lecture 9, fall 2014
TRANSCRIPT

Lecture 9
Laboratory Monitoring of An3coagulant Therapy
Assays to Monitor An3coagulant Response to Therapy

An3coagulant Therapy
• Goal ▫ Prevent the forma-on or extension of a thrombus
• Indica3ons ▫ Arterial thrombosis ▫ Atrial fibrilla3on ▫ Cerebrovascular disease ▫ Extracorporeal procedures – Renal dialysis, CPB ▫ Mechanical heart valves ▫ Myocardial infarc3on ▫ Peripheral vascular disease ▫ Radiologic procedures – Interven3onal/Diagnos3c ▫ Venous thromboembolism – DVT/PE
2
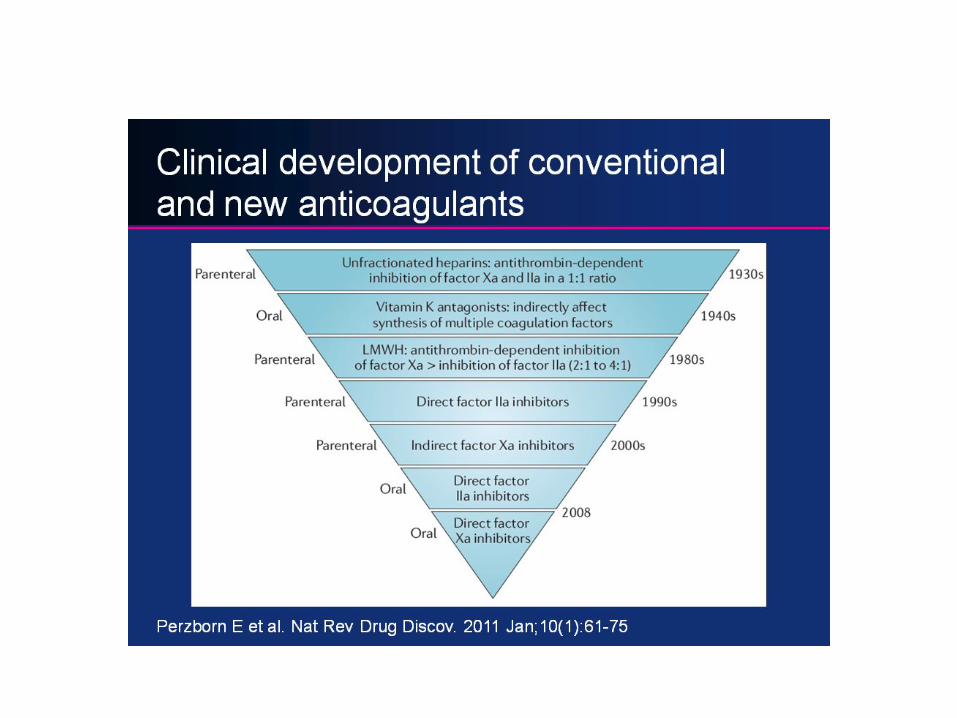

Tradi3onal Approach to An3coagulant Therapy
4
Heparin Coumarins Aspirin Clot busters
Venous thrombosis Arterial thrombosis
Target thrombin genera3on Interfere platelet func3on
Clot lysis
Two Classes of An3coagulant Drugs
• An3coagulant Drugs – Inhibit in vivo thrombosis – Prolong cloMng 3me – Show concentra3on-‐dependent effect on the clot-‐based assays
– Monitored with tradi-onal assays
• An3thrombo3c Drugs – Inhibit in vivo thrombosis – “Variable” prolonga3on of the cloMng 3me
– Monitored with nontradi-onal assays for monitoring effec3vely
5

Clot-‐based Assays Global screening assays Chromogenic Assays
• Nonspecific – PT, aPTT, TT, ACT – Depend on a func-onal coagula3on
cascade – Phospholipid dependent – Subject to numerous preanaly-cal
variables • Coagula3on factor abnormali3es • Inhibitors • Concurrent drug interac3ons
– Fast and inexpensive – PT, aPTT, TT, ACT
• Protein converted to its ac3ve form • Enzyme cleaves (hydrolyzes) a substrate
– Consists of a pep3de sequence and a chromophore (pNA)
• Pep3de releases the pNA à gives off a color • Measure intensity of the color • Subject to fewer preanaly3cal variables
6 Pa3ent Plasma
Ca2+ +
Reagent
Bates S M , Weitz J I Circulation 2005;112:e53-e60

Oral An3coagulants
• Most common of the oral an3coagulants • Frank W Schofield, 1922 ▫ Reported a bleeding diathesis in ca^le that simulated hemorrhagic sep3cemia and “black leg syndrome” ▫ Spoiled sweet clover mixed with hay
7

Oral An3coagulants
• Karl Paul Link, 1933, University of Wisconsin – A WI farmer—pail of blood that would not coagulate – Isolated and purified 3,3’-‐methylene-‐bis-‐[4-‐hydroxycoumarin] – Dicumarol and WARF-‐42
• Led to the iden3fica3on of Coumarin (Warfarin)
8

Oral An3coagulants
• Called Warfarin—WI Alumni Research Founda3on, 1948
• Mechanism à greatly diminished prothrombin ac3vity and delayed the blood cloMng mechanism ▫ Ini-ally used as a roden-cide ▫ Army inductee 1951 ▫ Dwight D Eisenhower 1955
9

