management of class ii and iii malocclusion
TRANSCRIPT

Management of Class II and Class III Malocclusion

What is Normal / Ideal / Gold Standard?• Dental Objectives:
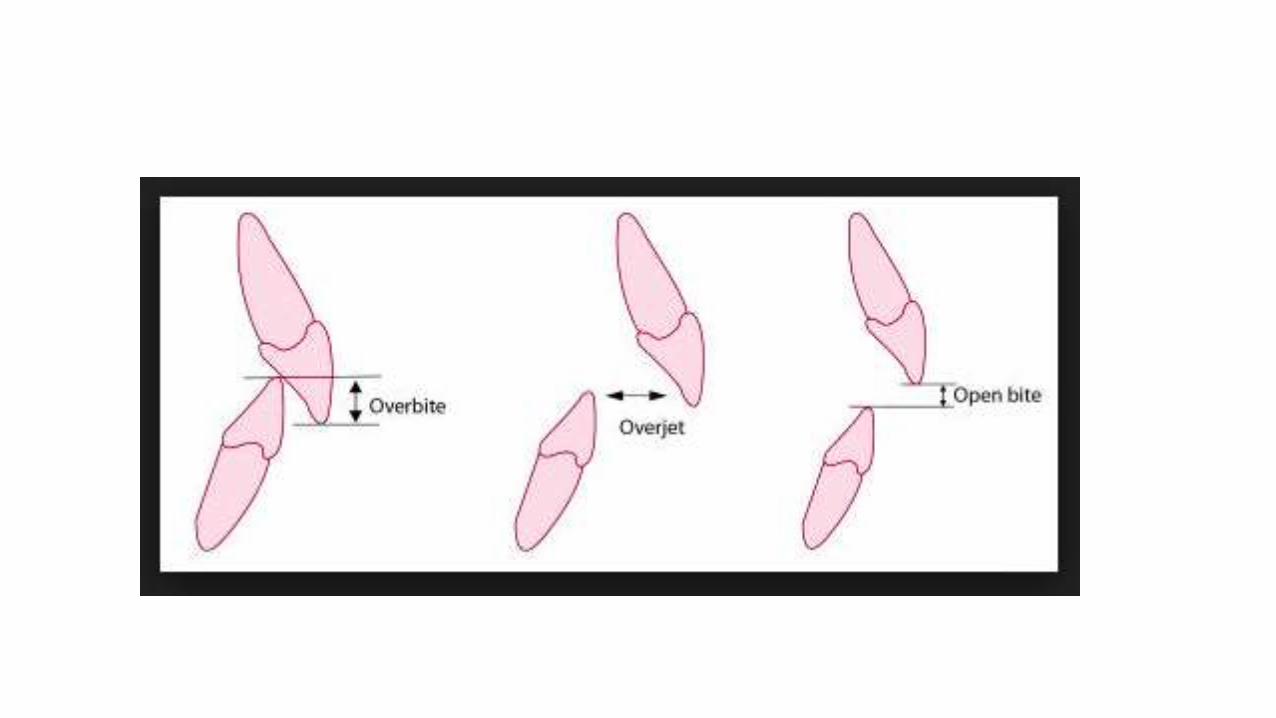
• Ideal Overjet
• Ideal Overbite
• Co-incident midlines
• Class I Incisor and canine Relationship
• Fully intercuspated molar relationship Class I / II / III
• Tight contacts
• Complete leveling and alignment
• Functional Occlusion
What is Normal / Ideal / Gold Standard?
• Facial / Skeletal Objectives:• Well balanced facial profile i.e. straight faical profile
• Normal / near normal vertical facial dimensions
• Improved competency of lips
• Balanced lip profile i.e. no lip procumbency or recumbency
• Ideal incisal display on smile and at rest
• Ideal esthetic line / smile arc
• Normal TMJ function
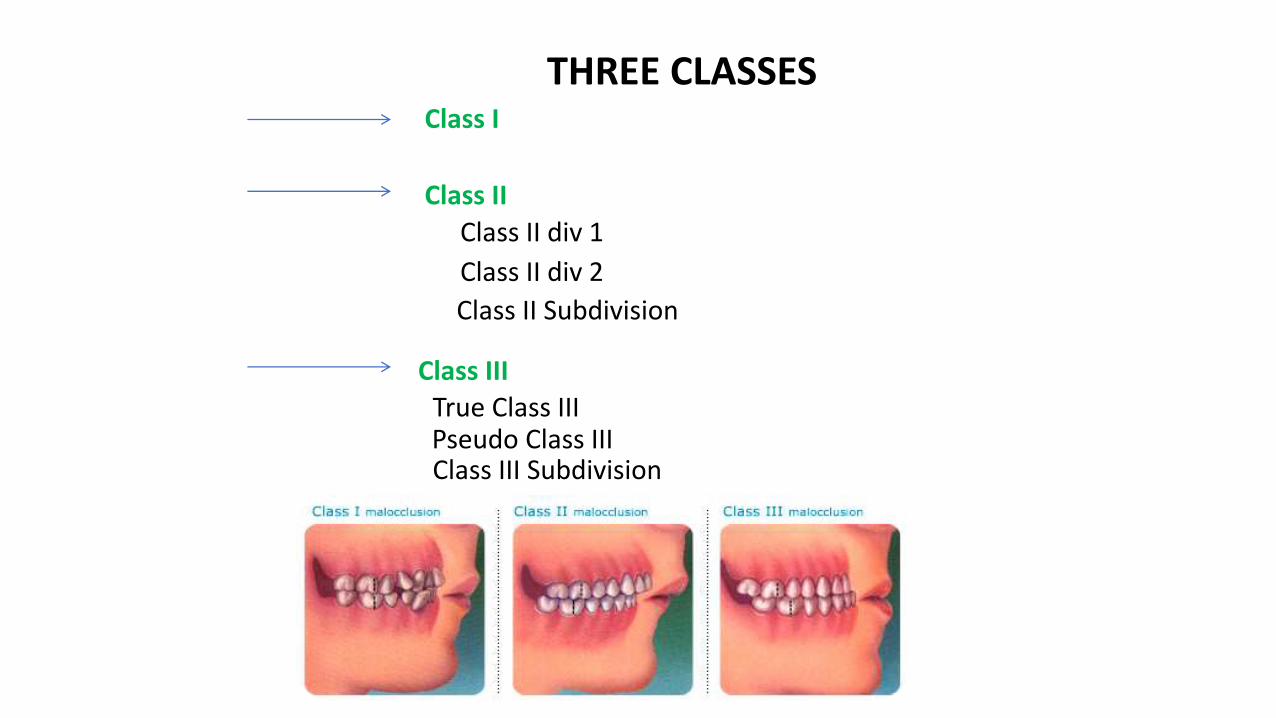
Class I
Class II
Class II div 1
Class II div 2
Class II Subdivision
Class III
True Class IIIPseudo Class III
THREE CLASSES
Class III Subdivision
Class II malocclusion
• Dental Class II• Class II Division 1
• Class II Division 2
• Skeletal Class II

Management of Dental Class II Malocclusion
Division 1
Division 2
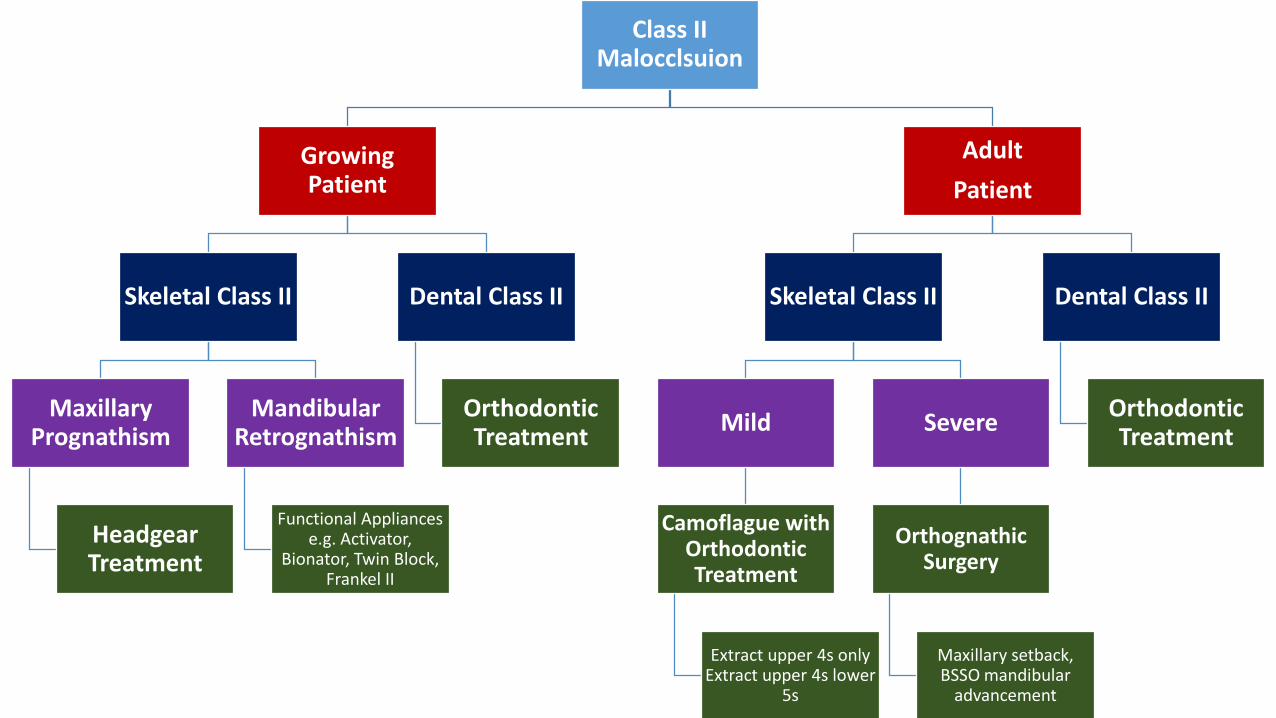
Class II Malocclsuion
Growing Patient
Skeletal Class II
Maxillary Prognathism
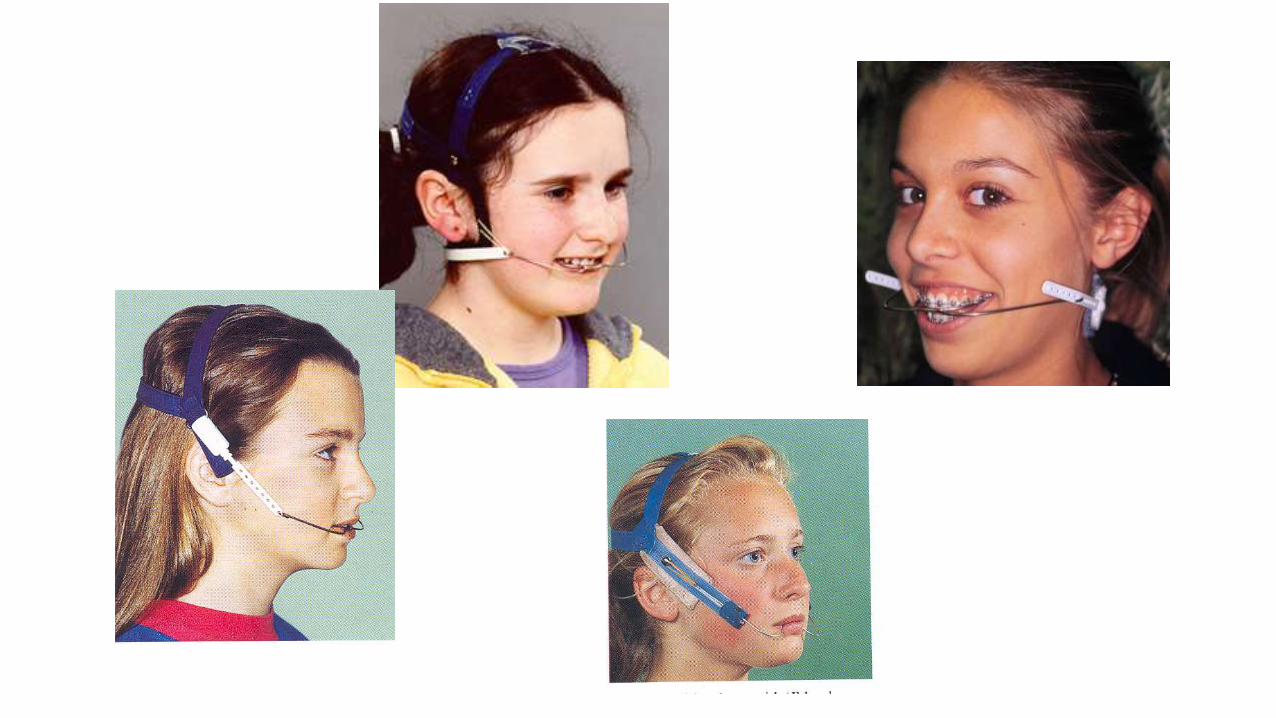
Headgear Treatment
Mandibular Retrognathism
Functional Appliances e.g. Activator,
Bionator, Twin Block, Frankel II
Dental Class II
Orthodontic Treatment
Adult
Patient
Skeletal Class II
Mild
Camoflague with Orthodontic Treatment
Extract upper 4s onlyExtract upper 4s lower
