class iii malocclusion by sooraj s pillai
TRANSCRIPT


CONTENTS
INTRODUCTION
DEFINITION
ETIOLOGY
FREQUENCY
CLASSIFICATION
CLINICAL EXAMINATION
GROWTH COSIDERATION
GOALS OF EARLY INTERCEPTIVE TREATMENT
TREATMENT OF PSEUDO CLASS III MALOCCLUSION
TREATMENT OF SKELETAL CLASS III MALOCCLUSION
CONCLUSION
REFERENCE

INTRODUCTION
Orthodontic treatment not only involves
establishment of physiologically and
anatomically functional occlusion but also
includes correction of the relationship of the
maxilla and mandible to each other and to the
rest of the craniofacial complex.
DEFINITION
According to Angle (1899): Class III
malocclusion occurred when the lower
teeth occluded mesial to their normal
relationship by the width of one premolar
or even more in extreme cases. (mesio-
occlusion)

ETIOLOGY
GENITIC
McGuigan (1966) – Inheritance of class III
malocclusion in Hapsburg Family, having
the distinct characteristics of prognathic
lower jaw.
Litton et al (1970) – Dental characteristics
of class III are related to genetic
inheritance.

Rakosi & Schilli (1981) environmental factors: Habits and mouth Breathing
Enlarged tonsils and naso-respiratory diseases.
Premature loss of deciduous molars:Results in anterior mandibular displacement.
TERATOGENS:
Cleft lip and palate result in maxillary deficiency in most occasions a
class III malocclusion is established. Teratogens causing cleft lip and
palate are aspirin, cigarette smoke (hypoxia), Dilantin, 6-
Mercaptopurine, valium etc
Vitamin D excess causes premature closure of sutures and
might lead to class III malocclusion

ACROMEGALY AND HEMI MANDIBULAR
HYPERTROPHY:
FREQUENCY
Caucasians - 1 to 4 %
African – Americans - 5 to 8%
Asians:
Japanese: 4 % younger / 14 % older
Chinese: 3 % younger / 13 % older
Indians: 1.3% (J Ind. Ped & Prev Dent: 1998 – Uteraja et
al)
Iranian: 2.1% (East Mediters Health J: 2006: Danaie et al)

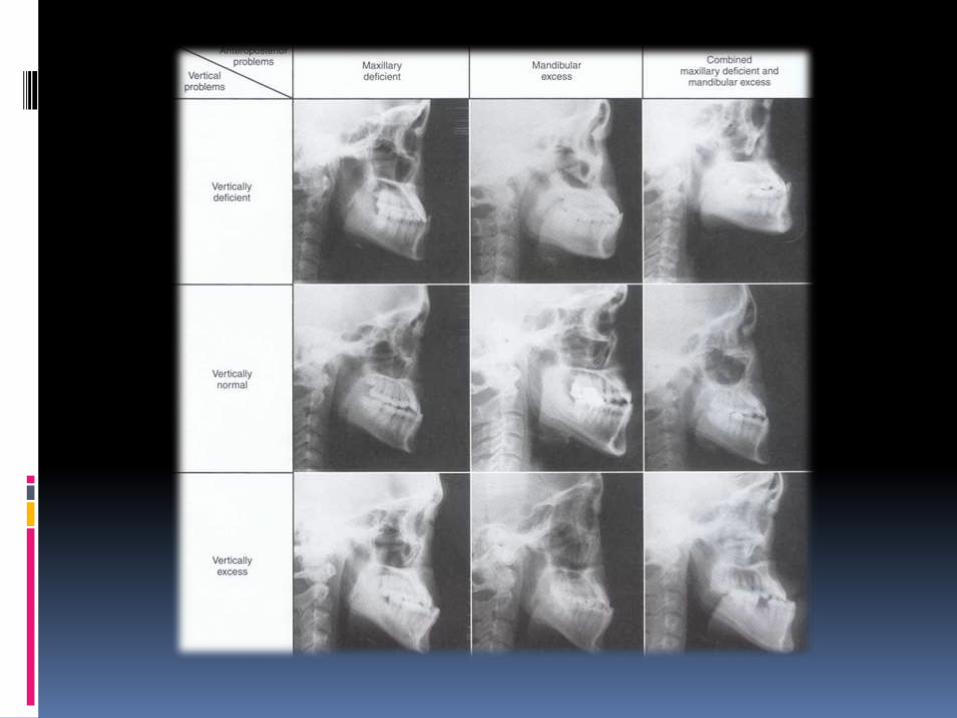
CLASSIFICATION
Generally of 2 types:
Dentoalveolar
Skeletal
Mandibular protrusion
Maxillary retrusion
Combination

