lena burri, ph.d krill oil
TRANSCRIPT

Lena Burri, Ph.D
KRILL OIL CONCENTRATEThe phospholipid factor that sets krill oil apartThe next generation Omega-3 Phospholipid product from Antarctic krill
2 KRILL OIL CONCENTRATE
To effectively maintain our bodily functions and to keep cells and body in balance,
we need a continuous supply of nutrients. Whereas in diseased conditions, it is also
important to address the fluctuations often seen in nutrient uptake and utilization.
There is excitement and growing evidence surrounding krill oil as an important nutrient
based on its major components:
• Long-chain omega-3 fatty acids (EPA/DHA)
• Phospholipids and specifically its choline via its phosphatidylcholine- “lecithin”
component
Krill oil is unique in that it is a combination of these naturally occurring
nutrients. And when ingested, it delivers EPA/DHA, phospholipids, and
choline to the body, where they work individually and in combination; i) as vital
constituents in the structure and functioning of cells, ii) for assisting in the balancing of
bodily functions, and iii) to address their deficiencies in health conditions related to the
heart, brain, inflammation, immunity, liver, etc.
Omega-3 fatty acids are one of the most recognized and studied compounds with more
than 20.000 scientific papers published. Research has shown that when omega-3 fat-
ty acids from marine sources, such as fish and krill, are ingested, they incorporate into
cells to affect cell structure and function. Unlike fish oil, krill oil not only delivers EPA
and DHA, but also phospholipids into cells, where they also exert their effects on re-
modeling cells’ structures, fluidity, and functions. With this, and their ability to affect
cholesterol metabolism, phospholipids may trigger downstream pathways and mecha-
nisms into meaningful health benefits.
This book identifies some of the research that addresses several of these pathways
and mechanisms important for conditions of e.g. the heart, brain, and liver. It details
Foreword
3 KRILL OIL CONCENTRATE
the above-mentioned aspects of krill oil, its components, and how science and research
points to its beneficial health effects while drawing comparisons to fish oil where
applicable.
The latest product development from Antarctic krill is also introduced. It is a highly
concentrated and purified product developed on the premise that a higher omega-3
phospholipid concentration may deliver better health benefits across various health
conditions than its predecessors. Thus, the next generation omega-3 phospholip-
id product is a krill oil concentrate with more omega-3 fatty acids being efficiently
delivered to tissues via more phospholipids high in choline.
Lena Burri, Ph.DAker BioMarine Antarctic AS
Oslo, Norway

4 KRILL OIL CONCENTRATE
Lena Burri, Ph.D
Lena Burri, Ph.D. has been involved in fundamental re search, has published
peer-reviewed articles in leading journals, and contributed review articles, as
well as book chapters on subjects including omega-3 fatty acids. Lena earned her
Master of Science from the University of Ba sel (Switzerland) and her Ph.D. at the
Ludwig Institute for Cancer Research (Switzerland). Her post-doctoral educa tion
included stays at Melbourne University (Australia), University of British Columbia
(Canada), and University of Bergen (Norway). She now works as R&D Director for Aker
BioMarine Antarctic AS.
ISBN: 978-82-690452-0-8All rights reserved. No part of this book may be reproduced in any form or by any means electronic or mechanical, including photocopying, recording or by any information storage and retrieval system without permission in writing from the copyright holder and the publisher.

5 KRILL OIL CONCENTRATE
Summary
• Krill oil is extracted from Antarctic krill.
• Antarctic krill lives in the Southern Ocean around Antarctica.
• The Convention of the Conservation of Antarctic Marine Living Resources (CCAMLR), an international treaty, regulates krill harvesting in a sustainable way. In Area 48 in the Southern Ocean, which is the only area where krill fisheries can operate, the krill industry is allowed to catch one per cent of the estimated 60 million tons of krill.
• Krill oil is rich in omega-3 phospholipids and therefore a good source o f both omega-3 fatty acids and choline from the phospholipid head group.
• What differentiates krill oil from fish oil is the molecular form, in which the omega-3 fatty acids are bound to, namely phospholipids in krill oil and triglycerides in fish oil.
• The long-chain omega-3 fatty acids EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid) promote healthy heart, brain and visual function and contribute to reducing and maintaining normal levels of inflammation, blood triglycerides, and blood pressure.
• Choline is vital for many biological functions (e.g. membrane structure, nerve signaling, methylation reactions, lipid transport, etc.) and deficiency can lead to fatty liver, muscle damage, atherosclerosis, etc.
• The typical Western diet contains inadequate amounts of omega-3 fatty acids and choline. This contributes to the approximately 90% of the American population who are deficient in omega-3 fatty acids and choline [1,2]. • Krill oil supplementation can help to increase levels of omega-3 fatty acids and choline in the body, thus reducing the deficiencies of these important nutriments.
• Several clinical studies have shown health benefits for supplementation with krill oil.

6 KRILL OIL CONCENTRATE
Table of Contents
Summary ............................................................................................5Krill background ................................................................................8Krill oil concentrate ..........................................................................11 Latest krill oil studies .....................................................................................15
Sport .................................................................................................................15
Skin ....................................................................................................................18
Phospholipids ....................................................................................22 What is a phospholipid? .................................................................................22
Functions of phospholipids in the body .................................................23
Cell membranes ...........................................................................................23
Lipid transport and cholesterol metabolism...................................24
Uptake of phospholipids ...............................................................................26
Phospholipid sources .....................................................................................26
Phospholipid deficiency ................................................................................27
Phospholipids in health and disease .......................................................27
Liver ..................................................................................................................27
Brain .................................................................................................................30
Choline................................................................................................31 What is choline? ................................................................................................31
Functions of choline in the body ................................................................32
Nerve signaling ............................................................................................32
Cell signaling .................................................................................................32
Methyl donor .................................................................................................32
Water balance ..............................................................................................33
Uptake of choline salt versus phosphatidylcholine ..........................33
7 KRILL OIL CONCENTRATE
Choline deficiency ...........................................................................................34
Choline in health and disease ......................................................................35
Brain .................................................................................................................35
Sport .................................................................................................................36
Omega-3 fatty acids ..........................................................................37 What are omega-3 fatty acids? ..................................................................37
Functions of omega-3 fatty acids .............................................................37
Membranes ....................................................................................................38
Gene transcription and enzyme activity ...........................................38
Eicosanoids ...................................................................................................39
Endocannabinoids ......................................................................................39
Omega-3 deficiency ..........................................................................40Omega-3 fatty acids in health and disease ....................................41 Heart ................................................................................................................41
Brain .................................................................................................................42
Krill oil: Phospholipids, choline, and omega-3 fatty acids all in one ...................................................44 Why krill oil? .......................................................................................................44
Uptake of krill oil in the body ......................................................................45
Krill oil in health and disease .......................................................................46
Omega-3 Index .............................................................................................46
Conclusion ..........................................................................................51Acknowledgements ...........................................................................51References .........................................................................................52

8 KRILL OIL CONCENTRATE
Euphausia superba (E. superba) is the scien-
tific name for ‘Antarctic krill’.
The shrimp-like crustaceans from the Eu-
phausiacea family are commonly referred
to as ‘krill’ and consist of 86 species [3].
Euphausia superba (E. superba), also called
‘Antarctic krill’, is the most dominant krill
species in the pristine oceans surrounding
Antarctica [4]. Even though Antarctic krill
are only about the size of your smallest fin-
ger, they are a keystone species of the Ant-
arctic marine ecosystem. Krill is considered
to be at the bottom of the food chain, since
they feed on phytoplankton and are food for
many marine animals, such as whales, seals,
penguins, squid, and fish. Of all multi-cellular
animal species on Earth, Antarctic krill is the
most abundant species with one of the larg-
est biomasses of around 500 million metric
tons.
Compared with other marine life, Antarctic
krill gathers in the largest groups [5] and
also has the most potent known digestive
enzymes on Earth [6].
These small pinkish-red transparent crea-
tures are one of the world’s largest swarm-
ing animals. They often aggregate in large,
dense swarms stretching for tens of kilome-
ters and measuring 30 meters deep.
They tend to swarm and migrate
vertically as methods of avoiding attacks
from predators. They also swim up to the
sea’s surface to feed and reproduce main-
ly during the night and then swiftly swim
down into deeper waters to avoid predators,
such as birds, penguins, seals, squid, fish or
whales. When larger, swarm-hunting animals
attack, they quickly scatter by swimming
backwards (as fast as 60 cm per second) in
all directions to confuse the predator. An-
other defense from smaller attackers is to
leave their exoskeleton behind as a food dis-
traction.
Some krill swarms may consist only of
young krill or either females or males.
Krill are bioluminescent, meaning
that their bodies can emit light by chemical
reactions involving oxygen molecules. These
reactions take place in photocytes, lumi-
nescent cells assembled into light organs.
Krill use muscle contraction and relaxation
Krill Background

9 KRILL OIL CONCENTRATE
for the regulation of the intensity of the light.
When special closure muscles relax, the light is
emitted, which is suspected to be due to more
oxygenated blood reaching the photocytes.
It is believed that this light emission
is important for recognizing members of the
same species and keeping them together in
a swarm [7]. Though suspected, but unknown,
this feature may also be valuable in defending
against detection from predators or in mating.
Another characteristic of krill are their large
dark brown compound eyes, and like with in-
sects, they consist of many little eyes. This
gives krill the ability to see in many differ-
ent directions at the same time, which helps
them to locate food and detect predators.
However, in comparison to human eyes that
can see in only one direction, the vision quali-
ty of each little eye in krill is lower.
Krill can survive up to 200 days with-
out food by shrinking and using their body’s
bio-material for storing energy in the form of
Krill Background
Antarctic krill is found in the Southern Ocean
Krill swarm
10 KRILL OIL CONCENTRATE
lipids. Some krill species hold their lipid
reserves in wax esters and others pre-
dominantly in triglycerides. However,
members of the Euphausiid family are
the only known species in which phospho-
lipids are used as their energy depot. In
particular, Antarctic E. Superba krill uses
phosphatidylcholine containing omega-3
fatty acids as their lipid reserve [3].
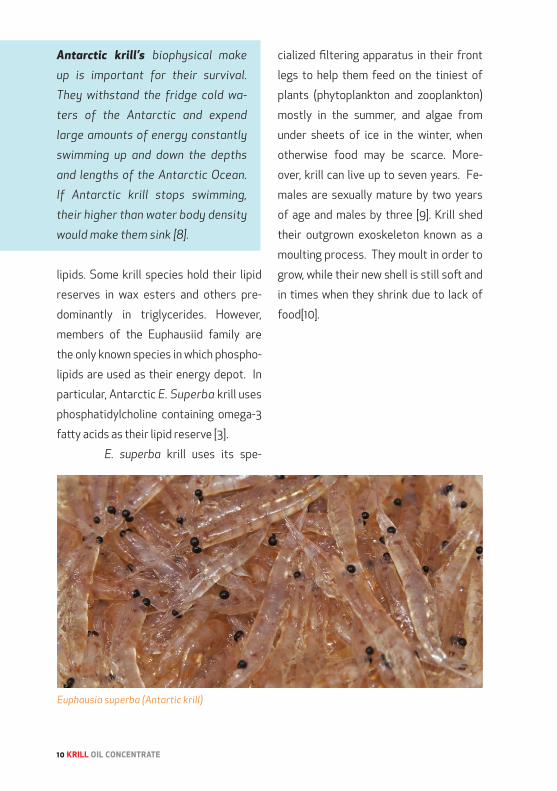
E. superba krill uses its spe-
cialized filtering apparatus in their front
legs to help them feed on the tiniest of
plants (phytoplankton and zooplankton)
mostly in the summer, and algae from
under sheets of ice in the winter, when
otherwise food may be scarce. More-
over, krill can live up to seven years. Fe-
males are sexually mature by two years
of age and males by three [9]. Krill shed
their outgrown exoskeleton known as a
moulting process. They moult in order to
grow, while their new shell is still soft and
in times when they shrink due to lack of
food[10].
Antarctic krill’s biophysical make
up is important for their survival.
They withstand the fridge cold wa-
ters of the Antarctic and expend
large amounts of energy constantly
swimming up and down the depths
and lengths of the Antarctic Ocean.
If Antarctic krill stops swimming,
their higher than water body density
would make them sink [8].
Euphausia superba (Antartic krill)

11 KRILL OIL CONCENTRATE
Krill oil is a pure, natural source of
eicosapentaenoic (EPA) and docosa-
hexaenoic (DHA) omega-3 fatty acids,
phospholipids (with choline), and astax-
anthin. This combination of important
nutrients extracted from Antarctic krill
distinguishes it from fish oil and is the
basis for krill oil’s uniqueness. Its natu-
rally occurring antioxidant astaxanthin
is responsible for the dark red color of
krill oil. In contrast, fish oil contains no
astaxanthin, and their omega-3 fatty ac-
ids are incorporated into triglycerides.
There is increasing evidence
that the differences between the mo-
lecular forms of omega-3 fatty acids
(triglycerides and ethyl-esters in fish
oil, and phospholipids in krill oil) are im-
portant. The phospholipid form (from
krill oil) has been shown to facilitate
the incorporation of omega-3 fatty
acids into tissues in a more effective
and efficient manner compared to tri-
glycerides and ethyl-esters (from fish
oil) [14]. Therefore, it is thought that a
lesser amount of omega-3 fatty acids
can be taken with krill oil compared to
fish oil in order to get the same amount
of omega-3 health benefits. Moreover,
there is evidence which points to phos-
pholipids (and choline) itself having
many health benefits.
Krill Oil Concentrate
Astaxanthin contained in krill is
a highly potent antioxidant and
accounts for krill oil’s red color
[11]. It assists in keeping the ome-
ga-3 fatty acids in krill oil stable.
In cells, it provides protection
against free radical attack and
it has been shown to normalize
oxidative stress in persons such
as those that are smokers or are
overweight. As a result, astaxan-
thin has been linked to health bene-
fits such as anti-inflammatory and
pain-relieving effects, faster re-
covery from exercise, UV light pro-
tection in the skin [12], aging and
age-related diseases, liver, heart,
eye, joint, and prostate health [13].

12 KRILL OIL CONCENTRATE
Phospholipids have two fatty acids
bound to a glycerol backbone, while
triglycerides, or triacylglycerols, are a
combination of three fatty acids with a
glycerol backbone. Fatty acid ethyl es-
ters are derived by a chemical process
to exchange the glycerol backbone of a
triglyceride with ethanol, an alcohol.
Each of krill oil’s major components
(phospholipids, choline, and omega-3
fatty acids) have shown to have effects
in the body’s cells and tissues. This is
thought to be the basis of its health
benefits in many bodily systems and
health conditions.
Fatty acids are important nu-
tritional elements of cells, and in partic-
ular phospholipids and omega-3 fatty
acids are essential in cell membrane
structure and function. They also play
an important role in the formulation of
lipoproteins, while their metabolites
serve as vital molecules within path-
ways of the body. For example, they can
modify molecules involved in inflam-
mation (cytokines), eicosanoids, gene
expression, and plasma triglyceride
synthesis, to name a few. Both omega-3
fatty acids and phospholipid deficien-
cies can be associated with damaged
cell structure and decreased fluidity,
which can result in cell dysfunction.
Cellular dysfunction has been linked to
health conditions of the heart, brain,
liver, joints, etc. Therefore, it is thought
that providing more phospholipids and
omega-3 fatty acids with krill oil con-
centrate will result in better cell func-
tioning and ultimately better health
benefits compared to other krill and
fish oil products.
Indeed, the importance of the
amount of phospholipids in krill oil was
shown in a comparison study of two krill
oils containing either a low (600 mg; LPL)
or a high (1200 mg; HPL) phospholipid
amount with the same omega-3 fatty acid
content of 600 mg [15]. LPL, HPL, or con-
trol oils were given to healthy male and
female volunteers for 4 weeks. At study
end, both plasma and red blood cell fatty
acid compositions were compared for the
different treatment groups. While both
the LPL and HPL groups showed signifi-
cantly increased plasma omega-3 levels
when compared to the control group,
there was no statistical difference be-
tween the LPL and HPL groups. However,
when incorporation into membranes was
compared, then LPL only changed EPA
in red blood cells, whereas HPL changed
both EPA and DHA. And the red blood cell
membrane EPA and DHA incorporation
was significantly higher in the HPL group
when compared to the LPL participants.