5s
Severe
OrthognathicSurgery
Maxillary setback,BSSO mandibular
advancement
Dental Class II
Orthodontic Treatment

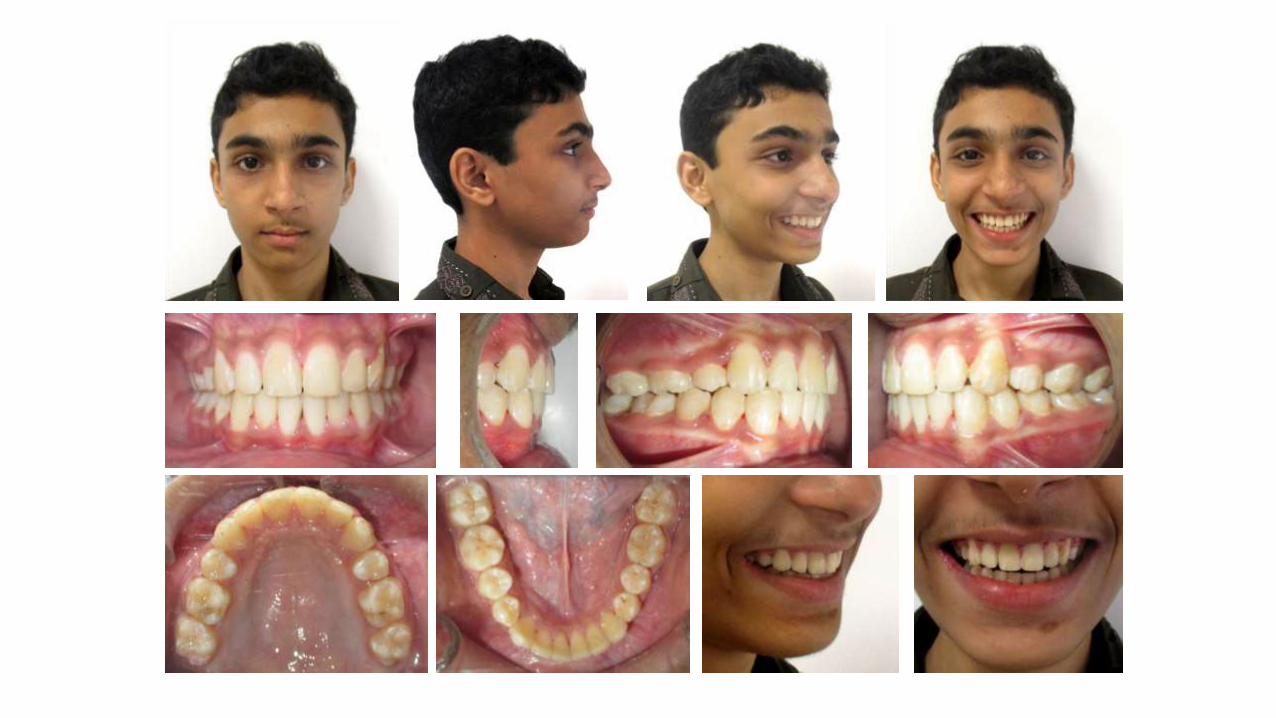
Class II Division 1 Malocclusion

Class II Division 2 Malocclusion

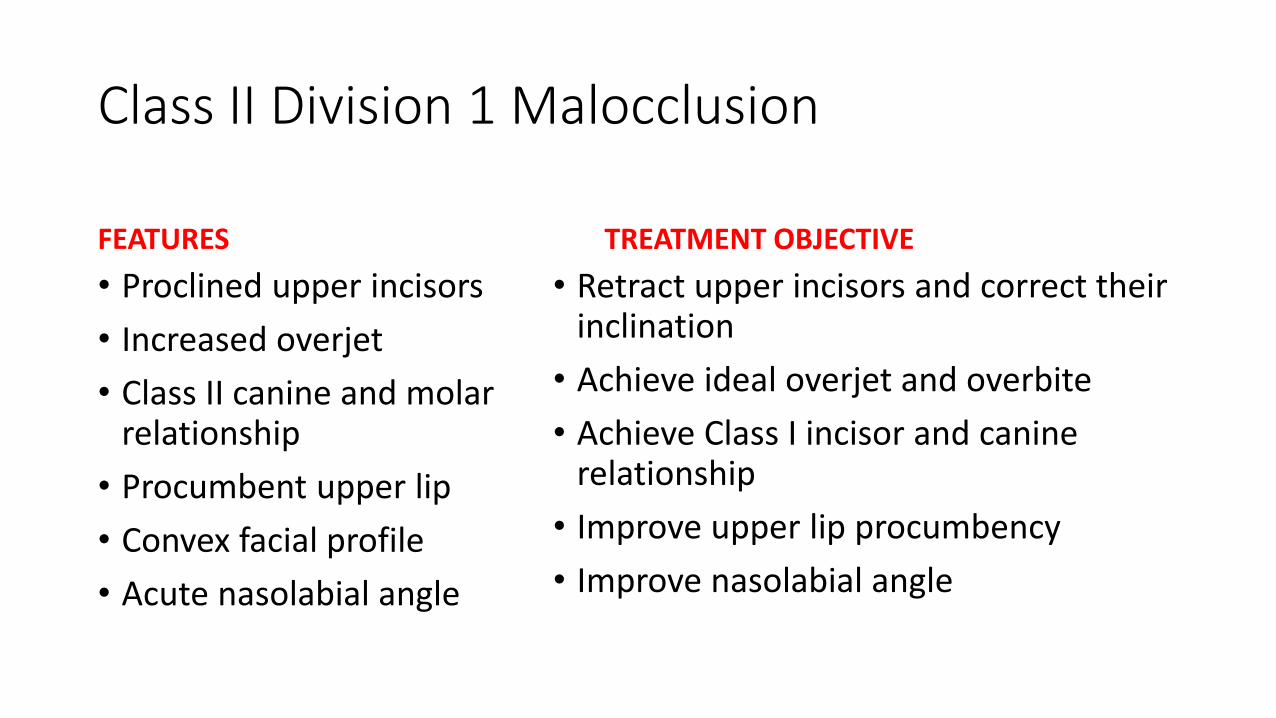
Class II Division 1 Malocclusion
FEATURES
• Proclined upper incisors
• Increased overjet
• Class II canine and molar relationship
• Procumbent upper lip
• Convex facial profile
• Acute nasolabial angle
TREATMENT OBJECTIVE
• Retract upper incisors and correct their inclination
• Achieve ideal overjet and overbite
• Achieve Class I incisor and canine relationship
• Improve upper lip procumbency
• Improve nasolabial angle
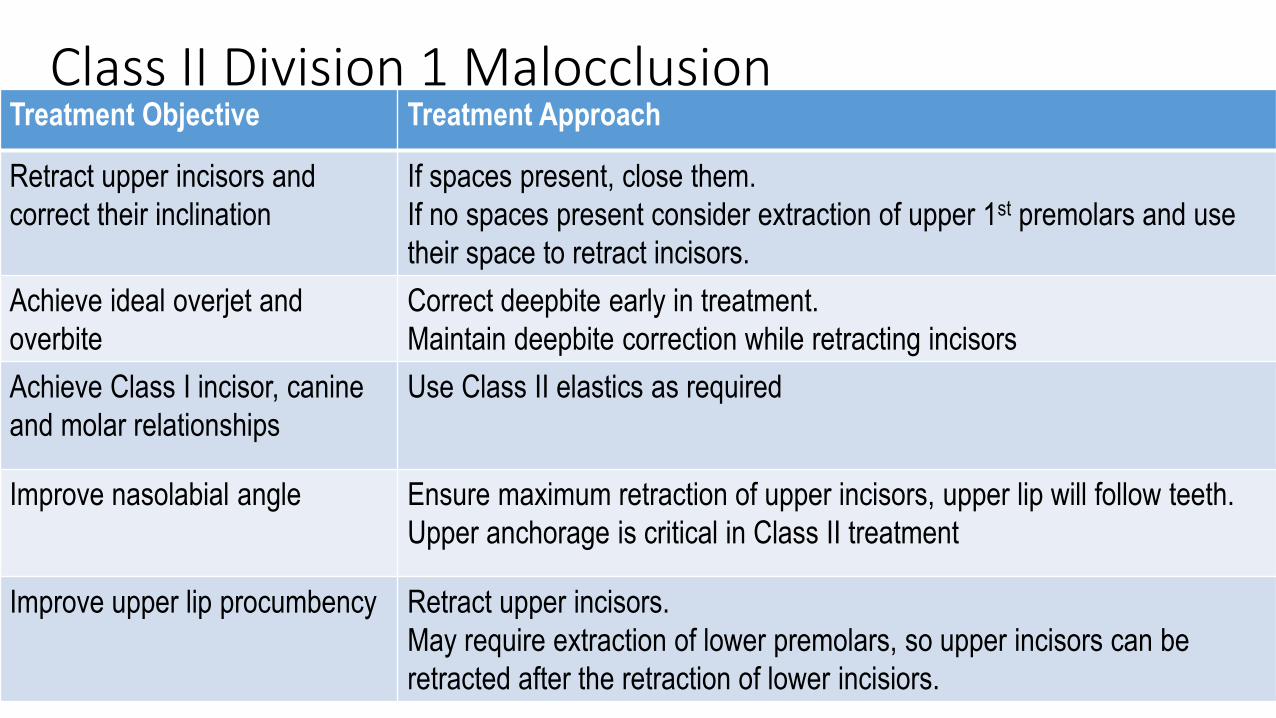
Treatment Objective Treatment Approach
Retract upper incisors and
correct their inclination
If spaces present, close them.
If no spaces present consider extraction of upper 1st premolars and use
their space to retract incisors.
Achieve ideal overjet and
overbite
Correct deepbite early in treatment.
Maintain deepbite correction while retracting incisors
Achieve Class I incisor, canine
and molar relationships
Use Class II elastics as required
Improve nasolabial angle Ensure maximum retraction of upper incisors, upper lip will follow teeth.
Upper anchorage is critical in Class II treatment
Improve upper lip procumbency Retract upper incisors.
May require extraction of lower premolars, so upper incisors can be
retracted after the retraction of lower incisiors.
Class II Division 1 Malocclusion
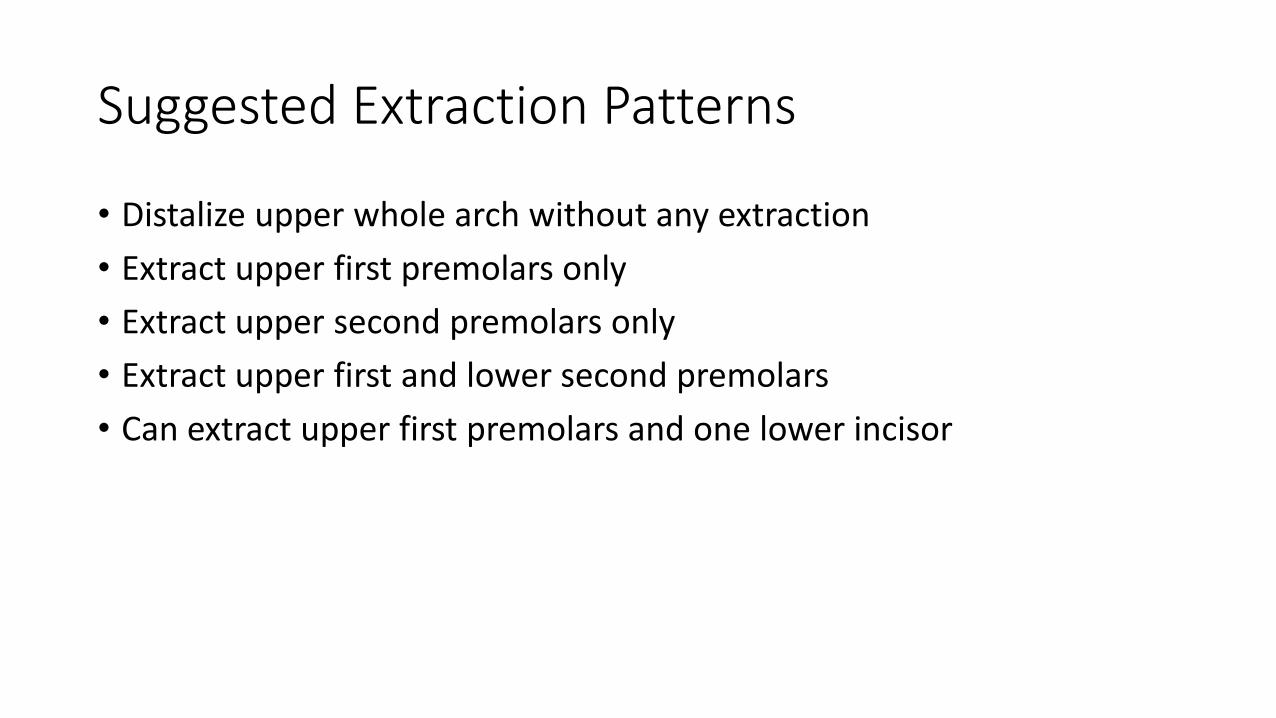
