indications, methodology, and classification of results of tilt-table testing
TRANSCRIPT

Indications, Methodology, andClassification of Results of Tilt-
Table TestingRichard Sutton, DScMed, and Daniel M. Bloomfield, MD
Tilt-table testing has become an important part of theevaluation of patients with unexplained syncope, al-though not every patient with vasovagal syncope re-quires it. Studies have attested to the effectiveness of thetechnique for providing direct diagnostic evidence of apatient’s susceptibility to vasovagal syncope. This articlereviews the need for tilt-table testing and the recom-mended methods for performing a test. In addition, a
detailed classification of the hemodynamic patterns ofcollapse displayed over the course of a tilt-table study isprovided. These distinctive collapse patterns documentthe evolution of a syncopal event and are particularlyimportant to identify because they can influence theselection of therapy. Q1999 by Excerpta Medica, Inc.
Am J Cardiol 1999;84:10Q–19Q
Over the past 15 years, tilt-table testing has becomean important part of the evaluation of patients with
unexplained syncope, and there is substantial agreementon the effectiveness of the technique for providing directdiagnostic evidence of susceptibility to vasovagal synco-pe.1,2 Tilt-table testing presents an orthostatic challengethat stimulates vasovagal syncope and, in patients whodo not have structural heart disease, provides the highestdiagnostic yield of all tests used to evaluate unexplainedsyncope. In some studies of unexplained syncope, tilt-table testing established the diagnosis of syncope in40–70% of patients.3,4 By allowing physicians to ob-serve the evolution of a patient’s syncope,5 tilt-tabletesting has significantly enhanced our understanding ofthe pathophysiology of the disorder and provided in-sights into potentially useful treatments.6,7 There areseveral different hemodynamic responses to tilt-tabletesting—a classification of which was proposed in1992.8 The goals of this article are to review indicationsfor and methods of tilt-table testing, describe the hemo-dynamic profiles of patients with positive tilt-table tests,and further refine the classifications of syncopal collapsepatterns.
RATIONALE FOR TILT-TABLE TESTINGTilt-table testing is a provocative test used to deter-
mine a patient’s susceptibility to vasovagal syncope. Theprovocation is rather simple: an orthostatic stimuluscauses blood to pool in the lower extremities and, insusceptible individuals, vasovagal syncope often ensueswithin approximately 20 minutes. The triggering mech-anism in vasovagal syncope is thought to result from a
relatively central hypovolemia, which occurs because ofblood pooling in the lower extremities. The afferent endof this reflex may be mediated by left ventricular or rightatrial mechanoreceptors that are activated during vigor-ous contraction around underfilled chambers in a situa-tion similar to severe hemorrhage. Information fromthese mechanoreceptors travels along vagal afferent Cfibers to the brain stem, which mediates the efferentresponse consisting of withdrawal of sympathetic vaso-motor tone and a vagally mediated bradycardia. Thisproposed mechanism remains a matter of debate and hasbeen reviewed more extensively in the literature andelsewhere in this supplement.
Several observations, which have been summarizedby Benditt et al,5 suggest the provoked response duringtilt-table testing is essentially equivalent to the responseduring a spontaneous vasovagal syncopal episode. Pa-tients often describe symptoms of their spontaneous ep-isodes as being remarkably reproduced by tilt-table test-ing. However, relatively little data exist on the collapsepatterns that occur in spontaneous attacks.
WHO NEEDS A TILT-TABLE TEST?In 1996, the American College of Cardiology pub-
lished an Expert Consensus on the use of tilt-tabletesting in the evaluation of patients with unexplainedsyncope.2 There is general agreement that tilt-tabletesting should be done in patients with recurrent syn-cope or in high-risk patients after a single syncopalepisode. Tilt-table testing is used primarily in patientswithout structural heart disease for whom the diagno-sis of syncope is not evident from the history and whohave a negative carotid sinus massage. However, tilt-table testing can be used in patients with structuralheart disease who have had a complete evaluationincluding a negative electrophysiology study. In con-trast, patients with unexplained syncope who do nothave structural heart disease may undergo tilt-tabletesting as the initial diagnostic test in their evaluation.
Not every patient with vasovagal syncope requiresa tilt-table test. Many patients, particularly youngerones, describe a long prodrome consisting of symp-toms of lightheadedness, nausea, and sweating before
From the Royal Brompton and Chelsea Westminster Hospitals, London,United Kingdom; and Columbia University, College of Physicians andSurgeons, New York, New York, USA.
This article may contain discussion of off-label or investigationaluses (not yet approved by the FDA) of various therapeutic agents.Please refer to the box provided on page 2Q of this supplement for adisclosure of such agents.
Address for reprints: Richard Sutton, DScMed, Pacing and Elec-trophysiology, Royal Brompton Hospital, 149 Harley Street, W1-N,1HG London, United Kingdom.
10Q ©1999 by Excerpta Medica, Inc. 0002-9149/99/$20.00All rights reserved. PII S0002-9149(99)00692-X

syncope. In a young person with a structurally normalheart, these symptoms strongly suggest a diagnosis ofvasovagal syncope, and further testing may not benecessary. Often, however, geriatric patients willpresent for evaluation of unexplained syncope andsimply describe waking up on the ground after losingconsciousness, having experienced no warning signsor prodromal symptoms. The absence of prodromalsymptoms is worrisome and makes the diagnosis ofsyncope more difficult. We have learned from tilt-table tests in geriatric patients that vasovagal syncopecommonly occurs without warning symptoms. Duringtesting, as blood pressure decreases, patients oftenreport feeling fine and adamantly deny any symptoms.A few seconds later, after the blood pressure decreasesbelow a critical threshold, the patient abruptly losesconsciousness. After the syncopal episode, after thetable has been returned to the supine position andconsciousness is regained, patients may deny any pro-dromal symptoms or even losing consciousness. Thistype of amnesic response is common in older patientsand may explain the complete lack of symptoms re-ported before losing consciousness.