Warfarin
• Coumarins—class of drugs which inhibit vitamin K ac3vity ▫ Warfarin (Coumadin) ▫ Acenocoumarol (Sintrom) ▫ Phenprocoumon (Marcoumar)
• Indica3ons ▫ Atrial fibrilla3on ▫ Prosthe3c heart valves ▫ Thromboembolic disease ▫ Hypercoagulable states ▫ Depressed cardiac func3on
10

Warfarin and Vitamin K
• Warfarin is an analogue of vitamin K • Vitamin K -‐ discovered from defects in
blood “koagula3on” • Vitamin K synthesized by plants and
bacteria ▫ Leafy green vegetables and intes3nal
flora • Vitamin K -‐ required coenzyme for post
transla3on modifica3on reac3on • γ-‐carboxyla3on of glutamic acid residues
1. Adds carboxyl group (COOH) onto Gla residues of the vitamin K dependent proteins
2. Needed for Ca2+ binding à clot forma3on
• Warfarin inhibits the ac-on of vitamin K • Vitamin K administra-on is the an-dote
for warfarin toxicity
11 Similari3es of Warfarin to Vitamin K

Vitamin K -‐ Carboxyglutamate FII, FV, FVII, FX, PC, PS
ACTIVE FII, FVII, FIX, FX, PC, PS
INACTIVE
oxidized reduced

Warfarin • Racemic mixture of two op3cally ac3ve
enan3omers– R and S ▫ S enanAomer is more potent
• “S” metabolized primarily by the CYP2C9 of cytochrome p450
• ½-‐life ~ 29 hours • Oral administra3on • Water soluble • Rapidly absorbed in stomach and
duodenum • Binds to albumin (~98%) ▫ Only the non-‐bound (FREE) form is
biologically ac3ve • Peak an3coagulant effect occurs 36-‐42
hours aper drug administra3on
13

Warfarin’s An3coagulant Effect
� Does NOT have a DIRECT an3coagulant effect � Onset of Warfarin’s effect is dependent on the ½-‐life of the VKDFs � PT/INR elevates rapidly due to the short ½-‐life of FVII • Full onset of Warfarin’s an3coagulant effect takes from 72-‐96 hours
� ***INR does NOT become stable un-l 72-‐96 hours
14
Factor Decreased aHer iniAaAon of Warfarin
Factor VII 6 hours
Factor IX 24 hours
Factor X 36 hours
Factor II 72 hours

Ac3on of Warfarin
InacAve FII, FVII, FIX, FX, PC, PS
WAR
FARIN
INACTIVE FII, FV, FVII, FX, PC, PS

Polymorphism CYP2C9
• CYP2C9*2 and CYP2C9*3 • Reduce clearance of S-‐enan3omer • Increase sensi3vity to warfarin
• Require ▫ Lower dose of warfarin ▫ Longer -me to reach steady state ▫ Result
� Higher risk for over-‐an-coagula-on and serious bleeding
� More common in Caucasian pa3ents
16
CYP2C9CYP2C9CYP1A1CYP1A1CYP1A2CYP1A2CYP3A4CYP3A4
RR--warfarinwarfarin
SS--warfarin
warfarin
Oxidized Vitamin KOxidized Vitamin K Reduced Vitamin KReduced Vitamin KOO22
HypofunctionalHypofunctionalF. II, VII, IX, XF. II, VII, IX, X
Protein C, S, ZProtein C, S, Z
Functional Functional F. II, VII, IX, XF. II, VII, IX, X
Proteins C, S, ZProteins C, S, Z
γ--glutamyl glutamyl carboxylasecarboxylase
Vitamin K Vitamin K ReductaseReductase
COCO22
WarfarinWarfarin
RR--warf
arin
warfari
n SS--warfarin
warfarin
Calumenin

Polymorphism of VKORC1
Ø VKORC1 is the “target” enzyme for Warfarin Ø VKORC1 is essen3al cofactor for
γ-‐carboxyla3on of VKDFs Ø Warfarin inhibits VKOR1’s ac3vity Ø Results in produc3on of “non-‐
func3on” PIVKAs
Ø VKORC1 polymorphisms
Ø Pa-ents have variable resistance and sensi3vity to Warfarin
Ø Need for lower doses of warfarin during long term therapy
17
Epoxide Reductase (VKORC1)
γ -Carboxylase (GGCX)
Warfarin
Molecular Interven-ons 6:223-‐227, (2006)

Heparin • Probably the most widely prescribed drug in the US • An3thrombo3c proper3es were described by McLean and Howell in 1918 • First used clinically as an an3thrombo3c agent in the 1930’s • Heterogeneous mixture of highly sulfated mucopolysaccharides ranging in
molecular weight from 3,000 – 30,000 Da –> averaging 15,000 Da • Contains alterna3ng residues of D-‐glucuronic acid and N-‐acetyl-‐D-‐
glucosamine
18

Heparin
• Naturally occurring an3coagulant produced by basophils and mast cells
• Exogenous heparin derived from two sources – Bovine lung 3ssue – Porcine intes3nal mucosa
• Two forms – Unfrac3onated Heparin (UFH)
– Low Molecular Weight Heparin (LMWH)
19

Heparin • Used clinically to treat
1. Prophylaxis and treatment of DVT
2. Treatment of PE or other clinically significant thromboses
3. Acute coronary syndrome, unstable angina, non-‐ST eleva3on AMI
4. Preven3on of stroke due to atrial fibrilla3on
5. Intra-‐opera3vely • Cardiopulmonary bypass surgery
• Coronary angioplasty • Vascular surgery • Hemodialysis
• Administered parentally—(degraded by oral administra3on)
20

