ipq international harmaceutical quality · for chromatography system suitability, the lab reviewer...
TRANSCRIPT

UNITED STATES
EDITOR’s NOTE: Welcome to IPQ’s “Monthly Update” on key CMC/GMP developments in the US, Europe, and internationally. The IPQ family of publications includes “The News in Depth” and”Updates in Brief” on our website as they occur, “Weekly News Alerts” sent via e-mail, and the “Monthly Update.” IPQ’s suite of offerings support our mission of helping readers under-stand, engage in and respond to the dialogue and developments around evolving and harmo-nizing the regulation of drug and biologic quality and manufacturing. Subscribers and license holders to IPQ have access to all of these sources of cutting-edge news and in-depth analysis as well as to the full IPQ archives. Visit IPQpubs.com for further information.
Bill Paulson, Editor-in-Chief
MONTHLY UPDATE - JANUARY 2014
IPQWWW.IPQPUBS.COM
INTERNATIONAL PHARMACEUTICAL QUALITY
Inside the Global Regulatory Dialogue
VOL. 5, NO. 1
CMC/REVIEW
• Top Analytical Method Problems in INDs and BLAsInclude Not Enough Detail for FDA Replication and Inade-quate Suitability Controls..............................................................2
GMP/INSPECTION
• CDER Compliance Office Quality Regulatory Priorities for2014 Include Implementing DQSA, FDASIA and Reorganiza-tion Plans........................................................................................13
INTERNATIONAL
CMC/REVIEW
• Biotherapeutics Developers Are Wrestling with Challeng-es of Connecting Quality Attributes to Immunogenicity....21
UPDATES IN BRIEF - p. 32
U.S.: • five-year IT plan • drug shortage report to Congress • unique device identifiers • USP storage temp revision
EUROPE: • EMA biosimilar quality statistics • MHRA Orange Guide revision • EMA EudraGMDP database
INTERNATIONAL: • US/Canada e-submissions • Canada drug quality submissions • FDA in China • ANVISA track and trace • Rx-360 in China • FDA and Europol on counterfeiting
IPQ is now on Facebook and Twitter. Come join the global regulatory dialogue.
BREAKING NEWS AT YOUR FINGERTIPIPQ’S RSS FEED

International Good Manufacturing Practices Conference
AGENDA HIGHLIGHTS:• Current Compliance Findings
and Trends • Analysis of an Injunction Case • Critical Role of the Quality
Control Unit• Field Alerts• Counterfeit Drugs• International Topics
Keynote by Commissioner Margaret Hamburg (invited) Featured speakers – Martin Van Trieste, Deborah Autor, Steve Solomon and Tor Graberg.
38thAnnual
www.internationalgmp.com for program and registration information
Sponsored by the FDA and the UGA College of Pharmacy
Many FDA speakers and a Health Canada speaker
MArCH 10-13, 2014 Athens, Georgia
Spotlighting Solutions to GMP Violations
$1095 – Before 1/17/2014
$1195 – January 17 to February 21, 2014
$1295 – After February 21, 2014
For every two paid registrations from the same company, get the third registration FrEE until 2/21/2014
Early Registration Discount
MONTHLY UPDATE - JANUARY 2014
WWW.IPQPUBS.COMJANUARY 2014 �
MONTHLY UPDATE - JANUARY 2014
UNITED STATES
International Pharmaceutical Quality TM (ISSN 1937-6898) is dedicated to helping its readers understand, engage in and respond to the dialogue and developments around evolving and harmonizing the regulation of pharmaceutical and biologic qual-ity and manufacturing.
Subscriptions and licenses include full access to IPQ’s news up-dates and in-depth analysis plus the full archives. See IPQpubs.com for individual subscription and company/organization license rates.
© 2013. All rights reserved. IPQ Publications LLC. Content cannot be transmitted except for internal use by companies/organiza-tions that have licenses. For copies/reprints for other use, contact Wayne Rhodes ([email protected], 202-841-9470).
INTERNATIONAL PHARMACEUTICAL
QUALITY™
Editor-in-ChiefBill [email protected]
Senior EditorJerry [email protected]
Chief Financial OfficerRob [email protected] ext.105
Sales/Marketing Coordinator Wayne [email protected]
ReportersTed Seabright [email protected] 571-213-6318
Aaron Kozloff [email protected] 240-678-4637
Food and Drug Law AdvisorEve [email protected]
7920 Norfolk Ave., Suite 900,Bethesda, MD 20814
Top Analytical Method Problems in INDs and BLAs Include Not Enough Detail for FDA Replication and Inadequate Suitability ControlsInsufficient detail to allow FDA to replicate an analytical method, and failure to include appropriate system suitability controls, are two prominent analytical method problem areas that FDA is finding in reviewing investigational new drug (IND) and biologic license application (BLA) submissions.
Other common deficiencies in analytical method submissions include not submitting the actual test instrument output, using a compendial method for a non-compendial product without sufficient validation, and not evaluating linearity.
At an IBC “Well Characterized Biologicals” conference in Washington, D.C. in late October, CBER Division of Biological Standards and Quality Control Analytical Chemistry Team Leader Alfred Del Grosso reviewed the “top ten” analytical method inadequacies in IND and BLA submissions and what companies need to submit to smooth out the application clearance process.
The FDA reviewing official stressed that such deficiencies are resulting in information requests and can delay application clearance.
These analytical concerns do not generally result in a “refuse to file” status or a rejection letter, as the agency is usually “able to iron out most issues regarding quality in a submission,” Del Grosso commented. However, paying attention to the agency’s expectations for these analytical
method submissions will “ease the process for everybody” involved.
Based on his extensive method reviewing experience, Del Grosso provided valuable insights into FDA’s expectations and how to avoid agency questions for each of the ten problem areas.
Common Lab Submission Deficiencies Explored
In his presentation, Del Grosso explored the top deficiencies he has seen in detail, and explained how each impacts FDA’s ability to review applications. [Del Grosso’s complete remarks are provided below.]
One of “the most common” deficiencies in laboratory submissions is a lack of sufficient detail to allow FDA personnel to replicate the submitted method in its labs.
Although a “fairly complete” SOP may be submitted, many times agency scientists are still unable to replicate the method. Upon inquiry, the agency finds out that important information – for example, regarding column conditioning or sample preparation – was not included in the submitted information.

MONTHLY UPDATE - JANUARY 2014 MONTHLY UPDATE - JANUARY 2014 MONTHLY UPDATE - JANUARY 2014
JANUARY 2014 �
INSIDE THE GLOBAL REGULATORY DIALOGUE™
“Full detail is critical,” Del Grosso stressed. He added that if the SOP is in a foreign language, a “good, detailed” translation is required.
A second inadequacy Del Grosso has seen “very often” is a failure to include appropriate system suitability controls. For chromatography system suitability, the lab reviewer recommends consulting USP Chapter <621> on chromatography.
System suitability, he noted, is required even in cases in which a chromatographic method yields a single peak, or if there is extremely good resolution between the peak of interest and any potential interferences. Whenever possible, a control sample procedure for tracking and trending throughout the lifecycle should be incorporated. If that is impractical due to analyte instability, then it should be justified, Del Grosso stressed. “At a minimum, a check standard or matrix spike should be part of the procedure.”
He characterized as fundamental to a chromatographic procedure: ● injection repeatability ● efficiency and resolution of symmetry or tailing, and ● an impurities or limits test of signal-to-noise determination. In addition, non-chromatographic procedures – for instance, titration – should include a blank, or in the case of polarimetry, a rotational standard. Immunoassays should include monitoring by a control sample or matrix spike as appropriate.
Actual output from analytical instruments showing the data used in submissions – for example, from chromatographs and mass spectrometers – is another important aspect of the review process, but is frequently not submitted.
“We like to see exactly what is going on,” the CBER lab leader commented. He recommended that chromatograms, for instance, should be submitted for standards, representative samples, and blanks, and also for a control sample, if one is used.
When instrumental outputs are submitted, it is important that they be labeled such that agency reviewers know what they are looking at. Standards, samples, and batches should be labeled as such, and samples should include a batch number. Axes on charts should be labeled and include the units used in the measurement.
In some cases – for example, for certain spectroscopic procedures that include extensive mathematical formulations or de-convolution, such as near-infrared – instrument output is not required. However, being able to see a basic spectrum before a convolution and some rationale why the
wavelength range was chosen is “useful.”
Also common in Del Grosso’s experience is an incorrect assumption that “just because a method is listed in a pharmacopeia somewhere, validation is not needed,” – an assumption that is not true when a non-compendial product is involved. And in all cases, suitability needs to be confirmed.
He pointed to 21 CFR 211.194(a)(2), which states that, for standard methods, validation data is not required, but that “the suitability of all testing methods used shall be verified under actual conditions of use.”
This means, Del Grosso emphasized, “that even though something is a standard method, it does have to be shown that it works for your product in your matrix.”
USP general chapter methods are only compendial when applied to compendial products, he pointed out.
Del Grosso noted that there are very few biologic products in the USP. “So if the USP general chapter method is applied to anything other than a compendial product, validation verification, or technically speaking, full validation of the method, may be required.”
European pharmacopeial products are not recognized as compendial for U.S. submissions, the CBER reviewer explained. “They may have some degree of status as standard methods, so the validation requirements may be a little bit less. If you want to make that case, come up with a good argument for it.”
Discussing analytical method lifecycle management at the CASSS/FDA “Symposium on the Interface of Regulatory and Analytical Sciences for Biotechnology Health Products” (WCBP) in late January in Washington, D.C., Del Grosso said that a draft guidance on analytical methods and procedure validation originally published in 2000 has been updated and is now in the queue to be released in the Federal Register for comment.
The guidance is a joint CDER/CBER effort and will include the concept of analytical life-cycle and monitoring, as well as quality-by-design concepts, with references to the supporting ICH documents.
Info Missing on the Peaks
Drawing discussion in the Q&A after Del Grosso’s presentation were: ● the assessing and labeling of peaks

MONTHLY UPDATE - JANUARY 2014
WWW.IPQPUBS.COMJANUARY 2014 �
MONTHLY UPDATE - JANUARY 2014
● requirements for validation of Phase I batches ● whereinformation should be submitted in the common technical document (CTD), and ● submitting changes to SOPs.
One participant asked if FDA expects each peak in a chromatogram to be identified and labeled.
The question, Del Grosso responded, is whether each peak is critical. “If that information is relevant to the submission, if it is something that you are quantitating or measuring, then yes.”
Referencing a fully validated peptide map, he suggested that ultimately “every peak should be identified, so some labeling and listing would be critical.”
Another participant asked about the expectations for assessment and validation of a profile judged to be similar to the reference standard – for example, regarding identification tests such as glycan profiles.
Del Grosso stressed that an identification test should not be simply a visual comparison – that the peaks being examined should be indicated along with an explanation of what peaks are expected and the retention time windows relative to the standard.
“I realize that can change,” he said, and that there may not be an “absolute” retention time window. However, the applicant should know in each case how different it can it be. By way of example, the reviewer suggested language such as, “we are looking for peaks one through six, and we expect to see these within a such-and-such a retention time difference percentage.”
Queries Extend From IND to Post-Approval
Addressing a question regarding the minimum analytical package that would be considered sufficient for a Phase I validation, Del Grosso indicated that submissions early in development are not expected to be definitive.
“We realize that there are going to be important formulation
changes, and that the actual range level has not been established yet,” he said.
“There should be some information as to why the assay is appropriate. There should be some information about precision, specificity, and accuracy. But no, a full validation at that point is not expected.”
Where validation information should go in the CTD and whether it should be repeated or cross-referenced was also addressed during the Q&A.
Validation information in sections P5, S4, and R2 can be submitted as summaries, Del Grosso explained. “We do like to see, if at all possible, a full validation report submitted as an attachment. It is most convenient if it is electronically linked to those attachments.”
Regarding cross-referencing or reproducing the information from P5 and S4 in R2, the CBER lab expert noted that “usually” the full report is either in the regional information or attachment section “with a link to the summaries and the analytical procedure and validation.”
Revisiting comments Del Grosso made during his presentation, a participant asked for clarification regarding what changes made to an SOP are considered major or minor – specifically, what the classification would be for changing the system suitability to improve a procedural method.
Del Grosso replied that changing system suitability is a minor change.
At issue is whether it is going to impact the final results. “If it is just a change of system suitability and does not impact results, in most cases it would go into an annual report rather than a changes being effected [CBE].”
DOWNLOADS FROM THE STORY: FDA submission guidances: • For drugs• For biologics
[Story continues on page 5.]

www.usp.orgGAMS292F_ 2014-1
Future USP Global Education and Training Courses, Meetings, Workshops and More!
Global Education and Training Courses
Featured Classroom Courses
§ Brazil: Excipient Performance; Developing and Validating Dissolution Methods
§ China: Essentials of Compendial Microbiology Testing; Analysis of Elemental
Impurities; Pharmaceutical Waters; Dissolution: Theory and Best Practices
§ Europe: In-Vivo In-Vitro Correlation (IVIVC); HPTLC for Identification
of Articles of Botanical Origin
§ India: Pharmaceutical Stability; Effectively Using USP–NF; Practical
Applications of Chapter <467> Residual Solvents
§ United States: Effectively Using FCC; Good Manufacturing Practices;
Analysis of Elemental Impurities; Dissolution: Theory and Best Practices
Webinars Increase your knowledge of compendial activities!
The USP Global Education and Training Department has launched a series of webinars to increase distance learning opportunities for the pharmaceutical industry. These sessions are conducted by USP Scientific Liaisons or Expert Committee Members who are directly involved in the standards-setting process.
For Classroom Course Information and Schedules Contact [email protected], or visit www.usp.org/meetings-courses/courses and click on the appropriate language if other than English. All Europe offerings are available in English. For India offerings, contact George Mathew at [email protected].
FOR MORE MEETING AND WORKSHOP INFORMATIONVisit www.usp.org/meetings, contact [email protected] or call +1-301-816-8130.
NOTE: Events held at USP Headquarters, Rockville, MD (U.S.) unless otherwise indicated. Courses, symposia, workshops and dates subject to change.
USP Workshop Series
March 24–25, 2014
§ Dissolution Testing of Capsules
June 2–3, 2014§§ 6th Bioassay Workshop
August 2014 (Date–TBA) § DNA Barcoding of Botanical Articles
September 8–9, 2014 § Alternative Microbiological Methods
October 1, 2014 § Synthetic Therapeutic Peptide—Regulations,
Standards and Quality
November 5–6, 2014 § Contaminants in Foods–Compendial
Approaches to Protect Public Health
MONTHLY UPDATE - JANUARY 2014MONTHLY UPDATE - JANUARY 2014 MONTHLY UPDATE - JANUARY 2014
JANUARY 2014 �
INSIDE THE GLOBAL REGULATORY DIALOGUE™
FDA REVIEWER AL DEL GROSSO ON TOP ANALYTICAL DEFICIENCIES IN INDS AND BLAS
At the IBC Well Characterized Biologicals conference in Washington, D.C. in late October, CBER Division of Biological Standards and Quality Control Analytical Chemistry Team Leader Alfred Del Grosso presented a listing he had made of the top ten analytical method inadequacies in IND and BLA submissions, based on his extensive reviewing experience. On the list are submission problems regarding: ● procedure detail ● arithmetic calculations ● system suitability ● inclusion of instrumental output ● validation characteristics or parameters ● instrumental output labeling ● use of statistics ● evaluating linearity of standards ● com-pendial method designation ● verifying of compendial procedures ● robustness evaluation, and ● validation report inclusion. Del Grosso’s insights into the problems and what can be done to avoid them is provided below.
I have been with FDA for a long time. I have spent most of my career reviewing analytical methods and validation studies submitted with Biologics License Applications [BLAs] and supplements. I know a very common point of interest is what goes wrong, what questions we have, what comes out of information requests, and what delays the approval process. I am happy to be here today to share some of this experience with you.
Just a couple of disclaimers – FDA does not insist on this, but I always like to throw it out: These are informal communications. They are my best judgment. They are my experience. They are based on certain things I have seen over a long period of time. They are not based on anybody’s specific BLA application or supplement in particular.
I will just give you a very quick outline of what I do. We will take a very quick look at regulations and submission requirements, and, as the title of the talk suggests, we will be talking mostly about common factors that delay approvals for analytical methods and the validation studies that are required to be submitted along with the analytical procedures.
Review Process and Requirements
Just to let you know my own perspective: I am in the Center for Biologics Evaluation and Research [CBER]. We cover the regulatory review and lot release of vaccines, blood products, allergenic extracts and allergen patch tests. Most of you probably know biotherapeutics and monoclonal antibodies. Years ago they were regulated by CBER but they are now under the jurisdiction of the Center for Drug Evaluation and Research, although still regulated as Biologics. I am in the Office of Compliance and Biologics Quality, the Division of Biological Standards and Quality Control, as the head of the analytical chemistry team.
One of the roles we have is product control testing for all the different products that we regulate. We do routine lot release. A certain percentage of the lots which are submitted for release onto the market are tested at our own discretion. We have what we call ‘program test plans’ for a number of products, in which typically anywhere from 10% to 100% of the lots that come in are tested for potency, physical characteristics, and certain critical components. We are involved in new product approval, biological license application reviews, and supplements. We do a certain amount of method development. We do a certain amount of physical/chemical analysis. Traditionally, a lot of this has been focused on impurities and components, but more and more we are getting into potency measurements.
For typical methods, such as ion exchange chromatography, we do a lot of work on glycoconjugate vaccines. And there is more and more interest in the use of marker peptides for quantitation of some biological products, including influenza virus vaccines – we are doing a lot of collaborative studies related to that. We do regulatory review of analytical methods, BLA supplements, some review of master files, and INDs [Investigational New Drug applications]. We do not get too involved with INDs – we are mostly involved with those on a consultative role.
Regulations are governed under Section 21 of the Code of Federal Regulations – the Food and Drug Regulations. The 210s and 211s are drug current good manufacturing processes [CGMPs], which covers both drugs and biologics. They cover organization, facilities, equipment, components, production and process controls. The 300s and 314s specifically cover new drug applications for pharmaceuticals – marketing authorizations. The 600s are specific to biologics – 601 is biologics licensing and 610 is biological product standards. Section 58 is also useful as far as good laboratory practice [GLP] and non-clinical studies in early product development….