13 KRILL OIL CONCENTRATE
FISH OIL
Omega-3 fatty acids EPA/DHA
Choline
Phosphatidylcholine
KRILL OIL
Phospholipids
Composition Krill oil Krill oil concentrate
Total phospholipids ≥40 ≥56
Choline ≥5 ≥7
Total omega-3 fatty acids 24 ≥27
EPADHA
≥12≥5,5
≥15≥7
Table 1: Typical content values (g/100g oil) for krill oil and krill oil concentrate.
Major components of krill oil and fish oil
Astaxanthin
Increasing the amount of phospholipids
in krill oil increases the incorporation of
EPA and DHA into membranes [15].
Since incorporation into red blood cells
relates to long-term and tissue absorp-
tion in general [16], and therefore health
benefits, an increased amount of ome-
ga-3 phospholipids will improve the ef-
fects of krill oil.
Hence, to profit from increased mem-
brane incorporation rates, a new prod-
uct advancement of a highly purified
and concentrated version of krill oil
was developed. It was made possible
by a specialized ion-exchange tech-
nology, Flexitech™, that also reduces
the TMA/TMAO (an osmolyte and pro-
tein sta bilizer) and the salt content of
the oil. This results in a product with a
con centrated amount of omega-3 fatty
acids, phospholipids, and astaxanthin,
which is almost taste- and smell-free
(see Table 1).
TriglyceridesOmega-3fatty
acids EPA/DHA

14 KRILL OIL CONCENTRATE
Sourced from the pristine
waters of the Southern Ocean around
Antarctica and due to its low position in
the food chain, krill oil is virtually free of
toxins and heavy metals. Superba™ krill
oil is certified by the Marine Steward-
ship Council (MSC) as being sustainable
and 100% traceable, from sea to shelf,
with the GPS coordinates to prove it.
Trimethylamine (TMA) has a ‘fishy’
odor and gives the characteristic odor
to seafood. Humans can convert TMA
in the liver to trimethylamine oxide
(TMAO).

15 KRILL OIL CONCENTRATE
Several articles on health benefits of
krill oil supplementation in both ani-
mals and humans have been published
over the years and positively changed
health parameters are presented in
more detail in the section on Krill oil
in health and disease. The very latest
krill oil science has emerged in the new
areas of sports nutrition and skin.
SPORTThe immune system is a complex inter-
play of cells, tissues and organs to sup-
port tissue repair and prevent invasion of
the body by bacteria, parasites, viruses,
and fungi. Omega-3 fatty acids enhance
the immune function by mixing into im-
mune cell membranes, which reduces the
amount of the pro-inflammatory fatty
acid, arachidonic acid. The incorporation
of omega-3 fatty acids instead promotes
the formation of the less potent EPA and
DHA-derived inflammatory mediators.
The immune-enhancing properties of
omega-3 fatty acids might particularly
help in situations where the immune sys-
tem function is reduced. Such a compro-
mised immune system can occur after
heavy training and sports competitions,
where the risk for infection is increased,
especially for upper respiratory tract in-
fections of athletes.
It is true that moderate exercise in
comparison to a sedentary lifestyle
lowers the risk of upper respiratory
tract infections (URTI). However, high
intensive exercise can have immune
system modulating effects that weak-
en the defense mechanisms of a recov-
ering body [6].
The relationship between exercise in-
tensity and risk of URTI was s hown in a
graph by Professor Nieman [17].
Latest Krill Oil studies

16 KRILL OIL CONCENTRATE
The immune system changes after
heavy exercise include a decrease of in-
terleukin 2 (IL-2) and interferon gamma
(IFN-γ), molecules that can regulate the
activity of immune cells. Likewise, nat-
ural killer (NK) cell function was shown
to be decreased after heavy exercise.
NK cells are the first line of defense by
reacting quickly to e.g. intruding bacte-
ria and viruses to keep them under con-
trol until the antigen-specific immune
system starts to act. Their activity can
be decreased by up to 60% for several
hours after extended exercise [17]. This
has led to the view that after intense
training or sport competitions, there is
an open window of 1-9 hours with low-
ered host defense, which increases the
likelihood for an infection.
Omega-3 supplementation has
been shown to increase IL-2 and INF-γ
production, as well as NK cell function
and might therefore help to increase host
protection after exercise.
It has been recommended by
Simopoulos that athletes at a leisure
level should eat up to 2 grams of fish oil
per day in a 2:1 ratio of EPA to DHA [18].
Athletes at a competition level should
probably consume even more omega-3
fatty acids to fully benefit from the im-
mune-modulatory effects. In a study of
106 German winter elite endurance ath-
letes, only one athlete was within the
optimal omega-3 target range that low-
ers the risk for cardiovascular events
and suboptimal brain function (reaction
time and executive function) [19]. These
surprisingly low omega-3 levels, which
were even lower than in heart disease
patients [20], may be explained by the
high need of energy of an athletes’ body
that might use these essential fatty ac-
ids as an energy source.
Omega-3 supplementation might there-
fore be crucial to help athletes to opti-
mize their physical and mental perfor-
mance, also in hindsight that EPA and
DHA have the ability to decrease heart
rate and oxygen consumption during
exercise [21].
The potential of krill oil to strengthen
the immune function after a simulat-
ed cycling time trial has been tested
in both male and female participants
[22]. The study was conducted at the Uni-
versity of Aberdeen, Scotland under the
supervision of Dr Stuart Gray, Senior Lec-
turer in Exercise Physiology.
The Omega-3 index, a mea-
sure of the percentage of EPA and
DHA of total fatty acids in red blood
cells, was measured after 6 weeks of
either 2 grams daily krill oil or placebo
consumption. The results showed that
those participants administered krill oil

17 KRILL OIL CONCENTRATE
Active people need omega-3 fatty acids
had a statistically significant increase
of their Omega-3 index.
After 6 weeks of study prod-
uct supplementation, the volunteers
performed an incremental maximal ex-
ercise test on a cycle ergometer. Par-
ticipants cycled at 70 revolutions per
minute with workload increasing by 30
Watts every minute for males, and 20
Watts every minute for females, until
volitional exhaustion.
Immune function parameters, like cell
signaling molecule production (IL-2, IL-
4, IL-10, IL-17 and IFN-γ) and the ability
to destroy target cells by NK cells were
measured at baseline and in the recov-
ery period after exercise (post-exer-
cise, 1h and 3h).
The results demonstrated
that supplementation of the diet with 2
grams per day of krill oil for 6 weeks can
significantly increase the production of
IL-2 and increase the toxic effect of NK
cells on other cells in the recovery pe-
riod after exercise. The effect was gen-
der-independent.
Study coordinator, Dr Stuart Gray com-
ments: “Our study is in agreement with
our previous work with fish oil, where
we have observed similar results. How-
ever, the krill oil EPA and DHA dose used
was only a quarter from the dose given
in the earlier fish oil study. It remains
to be proven if the different structural
form (omega-3 phospholipids from krill
oil versus omega-3 triglycerides from
fish oil) can explain this difference.”
Moreover, a previous dou-
ble-blind 6-week study on krill oil sup-
plementation to the Polish National
Rowing Team has shown that krill oil can
affect levels of pro- and anti-oxidant bal-
ance markers [23]. Study authors found
that exercise significantly increased
values of oxidative stress parameters
in both groups, but recovery levels were
significantly lower in athletes receiving
1 gram krill oil per day compared to the
control group. Based on these results
they concluded that supplementation
with krill oil in trained rowers dimin-
ished post-exercise oxidative damage

18 KRILL OIL CONCENTRATE
to red blood cells during recovery.
Overall, several sport studies
including omega-3 fatty acids highlight
the importance of an adequate ome-
ga-3 fatty acid intake for athletes.
The ability of krill oil to positively influ-
ence oxidative stress and immune func-
tion shows that regular consumption
of omega-3 phospholipids from krill oil
might be an effective nutritional strate-
gy to help athletes in the post-exercise
recovery phase.
Krill oil supplementation has beneficial
effects on oxidative stress and immune
function and can help to improve a bal-
anced sports nutrition for athletes.
SkinSkin is the organ that not only protects
against microbes, pollution, and phys-
ical assaults, it is further important
for sensory perception and
in maintaining the body’s wa-
ter content and temperature.
It consists of several layers.
The epidermis is towards the
outside, with the top cell layer
called the stratum corneum,
which mainly consists of dead
cells and oils. The body sheds
the dead cells with a rate of up
to 40 000 cells per hour. This
can amount to as much as 3.6 kg of dead
skin cells in a year. Under the epidermis
lies the dermis as an inside layer in-
cluding sweat glands, hair follicles, and
nerve endings needed to feel tempera-
ture, pressure, and pain.
The stratum corneum is im-
portant in preventing water loss to
keep the underlying living cells moistur-
ized. If its barrier function is disturbed,
the skin can become dry and flakey. Hot
water, soaps, medication, low humidity,
and medical conditions can all lead to
dry, irritated skin. For example, eczema
is characterized by dry, red skin patches
that can be very itchy, which might be
due to an overactive immune system,
but the exact causes are unknown. Also
in the case of psoriasis it is unknown
why the immune system is not working
properly, which leads to the formation
of excess skin cells that build up in

19 KRILL OIL CONCENTRATE
scales and red, itchy patches.
Healthy skin permits water loss only
to a limited amount. Damaged skin,
such as in atopic eczema, is character-
ized by increased water loss. Krill oil
was shown to alleviate water loss and
dry skin in a 12-week clinical study in
healthy persons.
Both omega-3 fatty acids and
phospholipids are important for skin
health. Deficiency leads to scaling and
dryness of the skin and enhanced tran-
sepidermal water loss (TEWL) [24,25].
TEWL describes the water loss over the
surface of the skin that happens by pas-
sive diffusion. The outer layer of dead
cells makes the skin flexible and elastic,
when it contains enough water. Howev-
er, when the TEWL is high and hydration
low, it becomes hard and rough. Hence,
skin function is negatively affected,
which can lead to discomfort or even
infection.
In general, the skin holds
about 30% of the body’s water and the
dead cells of the stratum corneum and
the lipids ‘waterproof’ the human body.
Water loss and hydration of the stra-
tum corneum is linked to its lipid con-
tent, the generation of new lipids in the
skin, and ultimately the level of damage
to the skin barrier function. A good bal-
ance between the skin’s water content
and the amount of water passing influ-
ences skin elasticity, smoothness, and
roughness and is crucial in maintaining
healthy skin [26].

20 KRILL OIL CONCENTRATE
The skin has several functions, but one
of the most critical ones is to maintain
the body’s water levels and to limit wa-
ter loss into the surroundings. Water
makes up 75 (infants) to 55% (elder-
ly) of the body’s weight and is vital for
biological processes and life. A way to
measure water loss is to assess trans-
epidermal water loss (TEWL).
In contrast to e.g. saturated
fatty acids and cholesterol, EPA and DHA
cannot be made in the skin and must be
obtained from outside sources. The skin
lacks the enzymes needed to convert
short-chain omega-3 fatty acids into the
longer chain EPA and DHA [27]. Omega-3
fatty acid levels in human skin are rather
low with under 2% of total skin fatty ac-
ids. However, significant increases can
be achieved by supplementation and 3
months of 4 grams daily EPA increased
skin EPA 8 times [28].
Krill oil is an attractive dietary
supplement that might help in the mainte-
nance of skin health and treatment of skin
disorders by both its omega-3 and phos-
pholipid components (see above ).
To explore the effects of krill
oil on skin health, 31 volunteers (mid-
dle-aged men and women with normal
skin) were included in an open label,
two-armed clinical trial (unpublished re-
sults). The subjects were randomized to
take 3 grams daily krill oil for 13 weeks.
All skin measurements were done on the
upper forearm and showed that krill oil
intake resulted in a significant increase
in skin hydration and elasticity, as well
as in a significant reduction in TEWL.
In addition, a significant cor-
relation for the change in hydration
and the changes both for elasticity and
TEWL were found. Meaning that the
volunteers that had a high change in
skin hydration also experienced a high
Changed lipid levels in the skin Modulation of inflamation Increased hydration Decreased water loss Improved elasticity Improved smoothness
KRILL OIL
Changed lipid levels in the skin Increased hydration Decreased water loss
Omega-3 effect
Phospholipid effect

21 KRILL OIL CONCENTRATE
change for both elasticity and TEWL.
By using a digital camera, the amount of
wrinkles (as a measure for roughness)
and width and size of wrinkles (as a mea-
sure for smoothness) were assessed at
the start and end of the trial. For both
parameters, i.e. roughness and smooth-
ness, there was a significant beneficial
change observed after krill oil supple-
mentation.
By increasing the amount of
omega-3 fatty acids in the body, krill
oil has the ability to not only influence
skin hydration and elasticity, but also
the amount and size of wrinkles. The
measure of how much omega-3 accumu-
lates in the body, given as the Omega-3
index, was increased significantly in the
study and correlated with the above
mentioned parameters. These results
indicate that the increases in Omega-3
index by krill oil supplementation di-
rectly relate to the positive changes in
skin parameters observed among study
subjects.
Krill oil improves skin parameters
22 KRILL OIL CONCENTRATE
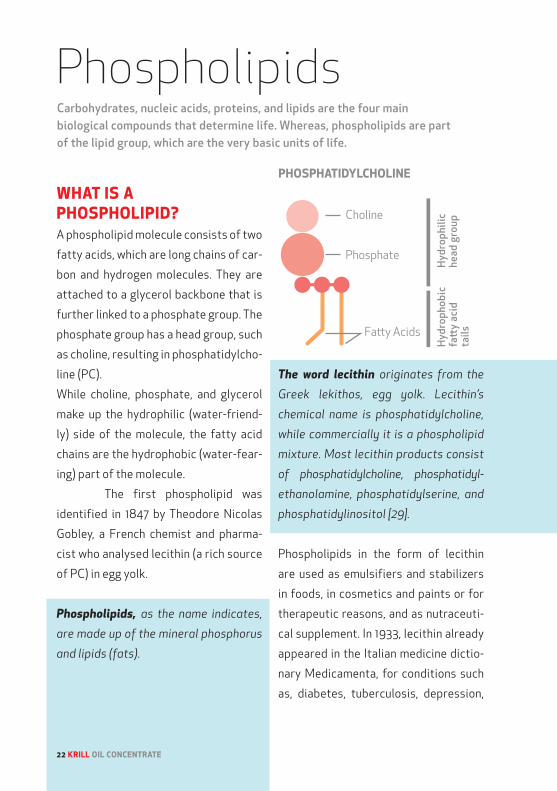
WHAT IS A PHOSPHOLIPID?A phospholipid molecule consists of two
fatty acids, which are long chains of car-
bon and hydrogen molecules. They are
attached to a glycerol backbone that is
further linked to a phosphate group. The
phosphate group has a head group, such
as choline, resulting in phosphatidylcho-
line (PC).
While choline, phosphate, and glycerol
make up the hydrophilic (water-friend-
ly) side of the molecule, the fatty acid
chains are the hydrophobic (water-fear-
ing) part of the molecule.
The first phospholipid was
identified in 1847 by Theodore Nicolas
Gobley, a French chemist and pharma-
cist who analysed lecithin (a rich source
of PC) in egg yolk.
Phospholipids, as the name indicates,
are made up of the mineral phosphorus
and lipids (fats).
The word lecithin originates from the
Greek lekithos, egg yolk. Lecithin’s
chemical name is phosphatidylcholine,
while commercially it is a phospholipid
mixture. Most lecithin products consist
of phosphatidylcholine, phosphatidyl-
ethanolamine, phosphatidylserine, and
phosphatidylinositol [29].
Phospholipids in the form of lecithin
are used as emulsifiers and stabilizers
in foods, in cosmetics and paints or for
therapeutic reasons, and as nutraceuti-
cal supplement. In 1933, leci thin already
appeared in the Italian medicine dictio-
nary Medicamenta, for condi tions such
as, diabetes, tuberculosis, depression,
PhospholipidsCarbohydrates, nucleic acids, proteins, and lipids are the four main biological compounds that determine life. Whereas, phospholipids are part of the lipid group, which are the very basic units of life.
22 KRILL OIL CONCENTRATE