Suggested Extraction Patterns
• Distalize upper whole arch without any extraction
• Extract upper first premolars only
• Extract upper second premolars only
• Extract upper first and lower second premolars
• Can extract upper first premolars and one lower incisor

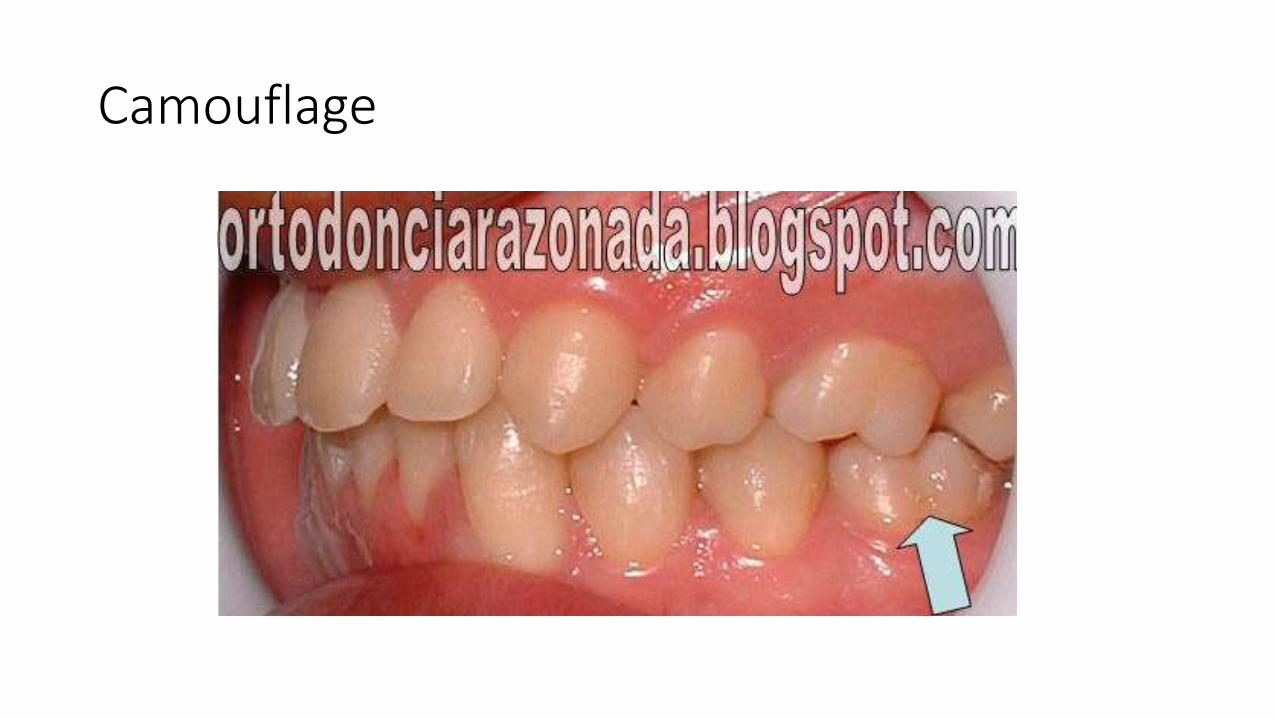
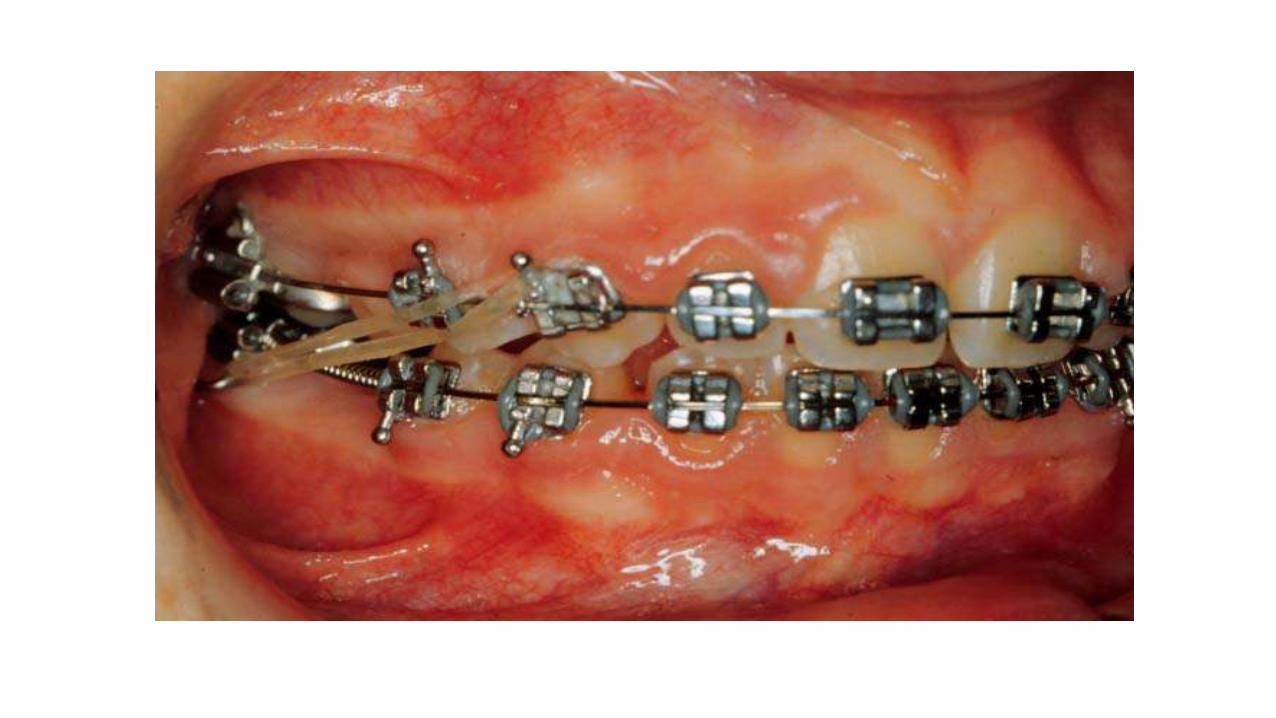
Camouflage
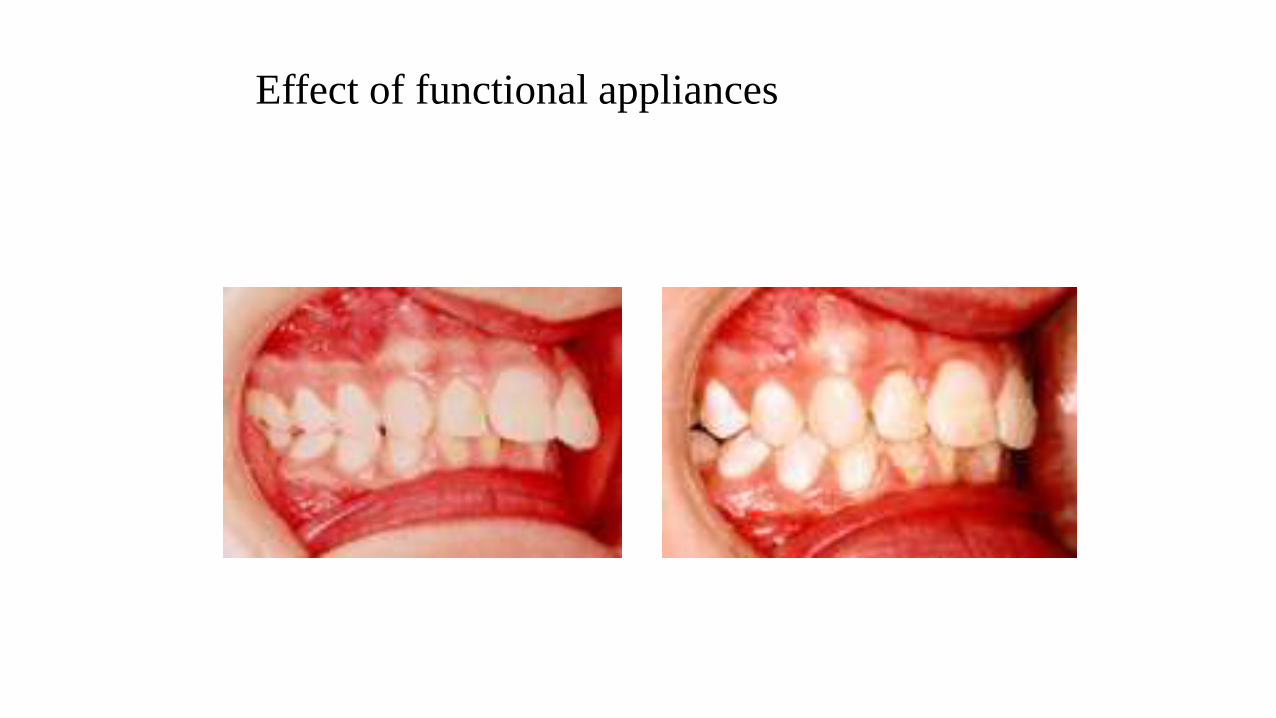
Effect of functional appliances
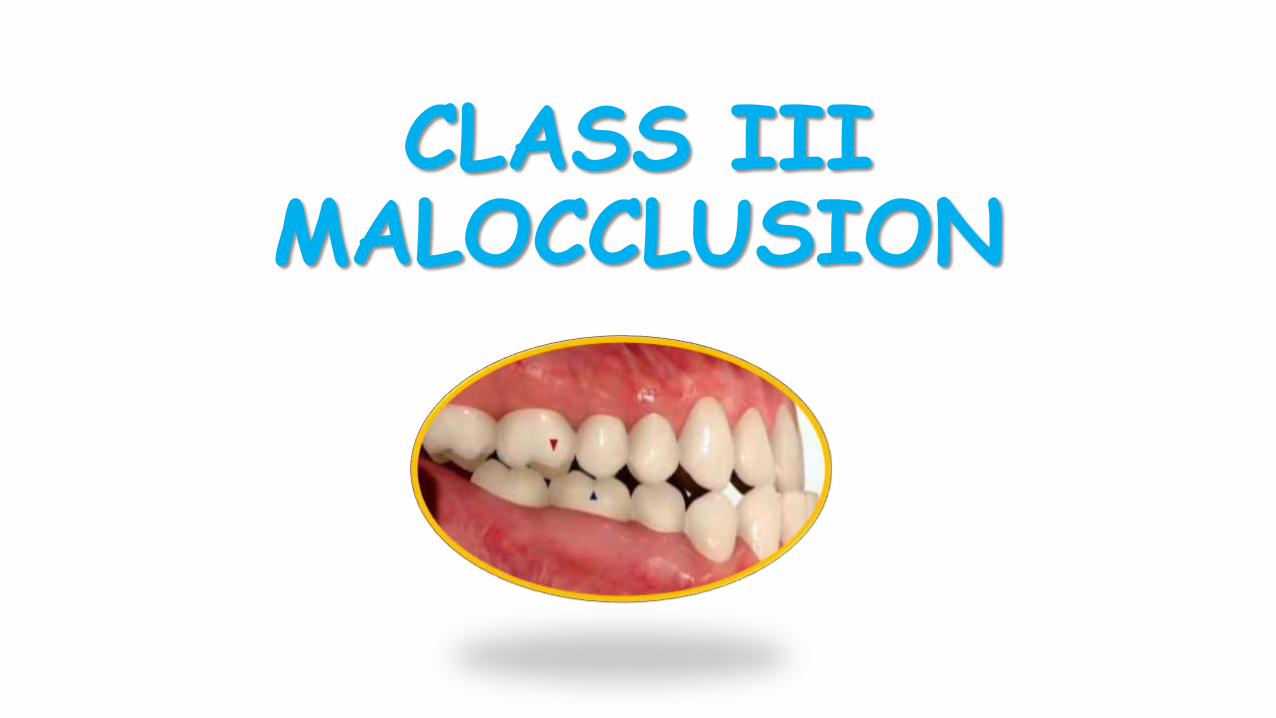
CLASS III MALOCCLUSION
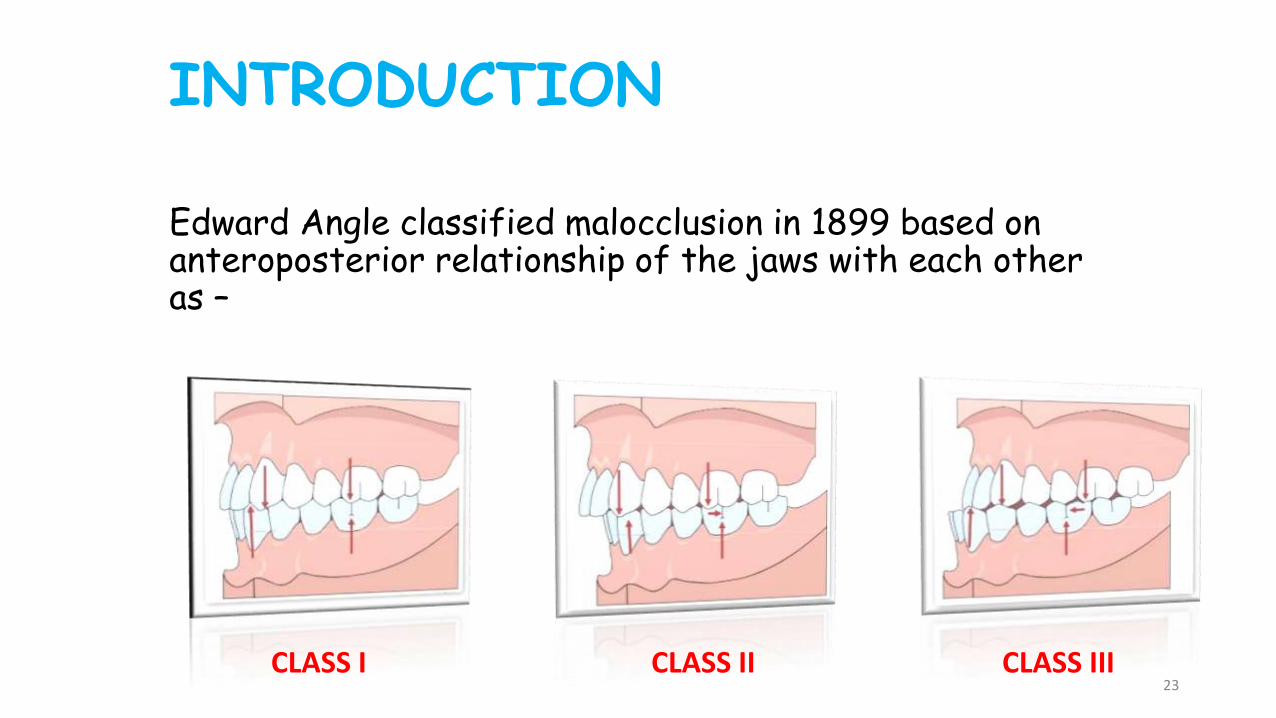
INTRODUCTION
Edward Angle classified malocclusion in 1899 based on anteroposterior relationship of the jaws with each other as –
CLASS I CLASS II CLASS III23
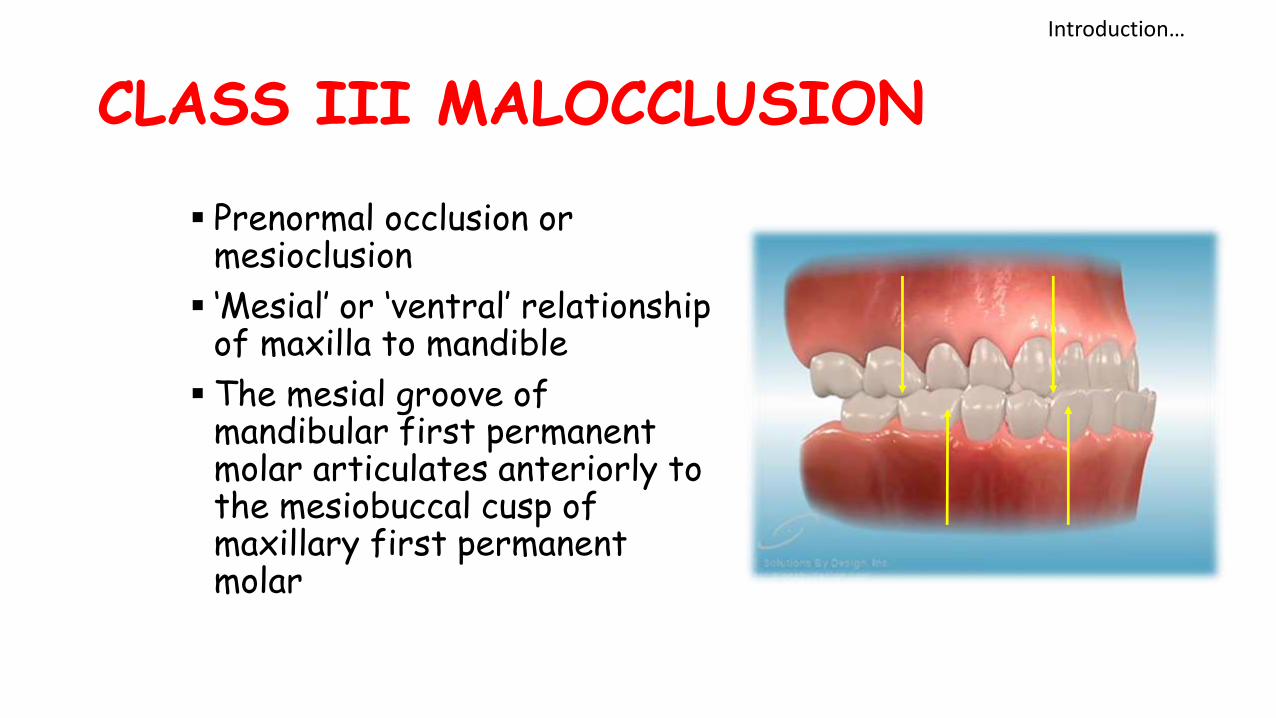
CLASS III MALOCCLUSION
Prenormal occlusion or mesioclusion
‘Mesial’ or ‘ventral’ relationship of maxilla to mandible
The mesial groove of mandibular first permanent molar articulates anteriorly to the mesiobuccal cusp of maxillary first permanent molar
Introduction…
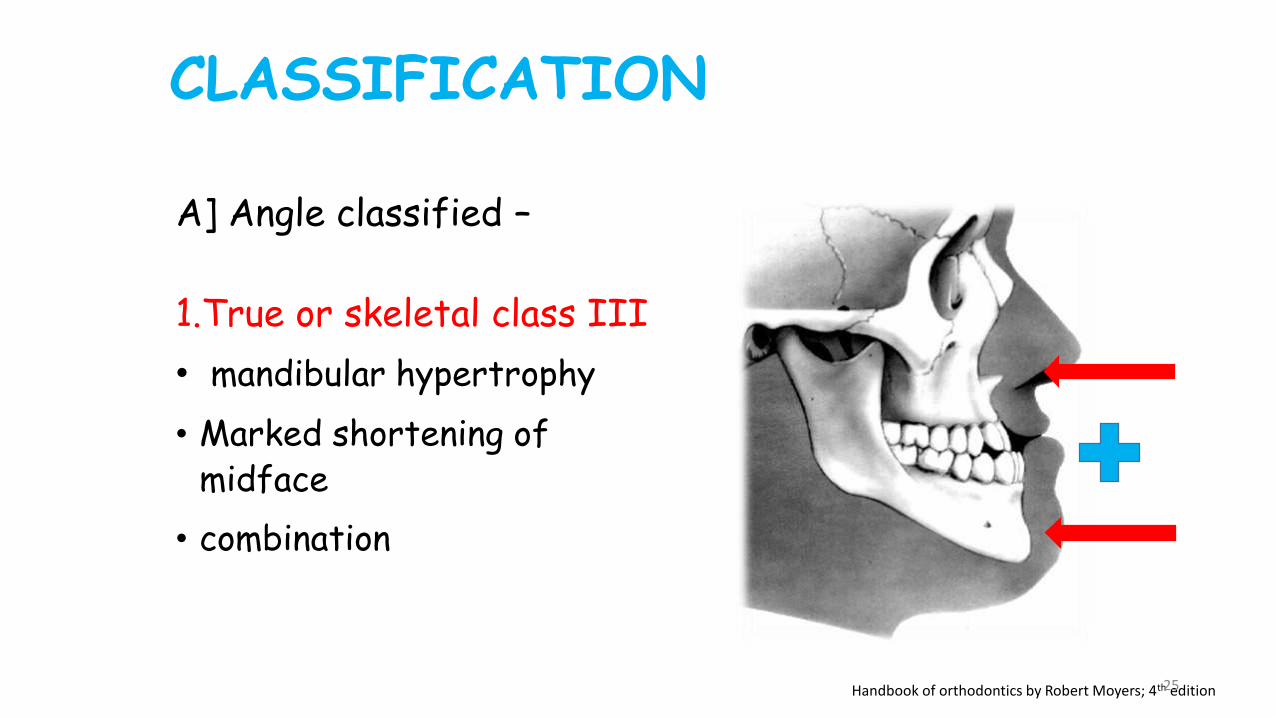
1.True or skeletal class III
• mandibular hypertrophy
• Marked shortening of midface
• combination
Handbook of orthodontics by Robert Moyers; 4th edition25
A] Angle classified –
CLASSIFICATION
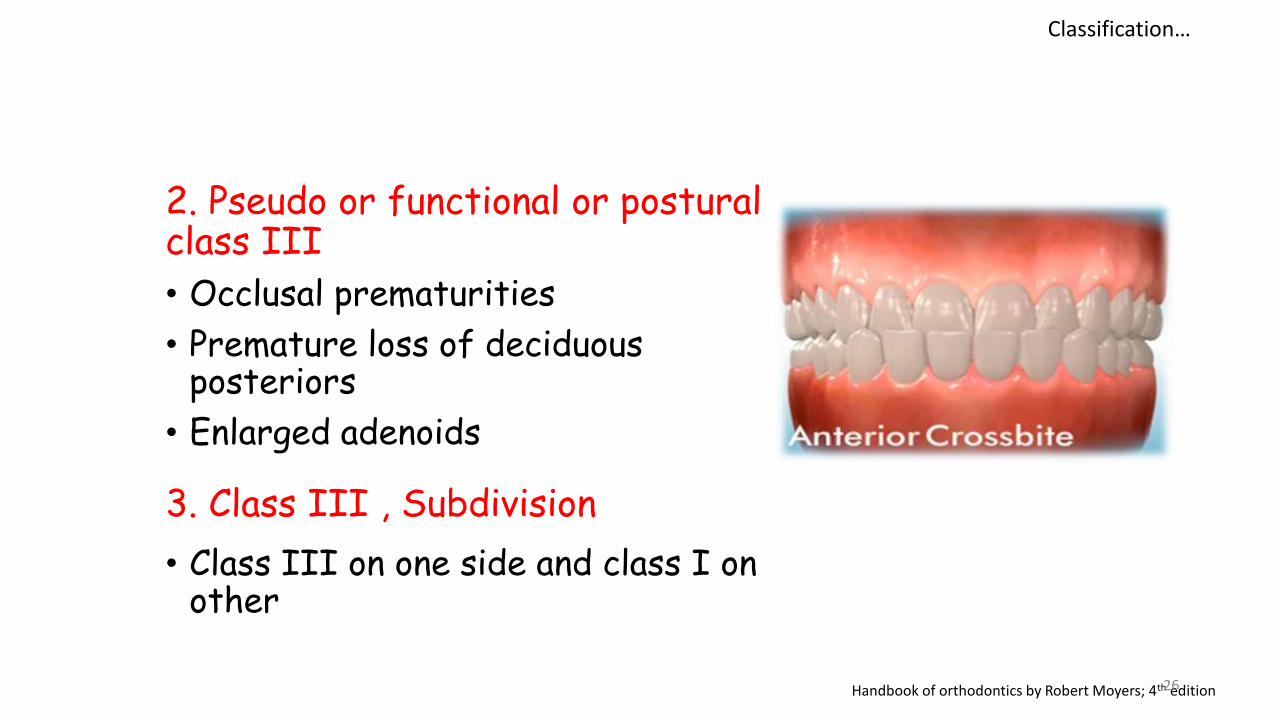
2. Pseudo or functional or postural class III
• Occlusal prematurities
• Premature loss of deciduous posteriors
• Enlarged adenoids
3. Class III , Subdivision
• Class III on one side and class I on other
Handbook of orthodontics by Robert Moyers; 4th edition26
Classification…
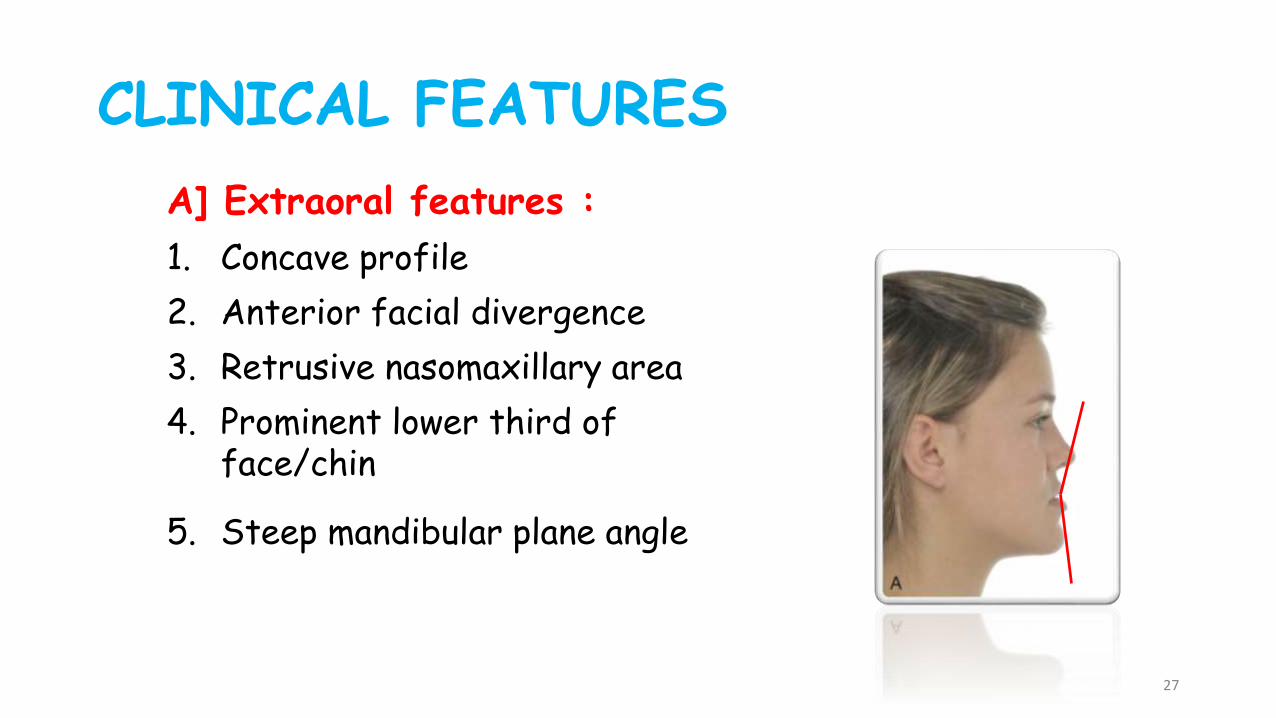
