integrating the nutrition education and counseling (nec) intervention into the rakai health sciences...
TRANSCRIPT

INTEGRATING THE NUTRITION EDUCATION AND COUNSELING (NEC) INTERVENTION INTO THE RAKAI HEALTH SCIENCES
HIV/AIDS CARE PROGRAM
BY FLORENCE T. TUSHEMERIRWE
MakSPH-CDC HIV/AIDS FELLOW
2011

b
INTEGRATING THE NUTRITION EDUCATION AND COUNSELING INTERVENTION INTO THE RAKAI HEALTH SCIENCES
HIV/AIDS CARE PROGRAM
BY FLORENCE T. TUSHEMERIRWE
BFST, MSc. PHN MakSPH-CDC HIV/AIDS FELLOW
April 2011

i
TABLE OF CONTENTS
TABLE OF CONTENTS ............................................................................................................... I
DECLARATION......................................................................................................................... IV
DEDICATION ..............................................................................................................................V
ACKNOWLEDGEMENTS ....................................................................................................... VI
EXECUTIVE SUMMARY ....................................................................................................... VII
1. INTRODUCTION AND BACKGROUND ..................................................................... 1
1.1. INTRODUCTION ............................................................................................................... 1 1.2 BACKGROUND ........................................................................................................... 8
2 LITERATURE REVIEW .................................................................................................... 12
2.1 RELATIONSHIP BETWEEN HIV AND NUTRITION .......................................................... 12 2.2 NUTRITION KNOWLEDGE, ATTITUDES AND FEEDING PRACTICES AMONG PLHIV ..... 14
3. CARE PROGRAM NEED FOR THE INTERVENTION, JUSTIFICATION, CONCEPTUAL FRAMEWORK ............................................................................................... 22
3.1 NEED FOR THE NEC INTERVENTION ............................................................................ 22 3.2 JUSTIFICATION ............................................................................................................... 23 3.3 CONCEPTUAL FRAMEWORK ......................................................................................... 25
4. PROGRAM OBJECTIVES ................................................................................................ 29
4.1 GENERAL OBJECTIVE .................................................................................................... 29 4.2 SPECIFIC OBJECTIVES..................................................................................................... 29
5 IMPLEMENTATION APPROACHES ........................................................................... 30
5.1 TARGET POPULATION ................................................................................................... 30 5.2 PROGRAM SITE .............................................................................................................. 30 5.3 THE NEC INTERVENTION ............................................................................................. 34
6 OUTPUTS ............................................................................................................................ 42
6.1 NUTRITION MESSAGES FOR PLHIV – LUGANDA AND ENGLISH VERSIONS ................ 42 6.2 DRAMA SCRIPT .............................................................................................................. 42 6.3 M & E PLAN .................................................................................................................. 42 6.4 NEC PROGRAM EVALUATION PROPOSAL .................................................................... 43 6.5 REFERENCE BOOKS ........................................................................................................ 44 6.6 OTHER OUTPUTS ........................................................................................................... 45
7 LESSONS LEARNT ........................................................................................................... 47
8 STRENGTHS AND WEAKNESSES OF THE NEC PROGRAM .............................. 48
8.1 STRENGTHS.................................................................................................................... 48 8.2 WEAKNESSES ................................................................................................................. 49
9 CHALLENGES FACED AND GAPS IDENTIFIED ..................................................... 50
9.1 CHALLENGES ................................................................................................................ 50 9.2 GAPS IDENTIFIED ........................................................................................................... 51

ii
10 CONCLUSION ................................................................................................................... 52
11 RECOMMENDATIONS ................................................................................................... 53
12 REFERENCES ..................................................................................................................... 55
13 APPENDICES ..................................................................................................................... 58
13.1 PROMOTED KEY NUTRITION MESSAGES FOR PLHIV .................................................... 58 13.2 NUTRITION DRAMA SCRIPT .......................................................................................... 68 13.3 DATA COLLECTION TOOLS ........................................................................................... 82 13.4 CONSENT FORM (ENGLISH VERSION) ......................................................................... 119

iii
List of Figures FIGURE 1: PERCENTAGE OF PLHIV WHO KNOW THE IMPORTANCE OF GOOD NUTRITION (KONIZ-
BOOHER P. ET AL., 2009.) ...................................................................................................... 15 FIGURE 2: THE MALNUTRITION AND HIV CYCLE ......................................................................... 26 FIGURE 3: BENEFITS OF NUTRITION INTERVENTIONS ..................................................................... 28 FIGURE 4: MAP SHOWING THE RAKAI DISTRICT LOCATION ......................................................... 32 FIGURE 5: MAP SHOWING THE DIFFERENT CLINIC LOCATION ....................................................... 33 FIGURE 6: THE FELLOW (IN BLUE) TRAINING THE DRAMA TEAM IN THE VILLAGE ........................ 36 FIGURE 7: PICTURE SHOWING PROTECTIVE AND EXTRA ENERGY FOODS AVAILABLE IN KAKUUTO,
RAKAI .................................................................................................................................... 38 FIGURE 8: A PEER SMART READY TO GIVE A PORRIDGE MIXTURE DEMONSTRATION IN KAKUUTO
............................................................................................................................................... 39 FIGURE 9: PEER SMARTS SERVING PEOPLE AFTER A COOKING DEMONSTRATION ......................... 40 FIGURE 10: THE RAKAI CAB MEMBERS POSE FOR A GROUP PICTURE AFTER A NUTRITION
TRAINING (FELLOW IN A RED TOP). ....................................................................................... 41
iv
Declaration
I, Florence Tushemerirwe do hereby declare that this program report
entitled ―Integrating the nutrition education and counseling intervention
into the Rakai Health Sciences HIV/AIDS Care program” has been
prepared and submitted in fulfillment of the requirements of the
MakSPH-CDC HIV/AIDS Fellowship Program and has not been
submitted for any academic qualifications.
Signed………………………… Date…………………….. Florence Tushemerirwe, Fellow Signed………………………… Date……………………….. Dr. Gertrude Nakigozi
Host Institution Mentor Signed………………………… Date……………………….. Dr. Esther Buregyeya
Academic Mentor
v
Dedication
I dedicate this report to the People Living with HIV that I worked with
that are enrolled on the HIV/AIDS Care program at Rakai Health Sciences
Program (RHSP). These worked tirelessly, learning a new concept and the
different themes of the Nutrition Education and Counselling program was
not easy. However, their dedication saw us through successful completion
of the program. May God richly reward you with healthier lifestyles that
you committed yourselves to achieving!
I also dedicate this report to the staff of RHSP that spent time and valuable
recourses learning about nutrition for PLHIV and for appreciating my
input into their Care program.

vi
Acknowledgements
It is my pleasure to thank everyone that participated in the Nutrition
education and counseling program that is integrated into the Rakai Health
Sciences HIV/AIDS Care program. Without you, this work wouldn’t
have reached this far.
I am grateful to my mentors; this work wouldn’t have been possible
without your support.
Thank you to the Ministry of Health staff I partnered with during this
program, your input is highly appreciated.
Special thanks go to the Makerere University School of Public Health-
Centres for Disease Control HIV/AIDS fellowship Program, for
facilitating my two years on the fellowship program. I appreciate your
input into my career development.
vii
Executive Summary
Rakai Health Sciences HIV/AIDS Care program had a need; to provide
holistc care to the PLHIV, enrolled on this program. A pilot nutrition
education and counselling program was therefore integrated into their
Care Program in thirteen community-based clinics, situated in rural Rakai
for 7 months, from July 2010 till December 2010.
The program goal was to improve nutrition Knowledge, Attitudes and
feeding Practices of people living with HIV enrolled on RHSP’s
HIV/AIDS Care Program. This report summarises the design,
implementation and outputs of this program. In addition, strengths,
weaknesses, challenges faced and exisiting gaps were identified for the
Institution to improve the program as they plan to roll it out to other
clinics.
Specifically, key nutrition messages were integrated into the health
education messages; drama and practical cooking demonstrations were
introduced into the health education sessions. A complete set of key
nutrition messages generated by Regional Center for Quality of Health

viii
Care and adapted to Rakai conditions in English and Luganda versions, a
Drama script in Luganda, an M & E plan for the program, a ready
proposal to evaluate the NEC program and a library are some of the
outputs of the program.
I would like to recommend addition of a nutrition concept to the
Institution Mandate, which would open more opportunities to carrying
out nutrition research and service programs in Rakai. Regular staff
refresher trainings and an evaluation of the initiated intervention are
further recommended.
ix
Acronyms AFASS Acceptable, Feasible, Affordable, Sustainable and Safe
AIDS Acquired Immune Deficiency Syndrome
ART Anti-Retroviral Therapy
BMI Body Mass Index
CAB Community Advisory Board
DK Don’t Know
QCD Quality Control Department
CDC Centers for Disease Control
CHWs Community Health Workers
Cm Centimeters
CTC Community-based Therapeautic Centers
ECSA-HC East, Central and Southern Africa Health Community
FANTA Food and Nutrition Technical Assistance
FGDs Focus Group Discussions
HE Health Education
HIV Human Immunodeficiency Virus

x
IEC Information, Education and Communication
IIs In-depth Interviews
KAP Knowledge, Attitudes and Practices
KIIs Key Informant Interviews
Kg/m2 Kilograms per meter squared
MakSPH Makerere University School of Public Health
MDGs Millenium Development Goals
M & E Monitoring and Evaluation
MII Macro International Inc
MoH Ministry of Health
MUAC Mid-Upper Arm Circumference
NEC Nutrition Education and Counseling
NIH National Institutes of Health
OIs Opportunistic Infections
PLHIV People Living With HIV
PMTCT Prevention of Mother-to-Child Transmission of HIV
RCQHC Regional Center for Quality of Health Care

xi
RHSP Rakai Health Sciences Program
SCN Scientific Committee on Nutrition
TB Tuberculosis
Tel. No. Telephone Number
UAC Uganda AIDS Commission
UBOS Uganda Bureau of Statistics
UNAIDS The Joint United Nations Programme on HIV/AIDS
UNAP Uganda Nutrition Action Plan
UNFP Uganda National Food and Nutiriton Policy
UVRI Uganda Virus Research Institute
WHO World Health Organization
Wt. Weight
Ht. Height
xii
Definition of terms
Anti-retroviral: Drugs that reduce multiplication of HIV in the body.
Body mass Index: It is the ratio of one’s weight in kilograms to recumbent
length or standing height in metres squared. It is a measure of a person’s
(both adults and children) body composition and depicts their nutritional
status.
Dietary: Anything that relates to diet or food consumed.
Good Nutrition: It is having enough food from all food groups in the
right quantities and quality, for proper functioning, growth, repair and
maintenance of health.
Immunity: Body’s natural resistance to infections.
Main Meal: Food eaten at a specified time of the day, e.g. breakfast, lunch
and supper.
Malnutrition: Ill health caused by inadequate intake of the right quantity
and quality of food to nourish the body.
xiii
Nutrient: It is the part of the food we eat that nourishes the body; e.g.
carbohydrates provide energy, proteins are body building while vitamins
and minerals are protective foods and provide water to the body.
Nutrition: It is how food and drink are taken, digested and absorbed by
the body to provide for normal growth, development and maintenance of
health.
Nutrition Education: Any set of learning experiences designed to facilitate
voluntary adoption of eating and other nutrition related behavior
conducive to health and well-being (Bukhari, et al. 2008).
Nutritional Status: A measurement of the extent to which individuals’
physiological needs for nutrients are met.
Snack: Food that is readily available and eaten in between meals. For
PLHIV these increase energy intake in their diets e.g. roasted ground nuts,
simsim seeds, soy beans, fruits, sugar cane, honey, and other healthy
Simple foods that individuals can financially and phyisically acces

1
1. Introduction and Background
1.1. Introduction
1.1.1. Importance of integrating nutrition into HIV/AIDS Care Programs
Integrating nutrition interventions into Human Immunodeficiency Virus
and Acquired Immune Deficiency Syndrome (HIV/AIDS) Care programs
prolongs patient survival and reduces death due to malnutrition among
People Living with HIV (PLHIV), receiving Anti-Retroviral Therapy
(ART) (Paton NI et al., 2006) and Prophylaxis. Nutrition interventions like
Nutrition Education and Counselling (NEC) are vital in HIV/AIDS care.
In resource limited settings, NEC empowers PLHIV to modify their diets,
using locally available, nutrient dense and culturally acceptable foods to
maintain good health, improve their nutritional status (Piwoz et al., 2004)
and daily functioning (SCN, 2004).
Through improved KAP, PLHIV can ably plan to utilise the limited
resources and modify diets to boost their immunity, better manage the
disease and improve response to ART and other treatment (ECSA-HC et
al., 2008, Bukusuba J. et al., 2010).

2
An improved/good nutritional status increases the opportunities for
PLHIV to slow down progression of HIV to AIDS, increases their ability to
fight the disease and reduces their vulnerability to opportunistic
infections (Piwoz et al., 2004, SCN, 2004).
Globally, nutrition is central to achieving the first six Millenium
Development Goals (MDGs) (SCN, 2004, FANTA-2, 2010). Specifically, for
MDG 6: ―Combat HIV/AIDS, malaria and other diseases‖, ―good nutrition
slows the progression of HIV to AIDS, increases malarial survival rates
and lowers the risk of diet-related chronic diseases‖ (SCN, 2004).
HIV/AIDS counteracts the MDG goal achievements through affecting
PLHIV’s nutritional status. However, incorporating nutrition into
HIV/AIDS programs is a sure means of addressing this challenge, paving
way to achieving the set MDG goals (SCN, 2004).
Research shows that PLHIV with poor nutritional status hardly adhere to
ART (Stuart Gillespie et al., 2001, Gillespie S. et al., 2001) experience
impaired immunity, increased vulnerability to opportunistic infections,

3
and hastened progression of HIV to AIDS (ECSA-HC et al., 2008, RCQHC,
2008, Bachou H. et al., 2006) .
In addition, ―poor knowledge and dietary practices among PLHIV
significantly contributes to the rapid progression of HIV to AIDS‖
(Bukusuba J. et al., 2010). Therefore, nutrition is critical in combating
HIV/AIDS and interventions can be implemented throughout prevention,
care, treatment and support strategies (SCN, 2004).
Sub-Saharan Africa, is home to 67% of the PLHIV in the world and still
faces challenges in combating the disease (UNAIDS, 2008). In addition,
there is underlying malnutrition, with 35% of the population in sub-
Saharan Africa malnourished (UNAIDS, 2008), which largely contributes
towards disease in the world (SCN, 2004).
In Uganda, 38.1% of under-five year old children are stunted, 6.1% are
wasted and 15.9% are under-weight. Also, 12.1% women of reproductive
age are under-nourished with their Body Mass Index (BMI) as low as
<18.0 kgs/m2; among all women in the nation, 41% are anaemic, while
64% of the pregnant women are anaemic (UBOS and MII, 2007).

4
Among PLHIV, it is estimated that 20-25% of people initiated on ART
have mild – severely malnutrition (BMI<18.5kg/m2), with the highest rate
being at 25% in rural areas, compared to 21% in Kampala (Ekoru, 2007).
At ART clinics level ―up to 23% adults and 50% children who are on
HIV/AIDS treatment have moderate malnutrition and 40% of the children
admitted at Mwanamugimu Nutrition Clinic in Mulago hospital have
both malnutrition and HIV‖(MoH, 2009). This underlying malnutrition is
a high risk to death in this vulnerable population.
To ensure holistic HIV/AIDS care, World Health Organisation (WHO)
recommends integration of nutrition interventions into care programs, as
a priority action (UNAIDS, 2008). This mitigates the two pronged disease
burden, caused by HIV/AIDS and malnutrition.
1.1.2. Uganda National policy and nutrition for PLHIV
Uganda has significant achievements in integrating nutrition into health
care programs; for instance development of nutrition policy and
guidelines for use by service providers. However, these policies and
guidelines ―did not provide adequate guidance on nutrition care and
support for PLHIV‖ (MoH, May 2006).

5
Consequently, integrating nutrition interventions into HIV/AIDS
program has met several challenges, for example, the food and nutrition
bill is not yet passed by the Ugandan Parliament (Mashoo, 2010) which
limits the scope, coverage and harmonisation of HIV support and service
programs and strategies (MoH, May 2006). Uganda has taken great steps
in addressing these challenges as depicted in the national constitution,
policies and guidelines.
The 1995 Republic of Uganda Constitution promises to ensure ―Food and
Nutrition Security for all‖ and section (c) states that the Government shall
―encourage and promote proper nutrition through mass education and
other appropriate means in order to build a healthy State‖ (FANTA-2,
2010).
The Uganda Food and Nutrition Policy (UFNP), 2003 is committed to
ensuring household food security for all citizens, and ―to promote
optimum nutrition for people living with HIV/AIDS‖ through
incorporating nutrition into Care programs (MoH, 2003).

6
The National HIV & AIDS Strategic Plan aims at ―mitigating the health
effects of HIV/AIDS by 2012‖ (UAC, 2007) and providing
―complementary support including nutrition to PLHIV‖. Also, the
Uganda Policy Guidelines on Infant and Young Child Feeding stresses
optimal feeding for HIV exposed children, exclusive breastfeeding of
infants to six months, regardless of their HIV-sero status (MoH, 2009).
Fortunately, Uganda is in the process of finalising the Uganda Nutrition
Action Plan (UNAP), which will focus on increasing acess to nutrition
education. This plan will use approaches like, but not limited to practical
demonstrations, capacity building, research, and committing the policy
makers to implementing the plan (Republic et al., February 2011). This
will go strides into curbing malnutrition through knowledge sharing with
Ugandan communities.
1.1.3. Why the Nutrition education and counselling gap?
There have been significant achievements in the care, treatment and
support for PLHIV in Uganda, since ART became accessible. However,
there is room for nutrition knowledge improvement, which is essential in
HIV/AIDS Care (MoH, May 2006).

7
In Uganda, the nutrition knowledge gap exists among PLHIV due to
inadequate nutrition education and counselling, as part of their Care at
health units and limited knowledge on use of the locally available food‖
(MoH, 2009) to manage the disease. Consequently, ―some of our PLHIV
are not aware of the importance of nutrition‖ (Ruhangariyo, 2010) to
maintain good health.
Much as ―nutrition counselling, care, and support is integral to
comprehensive HIV care‖ for PLHIV, (Piwoz et al., 2004, UAC, 2007), it
has not been prioritized in Uganda. Uganda lacked policies, guidelines,
harmonized strategies and information to address this gap. This led to
―inadequate nutrition counseling, and knowledge on use of the locally
available food‖ (Gillespie S. et al., 2001) to maintain good health. These
factors underpin the existence of malnutrition among PLHIV, which
would otherwise be prevented though community-based strategies.
In most rural settings, women ―produce the food, feed the children and
the family as a whole and are responsible for taking care of the health
needs of children‖ (Kakitahi, 2008). Nutrition is impacted by women’s
education and since they are not empowered in this aspect, communities
have pronounced nutrition knowledge gaps.

8
There are correlations between maternal education and nutritional status
and using informal education through community-based strategies boosts
communities’ nutrition knowledge base that can achieve improved
communities’ nutritional status (Kakitahi, 2008).
1.2 BACKGROUND
1.2.1 Rakai Health Sciences Program Overview
Rakai Health Sciences Program (RHSP) is a research collaboration
between the Uganda Virus Research Institute (UVRI)/Ministry of Health,
Uganda and researchers at Makerere, Columbia and Johns Hopkins
Universities.
The Program (RHSP) aims at improving public health through basic
sciences, clinical and population-based research and provides health
related services. There are six main departments, viz; Studies, Clinical
services, Community services, Data management and Biostatistics and
Administration.
9
Under the clinical services, we have the Anti-Retroviral Therapy (ART)
HIV/AIDS Care, prevention and support services provided to PLHIV.
Integrated into this HIV/AIDs care program, is the NEC program.
1.2.1 Rakai Health Sciences HIV/AIDS Care Program
The RHSP HIV/AIDS Care program is implemented through 13 clinics,
situated at pre-existing government health centres, serving 50
communities in rural Rakia District, South-western Uganda.
The field team is based at the clinics; each clinic has a Clinician and a
nurse plus a resident counsellor. This team is responsible for collecting
and entering clinic data into an electronic database. Institution medical
doctors regularly support the field teams to implement the HIV/AIDS
Care Program activities.
Services offered include: treatment of HIV/AIDS using ART, other
diagnosis, treatment and prophylaxis against Opportunistic Infections and
co-trimoxazole for prophylaxis. In additional family planning, Prevention
of Mother to Child Transmission of HIV (PMTCT) and Tuberculosis (TB)
diagnosis and treatment, general HIV counselling, adherence counselling
are offered too.

10
Health Education (HE) precedes all clinical sessions, in some of these,
nutrition education is given. Nutrition counselling is given at group and
individual levels by community resident HIV counsellors and two to four
community volunteers that are trained to give health education at each of
the 13 clinics.
At community level, PLHIV attend Drama shows, staged by RHSP that
have various HIV messages, targeting all community members, regardless
of age and HIV/AIDS status.
It is within this implementation framework that the integrated nutrition
education and counselling was designed and implemented.
1.2.2 Brief description of the integrated nutrition education and
counselling program
The pilot NEC program was initiated and implemented for six months,
from July 2010 till December 2010. It was initiated because the health
education messages given to the HIV/AIDS Care program clients lacked
standardised and targeted nutrition education messages for PLHIV.

11
In addition, there were no practical sessions and Information, Education
and Communication (IEC) materials to use in health education. Also, the
Drama shows staged didn’t include nutrition messages for PLHV.
Consequently clients experienced nutrition-related challenges that
compromise ART and other medication benefits. These would otherwise
be prevented if one received nutrition education.

12
2 LITERATURE REVIEW
2.1 Relationship between HIV and Nutrition
HIV compromises the body’s immune response and ability to resist
diseases, predisposes PLHIV to frequent opportunistic infections and
increases the body’s use and need for energy and nutrients. In addition,
HIV affects food intake, thus one does not meet the body’s nutrient
requirements, leading to malnutrition.
Malnutrition and HIV compromise ART benefits, further impair one’s
immune system, and increase vulnerability to Opportunistic Infections
(OIs) and hastens progression of HIV into AIDS (ECSA-HC et al., 2008,
RCQHC, 2008); (Bachou H. et al., 2006).
A compromised immune system affects food intake, and malnourished
PLHIV may not adhere to ART (RCQHC, 2008). Consequently, ART
affects food consumption and nutrient absorption, metabolism and
excretion through side effects (e.g. anaemia, nausea, vomiting) (FANTA,
2004); Kakitahi, 2008) and the cycle continues.

13
Nutrition is key in the care, treatment and support of PLHIV since energy
and nutrient requirements are increased to meet the increased metabolic
rate, better manage the disease and maximise ART benefits (Piwoz et al.,
2004). Failure to meet these nutritional needs due to poor food intake and
poor digestion and absorption/utilisation may lead to failure to adhere to
ART. In the absence of nutritional therapeutic care and support this may
result into organ failure and death.
To ensure holistic care, treatment and support of PLHIV, nutrition
interventions, especially NEC are integrated into HIV/AIDS programs.
These interventions are meant for PLHIV to use locally available food in
resource limited settings (FANTA, 2004).
In Uganda, one of the underlying causes of malnutrition among PLHIV is
lack of education as well as women empowerment (FANTA-2, 2010).
When the nutrition knowledge gap is filled through food-based
approaches, nutrition knowledge, attitudes and practices of PLHIV
improve. Approaches used include using indigenous food that is highly
nutritious and culturally acceptable; and targeted nutrition education,
(Aphane J. et al., 2002).