Heparin: Mechanism of Ac3on
• Mechanism is mediated through an3thrombin in the coagula3on cascade
• Exerts is an3coagulant ac3vity via 2 proteins 1. An3thrombin (AT)
� Binds to an3thrombin � Induces a conforma3on change in AT molecule � Enhances AT-‐mediated inhibi3on of
� Thrombin, Factor Xa � Factors XIIa, XIa, IXa
2. Heparin Cofactor II (HCII) � Binds to heparin cofactor II (HCII) � HCII requires higher levels of
heparin � Specifically bind to thrombin

Unfrac3onated Heparin • In the absence of exogenous heparin ▫ AT binds to heparinoid substances located on the endothelium surface
� Dermatan sulfate � Chondroi3n sulfate � Heparan sulfate
22 h^p://www.ncbi.nlm.nih.gov/pmc/ar3cles/PMC1915585/figure/Fig1/
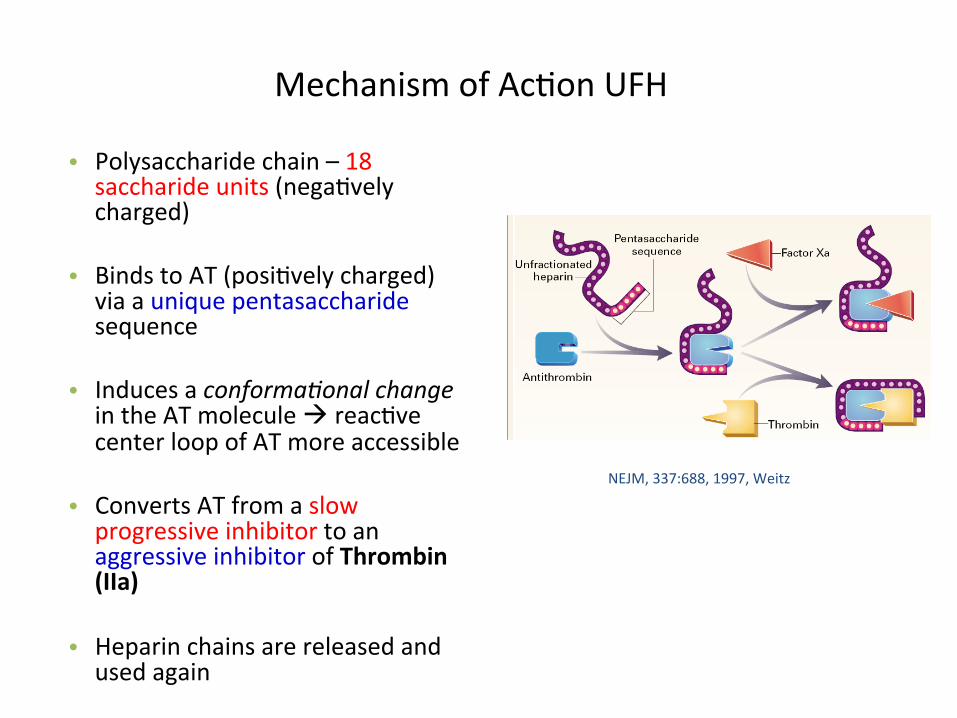
Mechanism of Ac3on UFH
• Polysaccharide chain – 18 saccharide units (nega3vely charged)
• Binds to AT (posi3vely charged) via a unique pentasaccharide sequence
• Induces a conforma-onal change in the AT molecule à reac3ve center loop of AT more accessible
• Converts AT from a slow progressive inhibitor to an aggressive inhibitor of Thrombin (IIa)
• Heparin chains are released and used again
23
NEJM, 337:688, 1997, Weitz

Mechanism of Ac3on UFH • Polysaccharide chain containing at
least 18 saccharide units • Binds to AT via a unique
pentasaccharide sequence • Induces a conforma3onal change in
the AT molecule • Converts AT from a slow progressive
inhibitor to an aggressive inhibitor of thrombin
• Heparin chain then serves as a template binding AT and Thrombin—(ternary complex)
• Heparin chain is released and is used again
• In the absence of exogenous heparin
– AT binds to heparinoid substances located on the endothelium surface
• Dermatan sulfate • Chondroi3n sulfate • Heparan sulfate
24
NEJM, 337:688, 1997, Weitz
Antithrombin
Thrombin
UFH
Pentasaccharide

Mechanism of Ac3on for LMWH
• Binds to AT via unique pentasaccharide sequence
• LMWH:AT complex binds to the ac3ve site of Xa and inhibits its ac3vity
• Exerts its an3coagulant ac3vity via AT
• Mean molecular weight 5000 Daltons – < 18 saccharide units
� Advantages � Bioavailability approaches 100% � Peak an3-‐Xa ac3vity occurs
between 3-‐5 hours sc � Rarely associated with HIT � Does not cause osteoporosis � Usually does not need to be
monitored
25
NEJM, 337:688, 1997, Weitz

1. FXa is added to plasma containing syntheAc factor Xa substrate with a chromophore a^ached to the end
2. Substrate is cleaved by FXa
3. Chromophore à color change à quan3fied – Directly propor3onal to enzyme ac3vity
4. If heparin (UFH/LMW) is present in plasma sample à it will promote factor Xa inhibi3on by AT à less FXa available to cleave substrate
5. Compared to standard curve using known amounts of heparin
Factor Xa Heparin Assay

