intervention and treatment: a call for a comprehensive, interdisciplinary approach to treating sleep...
TRANSCRIPT

intervention and treatment:a call for a comprehensive, interdisciplinary approach to treating sleep disorders
emerson m. wickwire, phd, abpp, cbsm
co-director, center for sleep disorders
pulmonary disease and critical care associates
disclosures:
The Sleep Apnea Success Guidebook
HealthMedia- scientific consultant (2009)

what you’ll learn…
I. almost everything you’ll ever need to know about the two most common sleep disorders
II. a whole is greater than the sum of its partsIII. multi-system problems require multi-prong
treatment approaches
essential facts: insomnia
I. definition: what disorder looks like
II. consequences: what disorder does
III. clinical aspects: how to evaluate and treat

sleep onset insomnia
trouble falling asleep

trouble staying asleep
sleep maintenance insomnia

waking too early
early morning awakening

non-restorative sleep
non-restorative sleep

DAYTIME CONSEQUENCE
insomnia symptoms frequently overlap
& complaints may change over time

• fatigue/malaise
• attention, concentration, or memory impairment
• social/vocational dysfunction or poor school performance
• mood disturbance/irritability
• daytime sleepiness
• motivation/energy/initiative reduction
• proneness for errors/accident at work or while driving
• tension headaches/GI symptoms
• concerns or worries about sleep
daytime consequences

epidemiology of the most common sleep disorder
• 30-40% transient
• 10-15% chronic
• clinical practice: >50%

Foley et al, 2004
80
Number of Medical Conditions
0
10
20
30
40
50
60
70
Per
cen
t o
f R
esp
on
den
ts
Rep
ort
ing
an
y In
som
nia
0 1 2 or 3 4
insomnia increases with medical problems
n=1506age 55-84

Taylor et al, 2007
p values are for Odds Ratios adjusted for depression, anxiety, and sleep disorder symptoms.
Heart Disease
Cancer HTN Neuro Pulm Urinary Diabetes Chronic Pain
GI Any medical problem
%
p<.05
p<.05
p<.01p<.01
p<.001p<.001
p<.001
p<.001
medical problems in insomnia
n=772age = 20 to 98

INSOMNIADecreased TST
Increased SOL/WASO
Impaired sleep efficiency
Decreased SWS
PSYCHIATRIC ISSUES
Anxiety
Depression
Insomnogenic drugs
Substance abuse
Altered ACTH and cortisol
Concerns or worries re: sleep

insomnia as a disease of physiologic hyperarousal
Bonnet, 1998; Bonnet & Arand, 1995; Lushington et al., 2000; McClure et al., 2001; Perlis, 2001; Stepanski, 1988
• increased metabolic rate
• increased body temperature
• increased heart rate
• increased catecholamines
• increased high-frequency eeg

hyperarousal: beta eeg
Perlis et al, 2001

hyperarousal: hpa axis
Vgontzas et al, 2001
ACTH elevated from 1400 to 1730 and 2100 to 0030 cortisol elevated from 2100-0030 only
p=.07 p=.04

increased brain metabolism
Nofzinger et al., 2004

Nofzinger et al., 2004
hyperarousal: neuroimaging

attentional systems are active
ARAS: activates/deactivates cortex; alertness
Hypothalamus: sleep & wake
Thalamus: sensory processing; activates/deactivates cortex
Mesial Temporal Cortex: memory; novelty detection
Cingulate: excitatory role in emotions & motivated behavior
Insular cortex: perceptions of disgust & pain

attentional systems are active
ARAS: activates/deactivates cortex; alertnessHypothalamus: sleep & wake
Thalamus: sensory processing; activates/deactivates cortex
Mesial Temporal Cortex: memory; novelty detection
Cingulate: excitatory role in emotions
Insular cortex: perceptions of disgust & pain