14
Increased consumption of all food types in the appropriate amounts,
balanced to suit their needs helps PLHIV to manage the treatment side
effects. This strengthens their immunity, increases resistance to OIs, and
improves food consumption and nutrient absorption.
Nutrition education and counselling, coupled with the ART, psychosocial
support, treatment of OIs and the recommended medical nutrient
supplementation given by RHSP, will lead to improved nutritional status
of PLHIV on the Care Program in the very long run.
2.2 Nutrition knowledge, attitudes and feeding practices among
PLHIV
There are very few studies done to assess nutritional knowledge, attitudes
and practices among PLHIV in Uganda and this has been linked to lack or
scanty knowledge of the importance of nutrition in the management of
HIV (Bukusuba J. et al., 2010).
15
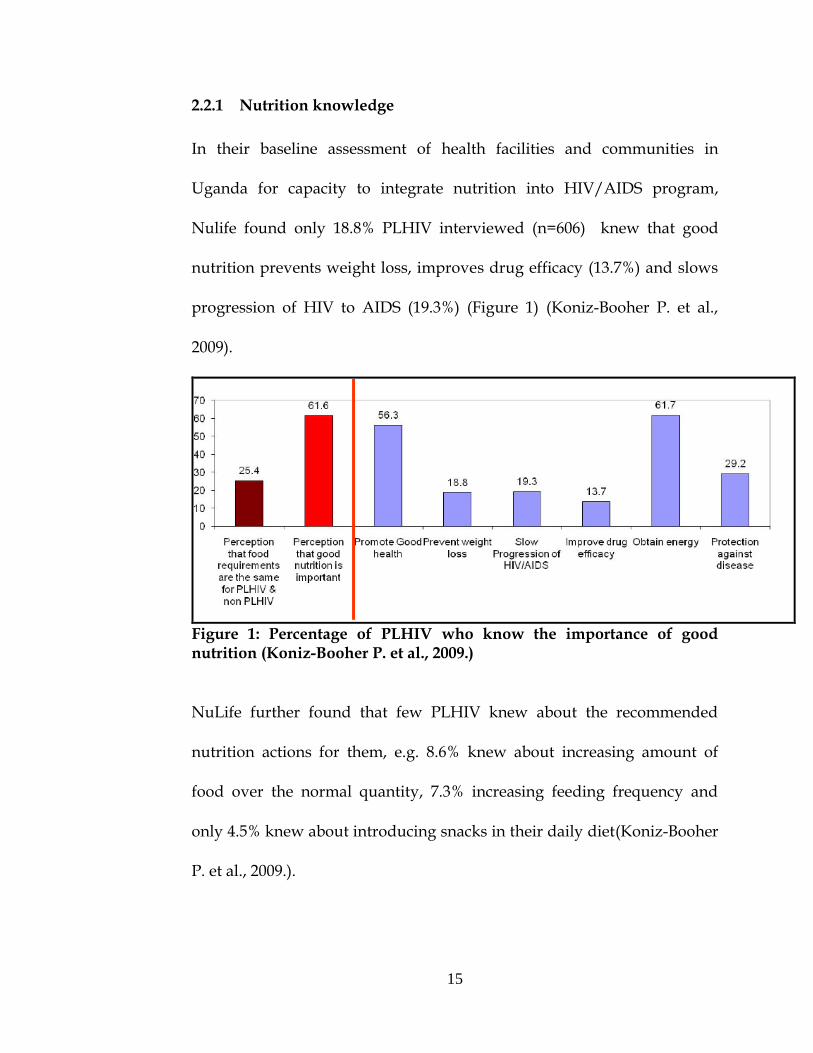
2.2.1 Nutrition knowledge
In their baseline assessment of health facilities and communities in
Uganda for capacity to integrate nutrition into HIV/AIDS program,
Nulife found only 18.8% PLHIV interviewed (n=606) knew that good
nutrition prevents weight loss, improves drug efficacy (13.7%) and slows
progression of HIV to AIDS (19.3%) (Figure 1) (Koniz-Booher P. et al.,
2009).
Figure 1: Percentage of PLHIV who know the importance of good nutrition (Koniz-Booher P. et al., 2009.)
NuLife further found that few PLHIV knew about the recommended
nutrition actions for them, e.g. 8.6% knew about increasing amount of
food over the normal quantity, 7.3% increasing feeding frequency and
only 4.5% knew about introducing snacks in their daily diet(Koniz-Booher
P. et al., 2009.).

16
In addition, only 16.5% and 1.6% knew about drinking plenty of water
and fluids and doing physical exercises respectively (Koniz-Booher P. et
al., 2009.).
In a study conducted among trained women LHIV in Eastern Uganda, to
assess the gaps in nutritional knowledge, attitudes and dietary practices,
only ―51.9% of the people interviewed understood the meaning of good
nutrition‖ and 45.1% knew about increasing the frequency of meals and
78.2% had consumed <3 meals in the preceeding 24 hours (Bukusuba J. et
al., 2010).
In Rakai district, despite giving HIV-positive mothers free formula as an
option for infant feeding to prevent MTCT of HIV and counseling on its
safe and hygienic use, mixed feeding (including formula) was largely
practiced, which was fatal (Kagaayi et al., 2008).
This practice depicts the nutrition knowledge gap that should be
addressed as a priority to avoid increases in infant mortality in Uganda.
Kagaayi’s findings highlight the fact that even when people are trained; it

17
is quiet challenging to positively modify behavior in rural settings, which
has serious implications towards nutritional programming.
2.2.2 Nutrition attitudes
In a study conducted in Eastern Uganda, majority (99.3%) of the women
LHIV interviewed understood the importance of consumption of balanced
diets (Bukusuba J. et al., 2010).
Bukusuba also found that understanding the meaning of good nutrition
was associated with consumption of a diversified diet. However, the same
study found that only 45.1% believed that increasing meal frequency is
important (Bukusuba J. et al., 2010).
NuLife, in her study conducted in 54 health facilities and communities in
Uganda found that 31.5% of the PLHIV interviewed thought that mixed
feeding for children <6 months old is advisable, while 44.2% thought that
breastfeeding provides the baby with protection from infections including
HIV (Koniz-Booher P. et al., 2009.).
18
These findings show mixed perceptions towards nutrition for PLHIV in
Uganda, which is important to address so that PLHIV have confidence in
modifying their feeding behavior.
2.2.3 Feeding Practices
(i) Feeding practices in Infants and children below 5 yrs
Much as exclusive breastfeeding is superior and is globally recommended
compared to all other feeding practices in resource limited settings, the
feeding practices are far from this.
It is gloabally known that exclusive breastfeeding is protective against
MTCT of HIV and all other infections among infants (Iliff P. J. et al., 2005,
RCQHC, 2008). However, An evaluation of a community- based service
program to prevent MTCT of HIV in Rakai district found that only 25%
exclusively breastfed their infants at one month postpartum and 18% at
six months (Kagaayi et al., 2008).
The same study found that mothers fed their infants on other foods, e.g.
cow’s milk (25%), mushroom soup (65%) and water (25%) at one month
19
(Kagaayi et al., 2008), which foods predispose infants to opportunistic
infections, regardless of their sero-status.
In a cross-sectional survey conducted among 235 HIV-positive mothers in
Mbale, Eastern Uganda, to compare feeding practices between infants and
children born to HIV positive mothers and the general population, 8.5%
(n=235) of HIV positive mothers exclusively practiced replacement
feeding (Fadnes et al., 2009) compared to 0.1% (n=727) in the general
population mothers.
In the same study, 64% infants born to HIV positive mothers received pre-
lacteal feeds, while only 28% HIV postitive mothers practiced exclusive
breastfeeding during the first three days of life(Fadnes et al., 2009).
In the same study, one-fifth of the infants below 6 months old were
exclusively breastfed (Fadnes et al., 2009). Also, more than half of the
infants (>75/150 infants) born to HIV positive mothers received mixed
feeding and solids before 6 months of age, which is quiet unfortunate.
Foods that were given to the infants below six months included water,
―non-human milk‖, ―bananas, maize, beans and alcoholic local
brew‖(Fadnes et al., 2009).

20
This study further found that the median duration of breastfeeding was 12
months and reasons for early cessation of breastfeeding included mothers’
sickness and their positive HIV sero-status (Fadnes et al., 2009).
The infant and child feeding practices quoted above depict mixed feeding,
the least safe infant feeding option that pre-disposes infants to a poor
nutritional status and vertical HIV transmission. It is a sure indication of
failure to or lack of proper knowledge to follow the safest feeding options
and adherence to guidelines.
(ii) Feeding Practices among adults
In a study done among women LHIV in Eastern Uganda, only 21.8% of
the people interviewed ate 3 or more meals in a day, while only 20.3%
consumed supplementary foods to meet their energy needs as
recommended for PLHIV (Bukusuba J. et al., 2010). The same study found
that foods that boost the immune system and build muscle are poorly
consumed.
21
In Northern Cape, South Africa, after two years of a nutrition education
program among adults in the general population, coupled with food aid,
participants’ knowledge and dietary practices improved by 10% and 5.9%
respectively (Walsh et al., 2003).
NuLife in her study conducted in 54 health facilities and communities in
Uganda found that 44.3% of pregnant and lactating women ate 3 meals,
12.4% ate two snacks and 14.2% consumed 3 meals and 3 snacks in a day.
In addition, barely 20% of children below 15 years consumed 3 main
meals and more than 3 snacks in day (Koniz-Booher P. et al., 2009.), yet
children LHIV require almost double their energy and nutrient
requirements.
Using the dietary diversity score, the same study found that in central
Uganda Region, PLHIV scored 4.2 and they mainly ate Legumes/pulses,
plantain, roots and tubers (Koniz-Booher P. et al., 2009.). This clearly
shows that in Central Uganda, fruits and vegetables are rarely consumed,
despite their role in boosting immunity among PLHIV.
Nutrition and feeding practices are largely affected by food availability,
which is also affected by seasonal variations (FANTA-2, 2010); knowledge

22
(Bukusuba J. et al., 2010) and food prices, thus certain foods are not
consumed as required even when they are produced. It is therefore
important to address the knowledge gap so that PLHIV can better manage
the limited food resources accessible.
3. CARE PROGRAM NEED FOR THE INTERVENTION,
JUSTIFICATION, CONCEPTUAL FRAMEWORK
3.1 Need for the NEC intervention
Integrating nutrition interventions, especially Nutrition Education and
Counselling (NEC) into HIV/AIDS programs ensures holistic care,
treatment and support to PLHIV. This is especially recommended in
resource limited settings to enhance the ART treatment benefits (Piwoz et
al., 2004).
The fellowship program was, therefore, an opportunity for RHSP to
initiate NEC pilot program activities into their community-based
HIV/AIDS Care program. The pilot NEC program was initiated and
implemented for six months, from July 2010 till December 2010.

23
The health education messages that were given to PLHIV lacked
standardised and targeted key nutrition education messages for PLHIV.
In addition, there were no practical sessions to further show the PLHIV
that the locally grown food is laden with nutrients for managing HIV.
Also, the program lacked Information, Education and Communication
(IEC) materials to use in health education. At community level, the PLHIV
get opportunities to watch RHSP Drama, however, this staged drama
lacked key nutrition messages for PLHV.
Consequently clients experienced nutrition-related challenges that
compromise ART and other medication benefits. These would otherwise
be prevented if one received nutrition education.
3.2 Justification
Routine field visits and patient dialogue revealed an existing nutrition
education and counselling gap both at program and client levels.
Therefore, improving client nutrition KAP was prioritised.

24
Since nutrition is a new concept at RHSP, the nutrition education and
counselling intervention would be the easiest to implement as a pilot
program. Also, it was preferred among all other nutrition interventions
because it is more sustainable to equip one with information than giving
them food to eat.
The NEC intervention, implemented as a pilot program, was most suitable
to implement within the RHSP framework. Its goal was to improve
PLHIV’s nutrition knowledge, attitudes and feeding practices. Imparting
knowledge unto PLHIV was best suited to achieve this goal.

25
3.3 Conceptual Framework
Malnutrition (macronutrient and micronutrient deficiencies e.g. weight
loss, wasting, ill bone health, vitamin and mineral deficiencies) in the
presence of HIV compromises ART benefits, impairs one’s immune
system, increases vulnerability to Opportunistic Infections (OIs) and
hastens progression into AIDS (ECSA-HC et al., 2008).
On the other hand, a compromised immune system leads to malnutrition
and food can affect ART efficacy. Also, malnourished PLHIV may not
adhere to ART (FANTA Project and AED, 2008).
Consequently, ART affects food consumption and nutrient absorption,
metabolism and excretion through side effects including but not limited to
anaemia, nausea, vomiting, anorexia (appetite loss), abnormal taste and
diarrhea (FANTA, 2004).
Nutrition is key in the care, treatment and support of PLHIV because all
their nutrient requirements (energy, protein, vitamins and minerals) are
increased to meet the increased metabolic rate, better manage the disease
and maximise ART benefits.
26
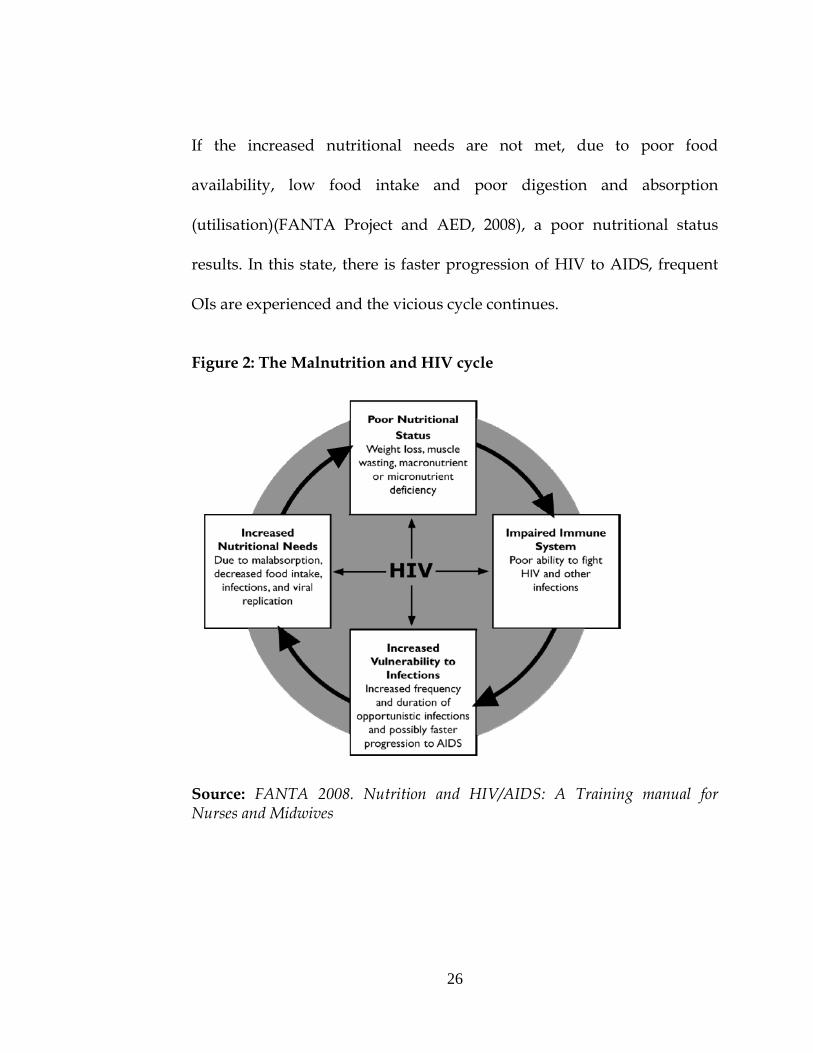
If the increased nutritional needs are not met, due to poor food
availability, low food intake and poor digestion and absorption
(utilisation)(FANTA Project and AED, 2008), a poor nutritional status
results. In this state, there is faster progression of HIV to AIDS, frequent
OIs are experienced and the vicious cycle continues.
Figure 2: The Malnutrition and HIV cycle
Source: FANTA 2008. Nutrition and HIV/AIDS: A Training manual for Nurses and Midwives

27
When nutrition interventions, especially nutrition education and
counselling are integrated into HIV/AIDS programs, using locally
available food and in resource limited settings (FANTA, 2004), PLHIV’s
nutritional knowledge improves.
When the targeted key nutrition messages for PLHIV are shared, their
nutrition knowledge, attitudes and feeding practices improve. A
knowledge base is created at the clinic level, which is anticipated to trickle
down to communities in the long run. There is increased consumption of
all food types in the appropriate amounts, balanced to suit their needs
(especially energy) and manage HIV.
As a result, PLHIV’s immunity is strengthened; there is increased
resistance to OIs, food consumption and nutrient absorption. This,
coupled with ART, psychosocial support, treatment of OIs and the
recommended medical nutrient supplementation given by RHSP, leads to
long-term improved nutritional status of PLHIV on the ART Program.

28
Figure 3: Benefits of nutrition interventions
Source: FANTA 2008. Nutrition and HIV/AIDS: A Training manual for Nurses and Midwives
29
4. PROGRAM OBJECTIVES
4.1 General Objective
The goal of this integrated NEC program was to contribute towards
empowering the PLHIV enrolled on the RHSP Care program to improve
their nutrition Knowledge, Attitudes and Practices (KAP).
4.2 Specific Objectives
4.2.1 To integrate nutrition into the different on-going research and
service programs at RHSP.
4.2.2 To improve nutrition knowledge, attitudes and feeding practices of
PLHIV enrolled on the Rakai Health Sciences HIV/AIDS Care
program that received the NEC Intervention.

30
5 IMPLEMENTATION APPROACHES
5.1 Target population
Since the fellowship was only two years, with 25% of the time spent at the
MakSPH for short courses, it was agreed that efforts should be focussed
on the Care program, since PLHIV had the greatest need for this
intervention.
The NEC program was conducted among all PLHIV (on ART and Pr-
ART), enrolled on the RHSP HIV/AIDS Care program, including children
(below 15 years). Institutional staff involved in provision of services to the
PLHIV, specifically, the Care Program, Community mobilisation,
Comunity resident HIV counsellors, Quality control and RHSP
management departments participated in this program too.
5.2 Program site
The NEC program was implemented in Rakai District, in 13 clinics,
situated at Government owned health centres in Urban, Semi-urban and
rural settings. Rakai district is situated between 31o and 32o longitudes
and 0o and 1o latitudes, in south-western Uganda. It is bordered by

31
Masaka, Mbarara, Lyantonde districts and Tanzania. Figure 1 below
shows this location.

32
Figure 4: Map showing the Rakai District Location
The different clinics in which the NEC program was implemented are
situated in: Kalisizo, Kasaali, Kabira, Nabigasa, Kasasa, Lwanda, Kifamba,
Kakuuto, Lyantonde, Lwamaggwa, Kyebe, Buyamba and Kibaale. Figure
5 shows the clinic physical location in Rakai district.

33
Figure 5: Map showing the different clinic location
34
5.3 The NEC Intervention
Before NEC implementation, routine field visits and patient dialogue
revealed an existing nutrition education and counselling gap both at
program and client levels. Therefore, improving client nutrition KAP was
prioritised.
Nutrition education was given using different communication channels;
theoretical workshops/trainings, Drama and Cooking demonstrations.
Elements of nutrition education promoted are summarized into: basic
nutrition, specific nutrition for PLHIV, using locally available food to
attain good nutrition at family level, home recipe formulation, food
preparation, hygiene and safety.
5.3.1 Theoretical /workshops
Internationally tested, accepted and recommended key nutrition messages
for PLHIV that were developed by the Regional Center for Quality of
Health Care (RCQHC) and Food and Nutrition Technical Assistance
(FANTA) were adapted and adopted to Rakai conditions.
35
Before each session, expectations were collected, and the trainings were
tailored to the PLHIV’s needs. Box 1 below shows the most common
expectations.
There are 8 themes, each with key nutrition messages for PLHIV that were
promoted. The themes are:
1. Have periodic nutrition assessments done (especially weight)
2. Increase energy intake by eating a variety of foods, especially
energy rich foods. Increase the frequency of meals, especially if you
are sick
3. Drink plenty of clean and safe (boiled or treated) water
4. Live positively and practice a healthy lifestyle by avoiding risky
behaviors
Box 1: PLHIV’s most common nutrition education PLHIV’s expectations
Nutrition for people/children on ART
Infant and or child feeding
Nutrition for pregnant and lactating mothers
Benefits of different classes of foods for the HIV positive
Frequency of feeding for people on ART
The danger of mixing alcohol and ART
Preparation/cooking and consumption of food for PLHIV
Benefits of fermented porridge to clients on ART
Learn how to mix foods to maximise nutrients
Food and drug interactions
When to take drinks e.g. water, juice, and milk (before/after meals?)
Using food to fight infections

36
5. Maintain high levels of hygiene and sanitation
6. Get physical activity (exercise)
7. Seek early treatment of infections and use dietary practices to
manage symptoms when possible
8. Manage food and drug interactions or drug side effects
The key nutrition messages were adapted to Rakai conditions by using
examples of locally available foods, and structuring sentences in a way
that is culturally acceptable in Rakai.
In addition, the fellow and the RHSP staff translated the key messages
into Luganda, the commonly used language to standardise what is
communicated to the PLHIV in the Pilot clinics. For each clinic, NEC was
done regularly and is currently done on Schedule.
5.3.2 Drama
The key nutrition messages for PLHIV were incorporated into the original
HIV and ARVs Drama.
A community-based drama team
was identified and trained in
basic and nutrition for PLHIV
(figure 6).
Figure 6: The fellow (in blue) training the drama
team in the field
37
The fellows and a few staff used the internationally recommended
RCQHC/FANTA guidelines for nutrition for PLHIV to train the drama
team. Several rehearsals were made both in the community and the main
field station for staff to have an input into the drama.
The drama team wrote a draft script that went through a series of editing
by the fellow and the Health education and Mobilisation team until a final
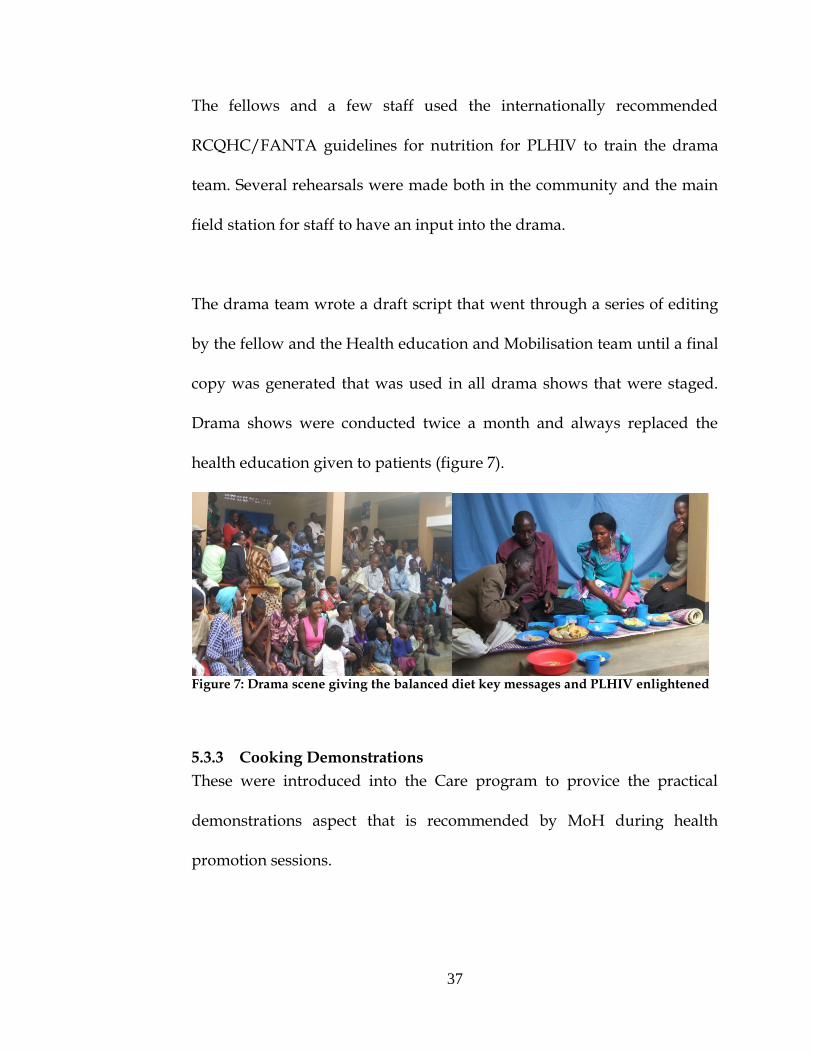
copy was generated that was used in all drama shows that were staged.
Drama shows were conducted twice a month and always replaced the
health education given to patients (figure 7).
Figure 7: Drama scene giving the balanced diet key messages and PLHIV enlightened
5.3.3 Cooking Demonstrations
These were introduced into the Care program to provice the practical
demonstrations aspect that is recommended by MoH during health
promotion sessions.

38
Locally available, culturally acceptable and highly nutritious food was
used in these demonstrations. These sessions were conducted twice a
month too, like the Drama, to enhance client nutrition attitude and
practice improvement.
The dishes prepared included but not limited to:
Go foods (energy giving) - Matooke, Rice, Cassava, Sweet Potatoes,
potatoes and Pumpkins. These included snacks like: Millet porridge,
maize porridge, tea, milk, roasted ground nuts mixed with corn.
Grow foods (protein rich): Ground nut source, beans, gold fish, eggs,
dried tilapia and mushrooms. Salt was added to the dishes to taste and to
add the iodine nutrient in the diet.
Glo foods (protective): Green leafy vegetables, Cabbage, egg plants, green
pepper, bitter tomatoes. Fruits promoted were: passion fruits, oranges,
tangerines, and other fruits in season.
Extra energy foods: Avocadoe,
Honey, Sugar, Sugar cane,
cooking oil and margarine
(Figure 7).
These foods were acquired
Figure 8: Picture showing some protective and
extra energy foods available in Kakuuto, Rakai

39
from the communities in which the clincs are situated. It was a varied
selection of foods, since some clinics are based in urban, semi-urban and
rural settings. It is notable to say that year round, people in this region are
able to have a balanced diet, if taught how to use their limited resources in
an organized way.
With the Nutritionist’s guidance (fellow), trained patient
volunteers/leaders (Peer Smarts) and Care program staff spearheaded the
practical sessions, which encouraged other patients to get involved and
learn as they participated in these sessions.
This provided a relaxed learning environment, enhanced their learning
from the experiences shared, testimonies given by fellow patients and led
to individual nutrition KAP improvements.
Care Program Volunteers (Peer Smarts) and Staff training
Peer Smarts/Care program
volunteers are PLHIV that
have excelled in taking their
medication and generally
following the health
Figure 9: A Peer Smart ready to give a porridge
mixture demonstration in Kakuuto
40
workers’ guidance. These are proactive and identified from people
enrolled on the RHSP Care program, who ably carry out health education
sessions (Figure 9), take patient vital signs and routinely register patients
for treatment refills.
The fellow trained Peer Smarts in basic nutrition and nutrition for PLHIV,
importance of good
nutrition, consequencies
of poor nutrition and the
key nutrition messages
for PLHIV (Figure 10).
In partnership with MoH staff, the fellow trained the Care program staff
and local government health workers in basic nutrition, nutrition for
PLHIV. In addition, we trained staff in the promoted themes and key
messages, and they further had role plays and cooking demonstrations
while practicing delivering the messages.
Figure 10: Peer Smarts serving people after a cooking
demonstration

41
Staff training was important, since nutrition is a new concept at RHSP;
staff were required to understand the concept and spend enough time
learning the themes. I am happy to report that they are currently confident
in giving nutrition education messages for PLHIV.
Also, the fellow briefly trained several groups of Community Health
Workers (CHWs) that are based in the RHSP target communities. These
trained in basic nutrition, importance of good nutrition and consequencies
of poor nutrition in an HIV/AIDS condition.
The Rakai Community
Advisory Board (CAB)
received a similar training,
and blessed the intervention
(Figure 7).
Figure 7: The Rakai CAB members pose for a group
picture after a nutrition training (fellow in a red top).

