l’idrocefalo normoteso - neuro.it regionali sin/2017/pi-li-va... · surgical...
TRANSCRIPT

L’IDROCEFALO NORMOTESO
Il Trattamento Chirurgico
Francesco Lupidi
ENTE OSPEDALIERO “OSPEDALI GALLIERA” - GENOVA
S.C. NEUROCHIRURGIA
Direttore: Dr. Paolo Severi
OUTLINE
DISCLOSURE
History
Procedures
Devices
Guidelines
Conflict of interest: none

…a reversible dementia [www.idrocefaloidiopatico.it]
SURGICAL TREATMENT
- Clinic
- Imaging
- Invasive tests: at least one CSF tap test
- Risk-benefit assessment > Comorbidity Index
GOAL
INDICATION
Clinical improvement through unidirectional
diversion of CSF to absorption cavity
effective outflow / pulse-synchronous transient outplacement
HISTORY
Mikulicz-Radecki (1893): cortectomy
Pair (1908): saphenous vein transplantation
Torkildsen (1947): first ventriculocisternostomy
Pudenz (1955): Teflon valve with slit mechanism
Hakim (1964): unidirectional pressure-regulated valve for NPH
…more than 200 shunt designs…
SURGICAL PROCEDURES
SHUNT INSERTION: standard of surgical care
diversion of CSF regulated by one-way flow valve
• Ventriculoperitoneal (lateral ventricles: frontal / occipital)
• Ventriculoatrial
• Ventricolopleural
• Lumboperitoneal (SINPHONI-2 trial)
ENDOSCOPIC THIRD VENTRICULOSTOMY (ETV)
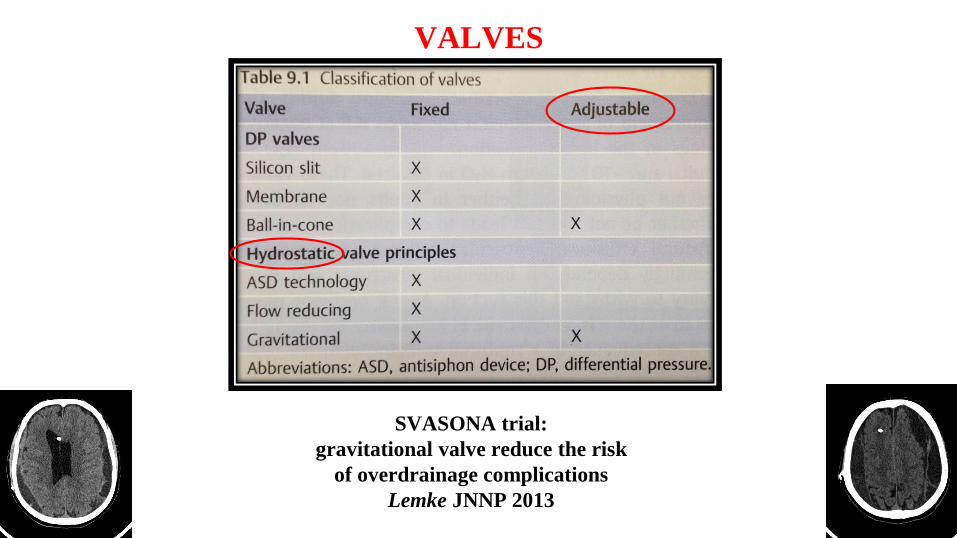
VALVES
SVASONA trial:
gravitational valve reduce the risk
of overdrainage complications
Lemke JNNP 2013

DEVICES
Siphonguard ®
Ventricular Catheter
Reservoir Adjustable valve Gravitational unit