MONTHLY UPDATE - JANUARY 2014
WWW.IPQPUBS.COMJANUARY 2014 �
MONTHLY UPDATE - JANUARY 2014
Generally speaking, we are usually able to iron out most issues regarding quality in a submission. If something is ultimately ‘refuse to file’ or receives a rejection letter, it is usually based on clinical considerations. However, we certainly do like to ease the process for everybody in terms of what we expect and what is easiest to review….
The general requirements for submission of a method include:
● The objective and the scope of a method
● What the principle of the method is – basically, is it chromatography? Is it mass spectrometry? Is it animmunological method?
● Details regarding the sampling
● Equipment and parameters
● Reagent stability and acceptance criteria
● Characterization of the reference material if it is a non-compendial method or a non-certified standard material
● System suitability requirements – I have to emphasize system suitability should be built into the method
● Whenever possible use a suitable control sample to track method performance. You have to realize this may notbe feasible because of stability of the analyte, which may be a consideration, in which case we recommend that a secondary check standard may be required. In general, a secondary check standard, while it is not absolutely required, is a good practice in any analytical procedure.
● Detailed standard operating procedure [SOP] – I really have to emphasize that. As you will see later, we geta lot very brief summaries submitted. But our standard is that the procedure should be detailed enough in most cases, unless it is a very straightforward compendial procedure, that we are able to replicate it – either because we may want to do that or because we simply need that much detailed information in order to do a proper review. It should include: the preparation of standards and samples; all calculations; method reporting, including exactly how reported results will be expressed; representative instrumental outputs, such as chromatograms and spectra for standards and samples; and the all-important validation report.
Top Ten Analytical Inadequacies
The organizers asked that I submit this in terms of the top ten inadequacies. It was not very hard to come with a top-ten list.
Sufficiently Detailed Procedures
Probably one of the most common ones is that the procedure just does not have enough detail. We want to see enough that we are able to replicate the procedure. Also, an inadequate description of calculations: Sometimes we see results and we just cannot understand how they came up with them, and so an information request may be necessary.
We highly recommend, even if you are going to give a method summary – some firms like to do this – to include a working SOP or a fully detailed translation. I know a lot of manufacturing and quality control may be done overseas. Maybe the actual working SOP is in a foreign language. But a good detailed translation with all the details is necessary for us to do the experiment.
A lot of times we get a fairly complete SOP, but if we try to replicate a method it just won’t work in our hands. Then we find out that there was something that was very important regarding column conditioning or sample preparation that was just not included or somehow did not make it into what we received. Full detail is critical. It has to be enough that

MONTHLY UPDATE - JANUARY 2014MONTHLY UPDATE - JANUARY 2014 MONTHLY UPDATE - JANUARY 2014
JANUARY 2014 �
INSIDE THE GLOBAL REGULATORY DIALOGUE™
we can successfully adopt or transfer the method into our laboratories.
A lot of firms do not like to submit SOPs. One of the reasons I have heard is that they are worried that any change in the SOP, if it is submitted with the BLA or supplement, could be considered to be a reportable change. Well, that has never been interpreted that way, unless the method is significantly altered. A minor change in an SOP is not considered to be a reportable change. I hope I can put everybody’s mind at rest regarding that.
System Suitability Tests
Inadequacy number two – system suitability tests: a failure to include appropriate system suitability controls. We very often see this. For chromatography system suitability, probably the best reference is USP Chapter <621> on chromatography. System suitability is required even in cases in which a chromatographic method yields a single peak, or if there is extremely good resolution between the peak of interest and any potential interferences. So yes, even in this case, an expression of chromatographic efficiency and tailing may be critical for proper integration, and should be built into the method.
Whenever possible, a control sample procedure for tracking and trending throughout the lifecycle should be incorporated. As I said before, it may be impractical due to analyte instability. If that is the case, then it should be justified. At a minimum, a check standard or matrix spike should be part of the procedure.
I think a lot of this is reiterative. It is a fundamental part of the procedure. A chromatographic procedure should include injection repeatability, efficiency and resolution of symmetry or tailing, and an impurities or limits test of signal-to-noise determination. Non-chromatographic procedures – for instance, titration – should include a blank polarimetry rotational standard. Immunoassays should include monitoring by a control sample or matrix spike as appropriate.
Representative Instrumental Output
We often get chromatographic or mass spectrometric or NMR submissions that do not include instrumental output. We like to see exactly what is going on. So chromatograms, for instance, should be submitted for standards, representative samples and blanks, and also for a control sample, if one is used.
Outputs should be labeled with the identity. We sometimes get chromatograms or other instrumental outputs included, and it is not clear what we are looking at. Is it a standard? Is it a sample? Is it a batch? If it includes a sample, do you know what the batch number is? It should be interpretable. Label the axes along with the units.
These may not be required for certain spectroscopic procedures that include extensive mathematical formulations or de-convolution – near-infrared, for instance. You just do not have much of an expressible spectrum for the final result. Even so, it is useful to be able to see a basic spectrum before your convolution and some rationale why this wavelength range was chosen.
Going on to validations – you are probably very familiar with…ICH Q2(R1), which covers the different validation characteristics that are required for different categories of tests. Content and potency, under assay, requires evaluation of accuracy – I should not say requires, but recommends. This is what we look for: ● accuracy ● repeatability ● short-term precision ● intermediate precision of replicate assays ● different assay procedures ● specificity ● a qualitative measure of the analyte response that is, in fact, due to the analyte ● linearity ● range, and ● robustness.
For quantitative impurities we require everything we just mentioned as well as limit of quantitation and possibly limit of detection.
A limits test is the most simplistic validation, with the lowest number of characteristics required to show specificity, limit of detection and, in most cases, the robustness of the procedure.
Identification tests require evaluation of specificity and detection limit, possibly robustness, depending on the nature
MONTHLY UPDATE - JANUARY 2014
WWW.IPQPUBS.COMJANUARY 2014 �
MONTHLY UPDATE - JANUARY 2014
of the test.
Test the physical properties: These can include things as diverse as molecular size distribution in the case of a glycoconjugate or polysaccharide product, or in the case of therapeutics, or monoclonal antibodies, or blood factors separating into monomer fragment aggregates – with the acceptance criteria for these.
Accuracy, repeatability, intermediate precision, specificity, and robustness should always be evaluated.
Some general guidelines for method validation: validation characteristics should be evaluated for reportable results with the exception of linearity.
Replicates should be done according to the method procedure. If the method procedure says three replicates, then that is what should be done in evaluating, say, intermediate precision and repeatability of each point. These should be done using representative lots of appropriate materials, whether you are looking at intermediates, bulk drug substance, final container, or final bulk form. It should involve multiple lots. And we do recommend design of experiment [DOE] methodology to evaluate validation characteristics simultaneously, and possibly the use of DOE software.
We often get the question, ‘is it okay to use data that is used to establish linearity to establish accuracy?’ Or, ‘can data from robustness studies be used for some of the other analytical characteristics?’ The answer is unequivocally ‘yes.’ Although in the case of robustness, where you are looking for subtle variations of analytical parameters, data used to support other characteristics should be within the operating parameters as determined by the final method.
Types of Validation Characteristics or Test Categorization
Inadequacy number four is sort of a general one: types of validation characteristics or test categorization. We find sometimes that not all of the validation characteristics are addressed for the category of test – for example, specificity may not be included. The tests may not be categorized properly. We often see limits tests applied for process and product impurities that should be quantified or monitored.
In most cases, limits tests – I don’t want to say they are discouraged, but they should be used when technological limits do not allow quantitation, or the limits are set so far below the level of any toxic concern that they may be justified just in terms of being able to ensure adequate process control. Product impurities should, we recommend, be quantified and monitored.
Failure to include all the data: A full validation report should be submitted or attached or linked to the submission. It is very important in doing a validation report that we are able to see most of the raw data that went into that report, not just a general summary table. That does allow elimination of a lot of information requests if we do have questions about it.
Regarding these issues, limit of quantitation as defined in ICH Q2(R1) is the lowest amount of analyte in the sample that can be quantitatively determined with suitable accuracy and precision, and should be expressed in most cases as concentration.
There are a number of estimation methods. USP recommends ten times signal to noise. ICH recommends ten times the standard deviation response divided by the slope of the calibration curve.
It is important that any estimates of LOQ [lowest observable quantity] need to be verified experimentally for linearity, accuracy, and precision. Very often we just see estimates. If you are actually going to be working down in that range, it is very important that the reliability in that range be demonstrated.
LOQ and LOD [limit of detection] are very often submitted, as we see, for component analytical procedures, and there is nothing wrong with that. We do not mind seeing the data. But it is only required for quantitative impurities tests.
I think I mentioned limits tests – the lowest amount of analyte in the sample that can be reliably detected but not

MONTHLY UPDATE - JANUARY 2014MONTHLY UPDATE - JANUARY 2014 MONTHLY UPDATE - JANUARY 2014
JANUARY 2014 �
INSIDE THE GLOBAL REGULATORY DIALOGUE™
necessarily quantitated.
Regarding estimation methods, ICH Q2(R1) mentions three different possibilities: ● peak height greater than two to three times signal to noise, which is also USP ● three times the standard deviation of the blank or matrix response, or ● two to three times the standard deviation of the y-intercept over the regression line when the analyte is down in the range of limit of detection.
Again, reliability estimations have to be verified experimentally. Basically, the ability to consistently detect the specifi-cation limit has to be established.
I did not list this as one of the top ten, but I thought I would point it out: A very common inadequacy, and I guess I already mentioned this, is the estimation of LOD or LOQ with no experimental verification to demonstrate reliability. Use of the limits test is not appropriate just because of a ‘less-than’ specification, and should be justified. The limits tests are often use to establish clearance of process impurities of toxic concern, and quantitative determination of impurities is advised whenever it is technologically possible.
Linearity in the Sample/Fully Representative Matrix
Inadequacy number five is linearity and matrix – the failure to evaluate linearity in the sample or fully representative matrix. This is very common. We will see linearity based just on the analyte alone, or just standard solutions. The definition of linearity, taken from ICH Q2(R1), is proportionality of response to the concentration of analyte in the sample.
We recommend a minimum of five concentrations. There can be some exceptions: Three levels may be acceptable for a narrow range, maybe 80 to 120% of expected concentration across the range of the method. This is very common for a lot of potency or component assays. It can be expressed using a correlation coefficient, r, or coefficient of determination, r-squared.
I know a lot of statisticians have an issue with the use of correlation coefficients to express linearity. They can be wrongly interpreted as a high r-squared and may not indicate that there may be some problems at some point throughout the range, if it is a wide range. However, I think this is so ingrained in the analytical community that we are not going to get away from it at this point. So r and r-squared, biased y-intercept, slope-regression line, and I did not include it in the slide, but a graphic portrayal of linearity – actually seeing what the points look like – [are recommended.]
We realize that some procedures, like immunoassays, may be essentially non-linear. In this case, the appropriate function of analytical response to analyte concentration should be described as well as some measure as to how well the data fit the proposed model. If weighting or complex regression is being used, it should be justified why you used this approach.
Verification of Compendial Procedures
This is a very common one. Sometimes validation information is not submitted or a validation study may not even be done. There is an assumption that just because a method is listed in a pharmacopeia somewhere, validation is not needed. Well, let’s look at the regulations: 21 CFR 211.194(a)(2) says that for standard methods, validation data is not required, but ‘the suitability of all testing methods used shall be verified under actual conditions of use.’ So this basically means that even though something is a standard method, it does have to be shown that it does work for your product in your matrix.
USP general chapter methods are only compendial when applied to compendial products. There are very few biologic products that are in the USP. I think the USP is writing up some monographs. But that is kind of getting into an area we don’t want to get into right now, as to whether CBER is going to accept that or not. So if the USP general chapter method is applied to anything other than a compendial product, validation verification, or technically speaking, full validation of the method, may be required.
It is also important to point out that European pharmacopeial products are not recognized as compendial for U.S. submissions. They may have some degree of status as standard methods, so the validation requirements may be a

