lab 5: respiratory system and bone bone … updated: 8/14/13 lab 5: respiratory system and bone the...
TRANSCRIPT
Last Updated: 8/14/13
LAB 5: RESPIRATORY SYSTEM AND BONE The focus of this week’s lab will be pathology of the respiratory tract and bone. BONE TISSUE There are two major types of bone compact (cortical) bone and cancellous (spongy or trabecular) bone. Compact bone forms the dense outer layer of all bone and makes up approximately 80 % of the adult skeletal mass. Spongy bone forma a meshwork in which bone marrow is found. You will see cases that include both types of bone. Remember that bone is constantly being remodeled throughout life and remodeling is dependent on many different factors including age, hormone levels, and nutritional status. You will also look at bone marrow, which contains the progenitors for bone cells (osteoblasts and osteoclasts) as well as stem cells for all blood cells. Disruption of bone cell and blood stem cell development can result in a wide variety of pathological states. The cases we will cover and their virtual microscope slides are given below:
A. Multiple Myeloma, Virtual microscope slide p41. https://med-vmicro.med.illinois.edu/v/543/
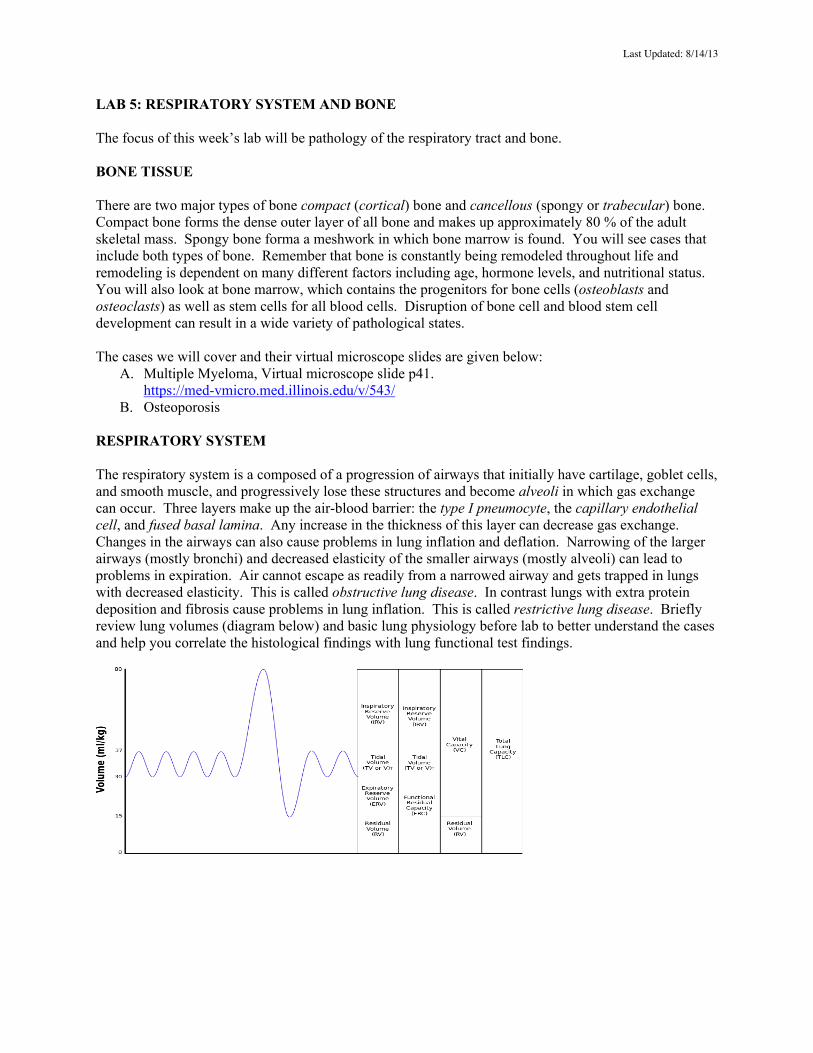
B. Osteoporosis RESPIRATORY SYSTEM The respiratory system is a composed of a progression of airways that initially have cartilage, goblet cells, and smooth muscle, and progressively lose these structures and become alveoli in which gas exchange can occur. Three layers make up the air-blood barrier: the type I pneumocyte, the capillary endothelial cell, and fused basal lamina. Any increase in the thickness of this layer can decrease gas exchange. Changes in the airways can also cause problems in lung inflation and deflation. Narrowing of the larger airways (mostly bronchi) and decreased elasticity of the smaller airways (mostly alveoli) can lead to problems in expiration. Air cannot escape as readily from a narrowed airway and gets trapped in lungs with decreased elasticity. This is called obstructive lung disease. In contrast lungs with extra protein deposition and fibrosis cause problems in lung inflation. This is called restrictive lung disease. Briefly review lung volumes (diagram below) and basic lung physiology before lab to better understand the cases and help you correlate the histological findings with lung functional test findings.