42
6 OUTPUTS
6.1 Nutrition messages for PLHIV – Luganda and English versions
The adapted, adopted and translated key nutrition messages for PLHIV
were compiled and a copy shared with the Institution Quality Control
Department (QCD). This resource is ready for use as the Institution plans
to roll out to program to other areas of operation. The different versions
of the messages are attached to this report (Appendix 11.1).
6.2 Drama script
A complete drama script with key nutrition and HIV/AIDS messages in
the local language (Luganda) was designed and produced by the fellow.
This script was used to stage all the drama shows in the nutrition
program. This resource is available for the Institution to use as they plan
to roll out the practical sessions to other program clinics (Appendix 11.2).
6.3 M & E plan
An M & E plan was drafted for the NEC program, specifically focussing
on activity follow up and capturing information on the attributes of
interest. Indicators/markers of change that would show the NEC program
progress and probable changes were identified.
43
The markers of change that were used to design the Monitoring and
Evaluation (M & E) plan for the NEC program include:
Knowing the three main food groups and their uses
Ability to know what foods belong to which food groups,
Knowing food servings and portions.
Reasons for eating food from all food groups at all times
Importance of drinking plenty of water throughout the day
Importance of monitoring their weight regularly
Knowledge of how to manage HIV/ART side effects using locally
available food.
The complete M & E plan and tools for data collection will be shared in a
different document.
6.4 NEC Program evaluation proposal
The implemented NEC pilot program was done as part of RHSP’s
HIV/AIDS Care health education package. It aimed at contributing
towards empowering PLHIV who are enrolled on the RHSP Care
Program to improve their nutrition Knowledge, attitudes and feeding
practices.
44
However, the nutrition knowledge, attitudes and feeding practices of
PLHIV who participated in the pilot program are not known. Nutrition
being a new theme at RHSP; the PLHIV’s perceptions of the NEC pilot
program and overall challenges, experiences and lessons learnt have never
been documented. Narrative information captured in the routine
quarterly reports cannot be used to make informed management decisions
for program scale up.
Therefore, it is important to evaluate this program and a ready proposal to
evaluate this program was designed by the fellow, reviewed; and it awaits
approvals and funding for implementation. The designed evaluation uses
both quantitative (survey) and qualitative [Focus Group Discussions –
(FGDs), and Key Informant Interviews (KIIS)] data collection methods and
the tools to use and consent forms are ready for approval (Appendices 11.3
– 11.4).
6.5 Reference books
A list of main reference books used in the desigining of the NEC program
as well as its evaluation is attached (Appendix 11.5) and copies have been
added to the resources center for future reference. Soft copies of similar
resources were forwarded to the resource center too. More nutrition

45
resources can be accessed from the Ministry of Health headquarters in
Kampala.
6.6 Other outputs
6.6.1 Staff trained
I trained 128 staff members in nutrition for PLHIV. These constituted of
Medical Doctors, Clinicians, nurses, counselors and clerical staff. In
addition, quality control and community mobilizations departmental staff
participated in these trainings. This activity aimed at equipping staff with
skills they can use in their different operational programs.
6.6.2 Government and Community Health workers’ trained
The fellow trained 120 Government and community health workers in
nutrition for PLHIV. Since the Care program partners with the local
government, these had to be trained for them to give similar messages to
communities where the clinics are based. Also, in the absence of the Care
program staff, governmental and community health workers can provide
the nutritional counselling desired by patients.

46
6.6.3 CAB members trained
A total of 12 CAB members received half a day’s training in Nutrition for
PLHIV. This training meant to enlighten this advisory board of the
addition of the nutrition intervention onto the Care program; however,
they also needed to understand its importance to health.
6.6.4 Drama sessions staged
A total of 9 Drama sessions were staged in 3 clinics: Kalisizo, Kakuuto and
Lwamaggwa. These aimed at improving PLHIV’s attitudes to good
nutrition using locally available foods. People learnt as well as getting
some entertainment to brighten up the day.
6.6.5 Cooking demonstrations conducted
A total of 8 cooking demonstrations were conducted in three clinics:
Kalisizo, Kakuuto and Lwamaggwa. These provided a relaxed
environment where PLHIV participated fully and enjoyed the activity as
they learnt form their peers.
6.6.6 Nutrition education theoretical/workshops conducted
Approximately 150 theoretical nutrition education sessions were
conducted.

47
7 LESSONS LEARNT
Simple nutrition and health messages go a long way in improving
people’s health and change lifestyles. Staff and PLHIV appreciated how
the NEC program was well integrated into the Care Program and how it
enriched the Care program. PeerSmarts and their colleagues had this to
say (Box 2):
The Care program staff appreciated the fact that innovative ways of
giving HE positively impacted on the PLHIV. For example, ―Drama
brought out the reality, yet messages were maintained in an agreed upon format;
Box 2: Lessons learnt from the NEC program
We used to just eat lots of food (omuwumbo gw’amatooke) but we didn’t
know the nutrients and their uses in the food we ate. We currently
diversify our diets, regardless of the seasons.
Since we learnt things practically and for a long time, we make sure we
look for foods that we do not have. We constantly have energy and we
don’t get frequent illinesses.
We have shared information with our care takers, they have also learnt to
look out for our food interests and we currently receive better Care.
―Men appreciated the cooking demonstrations and other theoretical
sessions, since we didn’t leave them out‖, says one of the ladies.
o We no longer burn our oil and onions till they are black, we know
its effects on our health
o We currently cook vegetables for a short period, to avoid
destroying the nutrients
o We are trying out our proposed recipes, e.g porridge with
avocadoe; it is really nutritious.

48
People have become knowledgeable, some clinics still have their teaching material
displayed and they teach/remind each other whenever they get a chance”, says
one of the staff members.
8 STRENGTHS AND WEAKNESSES OF THE NEC PROGRAM
8.1 Strengths
a) The staff, volunteers, CHWs, government health workers and
PLHIV all received training in nutrition for PLHIV. This is a
sustainability strategy and this work can be continued.
b) The NEC was integrated; the concept is currently promoted in
combination with medication.
c) The NEC program was so relevant to all those who
participated. Most especially, focusing on nutrition for PLHIV
fitted in well with the Care Program and the simple frequent
illinesses reduced (from Patient confessions).
d) It was participatory; staff and PLHIV were all involved. Staff
learnt what nutrition contributes towards patient’s health and
they whole heartedly promoted it.
e) It was practical and enjoyeable; yet met the key messages
communication targets. The cooking demonstrations and
drama introduced flavor to the care program

49
f) Staff were committed and they learnt the new concept and
themes quite quickly
g) It is sustainable, since we used locally available foods to convey
the nutrition messages
8.2 Weaknesses
a) The IEC materials that were used could not be printed (the ones
from one of the reference manuals). The printed ones from MoH
didn’t come through. This has limited the information to pass on.
b) The NEC program didn’t provide food (therapeutic food) for
PLHIV, neither did they provide for the severely malnourished,
whose immune systems were compromised. In addition, there is no
community-based Therapautic Center (CTC) to refer such people
to, for rehabilitation using locally available foods.
c) Most times, clinics were busy, so, sessions were cut short, yet
PLHIV had a lot of questions to ask. Some sessions were not fully
covered, e.g. nutrition for pregnant and lactating mothers and child
care
d) Staff were over-loaded; sometimes they and PLIVH would be
divided between the clinical work and nutrition teachings.
50
9 CHALLENGES FACED AND GAPS IDENTIFIED
9.1 Challenges
a) Food security – it is a challenge to tell people to balance their meals
and in return they tell you that some of the foods are not
available/are not in season. Seasonal variations affected the feeding
practices.
b) Change of the Care program set up – It is currently hard to follow
up on the different topics taught, because PLHIV do not visit the
clinics on the same appointment day like before (every after two
weeks, 1 month, 2 or 3 months). Patients no longer meet in big
numbers to share testimonies and learn from one another.
c) Some PLHIV have limited income to supplement their diets – they
are not able to economically access the foods they do not grow.
d) Like other community based program, feeding behaviour change is
quite slow among some PLHIV. These would have benefited from
frequent community trainings, which are not offered.

51
9.2 Gaps identified
a) The NEC activities were not planned for from the start of the Care
Program.
b) Not all clinics received practical sessions, yet these communicated
more to the PLHIV than the theoretical sessions.
52
10 CONCLUSION
It was a great learning experience, I enjoyed working in a research setting
and learning from others. It was so fulfilling to teach people the basics in
nutrition and how the concept improves health. I must mention that
egardless of education level, all people who participated in this program
immensely appreciated my contribution to their achieving healthier lives.
Since this is a new concept at RHSP, it would have been easier starting the
integratation of the intervention from the strategic plan downwards. It
would have been more appreciated and maybe, more promoted.
In addition, a nutrition unit would have been handy in carrying out the
activities, especially in my absence (off station) during the periodic
classes.
Also, in the absence of livelihood interventions, food security at
community level is a challenge. People had to rely on the meager
resources for them to practice what they learnt from the nutrition
trainings. They would also be faced with prioritizing, say, between using
maize flour for a snack or making ugali out of it for a meal.

53
11 RECOMMENDATIONS
Include nutrition in RHSP’s strategic plan/mandate. This
would ease application and winning of grants to do nutrition
work. Also, such activities should be embedded into the RHSP
budget as early as possible.
Start nutrition unit, however small it may be. This would
ensure daily nutrition education, the way HIV and ART
messages are given. There should be staff (a focal person) to
further the initiated program. The equipment to carry out the
work is available; linkages were made with MoH, MakSPH,
and other partners who can constantly provide technical
backstopping.
Conduct nutrition re-trainings for staff that are currently
carrying out nutrition education and counselling at the field
level. This will keep them equipped with up to-date nutrition
knowledge and skills.
Evaluate the Pilot nutrition program, to generate information
for smooth rolling out of the nutrition intervention to other
Institution programs.
54
Extend the intervention to the community level, so that all
people can receive the guidance, to avoid stigmatization of
PLHIV.
A Nutrition education Radio program could do better in
reaching the community.
Think of adding livelihood interventions to the NEC program
to bridge the gap between months of plenty and those of food
scarcity. These could be agricultural, marketing, or income
generating activities other than agriculture. These would aim
at ensuring food security at household level.
55
12 REFERENCES
APHANE J., CHADHA M.L. & M.O., O. Year. Increasing the consumption of micronutrient-rich foods through production and promotion of indigenous foods. In: KALB, T., ed. FAO-AVRDC International Workshop 5-8 March 2002 2002 Arusha, Tanzania. Shanhua, Taiwan: FAO.
BACHOU H., THORKILD T., DOWNING R. & TUMWINE, J. K. 2006. Severe malnutrition with and without HIV-1 infection in hospitalised children in Kampala, Uganda: differences in clinical features, haematological findings and CD4+ cell counts. Nutrition Journal, 5.
BUKUSUBA J., KIKAFUNDA J.K. & WHITEHEAD, G. R. 2010. Nutritional Knowledge, Attitudes and Practices of Women living with HIV in Eastern Uganda. Journal of Health, Population and Nutrition, 28, 182-188.
ECSA-HC, FANTA PROJECT, AED & LINKAGES, P. 2008. Nutrition and HIV/AIDS: A training Manual for Nurses and Midwives. In: ECSA-HC (ed.). Arusha, Tanzania: AED.
EKORU, K. 2007. Nutritional status and change in nutritional status among HIV-Infected adults initiating Antiretroviral Therapy at selected Health Facilities in Uganda. . Washington, DC.
FADNES, L. T., ENGEBRETSEN, I. M., WAMANI, H., SEMIYAGA, N. B., TYLLESKAR, T. & TUMWINE, J. K. 2009. Infant feeding among HIV-positive mothers and the general population mothers: comparison of two cross-sectional surveys in Eastern Uganda. BMC Public Health, 9, 124.
FANTA-2 2010. The analysis of the Nutrition Situation in Uganda. Washington: AED.
FANTA 2004. HIV/AIDS: A Guide for Nutritional Care and Support. 2nd
ed. Washington DC: AED. FANTA PROJECT & AED 2008. Nutrition Care for People Living With
HIV And AIDS (PLHIV). In: AED (ed.) Training Manual for Community and Home-Based Care Providers - Facilitator's Guide. Kampala: AED.
GILLESPIE S., HADDA, L. & ROBIN, J. 2001. HIV/AIDS, Food and Nutrition Security: Impacts and Actions. Washington DC: IFPRI.
ILIFF P. J., PIWOZ, E. G., TAVENGWA N. V., ZUNGUZA C. D., MARINDA E. T., NATHOOD K. J., MOULTONE H. L., WARDF B. J., THE ZVITAMBO STUDY GROUP. & HUMPHREY, H. J. 2005.

56
Early exclusive breastfeeding reduces the risk of postnatal HIV-1 transmission and increases HIV-free survival. AIDS, 19, 699-708.
KAGAAYI, J., GRAY, R. H., BRAHMBHATT, H., KIGOZI, G., NALUGODA, F., WABWIRE-MANGEN, F., SERWADDA, D., SEWANKAMBO, N., DDUNGU, V., SSEBAGALA, D., SEKASANVU, J., MAKUMBI, F., KIWANUKA, N., LUTALO, T., REYNOLDS, S. J. & WAWER, M. J. 2008. Survival of infants born to HIV-positive mothers, by feeding modality, in Rakai, Uganda. PLoS One, 3, e3877.
KONIZ-BOOHER P., KYENKYA M., NANGAI R., NUWAGABA D. & KIGOONYA, A. 2009. Facility Readiness to Introduce a Comprehensive Nutrition Package for PLHIV in Uganda. The Uganda Nutrition Congress. Kampala, Uganda.
MASHOO, E. 2010. Nutrition advocates call more support Uganda Health Reporter. Kampala: Uganda Communicationa Alliance.
MOH 2003. The Uganda National Food and Nutrition Policy. In: PARLIAMENT (ed.). Kampala: Government of Uganda.
MOH 2009. Comprehensive Nutrition Care for People Living with HIV/AIDS: Facility level participant's manual. In: MOH (ed.). Kampala, Uganda: Ministry of Health.
MOH May 2006. Nutrition care and Support for People Living with HIV/AIDS in Uganda. In: MOH (ed.). Kampala.
PATON NI, SANGEETHA S, EARNEST A & R, B. 2006. The impact of malnutrition on survival and the CD4 count response in HIV-infected patients starting antiretroviral therapy. HIV Medicine, 7, 323 - 330.
PIWOZ, E., BONNARD, P., CASTLEMAN, T., COGILL, B., ELDER, L., TEMANCUS, S. & TANNER, C. 2004. Nutrition and HIV/AIDS: Evidence, Gaps, and Priority Actions. Washington: FANTA, AED.
RCQHC 2008. Nutrition Care for People Living With HIV And AIDS (PLHIV): Training Manual for Community and Home-Based Care Providers - Facilitator's Guide. Kampala: AED.
REPUBLIC, OF & UGANDA February 2011. Uganda Nutrition Action Plan 2010 - 2015: Scaling-up Multi-Sectoral Efforts to Establish the Nutritional Foundation for Uganda’s Development. Kampala: National Planning Authority.
RUHANGARIYO, D. 2010. Ten things a journalist should know about nutrition. . Uganda Health Reporter. Kampala: Uganda Health Communications Alliance.

57
SCN 2004. 5th Report on the world nutrition situation: Nutrition for Improved Development outcomes. In: SCN (ed.). Geneva: United Nations System: Standing Committee on Nutrition.
STUART GILLESPIE, LAWRENCE HADDA & JACKSON, R. 2001. HIV/AIDS, Food and Nutrition Security: Impacts and Actions. Washington DC: IFPRI.
UAC 2007. Moving Towards Universal Access: National HIV & AIDS Strategic Plan 2007/8 - 2011/12. . Republic of Uganda.
UBOS & MII 2007. Uganda Health and Demographic Survey 2006. In: MOH (ed.). Calverton, Maryland, USA: UBOS and Macro International Inc.
UNAIDS 2008. Framework for Operations and Implementation Research in Health and Disease Control Programs. Geniva: UNAIDS.
WALSH, C. M., DANNHAUSER, A. & JOUBERT, G. (eds.) 2003. Impact of a nutrition education programme on nutrition knowledge and dietary practices of lower socioeconomic communities in the Free State and Northern Cape.

58
13 APPENDICES
13.1 Promoted key nutrition messages for PLHIV
English Version Clinical Nutrition Practice
Key Message Explanation of the message
1. Have periodic nutrition assessments done (especially weight).
If you have HIV-related symptoms, get weighed every month.
If you do not have HIV related symptoms, get weighed every 3 months
Unintentional weight loss or gain may imply poor health and may lead to hospitalization.
Keep a record of your weight in a book or on a weight chart.
This allows you to track your weight change and take action early if there are problems.
Seek clinical care if you lose more than 6 kg of weight in 2 or 3 months.
Such quick weight loss indicates poor health or eating habits.
When possible, ask the health provider to calculate your body mass index (BMI).
BMI under 18.5 indicates nutrition risk.
2. Increase energy intake by eating a variety of foods, especially energy rich foods. Increase the frequency of meals, especially if you are sick.
Eat locally available and affordable foods from each food group to develop a varied diet and increase energy intake.
PLHIV need to consume more energy every day than people of the same age, sex and physical activity who are not infected with HIV to make sure the body gets all the nutrients it needs.
Eat five times a day (three meals and two snacks in a day).
Because HIV affects digestion and absorption, you need to eat small meals often, especially when you are sick, to get the amount of energy your body needs
Eat foods from the different food groups at each meal.
Staple foods give energy, body-building foods build muscle and give strength, and fruits and vegetables

59
Clinical Nutrition Practice
Key Message Explanation of the message
strengthen immunity.
Enrich meals with energy-dense foods such as groundnut paste, avocadoes, oil/fat, sugar or honey or milk powder.
Most staple foods are low in energy and nutrient density and therefore need to be enriched or fortified.
Eat supplementary foods that contain high levels of energy, protein and micronutrients, such as corn-soy blend, where they are available and affordable.
If you have no appetite or are not eating enough, ask caregivers to help obtain and prepare food and help you to eat.
3. Drink plenty of clean and safe (boiled or treated) water.
Drink about 8 glasses of clean, safe water a day.
Drinking unclean, un-boiled water increases the risk of opportunistic infections in PLHIV, whose immune systems are weak, and can lead to severe diarrhoea and hence weight loss.
Boil or treat drinking water. To avoid food borne diseases and other opportunistic infections
Have enough clean, safe drinking water in the home at all times for drinking and taking medicine.
To avoid dehydration
To provide a good medium for the medication to work and to digest food well
4. Live positively and practice a healthy lifestyle by avoiding risky behaviors.
Practice safer sex (ask the community health worker or health care provider for condoms if needed).
Unsafe sex practices can lead to re-infection with HIV and hasten progression of HIV to AIDS. It is important to avoid infecting others.
Avoid alcohol, especially if taking medicines.
Alcohol interferes with digestion, absorption, storage and utilization of food, nutrients and medication.
Avoid smoking cigarettes and Smoking interferes with
60
Clinical Nutrition Practice
Key Message Explanation of the message
taking non- prescription drugs. appetite and increases the risk of cancer and respiratory infections, particularly tuberculosis.
Avoid eating junk foods such as chips and sodas and sugary foods such as cake and candy.
Most sweetened, coloured drinks sold in shops contain water, sugar, food colour and artificial flavour—they are not fruit juice.
Junk foods do not have enough energy for PLHIV; they can also cause nausea, diarrhoea, vomiting, due to the excess oil used to cook them.
Seek help to manage depression and stress.
Stress and depression may interfere with appetite and hence food intake.
Get enough rest. To renew your strength and proper functioning of the immune system
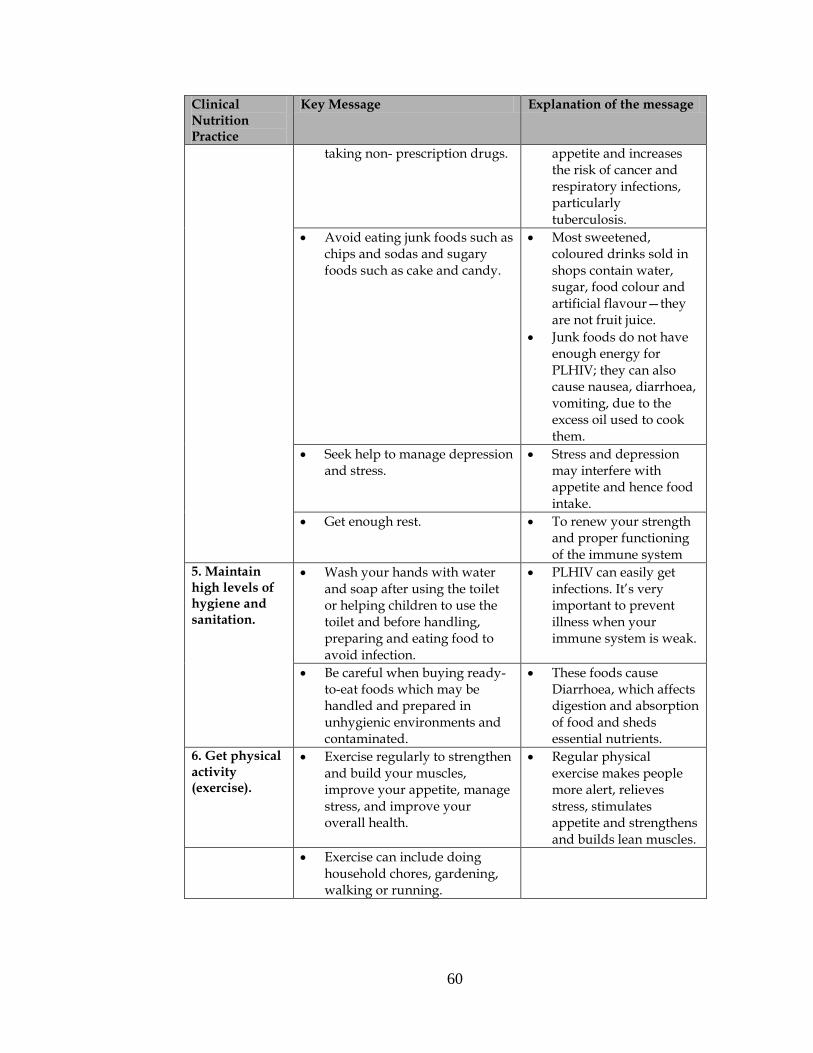
5. Maintain high levels of hygiene and sanitation.
Wash your hands with water and soap after using the toilet or helping children to use the toilet and before handling, preparing and eating food to avoid infection.
PLHIV can easily get infections. It’s very important to prevent illness when your immune system is weak.
Be careful when buying ready-to-eat foods which may be handled and prepared in unhygienic environments and contaminated.
These foods cause Diarrhoea, which affects digestion and absorption of food and sheds essential nutrients.
6. Get physical activity (exercise).
Exercise regularly to strengthen and build your muscles, improve your appetite, manage stress, and improve your overall health.
Regular physical exercise makes people more alert, relieves stress, stimulates appetite and strengthens and builds lean muscles.
Exercise can include doing household chores, gardening, walking or running.
61
Clinical Nutrition Practice
Key Message Explanation of the message
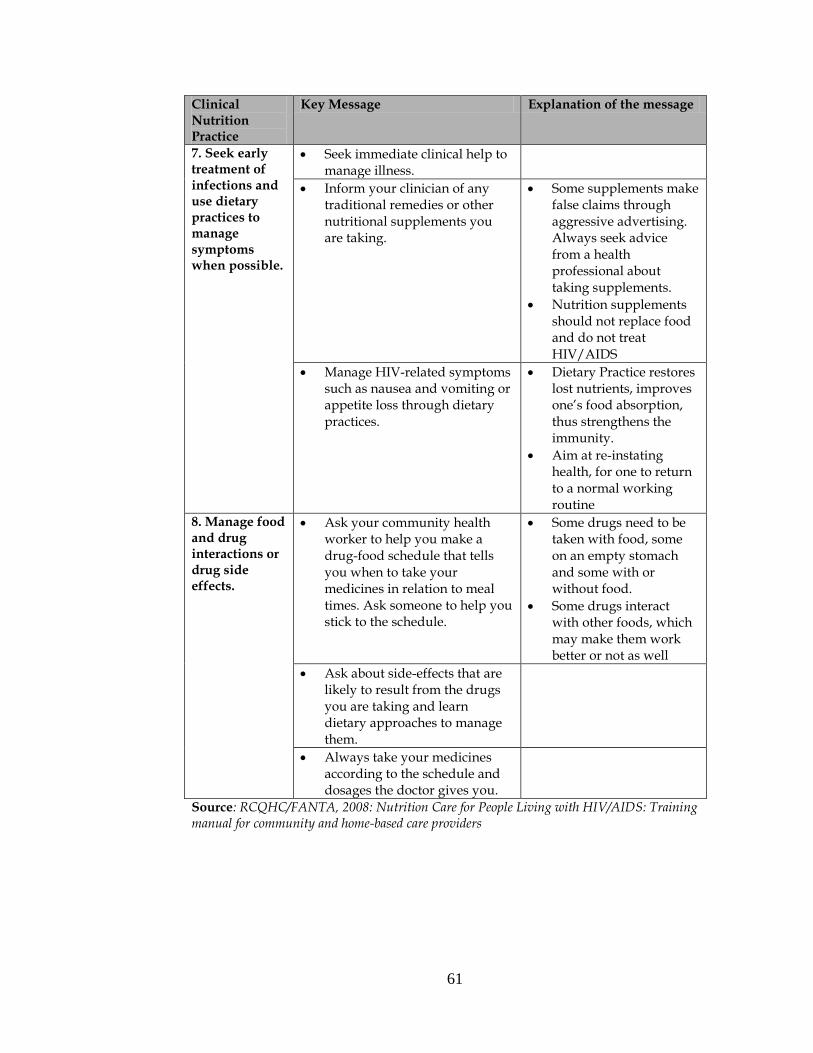
7. Seek early treatment of infections and use dietary practices to manage symptoms when possible.
Seek immediate clinical help to manage illness.
Inform your clinician of any traditional remedies or other nutritional supplements you are taking.
Some supplements make false claims through aggressive advertising. Always seek advice from a health professional about taking supplements.
Nutrition supplements should not replace food and do not treat HIV/AIDS
Manage HIV-related symptoms such as nausea and vomiting or appetite loss through dietary practices.
Dietary Practice restores lost nutrients, improves one’s food absorption, thus strengthens the immunity.
Aim at re-instating health, for one to return to a normal working routine
8. Manage food and drug interactions or drug side effects.
Ask your community health worker to help you make a drug-food schedule that tells you when to take your medicines in relation to meal times. Ask someone to help you stick to the schedule.
Some drugs need to be taken with food, some on an empty stomach and some with or without food.
Some drugs interact with other foods, which may make them work better or not as well
Ask about side-effects that are likely to result from the drugs you are taking and learn dietary approaches to manage them.
Always take your medicines according to the schedule and dosages the doctor gives you.
Source: RCQHC/FANTA, 2008: Nutrition Care for People Living with HIV/AIDS: Training manual for community and home-based care providers