23 KRILL OIL CONCENTRATE
and recovery from infec tious diseases
[30].
FUNCTIONS OF PHOSPHOLIPIDS IN THE BODYPhosphorus, found in the head group
of phospholipids, contributes to the
normal function of cell membranes, en-
ergy-yielding metabolism, and in bones
and teeth [31]. The phospholipid mol-
ecule has many functions and uses in
the body. For example , as a structural
element in cell membranes, a source of
choline for the neurotransmitter acetyl-
choline, an important factor in energy
production and storage, assisting in blood
clotting, antioxidant protection, and
cholesterol solubility to name just a few.
Moreover, it acts as surface-active wet-
ting agent that lines the outside of liver,
lungs, gastrointestinal tract, and kidney
cells.
CELL MEMBRANESThe structural skin around cells and
their organelles is called a membrane.
A phospholipid membrane is only five
millionths of a millimeter thick [32].
10,000 membranes on top of each other
have the same thickness as a piece of
paper.
Both the inside and the outside of
cells is water. When phospholipids are
exposed to water, they arrange them-
selves into a two-layered sheet (a bi-
layer) with all of their hydrophobic tails
pointing towards the center of the sheet
and the hydrophilic heads towards the
surrounding water.
The amount of phospholipids in the hu-
man body is enormous! The body con-
tains over 100 trillion cells with mem-
branes, consisting of phospholipids,
and proteins. The liver itself consists
of membranes that can fill four soccer
fields.
About 60% of what is made in a cell is
needed for membrane structures, either
for channels and receptors inside the
membrane or proteins attached on the
outside of membranes [33]. Membranes
not only give a defined volume to a cell,
they also allow for internal structures,
such as organelles (e.g. nucleus) and
transport vesicles between organelles.
It is important that our cells
maintain a sufficient amount of phos-
pholipids to ensure optimal cell func-
tion. Otherwise many cell functions can
be compromised, such as their ability to
control the exit of waste and the entry
of nutrients into cells, communication

24 KRILL OIL CONCENTRATE
between cells, membrane-bound en-
zyme functions, binding of molecules
(neurotransmitters, antigens, antibod-
ies, etc.) to receptors, and more.
Two of the many factors which
may affect the amount of phospholipids
in cells are, i) as we age phospholipid
amounts in cells decrease, and ii) cells
in skin, lungs, liver, heart, and blood
vessels can become vulnerable to at-
tack from free radicals and toxins [34].
Therefore, damaged and lost phospho-
lipids must be continuously replaced to
ensure optimal cell function and health.
Phospholipids with their unique po-
sition in cell walls are essential for
cell growth and the generation of new
cells. They promote molecule trans-
port across membranes, binding to
receptors and enzyme activities and
determine the fluidity of membranes.
They are a source of messengers in cell
signaling, choline, omega-3 fatty acids
and contain phosphate for energy pro-
duction. Moreover, they are needed in
fat emulsification in the stomach and
blood clotting.
LIPID TRANSPORT AND CHOLESTEROL METABO-LISMIn addition to the central role of phos-
pholipids in membrane function, they
are, together with apoproteins, part of
the outer layer of transport vehicles,
called lipoproteins, because they are
made of fat (lipid) and proteins. This
combination of solubilizers allows the
transport of cholesterol in the wa-
ter-based bloodstream. Cholesterol is
important for cell membrane function
and as precursor for other compounds.
However, in high amounts, it will accu-
mulate on and in blood vessel walls and
make them narrower and stiffer. The
hardening of arteries via the buildup

25 KRILL OIL CONCENTRATE
of cholesterol and fat plaques is called
atherosclerosis. If these plaques burst,
they can lead to blood clots that can
cause heart attacks and stroke.
By forming monolayers, phos-
pholipids surround all lipoproteins that
are classified according to their density
in chylomicrons, VLDL (very low-den-
sity), LDL (low-density), IDL (interme-
diate-density) and HDL (high-density)
particles. Whereas large lipoproteins
have low density and contain more fat
than protein. In short, cholesterol is
taken up in the small intestine and is
delivered to the liver in packages called
chylomicrons. VLDL and LDL are se-
creted by the liver and are risk factors
for atherosclerosis and heart disease
by providing cholesterol to plaques.
LDL is therefore often called the ‘bad’
cholesterol. In contrast, HDL, the ‘good’
cholesterol, has a protective effect by
removing excess cholesterol from the
arteries and bringing it back to the liver
on the ‘reverse transport pathway’.
Every 1% increase in blood HDL levels
has been associated with a 2-3% reduc-
tion in overall heart disease risk [35].
The levels of cholesterol in blood pri-
marily depends on the amount of cho-
lesterol that is ingested (from diet and
bile) or made by the liver. The absorp-
tion rate of cholesterol in the gut, can
vary substantially [36]. It is influenced
by the amount of phospholipids avail-
able, since phospholipids are needed for
the intestinal uptake of cholesterol, but
high amounts of phospholipids reduce
cholesterol absorption through molec-
ular interactions. Indeed, it was found
that a dose of 15mg lecithin can inhibit
cholesterol absorption by 50% in rat
guts [37]. There is also evidence for re-
duced intestinal cholesterol absorption
in the gut of humans after phospholipid
supplementation [38-40].
Research has shown that dietary phos-
pholipids may help to reduce blood LDL
particles, the ‘bad’ cholesterol and re-
duce the risk of heart disease by affect-
ing intestinal cholesterol uptake.

26 KRILL OIL CONCENTRATE
UPTAKE OF PHOSPHOLIPIDSDietary phospholipids are efficiently
(above 90%) taken up into the cells of the
intestinal wall after they are hydrolyzed
to lysoPC and free fatty acids by lipases
in the small intestine. In the intestinal
cells, they are reassembled and included
into chylomicrons for further transport
via the lymph and blood. Some studies
suggest that a fraction of the dietary
phospholipids is directly taken up into
HDL particles already in the intestine,
which later join the HDL blood pool.
Phospholipids move into cells
and their membranes by selective and
whole particle uptake routes. In liver
cells, about two-thirds of the phospho-
lipid uptake is by selective entry routes.
Thereby, phospholipids are transferred
directly from lipoproteins into the cell
membrane. In addition to selective up-
take pathways, cells can incorporate
entire lipoproteins by endocytosis,
which results in an unspecific incorpo-
ration of everything that was part of
the particle, including phospholipids.
Incoming phospholipids can be metab-
olized to triglycerides and can be used
in storage or energy generation, when
not used in membranes.
PHOSPHOLIPID SOURCESDaily phospholipid intake is usually be-
tween 2-8 grams, which corresponds
to 1-10% of the daily fat consumption
[41]. Phospholipids can be found in high
quantities in egg yolk, soybean, meat,
fish and internal organs, while fruits,
vegetables and grains have a much low-
er phospholipid content [42]. However,
the richest sources usually also have a
high content of fat and cholesterol.
Also krill contains high amounts of
phospholipids and E. superba is known
to use them as energy storage form. In
“Illustration provided and modified courtesy of the National Heart, Lung, and Blood Institute’s The Heart Truth® Program.”
27 KRILL OIL CONCENTRATE
the extracted krill oil concentrate, over
56% of the oil consists of phospholip-
ids.
PHOSPHOLIPID DEFICIENCYNot much is known about the optimal
intake levels of phospholipids, since
phospholipid deficiency symptoms are
unknown, except the ones associated
with choline deficiency that are de-
scribed later on. However, due to refine-
ment of oils and fats, cleaned raw ma-
terials, and changes towards a nutrition
low in fat and cholesterol, modern diets
contain only about one third of phos-
pholipids than what they contained a
century ago [43]. In particular, high-risk
groups for deficiency, such as the elder-
ly, athletes and diseased persons might
therefore benefit from phospholipid
supplementation.
PHOSPHOLIPIDS IN HEALTH AND DISEASEAlthough dietary phospholipids are
present in many foods, purified forms
can help to treat various health con-
cerns, including fatty liver, arthritis,
heart disease, cachexia, hypercholes-
terolemia, cancer, and more [44]. Major
health benefits of phospholipid sup-
plementation are presented in Table
2 that underlie their liver-protective,
anti-inflammatory, immune changing,
anti-obesity, memory enhancing, an-
ti-depressant, and anti-tumor effects
[45]. Their effects on liver health and
physical performance, are outlined in
more detail below.
LIVERThe liver is one of the organs that get
the most membrane damage because
of its blood filtering function. It deals
with incoming food nutrients and ei-
ther stores or prepares them for fur-
ther transport to other organs. It is
also responsible for filtering the blood
from harmful substances such as tox-
ins, alcohol, medication, fatty food,
waste products, viruses, etc. These are all
stressors for the integrity of the hepatic
membrane and fat accumulation or alco-
hol misuse can take its toll on the liver
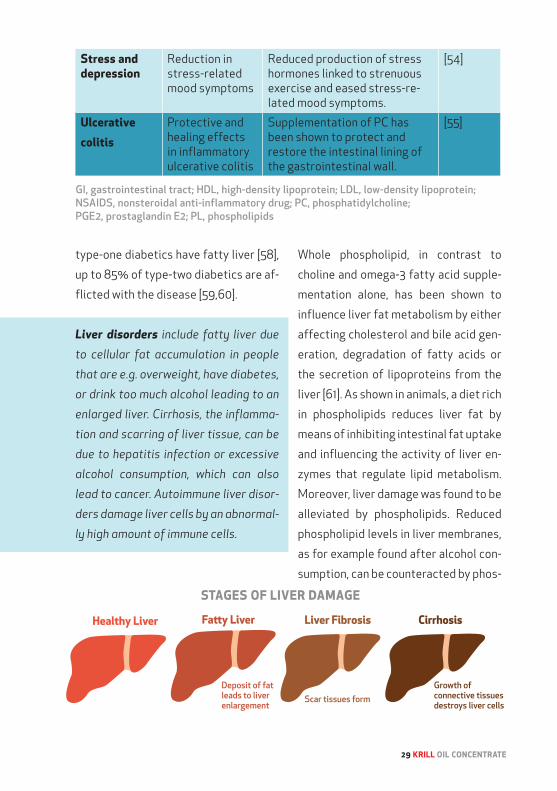
and eventually lead to fatty liver disease
that can progress into cirrhosis and liver
failure.
While studying 700 obese
children, it was found that 15% (10%
girls, 22% boys) of the children already
had fatty liver disease [56]. Overall, the
prevalence of suspected nonalcoholic
fatty liver disease lies at 50% of obese
males in the U.S. [57]. While 45% of

28 KRILL OIL CONCENTRATE
Table 2: Dietary phospholipid (PL) and choline health benefits.
Health area Benefit Explanation Referenc-es
Heart disease Reduced cardiovascular risks
PL improve parameters related to heart and cardiovascular diseases:• Blood lipid profiles (reduction of total cholesterol, LDL and TG levels and increased HDL levels) • Reduced hypertension • Reduced platelet aggregation and the risk of arteriosclerosis
[46-48]
Immune system
Improvement ofimmunological function
PL-induced improvement in phagocytosis, arachidonic acid concentration and neutrophil killing activity.
[49]
Infant development
Improved braindevelopment of fetus
Choline supplements during pregnancy have been shown to affect brain development of fetus and improve lifelong memory characteristics (animal studies).
[50]
Liver disease Improved hepat-
ic disorders
Reduced alcohol-induced liver damage and hepatic damage caused by toxins and virus infections (hepatitis).
[51]
Physical performance
Improved phys-ical performance by reduction of physical stress
PL stimulates acetylcholine synthesis, which triggers the release of neurotransmitters in the brain, thus improving physical performance.
[52]
Stomach and gastrointesti-nal tract (GI)
Reduction of stomach pain in-duced by gastric acid
PL-induced protection of the GI by reduced gastric mucosal lesions. Typical GI side effects of analgetic drugs (NSAIDS) are reduced, likely due to an increased production of cyto-protective mucosal PGE2.
[53]
29 KRILL OIL CONCENTRATE
type-one diabetics have fatty liver [58],
up to 85% of type-two diabetics are af-
flicted with the disease [59,60].
Liver disorders include fatty liver due
to cellular fat accumulation in people
that are e.g. overweight, have diabetes,
or drink too much alcohol leading to an
enlarged liver. Cirrhosis, the inflamma-
tion and scarring of liver tissue, can be
due to hepatitis infection or excessive
alcohol consumption, which can also
lead to cancer. Autoimmune liver disor-
ders damage liver cells by an abnormal-
ly high amount of immune cells.
Whole phospholipid, in contrast to
choline and omega-3 fatty acid supple-
mentation alone, has been shown to
influence liver fat metabolism by either
affecting cholesterol and bile acid gen-
eration, degradation of fatty acids or
the secretion of lipoproteins from the
liver [61]. As shown in animals, a diet rich
in phospholipids reduces liver fat by
means of inhibiting intestinal fat uptake
and influencing the activity of liver en-
zymes that regulate lipid metabolism.
Moreover, liver damage was found to be
alleviated by phospholipids. Reduced
phospholipid levels in liver membranes,
as for example found after alcohol con-
sumption, can be counteracted by phos-
Stress and depression
Reduction in stress-related mood symptoms
Reduced production of stress hormones linked to strenuous exercise and eased stress-re-lated mood symptoms.
[54]
Ulcerative colitis
Protective and healing effects in inflammatory ulcerative colitis
Supplementation of PC has been shown to protect and restore the intestinal lining of the gastrointestinal wall.
[55]
GI, gastrointestinal tract; HDL, high-density lipoprotein; LDL, low-density lipoprotein; NSAIDS, nonsteroidal anti-inflammatory drug; PC, phosphatidylcholine; PGE2, prostaglandin E2; PL, phospholipids
30 KRILL OIL CONCENTRATE
pholipid supplementation. Accordingly,
a study on chronic alcohol consumption
in baboons that were given either ethanol
or ethanol together with lecithin over 6.5
years reported that PC protects against liv-
er fibrosis and cirrhosis [62]. But also other
liver damages like e.g. from viral infections,
can benefit from phospholipid supplemen-
tation to decrease disease activity [63].
Fat accumulation in the liver will often not
lead to symptoms indicating that some-
thing is wrong. Inasmuch, fatty liver silently
increases heart disease risk 3 times in men,
14 times in women and up to 10 times in
type-one diabetics [64].
The majority of the studies performed
with phospholipids, did not include ome-
ga-3-containing phospholipids, indicating
that phospholipids in general have benefi-
cial effects. However, other studies have
demonstrated that phospholipids contain-
ing omega-3 fatty acids have more potent
effects on liver and blood plasma lipid
levels, compared to phospholipids without
omega-3s [65,66].
In particular, Shirouchi and col-
leagues have concluded in their study on
rats that the combination of omega-3 fatty
acids with phospholipids in comparison to
egg phospholipids alone can alleviate liver
steatosis better through the suppression of
fatty acid synthesis, enhancement of fatty
acid degradation, and increase of serum ad-
iponectin levels [66].
BRAINPhospholipids play a central role in brain
function and around 60% of the brain by
weight consists of phospholipids. Phos-
pholipids are particularly enriched in
dendrites and synapses and it has been
shown in vitro that nerve growth increas-
es the demand for phospholipids. Nerve
growth factor, a small protein controlling
nerve growth and maintenance, also stim-
ulates phospholipid generation [67].
The omega-3 fatty acid DHA can
only to a very little extent be made by the
brain, and must therefore be supplied by
the blood and imported over the blood-
brain barrier. Phospholipids are of utmost
importance in the transport of DHA, since
the recently discovered DHA transporter
(Mfsd2a, major facilitator super family
domain containing 2a) accepts DHA only
if it is bound to phospholipids; to be exact
to lysoPC [68]. Mice that are genetically
engineered to not have this transporter,
have very low DHA amounts in the brain
leading to neuronal cell loss and cognitive
deficits associated with severe anxiety.
In addition, humans identified with muta-
tions in Mfsd2a present defective brain
growth and intellectual disability due to
31 KRILL OIL CONCENTRATE
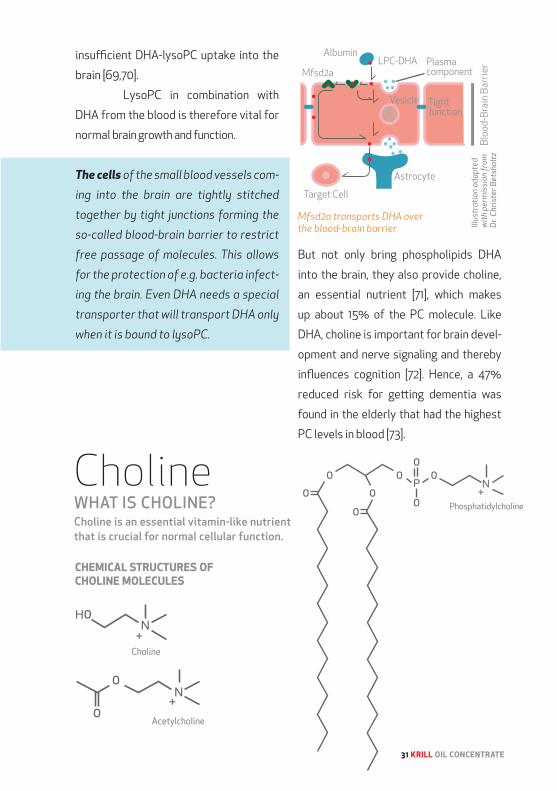
insufficient DHA-lysoPC uptake into the
brain [69,70].
LysoPC in combination with
DHA from the blood is therefore vital for
normal brain growth and function.
The cells of the small blood vessels com-
ing into the brain are tightly stitched
together by tight junctions forming the
so-called blood-brain barrier to restrict
free passage of molecules. This allows
for the protection of e.g. bacteria infect-
ing the brain. Even DHA needs a special
transporter that will transport DHA only
when it is bound to lysoPC.
But not only bring phospholipids DHA
into the brain, they also provide choline,
an essential nutrient [71], which makes
up about 15% of the PC molecule. Like
DHA, choline is important for brain devel-
opment and nerve signaling and thereby
influences cognition [72]. Hence, a 47%
reduced risk for getting dementia was
found in the elderly that had the highest
PC levels in blood [73].
Choline WHAT IS CHOLINE?Choline is an essential vitamin-like nutrient that is crucial for normal cellular function.
Mfsd2a transports DHA over the blood-brain barrier Ill
ustr
atio
n ad
apte
d
wit
h pe
rmis
sion
from
D
r. Ch
rist
er B
etsh
oltz