Last Updated: 8/14/13
The cases we will cover and their virtual microscope slides are given below: C. Emphysema, p235
https://med-vmicro.med.illinois.edu/v/542/ D. Acute Respiratory Distress Syndrome, p227
https://med-vmicro.med.illinois.edu/v/540/ E. Asthma, p139
https://med-vmicro.med.illinois.edu/v/541/ For reference to a normal lung, see virtual slide p178. https://med-vmicro.med.illinois.edu/v/544/
A. MULTIPLE MYELOMA https://med-vmicro.med.illinois.edu/v/543/
CC/HPI: A 64-year-old African American man suffers from bone pain, weight loss, and easy fatigability. He complains of recurrent upper respiratory tract infections and frequent nosebleeds.
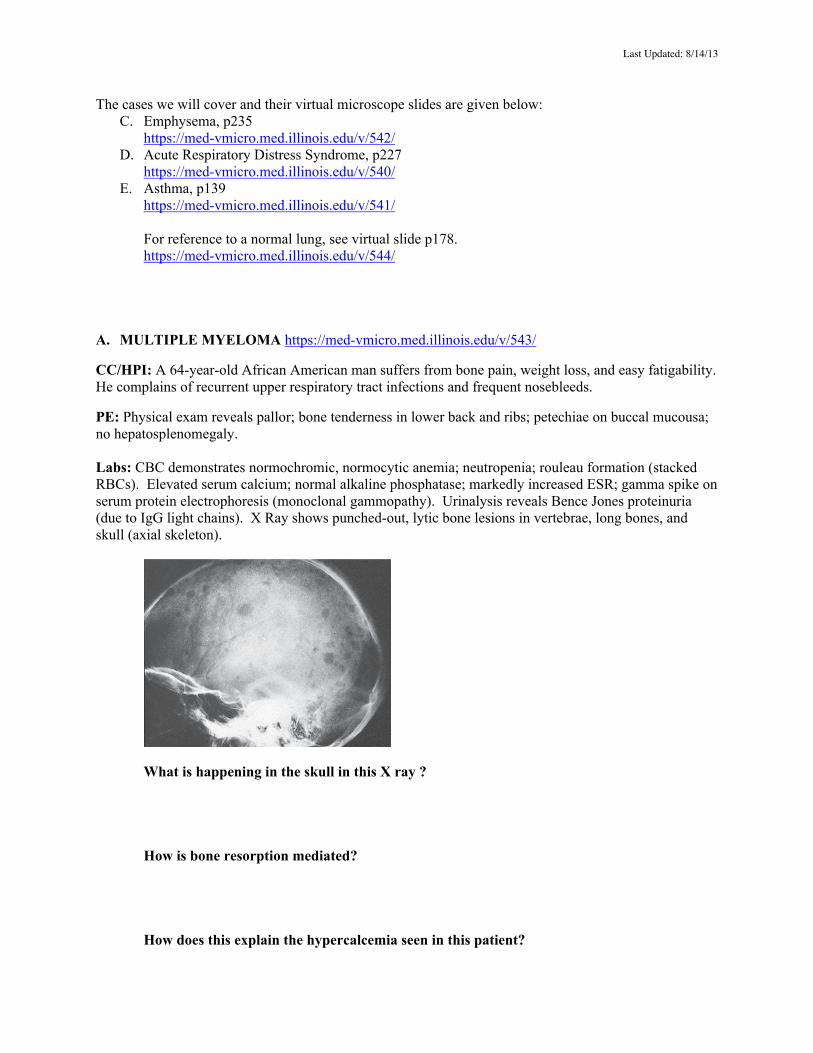
PE: Physical exam reveals pallor; bone tenderness in lower back and ribs; petechiae on buccal mucousa; no hepatosplenomegaly. Labs: CBC demonstrates normochromic, normocytic anemia; neutropenia; rouleau formation (stacked RBCs). Elevated serum calcium; normal alkaline phosphatase; markedly increased ESR; gamma spike on serum protein electrophoresis (monoclonal gammopathy). Urinalysis reveals Bence Jones proteinuria (due to IgG light chains). X Ray shows punched-out, lytic bone lesions in vertebrae, long bones, and skull (axial skeleton).