62
Luganda Version Ebikulu ebitunulirwa mu ngeri abantu gyebalina okwerisamu, obubaka obugiwagira wamu n’enyinnyonnyola yabyo
Engeri ey’omugaso gyosobola okwerabiriramu n’okwerisa
Obubaka obukulu Enyinnyonnyola y’obubaka
1. Genda bakwekebejje buli luvanyuma lwe bbannga eggere ku ndya ennungi (okusingira ddala okupima obuzito)
Bwoba nga olina obubonero obuletebwa akawuka ka sirimu, olina okugenda bakupime obuzito buli luvanyuma lwa mweezi gumu.
Bwoba nga tolina bubonero buletebwa kawuka ka sirimu, olina okugenda bakupime obuzito buli luvanyuma lwa myeezi esatu.
Okukendera oba okuteekako obuzito mu butali bugenderevu kiyinza okutegeeza embeera yobulamu embi era kiyinza okukuviramu okuwebwa ekitanda mu ddwaliro.
Kuuma bulungi ebivudde mu kupima obuzito bwo mu kitabo oba ku ka kaadi.
Kino kikuyamba okugoberera enkyukyuka eziri mu buzito bw’omubiri gwo era nokufuna ekyokukola mu bwangu bwewabaawo obuzibu..
Noonya obujjanjabi/tukirira omusawo bwoba okendede obuzito obussusa kilo mukaaga(6) mu banga ery’emyeezi ebiiri oba esatu.
.
Okukendera mu obuzito mu bwangu bwebutyo kiraga embeera yobulamu embi oba engeri gyewemanyizamu mubyendya..
Bwekiba kisoboka, saba omusawo agerageranye obuzito bwo no buwanvu. (Body Mass Index)
Obuzito no buwanvu (BMI) bwekka wansi wa 18.5 kiba kiraga nti endya ennungi esobozesa omuntu okubeerawo obulungi mumbeera yobulamu ennungi eri mukatyabaga.
Lya emmere eyabulijjo era esoboka mu bika by’emmere eby’enjawulo
Abantu abalina akawuka ka sirimu beetaaga okukozesa amaanyi mangiko buli

63
Engeri ey’omugaso gyosobola okwerabiriramu n’okwerisa
Obubaka obukulu Enyinnyonnyola y’obubaka
2. Yongera amaanyi mumubiri ng’olya ebika by’emmere eby’enjawulo naddala emmere ewa amaanyi. Yongeza ku mirundi gyolya naddala ng’oli mulwadde.
okufuna ekijjulo ekijjuvu n’okwongera amaanyi mu mubiri..
lunaku okusinga abantu abenkana nabo mumyaka, abekikula ekimu ara nga bakola emirimu gyegyimu nga tebalina kawuka ka sirimu okukakasiza ddala nti omubiri gufuna ekiriisa kye gwetaaga.
Lya emirundi etaano olunaku (ebijjulo emirundi esatu ate Obumpwakimpwaki emirundi ebiri).
Kubanga akawuka ka silimu kakosa enkozesa y’emmere mumubiri olina okulyako katono buli kiseera, naddala ng’oli mulwadde okufuna amaanyi omubiri gegwetaaga
Lya emmere eye bika eby’enjawulo ku buli kijjulo.
Emmere aya bulijjo okugeza nga muwogo, amatooke ewa amaanyi, emmere ezimba omubiri egumya nokuzimba ebinywa, ate ebibala n’enva endiirwa biyamba mukuzimba obutafaali obulwanyisa endwadde mumubiri.
Emmere gyongeremu ekiriisa ng’ogattako ebika by’emmere ebirimu ebirungo ebizito nga ekipoli ky’ebinyeebwa (groundnut paste), ovacado, omuzigo/buto, sukaali/omubisi gw’enjuki oba amata gobuwuunga
Emmere aya bulijjo okugeza nga muwogo, amatooke erimu ekirisa kitono nolwekyo yetaaga okugattirwako ebika byemmere ebirimu ebirungo ebizito.
Lya emmere ejjudde ebiriisa nge eyo ewa amaanyi, ezimba omubiri wamu neyamba mukuzimba obutafaali obulwanyisa endwadde mumubiri ga ekipoli ekirimu soya ne kasooli (corn-soy blend)

64
Engeri ey’omugaso gyosobola okwerabiriramu n’okwerisa
Obubaka obukulu Enyinnyonnyola y’obubaka
webisobola okufunibwa era nga bisoboka.
Bwoba toyagala kulya oba nga tolya kimala saba akulabirila akuyambe okufunira emmere, okugitegeka era akuyambe nemukugirya.
3. Nywa amazzi mangi nga mayonjo (amafumbe oba agatekedddwamu eddagala)
Nywa egiraasi nga munaana ez’amazzi amayonjo/amafumbe mulunaku.
Okunywa amazzi agatali mayonjo, agatali mafumbe kyongera obuzibu bwokufuna endwadde zinakigwanyizi mu bantu abalina akawuka ka sirimu, mwaabo abalina obunafu mukulwanyisa endwadde era kisobola okuleeta embiro/okuddukana okwamaanyi era ne kivaako okukogga..
Fumba amazzi g’okunywa oba gateekeemu eddaggala.
Okwewala endwadde eziva mu kulya ebyokulya nga sibiyonjo wamu ne ndwadde zinakigwanyizi.
Ebiseera byonna, awaka beerawo n’amazzi agamala okunywa nokumira eddaggala nga mayonjo bulungi.
Okwewala okuggwamu amazzi mu mubiri.
Okuwa embeera ennungamu eddaggala okukola wamu n’ekyenda okugaaya obulungi emmere.
4.Werabirire okusobola okusigala mu mbeera ennungamu wadde ng’olina akawuka ka mukenenya era weyise mumbeera y’obulamu etakuteeka nukatyabaga
Goberera enkola z’ebyobulamu ezitakuteeka mukatyabaga (saba omusawo wokukyalo community health worker oba akulabirira mu byobulamu akuwe abupiira (condom) bwoba obwetaaga).
Enkola zokwegatta enkyamu zikuteeka mukatyabaga kokweyongeramu akawuka ka silimu nokwanguwa okufuna mukenenya. Kikulu nnyo okwewala okusiiga abalala akawuka ka siriimu..
Wewale okunywa omwenge naddala ngomira/ng’oli ku ddaggala.
Omwenge gutaataagaanya/gukyankalanya okugaya, okutambuza, okutereka wamu nenkozesa
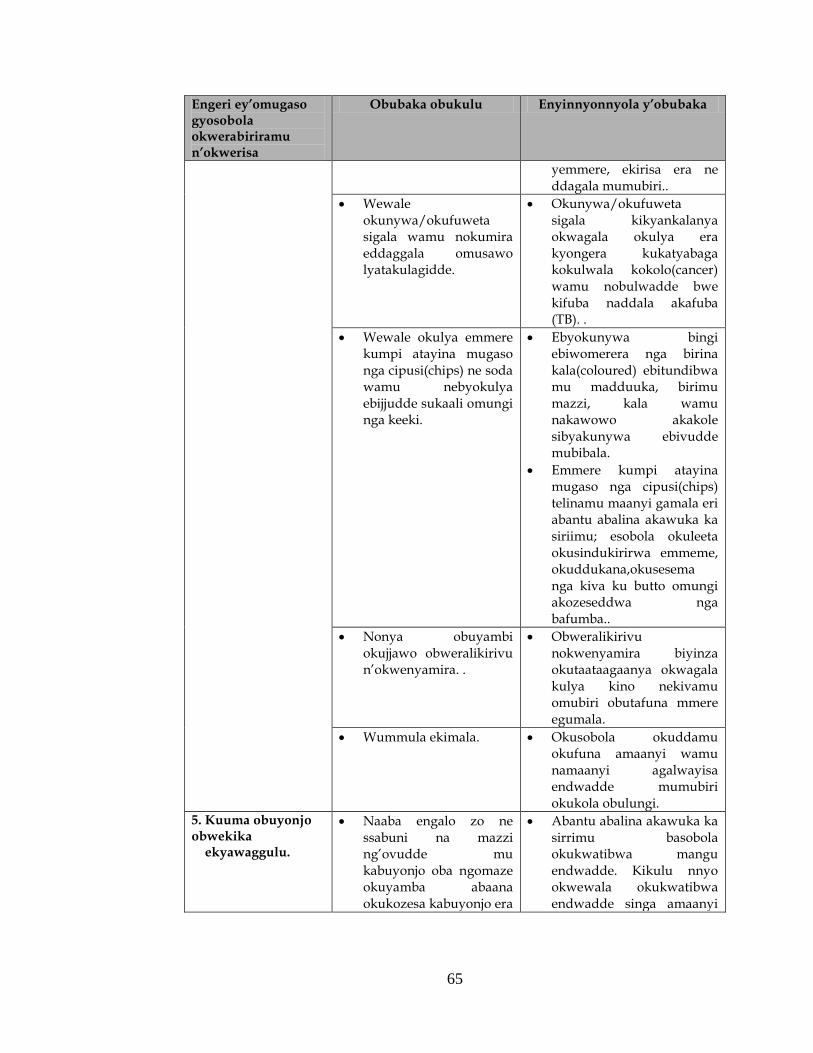
65
Engeri ey’omugaso gyosobola okwerabiriramu n’okwerisa
Obubaka obukulu Enyinnyonnyola y’obubaka
yemmere, ekirisa era ne ddagala mumubiri..
Wewale okunywa/okufuweta sigala wamu nokumira eddaggala omusawo lyatakulagidde.
Okunywa/okufuweta sigala kikyankalanya okwagala okulya era kyongera kukatyabaga kokulwala kokolo(cancer) wamu nobulwadde bwe kifuba naddala akafuba (TB). .
Wewale okulya emmere kumpi atayina mugaso nga cipusi(chips) ne soda wamu nebyokulya ebijjudde sukaali omungi nga keeki.
Ebyokunywa bingi ebiwomerera nga birina kala(coloured) ebitundibwa mu madduuka, birimu mazzi, kala wamu nakawowo akakole sibyakunywa ebivudde mubibala.
Emmere kumpi atayina mugaso nga cipusi(chips) telinamu maanyi gamala eri abantu abalina akawuka ka siriimu; esobola okuleeta okusindukirirwa emmeme, okuddukana,okusesema nga kiva ku butto omungi akozeseddwa nga bafumba..
Nonya obuyambi okujjawo obweralikirivu n’okwenyamira. .
Obweralikirivu nokwenyamira biyinza okutaataagaanya okwagala kulya kino nekivamu omubiri obutafuna mmere egumala.
Wummula ekimala. Okusobola okuddamu okufuna amaanyi wamu namaanyi agalwayisa endwadde mumubiri okukola obulungi.
5. Kuuma obuyonjo obwekika ekyawaggulu.
Naaba engalo zo ne ssabuni na mazzi ng’ovudde mu kabuyonjo oba ngomaze okuyamba abaana okukozesa kabuyonjo era
Abantu abalina akawuka ka sirrimu basobola okukwatibwa mangu endwadde. Kikulu nnyo okwewala okukwatibwa endwadde singa amaanyi

66
Engeri ey’omugaso gyosobola okwerabiriramu n’okwerisa
Obubaka obukulu Enyinnyonnyola y’obubaka
ne bwoba tonakwata, kutegeka wamu nokulya emmere okuziyiza endwadde.
gomubirigwo agalwanyisa endwadde gaba matono.
Wegendereze bwoba ogula emmere esangiddwa nga ntegeke okulirawo eyinza okuba nga yategekeddwa mu mbeera etali nyonjo era nga erimu obuwuka obuleeta endwadde..
Emmere eno erwaza ekiddukano ekikosa engaaya ne ntambuza y’emmere mumubiri era kifulumya ekiriisa eky’omugaso.
6.Omubiri guzanyise oba bako kyokola (exercise).
Omubiri guzanyise oba bako kyokola kumpi buli kiseera okugumya nokuzimba ebinywa, okwongera okukwagazisa okulya, okukendeeza obwerarikirivu wamu nokwongera okutereeza embeera yo bulamubwo okutwalira awamu.
Okuzanyisa/okukozesa omubiri kumpi buli kiseera kiyamba obwongo okukola obulungi, kikendeeza okweralikirira, kyongera okwagazisa okulya, kigumya nokuzimba ebinywa,
Okuzanyisa/okukozesa omubiri musobola okubeeramu okukola emirmo gy’awaka, okulimako, okutambulamu oba okudduka..
7. Nonya mangu obujjanjabi ng’olwadde era werise mundya
entufu era esanidde. okusobola okujjanjaba endwadde bwekiba kisoboka.
Nonya mangu omusawo akujjjanjabe obulwadde.
Buulira omusawo akujjanjaba eddaggala lyonna elyekinnansi oba eddaggala eririmu ebyokulya (nutritional supplements) lyokozesa/lyonywa/lyomira.
Eddaggala eririmu ebyokulya liwa ekifanaanyi ekikyamu nga kiyita mubulango. Bulijjo webuuze kumusawo webyobulamu omutendeke ku bikwata kukukozesa eddaggala lino.
Eddaggala eririmu ebyokulya (nutrition supplements) teririna kukozesebwa mukifo

67
Engeri ey’omugaso gyosobola okwerabiriramu n’okwerisa
Obubaka obukulu Enyinnyonnyola y’obubaka
kyemmere era terijjanjaba kawuka ka silimu.
JJanjaba obubonero obwefanaanyirizaako n’obuleetebwa akawuka ka silimu nga okusindukirirwa emmeeme, nokusesema oba obutayagala kulya ng’olya mundya entufu era esanidde..
Endya ennungi ezzaawo ebirungo mu mubiri, eyambako ku ntambula y’emmere n’okwongera amaanyi gomubiri agalwanyisa endwadde.
Kigenderera okuzzaamu obulamu omuntu nadda bulungi mumbeera ye eya bulijjo
8.Engeri gy’onokwataganyamu emmere n’eddaggala oba obuzibu obuvudde ku ddaggala
Saba omusawo wekyalo (community health worker) akuyambe mu kusengeka essawa/obudde bw’okulya n’obwo kumira eddaggala era Saba omuntu akuyambe okubunywerera ko.
Eddaggala erimu limiribwa nga mulubuto mulimu emmere, waliwo eddaggala eddala lyo limiribwa nga olubuto lukalu nga temuli mmere nakamu ate waliwo eryo erimiribwa obudde bwonna oba olubuto lukalu oba mulimu emmere.
Eddaggala erimu likwatagana/likontana ne mmere emu ekiyinza okuyamba okukola obulungi oba obutakola bulungi.
Buuza ku buzibu obusobola okuva ku ddaggala lyomira era oyige engeri gyosobola okulya okusobola okubuvvunnuka.
Bulijjo mira eddaggala lyo ng’ogoberera ebiragiro ne bipimo byeddagala omusawo (Doctor) by’akulagidde.
Source: RCQHC/FANTA, 2008: Nutrition Care for People Living with HIV/AIDS: Training manual for community and home-based care providers

68
13.2 Nutrition Drama script
Luganda version ASIIKA OBULAMU
(Omuzannyo ogukwata ku ndiisa ennungi guli mu balwadde ba mukenenya nga guzimbiddwa mu amaka abiri, aga Kyaterekera ne Musisi) ABAZANNYI: 1. Kyaterekera – Aliku ddagala (ARVs) naye tagoberera mateeka ga ddagala 2. Muky. Kyaterekera – Naye ali ku ddagala (ARVs) era ye mukyala wa
Kyaterekera 3. Musisi – Ali ku ddagala (ARVs) era agoberera bukungi amateeka g’abasawo 4. Muky. Musisi – Ye mukyala wa Musisi, talina kawuka ka mukenenya,
wabula afaayo nnyo ku bulamu bw’omwami ko n’okumulabirira 5. Nabugwamu – Mukwano gwa Musisi 6. Dominiko - Mukwano gwa Kyaterekera 7. Jjumba- Musawo wa byabuyonjo mu kitundu
EKITUNDU EKISOOKA (PART 1):
SCENE 1 (Tuwulira Kyaterekera ne mukyalawe nga bajja bayomba okutuukira ddala ku stage) Kyaterekera: Tekisoboka! nedda nedda gwe n’olima, ensalosalo
nga bw’oyingira ewange, siliimu gwonnangira gwe tosobola kumufuna?
Muky. Kyaterekera: Ye amukulangira, ffe twamunywa mu mazzi? Kyaterekera: Talabangayo bafa accident nga tebafudde kawuka.
(Awo bayingiza byebazze nabyo okuva munnimiro, Enku, Enkumbi, Ejambiya, Endagala)
Muky. Kyaterekera: Kulikayo mwami Kyaterekera: Nvuddeyo mukyala naawe kulikayo. Kyaterekera: Mpaayo ku mazzi nnyweeko. Muky. Kyaterekera: Kale sebo (baba bakyayogera ebyo Dominiko n’atuuka).

69
Dominiko: Abeeno gyemuli? Kyaterekera: Gyetuli baaba, nsanyuse okukulaba bwaana Dominiko Dominiko: Kale sebo (amulamusa). Muky. Kyaterekera: Tusanyuse okukulaba sebo (amulamusa). Dominiko: Kale nnyabo (balamusaganya) Dominiko: Ee! Bwana Kyate- nnakuliinze eggulo, ewa
―Nakamatte mu kirabo‖ saakulabye, nange bwenfunyeewo kenfunye , ko nze kanzirukire munywanyi wange Kyaterekera tugende tunyweemu, anti obulamu bumpi.
Kyaterekera: Ee….. leka nzigyemu engoye tugende.(Akyuusa engoye
nga bwe banyumya ne “Dominiko.”Baba basimbula awaka, Muky. Kyaterekera n’abakira bbaawe)
Muky. Kyaterekera: Naye mwami- kaakati ogeenda mu kunywa
mwenge, nga tolidde wadde okunywa akantu konna, weerabidde byebaatusomes a ku Suubi Clinic? Jjukira inti ku Suubi clinic baatusomesa okwewala okunywa omwenge naddala ng’oli kuddagala erikendeeza obungi bw’akawuka ka mukenenya mu musaayi.
Kyaterekera: Naye mukyala, tomanyi nti gyetulaga ebyokulya
n’okunywa gyebisinga? Tontekako kajanja (Era amukayukira nnyo).
Muky. Kyaterekera: Kale genda gwe onamanya (Awo ayogera ebigambo
bingi ebikwata ku bbaawe ko n’okuvumirira omenge mu balwadde ba mukenenya). Omwenge gutaataganya okugaaya, okutambuza, okutereka wamu n’enkozesa y’emmere, ekiriisa era n’eddagala mumubiri.

70
Tulaba Tibisilikirwa mu maka ga kyaterekera:
Tibisirikirwa: Ab’eno gyemuli baaba? Muky. Kyaterekera: Gyetuli nnyabo, tusanyuse okukulaba Tibisirikirwa: Kale nnyabo (balamusaganya) Tibisirikirwa: Omukulu mw’ali? Muky. Kyaterekera: Obadde omwagala? Tibisirikirwa: Nedda baaba…, Muky. Kyaterekera: Taliiwo, laba Dominiko wuuyo amunonye wano
mbu bageenze mwa Nakamatte kwenywera ku kabisi.
Tibisirikirwa: Anti munnange, nange kye kindeese ndukwokye,
ky’endesse beekola ewa Nakamatte kika! Bali mukukoona ndigi eno bwetumya ensaniya z’ebigodo, bajjawo zino bayingizaawo ndala.
Muky. Kyaterekera: Gamba obwedda naawe olya nabo, kirabika bwe
mubadde muyiringisa ensaniya kati ojja onjejemberako, mwe mumaze ssente za baze.
Tibisirikirwa: Nedda baaba nze nzize kukubbirako, ate mwana
wattu takikoze leero lwokka, bulijjo bw’atyo. Muky. Kyaterekera: Bulijjo bwatyo? Gwe ng’omulaba! Tewegaana, mubirya mwenna? Tibisirikirwa: Kale kitwale bw’otyo nti tubirya, anti
ne’bwanakulekawo obukyaafu bwakuyinga. Tunnulira wano ebisaaniko, toyera na lujja!! Eehe! Ate kankubuulire, bw’adda n’omugamba nti nze mmuloopye, ndi mwangu wa kukwegaana, ate waliwo andabye?