For some patients, tilt-table testing can be usefuleven if the diagnosis of vasovagal syncope is evidentfrom their history. One example is patients who havea psychological or emotional need to establish thediagnosis with provocative testing. Syncopal episodescan be extremely traumatic, and the ordeal is com-pounded upon recurrence. Emergency department vis-its and hospital admission can further increase con-cern, and the patient desires a definitive diagnosisrather than an empiric one based on history alone. Forthese patients, the provocation of syncope during tilt-table testing can be reassuring and therapeutic, espe-cially when their symptoms are reproduced. Tilt-tabletesting might also be required for patients who mustdocument their diagnosis for occupational reasons,even if a diagnosis of vasovagal syncope is evidentfrom their history.
Finally, the hemodynamic patterns of collapse evi-denced by tilt-table testing may provide subtle cluessuggesting an initial line of therapy.
METHODOLOGYThere are numerous variations in the methods used
for tilt-table testing—a review of which is beyond thescope of this article.1–3,9,10 Tilt-table tests are oftendone in 2 stages: a prolonged period of head-up tilt inthe drug-free state, followed by a shorter period ofhead-up tilt after administration of a provocative phar-maceutical agent. We believe that the most valuableinformation is obtained during drug-free passive tilt.
Tilt-table testing should be performed in a quiet,comfortable room with lights dimmed. Patients shouldfast for at least 3 hours before testing, or overnight inpreparation for early morning studies. We prefer totest without placement of intravenous or intra-arteriallines. Electrocardiogram recordings (2 or 3 leads)should be monitored, as should blood pressure. Duringtilt-table testing, it is essential to measure blood pres-sure on a beat-to-beat basis because the pattern of
blood pressure response cannot be observed by auto-mated cuff measurements at 2-minute intervals. Spe-cifically, we have noted large fluctuations in bloodpressure and transient periods of asymptomatic ormildly symptomatic hypotension that are missed by2-minute cuff measurements. In vasovagal syncope,blood pressure often decreases abruptly and precipi-tously. This is frequently missed by cuff measure-ments made at 2-minute intervals, but patients areuncomfortable with automated measurements taken atshorter intervals. We are aware of only 2 devicescurrently available for noninvasive, beat-to-beat bloodpressure monitoring. The Finapres (Amsterdam Uni-versity) measures blood pressure from a finger using aphotoplethysmographic technique. The Colin 7000(Colin Medical Instruments, San Antonio, Texas)measures blood pressure from the radial artery usingarterial tonometry. Corroborative data on the accuracyof blood pressure during tilt-table testing exist only forFinapres.11
As testing begins, patients are tilted head-up to anangle between 60° and 80° on a table with a footplateand safety straps. The precise angle of tilt within thisrange is probably not important; the results of testsusing 60° and 70° have been compared and only smalldifferences were noted.12 However, tilting patients to,60° is inefficient because the angle may not providesufficient orthostatic stress.13 Tilting to 90° is uncom-fortable because patients feel they might fall forward;this angle also may provide less passive postural stim-ulus. The duration of upright tilt should be at least30–45 minutes. In a few large series of patients un-dergoing tilt-table testing, the mean time to syncopewas approximately 25 minutes, with a standard devi-ation of 10 minutes.3,10,13,14The preference for a 45-minute head-up tilt is based on 2 standard deviationsbeyond the mean time to syncope,3 and capturing 95%of patients who are likely to develop syncope duringtesting. Although the long duration of head-up tilt canbe frustrating to physicians performing the tests, webelieve the most valuable information is obtainedfrom a patient who experiences syncope during adrug-free tilt. Although shortening the period of drug-free tilt and moving quickly to a tilt with a provocativeagent may be tempting, it sacrifices potentially impor-tant information in the drug-free state that could beuseful in selecting therapy.
The appropriate endpoint for a tilt-table test isinduction of syncope or presyncope associated withintolerable hypotension and resulting in an inability tomaintain postural tone.2 We do not believe the testsshould be terminated for asymptomatic hypotensionexcept in extreme cases (i.e., systolic blood pressures,50 mm Hg). Although the risk of developing a fatalventricular arrhythmia during a tilt-table test is ex-tremely small, we feel strongly that every tilt-tablelaboratory should have resuscitation equipment imme-diately available. Appropriate staffing for tilt-tabletests varies across laboratories in different areas of thecountry and in different parts of the world. An expe-rienced nurse or medical technician can perform drug-free tilt-table testing independently, provided a physi-
A SYMPOSIUM: TREATMENT FOR PATIENTS WITH VASOVAGAL SYNCOPE 11Q

cian is readily available. For tilt-table tests using pro-vocative agents, a physician should be present.
