long-term osteoporosis therapy - north … osteoporosis therapy what to do after 5 years? ooc...
TRANSCRIPT

Developing a Long-term Management Plan
Long-term Osteoporosis TherapyWhat To Do After 5 Years?
OOCOOC
Michael R. McClung, MD, FACPInstitute for Health and Ageing,
Australian Catholic University, Melbourne, Australia
Oregon Osteoporosis Center
Portland, Oregon, USA
North American Menopause SocietyPhiladelphia, PAOctober 11, 2017
Disclosures
I am disclosing financial relationships as follows:
Scientific Advisory Boards: Amgen, Radius
Honorarium for speaking: Amgen, Radius
OOCOOC
Michael McClung, MD 2017

Osteoporosis
Definition:
A disorder due to bone loss that damages skeletal architecture, weakens the skeleton
and predisposes a patient to fracture
•• Several osteoporosis drugs effectively and Several osteoporosis drugs effectively and
OOCOOC
•• Several osteoporosis drugs effectively and Several osteoporosis drugs effectively and quickly reduce fracture risk in patients with quickly reduce fracture risk in patients with osteoporosisosteoporosis
•• Osteoporosis is a chronic disease requiring Osteoporosis is a chronic disease requiring prolonged treatmentprolonged treatment
•• It is important to develop a strategy for longIt is important to develop a strategy for long--term managementterm management
Images Courtesy of Drs. David Dempster & Roger Zebazi
Black DM and Rosen CJ. N Engl J Med 2016; 374:254-62
Osteoporosis Therapies
OBJECTIVES OBJECTIVES 1,21,2
1.1. improve bone strengthimprove bone strength
2.2. reduce risk of reduce risk of fracturefracture
3.3. prevent rapid bone loss (less commonly)prevent rapid bone loss (less commonly)
OOCOOC
BENEFITS BENEFITS 2
1.1. effective protection from fractureseffective protection from fractures
vertebral fracture by 60vertebral fracture by 60--70%70%
hip fracture by 40hip fracture by 40--50%50%
nonnon--vertebral fracture by 20vertebral fracture by 20--35%35%
2.2. in general are well toleratedin general are well tolerated
3.3. in clinical trials, have in clinical trials, have a favorable safety profilea favorable safety profile
1. 1. SeemanSeeman E et al. Bone 2004;17 E et al. Bone 2004;17 SupplSuppl 2:23S2:23S--29S29S
2. McClung M et al. 2. McClung M et al. AmerAmer J MedJ Med. 2013;126:13. 2013;126:13--2020

Long-term Osteoporosis Therapy
Bisphosphonates and denosumab are the agents considered Bisphosphonates and denosumab are the agents considered for longfor long--term useterm use
Fracture Fracture protection protection
•• begins within months of starting therapybegins within months of starting therapy
•• continues with longcontinues with long--term therapyterm therapy
OOCOOC
•• continues with longcontinues with long--term therapyterm therapy
•• wanes when treatment is wanes when treatment is stoppedstopped
LongLong--term safetyterm safety
•• bisphosphonates: atypical femoral fracture bisphosphonates: atypical femoral fracture
incidence: 1/1000 after 8incidence: 1/1000 after 8--10 years of therapy10 years of therapy
•• denosumabdenosumab
over 10 years, no adverse events increased in frequency with over 10 years, no adverse events increased in frequency with longlong--term therapyterm therapy
1.1. Hanley DA, McClung MR, et al. Hanley DA, McClung MR, et al. Am J Med Am J Med 2017;130:862.e12017;130:862.e1--862.e7862.e7McClung MR et al. McClung MR et al. Am J Med Am J Med 2013;126:132013;126:13--2020
Bone Bone HG et al. HG et al. Lancet Diabetes Lancet Diabetes EndocrinolEndocrinol 2017 2017;5:5132017 2017;5:513--2323