• Harvey model
• sleep beliefs & worry
• insomnophobia
• battlemind
• sufferers: cognitive not somatic arousal
cognitive factors in insomnia
Harvey, 2002; Morin et al., 2007; Lichstein & Rosenthal, 1980

how insomnia develops:biobehavioral pathway

PredisposingRisk Factors
Biology/ Hard-wiringPersonality
Temperament
Insomnia
No Insomnia
Spielman, 1987

PredisposingRisk Factors
Biology/ Hard-wiringPersonality
Temperament
Insomnia
No Insomnia
Spielman, 1987

CompensatoryBehaviors
Spend more time in bed“Try harder” to sleep
Sleep in on weekendsTake naps
Sleep outside bedroomOveruse caffeine/stimulants
Various OTC sleep aids
Obsess/ overfocus on sleep
Insomnia
No Insomnia
EnvironmentalStressor
Medical illnessLoss of loved one
Job transitionCumulative effect
PredisposingRisk Factors
Spielman, 1987

Insomnia
No Insomnia
“Compensatory”Behaviors
Spend more time in bed“Try harder” to sleep
Go to bed earlierSleep in on weekends
Take napsSleep outside bedroom
Overuse caffeine/stimulants
Decrease daytime activityVarious OTC sleep aids
Obsess/ overfocus on sleep
PredisposingRisk Factors
EnvironmentalStressor
Spielman, 1987

Insomnia
No Insomnia
PredisposingRisk Factors
EnvironmentalStressor
“Compensatory”Behaviors
Spielman, 1987

Spielman, 1987

ACUTECHRONIC(> 1 mo)

CBT-i

insomnia causes problems
n=1741

insomnia, CVD & mortality
n=1741
n=3430

insomnia worsens quality of life
Leger et al., 2001
n=1053

insomnia precedes depression
n=1053 men
Chang et al., 1997

insomnia post-deployment:#1 symptom & may predict ptsd
n=2249

assessment

ask! (doctors don’t ask & patients don’t tell)
• frequency (>3x/ week)
• intensity (>30m sol/waso, quality)
• duration (>1 mo)
• daytime sequelae
• do you snore?

1. Please rate the SEVERITY of your sleep problem(s).
None Mild Moderate Severe Very Severe
Difficulty falling asleep:
Difficulty staying asleep:
Problem waking up too early:
2. How SATISFIED/dissatisfied are you with your current sleep pattern?
0 1 2 3 4
Very Unsatisfied Very Satisfied
3. To what extent do you consider your sleep problem to INTERFERE with your daily functioning (daytime fatigue, ability to function at work/daily chores, concentration, memory, mood, etc.)?
0 1 2 3 4
Not at all Interfere Interfere Very Much
4. How NOTICEABLE to others do you think your sleeping problem is in terms of impairing the quality of your life?
0 1 2 3 4
Not at all Noticeable Very much Noticeable
5. How WORRIED/distressed are you about your current sleep problem?
0 1 2 3 4
Not at all Worried Very much Worried
clinical screening:insomnia severity index
Bastien et al., 2001
<7 none>7 subthreshold>14 mod severe>21 severe

use CBT-I:
• recommended 1st line treatment
• primary & comorbid insomnias
• adults of all ages & hypnotic users*
combined therapies:
• no benefit over cbt-i alone
• cbt-i aids hypnotic taper

essential facts: insomnia

essential facts: srbd
I. definition: what disorder looks like
II. consequences: what disorder does
III. clinical aspects: how to evaluate and treat
snoring and sleep apnea

snoring and sleep apnea

noobstruction
hypopneasnoring apnea
Obstructive Sleep Apnea
(OSA)
Upper Airway Resistance Syndrome
(UARS)

noobstruction
hypopneasnoring apnea
AHI (OSA only)<5 none5-14 mild15-29 mod30+ severe
UARSflow-limited breaths
*subtle detection

↓O2
EEG arousal
↓ total sleep
mechanisms of srbd

• anatomical abnormalities
• genetic factors
• collapsibility of upper airway
• weight gain
• behavioral factors
causes of srbd