Monitoring UFH—aPTT
� Most widely used test � Adapted to monitor heparin therapy � Inexpensive and easy to perform
• Perform 4-‐6 hours aper bolus dosage and every 24 hours thereaper � A dose adjustment requires monitoring 6 hours aper the dose adjustment
� 1.5-‐2.5 x “normal”
� Advantages – Rapid – Easy to perform – Inexpensive – Widely available
27

Factors Affec3ng the aPTT
Variable Mechanism
Sample collec3on and processing
Time of blood sampling Diurnal varia3on
Citrate concentra3on > Concentra3on à > prolonga3on
Centrifuga3on • Delayed plasma separa3on (>1 hr) à shorter cloMng 3me à PF4
• Platelet count < 10 x 109/L
Test Characteris3cs Reagent Variable responsiveness to UFH
Coagulometer Differences in methods of end point detec3on
Biologic variables UFH pharmacokine3cs • Altered intravascular volume (obesity, aging) • Increased concentra3ons of heparin binding proteins
(infec3on, inflamma3on, malignancy)
aPTT dose-‐response to UFH • Increased FVIII and Fibrinogen • Low concentra3on of AT (congenital, acute thrombosis,
LD) • Reduced levels of coagula3on proteins (DIC, LD)
Baseline aPTT • LA • Specific factor deficiencies (PK, HMWK, XII, XI, IX, VIII) • Reduced levels of coagula3on proteins (DIC, LD)
28

Addi3onal Tests to Monitor UFH
• An3-‐factor Xa assay (UFH)
▫ 4 hours aper administra3on ▫ Therapeu3c target—0.3-‐0.7 anA-‐Xa U/mL ▫ Monitor platelet count daily ▫ SUPERIOR to the aPTT assay for monitoring UFH therapy
29

Laboratory Monitoring of LMWH • Monitoring not required in most pa3ents • Collect blood sample 4 hours aper subcutaneous dose • Monitored only by the chromogenic an3-‐factor Xa assay
• Calibra3on curve – LMWH that the pa3ent is on – Commercial calibrators
• Perform regular CBCs to monitor platelet count, anemia, occult bloods
• Ranges: – Target range for prophylaxis—0.2 -‐ 0.4 an--‐Xa U/mL – Therapeu-c target range for 2x/day dosing—0.5 -‐ 1.1 an--‐Xa U/mL – Therapeu-c target range for 1x/day dosing—1.1 -‐ 2.0 an--‐Xa U/mL
• aPTT can not be used to monitor LMWH – insensi-ve to LMWH
30

Heparins
h^p://quizlet.com/13750648/pharm-‐test-‐1-‐coagula3on-‐flash-‐cards/

Ac3vated CloMng Time
• Used to monitor pa3ents on extremely high doses of heparin – CPB
• Range = 71 – 180 seconds • Heparin = 400 – 500 seconds
• Does not correlate well with other coagula-on tests
32
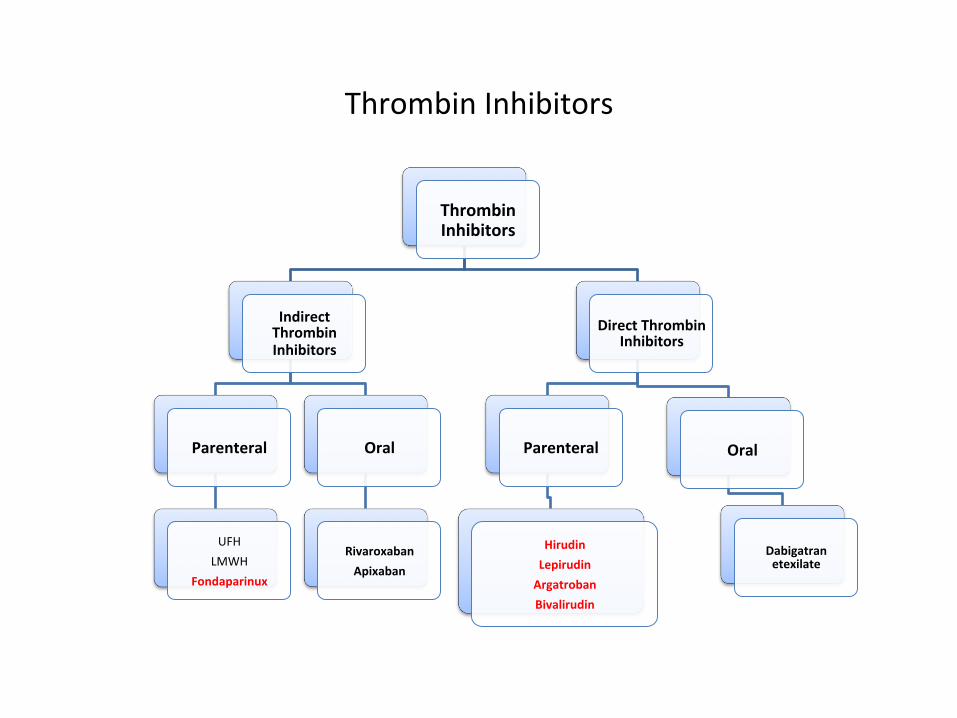
Thrombin Inhibitors
Thrombin Inhibitors
Indirect Thrombin Inhibitors
Parenteral
UFH LMWH
Fondaparinux
Oral
Rivaroxaban Apixaban
Direct Thrombin Inhibitors
Parenteral
Hirudin Lepirudin Argatroban Bivalirudin
Oral
Dabigatran etexilate
33