CLINICAL FEATURES
A] Extraoral features :
1. Concave profile
2. Anterior facial divergence
3. Retrusive nasomaxillary area
4. Prominent lower third of face/chin
5. Steep mandibular plane angle
27
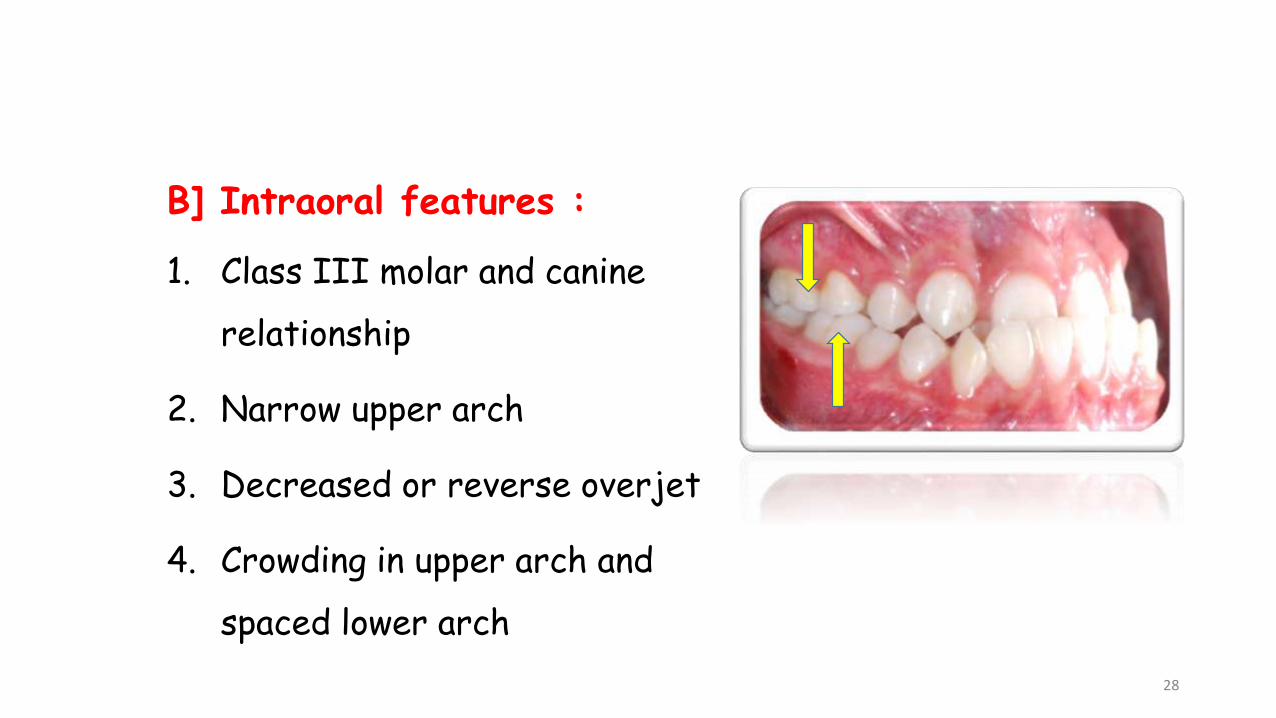
B] Intraoral features :
1. Class III molar and canine
relationship
2. Narrow upper arch
3. Decreased or reverse overjet
4. Crowding in upper arch and
spaced lower arch
28
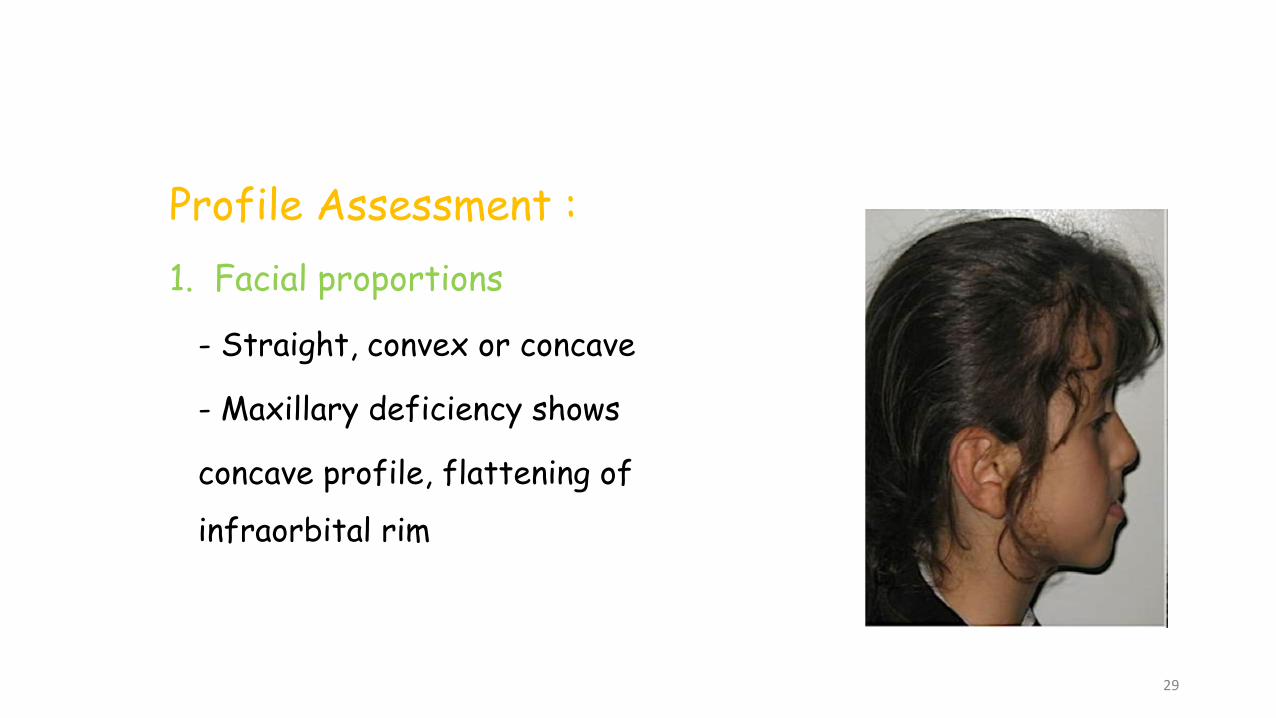
Profile Assessment :
1. Facial proportions
- Straight, convex or concave
- Maxillary deficiency shows
concave profile, flattening of
infraorbital rim
29
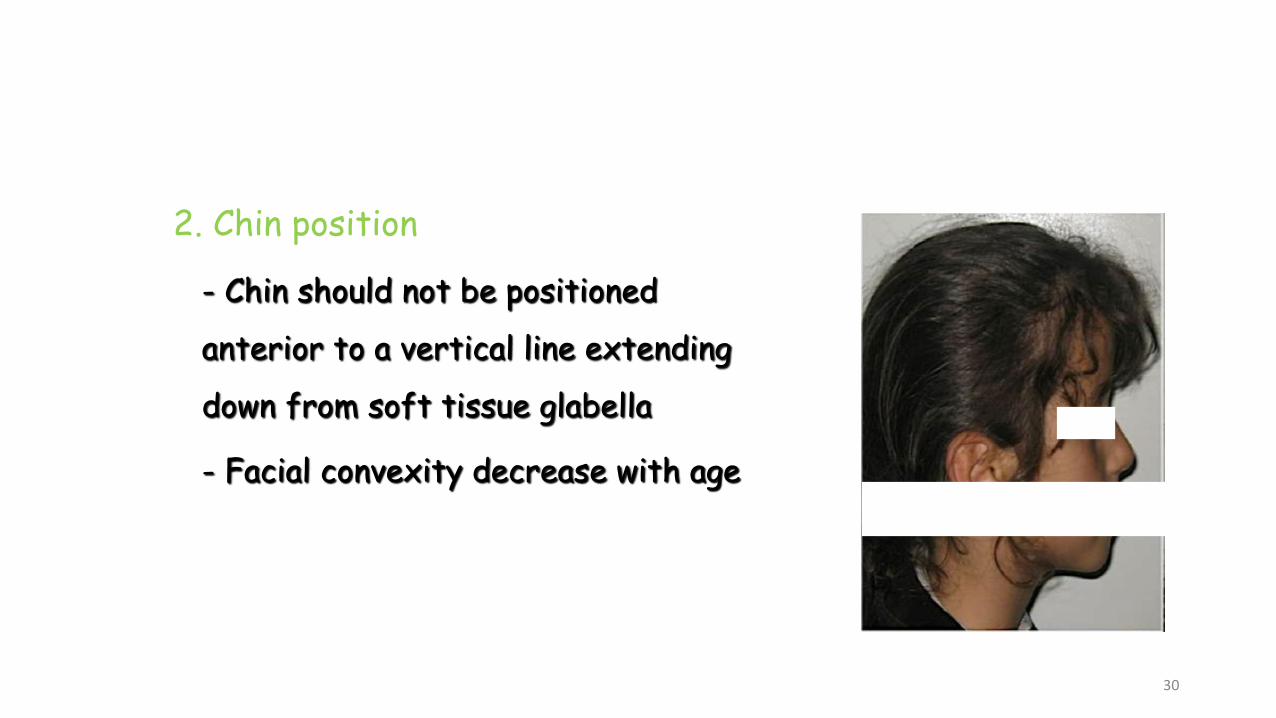
2. Chin position
- Chin should not be positioned
anterior to a vertical line extending
down from soft tissue glabella
- Facial convexity decrease with age
30
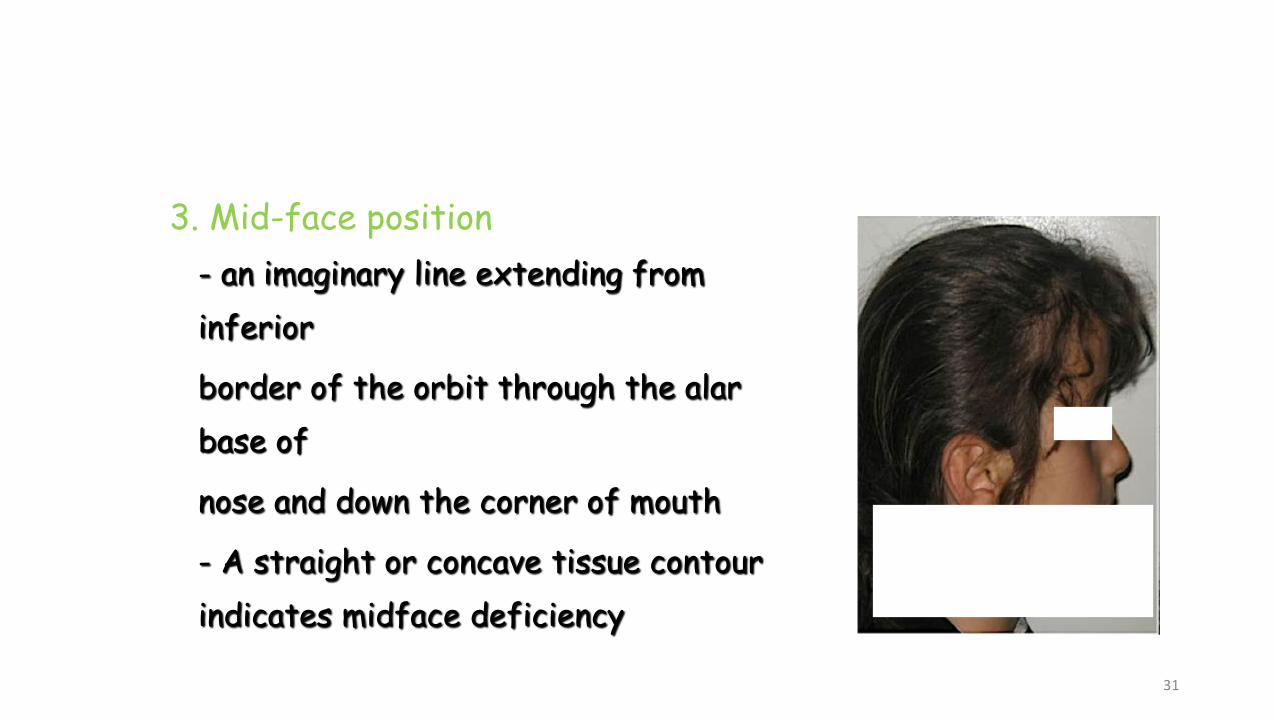
3. Mid-face position
- an imaginary line extending from
inferior
border of the orbit through the alar
base of
nose and down the corner of mouth
- A straight or concave tissue contour
indicates midface deficiency
31
4. Vertical proportions
- Checked in CO and CR
- Normal ratio for lower facial height to total facial
height is 0.55
- Decreased in patients with functional shift and
overclosure of mandible
32
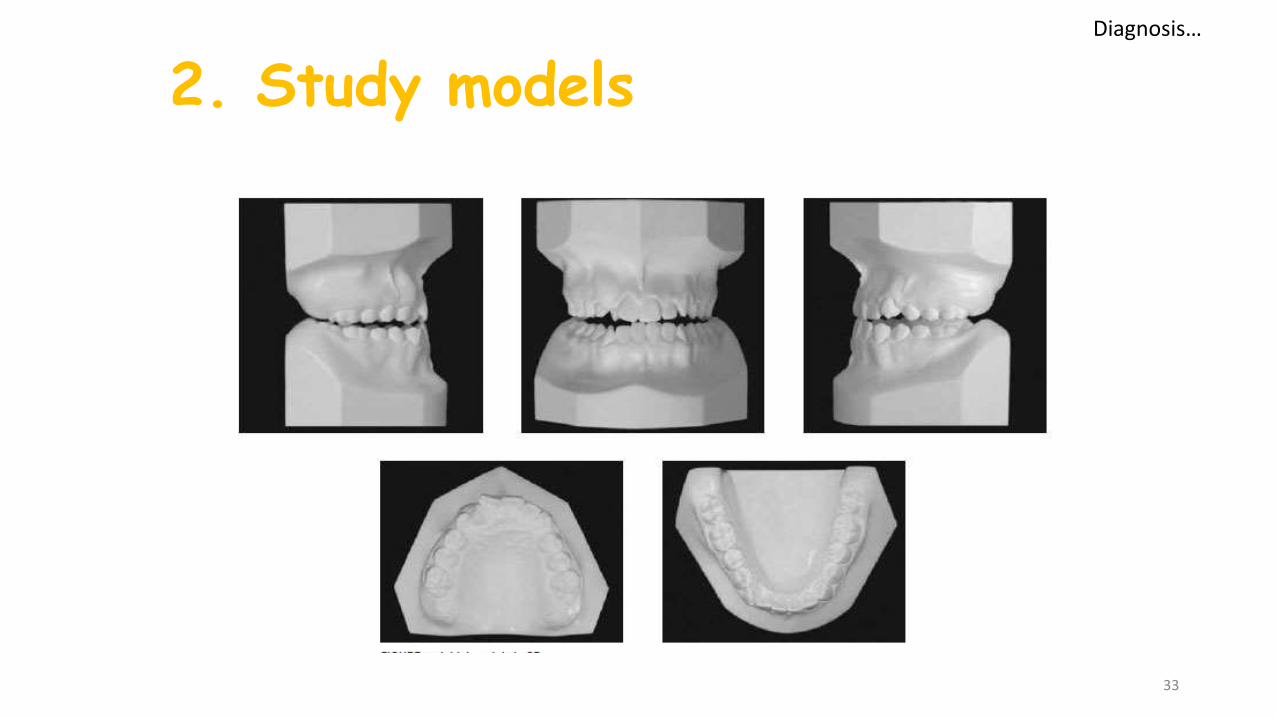
2. Study models
33
Diagnosis…
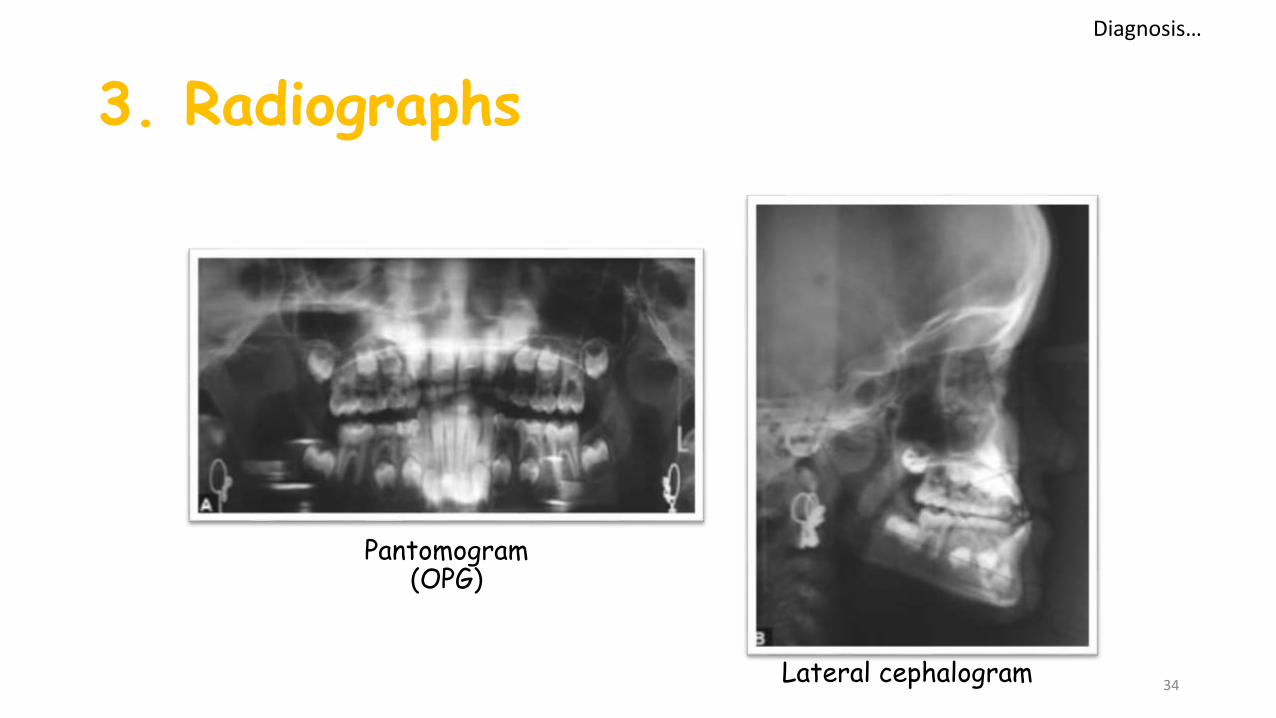
3. Radiographs
34
Pantomogram (OPG)
Lateral cephalogram
Diagnosis…

4. Cephalometric analysis
The SNA angle is significantly
lower
Negative ANB angle
Greater mandibular protrusion
Increased gonial angle
(more obtuse)