What is happening in the skull in this X ray ?
How is bone resorption mediated?
How does this explain the hypercalcemia seen in this patient?
Last Updated: 8/14/13
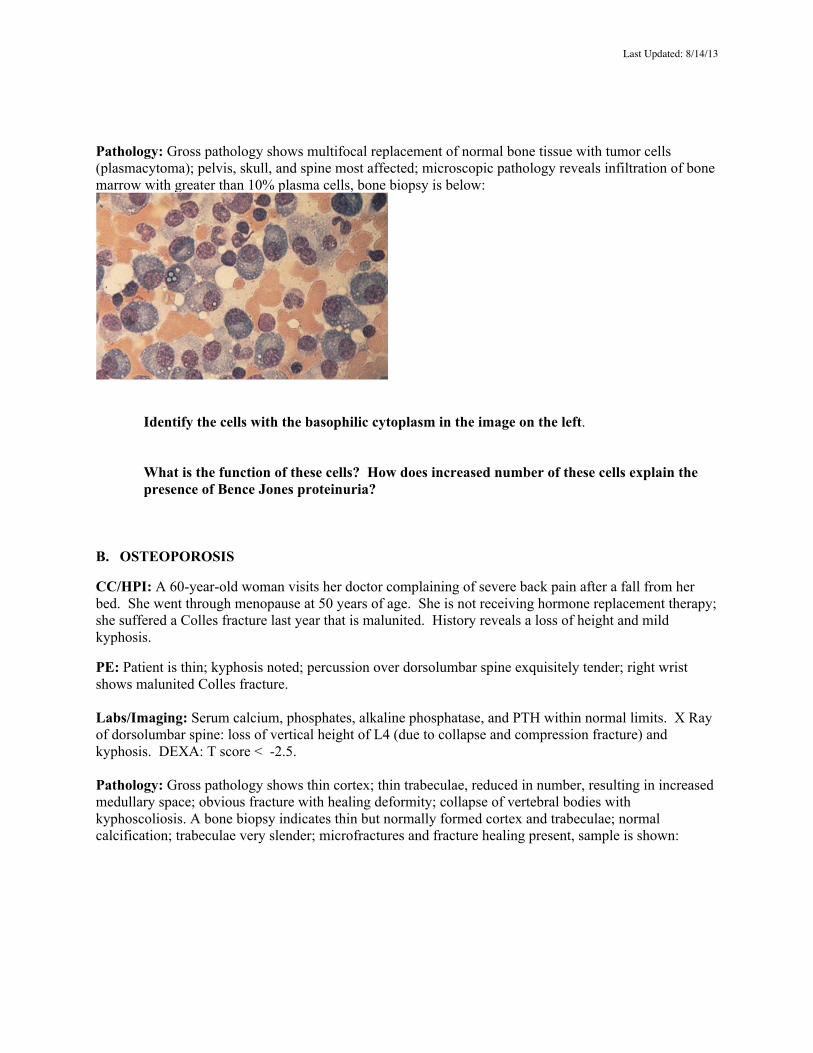
Pathology: Gross pathology shows multifocal replacement of normal bone tissue with tumor cells (plasmacytoma); pelvis, skull, and spine most affected; microscopic pathology reveals infiltration of bone marrow with greater than 10% plasma cells, bone biopsy is below:
Identify the cells with the basophilic cytoplasm in the image on the left. What is the function of these cells? How does increased number of these cells explain the presence of Bence Jones proteinuria?
