONSE PERIOD
Command Structure
� Establish an Emergency Operations Center (EOC). The EOC should include, but not be limited to, representatives of the following groups: community health centers, home health care organizations, hospitals, Public Health agencies (local, State, and Federal), Metropolitan Medical Response Systems, long-term care organizations, and other health-related groups.
� The EOC will coordinate all EMS resources including public, private, and volunteer.
� The EOC should encourage the use of area health operation centers to allow the EOC to communicate directly with a larger medical community, for guidance and direction.
� Determine in advance a trigger for opening an EOC.
Resource
Emergency Personnel Guidance: EMS and 9-1-1 Personnel - Managing Confirmed or Suspected Infections is available at http://www.cdc.gov/h1n1flu/guidance_ems.htm.
Communications� Establish a comprehensive public information strategy.
� Use mass media to provide the public information on preventive measures, home care management, and the appropriate time to seek health care services.
� Use community health care call centers to reinforce mass messaging and to provide additional and more tailored information to individuals with questions and concerns. Review these issues for their value as potential mass media messages.
Resources Managing Calls and Call Centers During a Large Scale Influenza Outbreak: Implementation Tool isavailable at http://www.cdc.gov/h1n1flu/callcenters.htm.
Adapting Community Call Centers for Crisis Support: A Model for Home-Based Care and Monitoring is available at http://www.ahrq.gov/prep/callcenters/.
44

� Use community call centers to assist with outpatient (home care) monitoring and support, thereby helping to extend the reach of public health and healthcare systems into households.
� Use information collected by the call centers for situational awareness and disease outbreak management and control.
� Engage mutual aid partners for sharing assets.
� Consider home care preparations. During a pandemic, it is likely that the home will serve as a major care site. Planners may want to consider the following steps:
� Ensure adequate stock of routine chronic care medications is available to the community.
� Include basic first aid supplies, including bandages, antipyretic medications (acetaminophen, ibuprofen, oral electrolyte solutions), and thermometers.
� Ensure that backup utility support is in place for those patients requiring electricity support for medical devices should the power grid be disrupted by decreased staffing.
� Provide advice on the establishment of a “sick room” in the home for primary management of ill household members.
� In the event of caring for patients with advanced symptoms too sick for hospital care, provide symptom palliation with a home care team coordinated by local public health authorities.
PREHOSPITAL: WIDESPREAD PANDEMIC RESPONSE PERIOD Set Up and Use of Casualty Treatment Areas
� Use formal triage and treatment protocols and complete triage and treatment in nontraditional triage/treatment areas by bringing prehospital personnel to those areas.
� Determine who can be treated on site to include those with moderate (yellow) and minor (green) triage status.
� Determine who should be transported to area hospitals and by what means, with the sickest casualties with a reasonable chance of survival treated and transported first.
� Consider suspension of some medical protocols (e.g., base contact for certain interventions, expansion of scope of practice, appropriate standard of care).
� Consider secondary triage methodologies such as one hospital triaging patients to another. 911 Dispatch Issues
� Arrange for dispatchers to screen response need.
� Provide precaution advice for scene responders.
� Limit the number of responders to the minimal necessary response.
� Provide a nonemergency information and advice line.
45

Best Use of Available Personnel
� Create modified shifts. Expand number of providers and vehicle types. Call for volunteers from within the hospital system. Assign to clean; transport specimens and patients; deliver oral fluids to patients; support those waiting to be seen with fluids oral fluids; and restock waterless hand cleaner, tissues, mask dispensers.Maximum Transport Capability
� Staff ambulances with one EMT and one non-EMT driver (such as a firefighter, police officer, etc.).
� Expand the use of paramedic-initiated alternative transport mechanisms (e.g., buses, taxis, privately owned vehicles).
� Load ambulances with more than one patient, e.g., two critical, one critical plus one or more noncritical. (Air transport probably will be of limited use.) Maximum Personal Protection Available to Personnel
� Distribute vaccine to personnel and consider including family members in the vaccine distribution.Maximum Destination Choices
� Encourage home care rather than transport, if possible.
� Transport patients not only to hospitals but also to clinics and ACSs.
� Consider “batching” noncritical calls in the same geographic area and transporting all patients to the closest appropriate facility rather than the facility of the patient’s choice.
HOSPITAL: PRE-PANDEMIC PERIOD
ResourcesA detailed hospital pandemic preparedness checklist is available at http://pandemicflu.gov/plan/healthcare/hospitalchecklist.html.
Overall hospital pandemic planning information is available atwww.hhs.gov/pandemicflu/plan/sup3.html#s3-III.
� The Hospital Planning Committee, a multidisciplinary committee including response partners (see box below), should complete all parts of the hospital pandemic influenza preparedness and response plans.
46

The potential hospital pandemic influenza planning committee may include representatives from the following departments, among others:
� Administration/senior management � Legal counsel/risk management (including
fiscal official � Infection control/emergency coordinator � Hospital disaster/emergency coordinator � Safety director� Engineering/physical plant� Nursing administration� Medical staff including outpatient� Intensive care unit� Laboratory services� Pharmacy� Environmental services (housekeeping,
laundry)� Public relations� Security� Materials management
� Education/training/staff development� Occupational health� Diagnostic imaging� Information technology� Adjunct staff (infectious diseases, mentall
health, union representatives, human resources, director of house staff/fellowship and other training programs, pathology, social work, critical care medicine, pathology)
� State and local health departments (communicable diseases division, laboratory services, medical examiners)
� Community partners (emergency medical technicians, local law enforcement, funeral service personnel, community service agencies, Federally qualified health centers and other health care safety net providers)
Source: HHS Pandemic Influenza Plan at www.hhs.gov/pandemicflu/plan/sup3.html#box1.
� Assess surge capacity (beds, ventilators, etc.) to meet expected increased needs.
� Develop plan to expand staff capacity. Determine how the hospital will meet staffing needs.
� Develop contingency plans for staff absences, particularly ED staff.
� Create procedures and policies for use of supplemental providers.
� Consider volunteers, ESAR VHP, CERT, MRC, clinic staff, out-of-State licensed staff, National Guard, retirees, non-health-care staff, among others.
� Ensure policies are in place to test and manage deployment of nonhospital personnel at both the community and hospital levels.
� Ensure that a plan for managing volunteers is in place.
� Initiate discussions of allocation of hospital resources; hospital administrators meet with hospital ethics committee early in planning process:
� Establish hospital process for scarce resource allocation.
� Develop communication process so community understands the rationale behind resource allocation policies.
� Stockpile supplies and equipment including PPE equipment (e.g., gloves, masks).
47
� Estimate increased need for medical equipment/supplies and develop strategy to acquire additional equipment/supplies if needed. Consult with local and State health departments about access to the Strategic National Stockpile.
� Develop facility access guidelines.
� Define essential and non-essential visitors and develop policies for restricting visitors during a pandemic (and mechanisms for enforcing the policies).
� Plan to limit hospital entry to a few key entrances.
� Plan for increased security needs.
� Develop a health care risk communication message, including criteria for seeking health care, such as postponement of elective procedures or surgeries.
HOSPITAL: EARLY PANDEMIC RESPONSE PERIOD
Command Structure
� Activate the Hospital Incident Command System (HICS), open a hospital command post and assign an Incident Commander (IC).
� Hold briefings for administrators and staff members. Review talking points and discuss general action plans to be followed in the event that a flu pandemic should spread across the United States.
� Confirm the hospital process for allocating scarce resources. Activate/test internal hospital committees on standards of care if necessary. Review policies and protocols. Training
� Conduct just-in-time-training for staff via e-mail, posters, and shift briefings. Include information on transmission, infection control, ventilator management, and hospital plans.
� Conduct personal protective equipment (PPE) training. Perform fit testing, donning and doffing instruction, practice, and competencies for inpatient and outpatient staff. Supplies
� Increase hospital supplies from the usual baseline of 3-day supply to 7-day supply if possible (based on an estimated 150 percent occupancy rate). Order, inventory, and increase par levels of IV fluids, medicines, linens, and other consumable medical goods.
� Estimate quantities of essential patient care materials and equipment and personal protective equipment that would be needed during an 8-week pandemic with subsequent 8-week waves. Communications
� Establish lines of communication among Public Health officials, hospitals, EMS and emergency medicine to provide daily updates. Identify personnel/procedures to run the Joint Information Center.
� Designate a public relations person as the hospital Public Information Officer.
� Reinforce the public information messaging begun in the pre-pandemic period.
48

Drills, Tests, and Reviews
� Test Health Alert Network (HAN) to include off-hours and notification of HAN alerts from the ED to infection control.
� Review plans for security, behavioral health, and general disaster contingencies.
� Review the facilities plan, including heating, ventilation, and air conditioning and other cohorting plans. Monitoring the Outbreak and Screening Outpatients
� Establish a local public health point of contact. Begin Department of Health monitoring of influenza-like illness (outpatient and inpatient). Screen outpatients per CDC guidance for influenza symptoms based on fever and/or respiratory symptoms and travel history. Begin screening at the Emergency Department and outpatient clinic check-in points.
Resource
Clinician guidance on identifying and caring for patients is available athttp://www.cdc.gov/h1n1flu/identifyingpatients.htm.
� Verify referral agreements with local hospitals to ensure that patients will be accepted. Clarify patient movement between hospitals for infectious cases (e.g., EMS protocol for transfer patients) and within a hospital (e.g., protocol for elevator transport of pandemic patients).
� Reinforce infection control and respiratory etiquette for those with respiratory symptoms using posters, staff reminders, educational materials, and patient masks and tissues at triage and clinic registration points and near common points such as elevators and major entrances.