PHYSICS OF VP SHUNTS
Opening Pressure
Boon (Dutch), JNS 1998: 100 vs 40 mm H2O
Lemke (SVASONA), JNNP 2013: 100 > 70 mm H2O
Delwel JNNP 2013 (DEPSS): optimal setting controversial
> highest opening pressure (140 mm H2O)
Pressure at the outlet
Hydrostatic Pressure
Siphoning
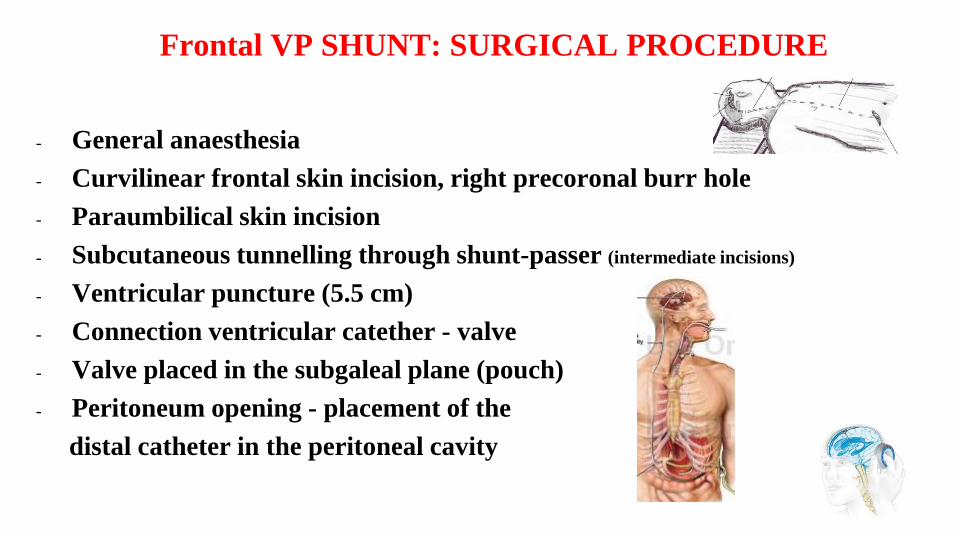
Frontal VP SHUNT: SURGICAL PROCEDURE
- General anaesthesia
- Curvilinear frontal skin incision, right precoronal burr hole
- Paraumbilical skin incision
- Subcutaneous tunnelling through shunt-passer (intermediate incisions)
- Ventricular puncture (5.5 cm)
- Connection ventricular catether - valve
- Valve placed in the subgaleal plane (pouch)
- Peritoneum opening - placement of the
distal catheter in the peritoneal cavity

Frontal VP SHUNT: SURGICAL PROCEDURE
Frontal skin incision
Right precoronal burr hole
Subcutaneous tunnelling
Ventricular puncture
TIPS & TRICKS
- Sterility: first case, limited number of personnel,
clippers, drapes, anti-microbial impregnated
catheter, etc.
- Time: straight-forward procedure (1 hour or less),
minimal amount of time for cranial incision
- Minimal intraoperative CSF leakage

OUTCOME: improvement
Toma Acta Neurochir 2013
71%
E iNPH MS 2013 69 / 84%
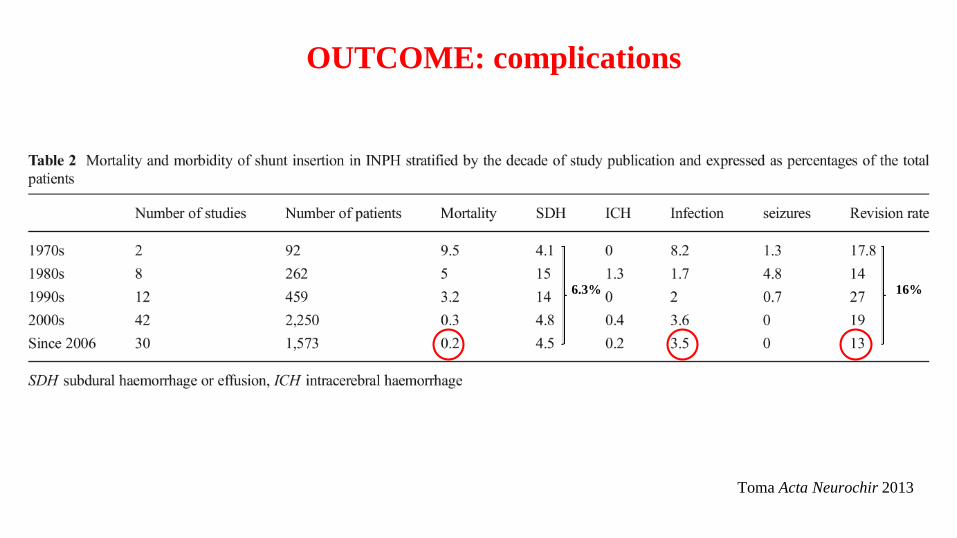
OUTCOME: complications
Toma Acta Neurochir 2013
16%6.3%

