“it’s not just cough and cold”
TRANSCRIPT

“It’s Not Just Cough and Cold”
Milagros Salvani-Bautista, MD UERMMMC Class 1976
27th Annual Convention and Reunion Marriott Legacy Plano, Texas
DISCLOSURE
NOTHING TO DECLARE In the preparation of this lecture
RESEARCHER: BOEHRINGER INGELHEIM GSK SANOFI LECTURER: PFIZER JOHNSON & JOHNSON CATHAY DRUG

COUGH & COLDS
Common colds Acute self limiting viral infection Most frequent human illness

COUGH & COLDS
Association Pathogens Relative Frequuency Agents frequently associated with colds
Rhinoviruses Coronavirus
Frequent Occasional
Agents primarily associated with other clinical syndromes that also cause common cold symptoms
Respiratory syncythial viruses Human metapneumovirus Influenza viruses Parainfluenza viruses Adenoviruses Enterovirusers Bocavirus
Occasional Occasional Uncommon Uncommon Uncommon Uncommon Uncommon
PATHOGENS ASSOCIATED WITH COMMON COLD
Ronald B. Turner, Gregory F. Hayden Chapter 371 Nelson Textbook of Pediatrics 19th Edition

CONDITIONS THAT CAN MIMIC THE COMMON COLD
CONDITION DIFFERENTIATING FEATURES ALLERGIC RHINITIS Prominent itching and sneezing
Nasal Eosinophils FOREIGN BODY Unilateral, foul smelling secretions
Bloody nasal secretions SINUSITIS Presence of fever, headache or
facial pain or periorbital edema, or persistence of rhinorrhea or cough for >14 days
STREPTOCOCCOSIS Purulent nasal discharges that Excoriates the nares
PERTUSSIS Onset of persistent or severe cough
CONGENITAL SYPHILIS Persistent rhinorrhea with onset in the 1st 3 months of life
Ronald B. Turner, Gregory F. Hayden Chapter 371 Nelson Textbook of Pediatrics 19th Edition
MANAGEMENT SYMPTOMATIC ANTIVIRAL TREATMENT
RIBAVIRIN approved for RSV : NO ROLE in the management of Common Cold NEURAMINIDASE INHIBITORS: Oseltamivir & Zanamivir: modest effect on the duration of symptoms associated with influenza viral infection in children OSELTAMIVIR: reduces the frequency of influenza-associated otitis media LIMITATION: difficulty in distinguishing influenza infection from other common cold pathogens necessity to start therapy within 48 hours
Ronald B. Turner, Gregory F. Hayden Chapter 371 Neelson Textbook of Pediatrics 19th Edition
LUNG INTRINSIC DEFENCES AGAINST INVADING PATHOGENS
Aerodynamic filtering from the nose, turbinates, tonsils and adenoids and airway branching
• Humidification
• Airway reflexes : Sneezing, bronchoconstriction and coughing
Kendig’s Disorders of the Respiratory Tract in Children 8th ed.

Cough a reflex……
important defense mechanism protects the airways from aspiration of foreign materials enhances clearance of secretions and particulates from the airways…. Healthy children cough! A healthy child coughs 11 times/day Arch Dis Child1996;74:531

* Cough receptors include rapid acting receptors (RAR), slow acting receptors (SAR), C fibers, and other cough receptors. Some receptors are mechanosensitive and others are chemosensitive. Impulses from these receptors are all carried by the vagus nerve.

Cough is the most common symptoms that results in new medical consultations [1,2]
US: 29.5M doctor visit/year are for cough [3]
Burden of cough: Billions of dollars > OTC cough medications > Number of consults/child
Australian study: number of medical consults: > 80% of children had ≥ 5 doctor visits 53% had > 10 visits [4]

EPIDEMIOLOGY:
Estimated prevalence: > 5-7% among pre-schoolers > 12-15% in older children Stein RT, Holberg CJ,et al Influence of parental smoking on respiratory Symptoms during the first decade of life: the Tucson Children’s Respiratory Study. Am L Epidemiol 1999:149:1030 Chang AB, PowellCV. Nonspecific cough in children: diagnosis and treatment. Hosp Med 1998;59:68o
Cough: more common among boys than girls up to 11 years of age
Stein RT, Holberg CJ,et al Influence of parental smoking on respiratory Symptoms during the first decade of life: the Tucson Children’s Respiratory Study. Am L Epidemiol 1999:149:1030
May be less common in developing countries than in affluent countries
Faniran AO, Peat JK Woolcock AJ, Measuring persistent cough in epidemiological studies: development Of a questionnaire and assessment of prevalence in two countries.Chest1999;115;434
?