� Plan for Vaccine Distribution. Arrange internal distribution to staff members based on prior planning and in concert with State and regional plan criteria for essential personnel. Patient Screening
� Limit hospital entry to a few key entrances.
� Screen patients for symptoms of influenza and relevant travel history and with rapid diagnostic tests if available.
� Mask patients with suspect symptoms and make sure that providers wear appropriate PPE.
Hospital Surge � Notify surgeons that elective surgeries must be suspended due to surge.
� Ramp up outpatient services by increasing clinic hours and personnel to provide nonurgent services. Extra staffing will be needed because outpatient services will be a likely place for screening for flu.
� Cohort to separate those with flu-like symptoms from those with chronic illnesses who could be susceptible to developing more severe illness.
� Ensure that backup utility support is in place should the power grid be disrupted by decreased staffing for those patients requiring electricity support for medical devices.
49

� Establish a hospital hotline and enable the prerecorded greeting to triage calls for information to nonclinical staff and clinical inquiries to appropriate staff at the department of health.
� Prepare flat space areas in conference rooms, auditoriums, etc., for patient care (organize cots, linens, etc.).
� Open a joint information center (JIC) with the hospital association acting as liaison with all hospitals in the region. The regional coordinating hospital provides updates and solicits baseline availability of ventilators and patient beds.
HOSPITAL: WIDESPREAD PANDEMIC RESPONSE PERIOD
Planning and Information
� Institute action planning. The planning section anticipates resource needs for the next operational period and gathers situational information from within the hospital and from regional/State entities. It also determines staffing and availability.
� Activate the Joint Information Center. The JIC is managed by the hospital association liaison for all hospitals in conjunction with Public Health and EMS. The JIC provides a daily briefing for staff and media, provides daily media messages and holds press conferences. Multiagency Coordination
� Have key representatives from public health, emergency medicine, EMS, and hospital staff monitoring information on the system status from all agencies/hospitals (including liaisons from neighboring States).
� Conduct action planning at the regional level.
� Compare the triage levels at area facilities to assure consistency.
� Request resources (when possible) via jurisdictional Emergency Medicine.
� Use the staffing coordinator to manage public health, emergency medicine, EMS, and hospital requests for staffing and allocates them based on the resources available, including the Medical Reserve Corps and ESAR VHP.
� Communicate with the local Emergency Operations Center or Department of Health about regional resource and policy needs.
� Ensure public health coordination with home care agencies and messaging, hotline, and Internet support for families. Review of Staffing Plans
� Use families to provide basic patient care. The hospital should engage the patients’ families (one person at a time) to provide basic patient care, such as feeding. Nurses (including Medical Reserve Corps, ESAR-VHP, and retirees with appropriate mentorship by current staff nurses) provide medications and assessments and review vital signs.
50

� Respiratory therapy manages ventilators only; other respiratory care services are to be provided by nurses. Train floor nurses in basic ventilator monitoring, with floor units supervised by a roving ICU nurse to monitor ventilated patients.
� Physicians see patients on an as-needed basis, providing critical interventions and assessment for interventions, transfer, and discharge.
� Consider expanding staff capacity with changes in staff scheduling (e.g., duration of shifts, staffing ratios, changes in staff assignments).Use of Hospital Space and Supplies
� Set up cohort areas of inpatient and outpatient units for infectious patient care. These areas can be used when volume allows. (The entire facility may be a cohort during peak periods.)
� Discontinue elective surgery scheduling. Only immediate need or emergent surgery is done.
� Select operating room and procedure room space to be used for additional ventilated patient care.
� Use minimal documentation. Use short assessment and plan notes – medication and vital signs documentation, for example.
� Reuse disposable supplies when possible. Clinical Care Committee
� Institute daily meetings of the clinical care committee to examine new guidance, the situation at the hospital, and the regional situation and to determine appropriate levels of care to be offered based on staffing and other resources.
� The committee adapts State guidance to the hospital level and reviews any updates.
� The committee submits recommendations to the Planning Chief and then to the IC.
� On approval of the IC, any changes to the previous day’s triage, treatment, and diagnosis protocols are communicated to the ED, outpatient, and inpatient areas. These may include:
o Guidance on laboratory and x-ray testing (both influenza case testing and clinical lab/x-ray guidance).
o Guidance on outpatient/ED denial of service (e.g., deny care to those who will not be seen because their injury/illness is too minor).
o Updated information for all patients and family members presenting to the facility to be handed out by a triage nurse and reviewed with the patient’s nurse or physician.
o Inpatient care guidelines (staff responsibilities).
o Inpatient triage/resource situation.
o Anticipated events/trends in the next operational period. Patient Triage
� Set up a triage team (may consist of one critical care and one infectious disease physician, among others) to review conflicting resource needs (e.g., two patients needing a single ventilator) on a case-by-case basis.
51
� Use a decision tool supplied by the State and the clinical care committee to assign resources.
� Physicians are to provide patient care when not performing triage functions.
� Identify a bed czar to monitor the bed and “hard” resources, e.g., ventilators, make assignments based on availability, and implement triage team recommendations. The bed czar receives periodic input from clinical units about patient statuses (improving, deteriorating, etc.).Hospital Decompression
� Establish alternative care sites in conjunction with other area hospitals as well as in conjunction with Public Health and Emergency Medicine to enable hospital decompression.
� Notify EMS, public health, and others of need to decompress the hospital, as appropriate.
� Transfer patients to and from facilities as needed based on hospital resources; critical care to be concentrated in hospitals. A Regional Home Death Management Process
� Set up regional hubs for body retrieval and processing with a review by the Medical Examiner, a registration process, and a temporary holding place awaiting definite management. Communicate this plan to affected parties.
� Deploy refrigerated trucks from the hospital for body management, exchanged daily to regional processing sites.
� Arrange for Web-based death certificate processing and secure tracking to the Department of Health. Hospitals in Rural Areas
� Some issues are more likely to apply to hospitals located in rural areas.
� The triage physician (and/or nurse) implementing decisions at the hospital/ward level.
� Promoting a regional hospital and multiagency coordination system to share staff and resources as possible and help hospitals in the region share information. Coordinate the setup of a regional ACS when needed (under the host city’s jurisdictional umbrella).
� Patient referral to regional hospitals (when possible) or supportive care provided to the extent possible at the facility.
� Offsite care (may be a single regional facility). The ACS is the screening and care point for noncritical patients. The ACS may meet the need for additional screening and minor treatment in a rural area. In smaller communities, hospitals and clinics may not have the space and resources for screening that urban areas have, so bottlenecks may occur in outpatient assessment as well as inpatient care.
� Coordination of care with home care/families.
� Hospital coordination with the local public health agency to determine the scope of care in the community and facilitate home and palliative care.
52
� Transfers from the hospital morgue to a regional processing point or local undertakers with the medical examiner as needed.
ALTERNATIVE CARE SITES: PRE-PANDEMIC PERIOD
Resource
The HHS Influenza Plan for Alternative Care Sites (ACS) is available atwww.hhs.gov/pandemicflu/plan/sup3.html#altcare.
� Define ownership, command, and control of ACS.
� Perform site selection based on best estimates of need.
� Decide on the scope of care to be provided in the ACS.
� Establish functional requirements based on the level of care to be provided:
� Acquire supplies, equipment (including communications equipment), and pharmaceuticals.
� Plan staffing, taking into account absentee rates from potential staffing sources.
� Develop MOUs for operational support of the ACS, including housing for health care workers.
� Develop policies of operation for the ACS, including:
� Role of incident commander
� Criteria for admission, discharge, and transfer
� Infection control
� Pharmacy and medication control
� Safety and security
� Housekeeping
� Food service
� Linen services
� Finances and documentation
� Supplies
� Engineering (plant operations, electrical, plumbing, etc.)
� Communications
� Develop criteria for hospital decompression.
53
ALTERNATIVE CARE SITES EARLY PANDEMIC RESPONSE PERIOD
The following measures need to be undertaken to prepare for operation of the ACS:
� Perform resource assessment for standing up an ACS, including acquisition of additional necessary disposable supplies.
� Review and finalize policies of operation for the ACS.
� Exercise the ACS if possible. As early as possible, explore the legal issues around standing up an ACS for full functional exercise with patients.
� Test communications.
� Identify and roster the ACS staff.
� Establish a process of immunization and prophylaxis of potential staff members.
� Establish incident command structure for ACS. Planners should ensure that ACS is integrated with community, regional and State incident command systems.
� Unpack and inventory supplies at the selected site(s).
� Enable the security protection systems of the ACS.
� Develop a patient transport plan for movement of ACS patients to and from area hospitals.
ALTERNATIVE CARE SITES: WIDESPREAD PANDEMIC RESPONSE PERIOD � Ensure all ACSs are fully operational.
� Investigate the need for the establishment of other functional sites for supplying ambulatory care, inpatient care, quarantine, and/or palliative care.
� Establish criteria for closing the ACSs as the pandemic eventually passes.
PALLIATIVE CARE: PRE-PANDEMIC PERIOD � Hold planning discussions of treatment options limitations due to scarce resources. Decisions must be made that typically would not be considered under usual circumstances. Standards of care and treatment options will be appropriate to the situation at the time the decision is made. Community planners need to be aware that it may not always be possible to save a life during a pandemic. It is important to have these difficult discussions prior to the occurrence of a pandemic.
� Establish and maintain standards of palliative care. Ensure that the standards are published and available for consideration during planning efforts.
� Provide education and training for palliative care responders for understanding, recognizing and establishing response actions in a pandemic flu situation.
� Include instruction about self-protection and avoidance of the spread of disease.
