lesson 3: secondary assessment emergency reference guide p. 20-22
TRANSCRIPT

Lesson 3:Lesson 3: Secondary Assessment Secondary Assessment
Emergency Reference Guide p. 20-22Emergency Reference Guide p. 20-22

ObjectivesObjectives
• State the importance of taking a personal history from victim & know how to do it
• Demonstrate taking a personal history
• Demonstrate a hands on physical exam
• Demonstrate how to take vital signs
• Demonstrate how to document information gathered
Getting the Whole PictureGetting the Whole Picture
• After primary assessment comes a hands on secondary assessment
• Goal is to find EVERY problem
• Consider environment when removing clothing during checks
• Single person does exam, second person records results – why?
• SAMPLE history taken at this time

Getting the Whole PictureGetting the Whole Picture (cont’d.) (cont’d.)
• If patient can talk, take SAMPLE first
If patient can’t talk, check with other members, use medical forms for info (i.e. allergies, medications, etc.)
• Document signs & symptoms
• Look for signs of injury
• Listen to victims words & responses
• Feel body parts

Taking a SAMPLE HistoryTaking a SAMPLE History• S = Signs & symptoms: Ask what hurts?
What pain do they have, nausea, lightheadedness?
• A = Allergies: do they have any? Did they contact anything they are allergic to?
• M = Medications: on any, last time taken?
• P = Pertinent medical history: anything like this happened before? Existing conditions?

Taking a SAMPLE History Taking a SAMPLE History (cont’d.)(cont’d.)
• L = Last intake & output: Last time ate or drank? Last time urinated or defecated?
• E = Events: What led up to this injury (Mechanism Of Injury)?

Skill PracticeSkill Practice
• Break into pairs, one victim, one care giver
• Scenario:
• “While clearing some downed limbs from the trail, a person is apparently stung by a bee.”
• Practice taking, and recording SAMPLE
Why Documentation is Why Documentation is Important?Important?
• Responder’s ability to remember details is reduced due to stress/confusion
• Specific info helps rescue personnel know what they are facing
• Retention for legal/medical reasons
• Using a form helps you remember everything you need to look for/ask about
Documentation Documentation (cont’d.)(cont’d.)
• SOAP:
• S = subjective info (complaints)
• O = Objective info (i.e. physical exam, vital signs, SAMPLE
• A = Assess patient & situation, what do you think is wrong?
• P = Plan, what care do you give & how? Stay or evacuate?
Performing Hands On Performing Hands On Physical ExamPhysical Exam
• Using MOI or SAMPLE record circumstances & estimate injuries
• Do not make assumptions about MOI
• Systematically check from head to toe
• Ask where it hurts
• Check all body parts, don’t cause unneeded pain
Performing Hand OnPerforming Hand OnPhysical Exam Physical Exam (cont’d.)(cont’d.)
• Examples of Signs & Symptoms:– Pale sweaty skin– Nervousness– Unnatural position of limbs– Patient guarding an area or unable to move
body part
• Looks for “DOTS”

DOTSDOTS
• DOTS stands for:
• D = Deformities, depressions, indentations and discoloration
• O = Open injuries, penetrating wounds, cuts, scrapes
• T = Tenderness
• S = Swelling

Performing Hands OnPerforming Hands OnPhysical ExamPhysical Exam
• Check Circulation, Sensation, Motion– Ask about pain first, then touch
• Note medical ID bracelets, necklaces• Check pulse away from injury & away from heart
(i.e. on hand or foot)• Check for circulation in hands & feet • Pinch & check for capillary refill (nail bed) • If head/neck/back injury possible, ask patient to
not move, help restrain from moving