Cough and colds are the most common symptoms for which children are brought for consult
1.Office of Population Census and Surveys, Morbidity Statistics from General Practice: 4th National Study 1991-1992 Series MB5 no.3 London, Her Majesty’s Stationery Office, 1995 2.Schappert SM,Ambulatory care visits 0s physician offices, hospital outpatient departments, and emergency departments, US, 1995 Vital Health Stat 13 1997 3. Fendrick et al The economic Burden non infuluenza-related viral infection in the US.Arch Int Med 2003;163:487-494 4. Irwin RS, et al. Chronic cough the spectrum and frequency of causes, key components of the diagnostic evaluation,and Outcome of secific therapy. AmRev Respir Dis 1990;141:640-647
Acute cough – most prominent symptom and common cold, most frequent illness to afflict mankind.
Chronic cough as the sole presenting complaint accounts for 10-38% of all referrals to respiratory physicians

Manifestation of a serious pulmonary /extra pulmonary disease… Causes of chronic cough in children may be different from that of adults Chang AB, Glome WB , Chest 2006; 129:260S
COUGH:

DEFINITION: (guidelines)
CHRONIC COUGH: cough that lasts for more than 4 weeks
American College Chest Physicians Thoracic Society of Australia and New Zealand
cough that lasts for more than 8 weeks British Thoracic Society
“prolonged acute cough” cough that lasts for at least 3 weeks and “relentlessly progressive” …this type of cough – may warrant investigation before 8 weeks.
There is no consensus definition of the time frame for chronic cough in children
KEY SYMPTOMS & SIGNS: Certain symptoms and signs are highly predictive of a specific cough. These signs or symptoms narrow the diagnostic possibilities and call for further specific testing or referral.
Chronic wet cough Wheezing or crepitations (crackles)
Onset after an episode of choking, or sudden onset while eating or playing
Abnormal chest radiography or spirometry
Associated cardiac or neurologic abnormalities
Failure to thrive, feeding difficulties, or hemoptysis

ASSESSMENT: DETAILED HISTORY PHYSICAL EXMAMINATION
CHEST RADIOGRAPH
SPIROMETRY
BRONCHOSCOPY
OTHERS: Esophageal pH monitoring, sinus imaging
Tuberculin testing, allergy testing

ASSESSMENT:
Age and circumstances at the onset Neonatal onset: congenital malformation tracheomalacia Predisposition to aspiration:
TEF, laryngeal clef, neurologic disorder Chronic Pulmonary Infections: Cystic fibrosis Ciliary dyskinesia
Nature of the cough: Paroxysmal [with an inspiratory whoop] Barking/brassy cough Wet-moist cough Dry cough – throat clearing
(DETAILED HISTORY)
ASSESSMENT: Timing & Triggers Exposure to asthma triggers Swallowing Disappears with sleep
Associated symptoms Dyspnea Hemoptysis [bronchiectasis, cavitary lung lesions etc]
Past medical history Prenatal, neonatal course LBW and/or prematurity at risk of developing atopic sensitization and asthma [prematurity - BPD]
(DETAILED HISTORY)

Recurrent Coughing/ Wheezing Patterns in Childhood Based on Natural History [1]
Transient Early Wheezing
Common in early preschool years Recurrent cough/wheeze, primarily triggered by common respiratory infections Tends to resolve during the preschool years, without increased risk for asthma In later life Reduced airflow at birth, suggestive of relatively narrow airways, improves by school age
Taussig LM, Landau LI et al editors Pediatric Respiratory Medicine Ed 2 Philadelphia 2008 Mosby/Elsevier

Recurrent Coughing/ Wheezing Patterns in Childhood Based on Natural History [2]
Persistent atopy associated asthma
Begins in early preschool years Associated with atopy in early preschool years Clinical ( atopic dermatitis in infancy; AR and food allergy) Biologic (early inhalant allergen sensitization, increased IgE, increased Eo) Highest risk for persistence into later childhood and adulthood Lung function abnormalities: those with onset before 3 years of age acquire reduced airflow by school age those with later onset of symptoms or with later onset of allergen sensitization are less likely to experience airflow limitation
Taussig LM, Landau LI et al editors Pediatric Respiratory Medicine Ed 2 Philadelphia 2008 Mosby/Elsevier
Recurrent Coughing/ Wheezing Patterns in Childhood Based on Natural History [3]
Non Atopic Wheezing
Asthma with declining lung function Children with asthma with progressive increase in airflow limitation Associated with hyperinflation in childhood ,male gender
Wheezing and coughing beginning in early life often with RSV infections and resolves in later childhood and adulthood Associated with bronchial hyperresponsiveness near birth
Late-onset asthma in females, associated with obesity and early onset Puberty Onset between 8 and 13 years of age Associated with obesity and early onset puberty specifically for females
Taussig LM, Landau LI et al editors Pediatric Respiratory Medicine Ed 2 Philadelphia 2008 Mosby/Elsevier
Recurrent Coughing/ Wheezing Patterns in Childhood Based on Natural History [4]
Occupational type asthma in children Children with asthma associated with occupational-type exposure Known to trigger in adults in occupational settings i.e. endotoxin exposure in children raised on farms
Late-onset asthma in females, associated with obesity and early onset Puberty Onset between 8 and 13 years of age Associated with obesity and early onset puberty specifically for females
Taussig LM, Landau LI et al editors Pediatric Respiratory Medicine Ed 2 Philadelphia 2008 Mosby/Elsevier