54

PALLIATIVE CARE: EARLY PANDEMIC RESPONSE PERIOD � Discuss goals of care. Complications from the flu may result in the individual becoming too sick to survive. It may be necessary to discuss goals of care and preferences with the patient.
� Provide information on treatment options. Patients and families need to have updated information so they may understand their condition and treatment options.
� Decisionmaking about the patient’s care plan must be sensitive both to changes in the patient’s condition and to the availability of community resources.
� Address pain and symptom control, psychosocial distress, spiritual issues, and practical needs with patients and their families throughout the continuum of care.
PALLIATIVE CARE: WIDESPREAD PANDEMIC RESPONSE PERIOD � Establish patient triage criteria by levels of care.
� Classify patients who are already chronically ill, extremely old, or in long-term care facilities (e.g., by physician prognosis).
� Plan for use of long-term care facilities. Nursing homes can provide a preventive care response to an influenza pandemic (e.g., immunizations, drug management), thus providing relief to hospitals.
HOME CARE: EARLY PANDEMIC RESPONSE PERIOD� Address the myriad challenges of providing health care services in the home for people with substantial disability and/or illness or without family or other resources to provide care. Consider the following issues:
� Develop alternative ways to provide care to people in the community such as primary care vans that go into neighborhoods to provide care, answer questions, and provide resources.
� Establish telephone hotlines to answer questions regarding the flu, such as “Ask-A-Nurse”-type support services. Also make use of existing hotlines.
� Consider ways to provide incentives for people to work during times of crises. Health care workers may not want to leave their families to care for flu patients. Incentives should be considered (e.g., giving them priority status for vaccines).
55

BibliographyThe bibliography from the original Mass Medical Care With Scarce Resources has been updated for this guide to reflect resources newly available since its original publication.
1. Community-Wide Planning Agency for Healthcare Research and Quality. Altered Standards of Care in Mass Casualty Events: Bioterrorism and Other Public Health Emergencies. AHRQ Publication No. 05-0043. Rockville, MD:
Agency for Healthcare Research and Quality; April 2005, 16-18. Available at: http://www.ahrq.gov/research/altstand/index.html.Accessed November 27, 2006.
2. Ethical Considerations
Centers for Disease Control and Prevention. Ethical Guidelines in Pandemic Influenza. Available at: http://www.cdc.gov/od/science/phethics/guidelinesPanFlu.htm. Accessed July 21, 2009.
Devereaux A, Christian MD, Dichter JR, Geiling JA, and Rubinson L. Summary of suggestions from the Task Force for Mass Critical Care Summit, January 26-27, 2007. Chest 2008; 133;1-7.
Kass NE, An ethics framework for public health and avian influenza pandemic preparedness. Yale Journal of Biology and Medicine 2005: 78; 235-250.
Powell T, Christ KC, Birkhead GS. Allocation of ventilators in a public health disaster. Disater Med Pub Health Preparedness. 2008; 2:20-26.
Steinhauser KE, Clipp EC, McNeilly M, Christakis N, McIntyre LM, and Tulsky JA. In search of a good death: Observations of patients, families and providers. Annals of Internal Medicine.2000;132:825-831
Tabery J, Mackett CW, and the University of Pittsburgh Medical Center Pandemic Influenza Task Force’s Triage Review Board. Ethics of triage in the event of an influenza pandemic. Disater Med Public Health Preparedness. 2008; 2:114-118.
Veatch RM Disaster Preparedness and Triage: Justice and the common good. The Mount Sinai Journal of Medicine. 2005;72:236-241.
White DB, Katz MH, Luce JM, and Lo B. Who should receive life support during a public health emergency? Using ethical principles to improve allocation decisions. Ann Intern Med 2008, 150:132-138.3. Assessing the Legal Environment 50 U.S.C. §§ 1601(b) (2006).
3. Assessing the Legal Environment
Agency for Healthcare Research and Quality. Altered Standards of Care in Mass Casualty Events: Bioterrorism and Other Public Health Emergencies. AHRQ Publication No. 05-0043. Rockville, MD: Agency for Healthcare Research and Quality; April 2005, 16-18. Available at: http://www.ahrq.gov/research/altstand/index.html.Accessed November 27, 2006.
The Americans with Disabilities Act of 1990. Pub. L. No. 101-336.
Center for Law and the Public’s Health. Model State Emergency Health Powers Act. (2001). Available at: http://www.publichealthlaw.net/MSEHPA/MSEHPA2.pdf. Accessed April 15, 2006.
Center for Law and the Public’s Health, Health Resources and Services Agency. Emergency System for Advance Registration of Volunteer Health Professionals (ESAR-VHP) – Legal and Regulatory Issues. 2006:23.
Center for Law and the Public’s Health. MSEHPA Legislative Surveillance Table, July 15, 2006. Available at: http://www.publichealthlaw.net/MSEHPA/MSEHPA%20Surveillance.pdf. Accessed November 27, 2006.
Center for Law and the Public’s Health. Public health emergency legal preparedness checklist on interjurisdictional legal coordination. 2004. Available at:http://www.publichealthlaw.net/Resources/BTlaw.htm. Accessed November 27, 2006.
57
Center for Law and the Public’s Health. Checklist on local government public health emergency legal preparedness and response. Available at: http://www.publichealthlaw.net/Resources/BTlaw.htm. Accessed November 27, 2006.
Centers for Disease Control and Prevention. Public Health Law Program. Available at http://www2a.cdc.gov/phlp/. Accessed July 20, 2009.
Centers for Disease Control and Prevention. Public Health Law Program. Legislation for Public Health Emergencies. Available at http://www2a.cdc.gov/phlp/legislation.asp.
Emergency Management Assistance Compact (EMAC), Pub. L. No. 104-321.
Fox P. Cross-border assistance in emergencies: the New England/eastern Canadian model. New England Journal of International Contemporary Law. 2004;11:75.
Federal Volunteer Protection Act of 1997. Pub. L. No. 105-19, § 4, 111 Stat. 218, 219 (1997), 42 U.S.C. § 14503 (2000); Ala. Code. § 6-5-336(d)(1) (LexisNexis 2005); Miss. Code Ann. § 95-9-1(3) (LexisNexis 1972).
Gostin LO. Public Health Law: Power, Duty, Restraint. Berkeley: University of California Press; 2002:263-265.
Gostin, LO, Hodge JG Jr. The Model State Emergency Health Powers Act – A Brief Commentary. Seattle: Turning Point Statute Modernization Collaborative, 2002; 1-42. Available at:http://www.publichealthlaw.net/Resources/Modellaws.htm#MSEHPA. Accessed November 27, 2006.
Gostin LO, Sapsin JW, Teret SP, Burris S, Mair JS, Hodge JG Jr., Vernick JS. The Model State Emergency Health Powers Act: planning for and response to bioterrorism and naturally occurring infectious diseases. JAMA. 2002;288:622.
Hodge JG Jr. Bioterrorism law and policy: critical choices in public health. Journal of Law, Medicine, & Ethics. 2002;30:254-255.
Hodge JG Jr. Delaware Public Health Emergency Law - Review, Recommendations, and a Blueprint for Reform. Dover, DE: Delaware Department of Health and Social Services; 2004;1-62.
Hodge JG Jr. The intersection of Federal health information privacy and State administrative law: the protection of individual health data and worker’s compensation. Administrative Law Review.1999;51:117-144.
Hodge JG Jr. Legal issues concerning volunteer health professionals and the hurricane-related emergencies in the Gulf Coast region. Public Health Report. 2006;121:205-207.
Hodge JG Jr. Legal triage during public health emergencies and disasters. Administrative Law Review. In press.
Hodge JG Jr, Calves S, Gable LA, Meltzer E, Kraner S. Risk management in the wake of hurricanes and other disasters: Hospital civil liability arising from the use of volunteer health professionals during emergencies. Michigan State University Journal of Medicine and Law. In press.
Hodge JG Jr, Gable LA, Calves S. The legal framework for meeting surge capacity through the use of volunteer health professionals during public health emergencies and other disasters. Journal of Contemporary Health Law and Policy. 2006;22:5-71.
Hodge JG Jr, O’Connell J. The legal environment underlying influenza vaccine allocation and distribution strategies. Journal of Public Health Management and Practice. 2006;12(4):340-348.
Intergovernmental Mutual Aid Agreement for the establishment of the Illinois Public Health Mutual Aid System. Available at: http://www.idph.state.il.us/local/mutualaidagree_9.30.04.pdf . Accessed November 27, 2006.
M.C.L. §§ 418.161(g), 30.411 Sec. 11(1)(b)-(c).
Md. Code Ann., Public Safety §§ 14-3A-03(c), 14-3A-08 (Supp. 2004).
Massachusetts General Laws Annals. ch. 112, § 12B, ch. 111C, § 20 (West 2003).
Mid-America Alliance: Mutual Assistance for Public Health Preparedness (2005). Available at: http://app1.unmc.edu/midameria. Accessed November 27, 2006.
The New York “Human Rights Law,” New York Executive Law Art. 15 §290 et seq.
58
Public Health Service Act, 42 U.S.C. § 201 et seq. (2006).
Public Health Security and Bioterrorism Preparedness and Response Act of 2002, 42 U.S.C. § 247d. 2003.
The Robert T. Stafford Disaster Relief and Emergency Assistance Act, 42 U.S.C. §§ 5121-5206 (2002).
The Uniform Emergency Healthcare Services Act § 7(c). In press.
University of Maryland Center for Health and Homeland Security. Maryland Public Health Emergency Preparedness Legal Handbook. 2005:31.