MONTHLY UPDATE - JANUARY 2014
WWW.IPQPUBS.COMJANUARY 2014 10
MONTHLY UPDATE - JANUARY 2014
little bit less. But if you want to make that case, come up with a good argument for it.
For compendial or standard procedures, a good guidance to look at is USP <1226> general chapter on verification of compendial procedures. Good questions to ask are: Does the standard method meet the requirements? Does it show specificity in the matrix? Is it range-appropriate? The minimum requirements for adoption of the standard procedure that we consider are: ● the specificity of the matrix ● precision ● repeatability ● intermediate precision ● suitability of use ● establishing repeatability of intermediate precision in your own laboratory, and ● stability of standard solutions.
Robustness of Critical Assay Parameters
There is some confusion about whether robustness is considered to be a validation characteristic. I think a lot of the guidances do say that it should be part of method development, and it really should be before proceeding in the final validation of a method. Robustness is a characteristic that should be in the submission in the main part of the validation report. Or in some cases, if robustness is done, there may be some critical assay parameters that are not evaluated.
ICH Q2(R1) defines robustness as the ‘measure of the capacity of a method to remain unaffected by small but deliberate variations in method parameters, and provides an indication of its reliability during normal usage.’ It should be evaluated during method development and qualification. As I have said, data from robustness should be included as part of the validation report and the submission of the analytical methods package to the agency.
I am primarily a chromatographer, so looking at some of the HPLC method factors such as column manufacturing lot is critical. We have seen some submissions in which the whole validation was done on one column and when we sent it back and said, ‘we would like to see some evaluation of more than one lot of a column,’ they found that was then the assay failed, and the manufacturer basically had to submit a whole new analytical method.
Some other important HPLC method factors include: ● flow rate and gradient profile ● mobile phase composition, including cleaning buffer concentration, pH, organic modifier ● injection volume ● column temperature, and ● detection wavelengths or other parameters.
For all types of procedures, stability reagents, prepared samples and standards should be evaluated if they are not going to be used right away.
Evaluation factors include: ● critical pair resolution ● peak areas for injection repeatability ● capacity factors for retention time, and ● peak asymmetry.
Acceptance criteria for robustness should be set before the study is done. And ultimately the goal is to establish parameter limits for the method when it is in use.
Robustness can be done one factor at a time – varying one factor while keeping others at a nominal level. It took a long time to get away from this. Using DOE is definitely a big advantage for everybody because it reduces the number of experiments and also yields better information…. It allows looking at interaction effects and multiple changes at the same time and a significant reduction in the number of experiments.
Accuracy Calculations
We see this quite a bit. Validation of accuracy is recovery percentage of total amount of analyte after addition, and not the recovery of the added quantity. So the base amount of analyte in a sample is included as part of the total recovery. This does give a better overall percentage, but it is just not very good information. Definitely recovery should be calculated on the amount added, not on the total amount expressed as percent recovery.
Determination of accuracy on midpoint or label claim and not at the intended range of the assay [is also a problem]. Accuracy should be evaluated across the entire range of the assay. Three levels are recommended. The usual
MONTHLY UPDATE - JANUARY 2014MONTHLY UPDATE - JANUARY 2014 MONTHLY UPDATE - JANUARY 2014
JANUARY 2014 11
INSIDE THE GLOBAL REGULATORY DIALOGUE™
minimum is 80% to 120% of target across the range of the method. If 80% to120% is the acceptance criteria for the analyte being measured, that should be done at a minimum, and I would probably recommend to go beyond that, say to 50% to 150%.
Spiking, we realize, in some cases, may not be fully representative of recovery in extractive digestive sample preparations. In that case, it may be necessary to consider some other method of determining accuracy, such as an orthogonal method.
A biological products matrix without analyte may not be available, so it may be necessary to spike on top of what is already there. Percent recovery can be established by standard additions. We mentioned calculated recovery on quantity added, not total. Critical factors include the reference material.
Conversion factors: As I mentioned before, sometimes we do not get full information about all calculations, which makes it very difficult to do a review, and results in an information request.
Evaluation of Range
A common failure is to not evaluate precision and accuracy across the full defined range of the procedure. A range should not be based just on linearity or LOQ at the lower end of the range, particularly if LOQ is only determined by one of the estimation methods that we looked at earlier.
Range is defined as the interval for which precision, accuracy, and linearity have been validated. Range should be expressed as reportable results, using the same units as the test samples.
Choice of Factors and Intermediate Precision
Sometimes some factors are not included – for example, reagents, lots, analysts – maybe instruments or locations, if that is applicable, if the method is going to be used in more than one place, which is very often the case.
Repeatability is defined as multiple determinations of homogeneous samples. You have to distinguish this from injection repeatability. Injection repeatability might be six injections of the same material. Repeatability should include all steps in sample preparation, and each point should include the number of replicates which are used if two or three replicates or more are part of the standard procedure.
ICH Q2 recommends nine determinations at three concentration levels, or six at 100% of test concentration. If this approach is done for repeatability, it does not necessarily have to be done at the full range of the analytical procedure.
Intermediate precision, different analysts and equipment, and other random events should be done across the full range of the procedure. Reproducibility between laboratories may be factored into intermediate precision, but it is not normally required for regulatory submissions. It is, of course, in the USP general chapter <1225>, because that is a submission to the compendia, but it is not an analytical characteristic FDA requires for our submissions.
Summary
So just to go over some typical procedural and validation issues to reiterate what I have already said: ● insufficient detail in the procedure ● inadequate descriptions of the arithmetic calculations ● inadequate system suitability ● failure to include instrumental output ● incomplete validation characteristics or parameters ● failure to label instrumental outputs ● improper use of statistics ● linearity evaluation on standards ● incorrect designation of the method as compendial ● adoption of compendial procedures without verification ● inadequate robustness evaluation, and ● failure to include the validation report.
I would like to mention a few of the guidances that we find useful and recommend that everyone use as a basis for their own studies and submissions. ICH Q2(R1) is basically the principle, the text and methodology of validation procedures, and covers all the characteristics that we use as a guide in our own reviews. A lot of the FDA guidelines

MONTHLY UPDATE - JANUARY 2014
WWW.IPQPUBS.COMJANUARY 2014 1�
MONTHLY UPDATE - JANUARY 2014
are fairly dated – there is one from 1987, which is a CDER document about submitting samples and analytical data for method validation. As a reviewer guidance, validation and chromatographic procedures are from 1994.
As some of you know, there was a draft guidance published back in 2000 on analytical procedures and method validation. It was a joint document from CBER and CDER, and I was CBER’s principle representative on that. I still get a lot of questions on the status of that guidance. It sort of dropped into a regulatory black hole, unfortunately, and never made its way out until last year when we started, basically, almost looking at it from scratch.
We decided that some of what was in there was reiterative of what was already in ICH Q2(R1), so those parts are being dropped and references to ICH Q2(R1) will be included. There is going to be a lot of stuff in there, which includes incorporating the whole concept of analytical life-cycle and monitoring, as well as quality-by-design concepts. The draft has been finalized and with any luck it might be published in the Federal Register in 2014 for comment. We will keep our fingers crossed. I think it will be a very useful document.
I would like to mention a few other guidances: ● guidance to industry on changes to an approved application for biological products – very useful for post-approval changes ● similarly in CDER, changes to an approved NDA or ANDA (new and abbreviated new drug applications) ● also quality systems approach to pharmaceutical cGMP regulations from 2006, and of course ● all the USP general chapters on validation and verification, transfer, and chromatography.
For guidances with FDA drugs, here are a couple of websites where all the documents, except for the ones from USP, can be accessed (links provided below). In general, it is pretty easy to navigate there from FDA.gov, and 21 CFR is available at gpoaccess.gov.
WASTED ENOUGH TIME SEARCHING THE INTERNET?
Come to IPQpubs.com to find all the important CMC/review and GMP/inspection developments in the US, Europe and internationally.
All the stories that appear in IPQ’s real-time “In the News” web coverage and in our“Monthly Update” are indexed and searchable on our website
--with the relevant document links you need ready at hand.
We do the work so you don’t have to.Visit IPQpubs.com and relax.

The Advantage ofUnrivaled Quality...by Design
Components
Ensuring a drug product maintains its safety and ef� cacy from concept to commercialization while reducing total cost of ownership requires high-quality packaging components.
West designed NovaPure components within a Quality by Design framework. Our data-driven process provides a deeper understanding of our product development and manufacturing processes. We apply this knowledgeto components that can help customers build quality, safety and ef� cacy into their drugs.
Our holistic approach encompasses a thorough process review, from raw materials to commercial manufacturing to transportation of components to the customer’s facility.
NovaPure serum stoppers, lyophilization stoppers and syringe plungers are globally available with a reduced lead time, and are providedin optimized packaging that helps ease the transition through manufacturing environments.
West NovaPure®
#6731
The New Definition of High-Quality Components
West and the diamond logo and NovaPure® are registered trademarks of West Pharmaceutical Services, Inc., in the United States and other jurisdictions.
© Copyright 2012 West Pharmaceutical Services, Inc.
Unrivaled Quality…by Design
To learn more about West’s NovaPure technology, call your West account manager or a Technical Customer Support representative.
Contact West today.
North America +1 800-345-9800Europe +49 2403 7960Asia Paci� c +65 6860 5879
www.westpharma.com
6731 NovaPure Advert.indd 1 3/29/2012 8:46:01 AM
PAREXEL Internationalwww.PAREXEL.com
A proactive approach to achieving and sustaining
compliance is ideal. But, if the unforeseen occurs,
you need to make well-informed decisions to
overcome a product crisis.
PAREXEL has a rapid response staff consisting of
more than 25 former regulators in the U.S. and Europe.
Among this group are ex-FDA investigators and compli-
ance experts who have an average 25 years of FDA
experience, plus many years of worldwide compliance
consulting experience.
When knowledgeable, experienced advice is needed
to minimize regulatory enforcement risk and achieve
your objectives, we can help.
To learn more, please visit:
www.parexel.com/strategic-compliance
Sustainable compliance demands a proactive approach
PAREXEL CONSULTING
MONTHLY UPDATE - JANUARY 2014MONTHLY UPDATE - JANUARY 2014 MONTHLY UPDATE - JANUARY 2014
JANUARY 2014 1�
INSIDE THE GLOBAL REGULATORY DIALOGUE™
The top priorities at FDA’s Center for Drug Evaluation and Research (CDER) compliance office in 2014 will include implementing the compounding (Title I) and track and trace (Title II) provisions of the Drug Quality and Security Act (DQSA), signed into law in late 2013, along with the ongoing implementation efforts on the generic drug user fee (Title I), supply chain (Title VII) and drug shortage (Title X) facets of the 2012 FDA Safety and Innovation Act (FDASIA).
Also on the CDER compliance office front burner for this next year will be carrying out the center’s plan to reorganize and realign its quality regulatory structures and strengthen its product and facility surveillance capabilities.
While FDA has already come forward with guidances and Federal Register notices to begin to give regulatory flesh to the Title 1 compounding provisions of DQSA (see IPQ “Monthly Update” Nov./Dec. 2013, p. 28), the agency has not yet formally addressed Title II. It calls for an electronic inter-operable system to identify and trace certain prescription (Rx) drugs as they are distributed through the US.
Providing a review of CDER’s current compliance priorities at the Food Drug Law Institute (FDLI) enforcement conference in Washington, D.C in December, CDER Compliance Office Director Ilisa Bernstein emphasized that the track and trace objectives called for in DQSA have been in the works for “over ten years,” and that implementation will require the agency to write guidances, publish regulations, hold public meetings, launch pilot projects, and write standards.
“We are really working hard at moving forward” on DQSA Title II implementation, Bernstein commented.
The new law will ultimately require every Rx drug product package to have a unique identifier to facilitate tracking and tracing throughout the supply chain. Initially, products will be tracked by lot number. Over ten years, a system for item-level tracking by unique identifier will be put in place.
DQSA also provides for certain information to flow about products as they change hands.
The product verification provisions will require wholesalers and pharmacies to have systems and processes in place to read the unique identifier and verify that the number was issued by the manufacturer.
There are also detection and response provisions that require the identification of suspect products by wholesalers and pharmacies and provide directions on what the different
actors in the supply chain need to do when such products are identified.
FDA is required to set up wholesale distributor and third-party logistics provider (3PL) licensing programs and to set standards. If a state does not have a program that meets the new standards that are established, the impacted wholesalers and 3PLs would be licensed by FDA.
“There are some penalties for non-compliance,” Bernstein explained, “and also a national uniform policy, which basically says that for product tracing and for wholesale drug distributors there are preemption provisions as well.”
Drug Shortage Strategic Plan in Place
CDER’s effort to prevent and mitigate drug shortages during 2013 included developing a better understanding of the quality and manufacturing problems that can cause them and implementing the provisions in FDASIA Title X (see IPQ “Monthly Update” October, 2012, p. 4, Jan./Feb, 2013, p. 22, and March, 2013, p. 2).
FDASIA called for enhanced reporting require-ments on potential shortages and the creation of a task force to look at the appropriate measures to detect shortages in advance and mitigate them. The provisions served as the basis for a formal “Drug Shortage Strategic Plan” released by the agency in early November.
The plan identifies two central goals: improving FDA’s mitigation response to imminent or existing shortages; and implementing strategies for the long-term prevention of shortages by focusing on their root causes. (A link to the plan is provided below).
CDER Compliance Office Quality Regulatory Priorities for 2014 Include Implementing DQSA, FDASIA and Reorganization Plans
DQSA Track and Trace ComponentsDQSA calls for an electronic, interoperable system that identifies and traces certain Rx drugs during their US dis-tribution and contains the following features:
● Product identification● Product tracing● Product verification● Detection and response● Notification● Wholesaler (WDD) licensing/standards● Third-party logistics provider licensing/standards● Enhanced system – 10 years● Penalties● National uniform policy

MONTHLY UPDATE - JANUARY 2014
WWW.IPQPUBS.COMJANUARY 2014 1�
MONTHLY UPDATE - JANUARY 2014
that “important, safe, effective, quality products get to patients.”
Drug shortage problems have also been getting increasing attention by regulators in Europe as part of the implemen-tation efforts on the 2011 Falsified Medicines Directive (FMD) (see IPQ “Monthly Update” July/August 2013, p. 16).
Industry Associations Tackle Drug Shortages
Industry associations in the US have been notably active in working with FDA on drug shortage prevention and mitigation.
The Generic Pharmaceutical Association (GPhA) has been a key player in the Accelerated Recovery Initiative (ARI) – an FDA/industry partnership being coordinated by pharma data manager IMS aimed at forecasting, preventing, and mitigating the impact of drug shortages (see IPQ “Monthly Update” March, 2013, p. 2). A pilot program began in 2013.
ISPE has also been actively supporting the agency efforts (see box below).
The forty-page document includes an executive summary and introduction, and sections on: ● understanding and responding to drug shortages ● FDA’s strategic plan, and ● actions other stakeholders should consider.
Six appendices cover: ● the Federal Register notice announce-ment ● statutory elements ● collecting information on drug shortages ● FDA offices engaged in drug shortage efforts ● coordinating drug shortage efforts in CDER, and ● communicating with external groups.
Following Bernstein to the podium at the December FDLI conference to address the current Center for Biologics Evaluation and Research (CBER) compliance office concerns, Director Mary Malarkey explained that the strategic plan flowed from shortage prevention and mitigation efforts that her office has been involved in “for many years.” (See IPQ “Monthly Update” October 2013, p. 2, for a discussion by Malarkey of other key CBER compliance concerns.)
“This is taking a lot of time,” she emphasized. The agency is putting “a lot of resources” into the effort to ensure
ISPE Drug Shortage Activities
ISPE has developed the following “timeline and milestones” that chronicle its support of FDA’s drug short-age initiatives since mid-2012:
● July �01�: ISPE and a task force of industry leaders met with Dr. Janet Woodcock, Director of the Center forDrug Evaluation and Research at the US FDA, and presented a concept paper concerning proposed activities aimed at helping regulators and industry understand and address the challenge of drug shortages.
● August �01�-January �01�: The task force developed a comprehensive survey for industry professionals afterreviewing the existing body of knowledge on the topic of drug shortages and conducting a preliminary assessment of perceived contributing factors.
● February �01�: ISPE deployed its anonymous industry survey seeking information about root causes ofshortages that can be attributed to technical, manufacturing and quality issues.
● May �01�: ISPE met with the US FDA to discuss the early findings and ways of working together to mitigate oraddress key issues.
● June �01�: ISPE announced its findings to US and European audiences and published the highlights in apublicly available report.
● Q� �01�: The ISPE Drug Shortages Task Force began designing a plan to learn more about key issues revealedby the survey and to develop recommendations for important changes that could help mitigate shortages or reduce them altogether.
● October �01�: The Report on ISPE’s Drug Shortages Survey is cited in FDA’s Strategic Plan for Preventing andMitigating Drug Shortages.
● October �01�: ISPE presented highlights of its emerging plan to the EMA as an invite guest at EMA’s Londonworkshop on product shortages due to manufacturing and quality problems.
● November �01�: ISPE presented post-survey follow up activities and its 2014 plan at the ISPE Annual Meetingin Washington, DC.