Pharmacologic provocation: A number of provoca-tive agents have been employed during tilt-table test-ing for eliciting susceptibility to hypotension brady-carda.2 The 2 most common agents are isoproterenoland nitroglycerin.9,10 Isoproterenol is ab agonist thatincreases heart rate and contractility. Most important,it is a venodilator that produces greater amounts ofvenous pooling when the patient is tilted upright.Nitroglycerin is a vasodilator that principally affectsthe venous system and capacitance vessels. Becauseof their venodilating properties, both agents increasethe orthostatic stress associated with upright posture,and in so doing increase the likelihood of provokingvasovagal syncope.
When nitroglycerin is used as the provocativeagent, it is given at the end of a prolonged period ofhead-up tilt (30–45 minutes) while the patient is stillupright.10 After sublingual administration of nitro-glycerin (300 or 400mg tablets), the patient remainsupright for an additional 20 minutes. Recently, inves-tigators have begun using a sublingual nitroglycerinspray (400mg) that acts more quickly than tablets andrequires only 10 additional minutes of upright tilt.
Unlike nitroglycerin, isoproterenol is administeredintravenously. Ideally, the intravenous line should beplaced well in advance of the tilt-table test, becausethe discomfort associated with intravenous placementcan pollute the autonomic atmosphere. Unfortunately,this requires placing an intravenous line in all patientsbefore tilt-table testing, although 40–50% of patientshave a positive tilt-table test in the drug-free state.Isoproterenol is administered at the end of a negativedrug-free tilt after the patient has been returned to thesupine position.9 The dosage of isoproterenol variesfrom laboratory to laboratory, although most investi-gators use 1–3mg/min and avoid using 5mg/mingiven the loss of specificity as well as the patient’sdiscomfort at this high dose.12 Some clinicians titratethe isoproterenol dose to an increase in supine heartrate of 20–25% above baseline, which usually resultsin a dose of 1–2mg/min. After the vital signs reach asteady state at a given dose in the supine position, thepatient is tilted head-up for 5–15 minutes and thenreturned to supine before the isoproterenol dose isincreased to the next level.
The decision to use a provocative agent during atilt-table test depends largely on the goals of the test.To establish the diagnosis of vasovagal syncope, thereis no question that adding a drug challenge to a tilt-table test increases sensitivity and diagnostic yield.However, the diagnostic yield of a drug-free tilt-tabletest is still on the order of 30–50%, which is substan-tially higher than any other diagnostic test used toevaluate unexplained syncope. The problem with add-ing a drug challenge during a tilt-table test is theexpected loss of specificity. Because there is no goldstandard for making the diagnosis of vasovagal syn-cope, estimates of the specificity of tilt-table testingare made from the proportion of normal subjects whodevelop syncope during tilt-table testing. Most esti-
mates of the proportion of positive tilt-table test innormal subjects in the drug-free state are approxi-mately 5–15%.12,15 With low doses of isoproterenoland with nitroglycerin, the estimates are in the 15–25% range; with higher doses of isoproterenol, theproportion may be as high as 50%.10,12 Althoughnitroglycerin changes the profile of collapse patternsduring tilt-table testing, the results can still be usefulin selecting therapy.16
With this in mind, the optimal tilt-table test shouldinclude a prolonged period of drug-free head-up tilt—ideally 45 minutes—which is highly specific and pro-vides a high diagnostic yield. The other advantage toa prolonged period of head-up tilt in the drug-freestate is that the hemodynamic information obtainedfrom the test may be useful in guiding initial therapy.
PATTERNS OF COLLAPSE DURINGTILT-TABLE TESTING
In this section, we describe different patterns ofhemodynamic collapse that illustrate the pathophysi-ologic evolution of syncope (Figure 1). These patternsare displayed over the course of tilt-table studies and,in our opinion, suggest specific approaches to therapy.It is important to distinguish the hemodynamic patternof vasovagal syncope from the dysautonomic responseto head-up tilt and from the response seen in patientswith postural orthostatic tachycardia syndrome(POTS), because the 3 patterns represent distinctpathophysiologic processes that result in a decrease inblood pressure.
Vasovagal syncope: Patients with vasovagal syn-cope have an abrupt decrease in blood pressure ac-companied by some decrease in heart rate that isthought to represent a Bezold–Jarisch reflex. Withinthe group of patients with vasovagal syncope, we haveobserved several patterns of hemodynamic collapse.
It is important to note that the classification ofhemodynamic collapse patterns (i.e., determining therelation between decrease in blood pressure andchanges in heart rate) requires beat-to-beat monitoringof arterial blood pressure. We have observed manycases in which blood pressure decreases before adecrease in heart rate; if a test is terminated whenblood pressure begins to decrease, a subsequent de-crease in heart rate cannot be appreciated.
Mixed vasovagal syncope (type 1) is illustrated inFigure 2. Immediately after head-up tilt to 60°, theheart rate increases appropriately and blood pressurealso increases slightly. During the head-up tilt period,blood pressure remains stable and the heart rate in-creases slightly. In the example shown, the syncopalcrisis occurs at 43 minutes when a collapse in bloodpressure precedes a mild reduction in heart rate. In thistype of vasovagal syncope, the heart rate does not fallbelow 40 beats/min for.10 seconds.
Cardioinhibitory vasovagal syncope is character-ized by significant bradycardia during collapse and isdivided into 2 types based on the timing of the de-crease in blood pressure relative to the decrease inheart rate. The syncopal collapse occurs with a de-crease in heart rate to a ventricular rate of,40 beats/
12Q THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 84 (8A) OCTOBER 21, 1999

min for .10 seconds or with an asystolic pause.3seconds. In type 2A vasovagal syncope (Figure 3),blood pressure is somewhat unstable during head-uptilt. During the syncopal crisis, blood pressure clearly
decreases before the decrease in heart rate. There is aperiod of asystole, but it is relatively brief and, mostimportant, occurs after the decrease in blood pressure.
