is over: why building a collaborative the to and - acdis · the honeymoon is over: why building a...
TRANSCRIPT

©2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
1
The Honeymoon Is Over: Why Building a Collaborative Marriage Is the Key to Coding and CDI Success
Diana Ortiz, JD, RN, CDIPDirector of Clinical Documentation Excellence
Kaycie Wood, MSHCM, RHIA, CCSDirector of HIM System Coding
Ochsner Health System, New Orleans, LA
2
Learning Objectives
• At the completion of this educational activity, the learner will be able to:
– Develop a coding and CDI pre‐bill complication review process
– Implement a query escalation process
– Identify post ICD‐10 implementation coding/CDI collaborations
– Review a coding/CDI reconciliation process to eliminate rebills
– Implement a coding/CDI combined education process
3
Ochsner Health System
The Ochsner Clinic Foundation was founded in 1942 by five visionary physicians. Over the years, Ochsner continued to set milestones in healthcare history.
Fast forward to 2005, where under the leadership of CEO Dr. Patrick Quinlan and President and COO Warner Thomas, Ochsner and its more than 7,000 employees and physicians stood firm against a storm that would change the city forever.

©2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
4
• After 11 years of growth and progress, Ochsner Health System today is Louisiana's largest nonprofit, academic healthcare system. Under the leadership of president and CEO Warner Thomas, Ochsner’s team of 17,000 employees and 1,000 employed physicians coordinate and provide care across 25 owned, managed and affiliated hospitals and more than 50 health centers to care for patients from more than 90 countries worldwide.
Ochsner Health System
5
CDI Program Overview
• The CDI program began in 2004 under the direction of a registered nurse director of clinical documentation improvement within the case management department and transitioned to HIM in 2006 to address financial opportunity related to DRG assignment.
• The program has always been centralized at the system level, starting at the Jefferson Highway location and expanding to have a presence at each facility.
• The management and staffing structure has evolved over the years in an attempt to address the expansion on the department. Current structure includes 1 director & 3 managers.
• Today, the department is comprised of 32 employees including:
– Concurrent reviewers (remote & in‐house)– Lead reviewers – Retrospective reviewers– IS project manager– Administrative support
6
Coding Program
• The coding department is responsible for providing inpatient and outpatient hospital coding services for the Ochsner hospitals.
• The team consists of the coders, educators, internal consultants, project managers, and management staff.
Inpatient coding
Outpatient surgeries & procedures coding
Emergency dept technical
coding
Recurring outpatient coding
Outpatient diagnostic coding
ICD‐10‐CM diagnosis coding
ICD‐10‐PCS procedure coding
CPT procedure coding
MS‐DRG assignment
APR‐DRG assignment
APC assignment

©2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
7
1.Navigate to the event Agenda in the main menu
2. Tap the name of the current session to view the session details page
3. Tap Polls
4. Tap the name of the poll
5. Tap your answerchoice and then tap Submit
Steps for Attendees to View/Answer POLLING QUESTIONS
8
• Does your facility have a concurrent complication review process?
– Yes
– No
– I don’t know
Polling Question 1
9
Develop a Coding and CDI Pre‐Bill Complication Review Process
Overview
• Describe the Ochsner process and related roles/responsibilities, including coding, CDI, quality/PI, VPMA
• Define complications included for review: AHRQ PSIs, HACs, PPCs
• Concurrent or final coding triggers complication reviews
• Reviewed by PI/quality representative
• Escalated to VPMA for further review and clinical insight
• CDI/coding: Query as necessary for clarification