The White House. The Federal Response to Hurricane Katrina: Lessons Learned. 2006:58. Available at: http://www.whitehouse.gov/reports/katrina-lessons-learned/ 2006:58. Accessed November 27, 2006.
4. Prehospital Care
Avitzour M, Libergal M, Assaf J, et al. A multicasualty event: out-of-hospital and in-hospital organizational aspects. Academic Emergency Medicine. 2004;11:1102–1104.
Bostick NA, Subbarao I, Burkle FM Jr, Hsu EB, Armstrong JH, James JJ. Disaster triage systems for large-scale catastrophic events. Disaster Med Public Health Prep. 2008 Sep;2 Suppl 1:S35-9.
Briggs SM, Brinsfield KH. Advanced Disaster Medical Response Manual for Providers.Cambridge, MA: Harvard Medical International Trauma & Disaster; 2003.
Christen HT, Maniscalco PM. The EMS Incident Management System – EMS Operations for Mass Casualty and High Impact Incidents. Upper Saddle River, NJ: Brady – Prentice Hall; 1998. Christen HT, Maniscalco PM. Mass Casualty and High Impact Incidents: An Operations Guide. Upper Saddle River, NJ: Brady – Prentice Hall; 2002.
de Boer J. An attempt at more accurate estimation of the number of ambulances needed at disasters in the The Netherlands. Prehospital and Disaster Medicine. 1996;11:125–128.
de Boer J, Debacker M. A more rational approach to medical disaster management applied retrospectively to the Enschede fireworks disaster, 13 May 2000. European Journal of Emergency Medicine.2003;10:117–123.
Dow AA, Clark WE, Farmer JC, et al. Disaster management. Organizations and academic perspective. Critical Care Clinics. 1991;7:257–270.
Doyle CJ. Mass casualty incident. Integration with prehospital care. Emergency Medical Clinics of North America. 1990;8:163–175.
Farmer CJ, Jimenez EJ, Talmor D, Zimmerman JL. Fundamentals of Disaster Management. Des Plains, IL: Society of Critical Medicine; 2003.
Farmer JC, Carlton PK, Jr. Providing critical care during a disaster: the interface between disaster response agencies and hospitals. Critical Care Medicine. 2006;34(3 Suppl):S56–S59.
Fenn J, Rega P, Stavros M, Buderer NF. Assessment of U.S. helicopter emergency medical services’ planning and readiness for disaster response. Air Medical Journal. 1999;18:12–15.
Fitzgerald DJ, Sztajnkrycer MD, Crocco TJ. Chemical weapon functional exercise – Cincinnati: observations and lessons learned from a “typical medium-sized” city’s response to simulated terrorism utilizing weapons of mass destruction. Public Health Report. 2003;118:205–214.
Flowers LK, Mothershead JL, Blackwell TH. Bioterrorism preparedness II: The community and emergency medical services systems. Emergency Medical Clinics of North America. 2002;20:457–476.
Graham CA, Hearns ST. Major incidents: training for on site medical personnel. Journal of Accident & Emergency Medicine. 1999;16:336–338.
Grissom TE, Farmer JC. The provision of sophisticated critical care beyond the hospital: lessons from physiology and military experiences that apply to civil disaster medical response. Critical Care Medicine. 2005;33(1 Suppl):S13–S21.
Jacobs LM, Gabram SG, Stohler SA. The integration of a helicopter emergency medical service in a mass casualty response system. Prehospital and Disaster Medicine. 1991;6:451–454.
59

Lerner EB, Schwartz RB, Coule PL, Weinstein ES, Cone DC, Hunt RC, Sasser SM, Liu JM, Nudell NG, Wedmore IS, Hammond J, Bulger EM, Salomone JP, Sanddal TL, Markenson D, O'Connor RE. Masscasualty triage: an evaluation of the data and development of a proposed national guideline.Disaster Med Public Health Prep. 2008 Sep;2 Suppl 1:S25-34.
Maningas PA, Robison M, Mallonee S. The EMS response to the Oklahoma City bombing. Prehospital and Disaster Medicine. 1997;12:80–85. Maniscalco PM, Christen HT. Public Health Guide for Emergencies, First Edition. Baltimore: The Johns Hopkins University School of Hygiene and Public Health and The International Federation of Red Cross and Red Crescent Societies; 2000.
Maniscalco PM, Christen HT. Understanding Terrorism and Managing its Consequences. Upper Saddle River, NJ: Brady – Prentice Hall; 2001.
Martchenke J, Rusteen J, Pointer JE. Prehospital Communications during the Loma Prieta earthquake. Prehospital and Disaster Medicine. 1995;10:225–231.
Martchenke J, Lynch T, Pointer J, Rooker N. Aeromedical helicopter use following the 1989 Loma Prieta earthquake. Aviation, Space, and Environmental Medicine. 1995;66:359–363.
Palafox J, Pointer JE, Martchenke J, Kleinrock M, Michaelis J. The 1989 Loma Prieta earthquake: issues in medical control. Prehospital and Disaster Medicine. 1993;8:291–297.
Peleg K, Michaelson M, Shapira SC, Aharonson-Daniel L. Principles of emergency management in disasters. Advances in Renal Replacement Therapy.2003;10:117–121.
Prezant DJ, Clair J, Belyaev S, et al. Effects of the August 2003 blackout on the New York City healthcare delivery system: a lesson for disaster preparedness. Critical Care Medicine. 2005;33(1 Suppl):S96–S101.
Risavi BL, Salen PN, Heller MB, Arcona S. A two-hour intervention using START improves prehospital triage of mass casualty incidents. Prehospital Emergency Care. 2001;5:197–199. SALT mass casualty triage: concept endorsed by the American College of Emergency Physicians, American College of Surgeons Committee on Trauma, American Trauma Society, National Association of EMS Physicians, National Disaster Life Support Education Consortium, and State and
Territorial Injury Prevention Directors Association.[No authors listed] Disaster Med Public Health Prep. 2008 Dec;2(4):245-6.
Sasser S. Field triage in disasters. Prehosp Emerg Care. 2006 Jul-Sep;10(3):322-3.
Shirm S, Liggin R, Dick R, Graham J. Prehospital preparedness for pediatric mass-casualty events.Pediatrics. 2007 Oct;120(4):e756-61. Stohler SA, Jacobs LM, Gabram SG. Roles of a helicopter emergency medical service in mass casualty incidents. Journal of Air Medical Transport.1991;10:7–13.
Thomas SH, Harrison T, Wedel SK, Thomas DP. Helicopter emergency medical services roles in disaster operations. Prehospital Emergency Care.2000;4:338–344.
U.S. Agency for International Development for Humanitarian Response (USAID), Office of Foreign Disaster Assistance. Field Operations Guide for Disaster Assessment and Response, v. 3.0. Washington: USAID; 1998.
Walsh DW, Christen HT, Miller GT, Callsen CE, Cilluffo FJ, Maniscalco PM. National Incident Management System: Principles and Practice.Sudbury, MA: Jones & Bartlett Publishers; 2005.
Withers MR, Christopher GW. Aeromedical evacuation of biological warfare casualties: a treatise on infectious diseases on aircraft. Military Medicine.2000;165(11 Suppl):1–21.
Zoraster RM, Chidester C, Koenig W. Field triage and patient maldistribution in a mass-casualty incident. Prehosp Disaster Med. 2007 May-Jun;22(3):224-9.
5. Hospital/Acute Care
Minnesota Healthcare System Preparedness Program Standards of Care for Scarce Resources http://www.health.state.mn.us/oep/healthcare/standards.pdf 2008.
Agency for Healthcare Research and Quality (AHRQ). Altered Standards of Care in Mass Casualty Events: Bioterrorism and Other Public Health Emergencies. AHRQ Publication No. 05-0043. Rockville, MD: AHRQ; April 2005. Available at: http://www.ahrq.gov/research/altstand/.
60
Agency for Healthcare Research and Quality (AHRQ). Health Emergency Assistance Line and Triage Hub (HEALTH) Model. Rockville, MD: AHRQ; March 2005. Available at: http://www.ahrq.gov/research/health/.
Agency for Healthcare Research and Quality (AHRQ). Rocky Mountain Regional Care Model for Bioterrorist Events: Locate Alternate Care Sites During an Emergency. Rockville, MD: AHRQ; December 2004. Available at: http://www.ahrq.gov/research/altsites.htm.
Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH. Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. JAMA.2002;288(16):1987–1993.
Alexander GC, Werner RM, Ubel PA. The costs of denying scarcity. Archives of Internal Medicine.March 22, 2004;164(6):593–596.
Alexander GC, Wynia MK. Ready and willing? Physicians’ sense of preparedness for bioterrorism. Health Affairs. September–October 2003;22(5):189–197.
American College of Emergency Physicians. Code of ethics for emergency physicians. Annals of Emergency Medicine. 1997;30:365–372.
American College of Emergency Physicians (ACEP). The duty to respond to out-of-hospital emergencies and disasters. ACEP 2006 Policy Compendium.Dallas: ACEP; 2006;35(3)(d).
American Hospital Association. Hospital Preparedness for Mass Casualties. August 2000. Available at: http://aharc.library.net/.
American Medical Association Council on Ethical and Judicial Affairs. Ethical considerations in the allocation of organs and other scarce medical resources among patients. Archives of Internal Medicine. 1995;155:29–40.
Barbera J, Macintyre A. Medical and Health Incident Management System: A Comprehensive Functional System Description for Mass Casualty Medical and Health Incident Management. Washington. DC: George Washington University Institute for Crisis, Disaster, and Risk Management; December 2002. Available at: www.gwu.edu/~icdrm.