B. OSTEOPOROSIS
CC/HPI: A 60-year-old woman visits her doctor complaining of severe back pain after a fall from her bed. She went through menopause at 50 years of age. She is not receiving hormone replacement therapy; she suffered a Colles fracture last year that is malunited. History reveals a loss of height and mild kyphosis.
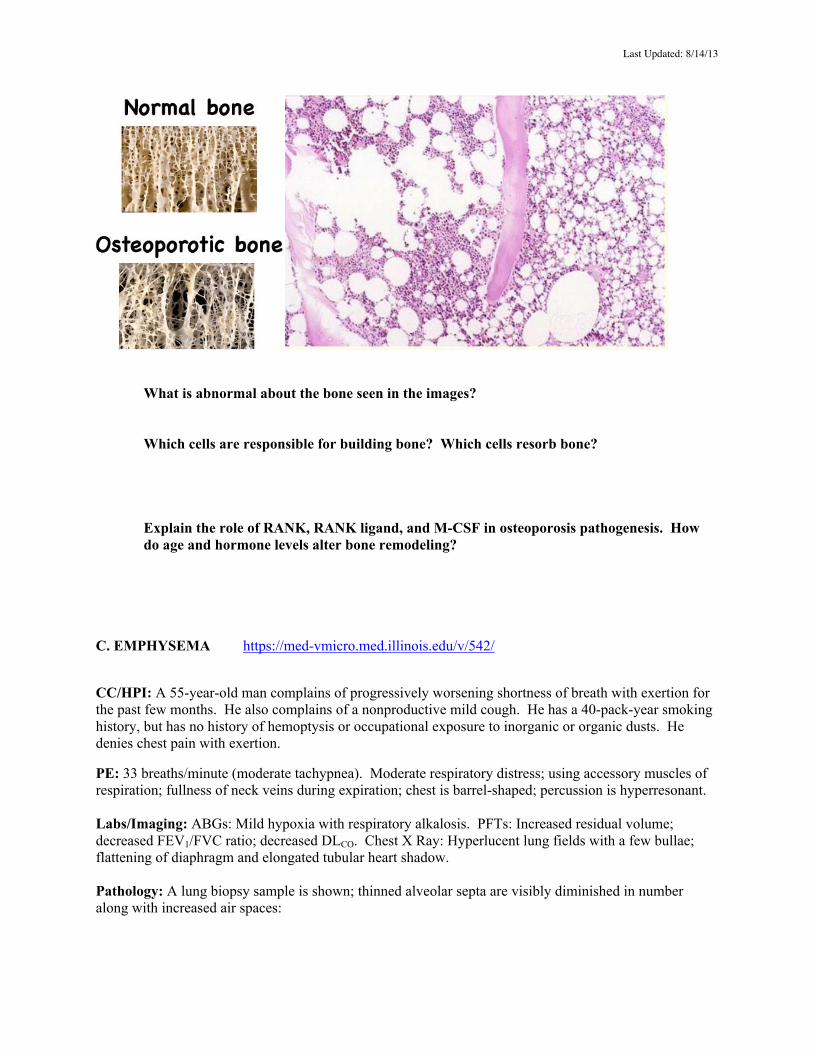
PE: Patient is thin; kyphosis noted; percussion over dorsolumbar spine exquisitely tender; right wrist shows malunited Colles fracture. Labs/Imaging: Serum calcium, phosphates, alkaline phosphatase, and PTH within normal limits. X Ray of dorsolumbar spine: loss of vertical height of L4 (due to collapse and compression fracture) and kyphosis. DEXA: T score < -2.5. Pathology: Gross pathology shows thin cortex; thin trabeculae, reduced in number, resulting in increased medullary space; obvious fracture with healing deformity; collapse of vertebral bodies with kyphoscoliosis. A bone biopsy indicates thin but normally formed cortex and trabeculae; normal calcification; trabeculae very slender; microfractures and fracture healing present, sample is shown:
Last Updated: 8/14/13
What is abnormal about the bone seen in the images?