32 KRILL OIL CONCENTRATE
FUNCTIONS OF CHOLINE IN THE BODYCholine as a component of phospha-
tidylcholine, choline plasmalogen and
sphingomyelin is a major component of
cell membranes.
95% of choline in the body is found in
phospholipid form as phosphatidylcho-
line (PC).
The derivatives of choline are ver-
satile and include functions such as
neurotransmitters (acetylcholine),
cell membrane signaling (phospholip-
ids), lipid transport (lipoproteins), and
methyl-group metabolism (homocys-
teine reduction) [74]. Besides, a fetus
depends on choline for brain and mem-
ory development [75] and to reduce the
risk for neural tube defects [76]. A lot of
the maternal choline goes to the fetus,
which might deplete the mother’s cho-
line reserves.
NERVE SIGNALINGCholine is converted to acetylcholine,
a neurotransmitter, in the nervous sys-
tem. Acetylcholine is of importance in
learning, breathing, memory, sleep, and
muscles metabolism. Whereas in heart
tissue, acetylcholine has an inhibitory
effect and leads to reduced heart rate,
in skeletal muscle it has the opposite
effect.
CELL SIGNALINGCholine is a part of the phospholip-
ids phosphatidylcholine and sphin-
gomyelin. They are the precursors of
diglycerides and ceramides, which are
lipid-signaling molecules in cells. Lipid
messengers can freely cross over mem-
branes and can therefore not be stored
in vesicles. They act locally on recep-
tors and enzymes to induce a specific
cellular response.
METHYL DONORCholine is required for the metabolism
of nucleic acids and amino acids and is
an important source of methyl (-CH3)
groups over the generation of S-ad-
enosylmethionine (SAMe). Up to 50
chemical reactions in mammals depend
on SAMe as a methyl donor [77]. These
methylation reactions are of impor-
tance in lipid biosynthesis, regulation Choline is important in nerve signaling

33 KRILL OIL CONCENTRATE
Betaine
Acetylcholine Neurotransmitter
S-adenosylhomocysteine
Phosphatidyl-ethanolamine
Methionine
Dimethylglycine
Brain HealthLiver Health
Brain Functions Memory
Homocysteine Related to heart
disease
Phosphatidyl-choline
Important componment of cell menbranes
S-adenosylmethionine
Important in control of DNA replication and cell growth
CHOLINE
Heart Health
of metabolic pathways, and detoxifica-
tion. Changes in DNA methylation, that
affects gene expression, have been
linked to cancer.
WATER BALANCECholine is converted to betaine, which
is an osmoregulator, meaning that it can
regulate the volumes and water con-
tent of cells [78]. Cells keep water lev-
els constant by allowing ions to enter,
which makes water to follow and move
into cells. Betaine is an organic water
attractant, in particular in cells with
high osmotic pressure such as kidney or
intestinal cells.
Betaine is further used to convert ho-
mocysteine, a risk factor for heart dis-
ease, to methionine.
UPTAKE OF CHOLINE SALT VERSUS PHOSPHATIDYL-CHOLINE Dietary choline is taken up by choline
transporters in the intestine. Most of the
choline is converted to PC and used in cell
membranes. The liver can recycle choline
and the intestine, lungs, and kidneys will
send choline to the brain and liver in time
of need.
Administration of choline will
significantly increase blood choline con-
Cour
tesy
of w
ww
.cho
linec
ounc
il.co
m

34 KRILL OIL CONCENTRATE
centrations [79,80]. It was found that cho-
line in the form of PC, is 12 times better
in raising human blood choline amounts
compared to choline salt [79,80]. While
choline salt show maximum levels after
30 minutes (86% increase, 4 hours until
normal), PC intake raises choline by 265%
and takes 12 hours until normal again [80].
It was suggested that 60% of the choline
in inorganic salts, such as choline chloride,
choline citrate, and choline bitartrate, is lost
to conversion to TMA by intestinal bacteria
[23]. In comparison, dietary PC leads to
three times less TMA [24].
CHOLINE DEFICIENCYOnly little choline can be made by the
body itself, the major part needs to be
taken up over the diet. Choline is found
in higher amounts in e.g. soybeans, eggs,
liver, beef, and milk. Although most di-
ets are considered to provide sufficient
choline, persons at risk of choline defi-
ciency exist. Specifically, the National
Health and Nutrition Examination Sur-
vey in 2003-2004 has concluded that
90% of the American population has an
inadequate intake of choline [1].
90% of the U.S. population is not con-
suming enough choline to ensure opti-
mal membrane function, neurotrans-
mission, and methyl donor availability.
The adequate intake level for choline
was set at 550 mg/day for men and 425
mg/day for women in sight of prevent-
ing liver damage. Choline deficiency-in-
duced fatty liver can occur, when not
enough choline is present for the for-
Cour
tesy
of w
ww
.cho
linec
ounc
il.co
m
35 KRILL OIL CONCENTRATE
mation of PC molecules that are need-
ed for the formation of VLDL particles.
If the fat becomes stuck in the liver, it
accumulates and will eventually lead
to liver damage. Excessive oxidative
stress that damages lipids and DNA in-
duces cell death and inflammation that
can ultimately culminate in end-stage
liver disease [81]. Choline deficiency is
also the only nutrient deficiency that
can lead to cancer.
Genetic predisposition, gender, and
age influences ones choline needs and
care should be taken to ensure an ade-
quate choline intake, since choline defi-
ciency is linked to an increased risk for
fatty liver, muscle dysfunction, athero-
sclerosis, and neurological disorders
[82].
CHOLINE IN HEALTH AND DISEASEWith its many diverse roles, it is not
surprising that choline deficiency will
cause disease in humans. The function
of many organs such as liver, muscle,
kidney, pancreas, and brain all depend
on an adequate choline intake.
BRAINIt was suggested that supplementation
with choline, as a precursor for acetyl-
choline, improves brain function in per-
sons affected by memory impairments
due to aging or pathological conditions.
Inasmuch, Alzheimer’s and Parkinson’s
disease patients have a reduction of
cholinergic neurons in the grey matter
of their forebrains [83]. Also elderly
persons have reduced forebrain cholin-
ergic neurons and acetylcholine [84]. On
the other hand, choline supplementa-
tion increases the amount of choline in
the blood, with a concomitant increase
of choline-containing compounds in the
brain [85]. However, in an analysis of
all available literature on studies with
lecithin given to individuals with Alzhei-
mer’s disease, Parkinsonian dementia
and subjective memory problems, no
clear benefit for memory performance
could be found for patients with Alz-
heimer’s disease and Parkinsonian de-
mentia [86]. Yet, people with subjective
memory difficulties, gained a very sig-
Choline supplementation might improve brain functions

36 KRILL OIL CONCENTRATE
Choline is important for muscle contractions
nificant benefit in one of the analysed
studies [87]. Thus, while the overall
analysis does not support lecithin for
dementia patients, people with sub-
jective memory complaints may profit
from lecithin supplementation.
SPORTIntense physical activity challenges
cellular functions, which are essential
to maintain for optimal sports perfor-
mance. Excessive radical formation and
trauma to the muscles during high-in-
tensity exercise leads to inflammation.
It has been suggested that supple-
mentation with phospholipids, such as
PC might be beneficial to endurance
athletes, because of the choline head
group [88]. Indeed, decreased blood
choline levels were shown in endurance
athletes such as cyclists and runners
[89]. Supplementation with PC signifi-
cantly increases circulating choline
levels; in fact twelve times better than
choline salts alone [79].
If, during exercise, enough choline is
available in the body, then also sufficient
acetylcholine is produced. Since acetyl-
choline is a signaling molecule important
for muscle contractions, sportive perfor-
mance might therefore be optimized by
PC supplementation.
Acetylcholine is a neurotransmitter im-
portant for muscle contractions made
from choline. The available free choline
influences acetylcholine synthesis rate.
If no choline is supplemented, mara-
thon runners can manifest up to a 40%
decrease in blood choline levels [16,17],
which is similar to the choline reductions
found in cyclists [5,18]. Besides, a study
with lecithin supplementation found fast-
er recovery after a bicycle ergometer tri-
al, when compared to the control group
[26,27]
During intense exercise, free choline is
reduced, which might impact on acetyl-
choline release and therefore sportive
performance.

37 KRILL OIL CONCENTRATE
WHAT ARE OMEGA-3 FATTY ACIDS?The main bioactive omega-3 fatty acids
that have been described extensively
are eicosapentaenoic (EPA or 20:5n-
3) and docosahexaenoic acid (DHA or
22:6n-3). EPA consists of 20 carbons
and 5 double bonds and can be convert-
ed enzymatically into DHA. DHA is the
longest fatty acid chain, with 22 carbons
and 6 double bonds. They are called
omega-3 fatty acids, because they have
their first double bond at three carbon
atoms from the methyl end. In compar-
ison, an omega-6 fatty acid has its first
double bond at 6 carbon atoms from
the methyl end.
FUNCTIONS OF OMEGA-3 FATTY ACIDSAside from being a source of nutritional
energy, the functions of omega-3 fatty
acids have a molecular basis. Inasmuch,
the omega-3 fatty acids have the ability
to change membrane fatty acid com-
position and function, regulate gene
transcription, and alter metabolic and
Omega-3 Fatty AcidsOmega-3 fatty acids played an essential role in human evolution and develop-ment. A turning point for the evolution of human intelligence was the diet change from red meat of animals mainly consumed by the Neanderthals to the inclusion of coastal seafood and inland freshwater sources [90]. This might have initiated the growth of the brain about two million years ago.

38 KRILL OIL CONCENTRATE
signal transduction pathways. This in-
volves a wide array of mechanisms that
overlap and interplay in complicated
metabolic networks that maintain the
body’s equilibrium.
MEMBRANESMost importantly, omega-3 fatty ac-
ids, as well as the overabundant ome-
ga-6 fatty acids, are crucial as building
blocks of membrane structures and a
cell’s development, integrity and func-
tion. The flexible structure of omega-3
fatty acids determines the fluidity of
membranes. Membrane fluidity is im-
portant for the correct functioning of
membrane proteins such as receptors,
ion channels, transporters, and en-
zymes. A change in fluidity due to al-
tered membrane fatty acid composition
will change activities and movements
of these proteins. It will also affect how
extracellular signals are transmitted
from receptors to intracellular signal-
ing networks, which is important in e.g.
neurons, cardiac cells and hormone-se-
creting cells. Additionally, membrane
permeability increases with the number
of double bonds present in fatty acid
chains of membrane phospholipids.
The amount of omega-3 fatty acids that
constitute membrane phospholipids
can be influenced by diet.
GENE TRANSCRIPTION AND ENZYME ACTIVITYWhen omega-3 fatty acids reach cells,
they can activate transcription factors
that stimulate the expression of certain
genes [91-94]. This means that omega-3
fatty acids indirectly influence the pro-
duction of functional gene products
(often proteins) in our cells. The ome-
ga-3 fatty acids thereby influence
which proteins are made in a cell and,
ultimately, how the cellular metabolic
functions are impacted. It is still un-
clear to which extent EPA and DHA bind
specifically to different transcription
factors, but there are at least some in-
dications that there are preferences as
to which fatty acid can regulate which
gene expression [91]. However, not only
can fatty acids change the expression
of genes, they can also modulate en-
zyme activities by directly binding to
them [95,96].
Omega-3 fatty acids influence gene expression

39 KRILL OIL CONCENTRATE
EICOSANOIDSThe ratio of omega-6 to omega-3 fatty
acids is important since they compete
for the same metabolic enzymes that
convert them into eicosanoids (i.e.
prostaglandins, prostacyclins, throm-
boxanes, and leukotrienes). Eicosa-
noids are hormone-like compounds,
called cellular hormones that control
key functions in the body, such as the
central nervous system, immunity, and
inflammation.
Whereas prostaglandins, leu-
kotrienes, and lipoxins play a regulatory
role in inflammation, thromboxanes and
prostacyclins are important for con-
trolling bleeding. Resolvins and protec-
tins, metabolites of EPA and DHA, help
reduce inflammatory responses [97].
In general, eicosanoids from
omega-3 fatty acids are less inflam-
matory than those from omega-6 fatty
acids. Hence, a disturbed ratio with high
omega-6 versus omega-3 fatty acids
and a low omega-3 intake in general
will tip the balance towards the produc-
tion of pro-inflammatory eicosanoids.
Therefore, a replacement of the ome-
ga-6 arachidonic acid by EPA or DHA
may lead to a less inflammatory active
eicosanoid profile, decreasing the risk
for inflammatory diseases.
ENDOCANNABINOIDSThe endocannabinoid system is based
on the action of endocannabinoids
(ECs) that are hormones made from
omega-6 fatty acids. The binding of ECs
to receptors influences the expression
of proteins in organs (e.g. liver, skeletal
muscle, pancreas, intestine, bone, and
adipose tissue) and affects the action
of the central nervous system. There-
by they can influence not only enzyme
activities, but also appetite, energy
balance, mood, memory, pain percep-
tion, stress response, anxiety, immune
functions, and reproductive processes.
An overactive EC system is believed to
promote increased fat mass and var-
ious markers of metabolic syndrome
[98].
The quantities of ECs made, ul-
timately depend on the amounts of ome-
ga-6 arachidonic acid available in mem-
branes, which depends on the amount of
arachidonic acid ingested. Increased in-
take of fatty acids of the omega-3 family
positively influences the ratio of omega-3
to omega-6 fatty acids in blood and or-
gans. In this way, less arachidonic acid is
incorporated into phospholipids, result-
ing in decreased conversion of arachidon-
ic acid to ECs. Thus, dietary fatty acids
constitute a means to change the body’s
fatty acid composition and thereby EC

40 KRILL OIL CONCENTRATE
levels, ultimately affecting membrane
signaling events and leading to changed
energy metabolism (food intake and en-
ergy processing).
OMEGA-3 DEFICIENCYBoth omega-3 and omega-6 fatty acids
are needed for optimal health. Howev-
er, since there is an abundance in the
Western diet of omega-6 fatty acids
compared to omega-3 fatty acids, the
balance between the two is highly dis-
turbed [99,100]. The underlying reason
is the vast increase in the consumption
of vegetable oils rich in omega-6 fatty
acids, which are present in corn, sun-
flower seeds, cottonseed and soybean
and industrially produced meat. At the
same time, the consumption of omega-
3-rich fish has decreased markedly.
The human body has evolved on a del-
icate balance of omega-6 to omega-3
fatty acids. Cells in the body rely on a
specific ratio of these fatty acids in
order to function properly. If out of bal-
ance, health is affected and it is of no
surprise that our modern unbalanced
diet promotes health issues such as
heart disease, arthritis, depression,
and dementia.
Nowadays, the ratio between omega-6
to omega-3 can be as high as 10-20:1,
whereas historically it was as low as
1-2:1 [101]. The recommendations today
call for a ratio of 5:1 [102]. Some studies
further indicate that the optimal ratio
may depend on the disease state [102].
When it comes to heart disease, a ratio
of 4:1 was linked to a reduction of 70%
in total mortality. Rectal cell prolifera-
tion in patients with colorectal cancer
were reduced at a ratio of 2.5:1, while a
ratio of 2-3:1 suppressed inflammation
in patients with rheumatoid arthritis. A
ratio of 5:1 was needed to induce bene-
fits for asthma patients, whereas a 10:1
ratio had negative effects.
The right amount of omega-6
and the right balance between omega-6
to omega-3 fatty acids is therefore
essential for health, as otherwise too
many pro-inflammatory molecules are
produced from omega-6 fatty acids
that can affect disease outcomes.
Most people do not consume
the recommended twice a week of
fatty fish and hardly reach the recom-
mended daily intake doses of EPA and
DHA. Although the recommended daily
dose varies highly between different
countries (1000mg in Japan and South
Korea, 500mg in France, and 450mg in
Norway), most countries recommend
40 KRILL OIL CONCENTRATE