PREDICTORS
Halperin Neurology 2015
- elevated Ro (1 Class I, multiple Class II, level B)
- impaired cerebral blood flow reactivity to acetazolamide
(by SPECT) (1 Class I, level C)
- positive response to either external lumbar drainage (1
Class III) or repeated lumbar punctures (level C)
- Age may not be a prognostic factor (1 Class II, level C).
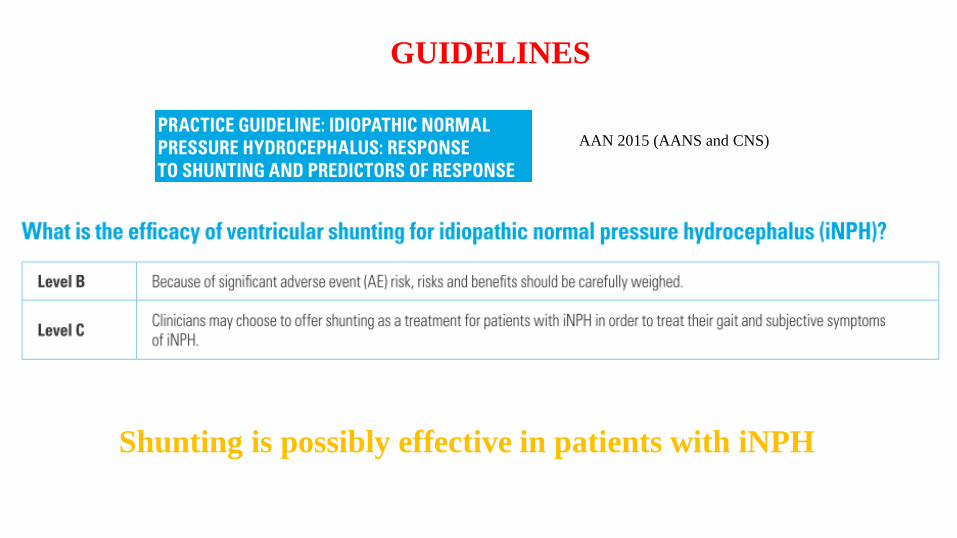
GUIDELINES
AAN 2015 (AANS and CNS)
Shunting is possibly effective in patients with iNPH
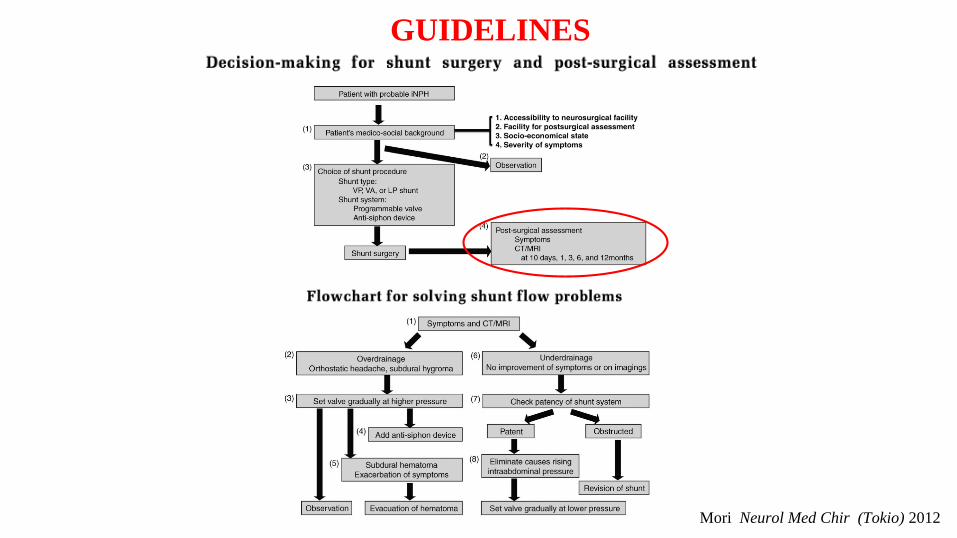
GUIDELINES
Mori Neurol Med Chir (Tokio) 2012