In contrast, type 2B vasovagal syncope exhibits a
FIGURE 1. Outline of the hemodynamic response to tilt-table testing.
FIGURE 2. (A) Type 1 (mixed) vasovagal syncope. The upper panel shows heart rate inbeats/min (range 40–140) and the lower panel shows digital plethysmographic arterialpressure calibrated in mm Hg (blood pressure range 30–180). The time intervals on the hor-izontal axis are in 1-minute increments. The point of adoption of 60& head-up tilt is noted byT (tilt) and return to supine by F (flat). S denotes symptoms. (B) The syncopal crisis is shownon an expanded time base (time intervals 5 1 minute). (Reproduced with permission fromEur J Pacing Electrophysiol.8)
A SYMPOSIUM: TREATMENT FOR PATIENTS WITH VASOVAGAL SYNCOPE 13Q

decrease in blood pressure concurrently with a dra-matic decrease in heart rate and asystole. In the ex-ample shown (Figure 4), the heart rate increases byapproximately 25 beats/min immediately afterhead-up tilt and then decreases abruptly. A long asys-tolic pause associated with a concurrent decrease inblood pressure is also recorded.
Pure vasodepressor or type 3 vasovagal syncope,which in our experience is relatively uncommon, usu-ally refers to pure hypotension without bradycardia(Figure 5). The heart rate increases appropriately im-mediately after head-up tilt. During the syncopal cri-sis, the blood pressure decreases with only a slightdecrease in heart rate.
Our classification of the subtypes of vasovagalsyncope builds on that proposed by investigators forthe Vasovagal Syncope International Study (VASIS).8
Here, the earlier classification is expanded to include2 important responses to tilt-table testing that shouldbe distinguished from the vasovagal syncope respons-es: a dysautonomic response to head-up tilt and POTS.These disorders likely represent pathophysiologic re-sponses to upright posture that may be different fromthe pathophysiology of vasovagal syncope.
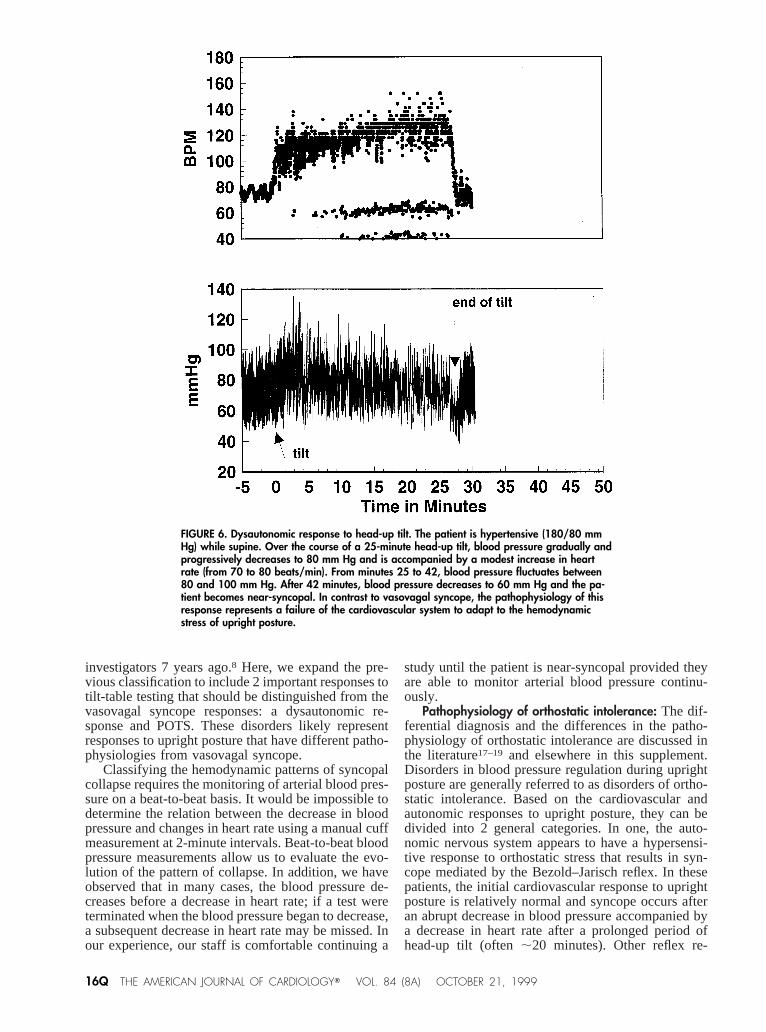
Dysautonomic response to head-up tilt: Patients witha dysautonomic response to head-up tilt demonstrate agradual and progressive decrease in blood pressure,usually with only a small or insignificant change inheart rate (Figure 6). The pathophysiology of thisresponse, in contrast to that of vasovagal syncope,
represents a failure of the cardiovascular system toadapt to the hemodynamic stress of upright posture.