PSEDUO CLASS III
Malocclusion is produced by a forward movement of
mandible during jaw closure.
Also known as habitual or postural class III malocclusion.

Angles classification
The mesio – buccal cusp of the maxillary first
permanent molar occluding in the inter dental space
between the mandibular first and second molars.

Class III Modification of Dewey

MOYERS CLASSIFICATION
ACCORDING TO THE CAUSE
OSSEOUS
MASCULAR
DENTAL

CLINICAL EXAMINATION
EXRAORAL FEATURES:
A CONCAVE FACE,DEFICIENT MAXILLA OR PROMINENT CHIN.
MALAR DEFICIENCY RESULTING INTO FLAT FACE
INCREASED LOWER ANTERIOR FACIAL HEIGHT
ANATOMICALLY LARGE LOWER LIP LENGTH

INTRAORAL FEATURES
ZERO OR –VE OVERJET
NARROW MAXILLARY ARCH WITH CROWDING
UNILATERAL OR BILATERAL POSTERIOR CROSSBITE
PROCLINED MAXILLARY INCISORS
RETROCLINED MANDIBULAR INCISORS
LOW TONGE POSTURE
FLAT CURVE OF SPEE.

GROWTH COSIDERATIONS
Sugawara and Mitani :Reported similar increments
between patients with Class III and Class I malocclusions
during the prepubertal pubertal and postpubertal growth
periods.
Battagel :found that the largest increment of facial
growth for males occurred between the ages of 14 and 16
years.
whereas in female patients the maximum increment of
facial growth occurred between the ages of 9.5 to12 years,
although active growth continued in the nasal area and
both jaws after the age of 15 years.

Goals of early interceptive treatment
(1) preventing progressive, irreversible soft tissue, or
bony changes.
(2) improving skeletal discrepancies and providing a more
favourable environment for future growth.
(3) improving occlusal function;
(4) simplifying phase II comprehensive treatment
and minimizing the need for orthognathic surgery
(5) providing more pleasing facial esthetics
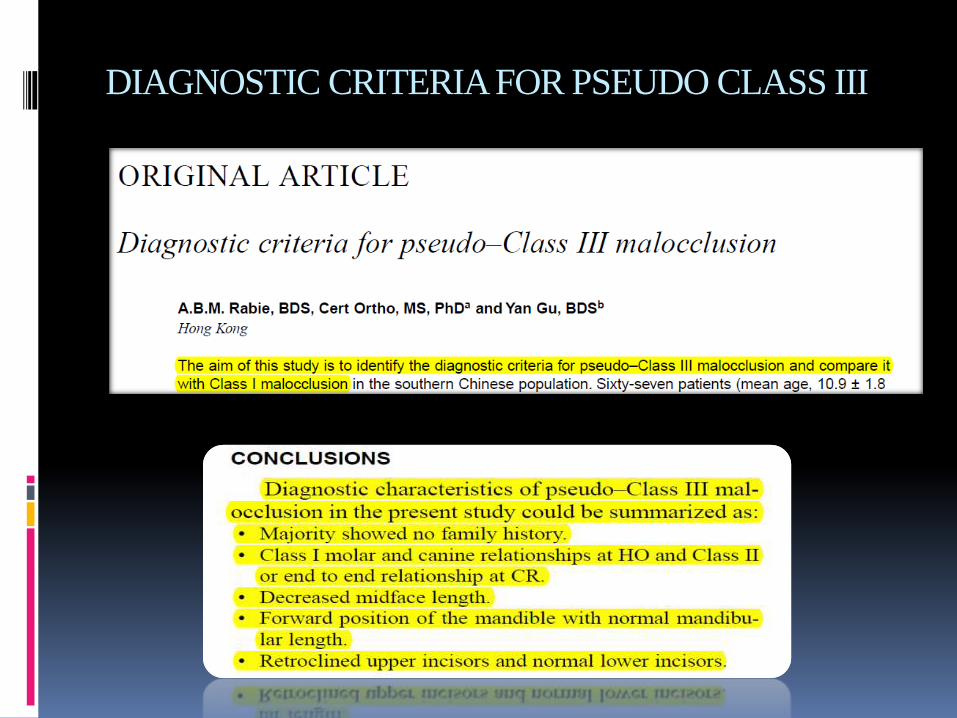
DIAGNOSTIC CRITERIA FOR PSEUDO CLASS III