©2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
10
Define Complications Included for Review: AHRQ PSIs, HACs, PPCs
PSI 90 inclusion Key terms/concepts/potential query opportunities
PSI 03 Pressure Ulcer POA status of pressure ulcer, hemiplegia, late effect hemiplegia, cauda equina
PSI 06 Iatrogenic Pneumothorax Clinical significance of pneumothorax, rib fracture, pleural effusion
PSI 07 Central Venous Catheter-Related Blood Stream Infection
Confirm the source of the bloodstream infection
PSI 08 Postoperative Hip Fracture Secondary diagnosis of malignancy, musculoskeletal disorders
PSI 09 Perioperative Hemorrhage or Hematoma
Coagulation disorders (inc. thrombocytopenia) and etiology
PSI 10 Postoperative Physiologic Metabolic Derangement
Admission type: Acute blood loss anemia; underlying chronic renal failure; shock
PSI 11 Postoperative Respiratory Failure Admission type: Clinical illness myopathy; acute delirium; Alzheimer’s disease or dementia
PSI 12 Perioperative Pulmonary Embolism or Deep Vein Thrombosis
Clinical significance of DVT/PE (vs. incidental finding), POA status (especially regarding transfers)
PSI 13 Postoperative Sepsis Admission type; other infection POA status
PSI 14 Postoperative Wound Dehiscence Immunocompromised state
PSI 15 Accidental Puncture or Laceration Clear documentation of whether it is inherent or a complication of the procedure
11
Coder identifies complication (dx code or PSI)
If not OK, escalate to VPMA
VPMA and coding discuss
Weekly status report
VPMA review
PI coordinators review record
Weekly status report
Status review with team
Process measure review:•PI coordinator queue volume•Lag in billing•Time spent by PI in managing queue•Correction rate by service line/MD
Complication validation with coding
leader
Billed as complication
Re‐coded without
complication
If OK, billed as complication
Pre‐Bill Workflow
12
• What is your VPMA review turnaround time?
– 0–24 hours
– 24.1–48 hours
– 48.1+ hours
Polling Question 2

©2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
13
• Continuous management of bill hold for review of concurrent/retro quality indicators
• Overall metrics related to the comparison of concurrently reviewed accounts with final coded submissions for quality reporting
• Tracking spreadsheet with turnaround times
Physician Advisor Role
14
Sample Spreadsheet Image
15
• Has your facility adopted a formal query escalation policy and process?
– Yes
– No
– I don’t know
Polling Question 3

©2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
16
Implement a Query Escalation Process
• Appropriate querying will improve the accuracy, integrity, and quality of patient data; minimize variation in the query process; and improve the quality of provider documentation within the body of the medical record
• Departmental control processes are implemented to minimize potential compliance risks
• Queries will follow guidelines set forth by regulatory agencies, including but not limited to TJC, CMS, AHIMA, ACDIS
17
Implement a Query Escalation Process –Roles and Responsibilities
• Coding – Evaluates if there is an open query at discharge; places account
on hold and marks for escalation
– Continues to monitor account and does not final code until escalation process is complete
• CDI – Concurrently – monitors open queries and designates for
escalation as needed based on response or lack of response
– Retrospectively – monitors accounts on hold for progress of escalation
• VPMA – For concurrent and retrospective accounts – works with queries
provider to answer query, document efforts and resolution
18
Coder
VPMA
CDS nurse
CDI leadershipConcurrent query escalation process
CDS nurse monitors account and updates escalation message and closes out when complete
Codermonitors account on hold for escalation progress
Answered Unanswered
Attempt 1Original query
Attempt 21 day after original
query sent
Attempt 32 days after original
query sent
Escalate to CDI leadership
CDS nurse to send notification
CDS nurse to close query
Answered(required physician peer review)
CDI leadership reviews and escalates account to VPMA
VPMA reviews account until answered and documents efforts and resolution
Query Escalation Process – Concurrent

©2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
19
Query Escalation Process – Retrospective
(Query issued retrospectively)
escalation process
CDS nurse monitors the discharged and pending worklist and updates
response to close it out
Coder reviews bill hold and does not final code until escalation process is
complete
Answered
Query answered & resolved
CDI leadership to close/withdraw, change account activityCDI leadership to resolve notification and change recipient to CDS
CDS nurse to close query CDI leadership reviews and escalates account to VPMA via WQ
Answered(needs peer review)
CDS nurse reviews discharge with no review worklist accounts
CDS nurse issues query
Coding manager will review query and withdraw/delete query if unnecessary
Coder issues query
Coder/ coding manager or CDS nurse place account on CDI bill hold
Escalate to CDI leadership
CDS nurse to send notification and select on site leader for recipient
CDI leadership reviews and escalates account to VPMA via WQ
Query answered or peer resolution resolved
1. CDI leader to change account status2. CDI leader to resolve escalation message and notify CDS
3. CDS nurse to close query
Coder will add flag/activity to place on coding manager review WQ
VPMA reviews account until answered and adds resolve flag when done, adds account notes as needed to document efforts and resolution
CDS nurse to change account activity
Unanswered (3 attempts) or CDI leadership discretion
Coder manager
VPMA
CDS nurse
CDI leadership
Coder
20
Query Escalation Process Metrics
• Final analysis: Metrics related to this post go live, since Ochsner established formal process before ICD‐10 implementation
21
• Did your hospital/health system utilize individual CDI staff for provider education prior to ICD‐10 go live?
– Yes
– No
– I don’t know
Polling Question 4