71
Muky. Kyaterekera: Nja kubimugamba; nkuloge olugambo olukuwunyako?
Tulaba Ndevu ne muswangali (ku street)
(Boogera ku ngeri Kyaterekera ne Dominiko gye baabagobye ku mwenge era nga bwe bagenda okubesasuza). Ndevu: Muswangali nkubulire, gwe baleke nange njakukibakola.
Ne batugoba mu kirabo, ate nebatudduulira!! Muswangali: Haaa! simanyi na kumanya naye kangende njiiye, naffe tujja
kubalaga naffe ―touch‖, ate tujja kubagera nga tebalina ssnte tubesasuze.
SCENE II
Tulaba Kyaterekera ne Dominiko bakomawo nga bamaze okunywa omwenge:
Kyaterekera ne Dominko bajja bewaana nga bwebanywedde omwenge, ogufisse nebagunaaba ebigere.(Bino byonna babyogera bali kumpi okutuuka mumaka ga Kyaterekera. Baba banaatera okutuuka Dominikon’ asibuula Kyaterekera ne yeyongerayo. Kyaterekera: (Ayita), Mukyala…… x2, tukubye omubisi
komannyoko.( Awo ayongerako ebigambo bingi eby’okubalaata.)
Muky. Kyaterekera: Naye gusajja gwe, oli musajja ki atebalirira yadde
okulowooza ku bulamu bwo? Onywa otya omwenge neweerabira n’abasawo bye baakusomesa?
Kyaterekera: Kikazi ggwe, olimusiru totegeera? Baatugamba
kunywa nnyo, era kati kyennyini kye nva okukola!! Muky. Kyaterekera: Baakusomesa kunywa mwenge oba baakusomesa
kunywa ebyo ebinaayamba omubiri okuba n’obulamu obulungi nga amazzi; eggiraasi munaana,

72
oba chaayi, n’obutunda oba obuugi, gamba n’obushera (Baba bakyayogera, ebyo Nabugwamu abasanga bayomba).
Nabugwamu: Abataka- abataka gyemuli?? Kyaterekera: Gyetuli –gyetuli (Balamusaganya naye baba tebannamalayo, ko Nabugwamu) Nabugwamu: Nga muli bulala ate mufaaki? Kyaterekera: Ndaba ono omusirusiru… (Annyonyola Nabugwamu nga bwebibadde) Nabugwamu: Mukube bukubi tomanyi kukuba, omukazi ategeera miggo. Muky. Kyaterekera: Ankube? Kye kikuleese, anti ekyo ggwe kye
kyakulemya amaka (Ayogera ebyo bw’asemberera Nabugwamu ne bbaaweng’ayagala okubambalira)
Nabugwamu: Nedda nnyabo ebyo sibyebyandeese mweraba
(Kyaterekera amuwerekera. Mukyala Kyaterekera ayingira ekisenge, olutimbe ne luddawo).
EKITUUNDU EKYOKUBIRI (PART II)
SCENE I
Tutandikira mu maka ga Musisi
Muky. Musisi: Annet emmere eyidde? Annet: Maama emmere yayidde dda, ngireete? Muky. Musisi: Nedda mbadde njagala kumanya oba eyidde, ate
tunajjula nga kitaawo tanadda? Annet: Naye maama abaana ku ssomero (annyonyola maama
we ebyetaago bye e’byessomero, era amusaba aabuulireko taata we ng’akomyewo)

73
Muky. Musisi: Kale tofaayo Annet, taata wo njakubimugamba.
(Tulaba musisi ng’akomyewo awaka okuva gy’badde)
Muky. Musisi: Kulikayo mwami (amulamusa) Musisi: Nvuddeyo mukyala (naye amulamusa) Muky. Musisi: Okooye nnyo mwami? Musisi: Nkoye mukyala, mpaayo kumazzi nnyweeko. Musisi: Era nga bw’ogambye, binkooyezza nnyo, anti
nnasoose kugenda gye, nnakugambye gye mmanja ssente zange, naye omusajja by’anyinyonnyode birala. Ndabye andwiisa, konze kanneeyune obudde, wuuyo ku SUUBI CLINIC. Mbasanzeemu abasawo, era nebankebera bulungi, awamu n’okumpima obuzito wange.(Amunyonyola kilo ezeeyongedde ku z’abadde alina n’ebirala bingiko ebigwa mu ttuba eryo)
Muky. Musisi: Olabye mwami? Kaakano tulina okugoberera
eby’abasawo bye batusomesa ku ndya ennungi eri abalwadde ba mukenenya, ng’okulya ebika by’emmere ebyenjawulo. Nze nkizudde nti omuntu bw’agoberera endya eno gye batusomeseza, obuzito bwe bweyongerako mu kiseera ekitono ddala. Ate okunywa ebintu ebiyamba emibiri gyaffe okukozesa eddagala, nokubeera obulungi ekyo nakyo kiyambira ddala obulamu bwaffe okulongooka.
(Tulaba Nabugwamu akyala mu mumaka ga Musisi)
Nabugwamu: Abeeno gyemuli? Musisi: Gyetuli sebo, ee… bwana Nabugwamu gwe wuyo?
Nsanyuse okukulaba (amulamusa) Nabugwamu: Kale ssebo, (amuddamu era n’omukyala amwanirizaera n’amulamusa)

74
Nabugwamu: Kanneme kubeera ng’eyajja okusaba eryato, kaakati
bwana Musisi ensonga endeese, nnalima obulime bwange, naye ensigo y’ebijjanjaalo yaampeddeko, ne nngamba nti, kanngende ewa munywani wange Musisi, anfunireyo obutaasa nga buubwo.
Musisi: Haa… bwana Nabugwamu ekyo tekyalibadde kizibu,
naye nninawo byange byakulya, byali bingi naye ne ntundako ensawo nga ziizo ne nsigaza bya kulya, baaba tewali.
Muky. Musisi: Mwami tuleete emmere? Musisi: Muleete baaba (baleeta emmere) Nabugwamu: Kangende mwattu, nja kegezaako awalala. Musisi: Naawe, emmere tekugoba, tumale kulya (n’omukyala
bwatyo). Nabugwamu: Anti engeri gyesifunye kyenjagala kanngende nga
bukyali. Musisi: Emmere tekwatira mu kifo, mala kulyako olyoke
ogende Nabugwamu: Ha-ha, owaaye, bagamba nti lukujja webajjula
nelukutwaala webasaanika (Atuul, anaaba mu ngalo era batandika okugabula ekijjulo)(Ekijjulo mulimu ebika by’emmere ebye’enjawulo, eby’okunywa n’ebibala).
Nabugwamu: Emmere ngirabye nja kulyako katono, naye ameenvu
gaaki? (Awo Musisi amunyonnyola omugaso gwago)
Musisi: Ebibala ng’amenvu, emiyembe, entuntunu, ennaanansi nebibala ebirala bituyamba okukuuma omubiri nga mulamu n’okulwanyisa endwadde zinnakigwanyizi.
Nabugwamu: Gano go amaggi tugendana (Atandika okulya amaggi).
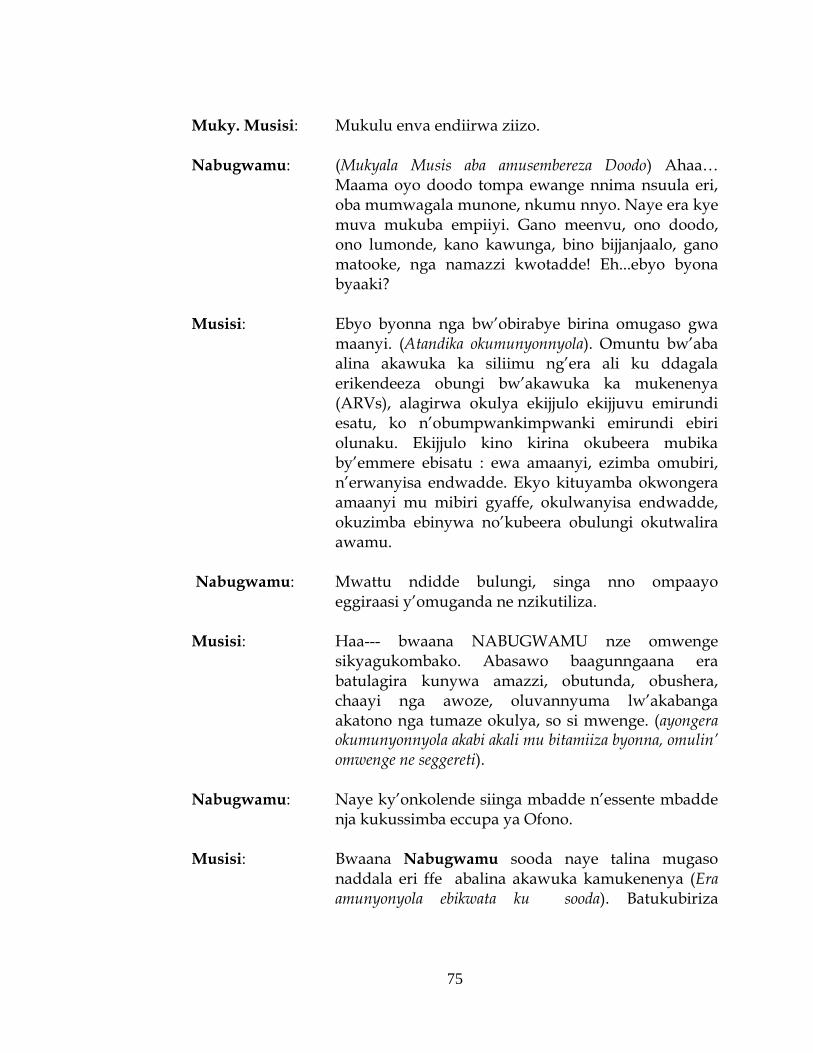
75
Muky. Musisi: Mukulu enva endiirwa ziizo. Nabugwamu: (Mukyala Musis aba amusembereza Doodo) Ahaa…
Maama oyo doodo tompa ewange nnima nsuula eri, oba mumwagala munone, nkumu nnyo. Naye era kye muva mukuba empiiyi. Gano meenvu, ono doodo, ono lumonde, kano kawunga, bino bijjanjaalo, gano matooke, nga namazzi kwotadde! Eh...ebyo byona byaaki?
Musisi: Ebyo byonna nga bw’obirabye birina omugaso gwa
maanyi. (Atandika okumunyonnyola). Omuntu bw’aba alina akawuka ka siliimu ng’era ali ku ddagala erikendeeza obungi bw’akawuka ka mukenenya (ARVs), alagirwa okulya ekijjulo ekijjuvu emirundi esatu, ko n’obumpwankimpwanki emirundi ebiri olunaku. Ekijjulo kino kirina okubeera mubika by’emmere ebisatu : ewa amaanyi, ezimba omubiri, n’erwanyisa endwadde. Ekyo kituyamba okwongera amaanyi mu mibiri gyaffe, okulwanyisa endwadde, okuzimba ebinywa no’kubeera obulungi okutwalira awamu.
Nabugwamu: Mwattu ndidde bulungi, singa nno ompaayo
eggiraasi y’omuganda ne nzikutiliza. Musisi: Haa--- bwaana NABUGWAMU nze omwenge
sikyagukombako. Abasawo baagunngaana era batulagira kunywa amazzi, obutunda, obushera, chaayi nga awoze, oluvannyuma lw’akabanga akatono nga tumaze okulya, so si mwenge. (ayongera okumunyonnyola akabi akali mu bitamiiza byonna, omulin’ omwenge ne seggereti).
Nabugwamu: Naye ky’onkolende siinga mbadde n’essente mbadde
nja kukussimba eccupa ya Ofono. Musisi: Bwaana Nabugwamu sooda naye talina mugaso
naddala eri ffe abalina akawuka kamukenenya (Era amunyonyola ebikwata ku sooda). Batukubiriza

76
okwewala okulya emmere nga kyenkana terina mugaso mu mibiri gyaffe nga chips, ne Sooda wamu n’ebyokulya ebirala ebirimu sukaali omungi nga keeki. Ate Soda alimu preservative, yandikufuukira ekizibu (bakola katemba nga bwebanyumya ku preservative). Naye gwe nga bw’olina emiziinga, olinayo omubisi gw’enjuki?
Nabugwamu: Naye naawe!! Kati ogaane sooda, ate onywe omubisi
gw’enjuki oguwoomerera nga sukaali kumpi n’okumusinga.
Musisi: Anti omubisi gwenjuki sukaali wagwo wabutoonde,
era takosa mubiri. Ezo endwadde zinnakigwanyizi, tazirabamu. Guno ggwo, ngwongerera ddala amaanyi mu mmere gyetulya.
Nabugwamu: Eeeeeh—kwe kugamba sukaali w’omubisi gwenjuki
y’asanidde? (Ebyo byona Nabugwamu –abuuza tateredde olw’ekijjulo ate ngan’ emmere eremye tagitwaale, era ku nkomerero asiibula nga naye omutima gumusigadde kummere , era Musisi amuwerekera. Mukyala Musisi asigala ategula ebintu).
(Tulaba Jjumba C.H.W. ayingira ewa musisi)
Musisi : Tusanyuse okukulaba sebo (asigala awerekera
Nabugwamu). Kankomewo nkulamuse. Muky. Musisi: Tusayuse okukulaba sebo (amwaniriza era amulamusa
oluva nyuma Musisi akomawo). Musisi: Tusanyuse okukulaba sebo (amulamusa era amubuuza
lwaki atambudde mumusana, era bamuwa e’kyokunwya) Jjumba: Ndi ku mulimo gwa kulambula abantu baffe ndabe
nga oba bye bwetwabasomesa ku buyonjo mwabikwata, anti omulimo gwaffe omukulu kulambula bya buyonjo mu maka, n’okulaba abantu baffe bwebali mu by’obulamu. Abantu baffe abamu

77
bakyali bubi nnyo, naye abo tetujja kubguumikiriza, tujja kubasiba busibi.
Musisi: Sebo ffe tufuba nnyo ne tukola kye tusobola, naye
banaffe abamu batuzza emabega, era bebasibye kuno endwadde eziva mu bukyafu. Leero waliwo ono muliranwa waffe, Kyate, Eeee, eyo kitalo butalo.
Jjumba: Mmulabye naye, oyo mmubuulidde nti wakusibwa
(bino abyogera alambula, kino akikorela akaseera katono n’asibuula).
SCENE II
(Tuddamu okulaba omusawo w’endiisa ennungi mu balwadde ba mukenenya nga’ali mu maka ga Kyaterekera)
Omusawo: Ab’eno gyemuli? Muky. Kyaterekera: Gyeetuli nnyabo tusanyuse okulaba (amulamusa) Kyaterekera: Tusanyuse okukulaba nnyabo (amulamusa, naye aba
amuwa engalo, agenda okulamusa omusawo, n’agwaamu ekidumusi era ne yeeyuna emmanju)
Omusawo: Kakati mwami Kyate, weewulira mungeri ki? Kyaterekera: Sirina ate tondaba. (Awo annyonyola ebimukwatako
byonna, kyokka abyogera mukyala amulumika nga bw’atabituukiriza, era nga bw’alemedde ku seggereeti, omwenge, ko n’obutamira bulungi ddagala).
Omusawo: Mwami Kyaterekera kyalibadde kirungi n’ogoberera
ebyakusomesebwa abasawo ku SUUBI CLINIC era n’obituukiriza. (Atandika okumusomesa).
a) Okulya emmere ey’ebijjulo, mu bika bye’mmere ebyenjawulo buli lunaku
b) Okwongera amaanyi mu mubiri ng’okozesa emmere erina amaanyi okusinga ku ya bulijjo, ng’ebikajjo, omubisi gw’enjuki, ekipooli ky’ebinyebwa n’entungo.

78
c) Okunywa amazzi nga mangi, amafumbe era nga mayonjo oba ng’otaddemu eddagala elirongoosa amazzi – eggiraasi munaana, oba elyakuweebwa ku suubi clinic, so, simwenge mungi.
d) Okubeera omuyonjo awaka, n’okuyonja omubiri gwo. e) Okumira eddagala, mu budde ate n’obutasussa ssaawa zomirirako buli lunaku. f) Okufangayo okupima obuzito bwo buli lw’ogenda ku
suubi clinic. (Era amulaga ebifaananyi bya mirundi ebiri):
a) Ebiraga omugaso gw’okulya obulungi ng’olina akawuka ka silimu ng’omira eddagala, ate
b) n’ebikutuuka ko singa oba tolidde bulungi ng’ate omira ddagal ly’akawuka ka mukenenya.
A) Eri oyo atuukiriza kye baamusomesa, a. Alya bulungi ebijjulo, b. Amira bulungi eddagala c. Obuzito bwe bweyongerako buli kiseera
ekitonotono, nga buli week 2 d. Azimba ebinywa e. Alwanyisa bulungi endwadde zi nnakigwanyizi f. Alina amaanyi agakola emirimo gye g. Aziyiza akawuka kasilimu okuzaala okweyongera
mu mubiri (Amulaga ekifaananyi ekyo’okubiri)
B) Oyo atatuukiriza kyebamusomesa, a. Abatakyayagala kulya, emmere agisamula eri, nga
bagimuwadde b. Akendeera obuzito c. Tamira bulungi ddagala d. Amaanyi ge ag’okulwanyisa endwadde gakendeera e. Endwadde zinnakigwanyizi zimuyiikiriza f. Ebinywa bikendeera g. Akosebwa akawuka ka silimu h. Tasobola kwekolera mirimu, era ebiseera ebisinga
abeera ku ndiri

79
(Omusawo afundikira nga Kyaterekera amukakasizza nga bw’agenda okussa ebimugambiddwa munkola era nga bali wamu n’omusawo ne mukyala we, bakkiriziganya nti omusawo addeyo abakyalire oluvannyuma lwa week 2 alabe we batuuse mu kukyusaamu. Omusawo asiibula)
(Tulaba Jane ne Charles ku street)
Jane: Nze njagala nkubuulire bye nkugambye bituufu, era
bw’okkiriza nange nja kukuwa ky’onsabye. Charles: Naye Jane awo ndaba nga ambuzaabuza kubanga buli
lwenkugamba mubulungi ky’ebazuula tokkiriza. Bali bakugu era tebasobola kulimba.
Jane: Tebalimba? Charles: Kati gwe b’akukeberera wa? Jane: Mu kitongelo kyaffe ekya RHSP; era kyebaba bakugambye,
kiba kyekyo. Gwe, bwo’kkiriza nga tugenda. Charles: Kale tugeende batukebere (Jane akulembera Charles
n’amuvaako emabega, era batambula bwe banyumya. Awo Charles asala ekimooni n’abomba).
Jane: (Asigala anyumya ng’amanyi akyali ne Charles wabula agenda
okukebera emabega nga munne tamulabako, era ayogera nti) ―kirabika ono, mulwadde!! Lwaki ate adduse?‖ (Naye avaawo ne yeyongerayo).
Charles: Kano kalubuuse, kawonye kanngeende nsagule awalala.
SCENE III
(Tulaba Musisi ne Nabugwamu boogera era basalawo okugenda okulaba ku Kyaterekera)
Omusawo: Ab’eno gyemuli? Muky. Kyaterekera: Gyetuli nyabo (Ategeka eby’okulya era ali na mu
kubyoza). Tusanyuse okukulaba nnyabo (amulamusa) (Tulaba Kyaterekera ng’ajja, adduka, ava mu mirimo gye,
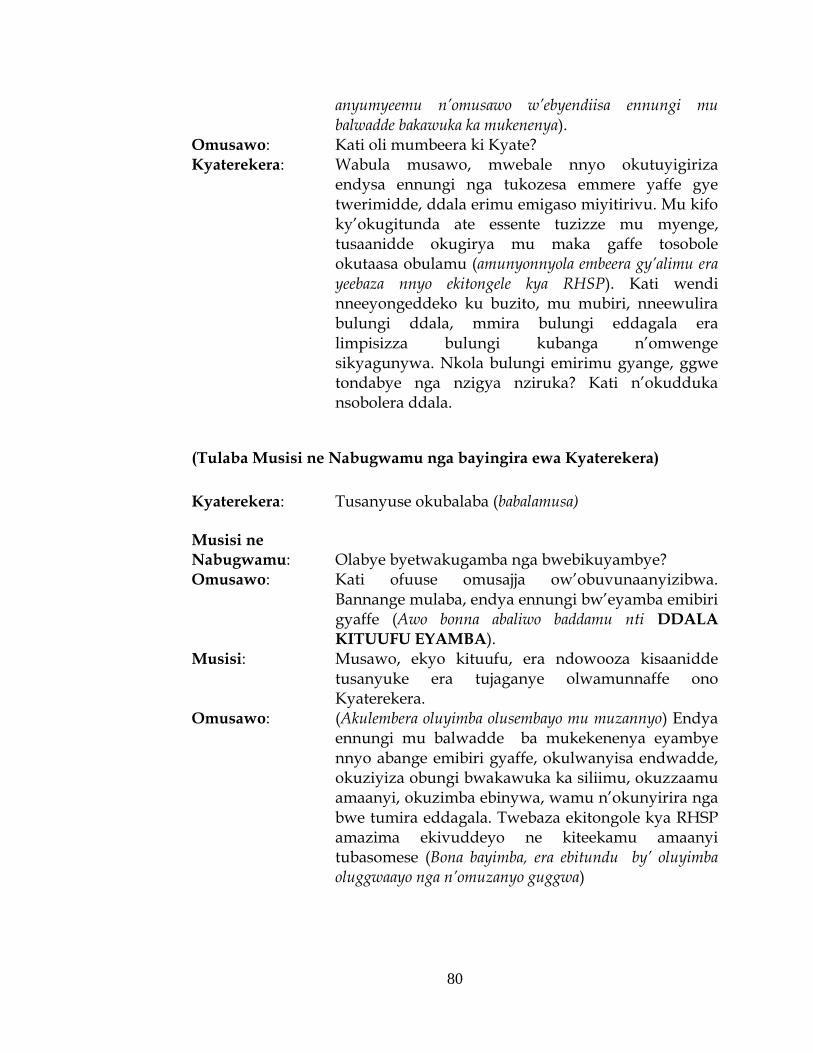
80
anyumyeemu n’omusawo w’ebyendiisa ennungi mu balwadde bakawuka ka mukenenya).
Omusawo: Kati oli mumbeera ki Kyate? Kyaterekera: Wabula musawo, mwebale nnyo okutuyigiriza
endysa ennungi nga tukozesa emmere yaffe gye twerimidde, ddala erimu emigaso miyitirivu. Mu kifo ky’okugitunda ate essente tuzizze mu myenge, tusaanidde okugirya mu maka gaffe tosobole okutaasa obulamu (amunyonnyola embeera gy’alimu era yeebaza nnyo ekitongele kya RHSP). Kati wendi nneeyongeddeko ku buzito, mu mubiri, nneewulira bulungi ddala, mmira bulungi eddagala era limpisizza bulungi kubanga n’omwenge sikyagunywa. Nkola bulungi emirimu gyange, ggwe tondabye nga nzigya nziruka? Kati n’okudduka nsobolera ddala.
(Tulaba Musisi ne Nabugwamu nga bayingira ewa Kyaterekera)
Kyaterekera: Tusanyuse okubalaba (babalamusa) Musisi ne Nabugwamu: Olabye byetwakugamba nga bwebikuyambye? Omusawo: Kati ofuuse omusajja ow’obuvunaanyizibwa.
Bannange mulaba, endya ennungi bw’eyamba emibiri gyaffe (Awo bonna abaliwo baddamu nti DDALA
KITUUFU EYAMBA). Musisi: Musawo, ekyo kituufu, era ndowooza kisaanidde
tusanyuke era tujaganye olwamunnaffe ono Kyaterekera.
Omusawo: (Akulembera oluyimba olusembayo mu muzannyo) Endya ennungi mu balwadde ba mukekenenya eyambye nnyo abange emibiri gyaffe, okulwanyisa endwadde, okuziyiza obungi bwakawuka ka siliimu, okuzzaamu amaanyi, okuzimba ebinywa, wamu n’okunyirira nga bwe tumira eddagala. Twebaza ekitongole kya RHSP amazima ekivuddeyo ne kiteekamu amaanyi tubasomese (Bona bayimba, era ebitundu by’ oluyimba oluggwaayo nga n’omuzanyo guggwa)

81
Abazannyi abalala (Extras):
1. Annet - Muwala wa Musisi 2. Jane 3. Namugera (omusawo w’ebyokulya) 4. Charles 5. Tibisirikirwa (walugambo) 6. Ndevu 7. Muswangali
Story line by: Flying Eagles Drama Group Original Written by: Bbira Samuel Arranged and Produced by: Tushemerirwe T. Florence (fellow) and
RHSP Health Education Team

82
13.3 Data collection Tools
13.3.1 Quantitative Methods (Questionnaire, English version)
RAKAI HEALTH SCIENCES PROGRAM NUTRITION KNOWLWEDGE, ATTITUDES AND PRACTICES ASSESSMENT FORM FOR PLHIV ENROLLED ON THE HIV CARE PROGRAM (Adults)
SECTION A: IDENTIFICATION
Hub name: __________________
Interviewer #: |___|___|___|
Interview date: ____/______/20___
Patient ID:
Lab Number:
Current address: Village/LC-1: ______________________ Contact Information: Tel No (if available): _____________________
SECTION B: SOCIO DEMOGRAPHIC CHARACTERISTICS
Age of patient: __________ Date of birth: ____/_____/_____ Gender: ____ dd mm yyyy Marital status: 1. Single (Never married) 2. Married 3. Separated
4.Divorced 5. Widowed Have you ever gone to School? 1. Yes 2. No. If No, → Occupation Highest level of Education: 1. P1-P2 2. P3-P4 3. P5-P7 4. S1 – S4 5. S5 – S6 6. Technical/University Occupation: _____________ _______________ ____________________________________

83
(for respondent) Record answer(s) as given, ____________________________ , _________________________ (Code up to two responses, code first mentioned occupation first.) Agriculture for home use/barter 01 Agriculture for selling 02 Housework in your own home 03 Housekeeper (for relative or employer) 04 Home brewing 05 Government/clerical/teaching 06 Fishing
07 Student
08 Military/police 09 Shopkeeper
10 Trading/vending 11 Bar worker or owner 12 Truck Driver 13 Unemployed (probe - no agric or house work?) 14 Medical worker (non-government) 15 Casual laborer 16 Waitress/Waiter/restaurant owner 17 Hair dresser/Salon owner 18