TREATMENT OF PSEUDO CLASS III
MALOCCLUSION
Elimination of the CO-CR discrepancy.
REVERSE STAINLESS STEEL CROWNS.
TONGUE BLADE

INCLINED PLANES.
AUXILLARY SPRINGS

TREATMENT OF SKELETAL CLASS III MAL OCCLUSION.
FUNCTIONAL APPLIANCE THERAPY
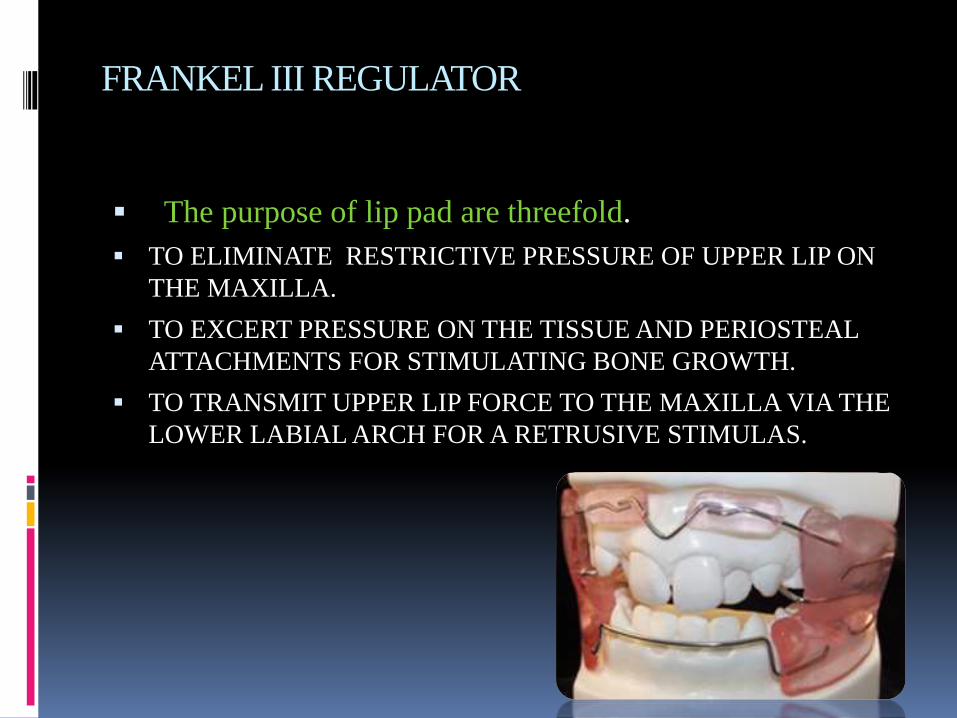
FRANKEL III REGULATOR
The purpose of lip pad are threefold.
TO ELIMINATE RESTRICTIVE PRESSURE OF UPPER LIP ON
THE MAXILLA.
TO EXCERT PRESSURE ON THE TISSUE AND PERIOSTEAL
ATTACHMENTS FOR STIMULATING BONE GROWTH.
TO TRANSMIT UPPER LIP FORCE TO THE MAXILLA VIA THE
LOWER LABIAL ARCH FOR A RETRUSIVE STIMULAS.

The FRIII appliance can also be used as a retentive device
following maxillary protraction treatment.
FRIII appliance was constructed to maintain the antero-
posterior and transverse corrections until the maxillary
incisors were fully erupted with sufficient overbite to
maintain the Class III correction.