©2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
22
Identify Pre/Post ICD‐10 Implementation Coding/CDI Collaborations
• Weekly coding round table – procedure discussion.
• Shared OLN (Online Learning Network) modules.
• Physician newsletter articles.
• CDI – rounding & at‐the‐elbow support – CDS rounding at nursing units, real‐time follow‐up, educating staff. Dual coding: Emphasize coder/CDI recognition of documentation gaps to remediate and educate providers through a real time process.
23
Weekly Coding Roundtable
24
E‐Learning Shared Modules

©2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
25
Provider Newsletter Sample
26
Provider Education Training
27
Provider Education Calendar

©2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
28
Provider Education Outline
29
• Does your hospital/health system have a 2‐step coding and CDI reconciliation process?
– Yes
– No
– I don’t know
Polling Question 5
30
Review a Coding/CDI Reconciliation Process to Eliminate Rebills
• Describe roles:
1. Coder – reconciliation, add comments
2. CDI – reconciliation, validate query impact

©2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
31
Review a Coding/CDI Reconciliation Process to Eliminate Rebills
• Coder reconciliation process includes coding and performing a DRG review with CDI last working DRG.
• CDI reconciliation process begins when final coding is complete. Identification of the reason for a DRG discrepancy between coding and CDI. Second‐level review includes the referral of any accounts where the discrepancy for a MS‐DRG or APR‐DRG mismatch cannot be reconciled.
32
Scope of potential rebills
Coder reconciliation includes coding in ICD‐10 and performing DRG comparison with CDS last
working DRG
CDI reconciliation process includes identification of the reason for a DRG discrepancy between coding and CDI. Mortality reviews are referred for any
diagnosis mismatch.
If CDI believes the account is a potential rebill, a notification should be created
Coding and CDI leadership review the accounts throughout the day at the “huddle” to
determine if rebill is necessary
Identify account from focus dashboard as a potential rebill
Escalation process: After receiving the notification email, if the CDS still has questions related to the final
DRG, they can refer to a CDI manager
Identify notification purpose:Potential rebill complete: Account was reviewed and NOT sent for a rebill. (use template Notification)
Potential rebill complete CDI education: Account was received and NOT sent for a rebill and CDI education is required. (use template Notification)
Account rebilled: Account was reviewed and SENT for a rebill. (If the DRG changed as a result of the CDI potential rebill process, open query and complete associated impact, financial versus non‐financial, and send manager account validation notification if necessary.)
Prebill resolution: Account was reviewed and SENT for a rebill. (template Notification account rebill if CDS needs to send manager account validation, template Notification SLR to Complete Manager Account Validation)
Continue to update the remaining fields on the notification:Recipient: Enter the name of the senderOther recipient: Leave blank/coder can receive notificationStatus: Change to Closed (this will complete the account from the worklist)Communication type: Change to EmailTemplate: May or may not change (Notification; Notification ‐ Account Rebilled; Notification SLR Manager Account Validation) Comments: Date and detail
Review a Coding/CDI Reconciliation Process to Eliminate Rebills
33
Review a Coding/CDI Reconciliation Process to Eliminate Rebills

©2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
34
Review a Coding/CDI Reconciliation Process to Eliminate Rebills
• Potential rebill form from Sharepoint screenshot
35
Review a Coding/CDI Reconciliation Process to Eliminate Rebills
• Rebill example
36
Review a Coding/CDI Reconciliation Process to Eliminate Rebills
• Not rebilled example