Which cells are responsible for building bone? Which cells resorb bone?
Explain the role of RANK, RANK ligand, and M-CSF in osteoporosis pathogenesis. How do age and hormone levels alter bone remodeling?
C. EMPHYSEMA https://med-vmicro.med.illinois.edu/v/542/
CC/HPI: A 55-year-old man complains of progressively worsening shortness of breath with exertion for the past few months. He also complains of a nonproductive mild cough. He has a 40-pack-year smoking history, but has no history of hemoptysis or occupational exposure to inorganic or organic dusts. He denies chest pain with exertion.
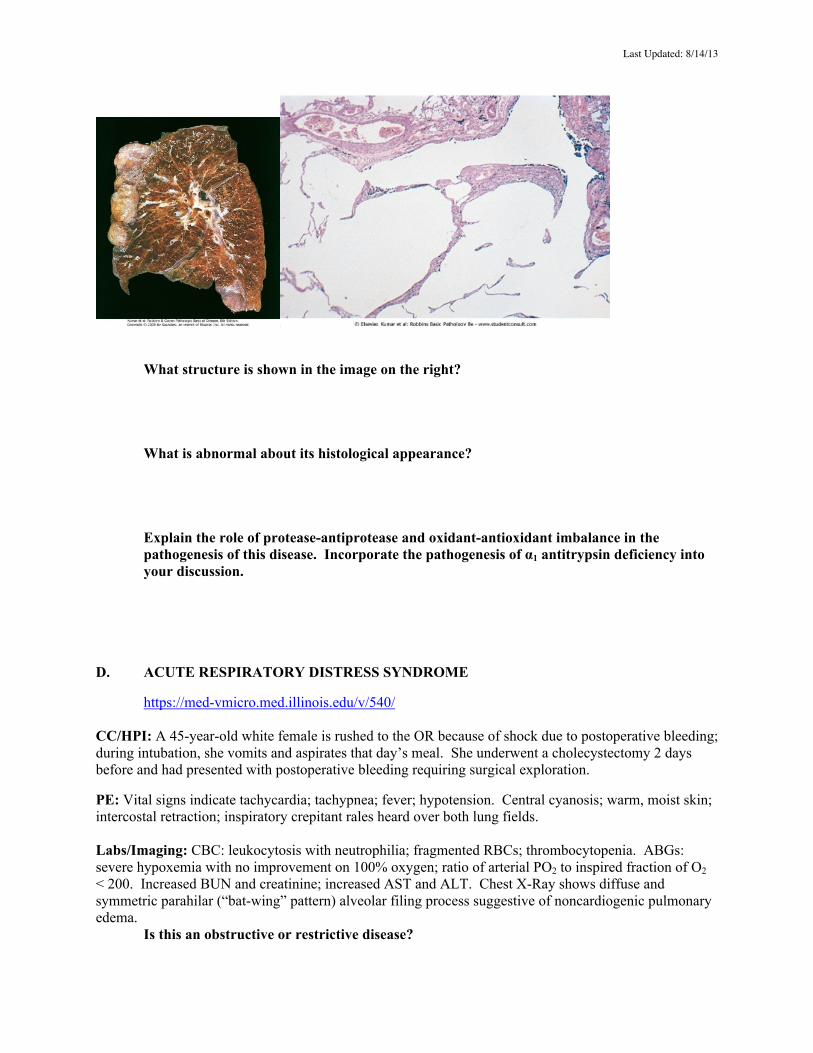
PE: 33 breaths/minute (moderate tachypnea). Moderate respiratory distress; using accessory muscles of respiration; fullness of neck veins during expiration; chest is barrel-shaped; percussion is hyperresonant. Labs/Imaging: ABGs: Mild hypoxia with respiratory alkalosis. PFTs: Increased residual volume; decreased FEV1/FVC ratio; decreased DLCO. Chest X Ray: Hyperlucent lung fields with a few bullae; flattening of diaphragm and elongated tubular heart shadow. Pathology: A lung biopsy sample is shown; thinned alveolar septa are visibly diminished in number along with increased air spaces:
Last Updated: 8/14/13
What structure is shown in the image on the right? What is abnormal about its histological appearance? Explain the role of protease-antiprotease and oxidant-antioxidant imbalance in the pathogenesis of this disease. Incorporate the pathogenesis of α1 antitrypsin deficiency into your discussion.
