joseph a. miller healthcare consultant september, 2002 the hospitalist movement in massachusetts the...
TRANSCRIPT

Joseph A. Miller
Healthcare Consultant
September, 2002
The Hospitalist MovementThe Hospitalist Movementin Massachusettsin Massachusetts
The Quiet RevolutionThe Quiet Revolution
In HealthcareIn Healthcare

Key Messages from the ReportKey Messages from the Report
Good news:Good news:• The Hospitalist movement has moved into The Hospitalist movement has moved into
the mainstream in Massachusettsthe mainstream in Massachusetts
Bad news:Bad news:• Hospitalist programs are about to receive Hospitalist programs are about to receive
more scrutinymore scrutiny

Definition of a HospitalistDefinition of a Hospitalist
• Term defined in 1996 Term defined in 1996 NEJMNEJM article by article by Wachter/Goldman from UCSFWachter/Goldman from UCSF
• Hospitalists are hospital-based physicians Hospitalists are hospital-based physicians that manage medical inpatientsthat manage medical inpatients
• An alternative to inpatient management by An alternative to inpatient management by an office-based PCPan office-based PCP

Why are there Hospitalists?Why are there Hospitalists?
Hospital motivations:Hospital motivations:• Vehicle for managing “unassigned” patientsVehicle for managing “unassigned” patients• Cost savings for DRG casesCost savings for DRG cases
PCP motivations:PCP motivations:• Managing fewer, sicker inpatientsManaging fewer, sicker inpatients• Stress of commuting to/from hospitalStress of commuting to/from hospital• More revenue in seeing patients in officeMore revenue in seeing patients in office

Hospitalist ResearchHospitalist Research
• Wachter/Goldman follow-up article in Wachter/Goldman follow-up article in January 2002 January 2002 JAMAJAMA reviewed 19 reviewed 19 published studies on hospitalist programspublished studies on hospitalist programs
• ““Empirical research supports the premise Empirical research supports the premise that hospitalists improve inpatient that hospitalists improve inpatient efficiency without harmful effects on efficiency without harmful effects on quality or patient satisfaction.”quality or patient satisfaction.”

Concerns re: HospitalistsConcerns re: Hospitalists
• Discontinuity of careDiscontinuity of care: the communications : the communications between PCP and hospitalistbetween PCP and hospitalist
• Patient dissatisfactionPatient dissatisfaction: a new MD is now : a new MD is now managing the casemanaging the case
• PCP dissatisfactionPCP dissatisfaction: loss of authority; turf : loss of authority; turf issues of PCP vs. hospitalistissues of PCP vs. hospitalist
• Provider communicationsProvider communications: hospital is no : hospital is no longer the meeting place for MDslonger the meeting place for MDs

The Hospitalist MovementThe Hospitalist Movementin Massachusettsin Massachusetts
The Quiet RevolutionThe Quiet Revolution
In HealthcareIn Healthcare

Joseph A. Miller CredentialsJoseph A. Miller Credentials
• 25+ years healthcare industry experience25+ years healthcare industry experience
• Focus: implementing/reporting on innovationFocus: implementing/reporting on innovation• Disease management, electronic medical recordsDisease management, electronic medical records• Outcomes analysis, case-mix adjustmentOutcomes analysis, case-mix adjustment• eHealth, managed care initiativeseHealth, managed care initiatives
• 5 years experience in survey research5 years experience in survey research• Partner at consulting firm responsible for researchPartner at consulting firm responsible for research• Products: reports, articles, seminars, conferences Products: reports, articles, seminars, conferences
Hospitalist ResearchHospitalist ResearchBackgroundBackground
• What was the motivation for this research?• Personal experience with a family member
• Who provided support to the research?• Winthrop Whitcomb, M.D., Mercy Medical Center• Joseph Li, M.D., Beth Israel Deaconess Med. Center
• What is the unique contribution of the research?• 1st analysis of the impact of hospitalist medicine on a
defined community

Target PopulationTarget Population
• 75 acute care hospitals in the state
• 27 academic hospitals (average: 342 beds)• 48 community hospitals (average: 148 beds)
• 18 “major” medical groups in the state
• 3 primary care groups (average: 18 MDs)• 15 multi-specialty groups (average: 94 MDs)

Survey MethodologySurvey Methodology
• For hospitals/medical groups without hospitalist programs
• 1-page fax back survey completed by Chief Medical Officer
• For hospitals/medical group with hospitalist programs
• 15-20 minute phone survey with Director of the Hospitalist Program

Response RateResponse Rate
• Hospitals without hospitalist programs
• 39 of 47 responded (83%)
• Hospitals with hospitalist programs• 26 of 28 responded (93%)
• Major medical groups• 16 of 18 responded (89%)

Data Analysis IssuesData Analysis Issues
• Not all hospitalist programs are hospital-based• There are medical group-based programs
• A hospitalist program can support >1 hospital• More likely to apply to medical group-based programs
• There are adult and pediatric hospitalist programs• A hospital or medical group can operate 2 hospitalist
programs

The Hospitalist MovementThe Hospitalist Movementin Massachusettsin Massachusetts
The Quiet RevolutionThe Quiet Revolution
In HealthcareIn Healthcare

