itch without a rash compartmentalize - healthed · pregnancy, prurigo of pregnancy, pemphigoid...
TRANSCRIPT

02-Sep-16
1
Itch without a rash
Commercial in-confidence. Not for distribution.
Prof. Pete SmithAllergist, Clinical Medicine
Griffith UniversityDirector Allergy Medical Brisbane and Sydney
Objectives
• Why do we itch?
• How do we itch?
• Compartmentalize
• Acute and Chronic models
• What investigations should we do
• How should we manage it?
Disclosures
• Patent in molecular pain 2 commercial
products + 2 Pipeline
• GU have patent
pending related to TRPs
and ACh in hypersensitivity
conditions
• Recent Wool Industry Advisory Board NFP Aus
• I also have a
multimedia / graphic design / medical
illustration company
• I also have a cosmetic
company
• Director of Allergy Medical in Sydney and
Brisbane
Pruritis, Itch is largely an aberrant response to a threat
• We have not evolved to have allergies or itch, but we have preferential evolution because of our responses to threat.
• Scratch and itch.
Threat and evolution Scratch, itch and dermatitis
• Most morbidity is secondary to scratching
• Scratching is a reflex designed to:
• 1. make the individual aware of a threat to avoid the threat
• 2. make the individual aware of a threat to remove it
• Part of the the activation of innate threat receptors in
the skin with atopic dermatitis activate ancient threat responses (epidermal, leukocytic and neural)
02-Sep-16
2
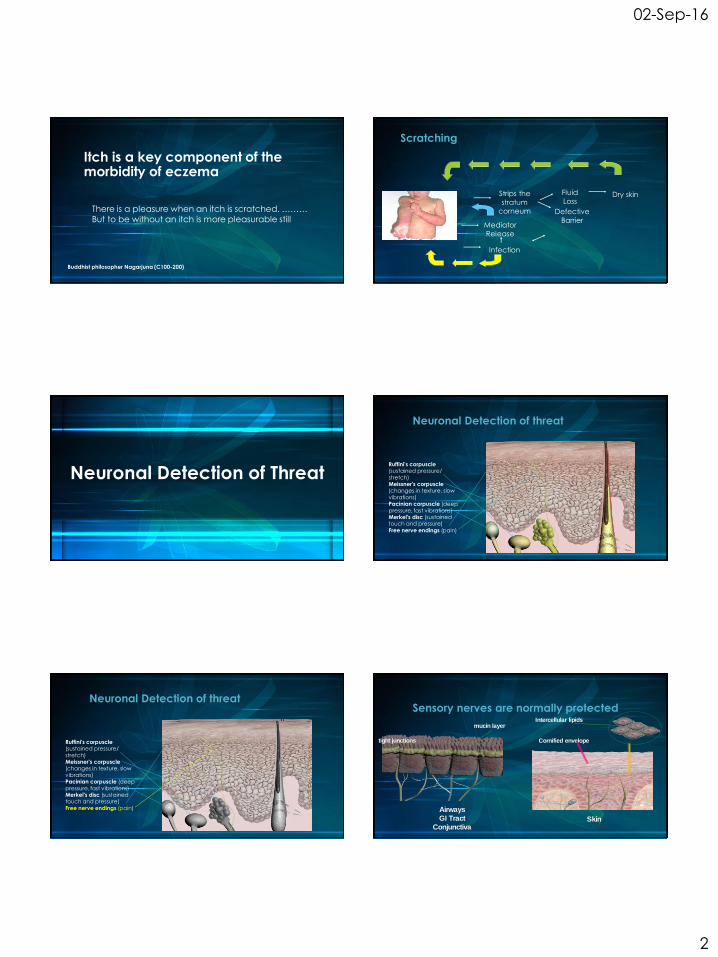
Itch is a key component of the morbidity of eczema
Buddhist philosopher Nagarjuna (C100-200)
There is a pleasure when an itch is scratched. ………
But to be without an itch is more pleasurable still
Scratching
Infection
MediatorRelease
Strips the
stratum
corneum
Fluid Loss
Dry skin
DefectiveBarrier
Neuronal Detection of Threat
Neuronal Detection of threat
Ruffini's corpuscle (sustained pressure/
stretch) Meissner's corpuscle (changes in texture, slow
vibrations) Pacinian corpuscle (deep
pressure, fast vibrations) Merkel's disc (sustained touch and pressure)
Free nerve endings (pain)
Neuronal Detection of threat
Ruffini's corpuscle (sustained pressure/
stretch) Meissner's corpuscle (changes in texture, slow
vibrations) Pacinian corpuscle (deep
pressure, fast vibrations) Merkel's disc (sustained touch and pressure)
Free nerve endings (pain)
Sensory nerves are normally protected
Skin
Airways
GI Tract
Conjunctiva
tight junctions
mucin layerIntercellular lipids
Cornified envelope