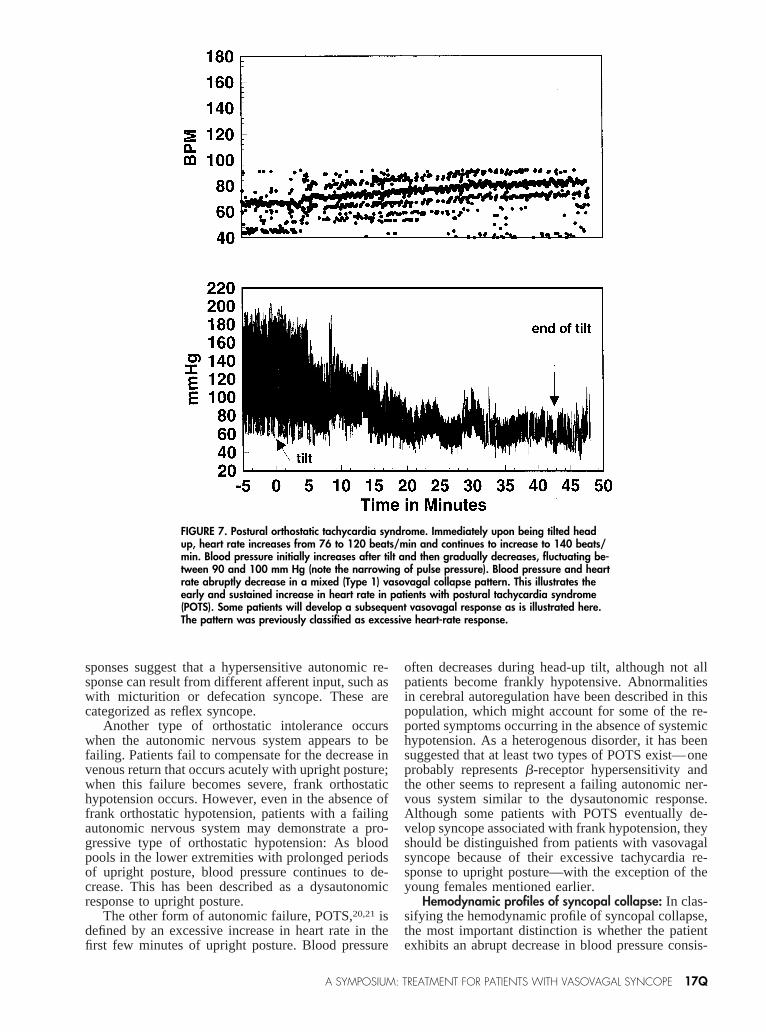
POTS: Patients with POTS demonstrate an earlyand sustained increase in heart rate, often associatedwith a progressive decrease in blood pressure, al-though it can be associated with frank hypotensionand syncope (Figure 7). Some vasovagal patients,especially young females, present with a very promi-nent sinus tachycardia (.120 beats/min) before a va-sovagal-type collapse with blood pressure decreaseand some slowing from the peak heart rate. The pat-tern was previously classified as excessive heart rateresponse.8
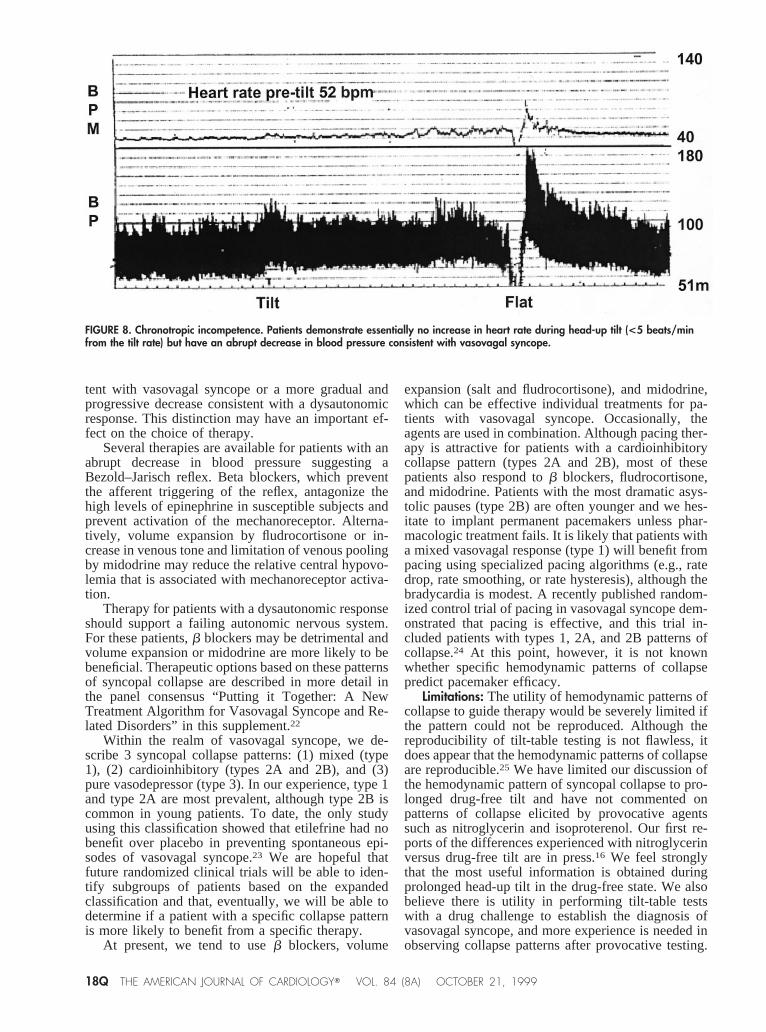
Exclusion—chronotropic incompetence: There arepatients with chronotropic incompetence who developvasovagal syncope during tilt-table testing. These pa-tients demonstrate essentially no increase in heart rateduring head-up tilt (,5 beats/min from the tilt rate)but have an abrupt decrease in blood pressure consis-tent with vasovagal syncope (Figure 8). Originally,these patients were thought to have sinoatrial nodedisease, but studies suggest the response is seen mostin elderly patients with structural heart disease.14 Pac-ing may be indicated based on these findings.