Head to Toe AssessmentHead to Toe Assessment
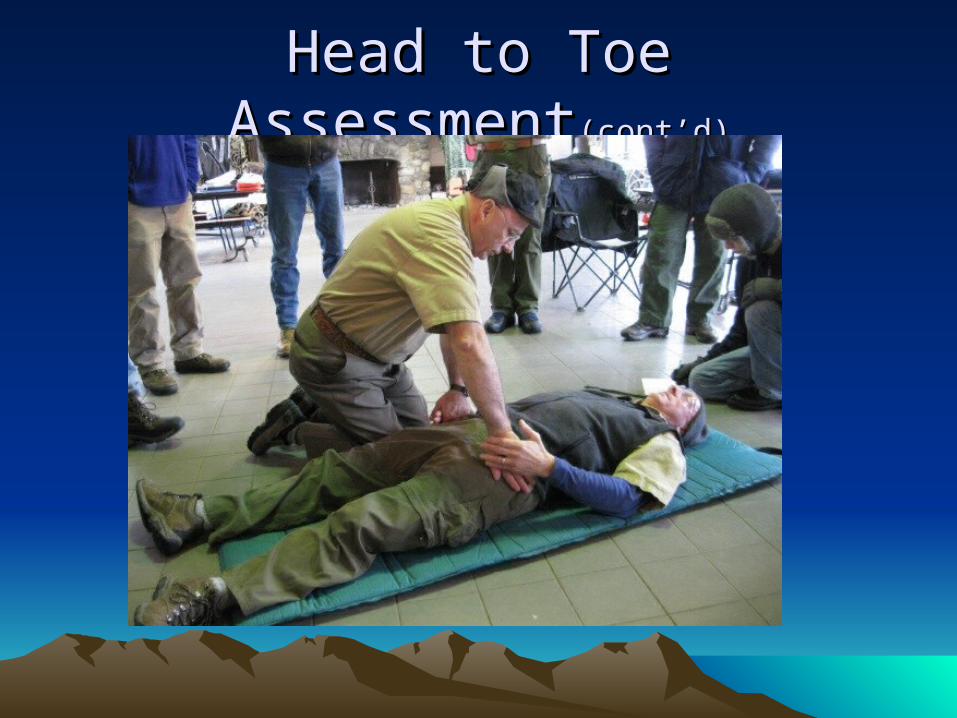
Head to Toe AssessmentHead to Toe Assessment(cont’d)(cont’d)

Physical Exam Physical Exam Practice SessionPractice Session
• Form into groups of 3:– One victim– 2 rescuers
• Perform SAMPLE
• Head to toe check

Taking Vital SignsTaking Vital Signs• Vital signs are a measure of the processes
needed for life• Changes in time indicate patient condition
changing• Take & record vital signs regularly• Basic Set:
– Level of Responsiveness– Breathing Rate– Pulse– Skin Color, Temp, Moisture (SCTM)

Level of ResponsivenessLevel of Responsiveness• AVPU:
– Alertness• A + Ox4: knows who, where, when, what• A + Ox3: knows who, where, when• A + Ox2: knows who, where• A + Ox1: knows who
– V = Responds to verbal stimuli– P = Responds to pain– U = Unresponsive

Respiratory Rate/Heart RateRespiratory Rate/Heart Rate
• Respiratory: Number breaths/min., note rhythm and quality:– Normal 12-20 for adults– Place hand on chest to measure– Note any unusual sounds
• Heart Rate (pulse): Measure at wrist, brachial artery, or neck– Use 2 fingers (no thumb)– Count for 30 seconds– Note rhythm, quality (strength)
Skin Color, Temp, MoistureSkin Color, Temp, Moisture
• Note any differences from normal:– Skin Color should be pink (non-pigmented
areas)– Temperature should be warm– Moisture: skin should be dry

Practice SessionPractice Session• Form into groups of 3
– One victim– One takes vital Signs– One records

Re-Checking ResourcesRe-Checking Resources
• After patient assessment:– Observe changing conditions in environment– Getting unsafe for patient or you?– Getting difficult to get help?– What resources do you have, how can you
use them?– Do you need to move the patient?
Questions???Questions???
What else could you add to your What else could you add to your First Aid Kit?First Aid Kit?