©2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
37
Future State – Coding & CDI Joint Education
38
• Do you have combined coding & CDI education efforts?
– Yes
– No
– I don’t know
Polling Question 6
39
Implement a Coding/CDI Combined Education Process
• Describe the overall Ochsner education process for regular coding and CDI education.
• Describe roles for education preparation and delivery: Coding leadership, CDI leadership, and internal consultant(s), rev cycle training analyst.
• Metrics: Online learning module completion and quiz scores. Staff engagement scores year over year.
©2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
40
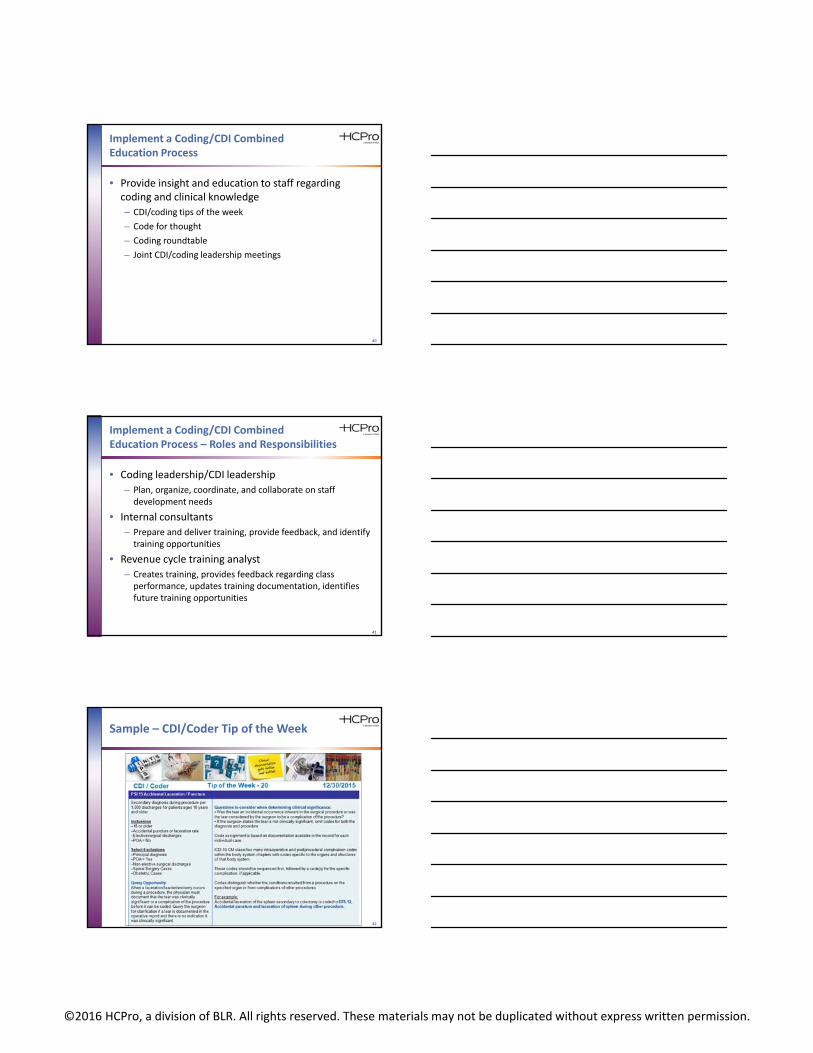
Implement a Coding/CDI Combined Education Process
• Provide insight and education to staff regarding coding and clinical knowledge
– CDI/coding tips of the week
– Code for thought
– Coding roundtable
– Joint CDI/coding leadership meetings
41
Implement a Coding/CDI Combined Education Process – Roles and Responsibilities
• Coding leadership/CDI leadership
– Plan, organize, coordinate, and collaborate on staff development needs
• Internal consultants
– Prepare and deliver training, provide feedback, and identify training opportunities
• Revenue cycle training analyst
– Creates training, provides feedback regarding class performance, updates training documentation, identifies future training opportunities
42
Sample – CDI/Coder Tip of the Week

©2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
43
Sample –OLN Completion
44
Sample – Staff Engagement Scores
2014 2015
Clinical documentationimprovement
27.7% 38%
Coding 44.9% 44.9%
In an effort to create an even better place to work,Ochsner conducts employee, leader, and clinician surveys to identify organizational anddepartmental strengths and opportunities for improvement. Input is very important in order to determine what we are doing well and what we can improve.
45
Thank you. Questions?
[email protected]@ochsner.org
In order to receive your continuing education certificate(s) for this program, you must complete the online evaluation. The link can be found in the continuing education section at the front of the program guide.