Fondaparinux (Arixtra) � Synthe3c pentasaccharide
� Mechanism � Contains the unique pentasaccharide sequence � Binds to AT à Inhibits Factor Xa
� Indirect inhibitor of IIa
34 NEJM

Pharmacology of the Pentasaccharides • Predictable dose response
– Administered 1x/day – Plasma half-‐life 14-‐24 hours – Does not bind PF4 or plasma proteins – Monitoring generally not necessary
• Peak ac3vity – 3 hours
• No an3dote, protamine ineffec3ve – Most common adverse reac3on is bleeding – Excreted by the kidneys
• Indica3ons
– Orthopedic periopera3ve DVT prophylaxis • Approved for use in the preven3on of DVT in hip and knee replacement à Fondaparinux
35
Pa-ents with history of HIT Despite no reac-on with PF4*

Hirudin • Most powerful naturally occurring
inhibitor of thrombin
• Found in the salivary glands of medicinal leech (Hirudo medicinalis)
• 65-‐amino acid polypep-de
• Available in recombinant form – Lepirudin and Desirudin – Differ from the natural form
only by the absence of sulfated tyrosine residue at posi-on -‐63
• Plasma half-‐life— 60-‐120 minutes ader subcutaneous injec-on
• Excreted by the kidneys
36 h\p://www.theguardian.com/money/us-‐money-‐blog/2014/mar/09/leech-‐therapy-‐brooklyn-‐immigrants-‐favor-‐leeches

Lepirudin (Refludan—Berlex)
• Recombinant form of Hirudin released in 1988
• ~65 amino acids with a molecular weight of 7000 Daltons
• First direct thrombin inhibitor approved
by FDA for HIT
• Pharmacology – Inhibits both circula3ng and clot-‐
bound thrombin – Does not cross-‐react with HIT
an3bodies – Plasma half-‐life—60-‐120 minutes – ~40% of pa-ents develop
an-bodies to Lepirudin • Prolongs clearance without
abroga3ng its ac3vity
▫ Monitoring with aPTT ▫ aPTT target is 1.5-‐2.5 3mes mean
reference value � 4 hrs aper ini3a3on
37

Argatroban
• Synthe33c compe33ve inhibitor of thrombin derived from L-‐arginine
• Pharmacology – Does not interact with PF4
– Smaller size makes if more effec3ve than hirudin at inhibi3ng clot-‐bound thrombin
– Metabolized in the liver and excreted in the feces
– Half-‐life ~ 45 minutes
38

Bivalirudin (Angiomax)
• Synthe-c 20 amino-‐acid-‐pep3de analog of Hirudin
• ½-‐life ~25 minutes • Neutralizes free and bound
thrombin • No an3body forma3on • Excreted by the kidney
• Indica3ons – Reduce the risk of acute ischemic
complica-ons a) Procedures in pa-ents with
unstable angina pectoris undergoing PCI
b) Has been successful in pa-ents with HIT
39

New “Oral” An3coagulants Direct and Indirect Thrombin Inhibitors
40

Dabigatran Etexilate Mesylate (Pradaxa) Boehringer-‐Ingelheim
• Novel oral factor IIa inhibitor • Cleared by FDA (10/19/2010) for stroke
preven3on in atrial fibrilla3on • Prodrug converted to an ac3ve drug • Several advantages over Warfarin and
Enoxaparin – Specifically and selec3vely inhibits both free
and clot bound thrombin – Predictable and consistent pharmacokine3c
profile – Not significantly affected by interac3ons
with food – Not metabolized by cytochrome P450
system • Does not affect the metabolism of other drugs that u-lize this system
• Lower poten-al for drug interac-ons
41
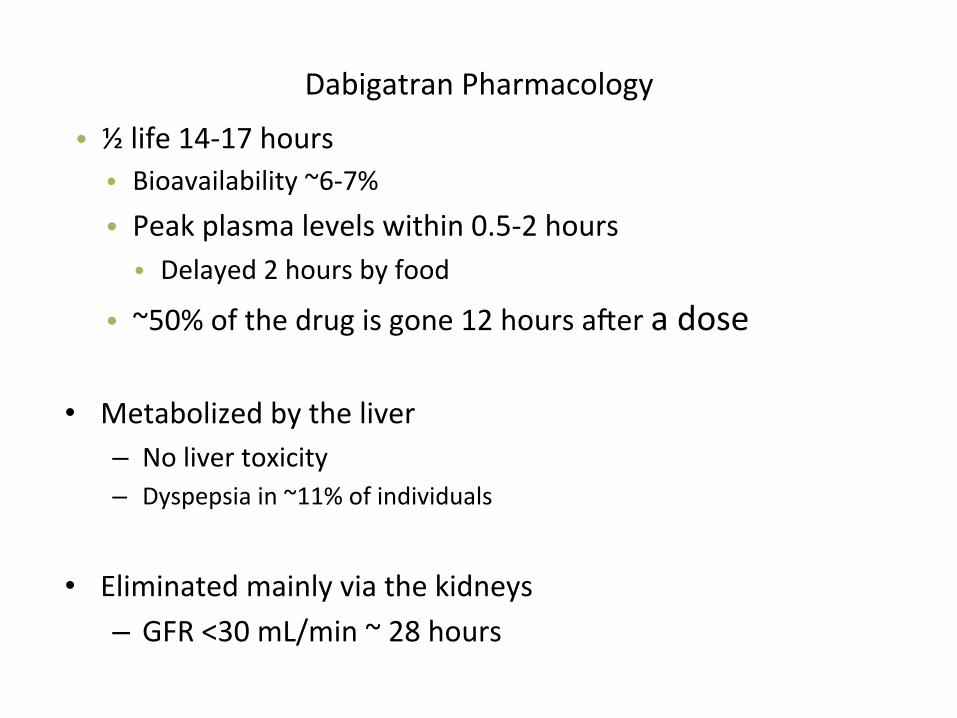
Dabigatran Pharmacology
• ½ life 14-‐17 hours • Bioavailability ~6-‐7% • Peak plasma levels within 0.5-‐2 hours • Delayed 2 hours by food • ~50% of the drug is gone 12 hours aper a dose
• Metabolized by the liver – No liver toxicity – Dyspepsia in ~11% of individuals
• Eliminated mainly via the kidneys – GFR <30 mL/min ~ 28 hours
42