DISCUSSIONWe have described several different hemodynamic
responses that can occur during tilt-table testing. Thissystem builds on the initial classification of the sub-types of vasovagal syncope proposed by the VASIS
FIGURE 3. (A) Type 2A (cardioinhibitory) vasovagal syncope. Note that the heart rate trendshows a persistent extrasystolic activity throughout the tilt that disappears at the time ofsyncopal crisis. (B) Expanded time base: the heart rate decreases to a brief period of asys-tole. (Reproduced with permission from Eur J Pacing Electrophysiol.8)
14Q THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 84 (8A) OCTOBER 21, 1999
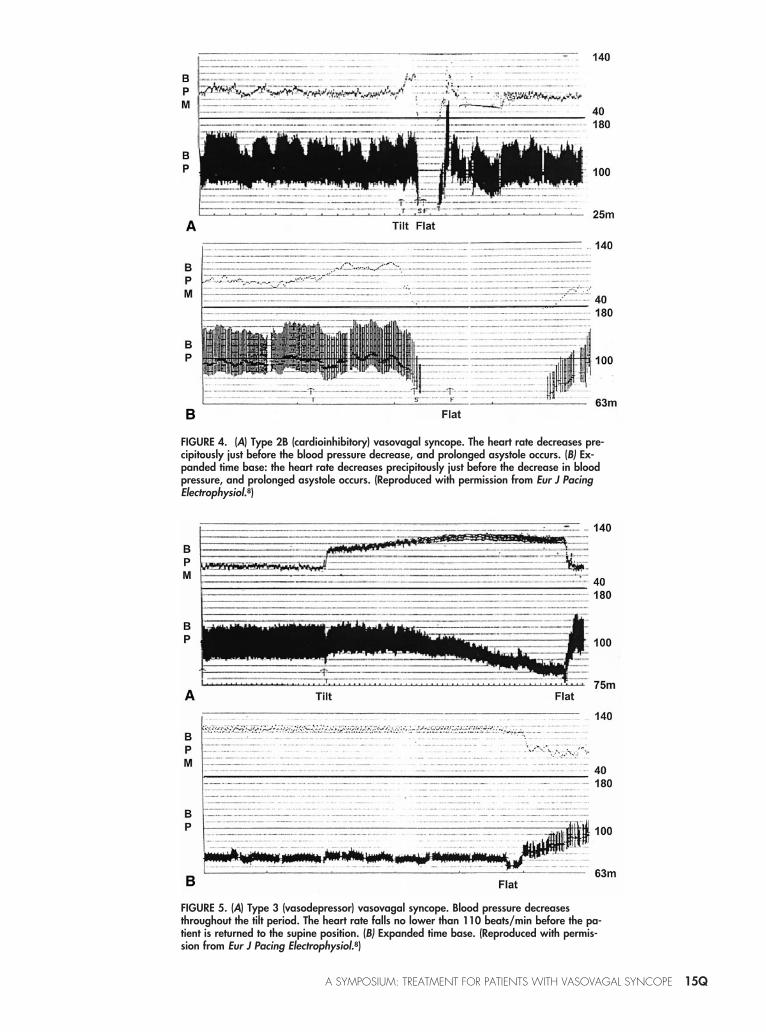
FIGURE 4. (A) Type 2B (cardioinhibitory) vasovagal syncope. The heart rate decreases pre-cipitously just before the blood pressure decrease, and prolonged asystole occurs. (B) Ex-panded time base: the heart rate decreases precipitously just before the decrease in bloodpressure, and prolonged asystole occurs. (Reproduced with permission from Eur J PacingElectrophysiol.8)
FIGURE 5. (A) Type 3 (vasodepressor) vasovagal syncope. Blood pressure decreasesthroughout the tilt period. The heart rate falls no lower than 110 beats/min before the pa-tient is returned to the supine position. (B) Expanded time base. (Reproduced with permis-sion from Eur J Pacing Electrophysiol.8)
A SYMPOSIUM: TREATMENT FOR PATIENTS WITH VASOVAGAL SYNCOPE 15Q
investigators 7 years ago.8 Here, we expand the pre-vious classification to include 2 important responses totilt-table testing that should be distinguished from thevasovagal syncope responses: a dysautonomic re-sponse and POTS. These disorders likely representresponses to upright posture that have different patho-physiologies from vasovagal syncope.
Classifying the hemodynamic patterns of syncopalcollapse requires the monitoring of arterial blood pres-sure on a beat-to-beat basis. It would be impossible todetermine the relation between the decrease in bloodpressure and changes in heart rate using a manual cuffmeasurement at 2-minute intervals. Beat-to-beat bloodpressure measurements allow us to evaluate the evo-lution of the pattern of collapse. In addition, we haveobserved that in many cases, the blood pressure de-creases before a decrease in heart rate; if a test wereterminated when the blood pressure began to decrease,a subsequent decrease in heart rate may be missed. Inour experience, our staff is comfortable continuing a
study until the patient is near-syncopal provided theyare able to monitor arterial blood pressure continu-ously.