41 KRILL OIL CONCENTRATE
250mg (Austria, Belgium, Czech Re-
public, Denmark, Finland, Germany,
Greece, Iceland, Ireland, Italy, Luxem-
bourg, Netherlands, Portugal, Slovakia,
Slovenia, Spain, Sweden, Switzerland,
and United Kingdom). While Australia
and New Zealand recommend 160mg of
EPA/DHA per day, other countries like
Canada, Hong Kong, Israel, Singapore,
Taiwan, and the United States do not
provide an official recommendation.
Most people have mean intake levels be-
low the optimal daily EPA and DHA dose
of 250mg recommended by the World
Health Organization (WHO) and the Euro-
pean Food Safety Authority (EFSA) and
could therefore benefit from omega-3
supplementation.
OMEGA-3 FATTY ACIDS IN HEALTH AND DISEASEMore than 20,000 studies on EPA and
DHA have assessed the health bene-
fits of omega-3 fatty acids [103,104].
Through their influence on membrane
integrity, gene expression, the balance
with omega-6 fatty acids and the gen-
eration of eicosanoids and endocanna-
binoids, they have the ability to modify
heart disease risk, inflammatory re-
sponse, neurological and psychiatric
balance, vision, and many more pro-
cesses in the body [105-107].
HEARTMost established is the influence
of EPA and DHA on cardiovascular
risk, since they can modify blood tri-
glycerides, HDL cholesterol, plaque de-
velopment, heart rate, and heart muscle
functions [108]. By doing so, EPA and
DHA reduce the risk for cardiac death.
Moreover, a meta-analysis that sum-
marizes all available research on heart
health found a connection between EPA
and DHA and a reduction in blood pres-
sure (decrease of systolic blood pres-
sure of around 4.5mm Hg and diastolic
blood pressure of 3mm Hg), especially
in those with high blood pressure [109].
Already a decrease of 2 mm Hg blood
pressure is of importance, since it is
linked to a 6% reduced stroke mortal-
ity, 4% reduced coronary heart dis-
ease mortality, and 3% reduced total
mortality [110].

42 KRILL OIL CONCENTRATE
Health area Benefit ReferencesBrain health DHA is highly concentrated in the brain and
is important for cognitive (memory and brain performance) and behavioral function. Effects were reported for: Mood Depression Cognitive function Emotional distress ADHD symptoms Alzheimer disease Memory Age-related cognitive decline Self-harm and suicidal thinking
[117-121]
Cancer Mainly in cancer with gastrointestinal origin work omega-3s as an anti-inflammatory agent.
[122,123]
Table 3: Omega-3 fatty acid health benefits.
BRAINOmega-3 fatty acids have been shown
to be essential for mental health and
brain development and function [111].
Research has indicated that the high-
er EPA and DHA intakes, the lower the
risk for Alzheimer’s disease, age-relat-
ed cognitive decline, depression, ag-
gression, and more [112-114]. Omega-3
fatty acids may improve mental health
by influencing nervous system activity,
memory, serotonin and dopamine lev-
els, neurotransmission, and the forma-
tion of synapses between neurons [115].
It has been shown that indi-
viduals with low blood EPA and DHA
levels have smaller brains and that the
lower brain volume corresponded to
two years of structural brain aging in
dementia-free study participants [116].
DHA was further associated with better
visual memory, executive function, and
abstract thinking. Generally, reduced
brain volume is linked to cognitive de-
cline and dementia. Already at the age
of 30, the brain volume starts to decline
due to the normal aging process, but
at twice the speed, if mild dementia is
present, indicating the need for optimal
omega-3 intake throughout life.
Besides their positive effect
on heart and brain health, EPA and DHA
have been linked to a variety of health
concerns of which a selection is listed in
Table 3.

43 KRILL OIL CONCENTRATE
Eye health Omega-3 supplementation are reported to have a positive effect on macular degener-ation (a serious age-related eye condition that can progress to blindness) and dry-eye syndrome.
[124,125]
Heart health Reduced risk of heart disease by: ↓ Cholesterol ↓ Triglyceride ↓ Plaque development ↓ Arteriosclerosis ↓ Blood pressure ↑ HDL (“good cholesterol”) ↑Omega-3 index
[126-129]
Inflammatory diseases
Reduced inflammatory responses in a range of diseases such as rheumatoid arthritis, inflammatory bowel diseases, systemic lupus erythematosus, and childhood asthma.The effect of omega-3s is due to a reduction in the production of many pro-inflammatory mediators such as: ↓ C-reactive protein ↓ Interleukins ↓ Prostaglandins ↓ Tumor necrosis factor alpha ↑Omega-3 index
[106,
130-132]
Metabolic disorders
By reducing triglycerides and inflammatory markers and improving insulin sensitivity, omega-3s can affect non-alcoholic fatty liver disease.
[133]
Skin health Maintenance of skin health by increasing hydration, reducing sunburn, aging, and skin cancer via photo-protective effects
[134,135]
Women health
Reduced menstrual pain [136]
ADHD, attention deficit hyperactivity disorder; DHA, docosahexaenoic acid; HDL, high-density lipoprotein

44 KRILL OIL CONCENTRATE
Krill Oil: Phospholipids, Choline, And Omega-3 Fatty Acids All In One
Krill live in a very pure environment
WHY KRILL OIL? To fulfill the global
demand for omega-3
fatty acids with grow-
ing pressure on fish
stocks, new sustain-
able sources are need-
ed. Krill oil is such a
source and WWF-Nor-
way clearly says: “Man-
agement of krill is sus-
tainable.”
Nina Jensen, CEO of
WWF-Norway: “WWF-Norway and Aker
BioMarine have worked together since
2008 for a sustainable management of
krill resources in the Antarctica. As a
result of the partnership and the MSC
(Marine Stewardship Council) certifi-
cation, Aker BioMarine has started an
extensive mapping of fish larval by-
catch, and is working with WWF-Nor-
way to document the potential overlap/
conflict between the fishery and land
based predators. WWF-Norway and
Aker BioMarine are also working ac-
tively towards CCAMLR (Commission
for the Conservation of Antarctic Ma-
rine Living Resources) on sustainability
issues. In addition, Aker BioMarine con-
tinues to be the most proactive player
in the krill fishery and has implemented
voluntary measures. This includes mea-
sures such as 100% observer coverage
and real-time reporting procedures to
ensure the continued sustainability of
this fishery. By permitting scientists
onboard at no cost, they are also con-
tributing to science and research. The
krill fishery has been going on for more
than 30 years and the catches have
been relatively stable and low. Howev-
er, WWF-Norway remains concerned
that while the precautionary catch limit
represents a smaller catch limit than
for most fisheries, it may fail to protect
krill predators at the local scale. It is
therefore important to have industry
45 KRILL OIL CONCENTRATE
players, like Aker BioMarine, to commit
to further research to understand the
complex marine ecosystem in the Ant-
arctica.”
The Marine Stewardship Council (MSC)
is an international nonprofit organiza-
tion that focuses on the health of ocean
stocks and how they are managed, in
addition to assessing the effects of
fisheries on the wider ecosystem. The
Aker BioMarine krill fishery has been
evaluated by an independent assess-
ment team, and the evaluators have
certified that the fishery is well man-
aged, that the krill stock is healthy, and
that Aker BioMarine’s krill fishery is
sustainable with minimal impact on the
ecosystem.
While krill oil comes from a sustainable
source, it has also been found to be pure
by extensive analysis for the presence
of contaminants, such as dioxins, fu-
rans, dioxin-like PCBs (polychlorinated
biphenyls), organochlorine pesticides,
PBDEs (polybrominated diphenyl
ethers), heavy metals, PAHs (polycyclic
aromatic hydrocarbons), arsenic spe-
cies, fluoride, trans fatty acids, and ma-
rine algal toxins. The krill’s place at the
bottom of the food chain and its clean
habitat impede accumulation of these
contaminants, which are often found in
marine life higher in the food chain.
The quality of krill oil has
been further increased by reducing
TMA/TMAO and salt contents giving
an almost taste- and smell-free krill oil
concentrate. Phospholipid, choline, and
omega-3 fatty acid concentrations are
increased, providing a special combina-
tion of these important nutrients in the
krill oil concentrate.
UPTAKE OF KRILL OIL IN THE BODY The evidence that phospholipids are
a more effective delivery molecule of
fatty acids to organs than triglycerides
is rising [137-140]. Of particular interest
is the accumulation of DHA into the
brain, since it makes up about 30-40%
of the fatty acids in the gray matter of
the cortex and is particularly concen-
trated in synaptic membranes [141]. In-
deed, in preclinical studies, when given
single-doses of radiolabeled DHA, the
DHA brain accumulation was twice as
high, when DHA was supplied in phos-
pholipid rather than triglyceride form
[137,138].
Omega-3 fatty acids from krill oil are
efficiently transported and integrat-
ed into cell membranes, because they
45 KRILL OIL CONCENTRATE
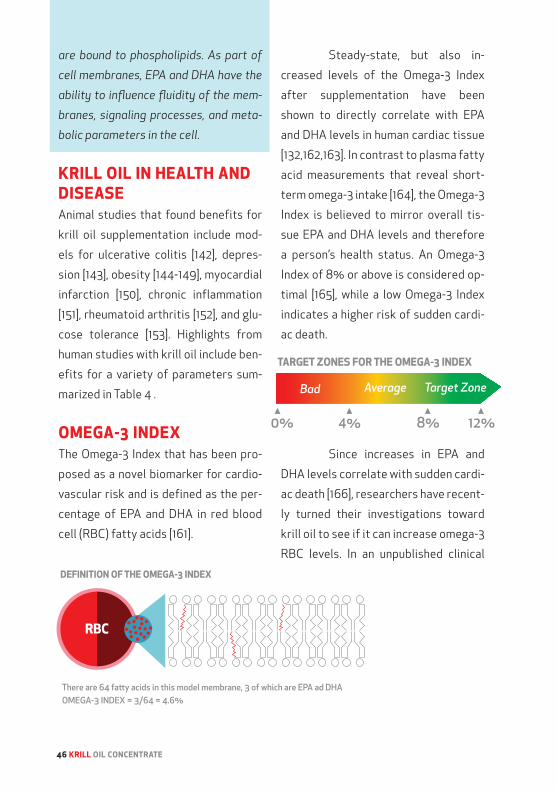
46 KRILL OIL CONCENTRATE
are bound to phospholipids. As part of
cell membranes, EPA and DHA have the
ability to influence fluidity of the mem-
branes, signaling processes, and meta-
bolic parameters in the cell.
KRILL OIL IN HEALTH AND DISEASEAnimal studies that found benefits for
krill oil supplementation include mod-
els for ulcerative colitis [142], depres-
sion [143], obesity [144-149], myocardial
infarction [150], chronic inflammation
[151], rheumatoid arthritis [152], and glu-
cose tolerance [153]. Highlights from
human studies with krill oil include ben-
efits for a variety of parameters sum-
marized in Table 4 .
OMEGA-3 INDEXThe Omega-3 Index that has been pro-
posed as a novel biomarker for cardio-
vascular risk and is defined as the per-
centage of EPA and DHA in red blood
cell (RBC) fatty acids [161].
Steady-state, but also in-
creased levels of the Omega-3 Index
after supplementation have been
shown to directly correlate with EPA
and DHA levels in human cardiac tissue
[132,162,163]. In contrast to plasma fatty
acid measurements that reveal short-
term omega-3 intake [164], the Omega-3
Index is believed to mirror overall tis-
sue EPA and DHA levels and therefore
a person’s health status. An Omega-3
Index of 8% or above is considered op-
timal [165], while a low Omega-3 Index
indicates a higher risk of sudden cardi-
ac death.
Since increases in EPA and
DHA levels correlate with sudden cardi-
ac death [166], researchers have recent-
ly turned their investigations toward
krill oil to see if it can increase omega-3
RBC levels. In an unpublished clinical

47 KRILL OIL CONCENTRATE
Table 4: Benefits of krill oil in clinical studies.
Parameters Explanation Effects of krill oil ReferencesADHD symptoms
Attention deficit hy-peractivity disorder; a neurodevelopmental psychiatric disorder characterized by attention deficits, hyperactivity, and impulsiveness.
↑ Improvement in behavior and daily function capacity in children
Unpublished data
Cachexia Loss of body mass that cannot be reversed nutritionally (cancer patients) and is characterized by anorexia, muscle wasting, and lipid profile disorder.
↑ Improved blood lipids in advanced cancer patients with cachexia (TG reduced, HDL increased, LDL reduced). Endocannabinoid system parame-ters normalized and inflammation markers reduced
Unpublished data
CRP C- reactive protein; CRP blood levels rise in response to inflam-mation.
↓ Reduced CRP, inflammation, and arthritic symp-toms (WOMAC scores)
[155]
Endocanna-binoids
Lipid signaling molecules made from omega-6 fatty acids involved in a variety of physiological processes including appetite, pain-sensa-tion, mood, and mem-ory. Obese persons have an overactive endocannabinoid system.
↓ Reduced endo-cannabinoids in obese persons
[156]
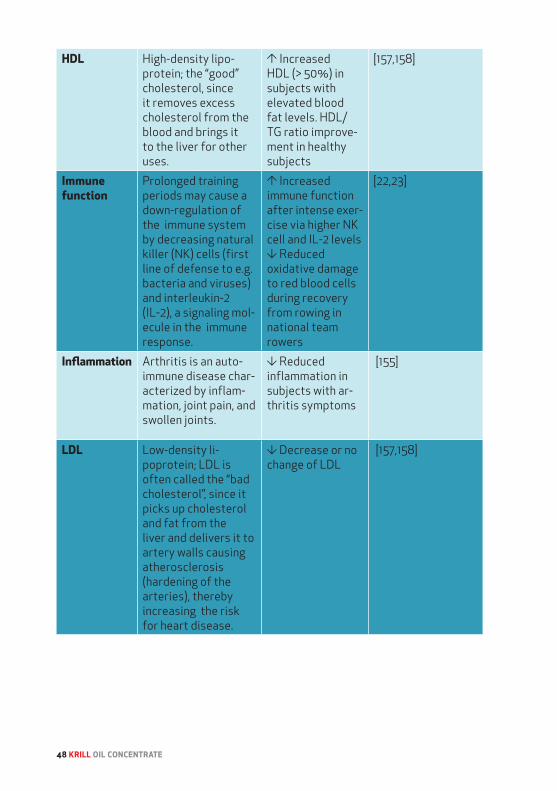
48 KRILL OIL CONCENTRATE
HDL High-density lipo-protein; the “good” cholesterol, since it removes excess cholesterol from the blood and brings it to the liver for other uses.
↑ Increased HDL (> 50%) in subjects with elevated blood fat levels. HDL/TG ratio improve-ment in healthy subjects
[157,158]
Immune function
Prolonged training periods may cause a down-regulation of the immune system by decreasing natural killer (NK) cells (first line of defense to e.g. bacteria and viruses) and interleukin-2 (IL-2), a signaling mol-ecule in the immune response.
↑ Increased immune function after intense exer-cise via higher NK cell and IL-2 levels ↓ Reduced oxidative damage to red blood cells during recovery from rowing in national team rowers
[22,23]
Inflammation Arthritis is an auto-immune disease char-acterized by inflam-mation, joint pain, and swollen joints.
↓ Reduced inflammation in subjects with ar-thritis symptoms
[155]
LDL Low-density li-poprotein; LDL is often called the “bad cholesterol”, since it picks up cholesterol and fat from the liver and delivers it to artery walls causing atherosclerosis (hardening of the arteries), thereby increasing the risk for heart disease.
↓ Decrease or no change of LDL
[157,158]