84
Construction (brick maker, painter, builder, porter, roofing) 19 Mechanic (automobiles, bicycles, electronics) 20 Other (specify) _____________________________ 21 No additional occupation (use code in 2nd field if one occupation is cited) 88 Parent/Guardian’s occupation: ____________________________________ (for unemployed older children, please ask for parent’s occupation) Record answer(s) as given: ____________________________ ____________________________ Code up to two responses, code first mentioned occupation first.) Agriculture for home use/barter 01 Agriculture for selling 02 Housework in your own home 03 Housekeeper (for relative or employer) 04 Home brewing 05 Government/clerical/teaching 06 Fishing 07 Student 08 Military/police 09 Shopkeeper 10 Trading/vending 11 Bar worker or owner 12 Truck Driver 13 Unemployed (probe - no agric or house work? 14
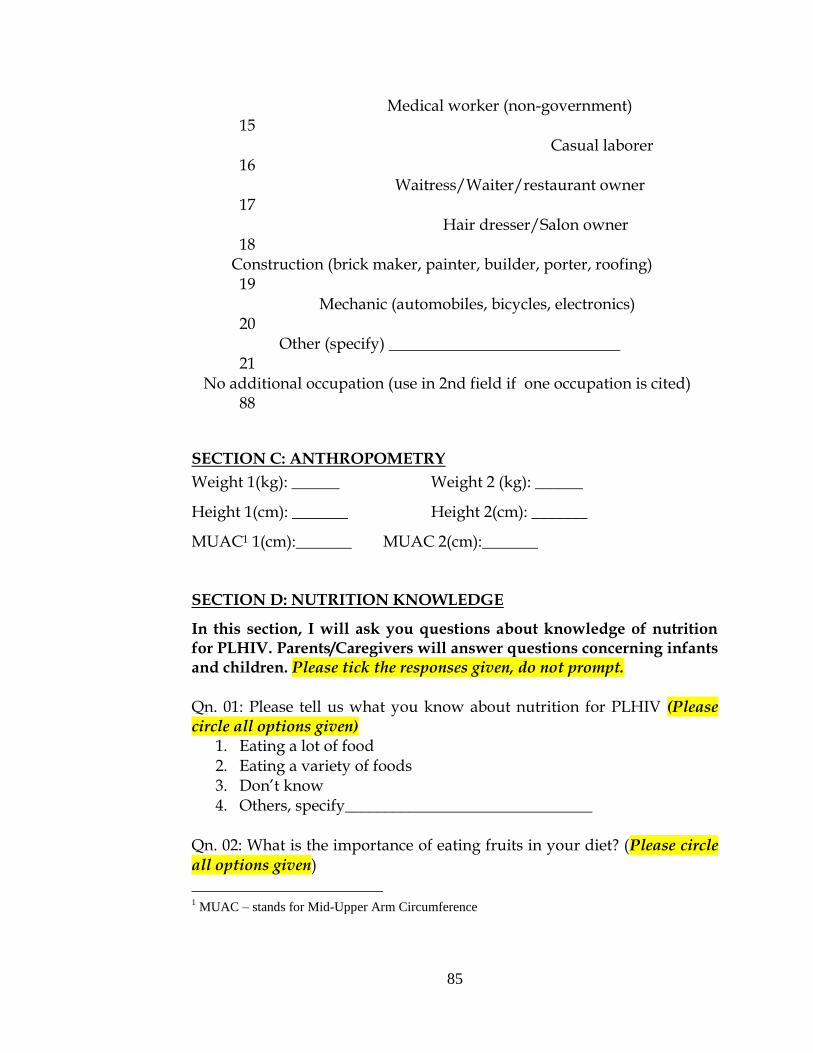
85
Medical worker (non-government) 15 Casual laborer 16 Waitress/Waiter/restaurant owner 17 Hair dresser/Salon owner 18 Construction (brick maker, painter, builder, porter, roofing) 19 Mechanic (automobiles, bicycles, electronics) 20 Other (specify) _____________________________ 21 No additional occupation (use in 2nd field if one occupation is cited) 88
SECTION C: ANTHROPOMETRY
Weight 1(kg): ______ Weight 2 (kg): ______
Height 1(cm): _______ Height 2(cm): _______
MUAC1 1(cm):_______ MUAC 2(cm):_______
SECTION D: NUTRITION KNOWLEDGE
In this section, I will ask you questions about knowledge of nutrition for PLHIV. Parents/Caregivers will answer questions concerning infants and children. Please tick the responses given, do not prompt. Qn. 01: Please tell us what you know about nutrition for PLHIV (Please circle all options given)
1. Eating a lot of food 2. Eating a variety of foods 3. Don’t know 4. Others, specify_______________________________
Qn. 02: What is the importance of eating fruits in your diet? (Please circle all options given)
1 MUAC – stands for Mid-Upper Arm Circumference

86
1. To help in fighting infections 2. To prevent constipation 3. Don’t Know 4. Others, specify_______________________________
Qn: 03: What is the importance of eating vegetables in your diet? (Please circle all options given)
1. To add water in the diet 2. To help in fighting infections 3. To prevent constipation 4. Don’t Know 5. Others, specify_______________________________
Qn. 04: Do you know anything about food fermentation in this community?
1. Yes 2. No
Qn. 05: If yes, what is the importance of Food fermentation?
1. Improves food quality 2. Aids in the digestion of food 3. Helps in nutrient absorption 4. Reduces food cooking time 5. Don’t know.
Qn. 06: What do you understand by eating well/good nutrition?
1. Eating meat 2. Eating fish 3. Eating Chicken 4. Eating at least fish, meat or chicken 5. Don’t Know
Qn. 07: Good nutrition, among PLHIV means the following (Please prompt):
1. Eating foods from all food types, e.g. Matooke, Sweet Potatoes, Bbugga, beans, and sweet bananas.
2. Eating a lot of food on the plate 3. Eating foods like chapatti, mandazi, splash. 4. I don’t know 5. Other, Specify ____________________________________

87
SECTION E: NUTRITION ATITUDES
Qn. 08: What do you think are the advantages of good nutrition, among PLHIV? (Please circle all options given)
1. Helps in keeping healthy 2. Helps the body to use ART medicines 3. Don’t Know 4. Others, Specify____________________________________
Qn. 09: What do you think would be the effects of poor nutrition among PLHIV? (Please circle all options given)
1. Weight loss 2. Frequent illnesses, e.g. cough, diarrhea 3. They die 4. Don’t know 5. Others, Specify______________________________________
Qn. 10: Do you think PLHIV require more energy every day than uninfected people? If Yes, →Qn.11)
1. Yes 2. No 3. Don’t Know
Qn. 11: If yes, why do you think PLHIV require more energy than the uninfected people?
1. To maintain good health 2. To stay strong 3. To fight the infection 4. To replace energy used by the infection 5. Don’t Know
Qn. 12: Do you think HIV and other frequent infections affect PLHIV’s food intake? If Yes, →Qn. 13.
1. Yes 2 No 3. Don’t Know
Qn. 13: If yes, in what ways do you think HIV and other frequent infections affect PLHIV’s food intake? (Please circle all options given)
1. Vomiting 2. Reduced appetite

88
3. Lack of energy to cook 4. Don’t Know 5. Other, Specify _________________________________________
I will read the sentences below, please tell me if you: 1. Strongly agree, 2. Agree, 3. Disagree, Strongly disagree or 5. Don’t know (Do not prompt for option 5) Qn. 14: Eating different types of food (like Posho, Matooke, Avocadoes, Jjobyo, and beans) daily is good for PLHIV and helps to prevent frequent infections.
1. Strongly agree 2. Agree 3. Disagree 4. Strongly disagree 5. Don’t know
Qn. 15: It is important for all family members to help PLHIV in their homes to have good and balanced meals.
1. Strongly agree 2. Agree 3. Disagree 4. Strongly disagree 5. Don’t know
Qn. 16: HIV positive women who are lactating or pregnant must eat an extra amount of food from all food types on a daily basis
1. Strongly agree 2. Agree 3. Disagree 4. Strongly disagree 5. Don’t know
Qn. 17: Children born to HIV positive mothers must be breastfed for:
1. 0-6 months 2. 0-4 months 3. 0-24 months 4. Don’t know 5. Other, Specify _________________________

89
SECTION F: NUTRITION PRACTICES
Qn. 18: In order to meet your energy needs, how many meals do you eat in a day? (Main meals are breakfast, lunch and supper while snacks are meals eaten in the middle of the main meals)
1. Eat at least 3 main meals 2. Eat at least 3 main meals and 2 snacks 3. Eat food whenever I get it in a day 4. Don’t Know 5. Other, Specify ___________________________
Qn. 19: How many times in a day do you eat fruits in your diet (e.g. sweet bananas, pawpaws, oranges, pineapples, and others locally available)?
1. Once 2. Twice 3. Three times 4. I don’t eat fruits 5. Other, Specify ___________________________
Qn. 20: How many times in a day, do you eat vegetables in your diet (e.g. dodo, nakati, jjobyo, ntula, carrots, Avocadoes, and others locally available)?
1. Once 2. Twice 3. Three times 4. I don’t eat fruits 5. Other, Specify ____________________________
Qn: 21: Do you ferment any foods in your home?
1. Yes 2. No
Qn. 22: If yes, why do you ferment food in your home? (circle all options given)
1. Improves food taste 2. Improves food flavor 3. Makes food easy to eat 4. It is my culture

90
5. Don’t Know 6. Other, Specify ___________________________
I will ask you questions about nutrition management of two HIV-related complications, Diarrhea and Nausea or vomiting (Interviewer, please circle all options given, do not prompt) Qn. 23: When you (a PLHIV) experience Diarrhea how do you eat?
1. I stop eating 2. I drink very few fluids to avoid worsening the situation 3. I eat a lot of fruits and vegetables to replace lost water 4. Never got this condition 5. Other, Specify ________________________________
Qn. 24: When you (a PLHIV) experiences Nausea and Vomiting, how do you eat?
1. Eat small but frequent meals 2. Lie down immediately after eating 3. Eat sugary foods 4. Never got this condition 5. Other, Specify ________________________________
I am aware that women of reproductive age in this community make choices to give birth to babies, or to start families with their partners. Qn. 25: When an HIV-positive pregnant woman recognizes that she is losing weight, she does the following (Please prompt): Y N DK
1. Consult her doctor to get treatment 1 2 7 2. Eat all 3 main meals and 2 snacks in a day 1 2 7 3. Continue taking her ART treatment 1 2 7 4. Others, Specify ____________________________________________
Qn. 26: In your culture, are there foods that a lactating or pregnant woman, is not allowed to eat?
1. Yes 2. No (if no, ask qn. 29) 3. Don’t know Qn. 27: If yes, what foods are they? (Please list as given)
1. ________________________________
2. ________________________________

91
3. ________________________________
4. ________________________________
Qn. 28: Please tell me why pregnant or lactating women are not allowed to eat the listed foods. (Please insert given food items and the reasons given Food item Reasons
Qn. 29: When HIV-positive mother give birth to babies, how are they fed:
1. Breastfed for only 4 months 2. Not breastfed at all 3. Given other soft foods 4. Other Specify_______________________________________
SECTION E: FEEDING FREQUENCY AND DIET DIVERSITY
Qn. 29: During the previous 24 hours, did you consume:
Eating occasion Yes = 1 No = 0
Any food before a morning meal (breakfast) A morning meal Any food between morning and lunch Lunch Any food between lunch and supper Supper Any food after supper Total
Qn. 30: In the previous 24 hours (yesterday) did you consume:
Foods Yes = 1
No = 0
a) Cereals (maize, sorghum, rice, bread)

92
b) Roots/Tubers (potatoes, cassava, sweet potatoes, yams) c) Legumes (beans, peas, lentils, G.nuts) d) Milk/Milk products (milk, Yoghurt, cheese, shabwe) e) Eggsa f) Meat/Offals (beef, goat, sheep, rabbit, chicken, byenda, liver, pork) g) Fish (mukene, nkejje, mpuuta, ngege, male, nsonzi) h) Oil/fat (vegetable oil, ghee, margarine/blue band, cow boy, kimbo) i) Sugar/Honey (sugarcane) J) Fruits (bananas, oranges, passion, pineapple, paw paw, mangoes, yellow berries) k) Vegetables (Ntulla, nakati, doodo, onions, carrots, cabbage, Avodavo, french
beans) Total Comment:
Please thank the respondent
Quantitative Methods (Questionnaire, luganda version)
RAKAI HEALTH SCIENCES PROGRAM EKIWANDIIKO EKYOKUNEDDANYEREZA KU BUMANYIRIVU, ENDOOWOZA N’ENKLA KU BY’ENDIISA MU BANTU ABALINA AKAWUKA KA MUKENENYA ABAKOLWAKO MU NTEGEKA Y’OKUJANJABIBWA AKAWUKA KA MUKENENYA (Abakulu)
AKATUNDU A: EBINYONYOLA KU MULWADDE
Edwaliro w’ajanjabibwa: __________________
Ennamba y’omuntu abuuza ebibuuzo: |___|___|___|
Ennaku z’omwezi ebibuuzo lw’ebiddidwamu: ____/______/20___
Ennamba y’omulwadde eya computer:
Ennamba ya filo:
Kati Obeera wa: Ekyalo (ekifo wotera okusangibwa)/LC-1: __________________ Ennamba y’essimu (bwaba olina): _____________________

93
AKATUNDU B: EBITWATA KU MULWADDE Emyaka gy’omulwadde:_____ Wazaalibwa ddi: ____/_____/_____ Mukazi/Musajja? ____ dd mm yyyy Bufumbo bwa ngeri ki: 1. Ssimufumbo (tafumbirwangako) 2. Mufumbo
3. Yanoba 4. Bayawukana 5. Namwandu/Ssemwandu Wali osomyeko mu ssomero? 1. Yee 2. Nedda. Bwekiba nedda, → Omulimu gwakola Wakomawa? 1. P1 – P2 2. P3 – P4 3. P5 –P7 4. S1 – S4 5. S5 – S6 6. Technical/University Okola mulimu ki? ____________________________________ (kibuuze addamu ebibuuzo) Wandiika ekiddibwamu/ebiddibwamu nga bwebiri_______________ Wandiika ebiddidwamu bibiri, nga otandika nekisoose okuddibwamu) Okulima ebyokulya ewaka/okuwanyisa 01 Okulima ebyokutuunda 02 Okukola emirimu egyawaka 03 Alabirira awaka (nga muntu we oba mukamaawe) 04 Okusogola omwenge 05 Akola mu Gavumenti/mu office/asomesa 06 Muvubi 07 Asoma 08 Musirikale 09

94
Atuunda duuka 10 Musuubuzi 11 Atunda bbaala oba alina ebbaala 12 Avuga bimitoka binene 13 Bwaba talina mulimu (buuza oba talima wadde okukola emirimu gy’awaka 14 Musawo (si mu gavumenti) 15 Apatana mirimu egyabulijjo 16 Awereza mu kifo we batunda emmere/nanyini kifo ekitunda emmere 17 Akola Nviri/alina saluuni 18 Muzimbi 19 Makanika (emmotoka, obugaali, ebikozesa amasanyalaze) 20 Ekirala (Nnyonyola) _____________________________ 21 Bwaba nga talima mulimu gwakubiri (okozesa eNedda) 88 Muzaddewo/akulabirira akola mulimu ki? ____________________________________ (Abaaba abakulu abatakola, buuza omuzadde/amulabirira, ky’akola) Wandiika ekiddibwamu/ebiddibwamu nga bwebiri ____________________________ (Wandiika ebiddidwamu bibiri, nga otandika nekisoose okuddibwamu) Okulima ebyokulya ewaka/okuwanyisa 01 Okulima ebyokutuunda 02 Okukola emirimu egyawaka 03 Alabirira awaka (nga muntu we oba mukamaawe) 04

95
Okusogola omwenge 05 Akola mu Gavumenti/mu office/asomesa 06 Muvubi 07 Asoma 08 Musirikale 09 Atuunda duuka 10 Musuubuzi 11 Atunda bbaala oba alina ebbaala 12 Avuga bimitoka binene 13 Bwaba talina mulimu (buuza oba talima wadde okukola emirimu gy’awaka 14 Musawo (si mu gavumenti) 15 Apatana mirimu egyabulijjo 16 Awereza mu kifo we batunda emmere/nanyini kifo ekitunda emmere 17 Akola Nviri/alina saluuni 18 Muzimbi 19 Makanika (emmotoka, obugaali, ebikozesa amasanyalaze) 20 Ekirala (Nnyonyola) _____________________________ 21 Bwaba nga talima mulimu gwakubiri (okozesa eNedda) 88
AKATUNDU C: EBIPIMO BY’OMULWADDE
Obuzito 1(kg): ______ Obuzito 2 (kg): ______
Obuwanvu 1(cm): _______ Obuwanvu 2(cm): _______
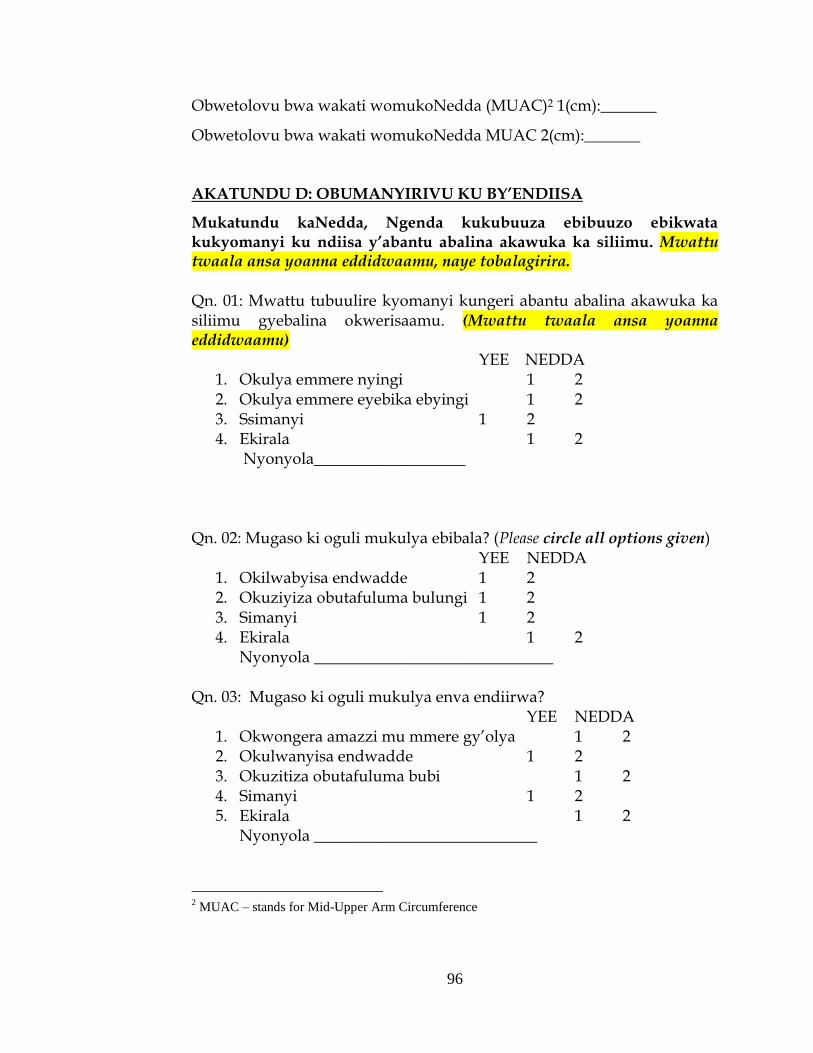
96
Obwetolovu bwa wakati womukoNedda (MUAC)2 1(cm):_______
Obwetolovu bwa wakati womukoNedda MUAC 2(cm):_______
AKATUNDU D: OBUMANYIRIVU KU BY’ENDIISA
Mukatundu kaNedda, Ngenda kukubuuza ebibuuzo ebikwata kukyomanyi ku ndiisa y’abantu abalina akawuka ka siliimu. Mwattu twaala ansa yoanna eddidwaamu, naye tobalagirira. Qn. 01: Mwattu tubuulire kyomanyi kungeri abantu abalina akawuka ka siliimu gyebalina okwerisaamu. (Mwattu twaala ansa yoanna eddidwaamu) YEE NEDDA
1. Okulya emmere nyingi 1 2 2. Okulya emmere eyebika ebyingi 1 2 3. Ssimanyi 1 2 4. Ekirala 1 2
Nyonyola___________________
Qn. 02: Mugaso ki oguli mukulya ebibala? (Please circle all options given) YEE NEDDA
1. Okilwabyisa endwadde 1 2 2. Okuziyiza obutafuluma bulungi 1 2 3. Simanyi 1 2 4. Ekirala 1 2
Nyonyola ______________________________ Qn. 03: Mugaso ki oguli mukulya enva endiirwa?
YEE NEDDA 1. Okwongera amazzi mu mmere gy’olya 1 2 2. Okulwanyisa endwadde 1 2 3. Okuzitiza obutafuluma bubi 1 2 4. Simanyi 1 2 5. Ekirala 1 2 Nyonyola ____________________________
2 MUAC – stands for Mid-Upper Arm Circumference
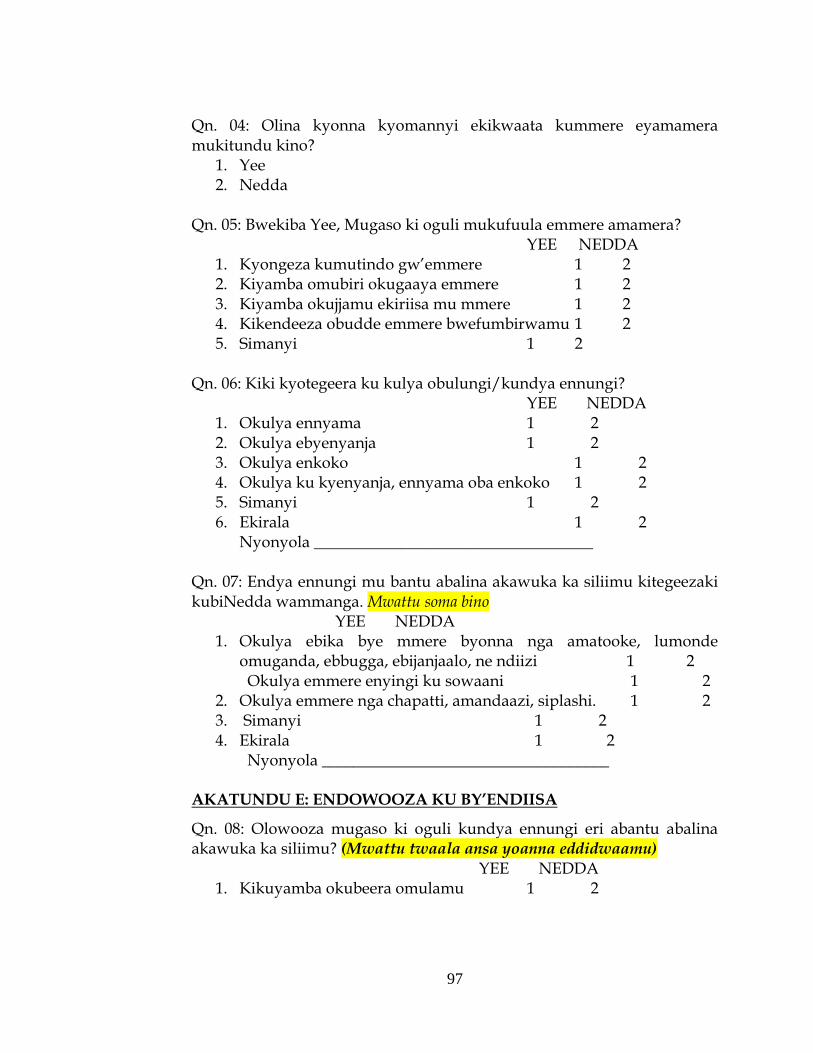
97
Qn. 04: Olina kyonna kyomannyi ekikwaata kummere eyamamera mukitundu kino?
1. Yee 2. Nedda
Qn. 05: Bwekiba Yee, Mugaso ki oguli mukufuula emmere amamera?
YEE NEDDA 1. Kyongeza kumutindo gw’emmere 1 2 2. Kiyamba omubiri okugaaya emmere 1 2 3. Kiyamba okujjamu ekiriisa mu mmere 1 2 4. Kikendeeza obudde emmere bwefumbirwamu 1 2 5. Simanyi 1 2
Qn. 06: Kiki kyotegeera ku kulya obulungi/kundya ennungi?
YEE NEDDA 1. Okulya ennyama 1 2 2. Okulya ebyenyanja 1 2 3. Okulya enkoko 1 2 4. Okulya ku kyenyanja, ennyama oba enkoko 1 2 5. Simanyi 1 2 6. Ekirala 1 2 Nyonyola ___________________________________
Qn. 07: Endya ennungi mu bantu abalina akawuka ka siliimu kitegeezaki kubiNedda wammanga. Mwattu soma bino YEE NEDDA
1. Okulya ebika bye mmere byonna nga amatooke, lumonde omuganda, ebbugga, ebijanjaalo, ne ndiizi 1 2
Okulya emmere enyingi ku sowaani 1 2 2. Okulya emmere nga chapatti, amandaazi, siplashi. 1 2 3. Simanyi 1 2 4. Ekirala 1 2
Nyonyola ____________________________________ AKATUNDU E: ENDOWOOZA KU BY’ENDIISA
Qn. 08: Olowooza mugaso ki oguli kundya ennungi eri abantu abalina akawuka ka siliimu? (Mwattu twaala ansa yoanna eddidwaamu)
YEE NEDDA 1. Kikuyamba okubeera omulamu 1 2