MONTHLY UPDATE - JANUARY 2014MONTHLY UPDATE - JANUARY 2014 MONTHLY UPDATE - JANUARY 2014
JANUARY 2014 1�
INSIDE THE GLOBAL REGULATORY DIALOGUE™
At an ISPE/FDA CGMP conference held in June in Baltimore, Maryland, Genentech VP Joe Famulare moderated a session on ISPE’s drug shortage efforts that included participation by Genentech Global Quality and Compliance Senior Advisor Steve Mahoney. The Genentech officials participated on the ISPE team that developed an industry survey conducted that spring to help understand the root causes of shortages.
By examining the six main manufacturing and testing “quality systems,” the survey identified underlying systemic issues that may have contributed to drug shortages or near misses. Among the key survey findings were that:
● aseptic processing equipment has been as a significantfactor in drug shortages, and
● production system issues leading to drug shortagesor near misses have been present during technology transfers or product development in a number of cases.
The ISPE report was cited in FDA’s “Drug Shortage Strategic Plan.” The plan indicates the agency’s intention to work with ISPE to further analyze the survey data.
A session was held at the ISPE annual meeting in Washington, D.C. in November to review the 24-page report prepared by ISPE analyzing the survey findings and potential paths forward.
The regulatory/industry dialogue on drug shortages has also been happening at PDA-sponsored forums including the September PDA/FDA conference in Washington, D.C., at which a breakout and an interest group session was held to focus specifically on the issue.
In conjunction with the 2014 PDA/FDA meeting next September, PDA will hold a “Drug Shortage Workshop” that will continue to explore “the application of risk and knowledge management for addressing drug shortages, incentives for manufacturers to build in proactive controls such as redundant capacity and new technology, more transparency and linkages to supply planning, manufac-turing site metrics and quality status for potential manufacturing partners, purchasers, and prescribers.”
CDER Reorg Driven by Quality Imperatives
In addition to Title X, portions of FDASIA that the CDER compliance office will continue to focus on implementing include: ● the generic drug user fee act (GDUFA) provisions, which are expanding FDA’s review and inspection resources (see IPQ “Monthly Update” November 2013, p. 2 , September 2012, p. 2), and ● Title VII on drug import admission standards, registration of foreign importers, border security, and good importer practices (GIPs) (see IPQ “Monthly Update” September 2013, p. 24 and May 2013, p. 16).
The reorganization of CDER to consolidate and enhance its drug quality regulatory functions will also be preoccupying the compliance office in the coming year.
An Office of Pharmaceutical Quality (OPQ) will consolidate all of the CMC and micro functions for the entire center, including the Office of Generic Drugs (OGD) chemistry divisions, the drug master file (DMF) group, and the micro group (see IPQ “Monthly Update” Nov./Dec. 2013, p. 28).
As part of the reorganization, OGD will become a separate ‘super office’ in CDER, putting it on parity with the other super offices that have user fee programs (ibid. and IPQ “Monthly Update” September 2012, p. 58.)
OGD will have an office of research and standards – the only user fee program that will have a regulatory science component. It will also include an office of bioequivalence with three divisions and a division of clinical review, creating more clinical presence in OGD.
The CDER reorganization and the creation of OPQ is being driven by the need for clear and consistent review and inspection standards and is intended to underscore the importance of the clinical/quality connection, including the increased emphasis that human factors analysis needs to get to help support this connection.
At a PDA conference on quality metrics in early December in Bethesda, Maryland, CDER Office of Strategic Programs Director Theresa Mullin noted that a “basic driver” for the design of OPQ is the desire to have “one program that is consistently applied across all the product types” along with a “focus on clinical performance.”
Central to the effort will be expertise-based standards developed for both reviews and inspections and a team-based approach to pre- and post-approval inspections.
New offices in OPQ, Mullin explained, will focus on: ● product review – defining the clinically relevant product specifications and standards that will be used and applied ● process and facility review – looking at processes andconducting high risk pre-approval inspections with an integrated approach to how the drug was made and where was it being made, and ● surveillance – looking at the inventory of facilities and products to understand how they are made and assess quantitatively how they are performing over their life cycle.
Office of Surveillance to Drive Better Industry Tracking
The CDER official spoke at some length about the Office of Surveillance, which she has played a key role in designing.

MONTHLY UPDATE - JANUARY 2014
WWW.IPQPUBS.COMJANUARY 2014 1�
MONTHLY UPDATE - JANUARY 2014
FDA wants to use these metrics to better target which sites, and which products, processes and systems at those sites, require agency attention, and to decrease the inspection burden on sites where the quality systems are stronger.
Underpinning the metrics development effort are sections 704, 705 and 706 of FDASIA (see IPQ “Monthly Update” May 2013, p. 16). The act calls for FDA to strengthen its electronic system for registration and listing (704) and its risk-based inspection approach (705), and empowers the agency to obtain records in advance or in lieu of inspections (706).
The agency’s outreach to industry for help in identifying appropriate metrics was advanced by a Federal Register notice in February that sought input on how to better predict drug shortages. The notice generated initial feedback on the metrics front from PDA, PhRMA and BIO (see IPQ “Monthly Update” June 2013, p. 12).
At a “CMC Workshop” cosponsored by the Generic Pharmaceutical Association (GPhA) and FDA in early June, CDER Office of Pharmaceutical Science (OPS) Scientific Coordinator, Russ Wesdyk, who is spearheading the metrics effort, fleshed out the agency’s “preliminary” thinking regarding their use and content. (Wesdyk’s complete remarks are provided in the IPQ story cited above.)
Wesdyk met the day after the GPhA meeting with the association’s Executive Committee to gain further input, and has continued to appear at a variety of public forums to continue the dialogue. These have included the ISPE/FDA CGMP conference in June, the PDA/FDA conference in September, the GPhA Fall Technical Conference in October, the ISPE annual meeting in November, and a PDA/FDA workshop focused on metrics in December. The industry/regulator dialogue on metrics continued at an ISPE/FDA “proactive compliance” conference in January.
In response to FDA’s request, written comments came in during the later part of December from PDA, ISPE, the Pharmaceutical Research and Manufacturers of America (PhRMA) and the Consumer Healthcare Products Associ-ation (CHPA). The PDA “points to consider” encompassed the discussions at its December workshop, and the ISPE “white paper,” submitted by its PQLI metrics team, reflected the previous ISPE conference discussions. [Editor’s Note: IPQ will be providing an update on the FDA/industry metrics dialogue in the February “Monthly Update.”]
The surveillance office will be charged with conducting and continually monitoring, assessing and reporting the state of quality of the facilities CDER regulates.
It will begin by “putting together a comprehensive, well-integrated inventory of all the facilities and products – where the facilities are, what they are making, and who they are making the products for, in the case of contract facilities.”
For this inventory of facilities, the intent is to use metrics to be able to predict and analyze the state of quality and look for trends—focusing in particular on specific questions that reviewers may have, Mullin explained.
To enable meaningful collection and analysis of data, the agency’s computer systems will need to be updated and different areas within the agency will need to use common systems.
Mullin characterized the current state of the agency’s systems as “fairly fragmentary,” with “many little component systems,” including access databases and spreadsheets, that have been “hand-crafted” by individuals and departments over the years.
“It sort of speaks to the lack of resources that we have had for a long time in the area of quality oversight,” she said. “We have multiple versions of the truth right now in terms of facilities – who is out there, what they are making, and so on. Some of this information is out of date. We do not have ways to readily update it right now, so we are looking at a variety of ways to really integrate this and make sure that we have one version of the truth.”
The first step will be to ensure that everyone at the agency is accessing the same data, which is “as accurate and up to date as possible” to support pre-market review, post-market quality and regulatory business functions. After that, work-flow management systems and reporting functions can be built.
“We have a number of streams of work on the way to try and standardize data and use the authorities that we have under FDASIA to try and see if we can come up with getting in some sort of more standardized information that at the end of the day will be less burdensome for industry and be more useful in terms of our regulatory oversight. That is where we are going.”
FDA and Industry Confer on Metrics
A component of the FDA effort, guided by the new office, to shift from an inspection to a more flexible surveillance-oriented mode is the development of objective and transparent metrics, and the agency has been dialoguing with industry on what metrics would be viable to achieve its objectives.
DOWNLOAD FROM THE STORY: • FDA Drug Shortages Strategic Plan
[Story continues on p. 17.]


MONTHLY UPDATE - JANUARY 2014MONTHLY UPDATE - JANUARY 2014 MONTHLY UPDATE - JANUARY 2014
JANUARY 2014 1�
INSIDE THE GLOBAL REGULATORY DIALOGUE™
CDER COMPLIANCE DIRECTOR BERNSTEIN ON HER OFFICE’S CURRENT PRIORITIES
At the FDLI enforcement conference in Washington, D.C. in December, CDER Compliance Office Director Ilisa Bernstein provided a review of her office’s current compliance priorities. She discussed: ● quality ini-tiatives ● FDASIA implementation ● the Drug Quality and Security Act ● international collaborations, and ● compliance and enforcement activities and actions.
It was hard when I was putting together the slides for my talk to include all that we have done in CDER in the last year and try to summarize that in ten to fifteen minutes. It was a challenge. But I am going to pick the high notes and try to categorize what we have done into some buckets.
The Office of Compliance, for those of you who are not familiar, has four offices: the Office of Drug Security, Integrity and Recall, which we call ODSIR; the Office of Manufacturing and Product Quality, or OMPQ; the Office of Scientific Investigations; and the Office of Approved Drugs and Labeling Compliance. Each office has a different mission and a different focus. But they are all based on compliance and oversight – ensuring that drugs are safe, effective, and of adequate quality in the United States.
Here is what we have been up to in the last year – just giving you an update: ● We are going to talk about some quality initiatives ● FDASIA implementation ● And as of last week, November 27, 2013, the president signed into law the Drug Quality and Security Act, which covers compounding and supply chain integrity and security. I will tell you a little bit about that and its implementation. ● We are doing a lot internationally, with several collaborations on many fronts across all of the offices in the office of compliance. ● And we have a lot of compliance and enforcement activities and actions. I won’t go into specific ones. But I will tell you the gist of some of the things we have been doing.
Quality Initiatives
In the area of quality, we at FDA, within CDER, are looking at improving our overall approach to regulation of pharmaceutical quality. And we are really looking at taking a comprehensive approach across the center and involving the Office of Regulatory Affairs [ORA] as well. We are planning to make coordinated organizational process and policy changes to move us to our vision for pharmaceutical quality, which would be a global benchmark for the regulation of pharmaceutical quality.
In doing so, within CDER, we are creating an Office of Pharmaceutical Quality [OPQ] (see IPQ “Monthly Update” June 2013, p. 2). That office is going to be pulling in folks from different parts of the center including what was the Office of Pharmaceutical Science [OPS], parts of the Office of Compliance [OC], and parts of the Office of Generic Drugs [OGD] to really pull together all the pharmaceutical quality parts of what we would do for regulating into one office. That is all under development right now in the planning stages. It is moving forward.
What I have listed here are the principles for change – the reasons for what we are doing. One is to really look at ensuring that we have clinically relevant standards across the product lifecycle – really looking at not just manufacturing, but what comes into the review and integrating that review and information into how and when we do our inspections and creating more definitive, clear, transparent standards so industry will know what to expect. It will be very much a team approach. The Office of Pharmaceutical Quality will also be working with the Office of Compliance, which will continue having the key responsibility for compliance and enforcement for products.
We also, within the Office of Compliance, plan on issuing some more clear enforcement policies and compliance policies for industry. We are also looking at using quality metrics in surveillance (see IPQ “Monthly Update” June 2013, p. 12). These are actual metrics that firms already collect and use. We are looking at how we can use those metrics to try and get a better sense of the state of manufacturing and compliance at a particular facility. That is still in the early stages of development. There were some meetings to try and identify what some of the good quality metrics are. What we are really striving for is a comprehensive approach to pharmaceutical quality, compliance, and enforcement.
Additionally in the area of quality we have an increased focus on contracting. In the last year we issued a draft guidance for quality agreements for contract manufacturing, focusing on what is needed (see IPQ “Monthly Update”

MONTHLY UPDATE - JANUARY 2014
WWW.IPQPUBS.COMJANUARY 2014 1�
MONTHLY UPDATE - JANUARY 2014
October 2013, p. 12). We got a lot of comments on that and we are reviewing the comments now (see IPQ “Monthly Update” Nov./Dec. 2013, p. 2).
We are looking at how we can promote modernization and innovation. That is really what FDASIA is all about. It is the FDA Safety and Innovation Act. It is about innovation across the lifecycle of a product. So we are looking at how to promote modernization and compliance with some of these new technologies and innovations, including continuous manufacturing….
Another area we have been focusing on tremendously is shortage prevention and mitigation. A lot of problems that have been happening, and the shortages that have been happening, are because of quality and manufacturing problems at facilities (see IPQ “Monthly Update” March, 2013, p. 2 and Jan./Feb, 2013, p. 22).
We have been working really closely with a lot of the firms that are creating some of the shortages, because we need to get those drugs to patients – this is thinking of and working on shorter term prevention and mitigation. FDASIA Title X has new provisions for drug shortages….
Just last month, FDA issued a strategic plan for drug shortages that focuses not only on short term but also some long term goals for shortage prevention and mitigation. The Office of Compliance was a key player in the development and implementation of that strategy.
FDASIA Implementation
With FDASIA, there are really three titles that impact our office: ● GDUFA, the generic drug user fees (see IPQ e “Monthly Update” Nov./Dec. 2013, p. 2 and September 2012, p. 44) ● the supply chain portion, which is Title VII (sIPQ “Monthly Update” September 2013, p. 44 and May 2013, p. 16) ● Title X, which is drug shortages (see IPQ “Monthly Update” October, 2012, p. 4).
For GDUFA, we have been really ramping up within the Office of Compliance – hiring more people and developing whatever improved processes are needed so that we can meet the GDUFA goals that are kicking into place, including getting rid of the backlog. There has been a huge backlog of ANDAs in the house and we are plowing through to try and break down that backlog.
For supply chain, Title VII, the Office of Compliance is the lead on many provisions. I have summarized here the supply chain provisions, but I am not going to go into any detail because of time. What we have are three types of new regulatory authorities:
● One is to help us get more risk information about products, about manufacturers, and ensure that people havemore information that is actually shared with the public, or it is information that we get, and how we can improve information exchange.
● We also have more authorities to help with the efficiencies of the global supply chain – working with ourregulatory counterparts, moving towards using their inspections, and getting better access to their records before an inspection.
● We also have new tools in our toolkit, which we like (ibid.), and we are moving forward on implementation.
In the last year we published two draft guidances – one focusing on a unique facility identifier, which we call the UFI. That will be a DUNS number. Every facility would have a DUNS number (see IPQ “Monthly Update” May, 2013, p. 16). We also issued a draft guidance defining the circumstances that would constitute delaying, denying, limitingan inspection or refusing entry (see IPQ “Monthly Update” September, 2013, p. 29). We held a public meeting on that one. We also issued a proposed rule for administrative detention (see IPQ “Monthly Update” October, 2013, p. 7). All of those documents are available on our website.
Drug Quality and Safety Act
Just recently, in the last few weeks, the Drug Quality and Safety Act was signed into law. It contains two titles: ● Title I