02-Sep-16
3
Antidromic Neuropeptide Release
Substance P
CGRP
NO, Bradykinin
VasoactiveIntestinal
Peptide
Edema
* PrimedMast Cell
Nicholas K. Mollanazar, Peter K. Smith & Gil Yosipovitch. Mediators of Chronic Pruritus in Atopic Dermatitis: Getting the Itch Out? Clinic Rev Allerg Immunol MAY 1 2015
Nicholas K. Mollanazar, Peter K. Smith & Gil Yosipovitch. Mediators of Chronic Pruritus in Atopic Dermatitis: Getting the Itch Out? Clinic Rev Allerg Immunol MAY 1 2015
Causes of Itch?
Etiologic classification of itch according to the
International Forum for the Study of Itch
Dermatological Systemic Neurogenic
PsychogenicMixedUnknown
Ständer S, Weisshaar E, Mettang T, et al. Clinical classification of itch: a position paper of the International Forum for the Study of Itch. Acta Derm Venereol 2007; 87: 291–4
Dermatologic: arising from skin; dry skin and any
specific skin disease
Inflammatory: contact dermatitis, atopic dermatitis, asteatotic eczema,
nummular eczema, stasis dermatitis, seborrheic dermatitis, urticaria, psoriasis,
lichen planus, drug reactions, polymorphous light eruption, mastocytosis,
pemphigoid, dermatitis herpetiformis, dermatomyositis
Infections: pediculosis, scabies, parasitic disease, tinea corporis, impetigo,
smallpox
Neoplastic: cutaneous T cell lymphomas
Dermatoses of pregnancy: pruritic urticarial papules and plaques of
pregnancy, prurigo of pregnancy, pemphigoid gestationis
Ständer S, Weisshaar E, Mettang T, et al. Clinical classification of itch: a position paper of the International Forum for the Study of Itch. Acta Derm Venereol 2007; 87: 291–4

02-Sep-16
4
Systemic: arising from diseases of organs other than
the skin, metabolic or other multifactorial disturbances or from drugs
Endocrine and metabolic disorders: chronic renal failure (dialysis), liver
diseases
with or without cholestasis, thyroid diseases
Infections: HIV, parasites, hepatitis C virus
Hematologic diseases: polycythemia vera, lymphomas
Tumors: solid organ tumors, carcinoid
Drug induced pruritus (with or without cholestasis
Ständer S, Weisshaar E, Mettang T, et al. Clinical classification of itch: a position paper of the International Forum for the Study of Itch. Acta Derm Venereol 2007; 87: 291–4
Neurologic (neurogenic/neuropathic): arising from
disorders of the central or peripheral nervous system and possibly also from liver disease
Multiple sclerosis; spinal or cerebral neoplasms, abscesses, or infarcts;
phantom itch; postherpetic neuralgia; transverse myelitis; notalgia
paresthetica; brachioradial pruritus; meralgia paresthetica; other conditions
associated with nerve damage, compression or irritation, such as
entrapment neuropathy, radiculopathy, or polyneuropathy (including
diabetes mellitus, vitamin B12 deficiency, etc.)
Ständer S, Weisshaar E, Mettang T, et al. Clinical classification of itch: a position paper of the International Forum for the Study of Itch. Acta Derm Venereol 2007; 87: 291–4
Psychogenic/psychosomatic
Delusion of parasitosis, psychogenic excoriations, somatoform pruritus, associated with psychiatric disorders
Mixed
Coexistence of dermatologic and neurologic itch in HIV infected patients or in patients with atopic dermatitis, association of uremic itch with skin xerosis, association of Hodgkin disease with potentially misleading paraneoplastic
cutaneous manifestations, such as unexplained adult onset eczema
Idiopathic
Senile 'idiopathic' pruritus, aquagenic 'idiopathic' pruritus, pruritus in anorexianervosa
Ständer S, Weisshaar E, Mettang T, et al. Clinical classification of itch: a position paper of the International Forum for the Study of Itch. Acta Derm Venereol 2007; 87: 291–4
Etiologic classification of itch according to the
International Forum for the Study of Itch
Dermatological Systemic Neurogenic
PsychogenicMixedUnknown
Ständer S, Weisshaar E, Mettang T, et al. Clinical classification of itch: a position paper of the International Forum for the Study of Itch. Acta Derm Venereol 2007; 87: 291–4
How do we develop itch / dermatitis?
• IgE & Non IgE
• Inflammatory
• Infection
• Acids, Hormones
Allergy /
InflammationIrritant
Hormonal• Proteolysis
• Disruption of outer lamellar layer increased TEWL
• ALARMINS
• Keratinocyte injury alarmins, ACh, TSLP, IL-33, IL-25
EpithelialIntegrity/Damage
Neurogenic
• ACUTE
• Neural-receptor activation
• Neuro-mediator release
• CHRONIC
• Upregulation
Compartmental Amplification
Immunological
Lymphocyte
Eosinophil
Dendritic
CellMast Cell
IgE
AMPLIFICATION
NeurogenicEpithelial
Substance
P
CGR
P
NO, Bradykinin
Vasoactive
Intestinal
Peptide
Edema
* Primed
Mast Cell