Rivaroxaban (Xarelto) Bayer/Johnson & Johnson
• Potent, selec3ve, oral factor Xa inhibitor
• Cleared by FDA (10/19/2012) for stroke preven3on in atrial fibrilla3on
• Minimal interac3ons with food and drugs
• Non-‐inferior to warfarin for preven3on of stroke and non-‐CNS embolism
43

Rivaroxaban Pharmacology
• ½ life ~13 hours • Bioavailability ~80% • Peak plasma level in 2-‐4 hours • ~12 hours in pa3ents >75, 5-‐9 hours (young individuals)
• Metabolized by liver • CYP3A4, CYP3A5, CYP2J2
• Excreted by Kidney • Urine 66% • Feces 33%
44

Apixaban (Eliquis) Bristol-‐Myers Squibb/Pfizer
• Oral, direct, selec3ve factor Xa inhibitor
• No forma3on of reac3ve intermediates
• No organ toxicity or LFT abnormali3es in chronic toxicology studies
• Low likelihood of drug interac3ons or QTc prolonga3on – Good oral bioavailability – No food interac3ons – Balanced elimina3on (~25% renal) – ½-‐life ~12 hrs
• FDA approval 12/28/2012
45
NN
NO
N O
NH2
O
O

Fibrinoly3c Agents
• Thromboly3c (fibrinoly3c) therapy is used to restore vascular patency in order to prevent loss of 3ssue, limb, and organ func3on
▫ Indica3ons � AMI � PE/DVT � Thrombo3c stroke � PAD � Occlusion of indwelling catheter
46

Fibrinoly3c Agents ▫ Mechanism of Ac3on
1. Acts by conver3ng plasminogen to plasmin 2. Plasmin lyses clots by diges3ng fibrin contained in clots
47

Two Classes of Fibrinoly3c Agents
� Streptokinase � 1st thromboly3c agent � Derived from Streptococcus � Long half-‐life � Pa-ents can develop an-bodies
� Urokinase � Direct ac3vator of plasminogen � Derived from human -ssue culture media and recombinant deriva-ves � Not used for coronary disease—more commonly used for catheter-‐based thrombosis
� tPA � One of the first recombinant forms � Secreted by endothelial cells � Converts plasminogen to plasmin
48
Fibrin Non
-‐Spe
cific
Fibrin Spe
cific
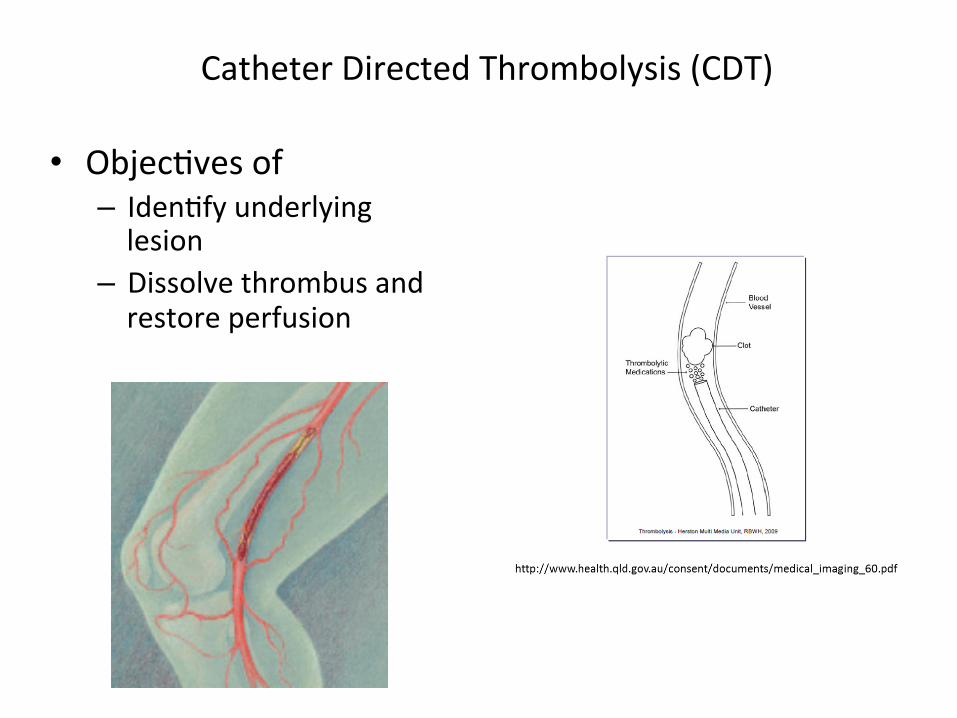
Catheter Directed Thrombolysis (CDT)
• Objec3ves of – Iden3fy underlying lesion
– Dissolve thrombus and restore perfusion