Barbera J, McIntyre A. Medical Surge Capacity and Capability: A Management System for Integrating Medical and Health Resources During Large-Scale Emergencies. Alexandria, VA: CNA Corporation; August 2004. Available at: http://www.cna.org/documents/mscc_aug2004.pdf.
Barbisch DF. Surge Capacity: Seamless Emergency Medical Logistics Expansion System. Presented at the National Disaster Medical System Conference, Dallas; 2004. Available at: http://ndms.chepinc.org/data/files/3/142.pdf.
Benson M et al. Disaster triage: START, the SAVE. Prehospital and Disaster Medicine. 1996;11:117–124.
Bostick NA, Subbarao I, Burkle FM Jr, Hsu EB, Armstrong JH, James, JJ. Disaster triage systems for large-scale catastrophic events. Disaster Med Public Health Preparedness. 2008;2:S35-39S.
Burkle FM Jr, Hsu EB, Loehr M, Christian MD, Markenson D, Rubinson L, Archer FL. Definition and functions of health unified command and emergency operations centers for large-scale bioevent disasters within the existing ICS. Disaster Med Public Health Preparedness.2007;1:135-141.
Center for Law and the Public’s Health – Georgetown and Johns Hopkins Universities. Turning Point State Legislative Update Table.Available at: http://www.publichealthlaw.net/Resources/Modellaws.htm#TP.
Centers for Disease Control and Prevention. Tiered use of inactivated influenza vaccine in the event of a vaccine shortage. MMWR Weekly. 2005;54:749–750.
Cheung TMT et al. Effectiveness of non-invasive positive pressure ventilation in the treatment of acute respiratory failure in severe acute respiratory syndrome. Chest. 2004;126:845–850.
Christian MD, Devereaux AV, Dichter JR, Geiling JA, Rubinson L. Definitive care for the critically ill during a disaster: current capabilities and limitations.Chest. 2008;133:8S-17S.
Church J. Modular Emergency Medical System – Expanding Local Healthcare Structure in a Mass Casualty Terrorism Event. Washington: Department of Defense; June 1, 2002. Available at: http://www.nnemmrs.org/documents/.
61
Clarke SP, Sloane DM, Aiken LH. Effects of hospital staffing and organizational climate on needlestick injuries to nurses. American Journal of Public Health. 2002;92(7):1115–1119.
CNN.com. Sniper Fire Halts Hospital Evacuation: Gunmen fire at medical workers and patients at Charity Hospital. September 1, 2005. Available at: http://www.cnn.com/2005/WEATHER/09/01/katrina.hospital.sniper/index.html.
Cone DC, Koenig KL. Mass casualty triage in the chemical, biological, radiological, or nuclear environment. European Journal of Emergency Medicine. December 2005;12(6):287–302.
Cone DC, MacMillan DS. Mass-casualty triage systems: a hint of science. Academic Emergency Medicine. 2005;12(8):739–741.
Cook R, Cook D, Tilley J, Lee K, Marshall J; Canadian Critical Care Trials Group. Multiple organ dysfunction: baseline and serial component scores. Critical Care Medicine. 2001;29(11):2046–2050.
Dacey MJ. Tragedy and response – the Rhode Island Nightclub Disaster. New England Journal of Medicine. 2003;349:1990–1991.
Daniels N. Accountability for reasonableness. British Medical Journal. 2000;321:1300–1301.
Daniels N. Am I My Patient’s Keeper? An Essay on Justice Between the Young and Old. New York: Oxford University Press, 1988.
Daniels N, Sabin J. Setting Limits Fairly: Can We Learn to Share Scarce Medical Resources?. New York: Oxford University Press; 2002.
Derse AR. Law and ethics in emergency medicine. Emergency Medicine Clinics of North America.1999;17(2):307–325.
Diaz GG et al. Non-invasive positive pressure ventilation to treat hypercapneic coma secondary to respiratory failure. Chest. 2005;127;952–960.
Emanuel EJ, Wertheimer A. Public health. Who should get influenza vaccine when not all can? Science. May 12, 2006;312:854–855.
Eschun GM, Jacobsohn E, Roberts D, Sneiderman B. Ethical and practical considerations of withdrawal of treatment in the intensive care unit. Canadian Journal of Anaesthesia. 1999;46(5):497–504.
Federal Emergency Management Agency. National Incident Management System. Available at: http://www.fema.gov/emergency/nims/index.shtm.
Gomersall CD, Tai DY, Loo S, Derrick JL, Goh MS,Buckley TA, Chua C, Ho KM, Raghavan GP, HoOM, Lee LB, Joynt GM. Expanding ICU facilities in an epidemic: recommendations based on experience from the SARS epidemic in Hong Kong and Singapore. Intensive Care Medicine. March 29, 2006;30:381–387.
Goold SD. Allocating health care: cost-utility analysis, informed democratic decision-making, or the veil of ignorance? Journal of Health Politics, Policy, and Law. 1996;21:68–97.
Gostin LO, Saprin JW, Teret SP, et al. The model State emergency health powers act. JAMA.2002;288:622–628.
Greater New York Hospital Association. Hospital Resources for Preparedness and Response. Available at: http://www.gnyha.org/eprc/general/ics/.
Greater New York Hospital Association. Security Planning Information for Hospitals. Available at: http://www.gnyha.org/eprc/general/security/.
Grow R, Rubinson L. The challenges of hospital infection control in response to bioterrorist attacks. Biosecurity and Bioterrorism. 2003;1:215–220.
Health Resources and Services Administration. Bioterrorism Hospital Preparedness Program 2006 Grant Guidance. Available at: http://www.hrsa.gov/bioterrorism/default.htm.
Herridge MS. Prognostication and intensive care unit outcome: the evolving role of scoring systems. Clinics in Chest Medicine. 2003;24(4):751–762.
Hick JL, Barbera JA, Kelen GB. Refining surge capacity: conventional, contingency, and crisis capacity. Disaster Med Public Health Preparedness.2009;3(Suppl 1):S59–S67.
62
Hick JL, Hanfling D, Burstein JL, DeAtely C, Barbisch D, Bogdan G, Cantrill S. Healthcare facility and community strategies for patient care surge capacity. Annals of Emergency Medicine.2004;44:253–261.
Hick JL, O’Laughlin DT. Concept of operations for triage of mechanical ventilation in an epidemic. Academic Emergency Medicine. 2006:13(2):223–229. Available at: http://www.aemj.org/cgi/content/full/13/2/223.
Iserson KV. Principles of biomedical ethics. Emergency Medicine Clinics of North America.1999;17(2):283–306.
Iserson KV, Pesik N. Ethical resource distribution after biological, chemical, or radiological terrorism. Cambridge Quarterly of Healthcare Ethics.2003;12:455–465.
Joint Commission on Accreditation of Healthcare Organizations (JCAHO). Disaster privileging standard. Comprehensive Accreditation Manual for Hospitals. Medical Staff Section MS.5.14.4.1. Oakbrook Terrace, IL: JCAHO; January 1, 2003.
Joint Commission on Accreditation of Healthcare Organizations (JCAHO). Healthcare at the Crossroads: Strategies for Creating and Sustaining Community-Wide Emergency Preparedness Systems.Oak Terrace, IL: JCAHO; 2004.
Joint Commission on Accreditation of Healthcare Organizations (JCAHO). Surge Hospitals: Providing Safe Care in Emergencies. Chicago: JACHO; 2006. Available at: http://www.jcrinc.com/generic.asp?durki=11627&site=11&return=http://www.ahrq.gov/research/altstand/405.
Joint Commission on Accreditation of Healthcare Organizations (JCAHO). The 2001 Joint Commission Comprehensive Accreditation Manual for Hospitals.EC 1.4 and 1.6 (rev). Oakbrook Terrace, IL: JCAHO; 2001.
Karnofsky DA. The use of nitrogen mustards in the palliative treatment of carcinoma. Cancer.1948;1:634.
Katz S. Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychosocial function. JAMA. 1963;185:914.
Kelen, G. Reverse triage: criteria for immediate inpatient disposition for creation of hospital surge capacity (abstract – 14th World Congress on Disaster and Emergency Medicine). Prehospital and Disaster Medicine. 2006;20(S1):S9–S10. Available at: http://pdm.medicine.wisc.edu/20-2%20PDFs/aedinburgh.pdf.
Koenig KL, Cone DC, Burstein JL, Camargo CA, Jr. Surging to the right standard of care. Academic Emergency Medicine. 2006;13(2):195–198.
Koenig KL, Dinerman N, Kuehl AE. Disaster nomenclature – a functional approach: the PICE system. Academy of Emergency Medicine.1996;3(7):723–727.
Koenig KL, Goans RE, Hatchett RJ, Mettler FA, Jr., Schumacher TA, Noji EK, Jarrett DG. Medical treatment of radiological casualties: current concepts. Annals of Emergency Medicine. 2005;45(6):643–652.
Lanzilotti SS, Galanis D, Leoni N, Craig B. Hawaii medical professionals assessment. Hawaii Medical Journal. August 2002;61(8):162–173.
Larkin GL, Arnold J. Ethical considerations in emergency planning, preparedness, and response to acts of terrorism. Prehospital & Disaster Medicine.July–September 2003;18(3):170–178.
Larson EB. Scribner’s legacy serves public good. Seattle Post-Intelligencer. July 9, 2003. Available at: http://seattlepi.nwsource.com/opinion/129982_scribner09.html.
Lemeshow S et al. Modeling the severity of illness in ICU patients: a systems update. JAMA.1994;272:1049–1055.
Lemeshow S et al. Mortality probability models based on an international cohort of intensive care unit patients. JAMA. 1993;270:2478–2486.