ENDOSCOPIC THIRD VENTRICULOSTOMY (ETV)
• secondary NPH: acquired / developmental etiologies
- Late-onset Idiopathic Aqueductal Stenosis (LIAS)
- Longstanding Overt Ventriculomegaly (LOVA)
• alternative to shunt revision
Selected INDICATIONS:
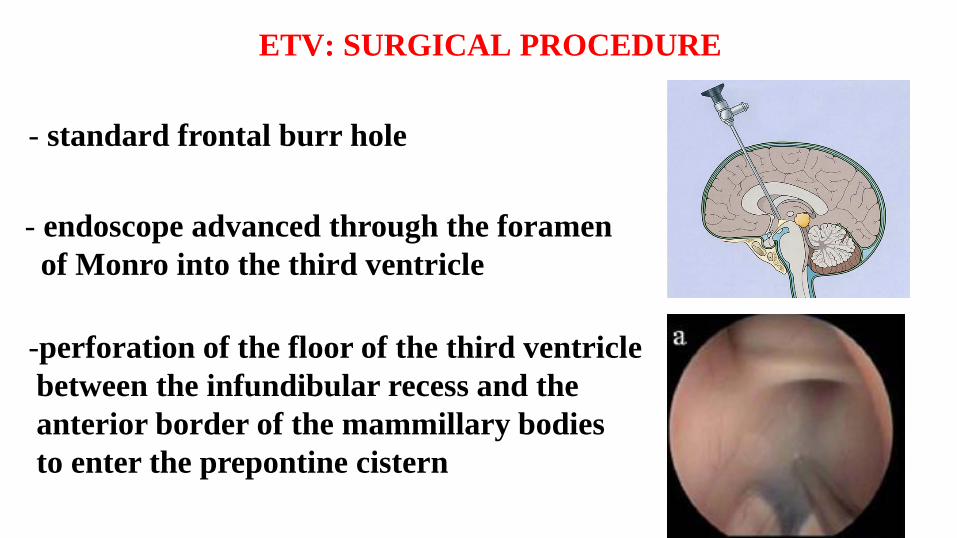
ETV: SURGICAL PROCEDURE
- standard frontal burr hole
- endoscope advanced through the foramen
of Monro into the third ventricle
-perforation of the floor of the third ventricle
between the infundibular recess and the
anterior border of the mammillary bodies
to enter the prepontine cistern
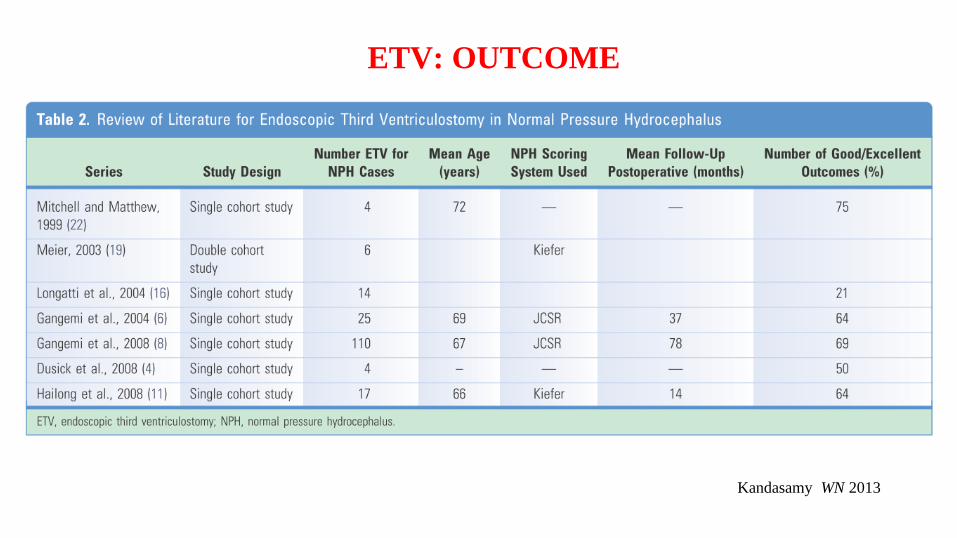
ETV: OUTCOME
Kandasamy WN 2013
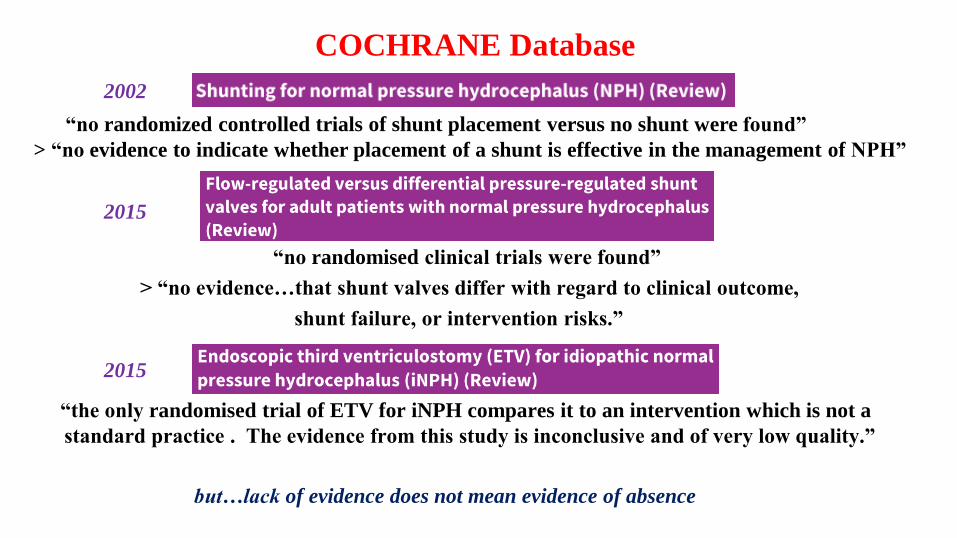
COCHRANE Database
“no randomized controlled trials of shunt placement versus no shunt were found”
> “no evidence to indicate whether placement of a shunt is effective in the management of NPH”
“no randomised clinical trials were found”
> “no evidence…that shunt valves differ with regard to clinical outcome,
shunt failure, or intervention risks.”
“the only randomised trial of ETV for iNPH compares it to an intervention which is not a