Pathophysiology of orthostatic intolerance: The dif-ferential diagnosis and the differences in the patho-physiology of orthostatic intolerance are discussed inthe literature17–19 and elsewhere in this supplement.Disorders in blood pressure regulation during uprightposture are generally referred to as disorders of ortho-static intolerance. Based on the cardiovascular andautonomic responses to upright posture, they can bedivided into 2 general categories. In one, the auto-nomic nervous system appears to have a hypersensi-tive response to orthostatic stress that results in syn-cope mediated by the Bezold–Jarisch reflex. In thesepatients, the initial cardiovascular response to uprightposture is relatively normal and syncope occurs afteran abrupt decrease in blood pressure accompanied bya decrease in heart rate after a prolonged period ofhead-up tilt (often;20 minutes). Other reflex re-
FIGURE 6. Dysautonomic response to head-up tilt. The patient is hypertensive (180/80 mmHg) while supine. Over the course of a 25-minute head-up tilt, blood pressure gradually andprogressively decreases to 80 mm Hg and is accompanied by a modest increase in heartrate (from 70 to 80 beats/min). From minutes 25 to 42, blood pressure fluctuates between80 and 100 mm Hg. After 42 minutes, blood pressure decreases to 60 mm Hg and the pa-tient becomes near-syncopal. In contrast to vasovagal syncope, the pathophysiology of thisresponse represents a failure of the cardiovascular system to adapt to the hemodynamicstress of upright posture.
16Q THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 84 (8A) OCTOBER 21, 1999
sponses suggest that a hypersensitive autonomic re-sponse can result from different afferent input, such aswith micturition or defecation syncope. These arecategorized as reflex syncope.
Another type of orthostatic intolerance occurswhen the autonomic nervous system appears to befailing. Patients fail to compensate for the decrease invenous return that occurs acutely with upright posture;when this failure becomes severe, frank orthostatichypotension occurs. However, even in the absence offrank orthostatic hypotension, patients with a failingautonomic nervous system may demonstrate a pro-gressive type of orthostatic hypotension: As bloodpools in the lower extremities with prolonged periodsof upright posture, blood pressure continues to de-crease. This has been described as a dysautonomicresponse to upright posture.
The other form of autonomic failure, POTS,20,21 isdefined by an excessive increase in heart rate in thefirst few minutes of upright posture. Blood pressure
often decreases during head-up tilt, although not allpatients become frankly hypotensive. Abnormalitiesin cerebral autoregulation have been described in thispopulation, which might account for some of the re-ported symptoms occurring in the absence of systemichypotension. As a heterogenous disorder, it has beensuggested that at least two types of POTS exist—oneprobably representsb-receptor hypersensitivity andthe other seems to represent a failing autonomic ner-vous system similar to the dysautonomic response.Although some patients with POTS eventually de-velop syncope associated with frank hypotension, theyshould be distinguished from patients with vasovagalsyncope because of their excessive tachycardia re-sponse to upright posture—with the exception of theyoung females mentioned earlier.
Hemodynamic profiles of syncopal collapse: In clas-sifying the hemodynamic profile of syncopal collapse,the most important distinction is whether the patientexhibits an abrupt decrease in blood pressure consis-
FIGURE 7. Postural orthostatic tachycardia syndrome. Immediately upon being tilted headup, heart rate increases from 76 to 120 beats/min and continues to increase to 140 beats/min. Blood pressure initially increases after tilt and then gradually decreases, fluctuating be-tween 90 and 100 mm Hg (note the narrowing of pulse pressure). Blood pressure and heartrate abruptly decrease in a mixed (Type 1) vasovagal collapse pattern. This illustrates theearly and sustained increase in heart rate in patients with postural tachycardia syndrome(POTS). Some patients will develop a subsequent vasovagal response as is illustrated here.The pattern was previously classified as excessive heart-rate response.
A SYMPOSIUM: TREATMENT FOR PATIENTS WITH VASOVAGAL SYNCOPE 17Q
tent with vasovagal syncope or a more gradual andprogressive decrease consistent with a dysautonomicresponse. This distinction may have an important ef-fect on the choice of therapy.
Several therapies are available for patients with anabrupt decrease in blood pressure suggesting aBezold–Jarisch reflex. Beta blockers, which preventthe afferent triggering of the reflex, antagonize thehigh levels of epinephrine in susceptible subjects andprevent activation of the mechanoreceptor. Alterna-tively, volume expansion by fludrocortisone or in-crease in venous tone and limitation of venous poolingby midodrine may reduce the relative central hypovo-lemia that is associated with mechanoreceptor activa-tion.
Therapy for patients with a dysautonomic responseshould support a failing autonomic nervous system.For these patients,b blockers may be detrimental andvolume expansion or midodrine are more likely to bebeneficial. Therapeutic options based on these patternsof syncopal collapse are described in more detail inthe panel consensus “Putting it Together: A NewTreatment Algorithm for Vasovagal Syncope and Re-lated Disorders” in this supplement.22
Within the realm of vasovagal syncope, we de-scribe 3 syncopal collapse patterns: (1) mixed (type1), (2) cardioinhibitory (types 2A and 2B), and (3)pure vasodepressor (type 3). In our experience, type 1and type 2A are most prevalent, although type 2B iscommon in young patients. To date, the only studyusing this classification showed that etilefrine had nobenefit over placebo in preventing spontaneous epi-sodes of vasovagal syncope.23 We are hopeful thatfuture randomized clinical trials will be able to iden-tify subgroups of patients based on the expandedclassification and that, eventually, we will be able todetermine if a patient with a specific collapse patternis more likely to benefit from a specific therapy.