CLASS III OR REVERSED BIONATOR.
Encourage development of maxilla Bite opened
2mm for this purpose
Acrylic portion Extends incisally from canine to
canine behind the upper incisors
Acrylic is trimmed away by 1mm behind the
lower incisors to prevent the tipping

Palatal bar
Runs forward with loop extending as far as
dec 1st m or premolar
Function – tongue to contact anterior portion
of palate , encouraging forward growth of this
area.

Labial bow
In front of lower incisors
Wire slightly touches the labial surface lightly / it is at a
paper thickness away

Construction bite
Construction bite- taken in more retruded position so as to
allow labial movement of maxillary incisors &also to
exert restrictive force on lower arch.

CHIN CUP
Skeletal Class III malocclusion with a relatively normal
maxilla and a moderately protrusive mandible can be
treated with the use of a chin cup.
The objective of early treatment with the use of a chin cup
is to provide growth inhibition or redirection and
posterior positioning of the mandible.

Effects on Mandibular Growth
Redirection of mandibular growth vertically.
Backward repositioning (rotation) of the
mandible.
Remodelling of the mandible with closure of the
gonial angle

EFFECT ON MAXILLA
Uner,Yuksel,and Ucuncu (Eur J Orthod 17:135-141, 1995)
Showed that early correction of an anterior crossbite with
a chin cup appliance prevents retardation of antero-
posterior maxillary growth.
Sugawara et a1 (Am JOrthod Dentofacial Orthop 98:127-133, 1990.)
Compared the growth changes of patients after chin cup
treatment with control subjects and reported that, at age
17, the midface is more deficient in patients of the control
groups than in those of the treatment groups.

Force Magnitude.
CHIN CUP 2 TYPES
OCCIPITAL PULL CHIN CUP.
VERTICAL PULL CHIN CUP.
300-500g PER SIDE
14hr/day

PROTRACTION FACE MASK THERAPY
Extraoral appliance that utilizes rests on the
chin and forehead(and occasionally the cheek
bones) as anchorage for elastic traction, with
the purpose of orthopaedically protracting the
maxilla.
Glossary of Orthodontic Terms

The use of a protraction face mask was first
described more than 100yrs ago in 1875 by
Johnson et al.
1944, Oppenheim: reported that it is impossible
to move the mandible backward, but that it is
possible to bring the maxilla forward to
compensate for mandibular overgrowth when
treating Class III malocclusions.

Although the facial mask was developed over 100
years ago, this approach was used infrequently
until reintroduced by Delaire in early 1970’s
Petit 1983: modified the basic concept of Delaire
by increasing the amount of force generated by
the appliance and decreasing the total treatment
time

1987 McNamara: introduced the use of a
bonded expansion appliance with acrylic
occlusal coverage for maxillary protraction.

ANATOMICAL CONSIDERATIONS
Circum-maxillary Sutures
A. Frontomaxillary
B. Nasomaxillary
C. Zygomaticomaxillary
D. Zygomaticotemporal
E. Pterygopalatine
F. Intermaxillary
G. Ethmomaxillary
H. Lacrimomaxillary

Melsen 1975 AJOProffit 5th Edition

BIOMECHANICAL CONSIDERATION
The orthodontist must first decide, whether to protract with a clockwise moment on the maxilla, a counter clockwise moment, or no moment
.
If the patient has normal overbite and normal vertical proportions, protraction without any moment is indicated.
If the patient has an anterior open bite in addition to the maxillary deficiency, a clockwise moment should be used.
If the patient has a deep bite, a counter clockwise momentshould be chosen.
Staggers JCO 1992

FACE MASK COMPONENTS
Forehead Piece
Main Frame
Protraction Bar
Chin Cup

Centre of Resistance of Maxilla
The center of resistance of the maxilla was found to be located at the
distal contacts of the maxillary first molars one half the distance from
the functional occlusal plane to the inferior border of the orbit.