• EDS, mood disturbance, performance
deficits
• quality of life, libido
• obesity, dm, htn, stroke, cardiovascular
death, overall mortality• enormous societal costs
consequences of srbd

assessment of srbd
out of lab(“at home”)
in lab(gold standard)
treatments for srbd
digeridoo oral appliance

surgery: not first-line treatment
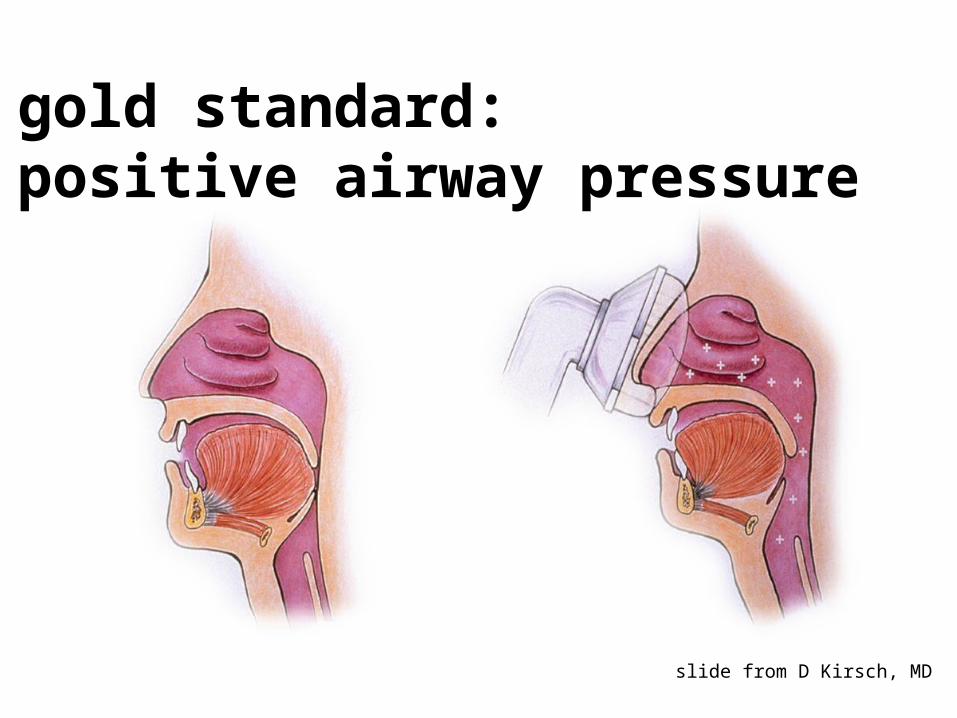
gold standard:positive airway pressure
slide from D Kirsch, MD

• 36 RCTs, N=1718vs control
↓objective & subjective sleepiness quality of life neurocognitive function
vs oral appliance (OA)↓ AHI sleep efficiency minimum O2
Giles, Lasserson, Smith, White, Wright & Cates, 2006
pap works

LESS BAD
eliminates OSA (95+%)
↓ sleepiness
↓ hospitalizations
↓ car accidents↓ HTN (esp nocturnal)↓ pulmonary artery pressures↓ GERD
MORE GOOD
↑ qol↑ cognition↑ glucose control↑ gas exchange↑ heart function in heart
failure pts↓ reduces cardiac
arrhythmias during sleep
srbd in ptsd
• evidence of increased srbd in ptsd
• especially uars
• hypothesis: massive sympathetic burst alters pharyngeal muscle tone
• ↑ increased respiratory effort = EEG
• sleep: 37% of variance in symptoms

a whole is greater than the sum of its parts: insomnia, srbd, or both?
I. secondary insomnia: a myth dismissed
II. frequent co-occurrence
III. hypothesized mechanisms

a myth…
NIH 1983 (that was then)
• insomnia is a symptom (only)
• treat the primary disorder
NIH 2005 (this is now)
• insomnia is a disorder, typically coexisting with other disorders
• treat both conditions
• improvements insomnia can improve other outcomes

a myth… dismissed
NIH 1983 (that was then)
• insomnia is a symptom (only)
• treat the primary disorder
NIH 2005 (this is now)
• insomnia is a disorder, typically coexisting with other disorders
• treat both conditions
• improvements in insomnia can improve other outcomes