MONTHLY UPDATE - JANUARY 2014MONTHLY UPDATE - JANUARY 2014 MONTHLY UPDATE - JANUARY 2014
JANUARY 2014 1�
INSIDE THE GLOBAL REGULATORY DIALOGUE™
is compounding, and ● Title II is supply chain, which we call track and trace. That is the new drug supply chain security act provision. It outlines new steps to build an electronic inter-operable system to identify and trace certain prescription drugs as they are distributed through the US.
Personally, I have been working on this for over ten years at the agency, and it is very exciting to see this finally coming to fruition.
It contains a lot of pieces – a lot of guidances, some regulations, public meetings, pilot projects, and standards that need to be done. We are really working hard at moving forward in implementation.
In a nutshell, what this new law will do is every product will have a unique identifier. Every package will have a unique identifier so it can be traced and tracked throughout the supply chain. Certain information will flow about products as they change hands….
Product verification is having systems and processes in place so that if a wholesaler or pharmacy wants to read the number – that unique identifier – they can verify that that number was issued by the manufacturer.
There are detection and response provisions that actually identify what is a suspect product, what is an illegitimate product, what different suppliers in the supply chain need to do in order to respond, and who they need to notify.
There are new provisions that require FDA to set up new wholesale distributor licensing and 3PLs – third party logistics provider licensing programs – as well as set standards. If a state does not have a program that meets the new standards that are established, those wholesalers and 3PLs would be licensed by FDA.
This actually creates, over the next 10 years, a system in which products will be tracked by lot number. But in 10 years they will be tracked by the unique individual ID number. So once we get to ten years there will be item-level tracking. There are some penalties for non-compliance, and also a national uniform policy, which basically says that for product tracing and for wholesale drug distributors there are pre-emption provisions in there as well.
We also announced in the last year a new supply chain pilot that will enable up to one hundred qualified firms to expedite importation of API and drug products into the United States (see IPQ “Monthly Update” September, 2013, p. 24). We are now accepting applications. Get your applications in by December 31st – we are going to move forwardwith the pilot.
In the last year – and you have probably seen in the paper – there have been some counterfeit incidences where products were being sold directly to medical facilities, doctor’s offices, and clinics, and used in patients. So we have been tackling this new distribution scheme as well.
With respect to compounding: Title I covers compounding. But as many of you are aware, over the last year we have been conducting a number of inspections. We conducted 73 inspections of firms. These include risk-based inspections identifying and focusing on firms that make sterile products. And we performed 42 for-cause inspections where there was a problem or potential problem identified (see IPQ “Monthly Update” May, 2013, p. 34).
Many inspections resulted in 483s being issued. We observed serious quality problems including contamination and sterile practices that create a risk of contamination. So there is a lot of information. A lot of this resulted in recalls. And a lot of this information is available on our website.
Title I of the new law removes some of the provisions – the unconstitutional provisions – of 503a, which was passed in 1997 that deals with pharmacy compounding. What it also did is create a whole new category under 503b of the Food, Drug, and Cosmetic Act of outsourcing facilities.
Firms can elect to register to become an outsourcing facility, and then they can qualify for exemptions under the act. They can qualify for exemptions from the drug approval requirements and the adequate directions for use requirements, but they still have to follow GMPs.
There is a lot that needs to be done for 503a and 503b. Last week we issued a number of guidances and Federal Register notices. They are on our website. Please comment.
MONTHLY UPDATE - JANUARY 2014
WWW.IPQPUBS.COMJANUARY 2014 �0
MONTHLY UPDATE - JANUARY 2014
International and Enforcement Efforts
International collaboration: I am not going to go into each of these because of time. But just to say that we are working and reaching out to our international partners on all different areas – for example, GMPs, GCPs and bioequivalence. We are also working with Health Canada on OTC monograph coordination. We are working with a whole bunch of different partners around the world — with PIC/S (the Pharmaceutical Inspection Cooperation Scheme), ICH, APEC, WHO, and others.
We also have our traditional compliance and enforcement activities. Our CGMP program is pretty strong and active. You are probably well aware of the warning letters, untitled letters, and other injunctions and import alerts that we have issued in the last year.
In the last year for the post-marketing enforcement program, authorized under the FDAAA, we took action for failure to perform post-marketing requirements. So we have been actually looking more closely at compliance with post-marketing requirements.
We had a joint program with CFSAN, CDER, and ORA on fraudulent diabetes products. We have issued some warning letters for homeopathics. We are still very interested in looking at homeopathic products.
The unapproved marketing and drug product initiative has been going on for many years. We are trying to get unapproved drugs off the market and bring them in so that they would actually come in and get approval.
And more so in the last year we have been noticing a lot of data integrity problems at firms, so we have been taking a more focused look at data integrity, compliance, enforcement, and prevention (see IPQ “Monthly Update” July/Aug. 2013, p. 32). So that is something you can look for in the next year.
So what is next? This is the same slide you saw at the beginning, but there is a lot more to be done in all of these areas. In the next year you are going to be seeing a lot more of what I have told you about: ● implementation of the DQSA ● more implementation and more documents for FDASIA implementation ● continuing with our compliance and enforcement actions; and ● all of the quality initiatives – you will see a whole lot more from CDER on that as well.
Implementation of DQSA Compounding ProvisionsIn early December, FDA issued the following draft guidances and notices aimed at implementing the compounding provisions of the DQSA.
● Guidance for Industry: Pharmacy Compounding of Human Drug Products Under Section 503A of the Federal Food,Drug, and Cosmetic Act [FDCA] (Draft)
● Guidance for Industry: Registration for Human Drug Compounding Outsourcing Facilities Under Section 503B of theFDCA (Draft)
● Guidance for Industry: Interim Product Reporting for Human Drug Compounding Outsourcing Facilities Under Section503B of the FDCA (Draft)
● List of Bulk Drug Substances That May Be Used in Pharmacy Compounding; Bulk Drug Substances That May BeUsed to Compound Drug Products in Accordance With Section 503A of the FDCA; Request for Nominations
● Bulk Drug Substances That May Be Used to Compound Drug Products in Accordance With Section 5038 of the FDCAConcerning Outsourcing Facilities; Request for Nominations Drug Products That Present Demonstrable Difficulties for Compounding Under Sections 503A and 5038 of the FDCA; Request for Nominations
● List of Drug Products That Have Been Withdrawn or Removed From the Market for Reasons of Safety or Effective-ness: Final Rule (1999)
The use of statistics in PV continues to be one of the most debated aspects of the 2011 FDA PV Guidance. Work alongside FDA representatives and experienced statisticians to interpret and clarify expectations for the use of statistics to plan each stage of the Process Validation lifecycle.
REGISTER TODAY:www.ISPE.org/2014StatisticianForum
A unique opportunity for statisticians to share, discuss, and collaborate in finding optimal approaches to implement
statistical elements within the FDA PV Guidance
Forum Benefits:
• Examinethemeritsandlimitationsoftraditionalandalternatestatisticalap-proachestosupportthelifecycleapproachtoPVwithfellowparticipants.
• Evaluatevariousapproachesandcasestudiesandselectordevelopcom-pliantapproacheswhichbestmeetthespecificdosageformtypeandpro-cess.
• Gaugeyourcompany’sprogressandapproachesascomparedwithothers,includingindustryleaders.
• Identifyvalueaddedconceptsforcontinuedcollaboration.
One of a Kind Event!

NSF-DBA, NSF-Pharmalytica and Becker & Associates are changing their names to NSF Health Scienceson January 1, 2014.
NSF Health Sciences [email protected] www.nsf.org
Testing Auditing Consulting Training
••
•••
C
M
Y
CM
MY
CY
CMY
K
HS - Contract Pharma Ad_1_14_PRINT.pdf 1 1/7/2014 10:18:15 AM

MONTHLY UPDATE - JANUARY 2014 MONTHLY UPDATE - JANUARY 2014 MONTHLY UPDATE - JANUARY 2014
JANUARY 2014 �1
INSIDE THE GLOBAL REGULATORY DIALOGUE™
INTERNATIONALBiotherapeutics Developers Are Wrestling with Challenges of Connecting Quality Attributes to ImmunogenicityThe developers of biotherapeutics are intensifying their efforts to understand the complex relationships between the structure of their molecules and immunogenicity and to expand the predictive power of their CMC toolbox. However, there is also a growing recognition of the long-term nature of the project and the difficulties in validating the quality analytical tools against the less than solid ground of immunogenicity assessments in the clinic.
The connection between the quality attributes of biotech products and their clinical impact is center stage in the industry/regulator dialogue, with implications that extend across the discussions on quality by design, investigational and marketing application filings, manufacturing changes, post-marketing surveillance, and biosimilars (see IPQ “Monthly Update” Nov./Dec. 2013, pp. 44-53).
Tightening the quality/clinical connection is proving to be a particularly daunting challenge in the immunogenicity arena, given the limitations in the clinical assessment capabilities and the lack of a firm foundation against which to validate the CMC methodologies.
The major players in the biotech arena are putting valuable resources into expanding the ability of their quality analytical techniques to assess and predict the structure/immunogenicity relationships and help make better choices in candidate selection and molecule design, while recogni-zing the limitations and gaps in the overall immunogenicity knowledge base and the long-term challenges involved in filling them.
In Basel, Switzerland in September, PDA held a workshop to review the current regulatory expectations in Europe and benchmark best practices on immunogenicity assessments for monoclonal antibodies (MAbs) and what role the CMC analytical toolbox can play in making them.
Included in the opening session on the current regulatory situation in Europe were presentations by two experts that have been heavily involved in framing the relevant EMA guidance – Austria Agency for Health and Food Safety (AGES) Biologics Preclinical Assessment Group Head Gunter Waxenecker and National Institute for Biological Standards and Control (NIBSC) Biotherapeutics Group Head Robin Thorpe.
The two regulators provided valuable insight into the
challenges of immunogenicity assessments in the MAb context and stressed the need to have a carefully crafted clinical strategy to facilitate the approval process for new monoclonals, changes to processes, and for biosimilars (see IPQ “Monthly Update” Nov./Dec. 2013, pp. 31-43).
Thorpe, in particular, cautioned on the danger of relying on immunogenicity predictions and generalizations short of this well-thought-out clinical evaluation, as he explored the lessons he has learned from his involvement at NIBSC in biotherapeutic research, application review, and guidance development.
In the second session, industry experts discussed the work their companies are now doing to try to understand better the linkages between quality attributes and unwanted immunogenicity and increase the power of their in-vitro and in-silico analytical toolbox in molecular engineering and immunogenicity risk mitigation.
Two additional sessions followed on day two of the MAb workshop focused on: ● the analytical challenges of two critical quality attributes with immunogenic potential – protein aggregates and host cell proteins (HCPs), and ● how the immunogenicity issues play out in the development of biosimilars.
Assessing the Value of the Toolbox
Serving as moderator for the second session, Eli Lilly Senior Research Fellow Michael DeFelippis provided a framework for the discussions that followed.
He noted that he has been characterizing the properties of proteins for over 20 years, and that it is “interesting to see how analytical advances have allowed us to find all sorts of degradants and product variants, and even detecting them at really low levels.”
As a CMC scientist, DeFelippis commented, “I am often asked, ‘do they matter?’ What I can usually say is that I can tell you what the species are and where they are in the protein sequence. I can tell you how much is there. I can even give you some insight as to how they got there from a mechanistic standpoint – do they form in cell culture or do they grow on stability? And oftentimes I can isolate some species or even enhance their amounts and do some bioassay determinations and get some bioactivity measurements. But from a CMC

MONTHLY UPDATE - JANUARY 2014
WWW.IPQPUBS.COM JANUARY 2014 ��
MONTHLY UPDATE - JANUARY 2014
in the clinic, and their predictive value can be substantiated. “We invest because we think that in the future we can use all the data we generate at the moment to have an estimate about the predictive power.”
He went on to review the work his team has done in evaluating four of the more relevant analytical techniques – the dendritic cell activation assay, in silico HLA binding prediction, MHC-associated peptide proteomics (MAPPs), and the in vitro T-cell activation assay. The Novartis’ evaluation has included a comparison of the capacities of the assays to each other and their respective correlation with clinical immunogenicity findings.
Validation Difficult Given Clinical Data Vagaries
Spindeldreher concluded with a discussion of the challenges involved in validating the prediction tools and determining their relative value, given the vagaries of the clinical immunogenicity data, particularly in the monoclonal context.
The reported clinical data is highly variable not only because of the different patient populations and concomitant treatments, but also because different assays have been used to produce the data, which have different sensitivity and specificity. The methodology for the same assay may also differ as well as the sample handling, the timepoints of sample collection, and the number of patients tested.
Spindeldreher cited as examples the wide ranges in immunogenicity that have been reported for: Campath (alemtuzumab) – 1.5-75%; Rituxan (rituximab) – 1-65%; Remicade (infliximab) – 10-51%; Humira (adalimumab) – 10-50%; and Zenapax (daclizumab) – 9-34%.
He noted that in one case, a 75% immunogenicity rate was reported. However, a closer look at the data shows that there were only four patients, three of which had immunogenicity – a not statistically significant finding.
The question is how the in vitro data can be correlated with these clinical immunogenicity ranges and what in the variable immunogenicity data is really of concern. “It is not enough to just look at the rates and what is reported,” Spindeldreyer stressed. “You really have to look into the details.”
On the problem of determining what is relevant immunogenicity, he pointed out that some of the assays “are highly sensitive. They measure immunogenicity in a very high number of patients. But most of these signals don’t have any impact. So is it really immunogenicity? Is it measuring something else? Is it relevant immunogenicity? So this is also an issue when we use public domain data.”
perspective, understanding clinical consequences beyond the bioactivity is very difficult.”
The purpose of the session, the Lilly moderator explained, would be to explore where industry currently is in making immunogenicity assessments and addressing the associated risks.
“We are going to take a look at some predictive tools that might be available to help with the assessment, as well as look at new technologies that might be able to optimize the properties to mitigate the risks associated with immunogenicity.”
Predictive Tools Are Long-Term Investment
The lead-off speaker at the session was Novartis Institutes for Biomedical Research Biologics Safety and Disposition Group Lead Sebastian Spindeldreher who focused on the predictive value of the available in silico and in vitro tools in assessing the immunogenic risk for biotherapeutics.
Before addressing the specific tools in the Novartis toolbox and their strengths and limitations in making clinical immunogenicity correlations, Spindeldreher provided some background on why the effort is being resourced and where the focus currently lies.
A lot of time is being invested at Novartis and at other biotech companies on predicting immunogenicity. However, he commented, while “we can predict to some extent a risk for immunogenicity, clearly, as outlined this morning, we are not capable of predicting the real immunogenicity rate at the moment” (see IPQ “Monthly Update” Nov./Dec. 2013, pp. 44-53).
Novartis’ current focus with these analytical techniques “is really on the candidate selection. So if you have 10 different candidates, you compare them in these assays and try to find the one which has lowest signal. And you think this is the one which has the lowest immunogenicity in the clinic as well.”
The predictive work is also done to support protein design. “So the idea, of course, is that we try to incorporate a low immunogenicity profile in the design of the molecules.”
However, a key issue is the need to be “absolutely sure that the predictive power of these tools is at the level where this selection process is leading to the right candidate.”
Investing in evaluating and enhancing the predictive power of the analytical tools, the Novartis expert explained, is a long-term project that will only bear substantial fruit when the methods are applied to many different projects that end up

MONTHLY UPDATE - JANUARY 2014 MONTHLY UPDATE - JANUARY 2014 MONTHLY UPDATE - JANUARY 2014
JANUARY 2014 ��
INSIDE THE GLOBAL REGULATORY DIALOGUE™
Another issue is that the predictive assays and readouts, such as for T-cell assays, are not standardized. “Which of these different methods do you really use in the end, because there is no standard yet?” Also there can sometimes be high variability in the results of the prediction tools, with repeated assays yielding different results.
Europe’s AIBIRISK Project Targets Assessment Gaps
Given all the uncertainities, “a prediction of a concrete immunogenicity rate in a defined patient population may never be possible,” the Novartis official maintained. What is possible is the ranking of candidates according to risk, he said, stressing, however, that “there is still a lot of work to be done” to achieve this goal.
“To really validate these assays clinically we need reliable clinical immunogenicity data. We need additional information on immunological mechanisms. Much has been identified already, so there is a huge knowledge base. But I think there is even more which is not known, and this has to be identified. Then also a systematic cross-comparison of the
available tools is required. Because one company is using assay one and another company is using assay two, and in the end the question is how they would compare.”
Spindeldreher ended by underscoring the importance of an EU project started in March 2012 under the aegis of its European Innovative Medicines Initiative (IMI) called “ABIRISK,” which is working to fill these gaps in the immunogenicity assessment arena. (Information on ABIRISK is available at HTTP://www.abirisk.eu/.)
Following the presentation, Roche’s Schreitmueller commented that another “big gap in principle” in the predictive potential of the assays is that the proteins that are being analyzed have thousands of receptors that can impact the results.
Spindeldreher agreed with the point, noting, however, that “there are different ways to overcome” the impact of the structure and mode of action on the assays. The issue would have been “too much to go into” during his talk, he said, reiterating that his central concern was “that if you don’t
COMPLICATING FACTORS IN IMMUNOGENICITY ASSESSMENT
At the PDA Europe MAb immunogenicity workshop, AGEs’ Waxenecker provided the following depiction of the complicating factors in immunogenicity assessment. He annotated the pieces of the puzzle as follows: ● We have CMC changes ● We have immunogenicity assay for drug sub-stance, for normal proteinaceous excipients, or for drug product ● We didn’t talk about the T-cell response – we know it is super-relevant, but we don’t have real good assays that help us in this regard ● We talked about preexisting immunity or false positive results ● Assay sensitivity and drug interference ● IG or mucosal immunity might be another issue that may be detected in the frame of clinical development ● And usually the duration of immunogenicity testing for chronic treatment is not sufficiently long and explored in the frame of clinical studies – so there is a strong need for the pharmacovigilence activities ● And don’t forget to prepare the background data that are relevant in the indication.
Correlation of immunogenicity with
T-cell response
Assay sensitivity
Duration of Imm. testing
Preexisting Immunity?
IgE / mucosal immunity? Background
data
CMC changes
Imm.Assay for DS,
excipient, DP?