Table of ContentsTable of Contents60-page report60-page report
• Executive SummaryExecutive Summary
• Ch 1Ch 1: The Emergence of the : The Emergence of the Hospitalist MovementHospitalist Movement
• Ch 2Ch 2: Research Methodology: Research Methodology
• Ch 3Ch 3: Overview of the : Overview of the Hospitalist Movement in MAHospitalist Movement in MA
• Ch 4Ch 4: Reasons for Starting : Reasons for Starting Hospitalist ProgramsHospitalist Programs
• Ch 5Ch 5: Characteristics of : Characteristics of HospitalistsHospitalists
• Ch 6Ch 6: Staffing of Hospitalist : Staffing of Hospitalist ProgramsPrograms
• Ch 7Ch 7: Types of Patients Seen by : Types of Patients Seen by HospitalistsHospitalists
• Ch 8Ch 8: Roles & Responsibilities of : Roles & Responsibilities of HospitalistsHospitalists
• Ch 9Ch 9: Hospitalist Communications : Hospitalist Communications with PCPs & Patientswith PCPs & Patients
• Ch 10Ch 10: Hospitalist Marketing to PCPs: Hospitalist Marketing to PCPs
• Ch 11Ch 11: Conclusions & Observations: Conclusions & Observations

Examples of detailed findingsExamples of detailed findings
• Characteristics of patients seen by hospitalists• 38% unassigned; 67% seniors
• Average patient load seen by hospitalists• Hospital-based programs: 10.5; Medical group programs: 17.0
• Profile of an average hospitalist• 37 year old general internist, slightly more likely to be male (60%) than
female (40%).
• Marketing efforts by hospital-based programs• 54% no direct marketing (“word of mouth”)
• 32% direct marketing (meetings, visits, mailings)
• 14% no marketing (have a waiting list of PCPs)

Examples of Mass. programsExamples of Mass. programs
• The largest hospitalist programs in Mass are at UMass Memorial Medical Center (20 MDs, 14 FTEs), the South Shore Hospitalists group practice (17 MDs, 13 FTEs), and Brigham & Women’s/ Faulkner (13 MDs, 10 FTEs).
• The increased inpatient load of summer tourists was the impetus for developing hospitalist programs at Martha’s Vineyard Hospital and Nantucket Cottage Hospital
• Adrienne Bennett M.D, Chief of the service at Newton-Wellesley Hospital has implemented a unique approach to round-the-clock coverage. Hospitalists are “on” 14 consecutive days and “off” for 7 days. When they are on, MDs are in the hospital 10-12 hours and available by pager for the remainder of the day.

Research ResultsResearch Results
5 major conclusions:5 major conclusions:
1. GROWTH: The number of hospitalist programs and hospitalists in Mass. has grown rapidly over the last 6 years
2. IMPACT: These programs have had a surprisingly significant impact on the delivery of inpatient care in the state
3. MORE GROWTH & IMPACT: The impact of hospitalist programs in Mass. will continue to grow rapidly over the next 5 years
4. SEGMENTATION: Hospitalist programs can be segmented into three categories each with distinct characteristics
5. MATURATION: The hospitalist movement in Mass. is in its early stages and will likely mature over the next 5-10 years
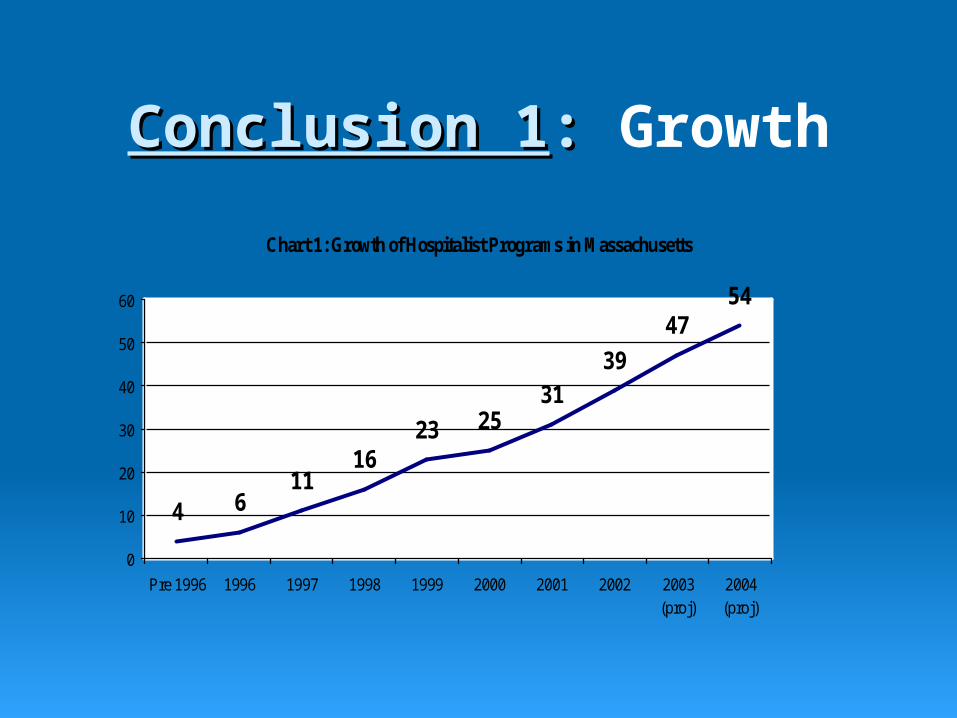
Conclusion 1Conclusion 1:: Growth
Chart 1: Growth of Hospitalist Programs in Massachusetts
4 611
1623 25
3139
4754
0
10
20
30
40
50
60
Pre 1996 1996 1997 1998 1999 2000 2001 2002 2003(proj)
2004(proj)