ASSESSMENT:
Family history Allergy & atopy Asthma Primary ciliary dyskinesia Current illness in the family members and contacts weight loss, night sweats ? TB possibility of HIV transmission from momchild
(DETAILED HISTORY)
Social and environmental exposure history
Medications

SOCIAL & ENVIRONMENTAL HISTORY:
Passive smoking or active exposure to smoke from tobacco and other substance
Arch Dis Child 1997;76:22
Outdoor air pollution are triggers of chronic cough…
Euro Respir J 1999;14:669 Pediatric Pulmonol Suppl;1999;18:9 Peditrics 2004;113:1037

Social & Environmental History
Indoors pollution: damp moldy and poorly ventilated homes
Indoor pollution: Use of biomass fuel for cooking [wood and crop & sugarcane residues]..
Pediatric Infectious Dis J 1996;15:859
Arch Dis Child 1997;76:22

Gas stoves are also associated with chronic cough
Chest 2008;134:1122

PHYSICAL EXAMINATION
General examination — The physical examination should pay close attention to the following signs of chronic underlying disease:

PHYSICAL EXAMINATION
General appearance of chronic illness Poor growth, thinness, or obesity
Increased work of breathing, retractions, accessory muscle use, chest wall hyperinflation or deformity, abnormal breath sounds (reduced intensity, asymmetry, wheezing, stridor, crackles) Shiners, swollen nasal turbinates, nasal obstruction, nasal polyps, allergic nasal crease, halitosis, tonsillar hypertrophy, pharyngeal cobblestoning, high arched or cleft palate, hoarseness

PHYSICAL EXAMINATION Tympanic membrane scarring or frank otorrhea Abnormal heart sounds, abnormal pulses Edema of the extremities, cyanosis and/or clubbing of the digits
Hepato and/or splenomegaly, abdominal masses, bloating, rectal prolapse Rashes and other skin lesions (eg, scars of healed recurrent impetigo) Neurologic abnormalities

ASSESSMENT
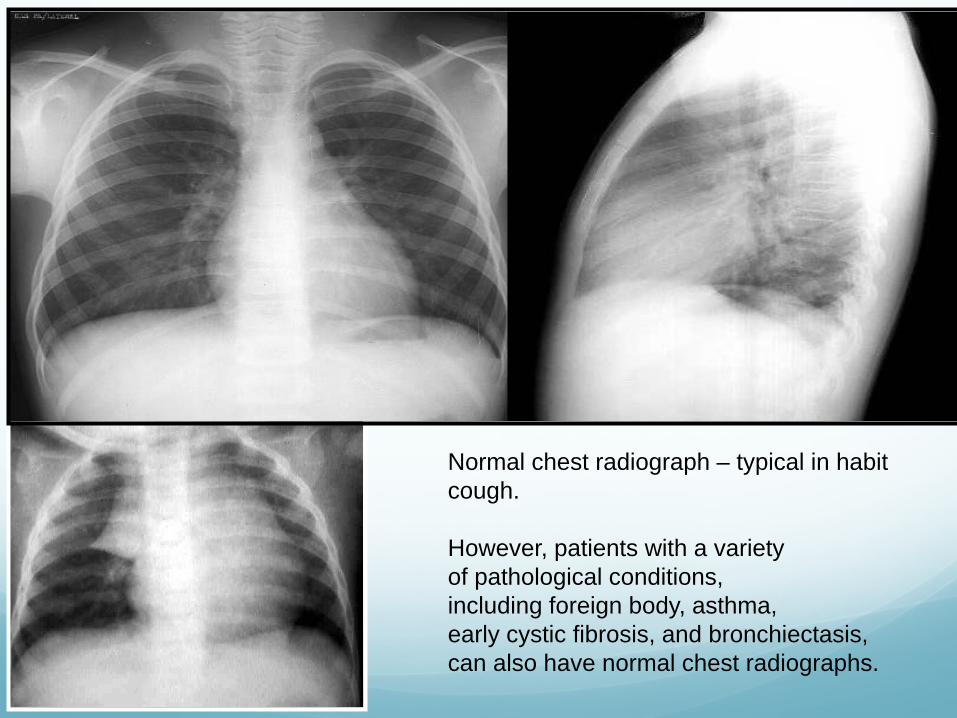
Normal chest radiograph – typical in habit cough. However, patients with a variety of pathological conditions, including foreign body, asthma, early cystic fibrosis, and bronchiectasis, can also have normal chest radiographs.