49 KRILL OIL CONCENTRATE
Omega-3 index
Percent EPA and DHA in red blood cells. Correlates with amount of EPA and DHA in other tissues. Low Omega-3 index is linked to higher risk of heart disease.
↑ Significant increase of Omega-3 index
[127,159]
PMS symptoms
Premenstrual syndrome; PMS syndrome might have an inflammatory connection.
↓ Significant re-duction in physical and emotional symptoms related to PMS measured as breast tender-ness, stress, irri-tability, depres-sion, joint pain, bloating, swelling, abdominal pain, and weight gain ↓ Significant re-duction in amount of painkillers used for painful cramps
[160]
Triglyceride A lipid molecule consisting of glycerol with three fatty acids bound to it. The fatty acids can be saturat-ed or unsaturated.
↓ Significant reduction of triglycerides in blood
[157-159]
ADHD, attention deficit hyperactivity disorder; CRP, C-reactive protein; DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid; HDL, high-density lipoprotein; IL-2, interleukin-2; LDL, low-density lipoprotein; NK, natural killer; PMS, premenstrual syndrome; TG, triglyceride; WOMAC, Western Ontario and McMaster Universities Arthritis Index

50 KRILL OIL CONCENTRATE
study, healthy volunteers took either 2
grams of Superba™ krill oil for 8 weeks
or 2 grams of an omega-3 enriched
fish oil. The goal of the study was to
compare the delivery of omega-3 fatty
acids, PLs versus TGs, to see if the mo-
lecular form influences the increase in
Omega-3 Index. The results of the study
showed that krill oil increased the Ome-
ga-3 Index significantly more than fish
oil after 8 weeks of supplementation.
In fact, krill oil increased the Omega-3
Index about 70% more than fish oil at
the end of study after dose adjustment
between the two treatment groups.
These results go hand in hand
with another study, which investigated
the effect of 12 weeks daily Superba™
krill oil intake in volunteers with “bor-
derline high” or “high” blood triglyceride
levels [159]. Triglycerides have an im-
portant role in lipid metabolism and are
a central biomarker of heart disease
risk [167].
In this study, a total of 300 vol-
unteers were divided into five groups
and supplemented with krill oil at either
0.5, 1, 2 or 4 grams per day or placebo
(olive oil). The individuals included in
the study had blood triglyceride values
between 150 and 499 mg/dL. Blood lip-
ids were measured at baseline, 6 weeks
and 12 weeks of treatment.
Relative to subjects in the
placebo group, those administered
krill oil had a statistically significant
10% reduction in serum triglycerides.
Moreover, LDL cholesterol levels were
not increased in the krill oil groups rela-
tive to the placebo group, an important
finding considering an increase in LDL
cholesterol has been observed in some
fish oil trials [159]. Additionally, the sub-
jects taking 4 grams of krill oil per day
raised their Omega-3 Index from 3.7%
51 KRILL OIL CONCENTRATE
to 6.3%. Comparable increases in the
Omega-3 Index have been linked to de-
creased risk for sudden cardiac death
in previous studies – in a prospective
cohort study by about 80% [168] and in
a case control study by 90% [169].
Thus, there seem to be ad-
vantages of krill oil, when it comes to
raising a person’s Omega-3 Index. Most
importantly, the mentioned studies
show that krill oil more effectively rais-
es the Omega-3 Index compared to fish
oil, even though krill oil delivers lower
amounts of EPA and DHA on a gram per
gram basis compared to fish oil. Clear
health benefits, in particular for heart
health, have been shown by raising one’s
Omega-3 Index higher than 8%.
CONCLUSION While Superba™ krill oil has demon-
strated its health benefits in numerous
studies, the new krill oil concentrate
holds even more promise in particular
in relation to health concerns that are
characterized by phospholipid and/or
choline deficiency. Reduced phospho-
lipid and choline levels are seen in e.g.
liver and brain disorders, heart disease,
intestinal inflammation, lung and skin
diseases, or after intense exercise.
Krill oil supplementation can
help to heal membranes and to opti-
mize omega-3 fatty acid, phospholipid,
and choline status in the body. The all-
in-one advantage of krill oil delivering
simultaneously omega-3 fatty acids,
phospholipids, and choline gives it a
unique standpoint in the omega-3 mar-
ket. However, the full elucidation of how
much each component benefits human
health must await further study.
ACKNOWLEDGEMENTSI am very grateful for editing help from
Gunhild Yksnøy and Michel Lockhart
and to everyone proofreading the text.
A special thanks for the contribution
of tables from Tove Julie Evjen and
Wenche Rasch.
52 KRILL OIL CONCENTRATE
REFERENCES
1. Jensen, H.H.; Batres-Marquez, S.P.; Carriqui-ry, A.; Schalinske, K.L. Choline in the diets of the us population: Nhanes, 2003-2004. FASEB J 2007, 21, LB46.
2. Shaikh, N.A.; Yantha, J.; Shaikh, S.; Rowe, W.; Laidlaw, M.; Cockerline, C.; Ali, A.; Holub, B.; Jackowski, G. Efficacy of a unique omega-3 formulation on the correction of nutritional deficiency and its effects on cardiovas-cular disease risk factors in a randomized controlled vascazen((r)) reveal trial. Mol Cell Biochem 2014, 396, 9-22.
3. Spiridonov, V.; Casanova, B. Order eu-phausiacea dana, 1852. In: F. R. Schram & j. C. Von vaupel klein (eds.), treatise on zoology - anatomy, taxonomy, biology - the crustacea. 2010, 9A, 5-82.
4. Everson, I. Introducing krill. In: Krill: Biology, ecology and fisheries – (i. Everson, ed.) fish and aquatic resources, series 6. Blackwell science, oxford:. 2000, 1-7.
5. Macauley, M.C.; English, T.S.; Mathisen, O.E. Acoustic characterisation of swarms of ant-arctic krill (euphausia superba) from elephant island and bransfield strait. J Crustacean Biol 1984, 1, 16-44.
6. Anheller, J.E.; Hellgren, L.; Karlstam, B.; Vincent, J. Biochemical and biological profile of a new enzyme preparation from antarctic krill (e. Superba) suitable for debridement of ulcerative lesions. Archives of dermatological research 1989, 281, 105-110.
7. Tomo, A. Observations on krill shoals luminescence on surface level and the accompanying fauna. - in: S. B. Schnack (ed.), on the biology of krill euphausia superba. Ber. Polarforsch 1983, 4, 196-198.
8. Kils, U. Swimming behaviour, swimmimg performance and energy balance of antarctic krill euphausia superba. Biomass Sci Ser 1982, 3, 1-121.
9. Siegel, V. Krill (euphausiacea) life history and aspects of population dynamics. Can J Fish Aquat Sci 2000, 57, 130-150.
10. Shin, C.; Nicol, S. Using the relationship between eye diameter and body length to detect the effects of long-term starvation on antarctic krill euphausia superba. Marine Ecology Progres Series 2002, 239, 157-167.
11. Camera, E.; Mastrofrancesco, A.; Fabbri, C.; Daubrawa, F.; Picardo, M.; Sies, H.; Stahl, W. Astaxanthin, canthaxanthin and beta-caro-tene differently affect uva-induced oxidative damage and expression of oxidative stress-re-sponsive enzymes. Experimental dermatology 2009, 18, 222-231.
12. Kidd, P. Astaxanthin, cell membrane nutrient with diverse clinical benefits and anti-aging potential. Altern Med Rev 2011, 16, 355-364.
13. Guerin, M.; Huntley, M.E.; Olaizola, M. Haematococcus astaxanthin: Applications for human health and nutrition. Trends in biotech-nology 2003, 21, 210-216.
14. Burri, L.; Hoem, N.; Banni, S.; Berge, K. Review. Marine omega-3 phospholipids: Metabolism and biological activities. Int J Mol Sci 2012, 13, 15401-15419.
15. Ramprasath, V.R.; Eyal, I.; Zchut, S.; Shafat, I.; Jones, P.J. Supplementation of krill oil with high phospholipid content increases sum of epa and dha in erythrocytes compared with low phospholipid krill oil. Lipids Health Dis 2015, 14, 142.

53 KRILL OIL CONCENTRATE
16. Harris, W.S.; Varvel, S.A.; Pottala, J.V.; War-nick, G.R.; McConnell, J.P. Comparative effects of an acute dose of fish oil on omega-3 fatty acid levels in red blood cells versus plasma: Implications for clinical utility. J Clin Lipidol 2013, 7, 433-440.
17. Nieman, D.C.; Ahle, J.C.; Henson, D.A.; Warren, B.J.; Suttles, J.; Davis, J.M.; Buckley, K.S.; Simandle, S.; Butterworth, D.E.; Fagoaga, O.R., et al. Indomethacin does not alter natural killer cell response to 2.5 h of running. Journal of applied physiology 1995, 79, 748-755.
18. Simopoulos, A.P. Omega-3 fatty acids and athletics. Curr Sports Med Rep 2007, 6, 230-236.
19. von Schacky, C.; Kemper, M.; Haslbauer, R.; Halle, M. Low omega-3 index in 106 german elite winter endurance athletes: A pilot study. International journal of sport nutrition and exercise metabolism 2014, 24, 559-564.
20. von Schacky, C. The omega-3 index as a risk factor for cardiovascular diseases. Prosta-glandins & other lipid mediators 2011.
21. Peoples, G.E.; McLennan, P.L.; Howe, P.R.; Groeller, H. Fish oil reduces heart rate and oxygen consumption during exercise. Journal of cardiovascular pharmacology 2008, 52, 540-547.
22. Da Boit, M.; Mastalurova, I.; Brazaite, G.; McGovern, N.; Thompson, K.; Gray, S.R. The effect of krill oil supplementation on exercise performance and markers of immune function. PLoS One 2015, 10, e0139174.
23. Skarpańska-Stejnborn, A.; Pilaczyńs-ka-Szcześniak, L.; Basta, P.; Foriasz, J.; Arlet, J. Effects of supplementation with neptune krill oil (euphasia superba) on selected redox parameters and proinflammatory markers in
athletes during exhaustive exercise. J Human Kinetics 2010, 25, 49-57.
24. Haruta, Y.; Kato, K.; Yoshioka, T. Dietary phospholipid concentrate from bovine milk improves epidermal function in hairless mice. Biosci Biotechnol Biochem 2008, 72, 2151-2157.
25. Prottey, C.; Hartop, P.J.; Press, M. Cor-rection of the cutaneous manifestations of essential fatty acid deficiency in man by application of sunflower-seed oil to the skin. The Journal of investigative dermatology 1975, 64, 228-234.
26. Lee, Y.; Je, Y.J.; Lee, S.S.; Li, Z.J.; Choi, D.K.; Kwon, Y.B.; Sohn, K.C.; Im, M.; Seo, Y.J.; Lee, J.H. Changes in transepidermal water loss and skin hydration according to expression of aquaporin-3 in psoriasis. Ann Dermatol 2012, 24, 168-174.
27. Chapkin, R.S.; Ziboh, V.A.; Marcelo, C.L.; Voorhees, J.J. Metabolism of essential fatty acids by human epidermal enzyme prepara-tions: Evidence of chain elongation. J Lipid Res 1986, 27, 945-954.
28. Rhodes, L.E.; Shahbakhti, H.; Azurdia, R.M.; Moison, R.M.; Steenwinkel, M.J.; Homburg, M.I.; Dean, M.P.; McArdle, F.; Beijersbergen van Henegouwen, G.M.; Epe, B., et al. Effect of eicosapentaenoic acid, an omega-3 polyunsat-urated fatty acid, on uvr-related cancer risk in humans. An assessment of early genotoxic markers. Carcinogenesis 2003, 24, 919-925.
29. Herslof, B.; Olsson, U.; Tingvall, P. Charac-terization of lecithins and phospholipids by hplc with light scattering detection. Phospho-lipids, Biochemical, Pharmaceutical and Ana-lytical Considerations, Hanin, I. and Pepeu, G., Plenum Press, New York 1990, 295-298.

54 KRILL OIL CONCENTRATE
30. Medicamenta, iv edn. Cooperativa Farma-ceutica, Milano 1933, 2122-2126.
31. EFSA. Scientific opinion on the substanti-ation of health claims related to phosphorus and function of cell membranes, energy-yield-ing metabolism and maintenance of bone and teeth The EFSA Journal 2009, 7, 1219-1236.
32. Shinitsky, M. Membrane fluidity and cellular functions. Physiology of membrane fluidity, CRC Press, Boca Raton FL 1984, 1045-1049.
33. Laggner, P. Life - as a matter of fat - the emerging science of lipidomics edited by ole g. Mouritsen. Eur J Lipid Sci Technol 2007, 109, 1237.
34. Kosicek, M.; Hecimovic, S. Phospholipids and alzheimer’s disease: Alterations, mecha-nisms and potential biomarkers. Int J Mol Sci 2013, 14, 1310-1322.
35. Sacks, F.M.; Expert Group on, H.D.L.C. The role of high-density lipoprotein (hdl) cholesterol in the prevention and treatment of coronary heart disease: Expert group recom-mendations. Am J Cardiol 2002, 90, 139-143.
36. Grundy, S.M. Absorption and metabolism of dietary cholesterol. Annu Rev Nutr 1983, 3, 71-96.
37. Rampone, A.J. The effects of bile salt and raw bile on the intestinal absorption of micel-lar fatty acid in the rat in vitro. The Journal of physiology 1972, 222, 679-690.
38. Beil, F.U.; Grundy, S.M. Studies on plasma lipoproteins during absorption of exogenous lecithin in man. J Lipid Res 1980, 21, 525-536.
39. Greten, H.; Raetzer, H.; Stiehl, A.; Schettler, G. The effect of polyunsaturated phosphati-
dylcholine on plasma lipids and fecal sterol excretion. Atherosclerosis 1980, 36, 81-88.
40. Kesaniemi, Y.A.; Grundy, S.M. Effects of dietary polyenylphosphatidylcholine on metabolism of cholesterol and triglycerides in hypertriglyceridemic patients. Am J Clin Nutr 1986, 43, 98-107.
41. Cohn, J.S.; Kamili, A.; Wat, E.; Chung, R.W.; Tandy, S. Dietary phospholipids and intestinal cholesterol absorption. Nutrients 2010, 2, 116-127.
42. Weihrauch, J.L.; Son, Y.S. The phospholipid content of foods. JAOCS 1983, 60, 1971-1978.
43. Duttaroy, A.K. Phospholipid technology and applications. The oily press lipid library - edited by FD Gunstone, PJ Barnes & Associ-ates, Bridgewater, England 22, 153-167.
44. Kuellenberg, D.; Taylor, L.A.; Schneider, M.; Massing, U. Health effects of dietary phospholipids. Lipids in health and disease 2012, 11, 3.
45. Sahebkar, A. Fat lowers fat: Purified phospholipids as emerging therapies for dyslipidemia. Biochim Biophys Acta 2013, 1831, 887-893 46. Eshiginia, S.; Gapparov, M.M.; Soto, K. Influ-ence of phospholipids on efficiency of dietary therapy and parameters of lipids metabolism in patients with hypertension. Vopr Pitan 2005, 74, 28-31.
47. Polichetti, E.; Janisson, A.; Iovanna, C.; Portuga, l.H.; Mekki, N.; Lorec, A.M.; Pauli, A.M.; Luna, A.; Lairon, D.; Droitte, P.L. Stimulation of the apo ai-high density lipoprotein system by dietary soyabean lecithin in humans - a new substrate for the measurement of lecithin:Cholesterol acyltransferaseactivity.