Vertebral Fractures with Zoledronic Acid%
Pati
en
ts
10.9%(310/2853)
70%†(62, 76)
ZOL PBO
10
15P = <0.001
Fracture protection persists with long term therapy
Years 1-3
OOCOOC
3.0%(14/469)
% P
ati
en
ts
Morphometric Vertebral Fractures
3.3%(92/2822)
0
5
Years 4-6
4.4%(3/68)
Years 7-9
Core study Extension study
Black DM et al. N Engl J Med 2007;356:1809–22Black DM et al. J Bone Miner Res 2012;27:243-54
Black DM et al. J Bone Miner Res 2015;30:934-44

Long-term Denosumab TherapyVertebral and Non-vertebral Fractures
Persistent reduction in fracture risk
OOCOOCBone Bone HG et al. HG et al. Lancet Diabetes Lancet Diabetes EndocrinolEndocrinol 2017 2017;5:5132017 2017;5:513--2323

• Hypocalcemia
• Intolerance
• upper GI symptoms: oral drugs
• acute phase reaction: IV drugs
• bone and muscle pain
Risks and Concerns with Long-term TherapyBisphosphonates
No increase with long-term therapy
OOCOOC
• bone and muscle pain
• Inflammatory eye problems
• Atrial fibrillation
• Esophageal cancer: oral drugs
• Osteonecrosis of the jaw
• Atypical fractures
• 1/1000 patients after 8-10 years
Unproven relationship; minimal evidence of
increased risk with long-term therapy
Concern here of risk of long-term therapy
Atypical Femoral Fracture and Long-term Bisphosphonate Therapy
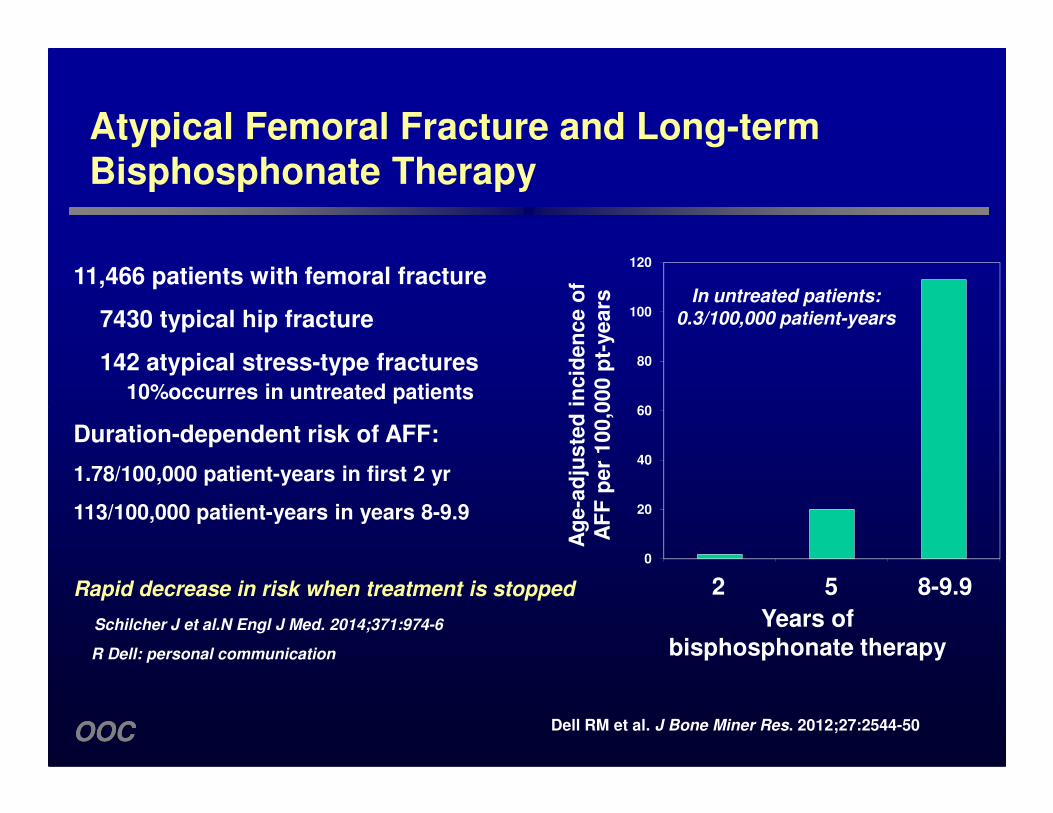
11,466 patients with femoral fracture
7430 typical hip fracture
142 atypical stress-type fractures10%occurres in untreated patients
ad
jus
ted
in
cid
en
ce
of
AF
F p
er
10
0,0
00
pt-
ye
ars
60
80
100
120
In untreated patients: 0.3/100,000 patient-years
OOCOOC Dell RM et al. J Bone Miner Res. 2012;27:2544-50
Duration-dependent risk of AFF:
1.78/100,000 patient-years in first 2 yr
113/100,000 patient-years in years 8-9.9
Rapid decrease in risk when treatment is stopped
Schilcher J et al.N Engl J Med. 2014;371:974-6
R Dell: personal communication
Ag
e-a
dju
ste
d i
nc
ide
nc
e o
f A
FF
pe
r 1
00
,00
0 p
tYears of
bisphosphonate therapy
0
20
40
60
2 5 8-9.9