02-Sep-16
5
Histamine works via TRPV1
Histamine and Itch: sensory C fibres
TRPV1H1
Histamine
Phospholipase C
&
12 Lipoxygenase
Phosphorylation
ITCH
Inward fluxof Ca++
TRPV1antagonist
No inward flux of Ca++
No ITCH
capsazepine
Shim WS, et al. TRPV1 mediates histamine-induced itching via the activation of phospholipase A2 and 12-lipoxygenase. J Neurosci 2007, 27:2331-2337.
TRPV1H1
Histamine
Phospholipase C
&
12 Lipoxygenase
Phosphorylation
Histamine and Itch: sensory C fibres
TRPV1H1
Histamine
Phospholipase C
&
12 Lipoxygenase
Phosphorylation
ITCH
Inward fluxof Ca++
No ITCH
No inward flux of Ca++
Shim WS, et al. TRPV1 mediates histamine-induced itching via the activation of phospholipase A2 and 12-lipoxygenase. J Neurosci 2007, 27:2331-2337.
H1
Histamine
Phospholipase C
&
12 Lipoxygenase
Phosphorylation
TRPV1 KO
TRPV1 (capsaicin receptor)
• Preferential Calcium Channel
• (5-10x > Na+)
ION CHANNEL
• SP
• CGRP
• High Affinity NGF TrkA
• TNFa
• DRG
• Trigeminal Nerve
• Nerve Ganglia
• Epithelium
• Endothelium
• Glandular structures
TRIGEMINALASSOCIATE
DEXPRESSION
EXPRESSED
Caterina, MJ et al. The capsaicin receptor: a heat-activated ion channel in the pain pathway. Nature 1997 389, 816–824Seki N, et al. Expression and localization of TRPV1 in human nasal mucosa. Rhinology 2006 44: 128–134, 2006
• Polymodalsensory molecule
• Preferential calcium channel
• Hot, burning noxious stimuli
• Cumulative stimuli effect
TRPV1
Carlos Belmonte* and Félix Viana. Molecular and cellular limits to somatosensory specificity. Molecular Pain 2008, 4:14
Voltage (mV)50 100 150-50-100
5
10
control 25oC
heat 44oC
pH 6
capsaicin
Cu
rre
nt
(nA
)
HEK239 transfected with TRPV1:Whole cell ion channel – voltage relationship
Temperature / Acid / Capsaicin 100nM
PKA
CaM
CaM
Allicin
ATP
CaMKII
T370
Capsaicin
PKC
RTXK160, L 163
C157
K155T144
S116
R114
S502Y511 M547
E761
S512
E600
T550
S800
T704
E636
D645
E648
C66
C621
C634
N604
N
C
H+ Mg2+
TRPV1
Heat
>42.6oC
Pete Smith
AWI Adv isory Board
12 Dec 2015

02-Sep-16
6
Histamine works via TRPV1
Smith PK and Nilius B. Transient Receptor Potentials (TRPs) and Anaphylaxis. Curr Allergy Asthma Rep. 2013 Feb;13:93-100.
Histamine works via TRPV1
Smith PK and Nilius B. Transient Receptor Potentials (TRPs) and Anaphylaxis. Curr Allergy Asthma Rep. 2013 Feb;13:93-100.
Orthodromic and Antidromicneural signaling
Orthodromic and Antidromic signals
Orthodromic
Antidromic
Antidromic Neuropeptide Release
Substance P
CGRP
NO, Bradykinin
VasoactiveIntestinal
Peptide
Edema
* PrimedMast Cell
Protease / Anti-Protease Balancein the epidermis