Monitoring Fibrinoly3c Agents
• D-‐Dimer • FDP • Euglobulin Lysis Time • Plasminogen • α2An3plasmin • Plasminogen ac3vator inhibitor-‐1
50

IVC Filters
51
Indica3ons: 1. Pa3ents in whom an3coagulant therapy is
contra-‐indicated 2. When an3coagula3on therapy is not working
Placed below the junc3on of the IVC and the lowest renal vein
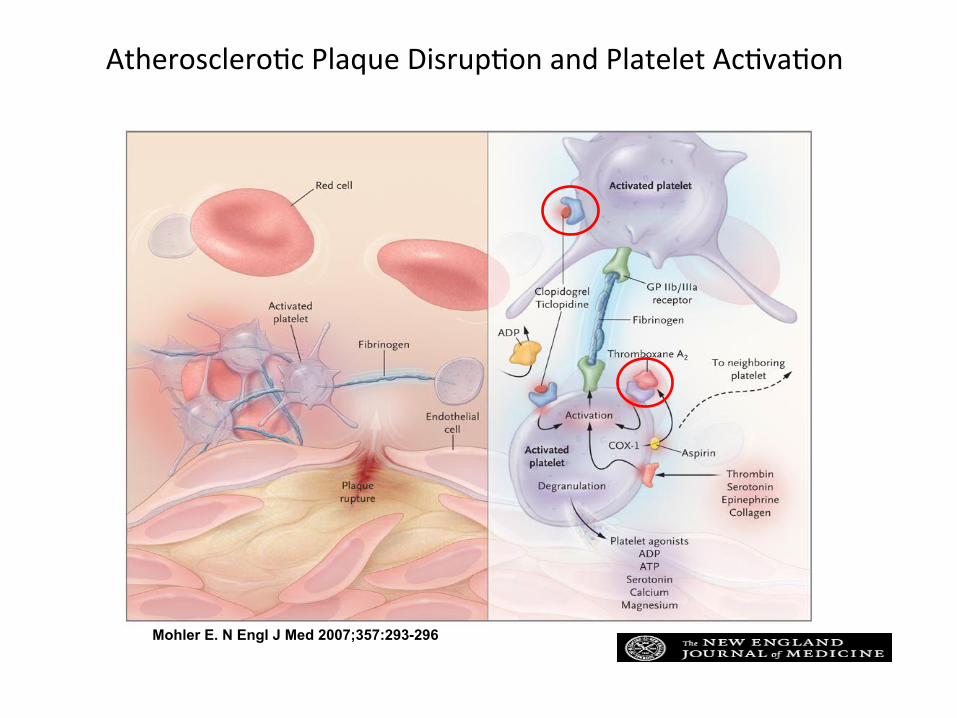
Atherosclero3c Plaque Disrup3on and Platelet Ac3va3on
Mohler E. N Engl J Med 2007;357:293-296

An3platelet Therapies • Proven efficacy in the treatment of acute thrombosis and preven-on of arterial
thrombosis • However they do increase the risk of bleeding
53
Target Drug Cyclooxygenase inhibitors Ø Aspirin
Ø NSAIDS Ø Ibuprofen (Motrin) Ø Indomethacin (Indocin) Ø Naproxen (Aleve)
ADP receptor antagonists Ø Thienopyridines Ø Ticlopidine Ø Clopidogrel
GPIIb/IIIa antagonists Ø Abciximab Ø Tirofiban Ø Ep3fiba3de
Phosphodiesterase inhibitors Ø Dipyridamole