FREEDOM Years 1–3 Extension Years 1–7
Placebo (N = 3883)
Cross-over Denosumab (N = 2206)
Long-term Denosumab(N = 2343)
All AEs 156.1 96.8 97.0
Infections 30.7 20.7 19.9
Denosumab: Long-term Safety
Exposure-adjusted Subject Incidence of Adverse Events (Rates per 100 Subject-years)
No adverse events increased in frequency with long-term therapy
OOCOOC
Malignancies 1.6 2.0 2.0
Eczema 0.6 0.9 0.9
Hypocalcemia < 0.1 < 0.1 < 0.1
Pancreatitis < 0.1 < 0.1 < 0.1
Serious AEs 10.4 10.1 10.3
Infections 1.3 1.4 1.5
Cellulitis or erysipelas < 0.1 < 0.1 < 0.1
Fatal AEs 0.8 0.8 0.8
Osteonecrosis of the jaw 0 < 0.1 < 0.1
Atypical femoral fracture 0 < 0.1 < 0.1
N = number of subjects who received ≥ 1 dose of investigational product. Treatment groups are based on the original randomized treatments received in FREEDOM. AEs coded using MedDRA v13.0. Cumulative osteonecrosis of the jaw cases: 6 cross-over, 7 long-term. Cumulative atypical femoral fracture cases: 1 cross-over, 1 long-term. Bone Bone HG et al. HG et al. Lancet Diabetes Lancet Diabetes EndocrinolEndocrinol 2017 2017;5:5132017 2017;5:513--2323
Osteoporosis Therapies
Fracture protection Fracture protection
•• begins within months of starting therapybegins within months of starting therapy
•• persists with longpersists with long--term therapyterm therapy
•• wanes when treatment is stopped wanes when treatment is stopped
–– even with bisphosphonateseven with bisphosphonates
OOCOOC
–– even with bisphosphonateseven with bisphosphonates
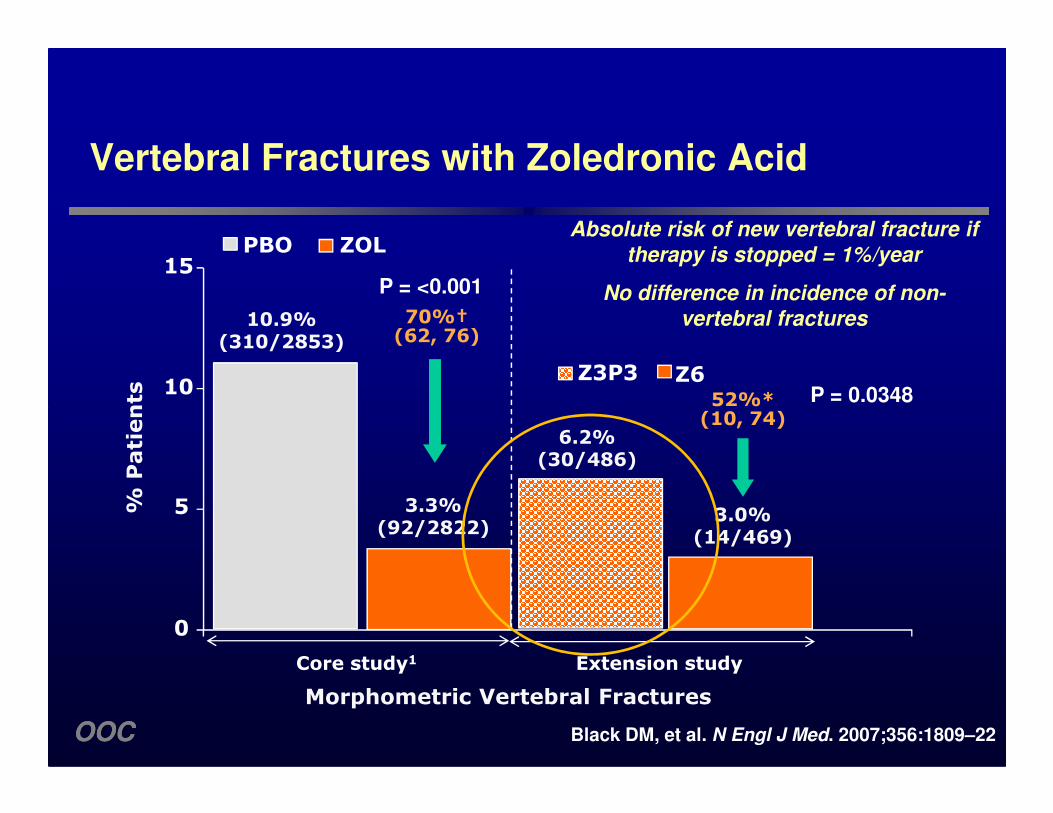
Vertebral Fractures with Zoledronic Acid
52%*(10, 74)
% P
ati
en
ts
10.9%(310/2853)
70%†(62, 76)
Z3P3 Z6
ZOL PBO
10
15
P = 0.0348
P = <0.001
Absolute risk of new vertebral fracture if therapy is stopped = 1%/year
No difference in incidence of non-vertebral fractures
OOCOOC Black DM, et al. N Engl J Med. 2007;356:1809–22
6.2%(30/486)
3.0%(14/469)
52%*(10, 74)
% P
ati
en
ts
Morphometric Vertebral Fractures
3.3%(92/2822)
Core study1 Extension study
0
5