Conclusion 2Conclusion 2:: Impact
• Hospitalists coordinate care for an estimated 42% of the 1.8M medical inpatient days in Mass.
• It took managed care plans over 25 years to achieve a 40% penetration of the Mass. healthcare marketplace. • Hospitalist programs have achieved that result in 6
years.

Conclusion 3Conclusion 3:: More growth & impact
• Existing hospitalist programs in Mass. expect to grow in size by 12% in the next year (i.e., add 24 physicians).
• 15 Mass. hospitals (virtually all community hospitals) that currently do not have hospitalist programs have active plans to implement one in the next 12-18 months.
• 11 hospitals are interested in hospitalist programs, but have no active plans to implement one.
• By 2005 hospitalists will coordinate care for two-thirds of the medical inpatient days in Massachusetts.

Conclusion 4Conclusion 4:: Segmentation
• Academic hospital-based programs
• Community hospital-based programs
• Medical group-based programs

Academic hospital-based programsAcademic hospital-based programs
• Leading the hospitalist movement in Massachusetts• 52% have programs vs. 23% for community hospitals
• Teaching is an important priority for these programs
• These hospitals often care for very sick patients • Hospitalists’ role often requires significant coordination with a
range of sophisticated specialists
• Because of house staff/specialization: • Hospitalists rarely perform procedures• Hospitalists less likely to see patients in ICU, CCU, or ED

Community hospital-based programsCommunity hospital-based programs
• Represent the growth market for new hospitalist programs• Virtually all hospitals with active plans to implement hospitalist
programs in the next 2 years are in this category
• Hospitalists have multi-dimensional responsibilities • Admit some patients, admit and round on other patients, perform
consultations, do medical procedures, and see patients in the ICU, CCU, and ED
• More likely to provide 24 hour, round-the-clock coverage and to employ administrative and/or clinical support staff

Medical Group-based programsMedical Group-based programs
• Almost 90% of major Medical Groups have programs• Many programs support multiple hospitals
• Cost savings are a strong motivation for using hospitalists • Often at financial risk (e.g., capitation) for inpatient services
• Programs good at integrating care across multiple settings • PCPs and hospitalists are partners in the medical group • PCP can explain hospitalist role to the patient before admission• The hospitalist can easily and frequently communicate with the
PCP and other MDs in the group (e.g, using an EMR)
• Smooth patient transfers to ECFs and rehab facilities because
groups often have contractual relationships with these providers

Conclusion 5Conclusion 5:: Maturation

The Diffusion of InnovationThe Diffusion of Innovation
• Enthusiasts – explorers, willing to experiment with break-through ideas. Little fear of failure; not intimidated by the pains/hassles of being 1st.
• Visionaries – courageous exploiters, willing to take a chance. Visionaries seeking to gain the benefits of being an early adapter.
• Pragmatists – practical users who will adapt an innovation if there is convincing evidence that it works.
• Conservatives – the “wait and see” population of users. They want to be sure that the innovation delivers on its promises.
• Skeptics – the group that stubbornly resists the innovation. Skeptics not only avoid change, they actively oppose it.
• The “CHASM” – the difficult passage from adaption by visionaries to adaption by pragmatists – the movement of an innovation into the mainstream. Many innovations do not successfully cross the chasm

Conclusion 5Conclusion 5:: Maturation
• The hospitalist movement in Mass. is crossing the chasm
• As hospitalist programs move into the mainstream:
• Visibility will increase – “hospitalist” will become a household word.
• Hospitals, physicians, etc. will demand that hospitalist programs show value: i.e., that they are proven, predictable, measurable, integrated, and comprehensive.
• Scrutiny by industry experts and the general public will put a spotlight on hospitalist program strengths and weaknesses... PEOPLE WILL HAVE OPINIONS!
• Hospitalists will be more actively engaged in classic industry conflicts re: money and turf.

What I plan to doWhat I plan to do
Facilitate the movement of the Massachusetts hospitalist movement into the mainstream
• Raise awareness of the hospitalist movement among policymakers and the general public
• Identify, describe, and communicate best practices of hospitalist programs

For more information:For more information:
Joseph A. MillerJoseph A. MillerHealthcare ConsultantHealthcare Consultant
Website: http://hospitalist.thecog.orgWebsite: http://hospitalist.thecog.orgPhone: 781-768-2501Phone: 781-768-2501
Email: [email protected]: [email protected]