98
2. Kiyamba omubiri okukozesa ART 1 2 3. Simanyi 1 2 4. Ekirala 1 2
Nyonyola____________________________________ Qn. 09: Olowooza kiki ekisobola okutuuka ku bulamu bw’omuntu alina akawuka ka siliimu singa alya bubi? (Mwattu twaala ansa yoanna eddidwaamu)
YEE NEDDA 1. Okukogga 1 2 2. Okulwalwala nga okukolola, okuddukana1 2 3. Baffa 1 2 4. Simanyi 1 2 5. Ekirala 1 2 Nyonyola______________________________________
Qn. 10: Abantu abalina akawuka ka siliimu beetaga amaanyi amangiko buli lunaku okusinga abatalina kawuka ka siliimu ?
1. Yee 2. Nedda 3. Simanyi
Qn. 11: Bwekiba Yee, Lwaki olowooza abantu abalina akawuka ka siliimu beetaaga amaanyi amanjiko buli lunaku okusinga abatalina kawuka ka siliimu?
YEE NEDDA 1. Kiyamba okubeera n’obulamu obulungi 1 2 2. Okusigara ng’oyina amaanyi 1 2 3. Okulwanyisa endwadde 1 2 4. Okuzzaawo amanyi agakozesedwa akawuka ka silimu 1 2 5. Simanyi 1 2 6. Ekirala 1 2 Nyonyola______________________________________
Qn. 12: Olowooza akawuka ka siliimu ne ndwadde endala ezikwata buli kadde bikosa abalwadde mungeri gyebalyaamu emmere?
1. Yee 2 Nedda

99
3. Simanyi Qn. 13: Bwekiba Yee, Mu ngeri ki gy’olowooza akawuka ka siliimu ne endwadde endala ezikwata buli kadde gye bikosaamu abalwadde mu ngeri gyebalyaamu emmere? (Mwattu twala ansa yonna eddidwaamu)
YEE NEDDA 1. Okisesema 1 2 2. Obutayagala kulya 1 2 3. Okubulwa amaanyi agafumba 1 2 4. Simanyi 1 2 5. Ekirala 1 2 Nyonyola ___________________________
Ngenda kukusomera emboozi wammanga, mwattu mbuulira oba: 1.Okkiriza nnyo, 2.Okkiriza, 3.Tokkiriza, 4.Tokkiriza nakatoNedda, oba 5.Simanyi (Mwattu ansa e’yokutaano tokibuuza) Qn. 14: Okulya ebika bye mmere ebyenjawulo (nga akawunga, amatooke, Ovacado, ejjobyo, n’ebijanjaalo) kirungi eri abantu abalina akawuka ka siliimu era kiyamba ku kuziyiza endwadde eza buli kadde.
Yee Nedda 1. Okkiriza nnyo 1 2 2. Okkiriza 1 2 3. Tokkiriza 1 2 4. Tokkiriza nakatono 1 2 5. Simanyi 1 2
Qn. 15: Kyamugaso abantu bonna mu maka okuyamba abantu abalina akawuka ka siliimu kukufumba emmere ennungi era nga erimu ekiriisa.
Yee Nedda 1. Okkiriza nnyo 1 2 2. Okkiriza 1 2 3. Tokkiriza 1 2 4. Tokkiriza nakatono 1 2 5. Simanyi 1 2
Qn. 16: Abakyala abalina akawuka ka siliimu nga bayonsa oba nga balina embuto bateekwa okulya emmere nyingiko nga erimu ebika byemmere byonna buli lunaku.
Yee Nedda 1. Okkiriza nnyo 1 2

100
2. Okkiriza 1 2 3. Tokkiriza 1 2 4. Tokkiriza nakatono 1 2 5. Simanyi 1 2
Qn. 17: Abaana abazaalibwa abakyala abalina akawuka ka siliimu bateekwa kuyonkera ebbanga:
1. Eritassukka myezi ena (4) 2. Eritassukka myezi mukaaga (6) 3. Eritassukka myezi abiri mwena (24) 4. Simanyi 5. Ekirala, Nyonyola _________________________
AKATUNDU F: ENKOLA KU BY’ENDIISA
Mukatundu kaNedda, ngenda kukuubuuza ebintu bitoNeddako, ku byo’kola ewaka wo, ebikwatagana Nedda’kweriisa obulungi nga olina akawuka ka silimu. Qn. 18: Okusobola okufuna amaanyi gewetaaga, olya ebijjulo bimeka mulunaku? (Ekijjulo kye kyenkya, ekyemisana ne e kyeggulo, ate obumpwankimpwanki kyekyokulya ekiriibwa wakati w’ebijjulo).
1. Wakiri ebijjulo bisatu 2. Wakiri ebijjulo bisatu n’obumpwankipmwanki bubiri 3. Okulya emmere w’enjifunira mu lunaku 4. Simanyi
Qn. 19: Mu lunaku, emirundi emeka gyolya ebibala (nga ndiizi, amapaapaali, emicungwa, ennaannaansi, nebirala ebiri mu kitundu)?
1. Omulundi gumu 2. Emirundi ebiri 3. Emirundi esatu 4. Ssirya Bibala 5. Ekirala, Nyonyola ___________________________
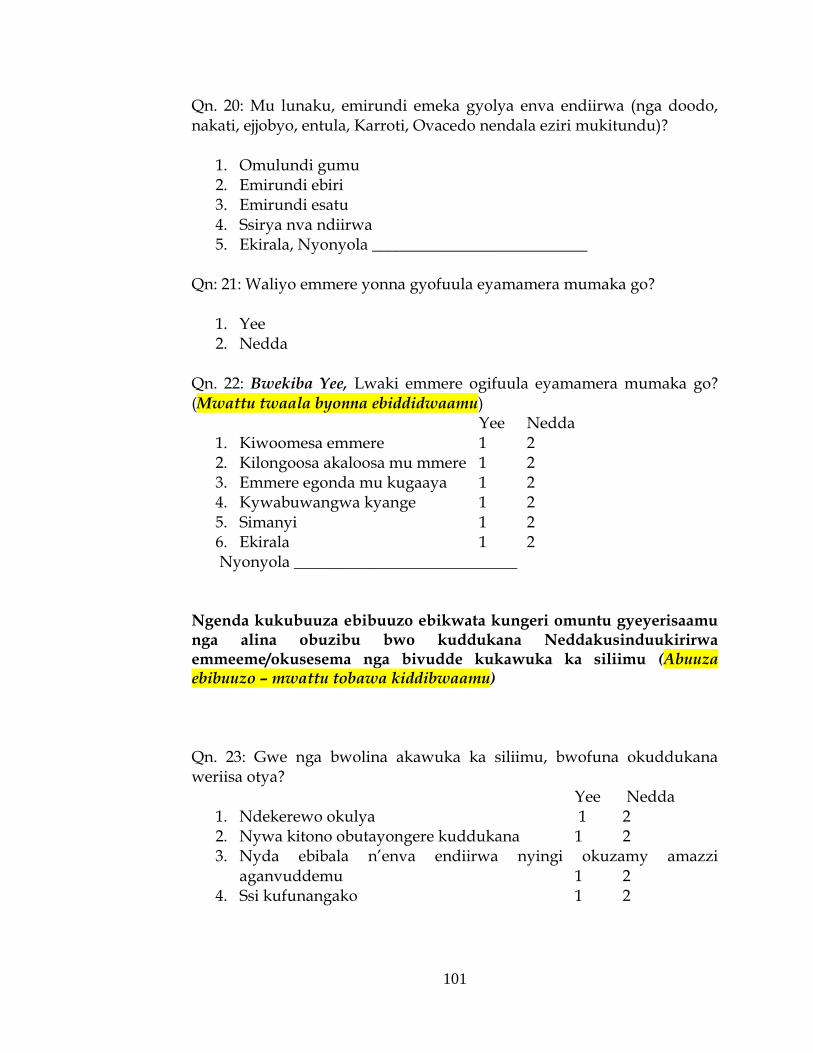
101
Qn. 20: Mu lunaku, emirundi emeka gyolya enva endiirwa (nga doodo, nakati, ejjobyo, entula, Karroti, Ovacedo nendala eziri mukitundu)?
1. Omulundi gumu 2. Emirundi ebiri 3. Emirundi esatu 4. Ssirya nva ndiirwa 5. Ekirala, Nyonyola ___________________________
Qn: 21: Waliyo emmere yonna gyofuula eyamamera mumaka go?
1. Yee 2. Nedda
Qn. 22: Bwekiba Yee, Lwaki emmere ogifuula eyamamera mumaka go? (Mwattu twaala byonna ebiddidwaamu)
Yee Nedda 1. Kiwoomesa emmere 1 2 2. Kilongoosa akaloosa mu mmere 1 2 3. Emmere egonda mu kugaaya 1 2 4. Kywabuwangwa kyange 1 2 5. Simanyi 1 2 6. Ekirala 1 2 Nyonyola ____________________________
Ngenda kukubuuza ebibuuzo ebikwata kungeri omuntu gyeyerisaamu nga alina obuzibu bwo kuddukana Neddakusinduukirirwa emmeeme/okusesema nga bivudde kukawuka ka siliimu (Abuuza ebibuuzo – mwattu tobawa kiddibwaamu) Qn. 23: Gwe nga bwolina akawuka ka siliimu, bwofuna okuddukana weriisa otya?
Yee Nedda 1. Ndekerewo okulya 1 2 2. Nywa kitono obutayongere kuddukana 1 2 3. Nyda ebibala n’enva endiirwa nyingi okuzamy amazzi
aganvuddemu 1 2 4. Ssi kufunangako 1 2

102
5. Ekirala 1 2 Nyonyola __________________________________
Qn. 24: Gwe nga bwolina akawuku ka siliimu, bwofuna okusindukirirwa emmeeme/okusesema, weriisa otya?
Yee Nedda 1. Nya akamere katono emirundi egiwera 1 2 2. Nebaka wansi nga nakamala okulya emmere 1 2 3. Ndya emmere ewomerera 1 2 4. Ssikufunangako 1 2 5. Ekirala 1 2 Nyonyola ________________________________
Manyi nti abakyala bomukitundu kiNedda abali mumyaka egizaala basalawo okuzaala abaana oba okutandika amaka n’abaagalwa baabwe. Qn. 25: Omukyala ali olubuto nga mulwadde wa akawuka ka siliimu bwa kizuula nti akendeera obuzito/akogga, akolaki? : (Mwattu buuza bino)
Y N DK 1. alya ebijjulo bisatu wamu Neddabumpwankimpwanki emirundi
ebiri olunaku 1 2 7 2. Agenda mumaaso Neddakumira eddagala lye erikendeeza akawuka
ka siliimu 1 2 7 3. Yebuuza kumusawo we ebyendiisa okufuna amagezi g’okwerisaamu
1 2 7 4. Ekirala, Nyonyola ____________________________________________
Qn. 26: Mubuwangwa bwo, waliwo emmere yonna omukyala ayonsa oba alina olubuto gyatakkirizibwa kulya?
1. Yee 2. Nedda (Buuza Qn. 29) 3. Simanyi
Qn. 27: Bwekiba Yee, Mmere ki? (Mwattu wandiika byonna ebiddidwamu)
1. ________________________________
2. ________________________________
3. ________________________________

103
4. ________________________________
Qn. 28: Mwattu tubuulire lwaki abakyala abali embuto oba abayonsa tebakkirizibwa kulya mmere eyo ewereddwa waggulu. (Mwattu wandiika emmere eddidwamu ku Qn.31, n’ensonga)
Emmere Ensonga
Qn. 29: Abakyala abalina akawuka ka siliimu bwe bazaala abaana babwe, babaliisa batya?
Yee Nedda 5. Bayonsa okumala emyeezi ena gyokka 1 2 6. Tebayonsa nakamu 1 2 7. Babawa emmere endala egonda 1 2 8. Ekirala 1 2
Nyonyola____________________________ AKATUNDU E: EMIRUNDI GYO’OLYA N’EBIKA BYE MMERE
EBYENJAWULO
Mukatundu kaNedda, tugenda kunyumya ku ngeri gye w’erisizzaamu mu ssawa abiri mu nya eziyise, ate Neddakumanya ebika bye’emmere gyewalidde. Qn. 29: Mwattu tubuulire, oba mussawa abiri munnya (24) eziyise walidde ku:
Omulundi gw’okulya Yes = 1 No = 0
Emmere yonna nga tonaba kulya kyankya Eky’enkya Emmere yonna wakati w’ekyenkya n’ekyemisana

104
Eky’emisana Emmere yonna wakati w’ekyemisana n’ekyeggulo Eky’eggulo Emmere yonna oluvannyuma lw’ekyeggulo Omuwendo
Qn. 30: Mussawa abiri munnya (24) eziyise walidde ku mmere eno wansi:
Foods Yes = 1 No = 0
a) Emmere ey’ensigo (Kasooli, Omuweemba, Omucere, Omugaati) b) Emmere e’yemirandira/ebirookwa (obummonde, Muwogo, Lumonde
omuganda, amayuuni) c) Enva ezilimibwa (ebijanjaalo, Kawo, Empokyi, ebinyeebwa) d) Amata/ebikolebwa mu mata (amata, bongo, omugizo, shabwe) e) Amaggi f) Ennyama/Byenda (ey’ente, embuzi, endiga, akamyu, enkoko, byenda,
ekibuumba, embizzi) g) Ebyenyanja (mukene, nkejje, mpuuta, ngege, male, nsonzi) h) Emizigo egisiika (egiva mubilime, ogwente, ogw’okumugaati, cow boy,
kimbo) i) Sukaali/Omubisi gw’enjuki (ekikajjo) J) Ebibara (ameenvu, emicungwa, obutunda, ennaanansi, amapaapali,
emiyembe, entuuntunu) k) Enva endiirwa(Ntulla, nakati, doodo, obutungulu, caroti, emboga, ovacedo,
obujanjaalo obu french) Omuwendo
Bwoba oyina ekirara ky’oyongerako, kiwandiike wano: Webaze azzeemu ebibuuzo
13.3.2 Qualitative Methods (Focus Group Discussions Guide)
English Version

105
DRAFT FOCUS GROUP DISCUSSION GUIDE
NUTRITION FOR PLHIV ENROLLED ON THE RAKAI HEALTH
SCIENCES HIV/AIDS CARE PROGRAM (1hr, 30 min)
Welcome (2 min)
Thank you for coming. We appreciate your joining us today. We would
like you to remember that you are the experts here and that you are here
so that we can learn from you.
Introduction (5 MIN)
We would like to remind you that our (RHSP) nutrition pilot program that aimed at improving the nutrition knowledge, attitudes, and practices of PLHIV who are enrolled on the RHSP HIV/AIDS Care Program ended in December 2010, we thank you for having participated in the activities. The purpose of our discussion today is to share gain an understanding of how this community perceived the nutrition activities, as far as your nutrition knowledge, beliefs and practices are concerned. The information will help RHSP to better plan for future interventions in this area. In addition, we shall identify benefits, lessons learnt and challenges faced and discuss how these can be turned into opportunities for better intervention planning at community level.
AT THIS POINT READ THROUGH THE CONSENT FORM
Discussion rules The only rules for this meeting are that we should all address the subject being asked when we decide to talk. Please try not to get us off track. Also, only one person should speak at a time. We would also like to remind you to please respect the privacy of the other participants here today and don’t tell other people who are not here, about our discussion. This is especially important if any of you know each other.

106
We would like to tape record this discussion. The recording is only to help us make sure we ―hear‖ everything that is said and to make good notes. Only people who are working on this program will ever hear any of the recordings or read the notes we take. After the planned study period and data analyses have been completed, these tapes will be destroyed. Does anyone have any objections to being tape-recorded? We are here to only learn from you, as far as our pilot nutrition program for PLHIV is concerned, but not to discourage you from taking part in any other program activities or to change any of your personal opinions or habits. We believe that you know what PLHIV enrolled on the RHSP Care program think about this pilot nutrition program. Please remember, there are no right or wrong answers. We want to hear what you think and how we can improve it. I will not do most of the talking, but let’s have a simple and brief discussion. In our discussion today, keep in mind that we are interested in your opinions and perspectives. We would like to know what you think, what you think other people think, and what you know other people have practiced. The purpose of this discussion is not to talk about your own personal experiences. However, if you feel you have had your own personal experience that is relevant to the discussion and that you are comfortable talking about, you are welcome to share this information. In summary, during our discussion, if you or someone you know has had an experience related to the topic, it would be most appreciated if you could share that story – but you don’t have to. We also want to know where your opinions differ from each other and from others we have already spoken to. Please remember to respect others when they are talking. This discussion will last about an hour and a half. Is there anyone who can’t stay for the duration of the discussion? Are there any questions before we begin?
Let us introduce ourselves before we begin our discussion. I am___________________ and I will lead our discussion today. Over there is _________________________ who will be taking notes during the discussion. (Introduce any other observers) As I mentioned, the entire session will be tape-recorded. To protect everyone’s privacy, we will use first names only in this room. Your response will not be linked to your personally, so feel free to say whatever is on your mind. I request our participants to introduce themselves. Let begin with you
107
_________________________ (choose someone). Please tell us your name and tell us a little bit about where you come from. Thank you.
NUTRITION KNOWLEDGE, ATTITUDES AND PRACTICES [1 hr]
I. General nutrition questions
Nutrition Knowledge
1. What do you know about nutrition for PLHIV? 2. What does good nutrition/eating well mean in this community?
Nutrition attitudes 3. What factors, other than frequent infections, do you think hinder
eating well in this community 4. What do you think are the consequences of poor nutrition among
PLHIV? 5. What do you think are the factors that influence nutrition for
PLHIV in this community? Nutrition Practices
6. Please tell us how the PLHIV get the required energy in their diets, using locally available foods.
7. What nutrition care do PLHIV, in this community, receive when they experience symptoms like loss of taste, appetite and weight loss?
8. Please share with us the different ways that PLHIV can get sufficient safe drinking water in a day
9. How many times do the PLHIV eat in a day?
II. Group Specific questions
Infant and child nutrition care – to be answered by parents and caretakers
1. During the first three days after delivery, how does this community feed the infants to ensure good nutrition?
2. Let’s discuss exclusive breastfeeding. What do you know about this issue? How is it done among PLHIV in this community?

108
3. How do you feed HIV-Positive children who are not breastfed? 4. What do parents/care takers do when a child living with HIV fails
to take in enough food yet they are on medication? Maternal nutrition and Care
5. In what ways are mothers living with HIV supported while lactating and pregnant in this community? What kinds of food do they eat?
6. How do HIV-Positive mothers ensure good nutrition in this community?
III. Recommendations
7. In your views, what can RHSP do to improve on their nutrition program?
CLOSING REMARKS [10 MIN]
1. Thank Participants 2. Give out compensation 3. Leave the site
109
Focus Group Discussion Guide (Luganda Version)
EKIWANDIIKO EKIKWATA KUKUBAGANNYA EBIROWOOZO
OKWAWAMU ENDYA ERI ABANTU ABALINA AKAWUKA KA SIRIIMU ABAWEBWA OBUJANJABI BW’AKAWUKA KA SIRIIMU OKUVA MU KITONGOLE KYA RAKAI HEALTH SCIENCES PROGRAM. (1hr, 30 min) Tubanirizza (2min) Mwebale nnyo okujja okutwegattako olwaleero. Mujjukire nti mwe bakafulu era muli wano tusobole okubako byetuyiga okuva gyemuli.
Ennyanjula (5min)
Twagala okubajjukiza nti okugezesa pulogulamu ekwata ku kusomesa nokubudabuda ku ndya
eyali egenderera okwongera ku mutindo gwokumannya, endowooza n’enkola ku ndya eri abantu abalina akawuka ka siriimu, abawebwa obujanjabi bw’akawuka ka siriimu okuva mu kitongole kya Rakai Helth Sciences program, yakolebwa okumala ebbanga lya myeezi ena, era yakoma mu December 2010. Ekigendererwa mu kukubagannya ebirowoozo olwaleero kwe kumannya abantu bo mukitundu kino gyebategeramu ebikwata ku ndya, nokumannya oba ggwe eyennyigira mu kukubaganya abirowoozo, omutindo gwo ogwokumannya, endowooza n’enkola ku ndya bweguyimidde. Amawulire ge munatuwa gajja kuyamba Rakai Program okukola entekateka ennungamu mu kukola enkola endala ezefananyirizako ngeno. Okwongerezako, tujja kulaba ebirungi, ebizibu abinaba bizuuliddwa bijja kukubaganyizibwako ebirowoozo bigonjoolwe okusobola okukola enkola endala nga ziri kumutindo mu byaalo.
110
(MWATTU SOMA ENZIKIRIZA, BW’OTUUKA WANO)
Ebyokugoberera mu kukubaganya ebirowoozo. Ebyokugoberera mulimu ffena okwogera ku malamwa bwetunaba tusabiddwa okwogera, gezaako okulaba nti tova ku mulamwa, omuntu omu yajja okuba ng’ayogera. Twagala okwongera okubajjukiza okuwangana ekitiibwa era nobutabulirako bantu balala abatali wano ebyo byetukubagannyizako ebirowoozo. Kino kikulu nnyo naddala eri abo abamanyiganye. Okukubagannya ebirowoozo kuno kujja kukwatibwa ku katambi. Akatambi kajja kutuyamba okuwuliririza obulungi ebyo byetunaba tukubaganyizako ebirowoozo. Abo bokka abakozi abakola ku pulogulamu eno bebayinza okuwuliriza ebyo ebikwatiddwa ku katambi oba okusoma ebyo ebiwadiikiddwa. Ekiseera ekyokunoonyereza bwekinagwako, nga nokwekenennya ebivudde mukunoonyereza kumaze okukolebwa, obutambi okuli amaloboozi bujja kusanyizibwawo. Waliwo atandyagadde doboozi lye kukwatibwa kukatambi? Tuli wano okubako byetuyiga okuva gyemuli ku pulogulamu ekwata ku kusomesa, nokubudabuda ku
ndya eri abantu abalina akawuka ka siriimu nga bweyimiridde, naye si kubagana kwenyigira mu
bintu ebirala Rakai Program byekola oba okubakyusa mu ndowooza. Tukimanyi nti mumanyi biki abantu abafuna obujanajabi okuva mu kitongole kya Rakai Program byebalowooza ku pulogulamu eno ey’endya. Mujjukire nti tewali ansa ntufu ate tewali nfu. Tawagala kuwulira biki byolowooza tulabe engeri gyetuyinza okubitereza. Sijja kwogera binji nnyo wabula tukubaganye ebirowoozo nga tuli ku mulamwa. Mukukubaganya ebirowoozo olwaleero, mukimanye nti twagala kumanaya ndowooza zamwe n’egeri gyemulabamu ebintu. Twagala okumanya ki kyolowooza, ki kyolowooza abantu abalala kye balowooza, nabiki byomannyi abantu abalala bye batadde mu nkola. Ekigenedererwa kyokukubaganya ebirowoozo si kwogera ggwe byomannyi. Wabula, oli wa ddembe okukubaganya ebirowoozo kwekyo kyomanyi ekyali kikutuuseko nga kyamugaso eri abakubaganya ebirowoozo abalala. Mubimpimpi bwetunaba tukubaganya ebirowoozo, bwoba ggwe oba omuntu omulala gwomannyi bwaba alina ekyali ki mutuseeko nga
111
kikwata ku mulamwa kyandibadde kirungi notubulira nga bwe byali naye ekyo tekikirizibwa. Twagala era okumanya wa endowooza zamwe wezawukanira, era nawa wezawukanira n’abantu abalala betwamala edda okukubaganya nabao ebirowoozo. Jukira okuwa ekitiibwa abalala nga bogera. Okukubaganya ebirowoozo kujja kutwala ebbanga lya saawa emu n’ekitundu. Waliwo omuntu yenna atasobola kuwayo budde obwo? Nga tetunaba kutandika waliwo alina ekibuuzo kyonna? Katweyanjule nga tetunatandiika kukubagannya birowoozo. Amannya gange nze _________________________________era nze ngenda okukubiriza okukubagannya ebirowoozo olwareero. Munange oyo ye___________________________ agenda kuba nga awandiika byetukubaganyako ebirowoozo. (Abantu abalala abatunuulizi nabo banjulibwa). Nga bwenakyogeddeko edda nti mukukubaganya ebirowoozo amaloboozi gajja kukwatibwa kukatambi, mukizimbe wano tujja kukozesa linnya lya ddini olwokukuma ebyama. Byonaba otuzemu tebijja kukwataganyizibwa na nkula yo. Nolwekyo oli wa ddembe okwogera kyowulira ku mutima. Nsaba abagenda okukubaganya ebirowoozo beyanjule. Katutandike nawe_____________________________ (londayo omuntu). Tusaba otubulire amannya go nawa gyobeera. Webale nnyo. ENDOWOOZA ENKOLA N’OKUMANNYA KU BY’ENDYA [1 hr]
I. Ebibuuzo eby’endiisa ebikwata ku buli omu
OKUMANNYA KU BY’ENDYA
1. Biki byomannyi ebikwatagana nebyendya eri abantu abalaina akawuka ka siriimu?
2. Okulya obulungi kitegeeza ki mu kitundu gyobeera?
ENDOWOOZA KU BY’ENDYA 3. Ngojeko okulwalalwala, bintu ki ebirala ebiremesa abantu okulya
obulungi mu kitundu kino? 4. Biki byolowooza ebiyinza okutuuka ku muntu alina akawuka ka
siriimu nga bivudde ku ndya embi?