standard practice . The evidence from this study is inconclusive and of very low quality.”
2002
2015
2015
but…lack of evidence does not mean evidence of absence
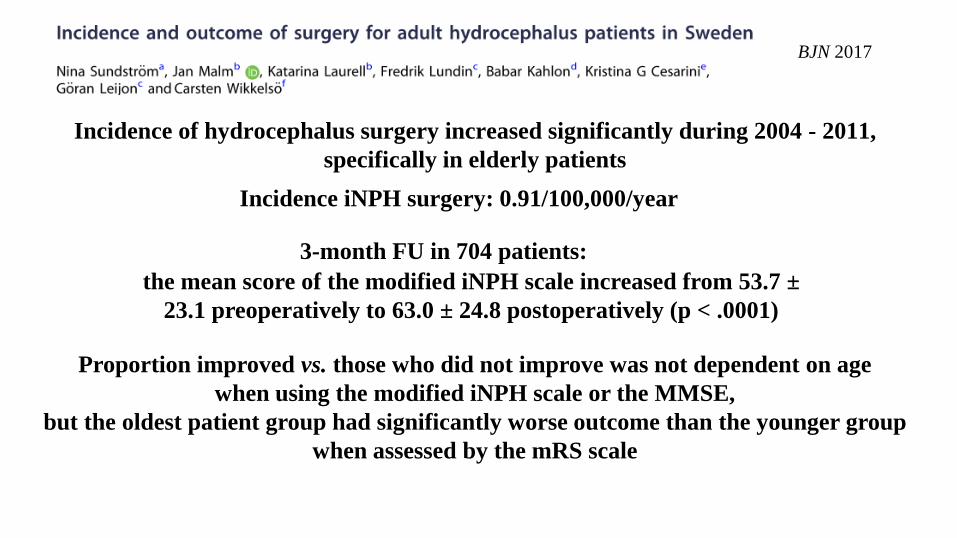
Incidence of hydrocephalus surgery increased significantly during 2004 - 2011,
specifically in elderly patients
BJN 2017
Incidence iNPH surgery: 0.91/100,000/year
3-month FU in 704 patients:
the mean score of the modified iNPH scale increased from 53.7 ±
23.1 preoperatively to 63.0 ± 24.8 postoperatively (p < .0001)
Proportion improved vs. those who did not improve was not dependent on age
when using the modified iNPH scale or the MMSE,
but the oldest patient group had significantly worse outcome than the younger group
when assessed by the mRS scale
PREOPERATIVE Video

POSTOPERATIVE Video: 6 months
DISCUSSION / CONCLUSIONS
- Safe ed effective management (proper selection)
- Long lasting improvement (even after shunt revision)
- Aging: older patient increasingly operated improved QOL
- Role of physiotherapy
- Need for randomized controlled trials

GRAZIE PER
L’ATTENZIONE!