• impacts quality of life
• worsens clinical outcomes
• frequently does not remit with
treatment of “primary” condition
comorbid insomnia is a disorder

not just a symptom
• consistency of complaints
• independent course of disorder
• responds to different treatment than comorbid disorder
• responds to same type of treatment across different disorders
Harvey, 2001; Lichstein et al., 2004
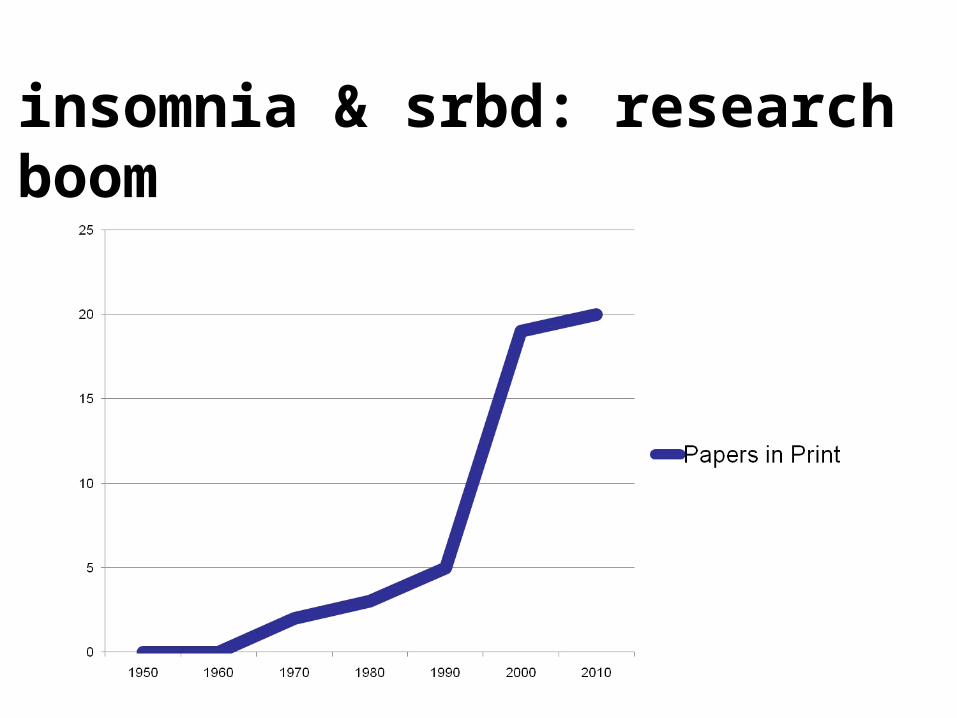
insomnia & srbd: research boom

insomnia is common in srbd

insomnia is there (and not just a symptom)
n=105
70% men
M age=53.9±14
insomnia criteria:
ISI>15duration>6 months
PSG SOL or WASO>30m
w/daytime impairment
Smith et al., 2004
39% moderate-severe insomnia(insomnia unrelated to SRBD)

(n=100, 43 men, M age=49±14)
Hagen, Patel, & McCall, 2009; Nguyen et al., 2010; Lichstein et al., 2010
half or more of patients…
61% moderate-severe insomnia (ISI)
(n=166, 138 men, M age=54.8±11.8)49.3% moderate-severe insomnia (ISI)
84% of OSA patients also meet DSM-IV/ ICSD-2 criteria for chronic insomnia

29-43%
40-64.4%
92.7%(15.7 UARS)
90.9%(40.9 UARS)
Wickwire & Collop, 2010
and it works both ways:occult srbd in insomnia