02-Sep-16
7
Proteases and Itch
Cork M. J of Investigative Dermatology (2009).doi:10.1038/jid.2009.133
• Environment meets genes
• Proteases (or lack or anti-proteases) increased TEWL
• pH of skin increases and increases proteolyticenzyme activity increases TEWL
Protease-Anti-protease balance
exogenousproteases
block
block
endogenous proteins
Smith PK, Harper J. Serpins: their inhibitors and Allergy. Allergy. 2006 Dec ;61 (12):1441-7.
infection allergens
imbalance
trans-epidermal water loss
Anti-proteases
What investigations should we do?
How do we develop itch / dermatitis?
• IgE & Non IgE
• Inflammatory
• Infection
• Acids, Hormones
Allergy /
InflammationIrritant
Hormonal• Proteolysis
• Disruption of outer lamellar layer increased TEWL
• ALARMINS
• Keratinocyte injury alarmins, ACh, TSLP, IL-33, IL-25
EpithelialIntegrity/Damage
Neurogenic
• ACUTE
• Neural-receptor activation
• Neuro-mediator release
• CHRONIC
• Upregulation
How do we develop itch / dermatitis?
• IgE, specific RASTs
• Patch testing
• Pregnancy, TSH, T4
• Renal and LFTs
• FBE, ESR, CRP
Allergy /
InflammationIrritant
Hormonal
EpithelialIntegrity/Damage
Neurogenic
Medications that can cause itch without a rash
Ständer S, Weisshaar E, Mettang T, et al. Clinical classification of itch: a position paper of the International Forum for the Study of Itch. Acta Derm Venereol 2007; 87: 291–4
Antihypertensives ACE2Ra (sartans), b-adrenoreceptor antagonists, Ca channel blockers, Methyldopa, Sidenafil,
Antiarrhythmic drugs Amiodarone
Anticoagulants Ticlopidine, Fractionated heparins
Anti-diabetic drugs Biguanides, Sulphonylurea derivates
Hypolipidemic drugs HMG-CoA reductase inhibitors (statins)
Antibiotics Penicillins, Cephalosporins, Macrolides, Cabapenems, Monobactams, Quinones, Tetracyclines, Metranidazole, Rifampicin, Trimethoprim/Sulphamethoxazole,
Antimalarials
Psychotropic drugs Tricyclic antidepressants, SSRA, Antipsychotics
Anticonvulsants Carbamazepine, Phenytoins, Toprimates
Cytostatics Tamoxifen, Chlorambucil, Paclitaxel,

02-Sep-16
8
Medications that can cause itch without a rash
Ständer S, Weisshaar E, Mettang T, et al. Clinical classification of itch: a position paper of the International Forum for the Study of Itch. Acta Derm Venereol 2007; 87: 291–4
Growth Factors and Monoclonal Antibodies
GM-CSF, IL-2, Mauzumab, Lapatinib, Epidermal growth factor receptor
Plasma Expanders Hydroxyethyl starch
Others Antithyroid agents
NSAIDs
Corticosteroids
Sex Hormones
Opioids
Okay !!So how can we treat itch?
How do we treat itch / dermatitis?
Allergy /
Inflammation
EpithelialIntegrity/Damage
Neurogenic
Reduce Allergen Exposure / Irritation / Damage / Nerve Stimulation + Barrier
Corticosteroids (immune suppressants), Phototherapy
Antihistamines
LRTAMonoclonal Abs
Vitamin D
Treat infections
Ion Channel
Peripheral NerveCentral Pain
Cyclosporin, Antidepressants, Oral Retinoids, Pimecrolimus, Thalidomide
normal eczema
Straum cornuem
Lamellar envelope
subdermis
Atopic Dermatitis– a disrupted barrier
The Golden Ratio
Cholesterol, ceramides and essential / nonessential free fatty
acids (FFAs) in an equimolar ratio allows normal barrier
recovery whereas any 3:1:1:1 ratio of these four ingredients
accelerates barrier recovery
Zetterstin EM, et al. J. Am AcadDermatol 1997 Sept 47 (3 part 1) 403-8
The Barrier Function
Barrier
Sun Chemicals Infective Agents
Water
(and proteins)
Pete Smith
AWI Adv isory Board
12 Dec 2015

02-Sep-16
9
Natural Moisturizing
Factor
In the upper epidermis, water is found predominantly in a bound
form
urea, lactic acid, pyrrolidine carboxylic acid etc.
Filaggrin, intermediate filament and keratin
Water Balance
Pete Smith
AWI Adv isory Board
12 Dec 2015
If not improving within 2 weeks of skin care and treatment -
consider biopsy
Objectives
• Why do we itch?
• How do we itch?
• Compartmentalize
• Acute and Chronic models
• What investigations should we do
• How should we manage it?