Clinical Vertebral Fractures in FLEX StudyC
um
ula
tive I
ncid
en
ce
of
Fra
ctu
res (
%)
3
4
5
6
ALN 5 years ���� Placebo 5 years
Alendronate 10 years
5.4%
RR ���� 55%
P = 0.013
2.5%
OOCOOC
0 1 2 4 5
Cu
mu
lati
ve I
ncid
en
ce
of
Fra
ctu
res (
%)
Years Since FIT
ALN/PLB 437 436 425 412 398 387
ALN/ALN 662 660 646 631 615 597
3
0
1
2
2.5%
Black DM et al. JAMA. 2006;296:2927-38

Bisphosphonate “Drug Holiday”
• Justification
• Protection from fragility fracture persists 1-2 years upon stopping therapy
• Risk of atypical fracture may decrease when treatment stopped
OOCOOC
• After 3-5 years of therapy:
• Patients at moderate fracture risk: consider a “holiday”
• Patients at high risk (low BMD, prior vertebral fracture, elderly): continue to treat and follow to 10 years
Whitaker et al. N Engl J Med 2012;366:2048-51

OOCOOC Adler R et al. J Bone Miner Res 2016; 31:16–35
Low riskHigh risk

Bisphosphonate “Drug Holiday”
• An “opportunity” – not a necessity and not mandatory
• There is no “rule” that therapy must be stopped after any interval of time
OOCOOC
That decision has to be made on a case-by-case basis
McClung M. Personal opinion, 2017
Denosumab Drug Holiday?
OOCOOC