Steep mandibular plane angle
Increased lower facial height
35
Diagnosis…
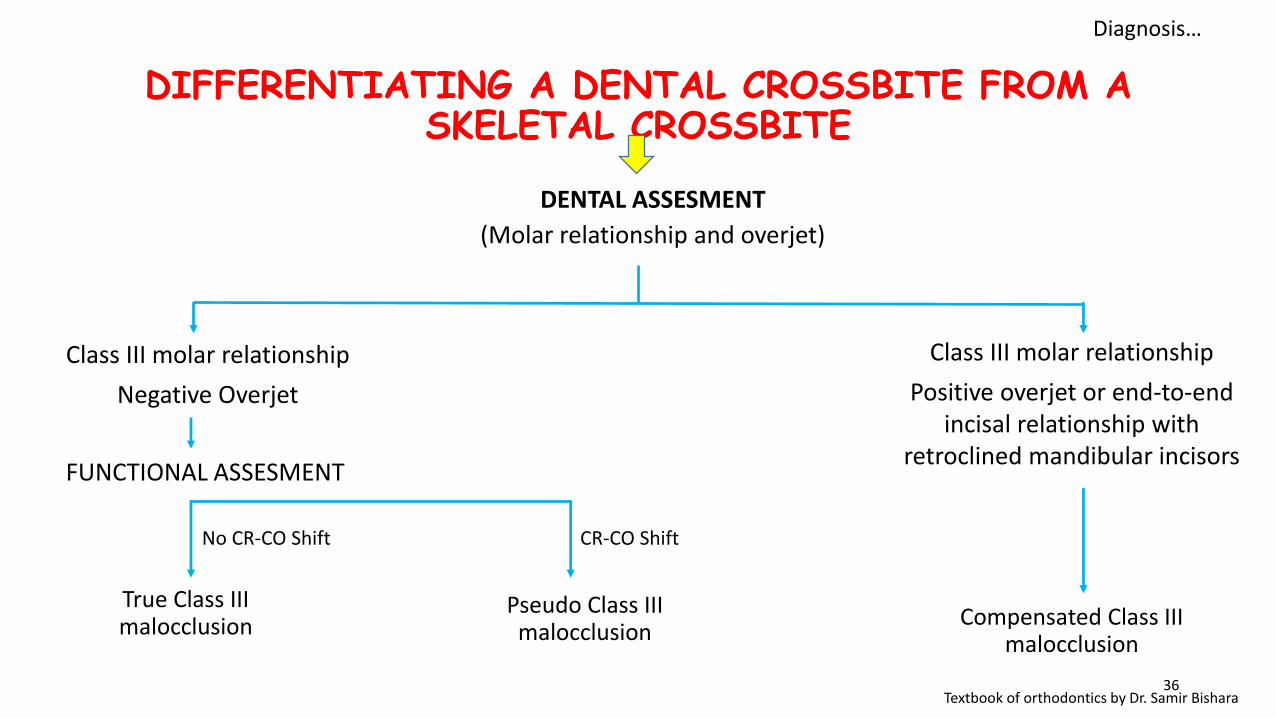
DIFFERENTIATING A DENTAL CROSSBITE FROM A SKELETAL CROSSBITE
36
DENTAL ASSESMENT
(Molar relationship and overjet)
Class III molar relationship
Positive overjet or end-to-end incisal relationship with
retroclined mandibular incisors
Class III molar relationship
Negative Overjet
FUNCTIONAL ASSESMENT
Compensated Class III malocclusion
Pseudo Class III malocclusion
True Class III malocclusion
CR-CO ShiftNo CR-CO Shift
Textbook of orthodontics by Dr. Samir Bishara
Diagnosis…
TREATMENT OF PSEUDO CLASS III
Removal of CO-CR discrepancy – avoid normal wear and
traumatic occlusal forces to affect the teeth
Removes potential adverse effects on growth of jaws
Establishes good functional occlusal
Improves facial aesthetics
37
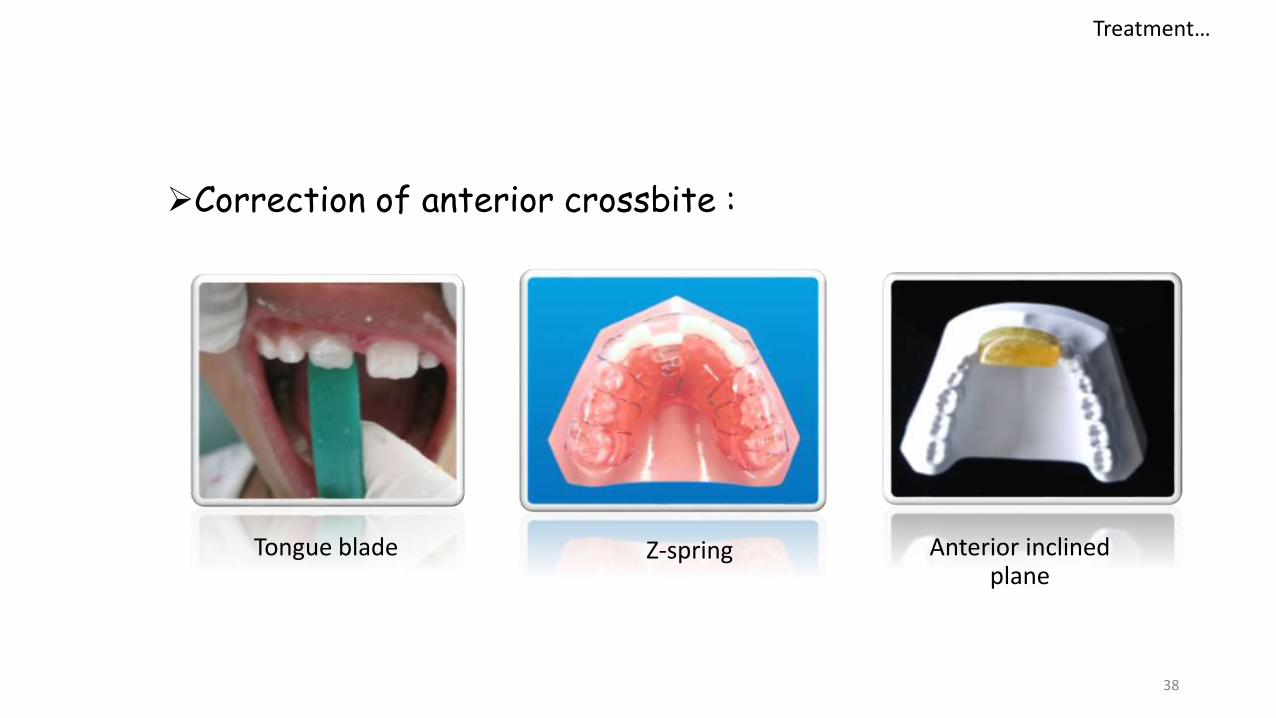
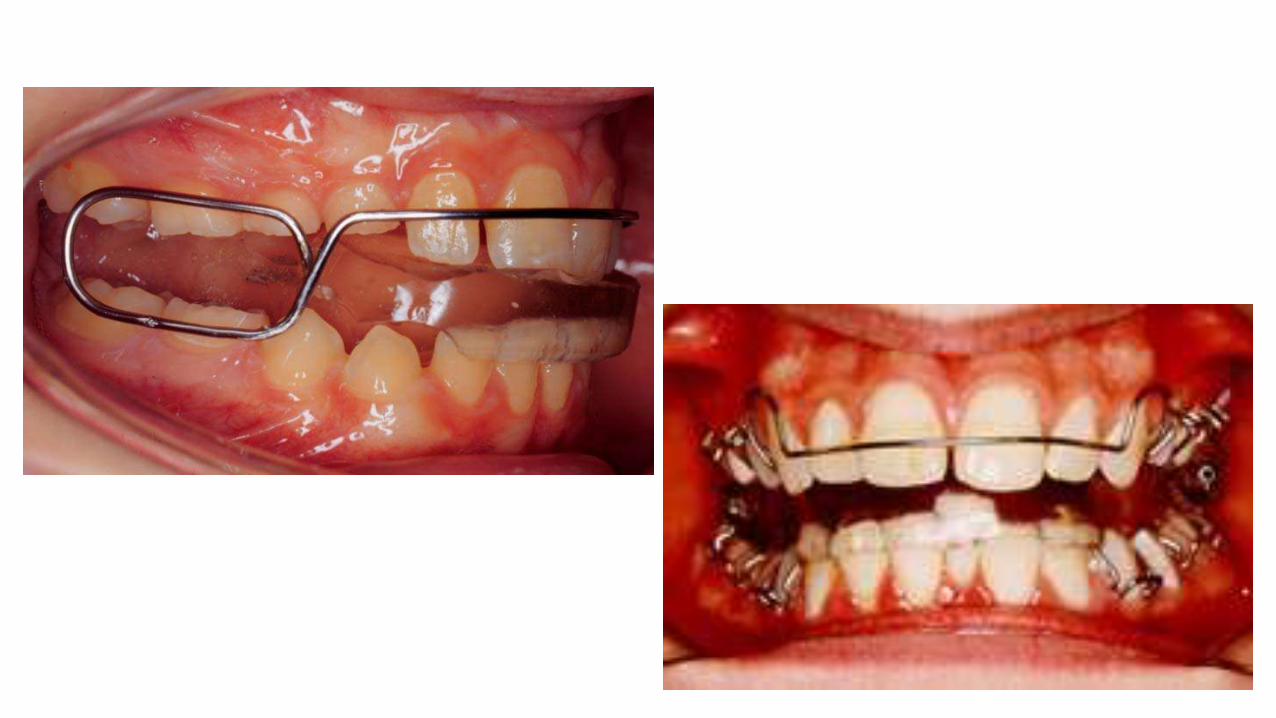
Correction of anterior crossbite :
38
Tongue blade Anterior inclined plane
Z-spring
Treatment…
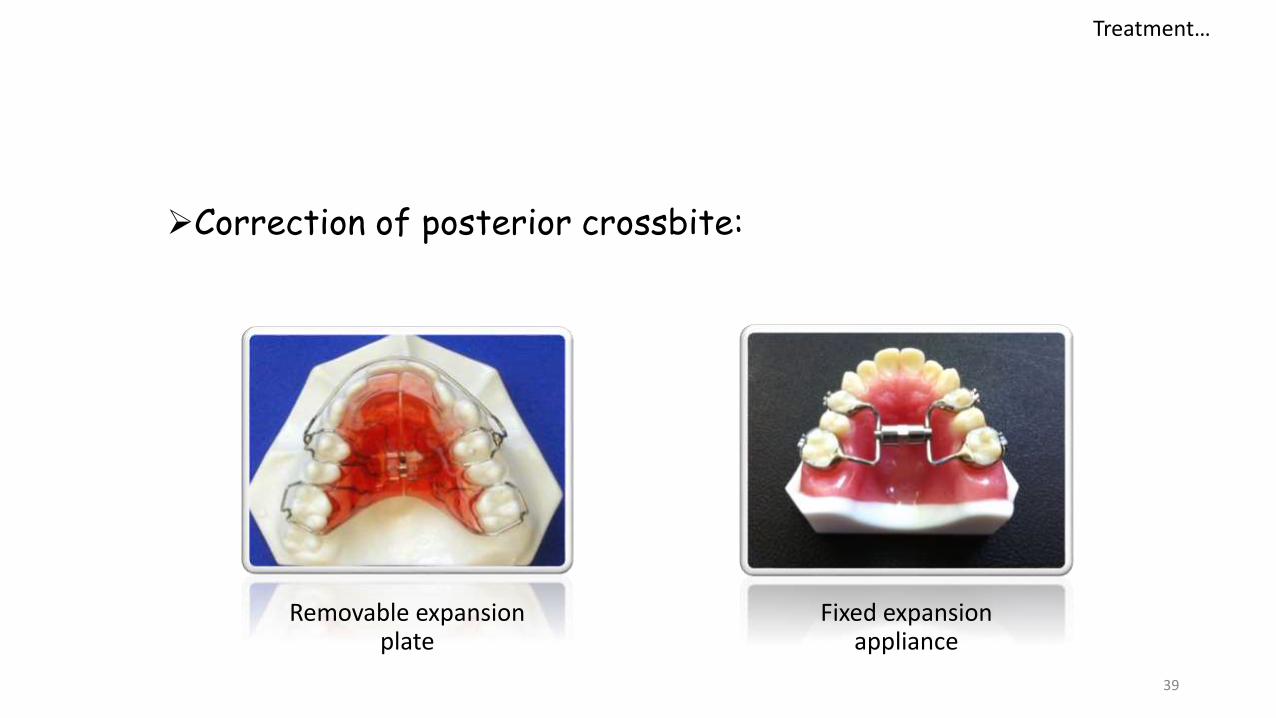
Correction of posterior crossbite:
39
Removable expansion plate
Fixed expansion appliance
Treatment…
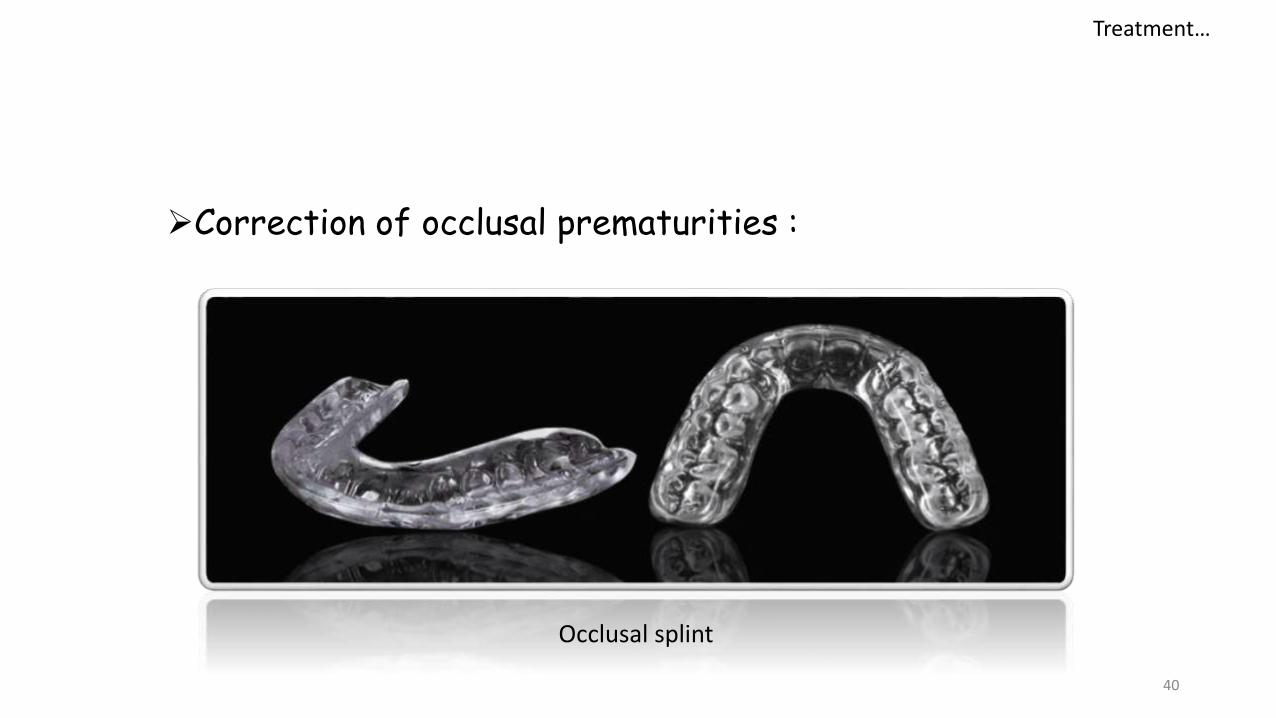
Correction of occlusal prematurities :
40
Occlusal splint
Treatment…
TREATMENT OF TRUE CLASS III
Why should the treatment be started early ?
Facilitates the eruption of canines and premolars in a normal relation
Eliminates the traumatic occlusion of incisors
Provides an adequate maxillary growth
Improves the self esteem of the child
41
42
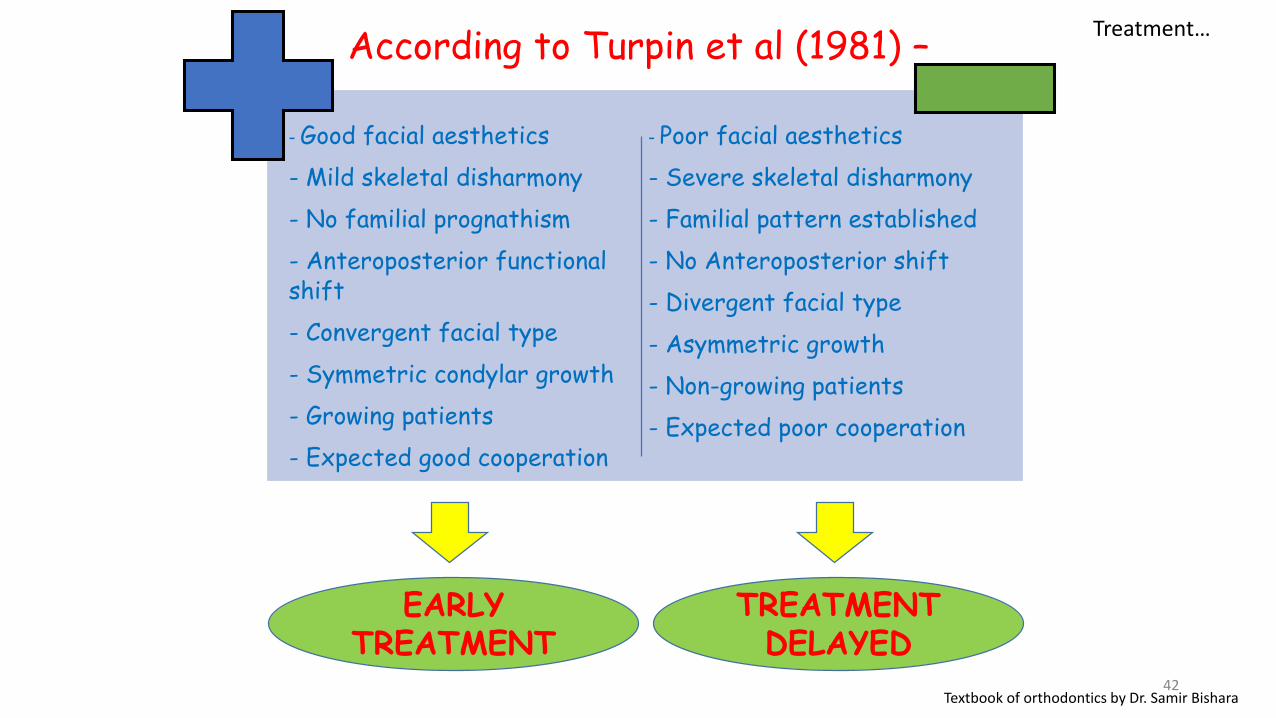
According to Turpin et al (1981) –