Lemeshow S et al. Mortality probability models for patients in the intensive care unit for 48 or 72 hours: a prospective, multicenter study. Critical Care Medicine. 1994;22:1351–1358.
MacVittie TJ. Therapy of radiation injury. Stem Cells. 1997;15(Suppl 2):263–268.
Marshall JC, Cook DJ, Christou NV, et al. Multiple organ dysfunction score: a reliable descriptor of a complex clinical outcome. Critical Care Medicine.1995;23:1638–1652.
63

McKneally MF, Dickens BM, Meslin EM, Singer PA. Bioethics for clinicians: 13. Resource allocation. Canadian Medical Association Journal.1997;157(2):163–167.
Minnesota Department of Health (MDH). State/regional/local patient care responsibilities defined and outlined. Patient Care Coordination Planning Guide. Available on CD by request to the MDH Office of Emergency Preparedness: [email protected].
Monchi M, Bellenfant F, Cariou A, Joly LM, Thebert D, Laurent I, Dhainaut JF, Brunet F. Early predictive factors of survival in the acute respiratory distress syndrome. A multivariate analysis. American Journal of Respiratory & Critical Care Medicine. October 1998;158(4):1076–1081.
Moreno R, Vincent JL, Matos R, Mendonca A, et al. The use of maximum SOFA score to quantify organ dysfunction/failure in intensive care. Results of a prospective, multicentre study. Intensive Care Medicine. 1999;25(7);686–696.
Moskop JC, Iserson KV. Triage in medicine, part II: underlying values and principles. Ann Intern Med.2007;49(3):282-287.
Needleman J, Buerhaus P, Mattke S, Stewart M, Zelevinsky K. Nurse-staffing levels and the quality of care in hospitals. New England Journal of Medicine.2002;346(22):1715–1722.
Nickell LA, Crighton EJ, Tracy CS, Al-Enazy H, Bolaji Y, Hanjrah S, Hussain A, Makhlouf S, Upshur RE. Psychosocial effects of SARS on hospital staff: survey of a large tertiary care institution. Canadian Medical Association Journal. March 2, 2004;170(5):793–798.
O’Laughlin D, Hick JL. Ethical issues in resource triage. Respiratory Care. 2008;53(2):190 –197.
Peres Bota D, Melot C, Lopes Ferreira F, Nguyen Ba, Vincent JL. The multiple organ dysfunction score (MODS) versus the sequential organ failure assessment (SOFA) score in outcome prediction. Intensive Care Medicine. 2002;28(11):1619–1624.
Pesik N, Keim ME, Iserson KV. Terrorism and the ethics of emergency medical care. Annals of Emergency Medicine. 2001;37(6):642–646.
Peters MJ, Tasker RC, Kiff KM, Yates R, Hatch DJ. Acute hypoxemic respiratory failure in children: case mix and the utility of respiratory severity indices. Intensive Care Medicine. 1998;24(7):699–705.
Pettila V, Pettila M, Sarna S, Voutilainen P, Takkunen O. Comparison of multiple organ dysfunction scores in the prediction of hospital mortality in the critically ill. Critical Care Medicine.August 2002;30(8):1705–1711.
Posner Z. Admi H. Menashe N. Ten-fold expansion of a burn unit in mass casualty: how to recruit the nursing staff. Disaster Management & Response. October–December 2003;1(4):100–104.
Powell T, Christ KC, Guthrie S. Birkhead. Allocation of ventilators in a public health disaster. Disaster Med Public Health Preparedness.2008;2:20-26
Public Engagement Pilot Project on Pandemic Influenza. Citizen Voices on Pandemic Flu Choices.Washington: National Academy Press; 2005.
Qureshi K, Gershon RR, Sherman MF, Straub T, Gebbie E, McCollum M, Erwin MJ, Morse SS. Health care workers' ability and willingness to report to duty during catastrophic disasters. Journal of Urban Health. September 2005;82(3):378–388.
Rizzo A, Colonel, USAF, MC, SFS Chief, Operations Division NORAD-USNORTHCOM/SG. Deployable Oxygen Solutions for FEMA. Briefing. Available at: http://www.denverhealth.org/bioterror/Document/DH2SupplyStaffing10-30-03.pdf (Appendix A).
Roccaforte JD. The World Trade Center attack. Observations from New York's Bellevue Hospital. Critical Care. 2001;5(6):307–309.
Rubinson L, Branson R, Pesik N, Talmor D. Positive pressure ventilation equipment for mass casualty respiratory failure. Biosecurity and Bioterrorism.2006;4:1–12.
Rubinson L, Hick JL, Curtis JR, Branson RD, Burns S, Christian MD. Devereaux AV, Dichter JR, Talmor D, Erstad B, Medina J, Geiling JA. Task Force for Mass Critical Care. Definitive care for the critically ill during a disaster: medical resources for surge capacity: from a Task Force for Mass Critical Care summit meeting, January 26-27, 2007, Chicago, IL. Chest. 2008;133(5 Suppl):32S-50S.
64
Rubinson L, Nuzzo JB, Talmor DS, O’Toole T, Kramer BR, Inglesby TV. Augmentation of hospital critical care capacity after bioterrorist attacks or epidemics: recommendations of the Working Group on Emergency Mass Critical Care. Critical CareMedicine. October 2005;33(10):2393–2403.
Sacco WJ, Navin DM, Fiedler KE, Waddell RK II, Long WB, Buckman RF, Jr. Precise formulation and evidence-based application of resource-constrained triage. Academic Emergency Medicine.2005;12(8):759–770.
Saffle JR, Gibran N, Jordan M. Defining the ratio of outcomes to resources for triage of burn patients in mass casualties. Journal of Burn Care & Rehabilitation. November–December 2005;26(6):478–482.
San Mateo County Emergency Medical Services Agency. Hospital Emergency Incident Command System III – January, 1998. Available at: www.emsa.cahwnet.gov/dms2/heics3.htm.
Sever MS, Vanholder R, Lameire N. Management of crush-related injuries after disasters. New England Journal of Medicine. March 9, 2006;354(10):1052–1063.
Skidmore S, Wall W, Church J. Modular Emergency Medical System Concept of Operation for the Acute Care Center: Mass Casualty Strategy for a Biological Terror Incident. U.S. Department of the Army, Soldier and Biological Chemical Command. May 2003. Available at: http://www.nnemmrs.org/documents/.
Society of Critical Care Medicine Ethics Committee. Attitudes of critical care medicine professionals concerning distribution of intensive care resources. Critical Care Medicine. 1994;22:358–362.
Society of Critical Care Medicine Ethics Committee. Consensus statement on the triage of critically ill patients. JAMA. 1994;271:1200–1203.
State of Minnesota, Office of the Revisor of Statutes. Minnesota Statutes 2006, Chapter 12, 12.03 (Definitions). St. Paul: State of Minnesota; 2006. Available at: http://ros.leg.mn/bin/getpub.php?pubtype=STAT_CHAP_SEC&year=current§ion=12.03
Tanabe P, Gimbel R, Yarnold PR, Kyriacou DN, Adams JG. Reliability and validity of scores on The
Emergency Severity Index version 3. Academic Emergency Medicine. January 2004;11(1):59–65.
Tanabe P, Travers D, Gilboy N, Rosenau A, Sierzega G, Rupp V, Martinovich Z, Adams JG. Refining Emergency Severity Index triage criteria. Academic Emergency Medicine. 2005;12(6):497–501.
Tauber AI. A philosophical approach to rationing. Medical Journal of Australia. 2003:178(9):454–456.
Trachsel D, McCrindle BW, Nakagawa S, Bohn D. Oxygenation index predicts outcome in children with acute hypoxemic respiratory failure. American Journal of Respiratory & Critical Care Medicine.July 15, 2005;172(2):206–211.
Turai I, Veress K, Gunalp B, Souchkevitch G. Medical response to radiation incidents and radionuclear threats. British Medical Journal. March 6, 2004;328:568–572.
University of Toronto Joint Centre for Bioethics, Pandemic Influenza Working Group. Stand on Guard for Thee: Ethical Considerations in Preparedness.November 2005.
U.S. Department of Health and Human Services (HHS). Food and Drug Administration Draft Guidance: Emergency Use Authorization of Medical Products. Washington: HHS; June 2005. Available at:http://www.fda.gov/oc/bioterrorism/emergency_use.html.
U.S. Department of Health and Human Services. HHS Pandemic Influenza Plan. S3-III (A)(2)(h). Available at: http://www.hhs.gov/pandemicflu/plan/.
U.S. Department of Health and Human Services. Hurricane Katrina: Waiver Under Section 1135 of the Social Security Act. September 4, 2005. Available at: http://www.hhs.gov/katrina/ssawaiver.html.
U.S. Department of Health and Human Services. National Disaster Medical System. Available at: http://ndms.dhhs.gov/.
U.S. Department of Health and Human Services. Pandemic Influenza Plan, Appendix D: NVAC/ACIP Recommendations for Prioritization of Pandemic Influenza Vaccine and NVAC Recommendations on Pandemic Antiviral Drug Use. Available at: www.hhs.gov/pandemicflu/plan/appendixd.html.
65

U.S. Department of Homeland Security, Federal Emergency Management Agency. Continuity of Operations (COOP) Programs. Available at: http://www.fema.gov/government/coop/index.shtm#0
Van den Bos K, Lind EA, Vermunt R, Wilke H. How do I judge my outcome when I do not know the outcome of others? The psychology of the fair process effect. Journal of Personality and Social Psychology. 1997;72(5):1034–1046.