MONTHLY UPDATE - JANUARY 2014
WWW.IPQPUBS.COMJANUARY 2014 ��
MONTHLY UPDATE - JANUARY 2014
of three of the analytical approaches, and ● the conclusions from the assessment. (Quarmby’s remarks are provided below.)
Immunogenicity understanding is informed by the “tremendously elegant” analytical characterization data and the animal study data at a firm’s disposal along with the information from its risk-based assessment. However, while companies like Genentech have “lots” of information and tools, “we really don’t have anything that is going to enable us to do definitive decision making.”
The variety of “immunogenicity prediction tools and technologies out there that are used in molecular design, and sometimes in lead optimization too” led her group at Genentech “to start to wonder if it was possible to use any of these as risk-ranking tools to enable data-driven decision making on relative risk assessments for immunogenicity of the monoclonal antibody therapeutics.”
“We wanted to actually generate data around this. There is a lot of speculation around the utility of these tools, but there is very little in the way of clinical validation for any of them. So we wanted to generate a data set to look critically, not at any one of them, but actually across a range of different methods.”
In her presentation, Quarmby discussed three of the test systems that have been evaluated – the PBMC-derived T-cell activation assay, the human artificial lymph node (ALN) system, and a transgenic mouse model – and the mixed results of those evaluations.
While these tools and others that have been developed for lead identification can be used to do some sample ranking, Quarmby summarized, “I think we need a lot more data to really clarify how you make a link, or if indeed you can make a link, to rankings from these tools and what really happens in the clinic. There are many, many additional variables that you have to take into account when you go into clinical trial populations – disease states, background genetics and so forth – that these models really don’t bring to bear at all.”
Echoing Novartis’ Spindeldreher and the cautionary note sounded by NIBSC’s Thorpe during the previous regulator session, she stressed that, while “this is a very important, really interesting area,...it is an area where I think with these models we have to proceed with caution until we have better clinical validation data or a better understanding of the limitations, if you will, around what the data from the systems really means.”
have reliable clinical data to compare the in vitro data with, how would you ever know which method is the best one?”
Genentech’s Review Also Shows Prediction Limitations
Presentations followed by Antitope’s Frank Carr and Full Spectrum Genetics Bob DuBridge on the work their respective companies are doing in the field of protein engineering to minimize immunogenicity.
Relevant to Shreitmuller’s comment on the predictive challenges that complex molecules present, DuBridge reviewed the “MapEng” platform his company has developed for quantifying the binding properties of large numbers of molecular variants, which provides a “comprehensive” 2D map for engineering and de-immunizing proteins and peptides. He explained the use of the 2-D genetic mapping to understand the variants in Avastin and calculate their relative binding efficiency, and more recently to help select non-immunogenic variant Humira molecules with similar affinity and bioactivity.
Genentech Bioanalytical Science Director Valery Quarmby was next at the podium, giving a talk that was similar in scope and thrust to Spindeldreher’s.
She provided an overview of the challenges of assessing immunogenicity risks in biotherapeutic development and how Genentech is working to meet those challenges. The talk was informed by Quarmby’s involvement in the development of several of Genentech’s prominent biotech products.
In her presentation, she explained why immunogenicity “is a very high profile concern for those of us who are in industry as well as for the regulatory authorities,” and what firms like hers are doing to lower the risks. It is a concern, she noted, that is heightened as more biotherapeutics are developed for chronic use.
“There are many implications to immunogenicity,” she pointed out, and, as such, “it is done in a highly cross-functional manner.”
Quarmby’s remarks at the session encompassed: ● why immunogenicity testing is important ● howthe immunogenicity profile is developed ● the available data on immunogenicity rates ● the various consequences of immunogenicity ● the critical quality attribute/immunogenicity relationship ● assessment and prediction prior to clinicals ●a study by Genentech/Roche of the predictive value
[Story continues on p. 25.]
You Can Count On Our Expertise To Realize Your Goals.
We help put your plan in motion… And then we f inish it with you.Our unique focus is helping you meet your development and commercialization needs by bringing your product to market quickly and successfully, while maximizing the expertise and resources you already have on board. With decades of experience and involvement in dozens of products that have been filed and approved in the United States and across the globe, we’re the experts you need to shape and execute your biopharmaceutical manufacturing and CMC needs.
Contact us for the resources to start delivering on your goals.Peter Dellva: (847) [email protected]
Or Visit: www.biotechlogic.comwww.processvalidation.com
Our approach is tailored to meet the requirements of your project. We can integrate into your development efforts, augment your team resources, or provide hands-on support.Our areas of expertise include:
Our success has been our ability to serve as your technical expert and be the additional resource that helps you drive and execute your plan.
Process Validation Regulatory Submissions Quality Assurance

MONTHLY UPDATE - JANUARY 2014MONTHLY UPDATE - JANUARY 2014 MONTHLY UPDATE - JANUARY 2014
JANUARY 2014 ��
INSIDE THE GLOBAL REGULATORY DIALOGUE™
GENENTECH’S QUARMBY ON ASSESSING IMMUNOGENECITY RISKS DURING BIOTHERAPEUTIC DEVELOPMENT
This has been a terrific conference already, and I am looking forward to the rest of the day and also to tomorrow. It is a very timely conference on a very pressing topic. And it is really exciting for me to be in Europe and meet with a lot of the subject matter experts in this area and learn from their presentations.
So I am going to talk about assessing immunogenicity risk in the context of biotherapeutic development this afternoon. By way of introduction, and I think you have heard similar introductions from several of the speakers:
In the context of biopharmaceutical development, immunogenicity really refers to the production of an unwanted immune response directed against a therapeutic. So we are in a very different context here than in the vaccine world where this is really what one is trying to elicit.
The hallmark of immunogenicity is the presence of host antibodies directed against a therapeutic. These are typically called anti-therapeutic antibodies (ATA), anti-drug antibodies (ADA), human anti-human antibodies, human anti-chimeric antibodies – there are a number of different acronyms, but they all really mean about the same thing.
Why Test for Immunogenicity?
One of the reasons that we are so interested in this area is that there can be clinical consequences to these unwanted immune responses. So we look for immunogenicity. It is a very high profile concern for those of us who are in industry as well as for the regulatory authorities.
Certainly immune responses can impact safety and/or efficacy of biotherapeutics. Especially as we develop more biotherapeutics for chronic use, the need to understand what the types of immune responses one sees for chronic use and what their clinical implications are is something that is of ongoing interest for many of us.
Immunogenicity strategies and the resulting data from these actually end up in many different components of filings. For us they start out sometimes even in our target product profiles as we are beginning the development of a new biotherapeutic program.
Certainly we will have information about our immunogenicity strategy, what we have seen in our animal models, in our IND filings. And we are generating data all the way through CTDs and into Phase IV studies as well as we go into new indications. And so we are constantly looking to see if our biotherapeutics are eliciting unwanted immune responses.
Certainly the health authorities require that immunogenicity of biotherapeutics be evaluated. So it is definitely something that we put a lot of time and effort that we put a lot of time and effort into. And I will tell you a little about some of the work that we have been doing at Genentech in this area in my presentation.
Developing the Immunogenicity Profile
So this just shows a sort of classic, if you will, timeline for biotherapeutic development. Starting with late stage research, going into animal studies, Phase I, Phase II, Phase III clinical trials, into regulatory filings and the post-marketing space, we are constantly looking at immunogenicity.
At the PDA Europe workshop, Genentech Bioanalytical Science Director Valerie Quarmby provided an over-view of the challenges of assessing immunogenicity risks in biotherapeutic development and how Genen-tech is working to meet those challenges. The following are the sections of her talk in which she addressed: ● why immunogenicity testing is important ● how the immunogenicity profile is developed ● the availabledata on immunogenicity rates ● the various consequences of immunogenicity ● the critical quality attribute/immunogenicity relationship ● assessment and prediction prior to clinicals ● a study by Genentech/Roche of the predictive value of three of the analytical approaches, and ● the conclusions from the assessment. Some of Quarmby’s description of the details of the assessment is not included as indicated by ellipses.

MONTHLY UPDATE - JANUARY 2014
WWW.IPQPUBS.COMJANUARY 2014 ��
MONTHLY UPDATE - JANUARY 2014
As a molecule comes out of research and into the early development space, we do a highly cross-functional risk-based assessment, where we look at the molecule, we look at the indication, the context it is going into, and we try and determine whether or not this is a low, medium or a high risk molecule. And we will design our methods, our strategies, and so on, accordingly.
As we move into our animal studies and finally into the clinic as well, we are also doing a lot of immunogenicity testing. We are looking at immunogenicity in our phase I, II and III clinical programs, generating data study-by-study.
By the end of our program, we will actually have a really quite detailed data package on the immunogenicity profile of our biotherapeutic in a particular indication. That information will go, both in an integrated way as well as in the context of information from individual clinical study reports, into our filing. And information on this also goes into product inserts, SmPCs and so on and so forth. So there are many implications to immunogenicity, and it is done in a highly cross-functional manner.
Immunogenicity Rates
So this data summarizes listings of immunogenicity fields, if you will, from US product inserts for monoclonal therapeutics (see box below). We have listed from left to right here: the product, what the target is, what type of molecule this is – whether it is chimeric, humanized, human and so forth; what type of molecule design; the year this was approved; the ATA or anti-therapeutic antibody incidence that is reported on the label; and also the company that generates the molecule. You can see that there is range of different incidences here. With the earlier molecules, murine and chimeric molecules, ATA incidences were as you might expect, quite high. We have gone into humanized technologies – those have dropped somewhat.
But even as people have pointed out earlier on today, with human monoclonal therapeutics, we don’t get down to 0. And that is not entirely surprising. If you look at immune response rates to other fully human molecules, growth
rhuMAb Therapeutics: Immunogenicity Data in Product Inserts
P roduct A ntigen Form Fc A pproved ATA (% ) C om panyO K T 3 C D 3 m urine IgG 2a 1986 86 J & J
R eoP ro IIb IIIa ch im eric Fab 1994 6-44 C entocorR ituxan C D 20 ch im eric IgG 1 1997 1 & 5 G enentech
R em icade T N F a ch im eric IgG 1 1998 10 C entocorS im ulect C D 25 ch im eric IgG 1 1998 1 N ovartis
E rb itux E G FR chim eric IgG 1 2004 5 Im cloneZenapax C D 25 hum anized IgG 1 1997 14-34 R ocheS ynag is R S V hum anized IgG 1 1998 1-2 M edIm m une
H erceptin H E R 2 hum anized IgG 1 1998 <1 G enentechM ylo targ C D 33 hum anized IgG 4 2000 0 W yethC am path C D 52 hum anized IgG 1 2001 2 G enzym e
Xola ir IgE hum anized IgG 1 2003 <1 G enentechR aptiva C D 11a hum anized IgG 1 2003 6 G enentechTysabri a lpha4 hum anized IgG 4 2004 10 B iogen IdecAvastin V E G F hum anized IgG 1 2004 <1 G enentech
A ctem ra IL-6 hum anized IgG 1 2010 3-9 R ocheH um ira T N F hum antransgen ic IgG 1 2002 5 A bbottVectib ix E G FR hum antransgen ic IgG 2 2006 4 A m gen
B enlysta B A FF hum an IgG 1 2011 5 H G S /G S K
C im zia T N F a hum anizedP E G -Fab '
xx 2008 8 U C B
A dcetris C D 30 ch im eric A D C IgG 1 2011 7 S eattle G enetics