Krakow et al., 2001; Krakow et al., 2002; Krakow et al., 2004
insomnia & srbd in ptsd
(n=44, 37 women, M age=40.9±12.4)
90.9% srbd (50% OSA; 40.9% UARS)
(n=78, 50 women, M age=51.5±13)
95% srbd (41% OSA; 54% UARS)
99% insomnia
(n=187 women, M age=37±11)
89.8% rdc symptoms srbd (confm’d in 21 tested)
↓ sleep (self-report and psg)
↓ neurocognitive function
↓ psychomotor reaction times
↑ sleepiness (self-report and mslt)
↑ psychiatric distress & pain
consequences are additive (1+1=3)

subtle, atypical presentations
• no loud snoring/ normal weight
• older patients
• postmenopausal women
• patients with chronic pain
• ptsd/mTBI?

onset insomnia & srbd severity:inverse relationship
Gold et al., 2007
%

osa patients not always sleepy
N=4653
Luyster, Buysse, & Strollo, 2010

Complex insomnia hypothesis.
Chung K Chest 2003;123:310-313
©2003 by American College of Chest Physicians

Complex insomnia hypothesis.
Chung K Chest 2003;123:310-313
©2003 by American College of Chest Physicians

Complex insomnia hypothesis.
Chung K Chest 2003;123:310-313
©2003 by American College of Chest Physicians

Complex insomnia hypothesis.
Chung K Chest 2003;123:310-313
©2003 by American College of Chest Physicians

Benetó et al., 2009

Benetó et al., 2009

Benetó et al., 2009

Benetó et al., 2009

multi-system problems require multi-prong treatment approaches
I. treatment interactions & combined therapies
II. case study & clinical recommendations
III. a comprehensive practice model

insomnia medications can worsen breathing
• older benzodiazepines bad
1. negatively impact breathing
2. raise arousal threshold
• newer hypnotics minimal impact AHI
• off-label meds may pose risk

untreated insomnia can compromise OSA treatment
only insomnia predicted negative
outcome in oral appliance for osa
Machado et al., 2006
N=188

sleep maintenance insomnia predicts poor cpap adherence
N=232
Wickwire, Smith, Birnbaum, & Collop, 2010

cbt-i #1 surgery #1
surgery #2 cbt-I #2
Guilleminault et al., 2009
combined treatments provide additive benefit

treating both disorders improves outcomes
Krakow et al., 2004, 2006
• in patients with symptoms of insomnia and srbd, nasal strips improved sleep
• treatment of srbd improved outcomes
following cbt-i (8/17 remit 15/17 remit)

• requires additional evaluation
• srbd may be common in patients with treatment-resistant insomnia
refractory insomnia
Guilleminault et al., 2002; Krakow et al., 2006, 2010

screen – insomnia and srbd– poor subjective sleep quality– nonrestorative sleep/ daytime fatigue
antennae up– older adults– postmenopausal women– trauma survivors
treat both conditions, concurrently if possible
clinical recommendations

insomnia– be very careful w/ benzodiazepines and off-label
medications– sleep hygiene not effective in isolation, not effective
in handout– refer to insomnia specialist if available
srbd– appreciate frequent co-morbidity of insomnia– intervene early for cpap adherence– refer to sleep specialist: snoring, obesity, htn, dm,
refractory insomnia
clinical cautions

• self-referred for insomnia study
• ineligible per phone screen (osa)
• discussed treatment options
• initial evaluation scheduled
Wickwire, Schumacher, Baran, Richert, & Roffwarg, 2007
the real-world: case study

• 61 y.o. Caucasian male• lifelong Mississippi resident• normal weight• college degree• US Army veteran• PT VA employee w/shift work• “happily” married 31 years• 2 adult daughters & 2 grandchildren
patient characteristics

• recently diagnosed w/ OSA (AHI=31)• GERD• chronic knee pain• denies past psychiatric treatment• denies history substance abuse• current daily meds: high blood pressure,
GERD, baby aspirin, otc sleep aid prn
medical history

• father had trouble falling asleep– blamed sciatic nerve– slept on sofa
• brother suffers PTSD– experiences sleep problems– takes sleep medication
• wife snores and suffers EDS
relevant family history

↑ SOL– I can’t fall asleep at night (25-year Hx)
– I don’t like to take pills (drug stupor)
OSA– I never dreamed I had apnea… I only started
snoring two years ago… they made a mistake– apnea is obstruction… obese people…– PAP is frustrating, loud, straps too tight, hard
to get adjusted right
what’s on his mind?