PNEUMONIA – RIGHT MIDDLE LOBE

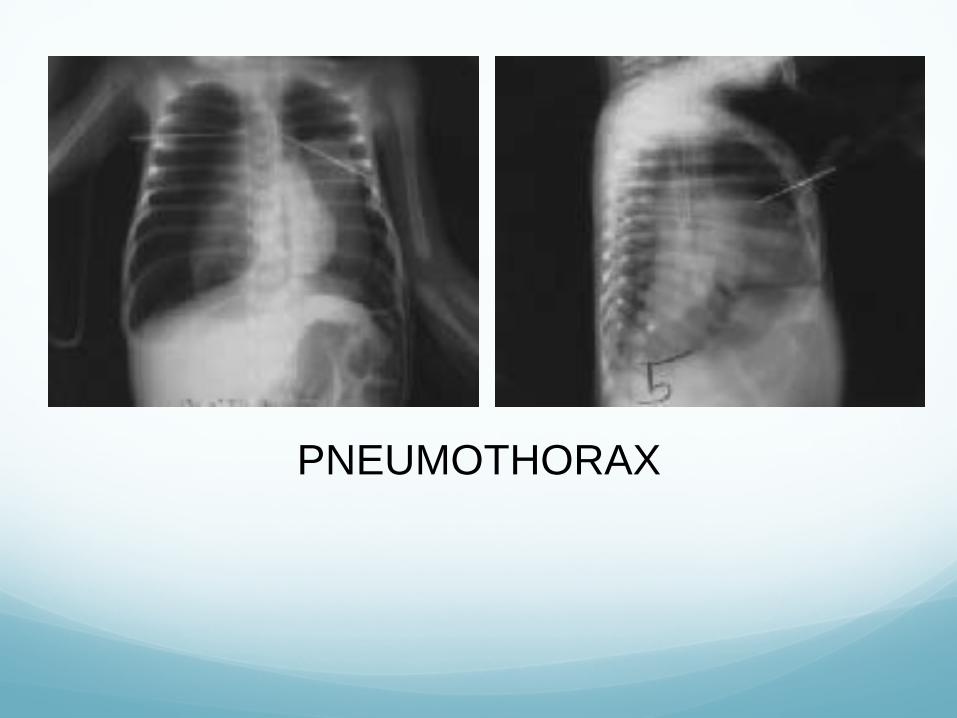
PNEUMOTHORAX
PULMONARY FUNCTION TEST

Tests for Diagnosis & Monitoring: • Spirometry - Measurement of the lung function
•FEV1 •FVC • FEV1/FVC ≥ 0.75-0.80 (≥0.90 in children)
• Reversibility with bronchodilator ≥ 12% Pellegrino R, Viegi G., Brusasco V., Crapo RO, Burgos F Casaburi R et al Eur Respir J 2005; 26 (5): 948-68
• Peak Expiratory Flow PEF measurements should be compared to the patient’s best measurements using his own peak flow meter
Redde HK, Salome CM, Peat JK, Woolcock AJ Am J Respir Crit Care Med 1995;151 (5):1320-5

PULMONARY FUNCTION TESTS SPIROMETRY


SUMMARY

Modified from: Shields MD, Bush A, Everard ML, et al. BTS guidelines: Recommendations for the assessment and management of cough in children. Thorax 2008; 63 Suppl 3:iii1.

1. Supportive interventions : hydration; ingestion of warm fluids; saline nose drops; sprays or irrigation 2. Not use OTC cough and cold medications in children with colds < 6 years of age (Grade 1A) 3. In the absence of secondary bacterial infection, it’s recommended not to use antibiotics 4. Symptomatic therapy may be warranted if symptoms bother the patient [ interfering with sleep, feeding etc.] 5. If cough with wheeze is present, one may give nebulized bronchodilator
Common colds and cough…..

There is no consensus definition of the time frame for chronic cough. Chronic cough can be a symptom of congenital anomalies, genetic disease, airway obstruction. Evaluation of a child with chronic cough should be thorough.

THANK YOU