55 KRILL OIL CONCENTRATE
Journal of Nutritional Biochemistry 1998, 9, 659-666.
48. Wojcicki, J.; Pawlik, A.; Samochowiec, L.; Kaldonska, M.; Mysliwiec, Z. Clinical evaluation of lecithin as a lipid-lowering agent. Phyto-therapy Research 2006, 9, 597-599.
49. Jannace, P.W.; Lerman, R.H.; Santos, J.I.; Vi-tale, J.J. Effects of oral soy phosphatidylcho-line on phagocytosis, arachidonate concentra-tions, and killing by human polymorphonuclear leukocytes. Am J Clin Nutr 1992, 56, 599-603.
50. Zeisel, S.H. Nutritional importance of choline for brain development. J Am Coll Nutr 2004, 23, 621S-626S.
51. Gundermann, K.J.; Kuenker, A.; Kuntz, E.; Drozdzik, M. Activity of essential phospho-lipids (epl) from soybean in liver diseases. Pharmacol Rep 2011, 63, 643-659.
52. Monteleone, P.; Beinat, L.; Tanzillo, C.; Maj, M.; Kemali, D. Effects of phosphatidylserine on the neuroendocrine response to physical stress in humans. Neuroendocrinology 1990, 52, 243-248.
53. Leyck, S.; Dereu, N.; Etschenberg, E.; Ghyczy, M.; Graf, E.; Winkelmann, J.; Parnham, M.J. Improvement of the gastric tolerance of non-steroidal anti-inflammatory drugs by polyene phosphatidylcholine (phospholipon 100). Eur J Pharmacol 1985, 117, 35-42.
54. Benton, D.; Donohoe, R.T.; Sillance, B.; Nabb, S. The influence of phosphatidylserine supplementation on mood and heart rate when faced with an acute stressor. Nutr Neurosci 2001, 4, 169-178.
55. Ehehalt, R.; Braun, A.; Karner, M.; Fullekrug, J.; Stremmel, W. Phosphatidylcholine as a con-stituent in the colonic mucosal barrier--phys-
iological and clinical relevance. Biochim Biophys Acta 2010, 1801, 983-993.
56. Gupta, R.; Bhangoo, A.; Matthews, N.A.; Anhalt, H.; Matta, Y.; Lamichhane, B.; Malik, S.; Narwal, S.; Wetzler, G.; Ten, S. The prevalence of non-alcoholic fatty liver disease and met-abolic syndrome in obese children. J Pediatr Endocrinol Metab 2011, 24, 907-911.
57. Welsh, J.A.; Karpen, S.; Vos, M.B. Increasing prevalence of nonalcoholic fatty liver disease among united states adolescents, 1988-1994 to 2007-2010. The Journal of pediatrics 2013, 162, 496-500.
58. Targher, G.; Bertolini, L.; Padovani, R.; Rodella, S.; Zoppini, G.; Pichiri, I.; Sorgato, C.; Zenari, L.; Bonora, E. Prevalence of non-alco-holic fatty liver disease and its association with cardiovascular disease in patients with type 1 diabetes. J Hepatol 2010, 53, 713-718.
59. Leite, N.C.; Salles, G.F.; Araujo, A.L.; Ville-la-Nogueira, C.A.; Cardoso, C.R. Prevalence and associated factors of non-alcoholic fatty liver disease in patients with type-2 diabetes mellitus. Liver Int 2009, 29, 113-119.
60. Prashanth, M.; Ganesh, H.K.; Vima, M.V.; John, M.; Bandgar, T.; Joshi, S.R.; Shah, S.R.; Rathi, P.M.; Joshi, A.S.; Thakkar, H., et al. Prev-alence of nonalcoholic fatty liver disease in patients with type 2 diabetes mellitus. J Assoc Physicians India 2009, 57, 205-210.
61. Yang, F.; Ma, M.; Xu, J.; Yu, X.; Qiu, N. An egg-enriched diet attenuates plasma lipids and mediates cholesterol metabolism of high-cholesterol fed rats. Lipids 2012, 47, 269-277.
62. Lieber, C.S.; Robins, S.J.; Li, J.; DeCarli, L.M.; Mak, K.M.; Fasulo, J.M.; Leo, M.A. Phospha-tidylcholine protects against fibrosis and

56 KRILL OIL CONCENTRATE
cirrhosis in the baboon. Gastroenterology 1994, 106, 152-159.
63. Jenkins, P.J.; Portmann, B.P.; Eddleston, A.L.; Williams, R. Use of polyunsaturated phospha-tidyl choline in hbsag negative chronic active hepatitis: Results of prospective double-blind controlled trial. Liver 1982, 2, 77-81.
64. Hamaguchi, M.; Kojima, T.; Takeda, N.; Nagata, C.; Takeda, J.; Sarui, H.; Kawahito, Y.; Yoshida, N.; Suetsugu, A.; Kato, T., et al. Nonal-coholic fatty liver disease is a novel predictor of cardiovascular disease. World J Gastroen-terol 2007, 13, 1579-1584.
65. Dasgupta, S.; Bhattacharyya, D.K. Dietary effect of eicosapentaenoic acid (epa) con-taining soyphospholipid. J Oleo Sci 2007, 56, 563-568.
66. Shirouchi, B.; Nagao, K.; Inoue, N.; Ohkubo, T.; Hibino, H.; Yanagita, T. Effect of dietary omega-3 phosphatidylcholine on obesity-re-lated disorders in obese otsuka long-evans tokushima fatty rats. J Agric Food Chem 2007, 55, 7170-7176.
67. Carter, J.M.; Demizieux, L.; Campenot, R.B.; Vance, D.E.; Vance, J.E. Phosphatidylcholine biosynthesis via ctp:Phosphocholine cytidyl-yltransferase 2 facilitates neurite outgrowth and branching. J Biol Chem 2008, 283, 202-212.
68. Nguyen, L.N.; Ma, D.; Shui, G.; Wong, P.; Cazenave-Gassiot, A.; Zhang, X.; Wenk, M.R.; Goh, E.L.; Silver, D.L. Mfsd2a is a transporter for the essential omega-3 fatty acid docosahexaenoic acid. Nature 2014, 509, 503-506.
69. Alakbarzade, V.; Hameed, A.; Quek, D.Q.; Chioza, B.A.; Baple, E.L.; Cazenave-Gassiot, A.; Nguyen, L.N.; Wenk, M.R.; Ahmad, A.Q.; Sreekantan-Nair, A., et al. A partially inac-tivating mutation in the sodium-dependent
lysophosphatidylcholine transporter mfsd2a causes a non-lethal microcephaly syndrome. Nat Genet 2015, 47, 814-817.
70. Guemez-Gamboa, A.; Nguyen, L.N.; Yang, H.; Zaki, M.S.; Kara, M.; Ben-Omran, T.; Akizu, N.; Rosti, R.O.; Rosti, B.; Scott, E., et al. Inactivat-ing mutations in mfsd2a, required for omega-3 fatty acid transport in brain, cause a lethal microcephaly syndrome. Nat Genet 2015, 47, 809-813.
71. IOM. Dietary reference intakes for thiamin, riboflavin, niacin, vitamin b6, folate, vitamin b12, pantothenic acid, biotin and choline. National Cholesterol Education Program Expert Panel on Detection, E., Ed. The National Academy Press Washington, D.C., 1998.
72. Zeisel, S.H. Choline: Critical role during fetal development and dietary requirements in adults. Annual review of nutrition 2006, 26, 229-250.
73. Schaefer, E.J.; Bongard, V.; Beiser, A.S.; Lamon-Fava, S.; Robins, S.J.; Au, R.; Tucker, K.L.; Kyle, D.J.; Wilson, P.W.; Wolf, P.A. Plasma phos-phatidylcholine docosahexaenoic acid content and risk of dementia and alzheimer disease: The framingham heart study. Archives of neurology 2006, 63, 1545-1550.
74. Zeisel, S.H.; da Costa, K.A. Choline: An essential nutrient for public health. Nutr Rev 2009, 67, 615-623.
75. Rees, W.D.; Wilson, F.A.; Maloney, C.A. Sulfur amino acid metabolism in pregnancy: The impact of methionine in the maternal diet. J Nutr 2006, 136, 1701S-1705S.
76. Shaw, G.M.; Carmichael, S.L.; Yang, W.; Selvin, S.; Schaffer, D.M. Periconceptional dietary intake of choline and betaine and neural tube defects in offspring. Am J Epidemiol 2004, 160, 102-109.

57 KRILL OIL CONCENTRATE
77. Stead, L.M.; Brosnan, J.T.; Brosnan, M.E.; Vance, D.E.; Jacobs, R.L. Is it time to reevaluate methyl balance in humans? Am J Clin Nutr 2006, 83, 5-10.
78. Ueland, P.M. Choline and betaine in health and disease. Journal of inherited metabolic disease 2011, 34, 3-15.
79. Hirsch, M.J.; Growdon, J.H.; Wurtman, R.J. Relations between dietary choline or lecithin intake, serum choline levels, and various meta-bolic indices. Metabolism 1978, 27, 953-960.
80. Wurtman, R.J.; Hirsch, M.J.; Growdon, J.H. Lecithin consumption raises serum-free-cho-line levels. Lancet 1977, 2, 68-69.
81. Rolo, A.P.; Teodoro, J.S.; Palmeira, C.M. Role of oxidative stress in the pathogenesis of nonalcoholic steatohepatitis. Free Radic Biol Med 2012, 52, 59-69.
82. Fischer, L.M.; daCosta, K.A.; Kwock, L.; Stewart, P.W.; Lu, T.S.; Stabler, S.P.; Allen, R.H.; Zeisel, S.H. Sex and menopausal status influence human dietary requirements for the nutrient choline. Am J Clin Nutr 2007, 85, 1275-1285.
83. Bigl, V.; Arendt, T.; Biesold, D. The nucleus basalis of maynert during aging and in dementing neuropsychiatric disorders. Brain Cholinergic Systems, Steriade, M. and Biesold, U., Oxford University Press, Oxford 1990.
84. de Lacalle, S.; Iraizoz, I.; Ma Gonzalo, L. Differential changes in cell size and number in topographic subdivisions of human basal nucleus in normal aging. Neuroscience 1991, 43, 445-456.
85. Stoll, A.L.; Renshaw, P.F.; De Micheli, E.; Wurtman, R.; Pillay, S.S.; Cohen, B.M. Choline ingestion increases the resonance of cho-line-containing compounds in human brain: An
in vivo proton magnetic resonance study. Biol Psychiatry 1995, 37, 170-174.
86. Higgins, J.P.; Flicker, L. Lecithin for de-mentia and cognitive impairment. Cochrane database of systematic reviews 2009.
87. Panijel, M. Therapeutische wirksamkeit von lecithin bei gedachtnis-und konzentra-tionsstorungen. Therapiewoche 1986, 36, 5029-5034.
88. von Allworden, H.N.; Horn, S.; Kahl, J.; Feld-heim, W. The influence of lecithin on plasma choline concentrations in triathletes and adolescent runners during exercise. European journal of applied physiology and occupation-al physiology 1993, 67, 87-91.
89. Jager, R.; Purpura, M.; Kingsley, M. Phos-pholipids and sports performance. J Int Soc Sports Nutr 2007, 4, 5.
90. Bradbury, J. Docosahexaenoic acid (dha): An ancient nutrient for the modern human brain. Nutrients 2011, 3, 529-554.
91. Jump, D.B.; Botolin, D.; Wang, Y.; Xu, J.; De-meure, O.; Christian, B. Docosahexaenoic acid (dha) and hepatic gene transcription. Chem Phys Lipids 2008, 153, 3-13.
92. Jump, D.B.; Thelen, A.; Ren, B.; Mater, M. Multiple mechanisms for polyunsaturated fatty acid regulation of hepatic gene tran-scription. Prostaglandins Leukot Essent Fatty Acids 1999, 60, 345-349.
93. Ou, J.; Tu, H.; Shan, B.; Luk, A.; DeBose-Boyd, R.A.; Bashmakov, Y.; Goldstein, J.L.; Brown, M.S. Unsaturated fatty acids inhibit transcrip-tion of the sterol regulatory element-binding protein-1c (srebp-1c) gene by antagonizing ligand-dependent activation of the lxr. Proc Natl Acad Sci U S A 2001, 98, 6027-6032.
58 KRILL OIL CONCENTRATE
94. Wisely, G.B.; Miller, A.B.; Davis, R.G.; Thorn-quest, A.D., Jr.; Johnson, R.; Spitzer, T.; Sefler, A.; Shearer, B.; Moore, J.T.; Miller, A.B., et al. Hepatocyte nuclear factor 4 is a transcription factor that constitutively binds fatty acids. Structure 2002, 10, 1225-1234.
95. Mirnikjoo, B.; Brown, S.E.; Kim, H.F.; Ma-rangell, L.B.; Sweatt, J.D.; Weeber, E.J. Protein kinase inhibition by omega-3 fatty acids. J Biol Chem 2001, 276, 10888-10896.
96. Seung Kim, H.F.; Weeber, E.J.; Sweatt, J.D.; Stoll, A.L.; Marangell, L.B. Inhibitory effects of omega-3 fatty acids on protein kinase c activity in vitro. Molecular psychiatry 2001, 6, 246-248.
97. Serhan, C.N.; Chiang, N.; Van Dyke, T.E. Re-solving inflammation: Dual anti-inflammatory and pro-resolution lipid mediators. Nature reviews. Immunology 2008, 8, 349-361.
98. Matias, I.; Petrosino, S.; Racioppi, A.; Capasso, R.; Izzo, A.A.; Di Marzo, V. Dysregu-lation of peripheral endocannabinoid levels in hyperglycemia and obesity: Effect of high fat diets. Mol Cell Endocrinol 2008, 286, S66-78.
99. Hibbeln, J.R.; Nieminen, L.R.; Blasbalg, T.L.; Riggs, J.A.; Lands, W.E. Healthy intakes of n-3 and n-6 fatty acids: Estimations considering worldwide diversity. Am J Clin Nutr 2006, 83, 1483S-1493S.
100. Simopoulos, A.P. The importance of the omega-6/omega-3 fatty acid ratio in cardio-vascular disease and other chronic diseases. Exp Biol Med (Maywood) 2008, 233, 674-688.
101. Simopoulos, A.P. Omega-3 fatty acids in health and disease and in growth and develop-ment. Am J Clin Nutr 1991, 54, 438-463.
102. Simopoulos, A.P. The importance of the ratio of omega-6/omega-3 essential fatty ac-ids. Biomed Pharmacother 2002, 56, 365-379.
103. Wassall, S.R.; Stillwell, W. Polyunsaturated fatty acid-cholesterol interactions: Domain formation in membranes. Biochimica et bio-physica acta 2009, 1788, 24-32.
104. Riediger, N.D.; Othman, R.A.; Suh, M.; Moghadasian, M.H. A systemic review of the roles of n-3 fatty acids in health and disease. Journal of the American Dietetic Association 2009, 109, 668-679.
105. Banni, S.; Di Marzo, V. Effect of dietary fat on endocannabinoids and related mediators: Consequences on energy homeostasis, inflammation and mood. Mol Nutr Food Res 2010, 54, 82-92.
106. Calder, P.C. Marine omega-3 fatty acids and inflammatory processes: Effects, mecha-nisms and clinical relevance. Biochim Biophys Acta 2015, 1851, 469-484.
107. Cottin, S.C.; Sanders, T.A.; Hall, W.L. The differential effects of epa and dha on cardio-vascular risk factors. The Proceedings of the Nutrition Society 2011, 70, 215-231.
108. Chowdhury, R.; Warnakula, S.; Kunutsor, S.; Crowe, F.; Ward, H.A.; Johnson, L.; Franco, O.H.; Butterworth, A.S.; Forouhi, N.G.; Thompson, S.G., et al. Association of dietary, circulating, and supplement fatty acids with coronary risk: A systematic review and meta-analysis. Ann Intern Med 2014, 160, 398-406.
109. Miller, P.E.; Van Elswyk, M.; Alexander, D.D. Long-chain omega-3 fatty acids eicosapentae-noic acid and docosahexaenoic acid and blood pressure: A meta-analysis of randomized controlled trials. Am J Hypertens 2014.