• can’t concentrate or read
• can’t stay alert deer hunting
• tired & eyes irritated
• wants to nod off during work
• irritable*
assessing daytime sleepiness

rumination: • grandson’s health, nephew’s safety, involved with family (softball)• thinking about “tomorrow”• previous day: “what someone said, what family goes through”
physical discomfort:• pressure on feet, sensitive to physical, blankets, spouse
bedroom environment:• tempur Pedic bed• TV in bedroom (wife falls asleep with TV)• wife snores; he hears her “rustling” around
assessing sleep onset insomnia

307.42 Primary insomnia
327.23 Obstructive sleep apnea
Plan:
1. CBT for PAP acceptance and adherencewhat, how, why
2. CBT for insomnia
diagnoses & treatment plan

OSA
#2: cbt
insomnia
#1: cpap
the plan: a systematic approach

OSA
mood
insomnia
#2: cbt#1: cpap

• 2 45-minute sessions
• principles of behavioral change
• elicit personalized risks & benefits
• incorporate guided imagery
motivational enhancement
Aloia et al., 2004

develop a pre-sleep routine
typical activity/ arousal level:
Wickwire, Schumacher, & Clarke, 2008

marker
ritual(“greased shoot” to sleep)
sacred sleeping environment
develop a pre-sleep routine
Last meal or snack of day
END DAY ACTIVITIES- Leave work
Change pajamas/ T-shirt
Read 30- minutes (paper, magazine, book)
Relaxation CD
Breathing exercises
Bathroom routine
EARPLUGS
Lights out/ Bed
pre-sleep routine

• self-report: 90-120 m/day, falling asleep with mask on, waking and removing it
• CPAP 30m-300m (mean = 108.5m/ night over 2 week pd)
improved pap adherence

51.8
33.2
20.9
0
10
20
30
40
50
60
Pre Post Follow-up
Minutes
61.5
13.818.6
0
10
20
30
40
50
60
70
Pre Post Follow-up
Minutes
345.2
422.6 439.9
0
50
100
150
200
250
300
350
400
450
500
Pre Post Follow-up
0.75
0.89 0.89
0.65
0.7
0.75
0.8
0.85
0.9
0.95
Pre Post Follow-up
sleep latency
total sleep time
wake aftersleep onset
sleepefficiency

before after
BDI-2 1 (0)
STAI-T 49th % 31st %
ISI 22 16
ESS 10 5
DBAS-10 59.7 51.4
knowledge 4/5 5/5
acceptability 65.7 75.4
quantitative improvement

• definitely not as tired• much less nodding• less drowsy in deer stand• no sleep aid in past 3 months• no TV in bedroom, no late eating• following pre-sleep routine & using
deep breathing exercises
qualitative improvement

silos & 3-month waits
pulmonary(psg)
psychology(cbt)
neurology
psychiatry(meds) surgery

patient hassle & system burden

a better alternative: our model

MDMOD-10in-lab psgat home test
MTF/PCPor specialist
MDPAPoral appliancemedication
PhDinsomniaactigraphyPTSD/mTBI
PhDCBTPAP successIRT
Follow-up Carepap adherence data
HIPAA secure websiteAHLTA friendly data
Treatment
Evaluation
promptscheduling
coordination w/ referring
providers

in conclusion: insomnia & srbd
I. common, bad, & highly treatable
II. frequently co-occur
additive negative effects
III. combined treatments are best
demand comprehensive care