Discontinuing Denosumab: BMDPhase 2 Study in Women With Low BMD
Discontinued Discontinued TreatmentTreatment
Discontinued Discontinued TreatmentTreatment
Lumbar SpineLumbar Spine Total HipTotal Hip
Perc
en
t C
han
ge
Perc
en
t C
han
ge
SE
)S
E) 66
88
1010
1212
1414
PlaceboPlacebo210 mg Q6M210 mg Q6MOpenOpen--label alendronate label alendronate
OOCOOC Adapted from Miller PD, McClung M et al. Adapted from Miller PD, McClung M et al. BoneBone 2008;43:2222008;43:222--2929
Perc
en
t C
han
ge
Perc
en
t C
han
ge
(LS
Mean
(L
S M
ean
±±S
E)
SE
)
MonthsMonths
−−−−−−−−66
−−−−−−−−44
−−−−−−−−22
00
22
44
MonthsMonths
00 66 1212 1818 2424 3636 4848−−−−−−−−44
−−−−−−−−22
00
22
44
66
88
1010
00 66 1212 1818 2424 3636 4848
–6.7%
N = 52
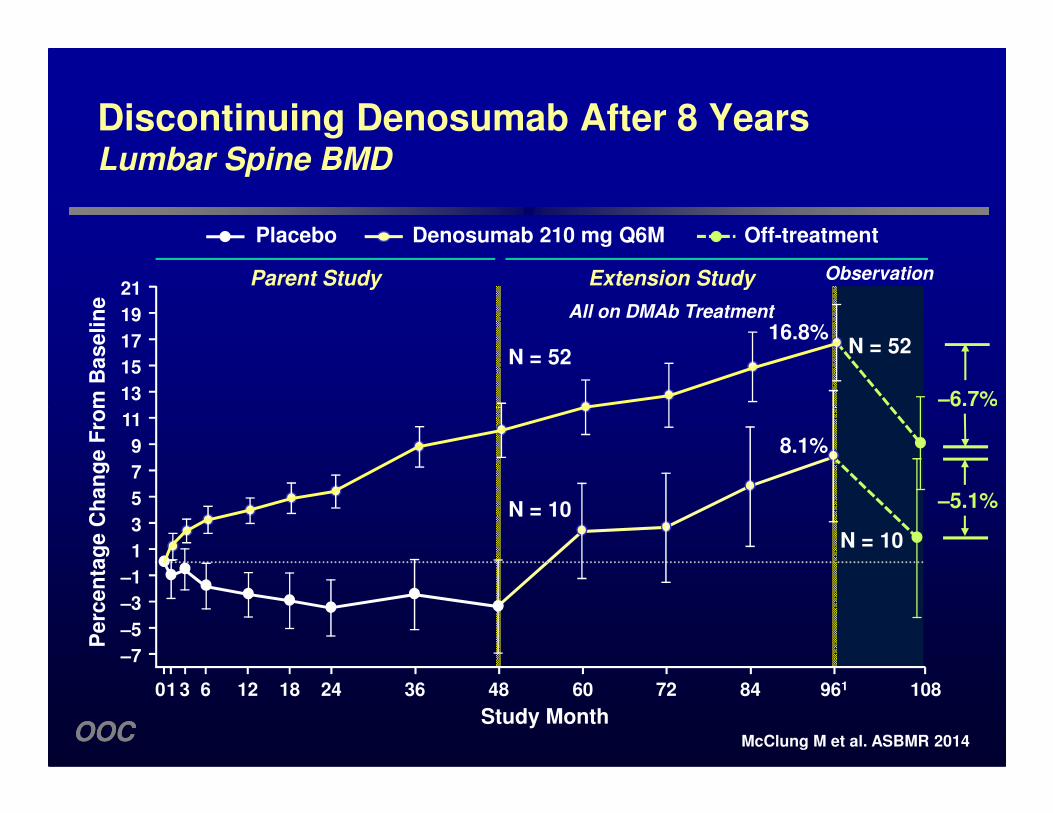
Discontinuing Denosumab After 8 YearsLumbar Spine BMD
Extension StudyParent Study
All on DMAb Treatment
13
15
17
19
21
16.8%N = 52
Observation
Pe
rce
nta
ge
Ch
an
ge
Fro
m B
as
eli
ne
Placebo Denosumab 210 mg Q6M Off-treatment
OOCOOC
–6.7%
–5.1%
N = 10
–7
–5
–3
–1
1
3
5
7
9
11
01 3 6 12 18 24 36 48 60 72 84 961 108
8.1%
N = 10
McClung M et al. ASBMR 2014
Study Month
Pe
rce
nta
ge
Ch
an
ge
Fro
m B
as
eli
ne