- Good facial aesthetics
- Mild skeletal disharmony
- No familial prognathism
- Anteroposterior functional shift
- Convergent facial type
- Symmetric condylar growth
- Growing patients
- Expected good cooperation
- Poor facial aesthetics
- Severe skeletal disharmony
- Familial pattern established
- No Anteroposterior shift
- Divergent facial type
- Asymmetric growth
- Non-growing patients
- Expected poor cooperation
EARLY TREATMENT
TREATMENT DELAYED
Textbook of orthodontics by Dr. Samir Bishara
Treatment…
43
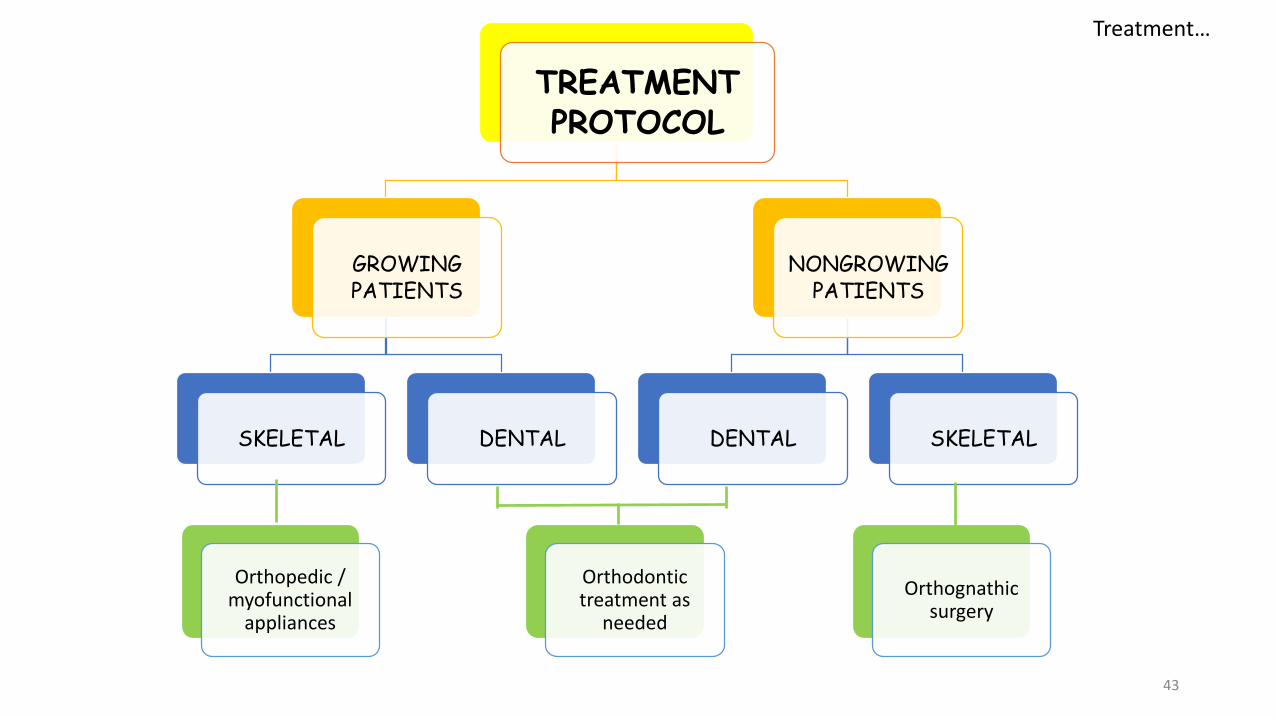
TREATMENT PROTOCOL
GROWING PATIENTS
SKELETAL DENTAL
NONGROWING PATIENTS
DENTAL SKELETAL
Orthopedic / myofunctional
appliances
Orthognathic surgery
Orthodontic treatment as
needed
Treatment…
1. REVERSE ACTIVATOR
44
Treatment…
*Removable orthodontic appliances by Graber and Neuman: 2nd Edition
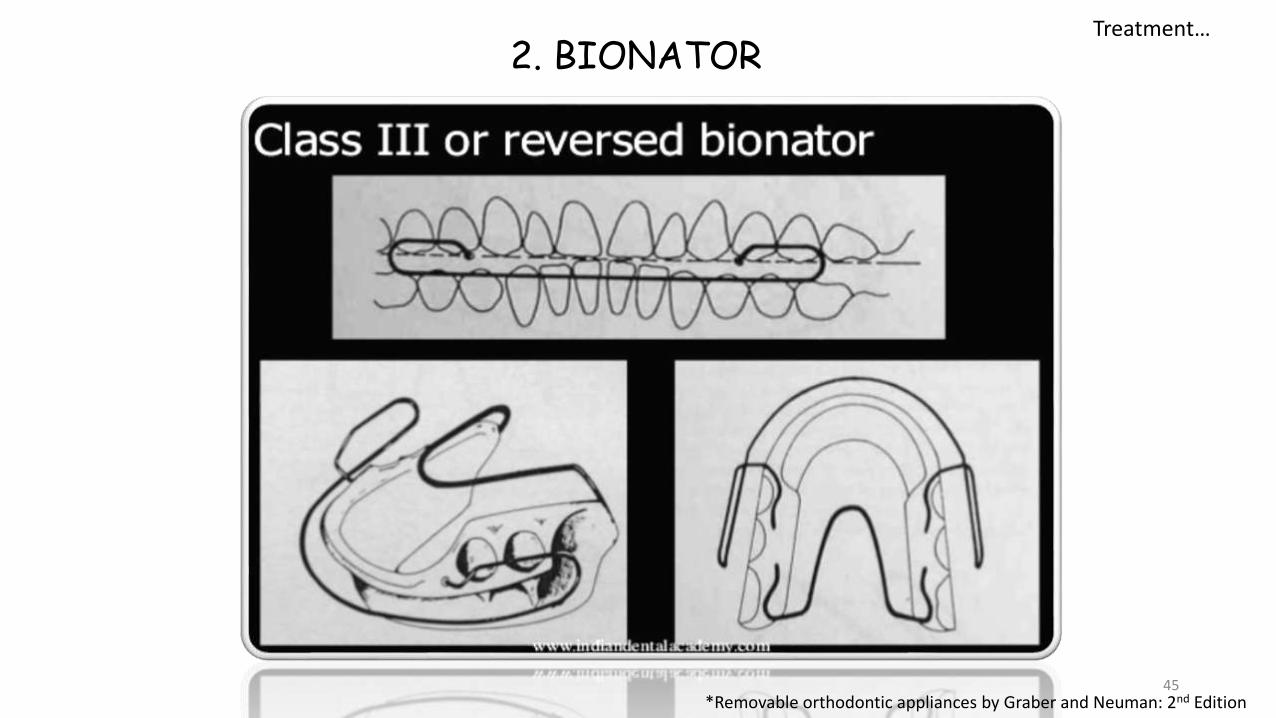
2. BIONATOR
45*Removable orthodontic appliances by Graber and Neuman: 2nd Edition
Treatment…
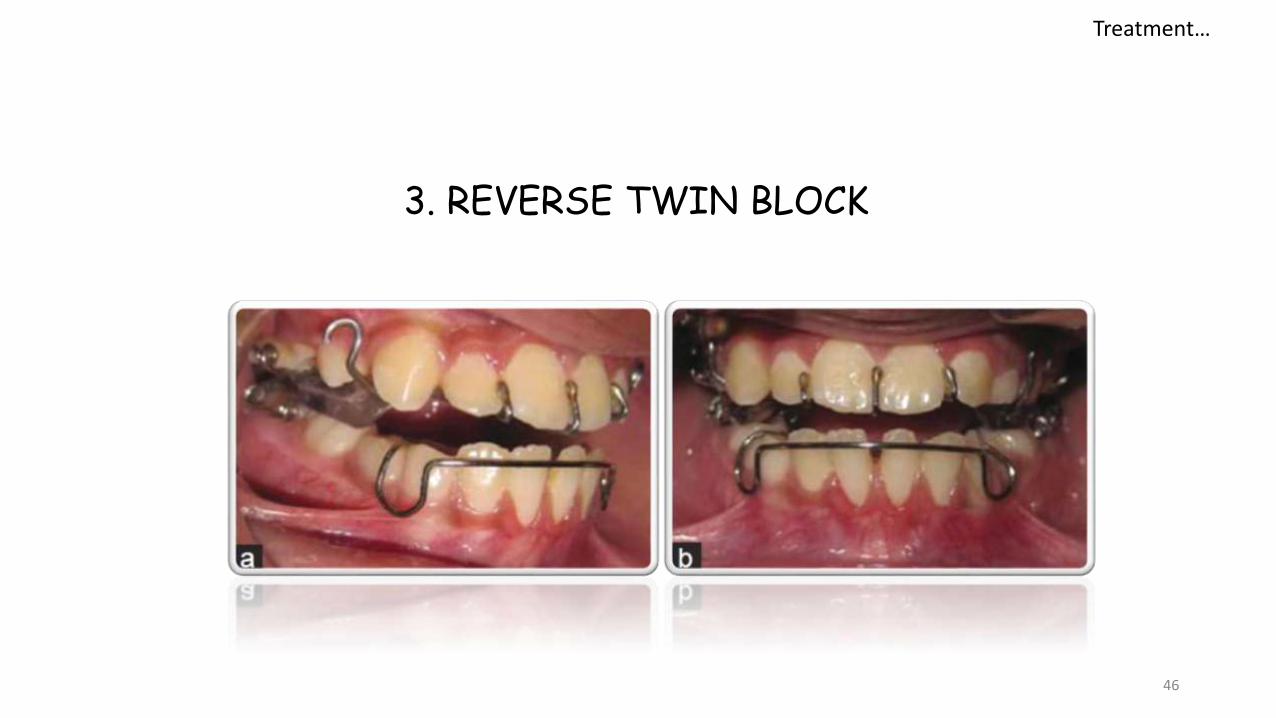
3. REVERSE TWIN BLOCK
46
Treatment…
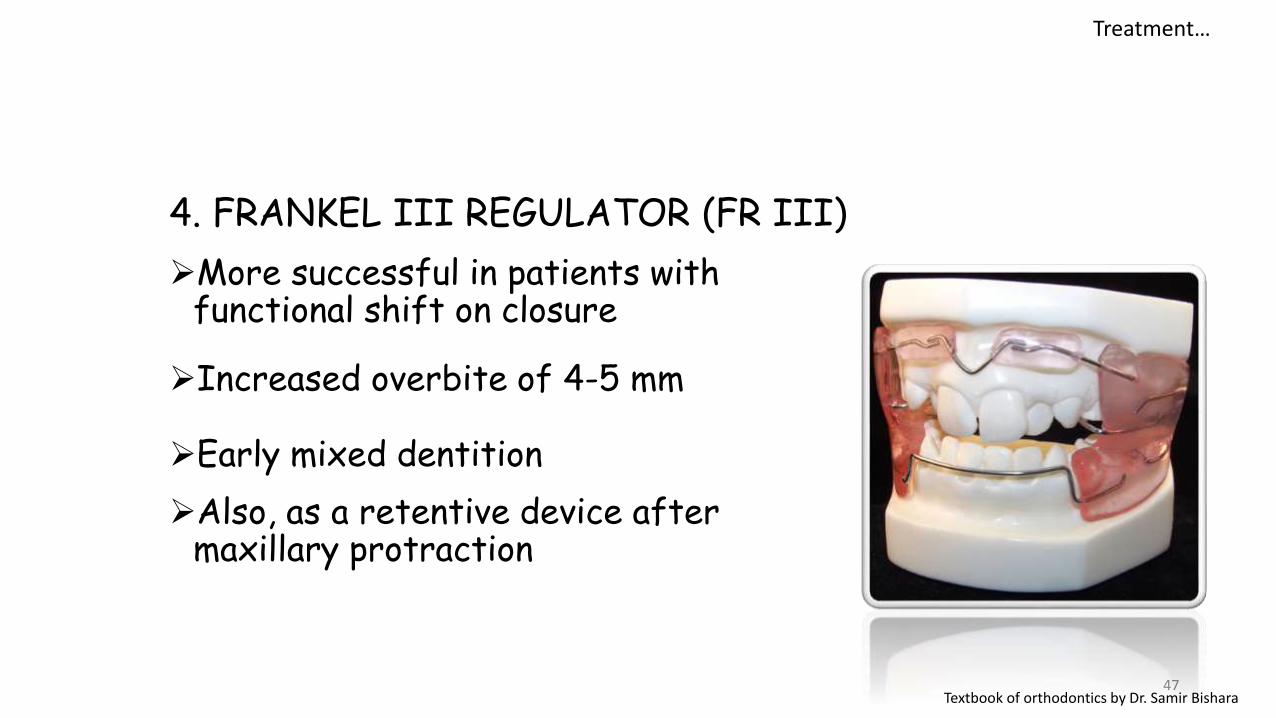
4. FRANKEL III REGULATOR (FR III)
More successful in patients with functional shift on closure
Increased overbite of 4-5 mm
Early mixed dentition
Also, as a retentive device after maxillary protraction
47Textbook of orthodontics by Dr. Samir Bishara
Treatment…
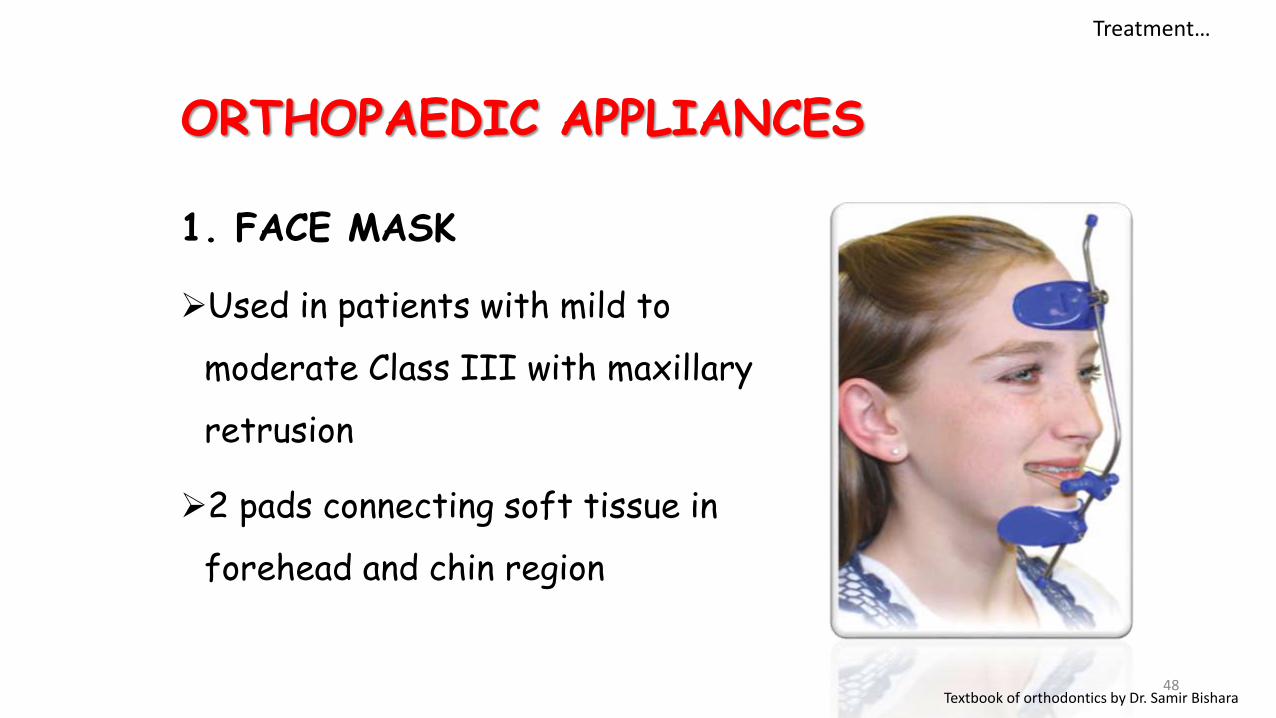
1. FACE MASK
Used in patients with mild to
moderate Class III with maxillary
retrusion
2 pads connecting soft tissue in
forehead and chin region
48
ORTHOPAEDIC APPLIANCES
Treatment…