Magnitude of Force
The sutural anatomy and age of the patient play a major role in
determining the amount of force needed to bring the maxilla forward
with the protraction forces.
Preadolescent patient (5-8yr) – 200-250gm
Early adolescent patient (8-11yr) – 300-350gm
Late adolesent patient (12yr and above) – 450-600gm
Bishara

Duration of Force
Most of the studies done recommend a minimum of
10-12 hours/day preadolescents
12-16 hours/day adolescents
McNamara Brudon

Treatment Timing
Takada et al EJO 1993 : Reported that face mask treatment is most
effective in prepubertal patients (mean age, 7.8 years) and pubertal
patients (mean age, 10.3 years) and becomes less effective after late
puberty.
Baccetti 1998: Showed that treatment of class III malocclusion with
bonded maxillary expander and face mask in the early mixed dentition
results in a more favourable craniofacial changes than treatment in
late mixed dentition

Turley 1998 AJODO: Cephalometric effects of face
mask/expansion therapy in Class III children: a
comparison of three age groups (4-7 years, 7-10 years, 10-
14 years)Most effective in younger age groups but
significant change in older groups too.
Franchi AJODO2004: it was shown that significant
maxillary advancement could be achieved orthopedically
only by treating Class III patients during the deciduous or
early mixed dentition phases.

DESIGNS
Delaire mask was popularized to protract
the maxilla in 1978
In this appliance design,
Extraoral anchorage regions were the chin
and forehead.

The intraoral part of the appliance was
constructed with 1 mm stainless steel
arches (buccal and lingual) soldered to
the upper molar bands, which were
cemented to the anchor teeth (1st
permanent or 2nd deciduous molars).
McNamara Brudon

The protraction elastics were attached
between theanterior hooks (facing the
distal side of the lateral incisors) soldered
on the intraoral arch, with the hooks on the
Pre labial arch of the mask placed at the
level of the labial commissural line.
To avoid an opening of the bite, the force,
which delivers about 400 g of force on
each side was directed downward about
20° to25° to the occlusal plane.
Delaire 1971

Petit Face Mask 1983
The Petit facial mask was originally
constructed on a patient-by-patient
basis, using .25" round lengths of
stainless steel, to which pads for the
forehead and chin were attached

video

CLASS III CAMOUFLAGE TREATMENT
Treatment approach were the underlying skeletal
deformity is left untreated but teeth are moved to such
positions to create an acceptable occlusion with out
violating the norms of aesthetics and stability is
categorised as camouflage treatment.

Treatment approaches
2 Approaches.
NON EXTRACTION
EXTRACTION
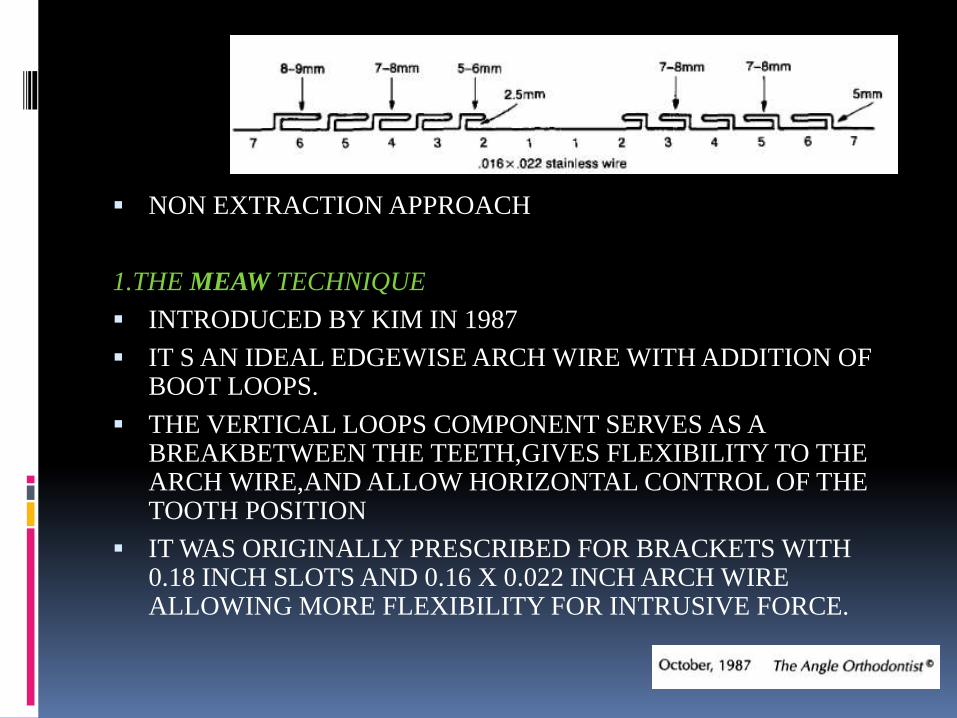
NON EXTRACTION APPROACH
1.THE MEAW TECHNIQUE
INTRODUCED BY KIM IN 1987
IT S AN IDEAL EDGEWISE ARCH WIRE WITH ADDITION OF BOOT LOOPS.
THE VERTICAL LOOPS COMPONENT SERVES AS A BREAKBETWEEN THE TEETH,GIVES FLEXIBILITY TO THE ARCH WIRE,AND ALLOW HORIZONTAL CONTROL OF THE TOOTH POSITION
IT WAS ORIGINALLY PRESCRIBED FOR BRACKETS WITH 0.18 INCH SLOTS AND 0.16 X 0.022 INCH ARCH WIRE ALLOWING MORE FLEXIBILITY FOR INTRUSIVE FORCE.