Serum Serum CTxCTx BSAPBSAP
1.21.2
1.41.4
1.61.6
Med
ian
ng
/mL
(Q
1,
Q3)
Med
ian
ng
/mL
(Q
1,
Q3)
2020
2525
Med
ian
mcg
/L (
Q1, Q
3)
Med
ian
mcg
/L (
Q1, Q
3)
**††
Discontinuing Denosumab: BMDDiscontinuing Denosumab: BMDPhase 2 Study in Women With Low BMDPhase 2 Study in Women With Low BMD
Discontinued Discontinued TreatmentTreatment
Discontinued Discontinued TreatmentTreatment
PlaceboPlacebo210 mg Q6M210 mg Q6MOpenOpen--label alendronate label alendronate
OOCOOC
**PP < 0.001 at month 36 and = 0.05 at month 48 vs placebo.< 0.001 at month 36 and = 0.05 at month 48 vs placebo.††PP = 0.008 at month 36 vs placebo.= 0.008 at month 36 vs placebo.
00
0.20.2
0.40.4
0.60.6
0.80.8
11.0.0
1.21.2
00 66 1212 1818 2424 3030 3636 4242 4848
Med
ian
ng
/mL
(Q
1,
Q3)
Med
ian
ng
/mL
(Q
1,
Q3)
00
55
1010
1515
2020
00 66 1212 1818 2424 3030 3636 4242 4848
MonthsMonths MonthsMonths
Med
ian
mcg
/L (
Q1, Q
3)
Med
ian
mcg
/L (
Q1, Q
3)
**
**
††
Adapted from Miller PD, McClung M et al. Adapted from Miller PD, McClung M et al. BoneBone 2008;43:2222008;43:222--2929

Effect of Withdrawing Alendronate or E/P: Urinary NTx
Mean Percent Change (Mean Percent Change (±± SE)SE)Stratum 1 OnlyStratum 1 Only
Me
an
Pe
rce
nt
Ch
an
ge
Me
an
Pe
rce
nt
Ch
an
ge
--2020
00
OOCOOC
YearsYears00 11 22 33 44 55 66
Me
an
Pe
rce
nt
Ch
an
ge
Me
an
Pe
rce
nt
Ch
an
ge
--100100
--8080
--6060
--4040
PBO/PBO/PBOPBO/PBO/PBO Estrogen/ProgestinEstrogen/Progestin-- Off TherapyOff Therapy
Wasnich, McClung et al. Wasnich, McClung et al. MenopauseMenopause 2004;1:6222004;1:622--630630

Denosumab “Drug Holiday”?
Vertebral Fractures After Discontinuing Denosumab Therapy
• At least 24 patients have been reported who experienced vertebral fractures within 3-18 months after discontinuing denosumab therapy. (1)
OOCOOC
therapy. (1)
• Many or most have had multiple and/or severe fractures
• Raised concern about “rebound” risk of fracture
• Similar to rapid loss of fracture protection when estrogen therapy is discontinued (2,3)
1. Anastasilakis AD et al. J Bone Miner Res. 2017 Feb 272. Heiss G et al. JAMA 299:1036–45
3. McClung MR. Osteoporos Int. 2016;27:1677-82