Venkataraman ST, Khan N, Brown A. Validation of predictors of extubation success and failure in mechanically ventilated infants and children. Critical Care Medicine. August 2000;28(8):2991–2996.
Vincent JL, Mendonca A, Cantraine F, et al. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Critical Care Medicine. 1998;26(11):1793–1800.
Vincent JL, Moreno R, Takala J, et al. The SOFA (sepsis-related organ failure assessment) score to describe organ dysfunction/failure. Intensive Care Medicine. 1996;22:707–710.
Wennberg JE, Fisher ES, Sharp SM, McAndrew M, Bronner KK (for the Dartmouth Atlas of Health Care Working Group). The Care of Patients with Severe Chronic Illness: An Online Report on the Medicare Program by the Dartmouth Atlas Project. Hanover, NH: The Dartmouth Atlas of Health Care; 2006. Available at: http://www.dartmouthatlas.org/atlases/2006_Chronic_Care_Atlas.pdf.
White DB, Katz MH, Luce JM, Lo B. Who should receive life support during a public health emergency? Using ethical principles to improve allocation decisions. Annals Intern Medicine.2009;150 (2)132-138.
6. Alternative Care Sites
Agency for Healthcare Research and Quality (AHRQ). Reopening Shuttered Hospitals to Expand Surge Capacity. Rockville, MD: AHRQ; March 2006. Available at: http://www.ahrq.gov/research/shuttered/. Accessed July 21, 2006.
Agency for Healthcare Research and Quality (AHRQ). Rocky Mountain Regional Care Model for Bioterrorist Events: Locate Alternate Care Sites During an Emergency. Rockville, MD: AHRQ; December 2004. Available at: http://www.ahrq.gov/research/altsites.htm. Accessed July 21, 2006.
Agency for Healthcare Research and Quality. Alternative Care Site Selection Tool from Rocky Mountain Regional Care Model for Bioterrorist Events. Available at: www.ahrq.gov/downloads/pub/biotertools/alttool.xls. Accessed July 21, 2006.
Barbera J, Macintyre A. Medical and Health Incident Management System: A Comprehensive Functional System Description for Mass Casualty Medical and Health Incident Management. Washington: George Washington University Institute for Crisis, Disaster, and Risk Management; December 2002. Available at: www.gwu.edu/~icdrm. Accessed July 21, 2006.
Blackwell T, Bosse M. Use of an innovative design mobile hospital in the medical response to Hurricane Katrina. Ann Emerg Med. 2007;49(5):580-588.
Bolster CJ. Mobile hospital provides care when disaster strikes. Healthc Financ Manage.2006;60(2):114-116,118.
Burkle FM Jr, Hsu EB, et al. Definition and functions of health unified command and emergency operations centers for large-scale bioevent disasters within the existing ICS. Disaster Med Public Health Prep.2007;1(2):135-141.
Church J. Mass Casualty Strategy for Biological Terror Incidents: Neighborhood Emergency Help Center. SBCCOM Department of the Army; May 2001. Available at: http://www.nnemmrs.org/documents/. Accessed June 12, 2006.
Church J. Mass Casualty Strategy for Biological Terror Incidents: Acute Care Center. SBCCOM Department of the Army; December 2001. Available at: http://www.nnemmrs.org/documents/. Accessed June 12, 2006.
Eastman AL, Rinnert KJ, et al.Alternate site surge capacity in times of public health disaster maintains trauma center and emergency department integrity: Hurricane Katrina. J Trauma. 2007;63(2):253-257.
66

Gavagan TF, Smart K, et al. Hurricane Katrina: medical response at the Houston Astrodome/Reliant Center Complex. South Med J. 2006; 99(9):933-939.
Hick JL, Hanfling D, Burstein JL, DeAtely C, Barbisch D, Bogdan G, Cantrill S. Healthcare facility and community strategies for patient care surge capacity. Annals of Emergency Medicine.2004;44:253–261.
Hick JL, Koenig KL, Barbisch D, Bey TA. Surge capacity concepts for health facilities: the CO-S-TR model for initial incident assessment. Disas Med Pub Health Prepared 2008; 2(Supp 1):S51-S57.
Joint Commission on Accreditation of Healthcare Facilities (JCAHO). Surge Hospitals: Providing Safe Care in Emergencies. Chicago: JCAHO; 2006.
Joint Commission on Accreditation of Healthcare Facilities (JCAHO). Faith-based Organizations as Partners in Emergency Management Planning, Response, and Recovery. Chicago: JCAHO; 2005. Krol DM, Redlener M, et al. A mobile medical care approach targeting underserved populations in post-Hurricane Katrina Mississippi. J Health Care Poor Underserved 2007;18(2):331-340.
Lanzilotti SS. Hawaii Medical Personnel Assessment 2003: A Longitudinal Study of Hawaii Doctors and Nurses, Their Knowledge, Skill, and Willingness to Treat Victims Related to Weapons of Mass Destruction and Naturally Caused Mass Casualty Incidents. Honolulu: Honolulu Emergency Services Department; October 2004.
Millin MG, Jenkins JL, et al. A comparative analysis of two external health care disaster responses following Hurricane Katrina. Prehosp Emerg Care.2006;10(4):451-456.
Sanford C, Jui J, et al. Medical treatment at Louis Armstrong New Orleans International Airport after hurricane Katrina: The experience of disaster medical assistance teams WA-1 and OR-2. Travel Med Infect Dis. 2007 5(4):230-235.
Schultz CH, Stratton SJ. Improving hospital surge capacity: a new concept for emergency credentialing of volunteers. Ann Emerg Med. 2007;49(5):602-609.
Sirbaugh PE, Gurwitch KD, et al. Caring for evacuated children housed in the Astrodome: creation and implementation of a mobile pediatric emergency response team: regionalized caring for displaced children after a disaster. Pediatrics. 2006;117(5 Pt 3):S428-438.
Trabert E, Giovachino M, et al. After Action Review of Federal Medical Station (FMS) Operations During Hurricanes Katrina and Rita. Washington: Department of Health and Human Services; 2006.
U.S. Department of Health and Human Services, Health Resources and Services Administration (HRSA). Emergency Systems for Advance Registration of Volunteer health Professionals (ESAR-VHP) Program: Interim Technical and Policy Guidelines, Standards and Definitions, v. 2. Rockville, MD: HRSA; June 2005.
Vest JR, Valadez AM. Health conditions and risk factors of sheltered persons displaced by Hurricane Katrina. Prehosp Disaster Med. 2006;21(2 Suppl 2): 55-58.
7. Palliative Care
Acquaviva, K. D. (2006). Disaster Palliative Assistance Team (DPAT), under the NDMS system. In A. Wilkinson (Ed.).
Aldrich, N., & Benson, W. F. (2007). Disaster preparedness and the chronic disease needs of vulnerable adults. Preventing Chronic Disease, 5(1), A27.
Alexander D. Nature’s impartiality, man’s inhumanity: reflections on terrorism and world crisis in a context of historical disaster. Disasters.2002;26(1):1–9.
Anonymous. Abstracts from the 14th World Congress for Disaster and Emergency Medicine. May 16–20, 2005. Edinburgh, Scotland. Prehospital and Disaster Medicine. 2005;20(3):s113–s151.
Anonymous. Elderly most in danger as hurricane strikes. SeniorJournal.com. September 2004. Available at: www.seniorjournal.com. Accessed July 12, 2006.
Anonymous. Louisiana nursing homes now vacated, many elderly feared dead. SeniorJournal.com. September 5, 2006. Available at: www.seniorjournal.com/NEWS/Eldercare/5-09-06NurseHomeRescue.htm . Accessed April 27, 2006.
67

Anonymous. More nursing home bodies being found after hurricane. SeniorJournal.com. September 16, 2005. Available at: http://www.seniorjournal.com/NEWS/Eldercare/5-09-16MoreBodies.htm. Accessed July 12, 2006.
Bankoff G. Rendering the world unsafe: "vulnerability" as Western discourse. Disasters.2001;25(1):19–35.
Bauman A. Amidst hurricanes, blackouts, and floods.... how prepared is your hospice? Insights.September 2005:14–17.
Bierce A. The coup de grace. In: Ingram J, David C, eds. The Collected Works of Ambrose Bierce, Vol. II: In the Midst of Life: Tales of Soldiers and Civilians.San Francisco: PG Distributed Proofreaders; 2005.
Black R. Ethical codes in humanitarian emergencies: from practice to research? Disasters. 2003;27(2):95–108.
Brown V, Jacquier G, Coulombier D, Balandine S, Belanger F, Legros D. Rapid assessment of population size by area sampling in disaster situations. Disasters. 2001;25(2):164–171.
Challen, K., Bentley, A., Walter, D., & Bright, J. (2008). Severity of illness assessment in community-acquired pneumonia.[comment]. Intensive Care Medicine, 34(5), 967; author reply 968.
Center for Biosecurity of the University of Pittsburgh Medical Center. National strategy for pandemic influenza and the HHS Pandemic Influenza Plan: thoughts and comments. Biosecurity and Bioterrorism: Biodefense and Strategy, Practice, and Science. 2005;3(4):292–294.
Christian, M. D., Devereaux, A. V., Dichter, J. R., Geiling, J. A., & Rubinson, L. (2008). Definitive Care for the Critically Ill During a Disaster: Current Capabilities and Limitations: From a Task Force for Mass Critical Care Summit Meeting, January 26-27, 2007, Chicago, IL. Chest, 133(5_suppl), 8S-17.