MONTHLY UPDATE - JANUARY 2014MONTHLY UPDATE - JANUARY 2014 MONTHLY UPDATE - JANUARY 2014
JANUARY 2014 ��
INSIDE THE GLOBAL REGULATORY DIALOGUE™
hormone, insulin, those also are able to generate quite robust responses in hosts. We do see immune responses to, basically I would say, all of the monoclonal therapeutics that are out there in the marketplace. It is something that we look at very carefully in drug development too.
The Consequences
The consequences of immunogenicity vary tremendously. In some cases you can see a signal in a very sensitive anti-therapeutic antibody assay, and there are no clinical consequences that you can link to that. In other cases, you may be able to link the appearance of anti-therapeutic antibodies to changes in the pharmacokinetic properties of your molecules, changes in efficacy, changes in safety (see box at right).
From the PK standpoint, you can have antibodies that bind to your therapeutic protein and actually modify its terminal half-life. In the case of monoclonal therapeutics, these typically accelerate the clearance of the monoclonal.
However, in the case of other types of therapeutic proteins, growth hormones, and insulin, your anti-therapeutic antibodies can act like a binding protein and actually prolong the terminal half-life of the molecule. So you can find the PK of your molecule a little bit challenging to manage in that case.
Certainly you can see impacts of unwanted immune responses on efficacy as well on safety. A couple of folks have already alluded to the fact that you can have anti-therapeutic antibody responses that functionally neutralize your therapeutic. You can see then loss of efficacy. A classic case of that is with Tsabri and with some of the beta interferons as well, where if you develop an immune response, a subset of patients actually have neutralizing antibodies, which can cause basically a loss of efficacy, which in the case of multiple sclerosis is typically seen by shifts in relapse rates.
You can also see impacts on unwanted immune responses on safety. Hypersensitivity is one area where clearly we look very carefully. The cetuximab story was already mentioned earlier today. And again there are other possible safety implications – immune complex formation being another.
So there are many potential impacts of unwanted immune responses. And again we look at these very carefully in biotherapeutic development.
Relationship to Critical Quality Attributes
As we are developing a biotherapeutic, concurrently our CMC colleagues are actually developing their manufacturing process, formulation, and so on.
What they are doing at the same time is developing not only the processes and the product, they are also developing a set of control systems. And as they are doing all of this, they are trying to understand for a number of different
facets of the molecule that they are developing, whether or not those facets of the molecule should be controlled by the control system.
So they do what is called a CQA or critical quality attribute assessment early on. This is done very early as soon as a molecule comes into early development.
Impact of Immunogenicity on Biotherapeutic DevelopmentClinical Impact Clinical Outcome
Safety �
�
�
Hypersensitivity or anaphylactic reactions
Neutralize activity of endogenous counterpart with unique function causing deficiency syndrome
Immune complex formation
Efficacy �
�
�
Neutralize activity of therapeutic protein
Increase or decrease efficacy by extending or curtailing half life
Increase or decrease efficacy by changing bio-distributionPharmacokinetics �
�
�
Extend, or curtail half life
Alter biodistribution
PK changes may dictate changes in dosing
None � No discernible impact
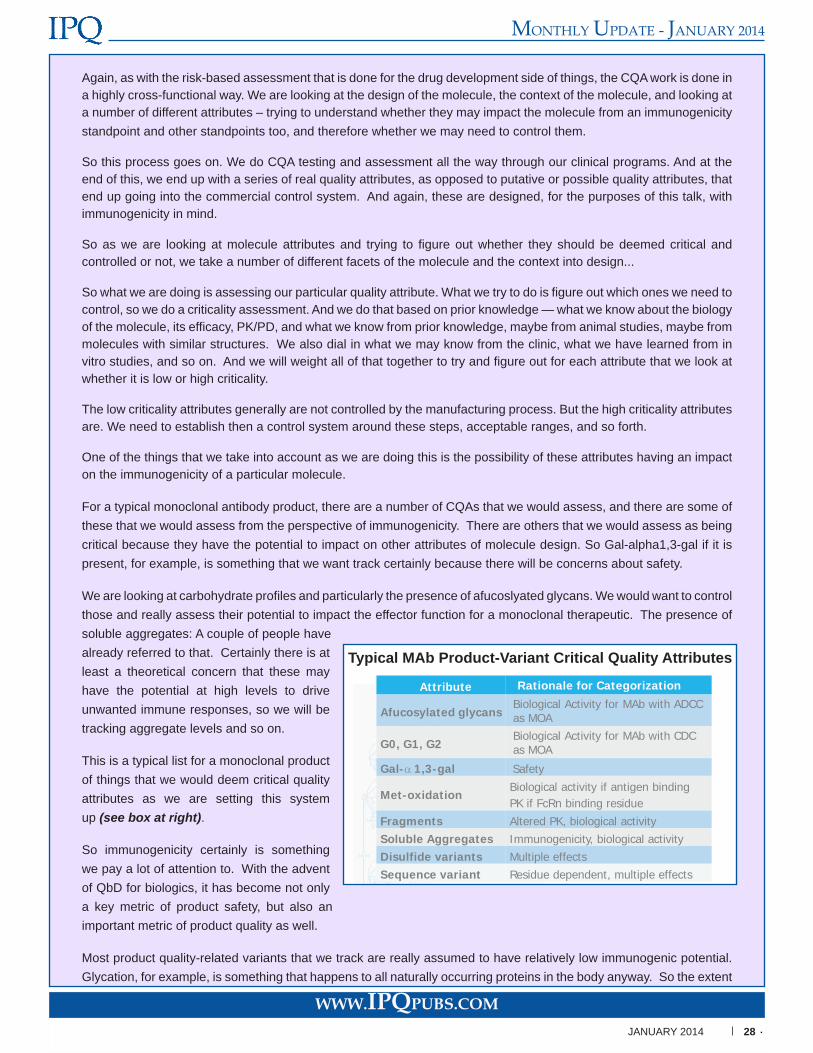
MONTHLY UPDATE - JANUARY 2014
WWW.IPQPUBS.COMJANUARY 2014 ��
MONTHLY UPDATE - JANUARY 2014
Again, as with the risk-based assessment that is done for the drug development side of things, the CQA work is done in a highly cross-functional way. We are looking at the design of the molecule, the context of the molecule, and looking at a number of different attributes – trying to understand whether they may impact the molecule from an immunogenicity standpoint and other standpoints too, and therefore whether we may need to control them.
So this process goes on. We do CQA testing and assessment all the way through our clinical programs. And at the end of this, we end up with a series of real quality attributes, as opposed to putative or possible quality attributes, that end up going into the commercial control system. And again, these are designed, for the purposes of this talk, with immunogenicity in mind.
So as we are looking at molecule attributes and trying to figure out whether they should be deemed critical and controlled or not, we take a number of different facets of the molecule and the context into design...
So what we are doing is assessing our particular quality attribute. What we try to do is figure out which ones we need to control, so we do a criticality assessment. And we do that based on prior knowledge — what we know about the biology of the molecule, its efficacy, PK/PD, and what we know from prior knowledge, maybe from animal studies, maybe from molecules with similar structures. We also dial in what we may know from the clinic, what we have learned from in vitro studies, and so on. And we will weight all of that together to try and figure out for each attribute that we look at whether it is low or high criticality.
The low criticality attributes generally are not controlled by the manufacturing process. But the high criticality attributes are. We need to establish then a control system around these steps, acceptable ranges, and so forth.
One of the things that we take into account as we are doing this is the possibility of these attributes having an impact on the immunogenicity of a particular molecule.
For a typical monoclonal antibody product, there are a number of CQAs that we would assess, and there are some of these that we would assess from the perspective of immunogenicity. There are others that we would assess as being critical because they have the potential to impact on other attributes of molecule design. So Gal-alpha1,3-gal if it is present, for example, is something that we want track certainly because there will be concerns about safety.
We are looking at carbohydrate profiles and particularly the presence of afucoslyated glycans. We would want to control those and really assess their potential to impact the effector function for a monoclonal therapeutic. The presence of soluble aggregates: A couple of people have already referred to that. Certainly there is at least a theoretical concern that these may have the potential at high levels to drive unwanted immune responses, so we will be tracking aggregate levels and so on.
This is a typical list for a monoclonal product of things that we would deem critical quality attributes as we are setting this system up (see box at right).
So immunogenicity certainly is something we pay a lot of attention to. With the advent of QbD for biologics, it has become not only a key metric of product safety, but also an important metric of product quality as well.
Most product quality-related variants that we track are really assumed to have relatively low immunogenic potential. Glycation, for example, is something that happens to all naturally occurring proteins in the body anyway. So the extent
Typical MAb Product-Variant Critical Quality Attributes
Attribute Rationale for Categorization
Afucosylated glycansBiological Activity for MAb with ADCCas MOA
G0, G1, G2Biological Activity for MAb with CDCas MOA
Gal-α 1,3-gal Safety
Met-oxidationBiological activity if antigen binding PK if FcRn binding residue
Fragments Altered PK, biological activitySoluble Aggregates Immunogenicity, biological activityDisulfide variants Multiple effectsSequence variant Residue dependent, multiple effects

MONTHLY UPDATE - JANUARY 2014MONTHLY UPDATE - JANUARY 2014 MONTHLY UPDATE - JANUARY 2014
JANUARY 2014 ��
INSIDE THE GLOBAL REGULATORY DIALOGUE™
to which a monoclonal therapeutic gets glycated is unlikely, we believe, to be pivotal in driving an immune response.
But some product-related variants and certainly process-related impurities at least theoretically could lead to an increase in the risk of immunogenicity. So again these are things that we do look at more actively. Aggregates, sequence variants, the presence of unwanted host cell proteins, LPS, and CpG DNA in the case eColi-derived products are all things that certainly have the potential to impact on the likelihood of an unwanted immune response.
Assessment Prior to Clinicals
When we have a new molecule and indeed a new process, how do we assess immunogenicity risk prior to first in human studies? What do we really have at our disposal to make those decisions?
We have a lot of data actually. For example, going into an IND filing, we will have a whole comprehensive package of
IND-enabling analytical characterization data – tremendously elegant data on amino acid sequence analysis, higher order structure, LC, MS, and so on.
And although we can characterize monoclonal therapeutics in a lot of detail, they do show a great deal of microheterogenicity. So it is impossible to definitely characterize 100%, if you will, of the molecules that are present in a particular product.
We will have a lot of IND-enabling animal study data as well. Even though we look at immunogenicity in our animal studies, what we learn from those studies does not inform the extent to which we are likely to see an immune response in the clinic. Because I think it is generally recognized now that usually data from animal studies is not truly predictive.
“Tremendously elegant” analytical characterization data along with animal study data and information from the firm’s risk-based assessment.
We will have information from a risk-based assessment as well. And so we have a lot of information, but we really don’t have anything that is going to enable us to do definitive decision making, which I think Sebastian alluded to earlier on today. There are lots of tools, but none of it really gives us definitive information.
There are a lot of immunogenicity prediction tools and technologies out there that are used in molecular design, and sometimes in lead optimization too. And so we started to wonder if it was possible to use any of these tools as risk-ranking tools to enable data-driven decision making on relative risk assessments for immunogenicity of the monoclonal antibody therapeutics.
I will run through this slide very quickly because Sebastian very nicely went through a similar slide earlier on. The kinds of tools that are out there are in silico tools to look at the presence or absence of T-cell epitopes. There are also in vitro binding assays to look at the ability of possible T-cell binding peptides to interact with MHC to form binding complexes. There are in vitro assays to look at T-cell activation of PbMC-derived and dendritic cell-derived systems. And there are also some in vivo models that can be used for this purpose, including some engineered mouse models – BLT mice, transgenic mice and so on.
Evaluation of Three Methods
So we wondered to what extent these systems could be used to assess immunogenicity risk from a CQA and product quality standpoint. We wanted to actually generate data around this. There is a lot of speculation around the utility of these tools, but there is very little in the way of clinical validation for any of them. So we wanted to generate a data set to look critically, not at any one of them, but actually across a whole range of different methods.
So we embarked on a program to create a panel of study samples. We picked a particular monoclonal therapeutic with an IgG1kappa consensus framework. It is a lyophilized drug product. It has been used in the clinic. It was given by sub-cutaneous delivery, which is always very interesting from an immunogenicity standpoint. And we actually have a very robust data set from clinical studies, so we sort of know what the answer is, if you will, for unmodified drug product
MONTHLY UPDATE - JANUARY 2014
WWW.IPQPUBS.COMJANUARY 2014 �0
MONTHLY UPDATE - JANUARY 2014
going into the clinic.
We created a test panel from this molecule using extreme temperatures. And we then went to size exclusion chromatography fractionate. And the idea here is to create a panel of preparations that are highly enriched for monomer, dimer, and high molecular weight aggregates, along with excipient control and the reference material control – the reference material control being very much analogous to what went into patients in the clinic.
So these panel samples were all created and then labeled in a coded manner. Actually we had a blinded replicate in there as well. So a very useful data set. What we wanted to do then was run these samples in a number of different test systems. We also wanted to characterize them. We have done a lot of characterization work. This just shows you one data set, SEC-MALS.
So to look again at the size distributions of the particular preparations that we used: You can see over here the monodispersed monomers. You can also see reference material. You can see that our dimer preparation is highly enriched for dimers, but there is some monomeric material present. You can also see that that has a lot of high molecular weight material and a small amount of other material too.
So we characterized these samples a number of different ways. The idea was to do a lot of analytical characterization work on them, but also some biological characterization work on these too, so we could truly understand what we were putting into our systems.
So we have data from a number of different test systems. I am going to discuss three of those test systems just very briefly today.
We put our samples into a PBMC-derived T-cell activation assay. Methods of this type have been described already by a couple of the speakers, so I won’t spend a lot of time on this….
[In reviewing the results,] what is really interesting is that we are not really seeing a very marked impact of high molecular weight aggregation or dimer actually on T-cell activation in this particular system. This is rather different than a lot of data in the literature on high molecular weight aggregate material that has been created in different ways…..
We believe that we could likely use this system to compare the ability of each sample to drive a response to an appropriate control – so for ranking. But we don’t think we can use this to absolutely predict what we would see in the clinic.
What is also interesting about the data set is that it does suggest that filtration or removal of subvisible particles in this particular situation at least has no impact on our responder rates. The sample type that we used – aggregates, dimers – don’t seem to make any difference. In this system, with this monoclonal, there is no impact of aggregation on T-cellactivation. As I mentioned already, the data is somewhat different from published information, where at least some types of aggregation do seem to have quite a profound impact on T-cell activation.
I am going to move on and talk very briefly about the other systems that we looked at. One of them is the human artificial lymph node [ALN] system…. The nice thing about this system is that you can use a longer term exposure to PBMC-derived population cells. So you can do repeated exposure with your antigen of choice….
We did not see a lot of useful data [from the study. There was] a lot of noise in the system, but really no systematic trends that we could see, and no evidence that we could find of antigen-specific ATA output from either the donor or the other systems that we looked at. Data from this analysis wasn’t consistent enough to allow us to assess the impact of sample type.
So the third system, which is a transgenic mouse model that we used: This was developed actually by colleagues here in Basel. The idea here is to develop a set of transgenic mice that express not just one particular monoclonal therapeutic, but actually express a mini-repertoire of human heavy and light chains, so that they are tolerant to actually a series of monoclonal therapeutics that are based on a particular heavy and light chain configuration….
The challenge with this system is really that the ranking abilities are limited by the mouse cohort size – so unlike with
For subscription and sponsorship information visit IPQpubs.com or contact Wayne Rhodes — [email protected], Tel: �0�-��1-���0.

MONTHLY UPDATE - JANUARY 2014MONTHLY UPDATE - JANUARY 2014 MONTHLY UPDATE - JANUARY 2014
JANUARY 2014 �1
INSIDE THE GLOBAL REGULATORY DIALOGUE™
the T-cell assay where you can take samples from 50 donors or 100 donors [and] can do a reasonable amount of ranking. When you just have a relatively small number of mice it is harder to do the…ranking. Of course both of these scales are very different to what we would do in a phase III clinical program where we are into thousands of patients, or in the real world where we are into hundreds of thousands of patients.
So again, I think there is some utility to these systems, but they all I think have their limitations.
Conclusions
Certainly in conclusion, immunogenicity is a key metric of product safety. It is now also a very important metric of product quality. Immunogenicity assessment in the context of biotherapeutic product and process development is multi-faceted. It is really highly nuanced. It is a really interesting area.
The tools that have been developed for lead identification can be used to do some sample ranking. But I think we need a lot more data to really clarify how you make a link, or if indeed you can make a link, to rankings from these tools and what really happens in the clinic. There are many, many additional variables that you have to take into account when you go into clinical trial populations – disease states, background genetics and so forth – that these models really don’t bring to bear at all.
So I think, again, this is a very important, really interesting area, but it is an area where I think with these models we have to proceed with caution until we have better clinical validation data or a better understanding of the limitations, if you will, around what the data from the systems really means.
IPQ wishes to thank the following sponsors:
For subscription and sponsorship information visit IPQpubs.comor contact Wayne Rhodes — [email protected], Tel: �0�-��1-���0.
EXHIBITION: APRIL 7-8 POST-CONFERENCE WORKSHOP: APRIL 9-10
COURSES: APRIL 10-11
www.pdaannualmeeting.org
Biopharmaceutical and Sterile Manufacturing – Embracing Innovation to Meet Global Challenges
April 7-9, 2014 | JW MARRIOTT SAN ANTONIO HILL COUNTRY | SAN ANTONIO, TEXAS
PDA’s premier event, the 2014 PDA Annual Meeting will provide you with a one of a kind learning opportunity. This year the series of parallel sessions, a key and well liked feature of the annual meeting, will focus on issues and challenges related to Biological Sciences, Product Manufacturing, and Quality Systems as well as valuable peer-to peer networking events among many other benefits. Look no further than this must attend meeting, which has much to offer and will provide an excellent forum for learning and discussing recent innovations and interacting with industry and regulatory experts.
For the first time, this year’s agenda is filled with leading FDA experts:
Thomas Arista, Investigator,
CDER, FDA
Kalavati Suvarna, PhD, Microbiologist,
CDER, FDA
Karen Takahashi, Senior Policy
Advisor, CDER,
FDA
Alex Viehmann, Operations
Research Analyst,
CDER, FDA
Following the conference, there will be a post-conference workshop, PDA Biofilm and Bioburden Workshop on April 9-10. The workshop will provide the latest
science and best practices around microbial control for the pharmaceutical manufacturing environment. Presentations will be provided by technical experts from academia, industry, and FDA.
From April 10-11, the PDA Training and Research Institute will host six in-depth training courses. These courses for professionals involved in developing and manufacturing quality pharmaceutical products will cover a
range of topics from implementation of quality risk management to process validation and verification.
The PDA Training and Research Institute presents the...
What Are You Waiting For? Register Today!