Vertebral Fractures After Discontinuing Denosumab or Placebo in FREEDOM Study
• Vertebral fracture risk was assessed in patients who discontinued either placebo or denosumab in the FREEDOM study or who stopped denosumab in the FREEDOM Extension study and who had a follow-up at least 7 months after their last dose
• Fracture risk increased upon stopping denosumab but not to levels greater than seen in those who stopped placebo
OOCOOC
Vertebral fractures Multiple vertebral fractures
Brown JP et al. ASBMR Abstract #1100, 2016

Effect of Withdrawing Hormone Therapy: Hip Fracture in WHI
• Within first year, of stopping hormone therapy, hip fracturerates approximate those in placebo group
• No evidence of rebound in fracture risk
OOCOOC Heiss G et al. JAMA. 2008;299:1036-45

2
An
nu
ali
zed
rate
s -
%CEE-MPA Treatment (N=8506)
CEE-MPA Post-treatment (N-8052) PBO Post-treatment (N=7678)
Placebo (N=8102)
Effect of Withdrawing Hormone Therapy: Fractures in WHI
No rebound or excess fracture risk after stopping estrogen
OOCOOC
0
0.5
1
1.5
An
nu
ali
zed
rate
s
Heiss G et al. JAMA 2008;299:1036-45
Hip fracture
Vertebral fracture
Other fractures

6
8
Denosumab and Alendronate (DAPS Trial)
Cross-over Treatment after 12 Months
Pe
rce
nt
Ch
an
ge
Fro
m B
as
eli
ne Denosumab Alendronate
Switching from denosumab to alendronate, bone loss did not occur
Lumbar spine
OOCOOC
0
2
4
6
0 12 24
Freemantle N et al. Osteoporos Int 2012;23:317-26
Pe
rce
nt
Ch
an
ge
Fro
m
Months
Total hip

• There are very few reasons to consider stopping denosumab therapy
• intolerance or side effect
• reaching a treatment “target”
Long-term Denosumab TherapySummary
OOCOOC
• If therapy is stopped after a year or more, consider options to prevent rapid bone loss and fracture risk
• At present, the most appealing strategy would be to treat with a bisphosphonate for 2 years and to then re-evaluate the patient. (1)
1. McClung MR. Cancel the denosumab holiday. Osteoporos Int. 2016;27:1677-82

Effects of Therapy on Total Hip BMD Through 10 Years
LongLong--term Denosumabterm Denosumab
FREEDOMFREEDOM ExtensionExtension
6
7
8
9
10 9.2%9.2%
6.8%6.8%
Perc
en
tag
e C
han
ge F
rom
Baseli
ne
Perc
en
tag
e C
han
ge F
rom
Baseli
ne
Alendronate 10 mg/dAlendronate 10 mg/d22
DenosumabDenosumab11
Total Hip BMDTotal Hip BMD
OOCOOC
-2
-1
0
1
2
3
4
5
Perc
en
tag
e C
han
ge F
rom
Baseli
ne
Perc
en
tag
e C
han
ge F
rom
Baseli
ne
Study YearStudy Year
11 22 33 44 5500 66 77 88 99 1010
4.6%4.6%
ZoledronicZoledronic acid 5 mg/yacid 5 mg/y33
1. Bone HG et al. 1. Bone HG et al. Lancet Diabetes Lancet Diabetes EndocrinolEndocrinol 2017 Published Online May 22, 20172017 Published Online May 22, 2017http://dx.doi.org/10.1016/S2213http://dx.doi.org/10.1016/S2213--8587(17)301388587(17)30138--99
2. Bone HG et al. 2. Bone HG et al. New New EnglEngl J J Med.2004Med.2004;350:1189;350:1189--99993. Black DM et al. 3. Black DM et al. New New EnglEngl J J Med Med 2012;27:2432012;27:243--5454