Devereaux, A. V., Dichter, J. R., Christian, M. D., Dubler, N. N., Sandrock, C. E., Hick, J. L., et al. (2008). Definitive Care for the Critically Ill During a Disaster: A Framework for Allocation of Scarce Resources in Mass Critical Care: From a Task Force for Mass Critical Care Summit Meeting, January 26-27, 2007, Chicago, IL. Chest, 133(5_suppl), 51S-66.
Domres B. The challenge of crisis. Pain Practice.2003;3(1):97–99.
Domres B, Manger A, Steigerwald I, Esser S. The challenge of crisis, disaster, and war: experience with UN and NGOs. Pain Practice. 2003;3(1):97–100.
Dyer BC. The Impact of Natural Disaster on Older Adults: Lessons Learned from Hurricane Katrina.American Geriatrics Society 2006 Annual Scientific Meeting. Edwards JCP, Stapley J, Akins R. Regional Strategies to Prepare for Public Health Disasters in Texas Offer Lessons About Community Resource Allocation. Rockville, MD: Agency for Healthcare Research and Quality; 2005.
EM-DAT Emergency Disaster Data Base. About EM-DAT. (2007). Retrieved 04/12/2008, from http://www.em-dat.net/who.htm.
Franco, C., Toner, E., Waldhorn, R., Maldin, B., O’Toole, T., & Inglesby, T. (2006). Systemic collapse: Medical care in the aftermath of Hurricane Katrina. Biosecurity and Bioterrorism: Biodefense Strategy, Practice, and Science, 4(2), 135-146.
Gibson, M. J. (2006). We can do better: Lessons learned for protecting older persons in disasters.Washington, DC,: AARP.
Health Systems Research, Inc. Altered Standards of Care in Mass Casualty. Bioterrorism and Other Public Health Emergencies. Rockville, MD:Agency for Healthcare Research and Quality; 2005.
Hearne SA, Segals LM, Earls MJ. Ready or Not? Protecting the Public’s Health from Diseases, Disasters, and Bioterrorism. Washington: Trust for America’s Health, 2005.
Hersey J. Hiroshima. The New Yorker. August 31, 1946.
Homan P. Responding to crisis: a bereavement perspective. Insights. September 2005:35–37. Homeland Security Council. National Strategy for Pandemic Influenza. Washington: Homeland Security Council; 2005.
Hooke WR, Rogers PG. Public Health Risks of Disasters: Communication, Infrastructure and Preparedness – Workshop Summary. Washington: National Institute of Medicine; 2005.
68
Institute of Medicine. Preparing for the Psychological Consequences of Terrorism: A Public Health Strategy. Washington: National Academies Press; 2003. Available at: http://www.nap.edu/openbook/0309089530/html.Accessed July 12, 2006.
Joint Commission on Accreditation of Healthcare Organizations (JCAHO). Standing Together: An Emergency Planning Guide for America’s Communities. Chicago: JCAHO; 2005. Light PC. The Katrina Effect on American Preparedness. New York: New York University Press; 2005.
Matzo, M., Wilkinson, A., Lynn, J., Gatto, M., & Phillips, S. J. (2009). Palliative Care Considerations for Mass Casualty Events with Scarce Resources. Biosecurity and Bioterrorism: Biodefense Strategy, Practice, and Science 6.
McGough MF, Leer L, Tipton S, Tinker TL, Vaughn E. Communicating the risks of bioterrorism and other emergencies in a diverse society: a case study of special populations in North Dakota. Biosecurity and BioTerrorism: Biodefense Strategy, Practice, and Science. 2005;3(3):235–245.
National Center for Disaster Preparedness (NCDP) at Columbia's Mailman School of Public Health. More than $5 billion spent on bioterrorism preparedness, but Americans remain deeply concerned about safety and a majority lack confidence in government and health system to respond effectively. NCDP Web site. September 8, 2003. Available at: http://www.ncdp.mailman.columbia.edu/files/press_release.pdf. Accessed July 12, 2006.
National Consensus Project for Quality Palliative Care (2009). from http://www.nationalconsensusproject.org/National Defense Medical System (NDMS). Report on the National Disaster Medical System 2005 Hurricane Response. Reno, NV: NDMS; 2006.
Okie, S. (2008). Dr. Pou and the hurricane—implications for patient care during disasters. NewEngland Journal of Medicine, 358(1), 1-5.
Orr, R. D. “Ethical Issues in Bioterrorism.” Bioterrorism email module #12, 2003. Retrieved April 27, 2006.
Pan American Health Organization. Management of Dead Bodies in Disaster Situations. Washington: Pan American Health Organization; 2004.
Pan American Health Organization. Management of Dead Bodies After Disasters: A Field Manual for First Responders. Washington: Pan American Health Organization; 2006.
Penner NR. Understanding the role of today’s relief agencies and how best to work with them. Insights.September 2005: 30–34.
Perry RW, Lindell MK. Preparedness for emergency response: guidelines for the emergency planning process. Disasters. 2003;27(4):336–350.
Pupavac V. Therapeutic governance: psychosocial intervention and trauma risk management. Disasters.2001;25(4):358–372.
Ringel, J. S., Chandra, A., Leuschner, K., Lim, Y. W., Lurie, N.(2007). Lessons learned from the State and local public health response to Hurricane Katrina.
Rioux P. St. Rita’s owners say no help offered before Katrina hit. SeniorJournal.com. April 27, 2006. Available at: www.seniorjournal.com/NEWS/Eldercare/5-09-15StRitaNoHelp.htm. Accessed July 12, 2006.
Roberts, M., & De Renzo, E. G. (2007). Chapter II. Ethical Considerations in Community Disaster Planning In Agency for Healthcare Research and Quality (AHRQ). Mass Medical Care with Scarce Resources: A Community Planning Guide.Retrieved. from www.ahrq.gov/research/mce
Robinson, L., Nuzzo, J. B., & Talmor, D. S. (2005). Augmentation of hospital critical care capacity after bioterrorist attacks or epidemics: Recommendations of the Working Group on Emergency Mass Critical Care. Crit Care Med, 33, 2393-2403.
Rubinson, L., Hick, J. L., Curtis, J. R., Branson, R. D., Burns, S., Christian, M. D., et al. (2008). Definitive Care for the Critically Ill During a Disaster: Medical Resources for Surge Capacity: From a Task Force for Mass Critical Care Summit Meeting, January 26-27, 2007, Chicago, IL. Chest, 133(5_suppl), 32S-50.
Roy M. Ten Steps in the Management of Biological Casualties on the Battlefield. USAMRIID’s Medical Management of Biological Casualties. Frederick, MD: U.S. Army Medical Research Institute of Infectious Diseases; 2001.
69
U.S. Department of Health and Human Services (DHHS). Mental Health Response to Mass Violence and Terrorism: A Training Manual. DHHS Pub. No. SMA 3959. Rockville, MD: Center for Mental Health Services, Substance Abuse and mental Health Services Administration; 2004.
Saliba D, Buchanan J, Kingston RS. Disaster preparedness for vulnerable populations: the disabled, seriously ill or frail elderly. American Journal of Public Health. 2002;94:1436–1441.
Saliba DM, Buchanan J, Kington RS. Function and response of nursing facilities during community disaster. American Journal of Public Health.2004;94(8):1436–1441.
U.S. Naval Reserve Commission. Dirty bombs.Backgrounder. April 2005:1–6.
U.S. Naval Reserve Commission. Dirty Bombs.Washington: Office of Population Affairs; 2006. Salinsky, E. (2008). Strong as the Weakest Link.
Issue Brief/National Health Policy Forum(65), 1-21. U.S. Department of Homeland Security, National Preparedness Guidelines. (2007). Retrieved 4/21/2009, from http://www.dhs.gov/xlibrary/assets/National_Preparedness_Guidelines.pdf
Viboud C. Interregional spread of influenza through United States described by virus type, size of population and commuting rates and distance. NIH News. April 19, 2006. Available at: http://www.nih.gov/news/pr/apr2006/fic-19.htm.Accessed July 12, 2006.
Spiegel PB, Sheik M, Woodruff BA, Burnham G. The accuracy of mortality reporting in displaced persons camps during the post-emergency phase. Disasters. 2001;25(2):172–180.
World Health Organization (WHO). Avian influenza – fact sheet. WHO Web site. January 15, 2004. Available at: www.who.int/csr/don/2004_01_15/en/print.html.Accessed July 12, 2006. Stanford University. The influenza pandemic of
1918. Stanford University Web site. Available at: http://www.stanford.edu/group/virus/uda/index.html. Accessed July 12, 2006.
Wein LM, Craft DL. Evaluation of public health interventions for anthrax: a report to the Secretary’s Council on Public Health Preparedness. Biosecurity and Bioterrorism; Biodefense and Strategy,Practice, and Science. 2005;3(4):348–356.Stoto M. Measuring Public Health Preparedness.
Presented at the RAND Performance Measurement Seminar, Center for Domestic and International Health Security, Washington, May 18, 2006. United States Government Accountability Office (GAO). Emergency Preparedness: States Are Planning for Medical Surge, but Could Benefit from Shared Guidance for Allocating Scarce Medical Resources. (2008). Retrieved. from http://www.gao.gov/htext/d08668.html.
United States: Who's to blame? Katrina deaths. (2007). The Economist, 385(8550). U.S. Department of Homeland Security (DHS). National Response Plan. Washington: DHS; 2004.
U.S. Department of Health and Human Services (DHHS). Mental Health All-Hazards Disaster Planning Guidance. DHHS Pub. No. SMA 3829. Rockville, MD: Center for Mental Health Services, Substance Abuse and Mental Health Services Administration; 2003.
70

540 Gaither Road, Rockville, MD 20850
AHRQ Publication No. 09-0016September 2009
ISBN No. 978-1-58763-388-1