D. ACUTE RESPIRATORY DISTRESS SYNDROME
https://med-vmicro.med.illinois.edu/v/540/
CC/HPI: A 45-year-old white female is rushed to the OR because of shock due to postoperative bleeding; during intubation, she vomits and aspirates that day’s meal. She underwent a cholecystectomy 2 days before and had presented with postoperative bleeding requiring surgical exploration.
PE: Vital signs indicate tachycardia; tachypnea; fever; hypotension. Central cyanosis; warm, moist skin; intercostal retraction; inspiratory crepitant rales heard over both lung fields. Labs/Imaging: CBC: leukocytosis with neutrophilia; fragmented RBCs; thrombocytopenia. ABGs: severe hypoxemia with no improvement on 100% oxygen; ratio of arterial PO2 to inspired fraction of O2 < 200. Increased BUN and creatinine; increased AST and ALT. Chest X-Ray shows diffuse and symmetric parahilar (“bat-wing” pattern) alveolar filing process suggestive of noncardiogenic pulmonary edema. Is this an obstructive or restrictive disease?
Last Updated: 8/14/13
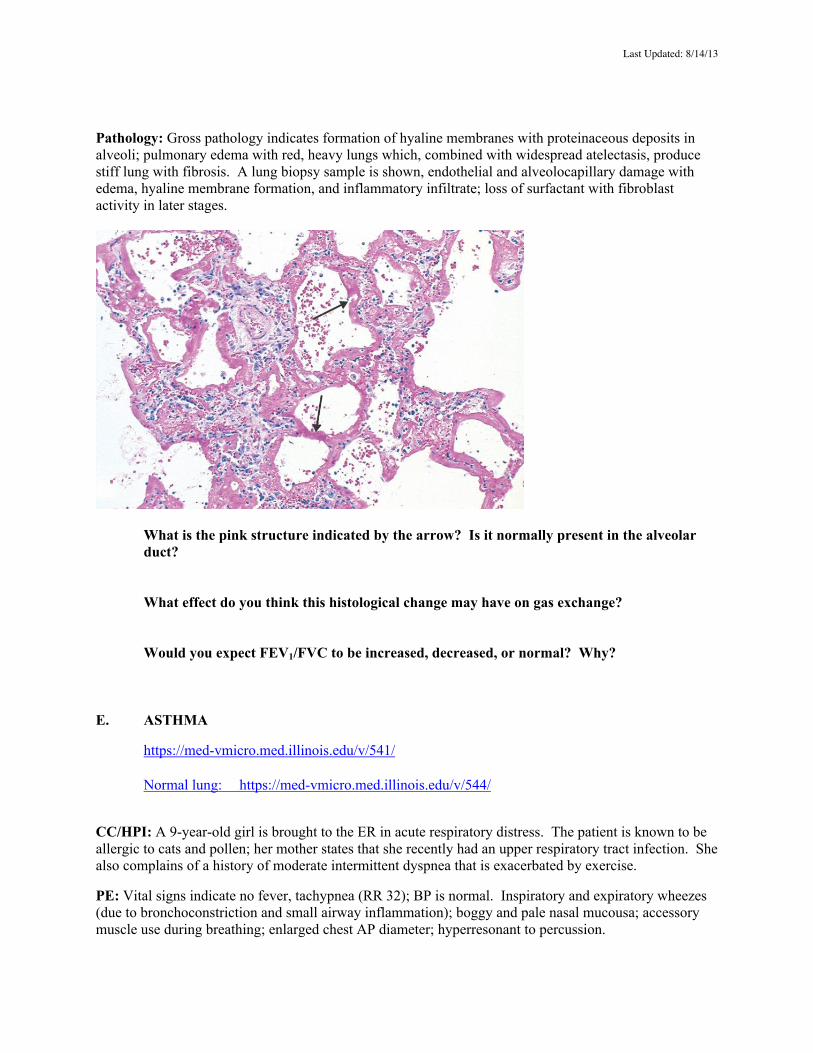
Pathology: Gross pathology indicates formation of hyaline membranes with proteinaceous deposits in alveoli; pulmonary edema with red, heavy lungs which, combined with widespread atelectasis, produce stiff lung with fibrosis. A lung biopsy sample is shown, endothelial and alveolocapillary damage with edema, hyaline membrane formation, and inflammatory infiltrate; loss of surfactant with fibroblast activity in later stages.