112
5. Biki byolowooza ebiyinza okuba nga biviirako endya okuba ennungi oba embi eri abantu abalina akawuka ka siriimu mu kitundu kyo?
ENKOLA KU BY’ENDYA
6. Mu kitundu kyo buki abantu byebakola okulaba nti abantu abalina akawuka ka siriimu bafuna amanyi gebetaga okuva mu mmere gyebalya, naye nga beyambisa emmere eyabulijjo.
7. Kubudabudibwa kwa ngeri ki abantu bomukitundu kyo abalina akawuka ka siriimu kwebafuna bwe bafuna obubonero buno nga: obutayagala obutawula oba byalya biwoma oba nedda, outayagala kulya oba okukogga?
8. Mwattu tubulire engeri abantu abalina akawuka ka silimu gye bafunamu amazzi agokunywa mu lunaku.
9. Abantu abalina akawuka ka Silimu balya emirundi emeka mu lunaku?
II. Bino bikwata ku bitundu ebimu eby’abantu bano wammanga
Abaana abato – biddibwaamu ba maama oba abalabirila abaana 8. Mu nnaku essatu ezisooka ng’omwana nga yakazaalibwa abantu
bomukitundu kino baliisa batya abaana okukasiza ddala nti balisibwa mu ndya ennungi?
9. Katukubaganye ebirowoozo ku byokuyoosa omwana kwooka nga taweebwa kintu kirala. Kino okimanyi ko ki? Kikolebwa kitya eri abantu abalina akawuka ka siriimu mu kitundu kyo?
10. Oliisa otya abaana abalina akawuka ka siriimu nga tebayonseddwa?
11. Biki abazadde/abalabirira abaana abalina akawuka ka siriimu bye bakola singa, abaana abalina akawuka ka siriimu balemererwa okulya emmere ebamala ate nga bali kuddagala?
Endiisa y’abamaama nendabirira yaabwe
12. Ngeri ki abakyala abalina akawuka ka siriimu gye bayambibwamu nga bayonsa oba nga bali mbuto mu kitundu kyo?
13. Ngeri ki abakyala abali embuto gye bakumamu endya ennungi mu kitundu kyo?
III. Endagirilo

113
14. Mundowooza yo biki Rakai Program byeyinza okukola okusobola
okutumbula omutindo gwa pulogulamu yayo eyebyendya.
OKUGGALAWO KW’OLUKIIKO [10 MIN]
4. Webaze ababadde mu lukiiko 5. Bawe entambula 6. Muddeyo ku ofiisi.
13.3.3 Key Informant Interviews (KIIs) Guide (English version)
NUTRITION FOR PLHIV ENROLLED ON THE RAKAI HEALTH
SCIENCES HIV/AIDS CARE PROGRAM (1.30 min)
WELCOME
Thank you for coming. We appreciate your joining us today. We would like you to remember that you are the experts here and in communities where we implemented our pilot nutrition program, so, we are here to learn from you.
Introduction
The purpose of talking to you today is to assess the changes so far, which have happened as a result of the pilot nutrition program that was successfully completed. We would like to talk to you about the pilot nutrition program that was integrated into the RHSP Care Program. We would like to know your perceptions of the nutrition program, so we can capture your experiences, lessons learnt as well as identify gaps that still exist. We would also like to get your suggestions on how RHSP might improve its nutrition education and counselling program as part of the health education package for PLHIV. (At this point, read the consent)

114
NUTRITION KNOWLEDGE, ATTITUDES AND PRACTICES
Nutrition Knowledge
1. Please tell us what you benefited from the Pilot Nutrition Program that was completed in December 2010.
a. In what ways did the key nutrition messages meet the PLHIV’s expectations?
b. How would you tell that knowledge in nutrition for PLHIV improved?
c. What aspects of the key nutrition messages did people like most?
Nutrition attitudes
2. What do you think about the NEC pilot program with all the practical sessions (cooking and Drama) that we had?
3. What fears did you have about nutrition for PLHIV? 4. How were these fears cleared?
Nutrition Practices
5. Of all that we taught about eating well for PLHIV, what have you been able to do?
6. What challenges do you face that would hinder eating well?
PILOT NEC PROGRAM PROCESSES
7. Please comment on the following processes: a. Designing of the nutrition program b. Staff training to implement the nutrition program c. Implementing the pilot program – interruptions, delegating,
acceptability
PILOT NEC PROGRAM EXPERIENCES/ LESSONS LEARNT 8. How would you describe your experience of eating the way we
taught? 9. In adopting eating well for PLHIV, what have you learnt along the
way? 10. What other problems do you think could hinder eating well in
PLHIV?

115
PILOT NEC PROGRAM CHANGES SO FAR 11. What are the positive effects of the NEC program on PLHIV’s
health? 12. What are the reasons for attaining the changes/lack of it? 13. Please tell us about the common complaints/challenges that PLHIV
faced throughout the nutrition pilot program implementation. IDENTIFYING GAPS
14. In your view, what do you consider as the strengths of the nutrition program?
15. What do you consider to be weaknesses of the nutrition program? 16. Are there areas in nutrition that you feel we didn’t cover, which
you would otherwise want to be knowledgeable? 17. Please tell us what other nutrition topics would you like to
learn/cover? 18. What sustainability plan do you have for the nutrition program?
RECOMMENDATIONS 19. What can RHSP do to improve the NEC program? 20. Is there anything else that you would like to talk about the NEC
program? CONCLUSION
We have finished with the interview now. I want to thank you very much for your time. This has been a very good discussion and I learnt a lot from you. Thank you.

116
Key Informant Interviews (KIIs) Guide (Luganda version) ENDYA ERI ABANTU ABALINA AKAWUKA KA SIRIIMU ABAWEBWA OBUJANJABI BW’AKAWUKA KA SIRIIMU OKUVA MU KITONGOLE KYA RAKAI HEALTH SCIENCES PROGRAM. (1hr, 30 min)
Tukwanirizza (2min) Tukwanirizza, webale kukirizza okujja n’otwegattako olwaleero. Twagala ojjukire nti wanno n’eyo gy’obeera, gyetwakolera emirimo gyaffe egy’okuyigiriza endiisa ennungi mu bantu abaina akawuka ka silimu, gwemukugu era tuzze okuyiga okuva gy’oli
Ennyanjula (5min)
Ekigendererwa ky’okwogeerako nawe olwaleero kwe kwekenennya enkyukakyuka oenjigiriza aya’endya emmungi mu bantu abalina akawuka ka silimu gyetwakamaliriza, gye yakaleetawo ku ndya ennumgi. Twagala okwogera ko naawe ku mpereeza ya RHSP ey’okuyigiriza abantu endya ennungi eri abantu abalina akawuka ka silimu. Twagala okumanya endowooza n’enzikiriza ya bantu ku nsomesa eya’endya ennungi, tulyooke tumanye biki bye’tuyiseemu, bye’tuyizeemu, nokunoonyereza biki byeturinza okwongera mu misomo gyaffee egyo. Era twagala okufuna ebirowoozo byo ku biki ekitongoole kya RHSP byekiyinza okukola okusobola okulongoosa empereeza yayo ey’okuyigiza endya ennungi eri abantu abalina akawuka ka silimu.
(Mukaseera kano, soma ekiwandiiko ekiraga enzikiriza)
ENDOWOOZA, ENKOLA, N’OKUMANNYA KU BY’ENDYA
OKUMANNYA KU BY’ENDYA
1. Mwattu mbulira biki bye’waganyurwaamu mu njigiriza e’yendiisa eri abantu abalina akawuka ka silimu gyetwakamaliriza mu December 2010.

117
a. Mungeri ki obubaka obukulu obukwata kundya ennungi bwatuukiriza ekyetaagisa eri abantu abayina akawuka ka silimu?
b. Omanya otya nti obumanyirizu kundya ennungi eri abantu abalina akawuka ka silimu bweyongeddeko?
c. Bitundu ki mu bubaka obukulu ku ndya ya’abantu abalina akawuka silimu byebasinga okwagala?
ENDOWOOZA KU BY’ENDYA
2. Biki by’olowooza ku njigiriza, ey’endiisa ennungi eri abantu abalina akawuka ka silimu, n’ebyakolebwa byonna, (nga okufumba n’omuzannyo) bye twamaliriza?
3. Biki bye’wali otya ku ndiisa eri abantu abalina akawuka ka silimu? 4. Bye wali otya kukino byagwaawo bitya?
ENKOLA KU BY’ENDYA
5. Ku byetwa’asomesa kundya ennungi erib abantu abalina akawuka ka silimu, biki by’osobodde okukola/okugoberera?
6. Bizibuki by’ofuna ebiziyiza endya yo ennungi? PILOT NEC PROGRAM PROCESSES
7. Mwattu baaki byoyogera ku nzirukanya y’emirimu gya endiisa ennungi eri abantu abalina akawuka ka silimu:
a. Enteekateeka y’emirimu gyino b. Enjigiriza y’abakozi okusobola okuweereza obubaka
obukulu ku ndiisa ennungi eri abantu abalina akawuka ka silimu.
c. Enkola y’emirimu gyino PILOT NEC PROGRAM EXPERIENCES
8. Onnyonyola otya ebyo by’osanze, mu kukola ebyo ebyayigirizibwa ku ndya ennungi eri abantu abalina akawuka ka silimu??
9. Mukulya obulungi eri abantu abalina akawuka ka silimu, oyizeemu biki?
10. Biki ebiyinza okuziyiza abantu abalina akawuka ka silimu okulya obulungi?
PILOT NEC PROGRAM CHANGES SO FAR
11. Birungi ki eri obulamu bwa’abantu abalina akawuka ka silimu eby’ava mu njigiriza eya’endiisa ennungi?

118
12. Nsonga ki ezireetedde bino okubeerawo oba obutabeerawo?/lack of it?
13. Mwattu tubuulire okwemulugunya oba obuzibu by’abantu abalina akawuka ka silimu byebaayitamu nga toweereza enjigiriza eeno.
LESSONS LEARNT
14. Oyizeemu biki munjigiriza ey’endya ennungi gye twasomesanga? IDENTIFYING GAPS
15. Mukulabakwo, biki by’otwala nga ebikulu mu pulogulamu y’endya ennungi?
16. Biki by’otwala nga ebitai bikulu/obunafu mu pulogulamu y’ebyendya ennungi?
17. Mwattu tubulire ebitundu ebirala mu ndiisa ennungi, gyewandiyagadde tusomeseeko oba tugabane obumanyirivu?
18. Oyina nteekateeka ki enasobozesa pulogulamu eno eyenya ennungi eri abantu abalima akawuka ka silimu okugenda mu maaso?
RECOMMENDATIONS
19. Olowooza biki RHSP byeyinza okukola okusobola okusikiriza
abantu abalala okwenyigira mu mpereeza yayo ey’endiisa ennungi eri abantu abalima akawuka ka Silimu?
20. Waliyo ekibrara kyonna kyewandiyagadde okwogera ekikwata ku puloguramu eyayigiriza endya ennungi eri abantu abalina akawuka ka silimu?
CONCLUSION Tumaliriza okukubaganya ebirowoozo byaffe.Njagala okukwebaza olw’obudde bwotuwadde.okukubaganya ebirowoozo kubadde kulungi nnyo era njize bingi nyo okuva gyoli. Webale

119
13.4 Consent form (English version)
Project Title: Process evaluation of the Pilot Nutrition Education and Counseling Program integrated into the RHSP HIV/AIDS Care program
Principal Investigator: Ms. Florence Tushemerirwe Other Investigators: Dr. Gertrude Nakigozi, Dr. Valerian Kiggundu,
Dr. Godfrey Kigozi and Dr. Esther Buregyeya My name is__________________________________________, I would like to invite you to participate in the evaluation of our Pilot Nutrition Education and Counseling (NEC) Program, for PLHIV. Background: This NEC pilot program was started to improve the nutrition knowledge, attitudes, and practices of PLHIV who are enrolled on the RHSP HIV/AIDS Care Program. The nutrition program activities included workshops, drama and cooking demonstrations. This program was implemented for four months, and we are currently evaluating it to capture its benefit to our clients so far, experiences and lessons learnt and any information on how we can improve it. Objectives and plan of the evaluation: General objective To describe the processes of the NEC pilot program, capture changes in nutrition KAP so far, experiences, lessons learnt and best practices that RHSP can gainfully apply to roll out the NEC Program in Care and other projects.
Specific Objectives
1. To document the processes, experiences and lessons learnt in nutrition knowledge, attitudes and feeding practices as a result of the Pilot NEC Program.
2. To capture changes/improvements so far, in nutrition knowledge, attitudes and feeding practices of PLHIV enrolled on the Rakai Health Sciences HIV/AIDS Care program.
3. To document any nutrition KAP changes/benefits from the Pilot NEC program among PLHIV between the three clinics.
We shall do this using a questionnaire, focus group discussions and Key Informant Interviews. The questionnaire is quiet brief, with simple and easy questions understand. Clients shall be sampled and invited to
120
participate in the interviews. The interviews shall take a maximum of 30minutes each. The Focus group discussions and key informant interviews take between one and one hour and half hours. Procedures If you agree to participate in this evaluation, and if you are sampled, we shall invite you to come to the clinic for the interview, focus group discussions and key informant interviews. During the interviews, we shall ask you questions about yourself like age; date of birth; education; marital status; occupation as well as weighing, measuring your height and Mid-Upper Arm Circumference. We shall also ask you about your current nutrition knowledge, attitudes and practices for PLHIV. During the focus group discussions and key informant interviews, we shall discuss topics about nutrition knowledge, attitudes and practices, your experiences and lessons learnt as well as your recommendations for the nutrition program improvement. Risks from participating in the evaluation There are no risks involved in participating in this evaluation. Benefits Free nutrition knowledge shall be shared with the evaluation participants and clarifications of un-clear information during the intervention shall be made. Nutrition counselling shall be provided for those who need it. Assurance of confidentiality The evaluation responses in the questionnaires shall be kept in secure data drawers in Kalisizo. Only the program personnel will have access to these records and all data shall be kept confidential to the full extent allowed by law. Participation is voluntary Your participation in this evaluation is completely voluntary. You are free to withdraw at any time or decline to participate in any or all components of the study (interview, focus group discussion). Such a decision will not affect your access to RHSP HIV/AIDS Care services now or in future. Cost of Participation Services related to your participation in this evaluation are provided at no cost to you.

121
Compensation All participants in this evaluation shall be reimbursed with their transport costs. Each participant shall receive between 2,000 – 10,000/= as transport re-fund and between 3,000 – 5,000/= as time compensation for the time lost as a result of participation in the evaluation activities. Questions/Points of Contact If you have any questions, please ask and we shall do our best to answer them. If you have additional questions or if you need to discuss any other aspects of the evaluation, you can contact: Ms. Florence Tushemerirwe and Mr. Micheal Juuko Ssajjabi– Nutritionists, RHSP Kalisizo Office (0701 444 244) Dr. Valerian Kiggundu, Dr. Gertrude Nakigozi, Medical Officers, RHSP Kalisizo Office (020 0900 384). If there is any portion of this consent explanation sheet that you do not understand, ask the interviewer before signing. You will receive a copy of this consent form. Statement of Participant Consent (Adults)
I _________________________________age ____________have been asked
to participate in the evaluation of the pilot Nutrition Education and
Counselling program for PLHIV enrolled on the RHSP HIV/AIDS Care
Program. The interviewer has explained the program to me, how long it
will take, as well as the risks and benefits of participation. The information
above has been read to me and I have been given an opportunity to ask
questions about this program. All questions were answered in a way that I
understand. If I have more questions about this program, I can ask the
program representative, Ms. Florence Tushemerirwe, the program
nutritionist or Dr. Valerian Kiggundu, Mr. Juuko Micheal, Mr. Stephen
Kigongo, the medical officers or their representatives.

122
I understand that my participation is voluntary and that I can decline to
be in the program evaluation or leave the program evaluation at any time,
without losing any benefits or access to RHSP Care services. I am signing
my name below to indicate my consent to participate in this program. I
will be given a copy of the signed consent form.
__________________________________ ___________________ SIGNATURE OF PARTICIPANT (Thumb print if non-literate) DATE _________________________________ ___________________ PRINTED NAME OF PARTICIPANT INITIALS INDICATING
CONSENT OR DO NOT CONSENT
ADDRESS OF PARTICIPANT
___________________________ ________________________ SIGNATURE OF WITNESS PRINTED NAME OF WITNESS DATE (same as participant)
123
Consent Form (Luganda version) EKIWANDIIKO EKIRAGA OKUKIRIZA
Project Title: Okugezesa pulogulamu ekwata ku kusomesa
nokubudabuda ku ndya eri abantu abalina akawuka ka Siliimu abawebwa obujanjabi bw’akawuka ka siliimu okuva mu kitongole kya Rakai Health Sciences program.
Akulira okunoonyereza: Muky. Tushemerirwe Florence Abanoonyereza abalala: Dr. Gertrude Nakigozi, Dr. Valerian Kiggundu,
Dr. Godfrey Kigozi ne Dr. Esther Buregyeya Erinnya lyange nze __________________________________ nkusaba wetabe mukunoonyereza okuzuula biki ebyava mukugeseza pulogulamu ekwata ku kusomesa nokubudabuda ku ndya eri abantu abalina akawuka ka Siliimu. Ennyanjula: Pulogulamu ekwata ku kusomesa nokubudabuda ku ndya eri abantu abalina akawuka ka Siliimu, yatandikia okwongera ku mutindo gwokumannya, endowooza n’enkola ku ndya eri abantu abalina akawuka ka Siliimu, abawebwa obujanjabi bw’akawuka ka Siliimu okuva mu kitongole kya Rakai Helth Sciences program. Mu pulogulamu eno mwalimu emisomo, okuzannya omuzannyo, n’okuyingiriza okufumba. Enkola eno yamala ebbanga lya myeezi ena, mu kiseera kino tugezako okulaba ebirungi abantu abalina akawuka ka Siliimu byebaganyuddwamu, byebayitamu, byebayimagu n’okufuna ebirowoozo okulaba engeri gyetuyinza okwongera okugitumbula. Ebigendererwa n’egeri yokubifunamu: Ekigendererwa ekikuru Okunnyonyola enkora yapulogulamu, okumnya enkyuukakyuuka mu bumanyirivu bw’endya ennungi, endoowooza n’enkola ku ndya eri abantu abalina akawuka ka Siliimu, abawebwa obujanjabi bw’akawuka ka Siliimu okuva mu kitongole kya Rakai Health Sciences program. Oluvannyuma, RHSP esobole okuddukanya pulogulaamu eno n’endala zinnewaayo, nga ekozesa amagezi gemujiwadde. Ebigendererwa ebilara
124
1. Okuwandiika ebyakolebwa, ebyayitibwaamuamu, nebyayigibwa eri obumanyirivu, endowooza n’ekola nga bivudde mu pulogulamu eeno.
2. Okuzuula pulogulamu nga bwerinyisizza erinyisiza omutindo gwokumannya, endowooza n’endiisa eri abantu abalina akawuka ka silimu nga bafuna eddagala okuva ku RHSP.
3. Okuwandiika enkyuukakyuuka mu bumanyirivu, endowooza n’endiisa eri abantu abalina akawuka ka silimu wakati wa amalwaliro agatuusibwako pulogulamu eeno.
Kino kijja kukolebwa nga tubuuza ebibuuzo ebya sekinomu n’okukubaganya ebirowoozo nga tuli kibija. Ebibuuzo ebya sekinomu si bingi nnyo era byangu okutegera. Abantu abalina akawuka, n’abaweereza ba RHSP bajja kulondebwa era bayitibwe okwetaba mu kubuzibwa ebibuuzo. Ebibuuzo bijja kutwala eddakiika nga makumi asatu. Okukubaganya ebirowoozo kujja kuberamu abantu munaana mu buli kibinja era kujja kutwala ebbanga sawa emu ne sawa emu n’ekitundu. Enkola nga bwenaba: Bwokiriza okwetaba mu kunoonyereza okuzuula biki ebyava mu kugezesa pulogulamu ekwata ku kusomesa nokubudabuda ku ndya eri abantu abalina akawuka ka Siliimu, era nga olondeddwa tujja kukuyita ojje ku kalwaliro ka SSuubi obuzibwe ebibuuzo nokukubaganya ebirowoozo. Tujja kukubuuza ebibuuzo ebikukwatako nga emyaka, ennaku z’omweezi zebakuzalirako, obuyigirize, oli mufumbo, omulimu gwokola wamu n’okukupima obuzito, obuwanvu okugerageranya obuzito bwo n’obuwanvu. Era tujja kukubuza okumannya kwo kati. endowooza yo n’ekola ebikwata ku ndya, eri abantu abalina akawuka ka Siliimu. Mu kukubaganya ebirowoozo, tujja kwogera ku kumanya, endowooza n’enkola ebikwata ku ndya era tubabuze biki ebisobola okukolebwa okusobola okwongera omutindo mu maaso. Ebizibu ebiyinza okubawo: Tewali buzibu bwonna bwojja kufuna nga wetabye mukunoonyereza kuno. Byonoganyulwamu: Okumanyisibwa okwobwerere okukwata ku ndya kujja kwogerwako wamu okuva eri abo abetabye mu kunoonyereza, ebinaba bitategerekese

125
bulungi bijja kunyonyolwa. Okubudabudibwa ku ndya kujja kuwebwa abo abanaba bakwetaze. Ebikukwatako bijja kukumibwa nga byakyaama. Byonoba otuzemu mu bibuuzo ebikubuziddwa awamu nebikukwatako bijja kukumibwa mu zikabadda ensibire ddala gguluggulu e Kalisizo, era bijja kukumibwa ng’amateeka bwegalagira. Abo bokka nga bakozi ba kitongole bebajja okutukirira zi kabadda ezo. Okwetaba mu kunoonyereza kwa kyeyagalire. Okwetaba mu kunoonyereza kwa kyeyagalire. Oli wa ddembe okukuvamu obudde bwonna oba okugana okukwetaba mu kimu oba byonna. (okubuzibwa ebibuuzo ebya sekinomu oba okukubaganya ebirowoozo). Okusalawo kwo tekujja kukulobera kufuna bujanjabi bwofuna obukwata kukawuka ka Siliimu kati oba gyebujja. Okusasulira okwetaba mukunoonyereza. Ebinakolebwa ku kwetabakwo mu kunoonyereza kuno bya kukolebwa nga tosasudde ka ssente konna. Okusasulirwa: Abo bonna abetabye mu kunoonyereza kuno bajja kudizibwa entambula. Buli omu ajja kudizibwa Uganda Shs 2,000 – Shs 10,000 nga za ntambula, era ne Uganda Shs 3,000 – Shs5,000 nga zabiseera nokutataganyizibwa nga wetaba mu kunoonyereza kuno. Ebibuuzo/abantu boyinza okutukirira: Bwooba olina ekibuuzo kyonna nkusaba obuze era nange ndi mwetegefu okubyanakula. Bwoba olina ebibuuzo ebirala byonna oba ekintu kyonna kyoyagala okukubaganyako ebirowoozo tukirira: Muky. Tushemerirwe Florence oba Mr, Juuko Ssajjabi Micheal abasawo abakola ku byendya, e Kalisizo essimu (0701 444 244). Dr. Valerian Kiggundu, Dr. Gertrude Nakigozi abasawo abebyobulamu abasangibwa e Kalisizo essimu (020 0900 384) Bwewabawo akatundu konna akekiwandiiko kino ko tategedde buuza omusawo nga tonasako mukono. Ojja kufuna kopi ye kiwandiiko kino. Ekiwandiiko ekiraga okukiriza kwo: Nze ____________________________________ ow’emyaka___________ nsabiddwa okwetaba mu pulogulamu Ekwata ku kusomesa nokubudabuda ku ndya eri abantu abalina akawuka ka Siliimu abawebwa obujanjabi bw’akawuka ka

126
Siliimu okuva mu kitongole kya Rakai Helth Sciences program. Omusawo anyinyonyodde ebikwata ku pulogulamu eno, ebbanga lyekunatwala obuzibu obuyinza okubawo wamu nokuganyulwa olwokwetaba mukunoonyereza. Ebyo byonna ebyogeddwako waggulu binsomeddwa era nempebwa omukisa okubuuza ebibuuzo ebikwata ku pulogulamu eyo. Ebibuuzo byonna binziriddwamu mu ngeri gyentegera obulungi. Bwemba nina ebibuuzo ebirala byonna ebikwata ku pulogulamu eno nsobola okubuza Muky.Tushemerirwe Florence, omusawo akola ku byendya, oba Dr. Valerian Kiggundu, Mr. Juuko Micheal, Mr. Kigongo Stephen abasawo abebyolamu oba abo ababakikiridde. Ntegera nti okwetaba kwange mukunooyereza kuno kwa kyeyagalire, era nti nsobola okukuvamu obudde bwonna nesibako kyenfiirwa wadde ebyo ebikolebwa ekitongole kya Rakai Health Sciences Program. Ntekako omukono okulaga nti nzikirizza okwetaba mu kunoonyereza kuno. Nja kuwebwa kopi yekiwandiiko gyentadeko omukono. ____________________________ ___________________ Omukono / Ekinkumu kya kirizza Ennaku z’omweezi __________________________________ __________________ Erinnya lya kirizza Enyukuta z’amanya eziraga nti
akkirizza oba nedda _______________________________________________________________ Endagiliro ya kirizza. _________________________ ________________ Omukono gwabaddewo Erinnya lyabaddewo _____________________________ Ennaku z’omweezi