USE OF DISTALIZATION OF LOWER ARCH USING
ANCHORAGE DERIVED FROM MINI IMPLANT
THE TADS HAVE PROVED USEFUL IN PROVIDING ANCHORAGE
REQUIRED TO DISTALIZE THE WHOLE MANDIBULAR ARCH
INCLUDING SECOND MOLAR.
THE PRESENCE OF THIRD MOLARWILL HAVE TO BE EVALUATED
AND IF NEEDED BE,IT MAY REQUIRE SURGICAL CORRECTION.

EXTRACTION APPROACH.
DEPENDING ON THE REQUIREMENT OF THE CASE
EXTRACTION CHOICES COULD BE.
MANDIBULAR INCISOR
UPPER SECOND AND LOWER FIRST BICUSPIDS
LOWER FIRST BICUSPIDS
MANDIBULAR SECOND MOLARS

MANDIBULAR INCISOR EXRACTION
SITUATIONS WHERE CROWDING IS NOT LARGE OR
SITUATIONS OF BOLTONS DICCREPANCY.
UPPER/LOWER MIDLINE MISMATCH
LONGTERM RIGID LINGUAL RETAINER AS MANDIBULAR
ARCH WITH THREE INCISORS HAS A TENDENCY FOR
LINGUAL COLLAPSE.

UPPER SECOND AND LOWER FIRST BICUSPIDS.
TO RESOLVE LARGE MANDIBULAR CROWDING,AND
INDUSE SIGNIFICANT TIPPING OF MANDIBULAR ARCH.
MAXILLARY ARCH WHICH HAS LESSER CROWDING,
CONSIDERD FOR SECOND PRE MOLAR EXTRACTION.

LOWER FIRST BICUSPIDS
WHEN UPPERARCH IS WELL ALIGNED OR CAN BE WELL ALIGNED WITH DENTAL EXPANSION OF THE ARHES.
LOWER ARCH NEEDS SPACE TO RESOLVE CROWDING AND
LINGUAL TIPPING OF MANDIBULAR INCISORS

MANDIBULAR SECOND MOLARS
FOR SIGNIFICANT DISTALIZATION OF ENTIRE LOWER
DENTAL ARCH
THE LOWER DENTAL ARCH CAN BE DISTALIZED EITHER
WITH CERVICAL HEADGEAR OR ANCHORAGE DERIVED
FROM INTRORAL IMPLANTS.

CONCLUSION
Early orthopedic treatment using face mask or chin cup
therapy improve skeletal relations which in turn minimizes
excessive dental de compensation.
Early treatment provides more pleasing facial profile,
thus improves psyco-social development of child.
It eliminates orthognathic surgery, maximizing growth
potential of maxilla may minimize the extent of surgical
procedures in cases of severe Class III malocclusion.

References
Contemporary orthodontics; william R. profit
Text of orthodontics, samier bishara
In clinical orthodontics, Ravindra nanda
Orthodontics current priciplesand techniques, T.M Graberand
vanarsdal
DENTOFACIAL ORTHOPEDICS WITH FUNCTIONAL APPLIANCES