What is the pink structure indicated by the arrow? Is it normally present in the alveolar duct? What effect do you think this histological change may have on gas exchange? Would you expect FEV1/FVC to be increased, decreased, or normal? Why?
E. ASTHMA
https://med-vmicro.med.illinois.edu/v/541/ Normal lung: https://med-vmicro.med.illinois.edu/v/544/
CC/HPI: A 9-year-old girl is brought to the ER in acute respiratory distress. The patient is known to be allergic to cats and pollen; her mother states that she recently had an upper respiratory tract infection. She also complains of a history of moderate intermittent dyspnea that is exacerbated by exercise.
PE: Vital signs indicate no fever, tachypnea (RR 32); BP is normal. Inspiratory and expiratory wheezes (due to bronchoconstriction and small airway inflammation); boggy and pale nasal mucousa; accessory muscle use during breathing; enlarged chest AP diameter; hyperresonant to percussion.
Last Updated: 8/14/13
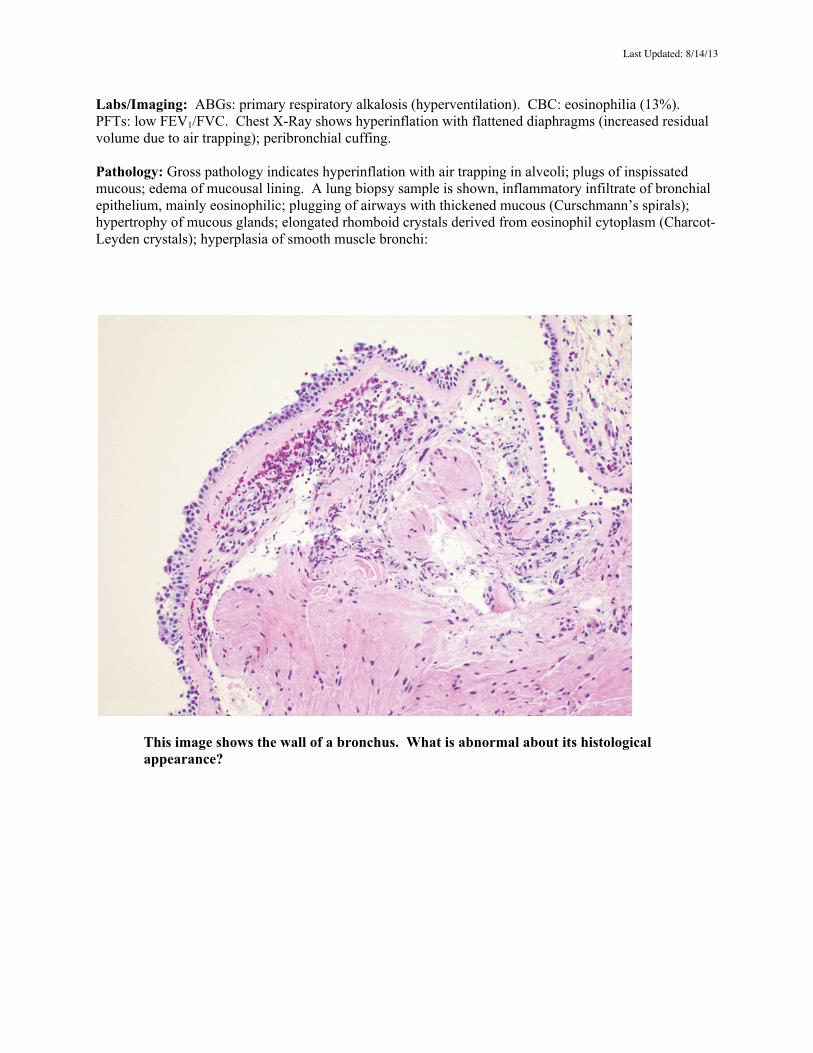
Labs/Imaging: ABGs: primary respiratory alkalosis (hyperventilation). CBC: eosinophilia (13%). PFTs: low FEV1/FVC. Chest X-Ray shows hyperinflation with flattened diaphragms (increased residual volume due to air trapping); peribronchial cuffing. Pathology: Gross pathology indicates hyperinflation with air trapping in alveoli; plugs of inspissated mucous; edema of mucousal lining. A lung biopsy sample is shown, inflammatory infiltrate of bronchial epithelium, mainly eosinophilic; plugging of airways with thickened mucous (Curschmann’s spirals); hypertrophy of mucous glands; elongated rhomboid crystals derived from eosinophil cytoplasm (Charcot-Leyden crystals); hyperplasia of smooth muscle bronchi:
This image shows the wall of a bronchus. What is abnormal about its histological appearance?