Switching From Bisphosphonates to Denosumab
1.6%*1.4%*
0.9%* 1.3%*
To
tal
Hip
Pe
rce
nt
Ch
an
ge
Fro
m B
as
eli
ne
3.0%
4.0%
Patients who had previously been treated with bisphosphonates randomly assigned to a bisphosphonate or denosumab.
OOCOOC
Data are least-squares means and 95% confidence intervals. *p < 0.0001 denosumab vs BP. (1) Roux C et al. Bone. 2014;58:48-54. (2) Recknor C et al. Obstet Gynec 2013;121:1291-9. (3) Kendler DL et al. J Bone Miner Res. 2010;25:72-81. (4) Miller PD et al. J Clin Endo Metab. 2016;101:3163-70.
IBNALN
ZOLRIS
To
tal
Hip
Pe
rce
nt
Ch
an
ge
Fro
m B
as
eli
ne
0.5% 0.9% 1.1% 0.6%2.0% 2.2% 1.9% 1.9%0.0%
1.0%
2.0%
vs RIS (1) vs IBN (2) vs ALN (3) vs ZOL (4)

FNIH Meta-regressionChange in Total Hip BMD vs Reduction in Hip Fracture
MORE (RAL)
FIT II(ALN)
HIP(RIS)
FREEDOM (DMAB)
Clodronate
R2=0.52The greater the increase in BMD, the greater reduction in NV fractures
OOCOOC
FIT I(ALN)
HORIZON(ZOL)
FREEDOM (DMAB)
WHI
*Bubble size ~ to # fractures in study Courtesy of Dr D Black et al, ASBMR 2015

Relationship Between OnRelationship Between On--Treatment Total Hip Treatment Total Hip BMD TBMD T--score score and Nonand Non--vertebral Fracture Riskvertebral Fracture Risk
Incid
en
ce o
f n
on
Incid
en
ce o
f n
on
--vert
eb
ral
vert
eb
ral
fractu
re a
t 1 y
ear
(%)
fractu
re a
t 1 y
ear
(%)
4.04.0
5.05.0
6.06.0
Treating to a BMD target Treating to a BMD target may now be feasiblemay now be feasible
Current NV fracture risk Current NV fracture risk was strongly correlated was strongly correlated
OOCOOC
Incid
en
ce o
f n
on
Incid
en
ce o
f n
on
fractu
re a
t 1 y
ear
(%)
fractu
re a
t 1 y
ear
(%)
--3.03.0 --2.52.5 --2.02.0 --1.51.5 --1.01.0 --0.50.5
1.01.0
2.02.0
3.03.0
4.04.0
Total Hip TTotal Hip T--scorescore
Ferrari S et al. ASBMR; Seattle, WAFerrari S et al. ASBMR; Seattle, WA; October ; October 20152015
was strongly correlated was strongly correlated with on target hip BMD with on target hip BMD

Treat to Target: An Evolving Concept
OOCOOC
Cummings SR et al. J Bone Miner Res 2017;32:3-10

Osteoporosis: Long-term Treatment Plan
Raloxifene
Bisphosphonate
When concerned about hip fracture
3-5 years
Low risk Consider drug holiday
Re-treat
OOCOOC
Teriparatide/abaloparatide
Denosumab
After 12-24 months
After 12-24 months
3-5 years
High risk Continue therapy?
Denosumab Bisphosphonatefor 1-2 years
If “target” is met

Osteoporosis Therapy: Long-term Management Plan
• Decisions about starting therapy must be individualized
• After 3-5 years of bisphosphonates, consider
• drug holiday for patients at modest risk
OOCOOC
• drug holiday for patients at modest risk
• switching to denosumab if hip BMD still low
• Denosumab
• very rarely a reason to stop therapy
• if denosumab therapy is to be stopped, consider an alternative anti-resorptive (e.g. bisphosphonate) to prevent rapid bone loss
McClung M. Personal opinion, 2017
Photo courtesy of Betsy Love McClung, RN, MN

Thank you
OOCOOC
Michael R. McClung, MD, FACPFounding Director
Oregon Osteoporosis CenterPortland, Oregon, USA