An3platelet Drugs
Ø Cyclooxygenase inhibitors – Aspirin
• Mechanism of ac3on 1. Irreversibly inhibits cyclooxygenase-‐1
in platelets and megakaryocytes 2. Blocks the forma3on of Thromboxane
A2
• Immediate an-thrombo-c effect lasts 7-‐10 days
a) Inhibi3on of COX-‐1 achieved with low doses of aspirin
b) Inhibi3on of COX-‐2 requires larger doses of aspirin
• Pharmacokine3cs – Absorbed in the stomach and upper
intes3ne – Peak plasma levels
• 30-‐40 minutes aper inges3on • 3-‐4 hours with enteric-‐coated
aspirin – Inhibi3on of platelet func3on occurs in
1 hour
54
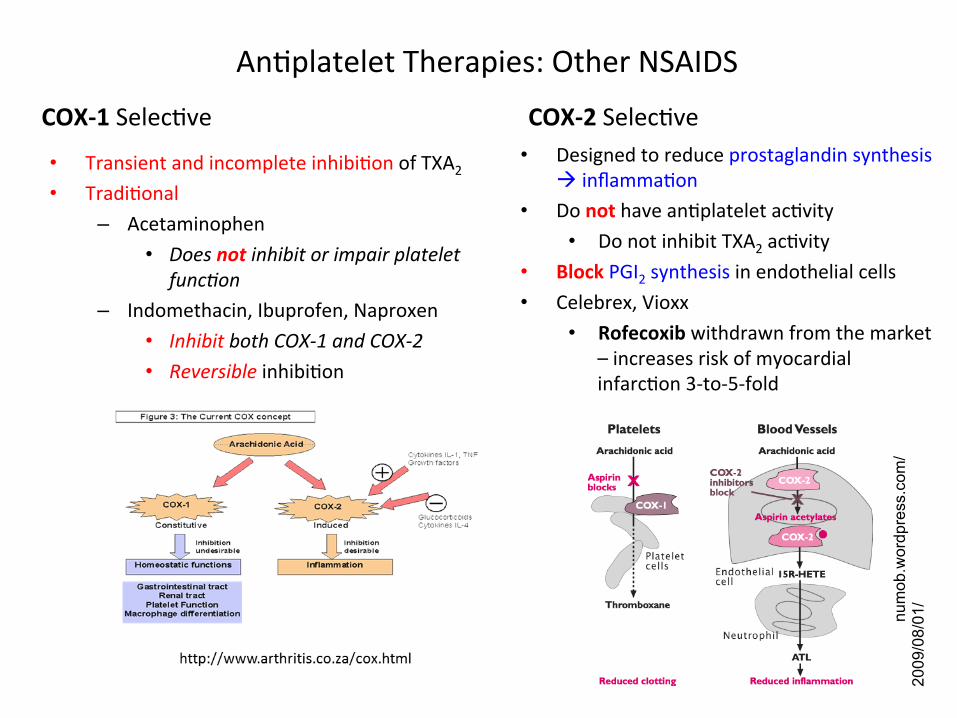
An3platelet Therapies: Other NSAIDS
COX-‐1 Selec3ve COX-‐2 Selec3ve • Transient and incomplete inhibi3on of TXA2 • Tradi3onal
– Acetaminophen • Does not inhibit or impair platelet
func-on – Indomethacin, Ibuprofen, Naproxen
• Inhibit both COX-‐1 and COX-‐2 • Reversible inhibi3on
• Designed to reduce prostaglandin synthesis à inflamma3on
• Do not have an3platelet ac3vity • Do not inhibit TXA2 ac3vity
• Block PGI2 synthesis in endothelial cells • Celebrex, Vioxx
• Rofecoxib withdrawn from the market – increases risk of myocardial infarc3on 3-‐to-‐5-‐fold
num
ob.w
num
ob.w
ordp
ress
.com
/20
09/0
8/01
/ord
pres
s.co
m/2
009/
08/0
1/ยา

An3platelet Therapies: Aspirin • Adverse effects ▫ Aspirin Resistance—inability of aspirin to:
1. Protect individuals from thrombo3c complica3ons � Inability to reduce TXA2 produc-on in pa-ents � Clinical aspirin resistance
2. To inhibit TXA2-‐dependent platelet aggrega3on – In one or more in vitro “tests” of platelet func-on – Laboratory (pharmacologic) resistance
▫ Associated with upper-‐GI toxicity ▫ Note:
� Aspirin does not cause a generalized bleeding abnormality unless given to pa-ents with an underlying � Hemosta-c defect � Uremia � Concomitant an-coagulant therapy
56

Aspirin

Aspirin on Platelets and Endothelial Cells
www.nbs.csudh.edu/chemistry/faculty/nsturm/CHE452/10_Arachidon…

An3platelet Drugs ADP receptor antagonists – THIENOPYRIDINES
▫ ADP ac3vates platelets by binding its purinergic P2Y1 and P2Y12 receptors � P2Y1 mediates Ca2+ mobiliza3on, shape
change and a transient reversible aggrega3on � P2Y12 induces las3ng aggrega3on and
decrease in cAMP
Thienopyridines 1. Clopidogrel (Plavix)
� Irreversibly blocks the ADP P2Y12 receptor à inhibi3on of gpIIb/IIIa receptor
� Inhibits platelet aggrega3on
2. Ticlopidine (Ticlid) � Blocks the ADP P2Y12 receptor à
inhib3on of gpIIb/IIIa receptor � Inhibits platelet aggrega3on and
release
59
Prasugrel -‐-‐ Effient® is an inhibitor of platelet ac3va3on and aggrega3on through the irreversible binding of its ac3ve metabolite to the P2Y12 class of ADP receptors on platelets

An3platelet Drugs Ø GPIIb/IIIa antagonists
Ø Block the gpIIb/IIIa fibrinogen binding receptor
Ø Prevent the crucial mechanical step in aggrega3on
Ø Strongest an3thrombo3c poten3al
1. Abciximab (ReoPro) � Monoclonal an3body that binds to the
IIb/IIIa receptor to block platelet aggrega3on
2. Ep3fiba3de (Integrelin) � SyntheAc cyclic hexapep3de
derived from a snake venom that irreversibly binds the IIb/IIIa receptor
3. Tirofiban (Aggrastat) � SyntheAc, non-‐pep3de inhibitor of
IIb/IIIa receptor
60

An3platelet Drugs Ø Phosphodiesterase inhibitors
Ø Inhibit platelet aggrega3on by increasing cAMP
Ø Elevated cAMP inhibits platelet func3on
ü Dipyridamole (PersanAne) � Inhibits the
phosphodiesterase enzymes which normally break down cAMP a. Increases cAMP ▫ Blocks platelet response
to ADP ▫ Inhibits aggregaAon
response to collagen, epinephrine, ADP
b. Does not prolong the bleeding 3me
61

h^p://circ.ahajournals.org/content/123/7/798/F3.large.jpg

www.nature.com/nrd/jo
urnal/v
9/n2
/full/n
rd2957.htm
l