Last Updated: 8/14/13
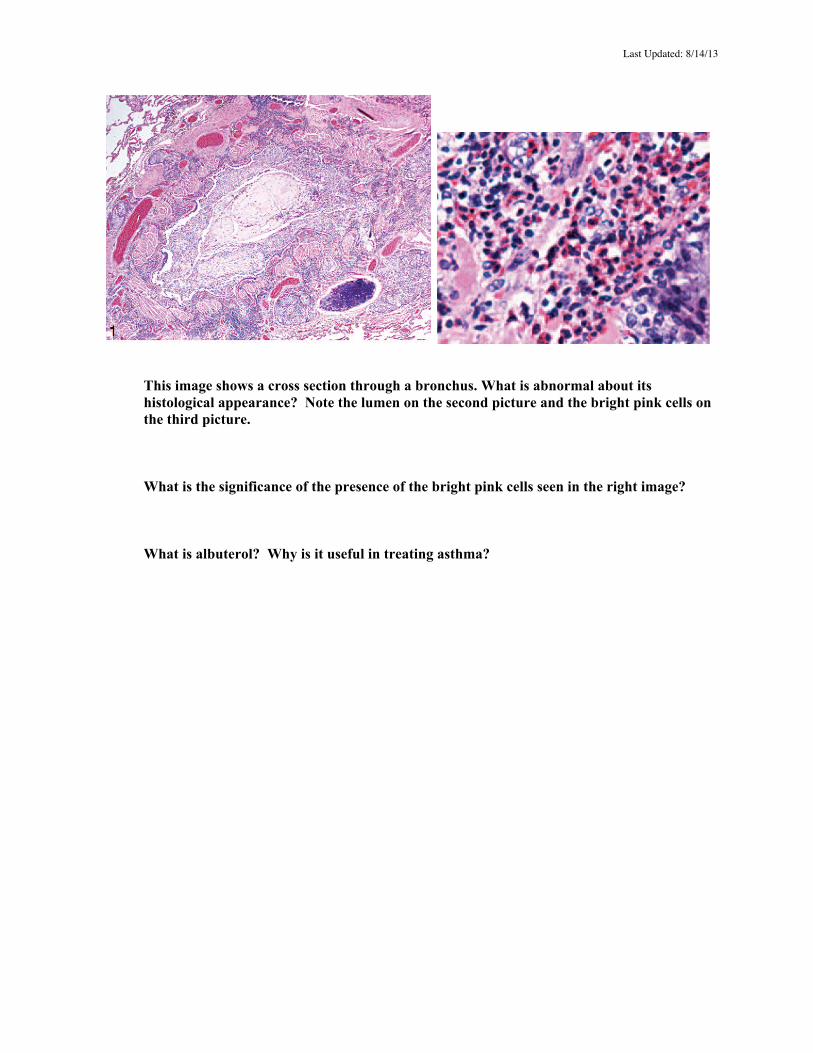
This image shows a cross section through a bronchus. What is abnormal about its histological appearance? Note the lumen on the second picture and the bright pink cells on the third picture.
What is the significance of the presence of the bright pink cells seen in the right image?
What is albuterol? Why is it useful in treating asthma?