Textbook of orthodontics by Dr. Samir Bishara
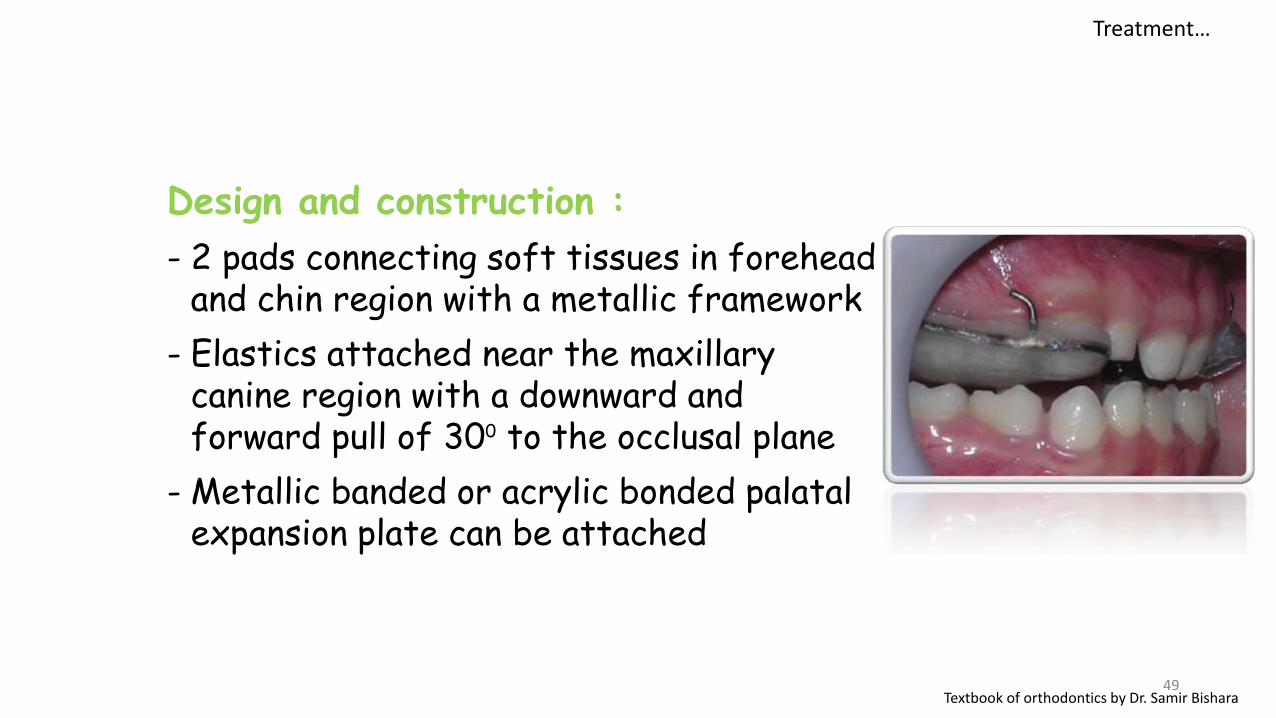
Design and construction :
- 2 pads connecting soft tissues in forehead and chin region with a metallic framework
- Elastics attached near the maxillary canine region with a downward and forward pull of 300 to the occlusal plane
- Metallic banded or acrylic bonded palatal expansion plate can be attached
49
Treatment…
Textbook of orthodontics by Dr. Samir Bishara
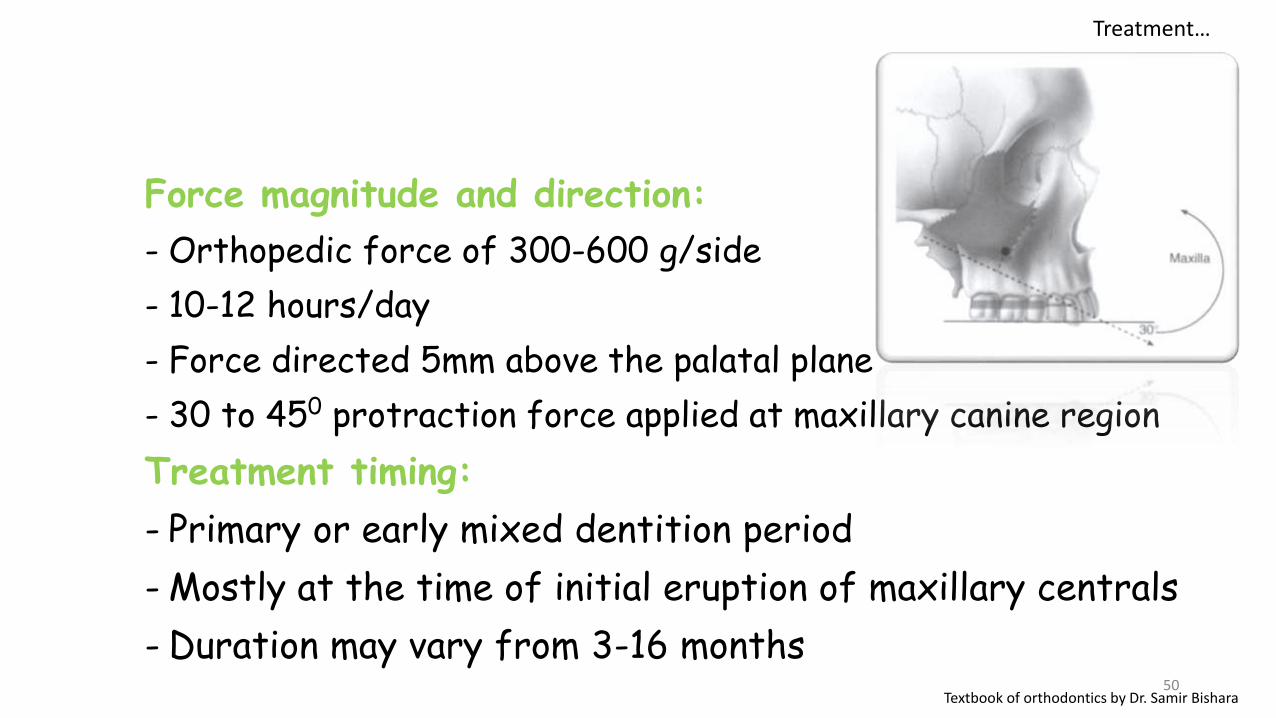
Force magnitude and direction:
- Orthopedic force of 300-600 g/side
- 10-12 hours/day
- Force directed 5mm above the palatal plane
- 30 to 450 protraction force applied at maxillary canine region
Treatment timing:
- Primary or early mixed dentition period
- Mostly at the time of initial eruption of maxillary centrals
- Duration may vary from 3-16 months50
Treatment…
Textbook of orthodontics by Dr. Samir Bishara
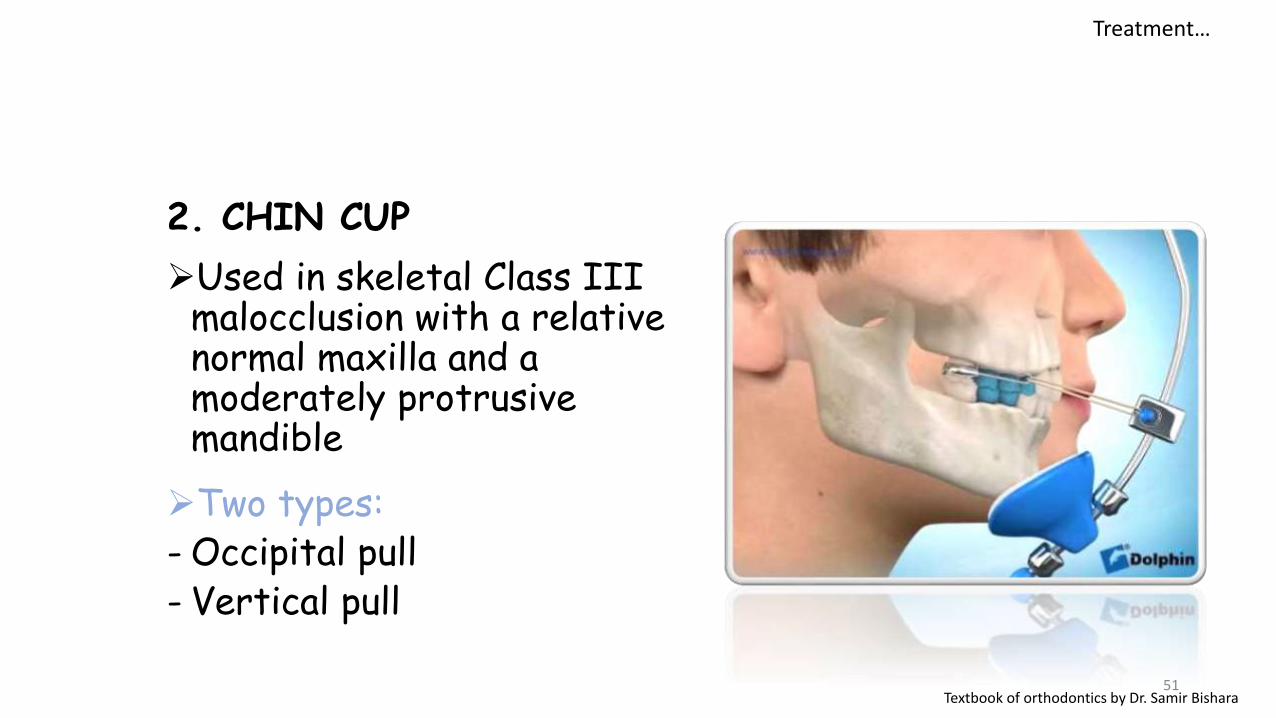
2. CHIN CUP
Used in skeletal Class III malocclusion with a relative normal maxilla and a moderately protrusive mandible
Two types:- Occipital pull- Vertical pull
51Textbook of orthodontics by Dr. Samir Bishara
Treatment…
Effects on growth:
A) Mandible- Redirection of mandibular growth vertically
- Backward repositioning or rotation
- Remodeling with closure of gonial angle
- Posterior movement of Point B and Pogonion
52Textbook of orthodontics by Dr. Samir Bishara
Treatment…
Force magnitude and direction:
- Orthopedic force of 300-500 g per side
- 14 hours/day
- Directed usually through condyle or below the condyle
Treatment timing:
- Primary or early mixed dentition
- Treatment time varies from 1 year to 4 year depending on severity
53Textbook of orthodontics by Dr. Samir Bishara
Treatment…
ORTHODONTIC CAMOFLAGE
Indications :
Skeletal discrepancies not resolved during mixed dentition
Malocclusions recurring during adolescence after treatment in childhood
Mild mandibular prognathism and moderate crowding
Types :
With extractions
Without extractions
54
Treatment…
Textbook of orthodontics by Dr. Samir Bishara
Depending on the malocclusion extraction can be done as follows:
Two lower premolars or a mandibular incisor
All four premolars
Maxillary 2nd and mandibular 1st premolars
Mandibular second molars
55Textbook of orthodontics by Dr. Samir Bishara
Treatment…
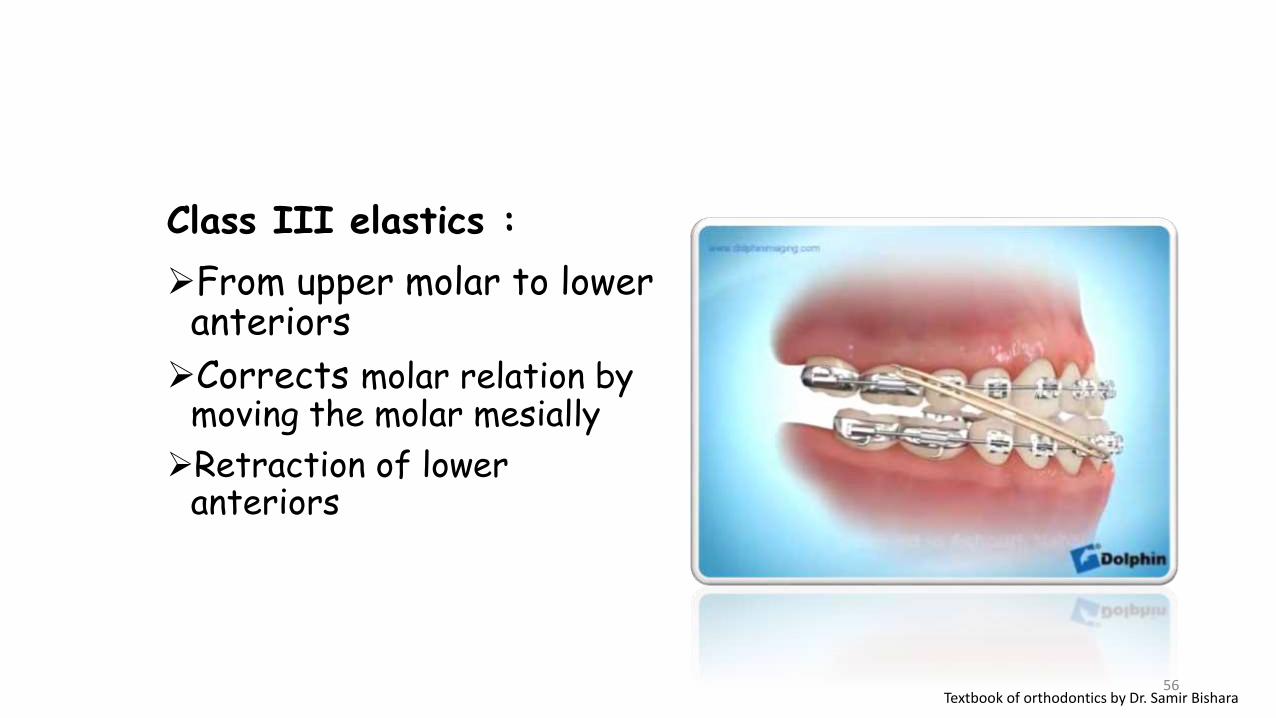
Class III elastics :
From upper molar to lower anteriors
Corrects molar relation by moving the molar mesially
Retraction of lower anteriors
56Textbook of orthodontics by Dr. Samir Bishara
ORTHOGNATHIC SURGERY
Indications :Continued disproportionate sagittal and vertical growth
Severe skeletal maxillary retrusion and mandibular prognathism or both
Non-growing patients
Cleft lip and palate
Facial asymmetries
57
Treatment…
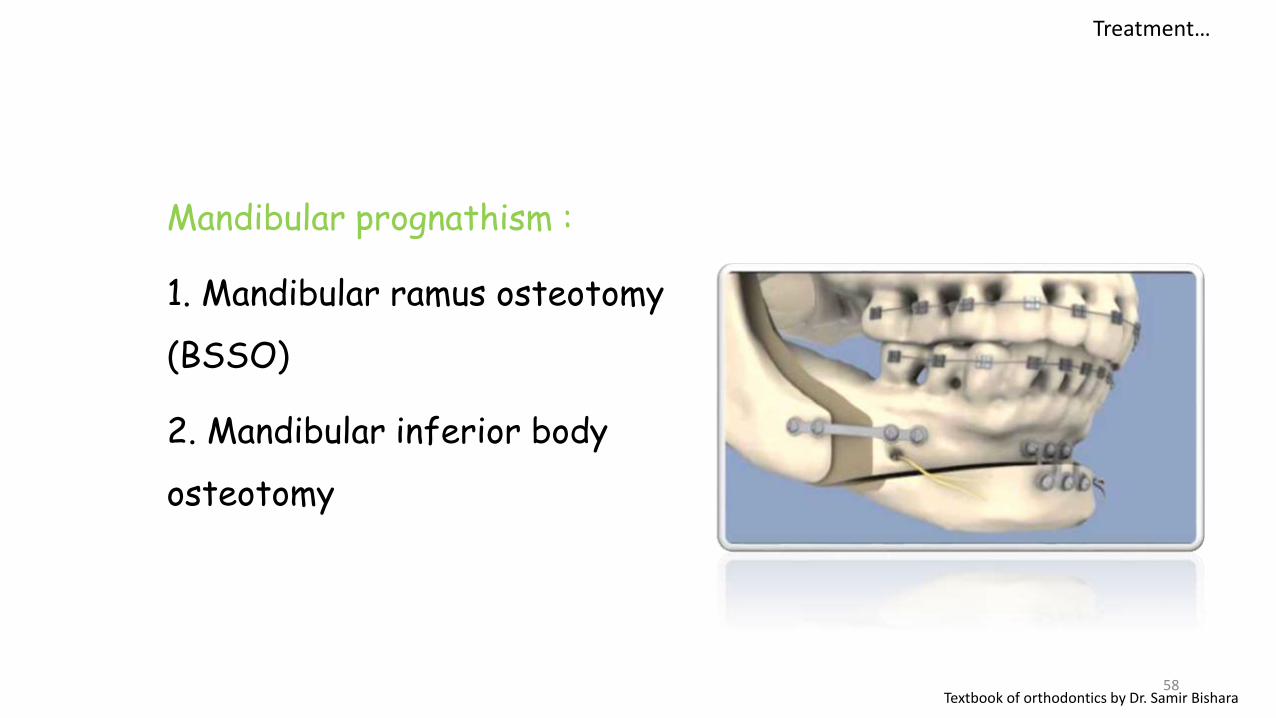
Mandibular prognathism :
1. Mandibular ramus osteotomy
(BSSO)
2. Mandibular inferior body
osteotomy
58Textbook of orthodontics by Dr. Samir Bishara
Treatment…
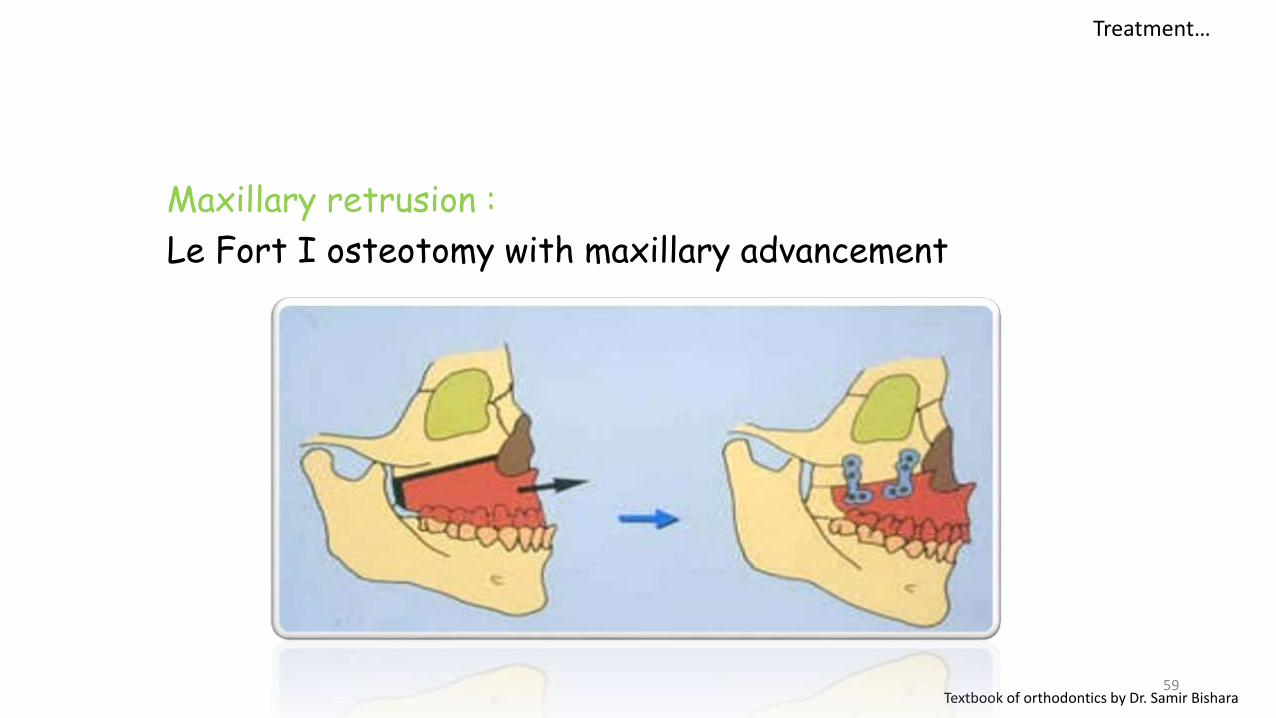
Maxillary retrusion :
Le Fort I osteotomy with maxillary advancement
59Textbook of orthodontics by Dr. Samir Bishara
Treatment…
THANK YOU
60