Visit www.pdaannualmeeting.org/courses for more information and to register.
COURSE SERIESApril 10-11, 2014 | JW MARRIOTT SAN ANTONIO HILL COUNTRY | SAN ANTONIO, TEXAS
Biosimilars – Understanding the CMC Challenges of Meeting ‘Similarity’ – New Course (April 10)
Understand what the developing FDA biosimilar pathway might look like by examining the existing regulatory guidelines from the European Medicines Agency (EMA) and the World Health Organization (WHO).
Risk Based Product Development Basics for Combination Products: Harmonizing Design Controls and Quality-by-Design in Product Development and Market Authorization Development and Market Authorization Documents – New Course (April 10)
Gain a better understanding of combination product requirements and be prepared to streamline the transfer of knowledge from product development to regulatory submissions at their companies.
Implementation of Quality Risk Management for Commercial Pharmaceutical and Biotechnology Manufacturing Operations (April 10-11)
Learn to utilize the principles of quality risk management to strengthen the decision-making process and aid in allocating resources in a rational way.
Process Validation and Verification: A Lifecycle Approach (April 10-11)
Come away with an up to date understanding of the process validation strategies and approaches are consistent with current regulatory and quality system thinking.
Validation of Moist Heat Sterilization Processes: Cycle Design, Development, Qualification and Ongoing Control (April 11)
Learn more about sterilization science and apply it to the selection of a cycle design approach, process performance qualification and more.
Quality Control and Quality Assurance of Cell-Based Therapeutic Products (April 11)
Discover quality control testing for both in-process testing and for product release, including tests for purity, potency, reproducibility, and methods development considerations.
The PDA Training and Research Institute presents the...
Don’t miss these six courses hosted by PDA TRI immediately following the 2014 PDA Annual Meeting.

MONTHLY UPDATE - JANUARY 2014
WWW.IPQPUBS.COM JANUARY 2014 32
MONTHLY UPDATE - JANUARY 2014
Updates in Brief
CMC/REVIEW
FDA Announces Five-Year IT Plan In order to meet the goals of the 2012 Generic Drug User Fee Act (GDUFA), FDA has announced a five year plan to update its IT system. Under the plan, the agency will publish a provisional data standards catalog and draft guidance requiring electronic submission of standardized data by 2015. [See IPQ story on pp. 13-20 for more on GDUFA implementation.]
GMP/INSPECTION
FDA Reports Drug Shortage Decline to Congress
The first annual FDA report to Congress on drug shortages indicates a clear reduction in new shortages during the first three quarters of 2013. The reduction follows the granting of additional tools to FDA by FDASIA in 2012 and an executive order in mid-2013. [See the CDER compliance priority story on pp. 13-20 for more on the drug shortage effort.]
FDA Accredits GS1 and HIBCC to Issue Unique Device Identifiers
GS1 and HIBCC have been named by FDA as two of the organizations able to assign Unique Device Identifiers (UDI). The UDI rule, issued in September 2013, requires the label of medical devices, including combination products that contain devices, to include a UDI. The labeler must submit product information concerning devices to FDA’s Global Unique Device Identification Database (GUDID).
USP Proposes Revision on Temperature Control During Storage and Distribution
USP has published a “stimuli article” in its Pharmacopeial Forum (PF) proposing revision of the current USP chapter regarding the temperature at which specific pharmaceutical products can be distributed and stored. Current stability studies, the PF article maintains, support significantly widening the range to 2-30º C from 15-25º C or 20-25º C.
UNITED STATES
EUROPE
CMC/REVIEW EMA Calls for Reflection Paper on Biosimilar Quality Statistics
EMA is asking its stakeholders for a reflection paper that will highlight some of the statistical issues of concern regarding biosimilars. The agency is looking, in particular, for how statistical principles should be applied in the regulatory assessment of biosimilar quality. For situations where a meaningful set of critical quality attributes (CQAs) can be identified, EMA suggests that the paper should give an overview of what statistical methods for comparison are available, and which of those might be preferred under which circumstances. GMP/INSPECTION
Revision of GMP “Orange Guide” Issued by MHRA
The UK’s Medicines and Healthcare products Regulatory Agency (MHRA) released a revision of its GMP “Orange Guide” in January that incorporates the changes made to EU’s GMP Guide in the wake of the Falsified Medicines Directive (FMD). Included are new chapters regarding brokers of finished medicines and active substance manufacturers, distributors and brokers, along with a new appendix of names and addresses of other EU medicines regulators. [See IPQ Monthly Update July/August 2013 pp. 16-21 for more on the impact of the FMD on the MHRA/EU GMPs.]

MONTHLY UPDATE - JANUARY 2014 MONTHLY UPDATE - JANUARY 2014 MONTHLY UPDATE - JANUARY 2014
JANUARY 2014 33
INSIDE THE GLOBAL REGULATORY DIALOGUE™
EMA Launches New Version of EudraGMDP Database
EMA announced in December its launch of a new version of the EudraGMDP database which includes, among other changes, the publication of statements of non-compliance with EU GMPs, along with the list of companies that have been issued GMP certificates. [See IPQ Monthly Update Jan./Feb. 2013, pp. 48-49 for more on the revision.]
INTERNATIONAL CMC/REVIEW US/Canada Common Electronic Submissions Gateway
The US and Canada have agreed to a common platform for medical product applications that will allow for their mutual elec-tronic submission in the two countries (link to FDA announcement).
Health Canada Releases Draft Guidance on Drug Quality Submissions
Health Canada released a draft guidance in late January that updates its expectations for New and Abbreviated New Drug Submissions based on current ICH guidelines including ICH’s guidance on quality by design (QbD). Other primary changes involve HC’s current interpretation of Canada’s food and drug regulations and clarification and expansion of the type of infor-mation which should be provided in Module 3 (Quality) of the CTD. Addressed are the expectations for quality overall sum-maries, certificates of suitability, and drug master files. Comments are due by April 13, 2014.
GMP/INSPECTION
China Agrees to House More FDA Investigators
Chinese officials have cleared the way for FDA to station ten additional drug and device investigators in China. The FDA investigators will work out of the U.S. embassy and will have diplomatic privileges and immunities, Bloomberg reports.
ANVISA Approves New Track and Trace Rules
In December, the Brazilian regulatory authority ANVISA issued new rules regarding supply chain track and trace that will be implemented over the next three years. The mechanisms and procedures defined include a bi-dimensional barcode for capturing and transmitting the electronic data needed for tracking in Brazil. A forthcoming rule will help define the process for communicating the supply chain tracking information to ANVISA.
Rx-360 Expanding Presence in China
Rx-360 is introducing a number of initiatives in China. According to Rx-360 Asia Work Group co-leader, Janice Berman, quality assurance VP at Takeda Pharmaceuticals USA, the objective is to set up work groups to help drive activities that have been going on in the US for several years, such as shared resources for supplier audits, supply chain security generally, and membership solicitations. A schedule of biennial meetings is being planned, with a meeting targeted for this spring.
FDA Increasing Involvement with Europol on Counterfeiting
FDA is expanding its collaboration with Europe in the fight against counterfeiting. The agency is placing an agent from its Office of Criminal Investigations within the EU law enforcement agency, Europol. A key focus of the joint effort is illegal website pharmacy trafficking.

Protecting Patients WorldwideProtecting Patients WorldwideProtecting Patients WorldwideProtecting Patients WorldwideProtecting Patients Worldwide®®
+1 (202) 230-5608 • [email protected] • www.rx-360.org+1 (202) 230-5608 • [email protected] • www.rx-360.org+1 (202) 230-5608 • [email protected] • www.rx-360.org+1 (202) 230-5608 • [email protected] • www.rx-360.org+1 (202) 230-5608 • [email protected] • www.rx-360.org+1 (202) 230-5608 • [email protected] • www.rx-360.org+1 (202) 230-5608 • [email protected] • www.rx-360.org
We the undersigned members of Rx-360 fully support the mission of Rx-360 which is to:
PROTECT PATIENT SAFETY BY SHARING INFORMATION AND
DEVELOPING PROCESSES RELATED TO THE INTEGRITY OF THE
HEALTHCARE SUPPLY CHAIN AND THE QUALITY OF MATERIALS WITHIN THE SUPPLY CHAIN.
ABBVIE • AMGEN • AMPAC FINE CHEMICALS • ASH STEVENS • ASTRAZENECA • AURISCO PHARMACEUTICAL CO. LTD. • AVANTOR • BASF • BAXTER • BAYER • BEND RESEARCH • BIOGEN IDEC • BO
EHR
ING
ER IN
GELH
EIM • B
RISTO
L-MYER
S SQU
IBB
• CA
MB
RID
GE M
AJO
R LA
BO
RATO
RIES • C
AR
DIN
AL H
EALTH
• CO
DEX
IS • DA
IICH
I SAN
KYO
• DK
SH IN
TERN
ATION
AL • D
OE &
ING
ALLS • D
SM N
UTR
ITION
AL P
RO
DU
CTS • ELI LILLY • FO
REST LA
BO
RATO
RIES • FU
JIFILM • G
E HEA
LTHC
AR
E • GLA
XO
SMITH
KLIN
E • HIKAL • HOSPIRA • HOVIONE • JOHNSON & JOHNSON • LABOCHIM • LIFECONEX • LIFE TECHNOLOGIES • LIGAND • MERZ • MERCK & CO. • MERCK KGaA • MYLAN • MYODERM • NOVARTIS • N
OV
OZ
YM
ES
BIO
PH
AR
MA
•
PE
RR
IGO
•
PR
OC
TE
R &
GA
MB
LE
• P
FIZ
ER
•
OS
O B
IOP
HA
RM
AC
EU
TIC
ALS
•
RO
CH
E/G
EN
EN
TE
CH
•
SA
NO
FI
•
SA
RT
OR
IUS
•
SIG
MA
ALD
RIC
H
• S
PE
CT
RU
M C
HE
MIC
AL
MF
G
• T
AK
ED
A
• T
EM
PT
IME
•
TE
VA
•
UC
B
• V
WR
•
WA
TS
ON
•
WE
ST
•
YO
RK
CO
NTA
INE
R
•
We support our suppliers and colleagues who share our support of Rx-360 and its critical mission to protect patient safety. And, recognizing the power of leadership by example, we
invite others who share our patient safety goals to join us in this important endeavor.
Wes SchmidtVP, Quality Systems
AbbVie
William ReisVP, Global Strategic Sourcing
Amgen Inc.
Martin VanTriesteSVP QualityAmgen Inc.
Gary A. BakerVP, QARA
Ash Stevens, Inc.
Ashley ReadshawChief Procurement Offi cer
Astrazeneca
Peng ZhienPresidentAurisco
Richard M SiberskiGlobal Director of Quality
Avantor Performance Materials
Jaspreet GillVP, Global Quality & ComplianceBaxter Healthcare Corporation
Dr. Paul Heiden SVP QHSE
Bayer HealthCare
Richard SpoorSVP ProcurementBayer HealthCare
Debra KatterVP, Corporate Quality
Bend Research
Melissa Stoutt SeymourSr. Director, Corporate Quality
Biogen Idec, Inc.
Robert PantanoSVP, Warehouse Operations and
Operational ExcellenceCardinal Health
John NicolsPresident and CEO
Codexis, Inc.
Allen WelsherGlobal Head QA
Daiichi Sankyo Co., Ltd.
Jennifer Finnegan McCafferty
VP External QualityGlaxoSmithKline
Luisa PauloCompliance Director
Hovione
Vincent AntleSr. Director of Technical Operations and Quality
AssuranceLigand Pharmaceuticals, Inc.
Robert NassVP Quality and Regulatory
Management Merck Millipore Merck KGaA
Matt AndersonVP Quality
Merz North America, Inc.
Patricia M. LatzoSVP Global Quality and Strategic
SourcingMylan Inc.
Michael CohenManaging Director
Myoderm
Michael HoffmanVP Global Procurement
Pfi zer Inc.
Heiko HackelVP Global Sourcing
Sartorius
Thomas PaustVP Supply Chain Management
Sartorius
Tom BeilVP, Quality and Regulatory
AffairsSigma-Aldrich
Tom TynerVP Quality & Technical Service
Spectrum Chemicals and Laboratory Products
Steve FeldmanVP Quality & Regulatory Affairs
Temptime Corporation
Angélique KlootwijkDirector Quality Management &
Quality AssuranceVWR International
Pfi zer Inc.
Heiko HackelVP Global SourcingVP Global Sourcing
Robert Pantano
Thomas Paust
Richard M Siberski Melissa Stoutt Seymour
GlaxoSmithKline
Luisa PauloCompliance Director
William Reis
Robert NassRobert NassVP Quality and Regulatory
Management Merck Millipore
Wes Schmidt
Tom BeilDebra Katter
Allen Welsher
Hovione
Vincent Antle
Patricia M. Latzo
Ashley Readshaw
Temptime Corporation
Angélique KlootwijkDirector Quality Management & Director Quality Management &
Michael Cohen
Peng ZhienPresidentAurisco
Martin VanTriesteSVP Quality
Myoderm
John Nicols
Sigma-Aldrich
Tom TynerVP Quality & Technical Service
Spectrum Chemicals and
Gary A. BakerVP, QARA
Ash Stevens, Inc.
Jaspreet Gill
Jennifer Finnegan McCafferty

IPAC-RS/UF Conference TUESDAY - THURSDAY, 18-20 MARCH 2014
Orlando Inhalation Conference – Approaches in International Regulation
Hosted by University of Florida and IPAC-RS University of Florida Research & Academic Center 6550 Sanger Road Orlando, FL 32827
IPAC-RS and the University of Florida are hosting a public conference Orlando Inhalation Conference - Approaches in International Regulation where industry, regulators and other interested parties will discuss best scientific and regulatory approaches for orally inhaled and nasal drug products. The goal of this conference is to identify, discuss, and develop strategies for a harmonized, science-based regulatory approach towards the development of generic and innovator inhalation and intranasal drugs. Participants will discuss the requirements of regulatory authorities in different world regions, including in emerging markets, regarding the data supporting marketing applications from the perspectives of quality and (bio)equivalence, in vitro tests and in vivo clinical trials. Lessons learned from product applications that were approved or denied will be part of the discussion. This conference will foster the exchange of ideas and knowledge in the global scientific and regulatory community.
Major Themes: • Overview of International Picture – How are inhaled products approved around the world? • In-Vitro Considerations for Demonstrating Equivalence • Biomarkers, PharmacoKinetic (PK) and PharmacoDynamic (PD) Studies • Biometrics, Biostatistics, Clinical Trial Design • Overall Relationship of In-Vitro to PK and PD Data • Device Similarity, Design, Patient Use Factors • Development Pharmaceutics • Harmonization
Visit http://www.ipacrs.com/2014OrlandoConference.html for details To reserve your hotel room: https://resweb.passkey.com/go/dbr2014
REGISTRATION IS NOW OPEN, EARLY BIRD RATES AVAILABLE UNTIL OCTOBER 1, 2013.