59 KRILL OIL CONCENTRATE
110. Stamler, R. Implications of the intersalt study. Hypertension 1991, 17, I16-20.
111. Dyall, S.C.; Michael-Titus, A.T. Neurological benefits of omega-3 fatty acids. Neuromolec-ular Med 2008, 10, 219-235.
112. Hibbeln, J.R.; Ferguson, T.A.; Blasbalg, T.L. Omega-3 fatty acid deficiencies in neuro-development, aggression and autonomic dysregulation: Opportunities for intervention. International review of psychiatry 2006, 18, 107-118.
113. Morris, M.C.; Evans, D.A.; Bienias, J.L.; Tangney, C.C.; Bennett, D.A.; Wilson, R.S.; Aggarwal, N.; Schneider, J. Consumption of fish and n-3 fatty acids and risk of incident alzheimer disease. Arch Neurol 2003, 60, 940-946.
114. Nilsson, A.; Radeborg, K.; Salo, I.; Bjorck, I. Effects of supplementation with n-3 polyunsaturated fatty acids on cognitive performance and cardiometabolic risk mark-ers in healthy 51 to 72 years old subjects: A randomized controlled cross-over study. Nutr J 2012, 11, 99.
115. Schlange, H. Electroencephalographic findings in child behavior disorders and the therapeutic consequences resulting from them. Arch Kinderheilkd 1963, 169, 123-132.
116. Tan, Z.S.; Harris, W.S.; Beiser, A.S.; Au, R.; Himali, J.J.; Debette, S.; Pikula, A.; Decarli, C.; Wolf, P.A.; Vasan, R.S., et al. Red blood cell omega-3 fatty acid levels and markers of accelerated brain aging. Neurology 2012, 78, 658-664.
117. Antypa, N.; Van der Does, A.J.; Smelt, A.H.; Rogers, R.D. Omega-3 fatty acids (fish-oil) and depression-related cognition in healthy volunteers. Journal of psychopharmacology 2009, 23, 831-840.
118. Fontani, G.; Corradeschi, F.; Felici, A.; Alfatti, F.; Migliorini, S.; Lodi, L. Cognitive and physiological effects of omega-3 polyunsat-urated fatty acid supplementation in healthy subjects. Eur J Clin Invest 2005, 35, 691-699.
119. Freund-Levi, Y.; Eriksdotter-Jonhagen, M.; Cederholm, T.; Basun, H.; Faxen-Irving, G.; Garlind, A.; Vedin, I.; Vessby, B.; Wahlund, L.O.; Palmblad, J. Omega-3 fatty acid treatment in 174 patients with mild to moderate alzhei-mer disease: Omegad study: A randomized double-blind trial. Arch Neurol 2006, 63, 1402-1408.
120. Hibbeln, J.R. Depression, suicide and deficiencies of omega-3 essential fatty acids in modern diets. World Rev Nutr Diet 2009, 99, 17-30.
121. Richardson, A.J.; Burton, J.R.; Sewell, R.P.; Spreckelsen, T.F.; Montgomery, P. Docosahex-aenoic acid for reading, cognition and behav-ior in children aged 7-9 years: A randomized, controlled trial (the dolab study). PLoS One 2012, 7, e43909.
122. Nkondjock, A.; Shatenstein, B.; Maison-neuve, P.; Ghadirian, P. Specific fatty acids and human colorectal cancer: An overview. Cancer Detect Prev 2003, 27, 55-66.
123. Theodoratou, E.; McNeill, G.; Cetnarskyj, R.; Farrington, S.M.; Tenesa, A.; Barnetson, R.; Porteous, M.; Dunlop, M.; Campbell, H. Dietary fatty acids and colorectal cancer: A case-con-trol study. Am J Epidemiol 2007, 166, 181-195.
124. Krishnadev, N.; Meleth, A.D.; Chew, E.Y. Nutritional supplements for age-related macular degeneration. Curr Opin Ophthalmol 2010, 21, 184-189.
125. Liu, A.; Ji, J. Omega-3 essential fatty acids therapy for dry eye syndrome: A meta-analysis

60 KRILL OIL CONCENTRATE
of randomized controlled studies. Medical sci-ence monitor : international medical journal of experimental and clinical research 2014, 20, 1583-1589.
126. Casula, M.; Soranna, D.; Catapano, A.L.; Corrao, G. Long-term effect of high dose ome-ga-3 fatty acid supplementation for secondary prevention of cardiovascular outcomes: A me-ta-analysis of randomized, placebo controlled trials [corrected]. Atheroscler Suppl 2013, 14, 243-251.
127. Ramprasath, V.R.; Eyal, I.; Zchut, S.; Jones, P.J. Enhanced increase of omega-3 index in healthy individuals with response to 4-week n-3 fatty acid supplementation from krill oil versus fish oil. Lipids Health Dis 2013, 12, 178.
128. Wang, C.; Harris, W.S.; Chung, M.; Lichten-stein, A.H.; Balk, E.M.; Kupelnick, B.; Jordan, H.S.; Lau, J. N-3 fatty acids from fish or fish-oil supplements, but not alpha-linolenic acid, benefit cardiovascular disease outcomes in primary- and secondary-prevention studies: A systematic review. Am J Clin Nutr 2006, 84, 5-17.
129. Wen, Y.T.; Dai, J.H.; Gao, Q. Effects of omega-3 fatty acid on major cardiovascular events and mortality in patients with coronary heart disease: A meta-analysis of randomized controlled trials. Nutr Metab Cardiovasc Dis 2014, 24, 470-475. 130. Cleland, L.G.; French, J.K.; Betts, W.H.; Murphy, G.A.; Elliott, M.J. Clinical and biochem-ical effects of dietary fish oil supplements in rheumatoid arthritis. J Rheumatol 1988, 15, 1471-1475.
131. Harris, W.S. The omega-3 index as a risk factor for coronary heart disease. Am J Clin Nutr 2008, 87, 1997S-2002S.
132. Harris, W.S.; Von Schacky, C. The omega-3 index: A new risk factor for death from coronary heart disease? Prev Med 2004, 39, 212-220.
133. Masterton, G.S.; Plevris, J.N.; Hayes, P.C. Review article: Omega-3 fatty acids - a prom-ising novel therapy for non-alcoholic fatty liver disease. Aliment Pharmacol Ther 2010, 31, 679-692.
134. Balbas, G.M.; Regana, M.S.; Millet, P.U. Study on the use of omega-3 fatty acids as a therapeutic supplement in treatment of psoriasis. Clin Cosmet Investig Dermatol 2011, 4, 73-77.
135. Rhodes, L.E.; Durham, B.H.; Fraser, W.D.; Friedmann, P.S. Dietary fish oil reduces basal and ultraviolet b-generated pge2 levels in skin and increases the threshold to provocation of polymorphic light eruption. The Journal of investigative dermatology 1995, 105, 532-535.
136. Harel, Z.; Biro, F.M.; Kottenhahn, R.K.; Rosenthal, S.L. Supplementation with omega-3 polyunsaturated fatty acids in the management of dysmenorrhea in adolescents. Am J Obstet Gynecol 1996, 174, 1335-1338.
137. Graf, B.A.; Duchateau, G.S.; Patterson, A.B.; Mitchell, E.S.; van Bruggen, P.; Koek, J.H.; Melville, S.; Verkade, H.J. Age dependent in-corporation of 14c-dha into rat brain and body tissues after dosing various 14c-dha-esters. Prostaglandins Leukot Essent Fatty Acids 2010, 83, 89-96.
138. Liu, L.; Bartke, N.; Van Daele, H.; Lawrence, P.; Qin, X.; Park, H.G.; Kothapalli, K.; Windust, A.; Bindels, J.; Wang, Z., et al. Higher efficacy of dietary dha provided as a phospholipid than as a triglyceride for brain dha accretion in neona-tal piglets. J Lipid Res 2014, 55, 531-539.

61 KRILL OIL CONCENTRATE
139. Rossmeisl, M.; Jilkova, Z.M.; Kuda, O.; Jele-nik, T.; Medrikova, D.; Stankova, B.; Kristinsson, B.; Haraldsson, G.G.; Svensen, H.; Stoknes, I., et al. Metabolic effects of n-3 pufa as phospho-lipids are superior to triglycerides in mice fed a high-fat diet: Possible role of endocannabi-noids. PLoS One 2012, 7, e38834.
140. Wijendran, V.; Huang, M.C.; Diau, G.Y.; Boehm, G.; Nathanielsz, P.W.; Brenna, J.T. Efficacy of dietary arachidonic acid provided as triglyceride or phospholipid as substrates for brain arachidonic acid accretion in baboon neonates. Pediatr Res 2002, 51, 265-272.
141. Bazan, N.G.; Scott, B.L. Dietary omega-3 fat-ty acids and accumulation of docosahexaenoic acid in rod photoreceptor cells of the retina and at synapses. Upsala journal of medical scienc-es. Supplement 1990, 48, 97-107.
142. Grimstad, T.; Bjorndal, B.; Cacabelos, D.; Aasprong, O.G.; Janssen, E.A.; Omdal, R.; Svardal, A.; Hausken, T.; Bohov, P.; Portero-Otin, M., et al. Dietary supplementation of krill oil attenuates inflammation and oxidative stress in experimental ulcerative colitis in rats. Scand J Gastroenterol 2012, 47, 49-58.
143. Wibrand, K.; Berge, K.; Messaoudi, M.; Duffaud, A.; Panja, D.; Bramham, C.R.; Burri, L. Enhanced cognitive function and antidepres-sant-like effects after krill oil supplementation in rats. Lipids Health Dis 2013, 12, 6.
144. Batetta, B.; Griinari, M.; Carta, G.; Murru, E.; Ligresti, A.; Cordeddu, L.; Giordano, E.; Sanna, F.; Bisogno, T.; Uda, S., et al. Endocannabinoids may mediate the ability of (n-3) fatty acids to reduce ectopic fat and inflammatory mediators in obese zucker rats. J Nutr 2009, 139, 1495-1501.
145. Di Marzo, V.; Griinari, M.; Carta, G.; Murru, E.; Ligresti, A.; Cordeddu, L.; Giordano, E.; Bisog-
no, T.; Collu, M.; Batetta, B., et al. Dietary krill oil increases docosahexaenoic acid and reduces 2-arachidonoylglycerol but not n-acylethanol-amine levels in the brain of obese zucker rats. Int Dairy J 2010, 20, 231-235.
146. Ferramosca, A.; Conte, A.; Burri, L.; Berge, K.; De Nuccio, F.; Giudetti, A.M.; Zara, V. A krill oil supplemented diet suppresses hepatic steatosis in high-fat fed rats. PLoS One 2012, 7, e38797.
147. Piscitelli, F.; Carta, G.; Bisogno, T.; Murru, E.; Cordeddu, L.; Berge, K.; Tandy, S.; Cohn, J.S.; Grii-nari, M.; Banni, S., et al. Effect of dietary krill oil supplementation on the endocannabinoidome of metabolically relevant tissues from high-fat-fed mice. Nutr Metab (Lond) 2011, 8, 51.
148. Tandy, S.; Chung, R.W.; Wat, E.; Kamili, A.; Berge, K.; Griinari, M.; Cohn, J.S. Dietary krill oil supplementation reduces hepatic steato-sis, glycemia, and hypercholesterolemia in high-fat-fed mice. J Agric Food Chem 2009, 57, 9339-9345.
149. Tillander, V.; Bjorndal, B.; Burri, L.; Bohov, P.; Skorve, J.; Berge, R.K.; Alexson, S.E. Fish oil and krill oil supplementations differentially regulate lipid catabolic and synthetic pathways in mice. Nutr Metab (Lond) 2014, 11, 20.
150. Fosshaug, L.E.; Berge, R.K.; Beitnes, J.O.; Berge, K.; Vik, H.; Aukrust, P.; Gullestad, L.; Vinge, L.E.; Oie, E. Krill oil attenuates left ven-tricular dilatation after myocardial infarction in rats. Lipids Health Dis 2011, 10, 245.
151. Vigerust, N.F.; Bjorndal, B.; Bohov, P.; Brat-telid, T.; Svardal, A.; Berge, R.K. Krill oil versus fish oil in modulation of inflammation and lipid metabolism in mice transgenic for tnf-alpha. Eur J Nutr 2013, 52, 1315-1325.

62 KRILL OIL CONCENTRATE
152. Ierna, M.; Kerr, A.; Scales, H.; Berge, K.; Griinari, M. Supplementation of diet with krill oil protects against experimental rheumatoid arthritis. BMC Musculoskelet Disord 2010, 11, 136.
153. Ivanova, Z.; Bjorndal, B.; Grigorova, N.; Roussenov, A.; Vachkova, E.; Berge, K.; Burri, L.; Berge, R.; Stanilova, S.; Milanova, A., et al. Effect of fish and krill oil supplementation on glucose tolerance in rabbits with experimen-tally induced obesity. Eur J Nutr 2014.
154. Konagai, C.; Yanagimoto, K.; Hayamizu, K.; Han, L.; Tsuji, T.; Koga, Y. Effects of krill oil containing n-3 polyunsaturated fatty acids in phospholipid form on human brain function: A randomized controlled trial in healthy elderly volunteers. Clin Interv Aging 2013, 8, 1247-1257.
155. Deutsch, L. Evaluation of the effect of neptune krill oil on chronic inflammation and arthritic symptoms. J Am Coll Nutr 2007, 26, 39-48.
156. Banni, S.; Carta, G.; Murru, E.; Cordeddu, L.; Giordano, E.; Sirigu, A.R.; Berge, K.; Vik, H.; Maki, K.C.; Di Marzo, V., et al. Krill oil sig-nificantly decreases 2-arachidonoylglycerol plasma levels in obese subjects. Nutr Metab (Lond) 2011, 8, 7.
157. Bunea, R.; El Farrah, K.; Deutsch, L. Evalu-ation of the effects of neptune krill oil on the clinical course of hyperlipidemia. Altern Med Rev 2004, 9, 420-428.
158. Ulven, S.M.; Kirkhus, B.; Lamglait, A.; Basu, S.; Elind, E.; Haider, T.; Berge, K.; Vik, H.; Pedersen, J.I. Metabolic effects of krill oil are essentially similar to those of fish oil but at lower dose of epa and dha, in healthy volun-teers. Lipids 2011, 46, 37-46.
159. Berge, K.; Musa-Veloso, K.; Harwood, M.; Hoem, N.; Burri, L. Krill oil supplementation lowers serum triglycerides without increasing low-density lipoprotein cholesterol in adults with borderline high or high triglyceride levels. Nutr Res 2014, 34, 126-133.
160. Sampalis, F.; Bunea, R.; Pelland, M.F.; Kowalski, O.; Duguet, N.; Dupuis, S. Evalua-tion of the effects of neptune krill oil on the management of premenstrual syndrome and dysmenorrhea. Altern Med Rev 2003, 8, 171-179.
161. Albert, C.M.; Campos, H.; Stampfer, M.J.; Ridker, P.M.; Manson, J.E.; Willett, W.C.; Ma, J. Blood levels of long-chain n-3 fatty acids and the risk of sudden death. N Engl J Med 2002, 346, 1113-1118.
162. Harris, W.S.; Sands, S.A.; Windsor, S.L.; Ali, H.A.; Stevens, T.L.; Magalski, A.; Porter, C.B.; Borkon, A.M. Omega-3 fatty acids in cardiac biopsies from heart transplantation patients: Correlation with erythrocytes and response to supplementation. Circulation 2004, 110, 1645-1649.
163. Metcalf, R.G.; Cleland, L.G.; Gibson, R.A.; Roberts-Thomson, K.C.; Edwards, J.R.; Sanders, P.; Stuklis, R.; James, M.J.; Young, G.D. Relation between blood and atrial fatty acids in patients undergoing cardiac bypass surgery. The American journal of clinical nutrition 2010, 91, 528-534.
164. Metcalf, R.G.; James, M.J.; Gibson, R.A.; Edwards, J.R.; Stubberfield, J.; Stuklis, R.; Roberts-Thomson, K.; Young, G.D.; Cleland, L.G. Effects of fish-oil supplementation on myocardial fatty acids in humans. The American journal of clinical nutrition 2007, 85, 1222-1228.

63 KRILL OIL CONCENTRATE
165. von Schacky, C.; Fischer, S.; Weber, P.C. Long-term effects of dietary marine omega-3 fatty acids upon plasma and cellular lipids, platelet function, and eicosanoid formation in humans. J Clin Invest 1985, 76, 1626-1631.
166. Mozaffarian, D.; Ascherio, A.; Hu, F.B.; Stampfer, M.J.; Willett, W.C.; Siscovick, D.S.; Rimm, E.B. Interplay between different poly-unsaturated fatty acids and risk of coronary heart disease in men. Circulation 2005, 111, 157-164.
167. Miller, M.; Stone, N.J.; Ballantyne, C.; Bit-tner, V.; Criqui, M.H.; Ginsberg, H.N.; Goldberg, A.C.; Howard, W.J.; Jacobson, M.S.; Kris-Ether-ton, P.M., et al. Triglycerides and cardiovascu-lar disease: A scientific statement from the american heart association. Circulation 2011, 123, 2292-2333.
168. Harris, W.S. The omega-3 index: Clinical utility for therapeutic intervention. Curr Cardiol Rep 2010, 12, 503-508.
169. Siscovick, D.S.; Raghunathan, T.E.; King, I.; Weinmann, S.; Wicklund, K.G.; Albright, J.; Bovbjerg, V.; Arbogast, P.; Smith, H.; Kushi, L.H., et al. Dietary intake and cell membrane levels of long-chain n-3 polyunsaturated fatty acids and the risk of primary cardiac arrest. JAMA : the journal of the American Medical Associa-tion 1995, 274, 1363-1367.

64 KRILL OIL CONCENTRATE