At present, we tend to useb blockers, volume
expansion (salt and fludrocortisone), and midodrine,which can be effective individual treatments for pa-tients with vasovagal syncope. Occasionally, theagents are used in combination. Although pacing ther-apy is attractive for patients with a cardioinhibitorycollapse pattern (types 2A and 2B), most of thesepatients also respond tob blockers, fludrocortisone,and midodrine. Patients with the most dramatic asys-tolic pauses (type 2B) are often younger and we hes-itate to implant permanent pacemakers unless phar-macologic treatment fails. It is likely that patients witha mixed vasovagal response (type 1) will benefit frompacing using specialized pacing algorithms (e.g., ratedrop, rate smoothing, or rate hysteresis), although thebradycardia is modest. A recently published random-ized control trial of pacing in vasovagal syncope dem-onstrated that pacing is effective, and this trial in-cluded patients with types 1, 2A, and 2B patterns ofcollapse.24 At this point, however, it is not knownwhether specific hemodynamic patterns of collapsepredict pacemaker efficacy.
Limitations: The utility of hemodynamic patterns ofcollapse to guide therapy would be severely limited ifthe pattern could not be reproduced. Although thereproducibility of tilt-table testing is not flawless, itdoes appear that the hemodynamic patterns of collapseare reproducible.25 We have limited our discussion ofthe hemodynamic pattern of syncopal collapse to pro-longed drug-free tilt and have not commented onpatterns of collapse elicited by provocative agentssuch as nitroglycerin and isoproterenol. Our first re-ports of the differences experienced with nitroglycerinversus drug-free tilt are in press.16 We feel stronglythat the most useful information is obtained duringprolonged head-up tilt in the drug-free state. We alsobelieve there is utility in performing tilt-table testswith a drug challenge to establish the diagnosis ofvasovagal syncope, and more experience is needed inobserving collapse patterns after provocative testing.
FIGURE 8. Chronotropic incompetence. Patients demonstrate essentially no increase in heart rate during head-up tilt (<5 beats/minfrom the tilt rate) but have an abrupt decrease in blood pressure consistent with vasovagal syncope.
18Q THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 84 (8A) OCTOBER 21, 1999

Testing with a provocative agent should follow anegative drug-free tilt.
1. Kenny RA, Bayliss J, Ingram A, Sutton R. Head-up tilt: a useful test forinvestigating unexplained syncope.Lancet1986;1:1352–1355.2. Benditt DG, Ferguson DW, Grubb BP, Kapoor WN, Kugler J, Lerman BB,Maloney JD, Raviele A, Ross B, Sutton R, Wolk MJ, Wood DL. Tilt table testingfor assessing syncope: American College of Cardiology.J Am Coll Cardiol1996;28:263–275.3. Fitzpatrick A, Sutton R. Tilting towards a diagnosis in recurrent unexplainedsyncope.Lancet1989;i:658–660.4. Abi-Samra F, Maloney JD, Fouad-Tarazi FM, Castle LW. The usefulness ofhead-up tilt testing and hemodynamic investigations in the workup of syncope ofunknown origin.PACE Pacing Clin Electrophysiol1988;11:1202–1214.5. Benditt DG, Remole S, Bailin S, Dunnigan A, Asso A, Milstein S. Tilt tabletesting for evaluation of neurally-mediated (cardioneurogenic) syncope: rationaleand proposed protocols.PACE Pacing Clin Electrophysiol1991;14:1528–1537.6. Fitzpatrick A, Williams T, Ahmed R. Echocardiographic and endocrinechanges during vasovagal syncope induced by prolonged head-up tilt.Eur JPacing Electrophysiol1992;2:121–128.7. Klingenheben T, Kalusche D, Li YG, Schopperl M, Hohnloser SH. Changes inplasma epinephrine concentration and in heart rate during head-up tilt testing inpatients with neurocardiogenic syncope: correlation with successful therapy withbeta-receptor antagonists.J Cardiovasc Electrophysiol1996;7:802–808.8. Sutton R, Petersen M, Brignole M, Raviele A, Menozzi C, Giani P. Proposedclassification for tilt induced vasovagal syncope.Eur J Pacing Electrophysiol1992;3:180–183.9. Almquist A, Goldenberg IF, Milstein S, Chen MY, Chen X, Hansen R,Gornick CC, Benditt DG. Provocation of bradycardia and hypotension by iso-proterenol and upright posture in patients with unexplained syncope.N EnglJ Med1989;320:346–351.10. Raviele A, Menozzi C, Brignole M, Gasparini G, Alboni P, Musso G, LolliG, Oddone D, Dinelli M, Mureddu R. Value of head-up tilt testing potentiatedwith sublingual nitroglycerin to assess the origin of unexplained syncope.Am JCardiol 1995;76:267–272.11. Petersen ME, Williams TR, Sutton R. A comparison of non-invasive contin-uous finger blood pressure measurement (Finapres) with intra-arterial pressureduring prolonged head-up tilt.Eur Heart J1995;16:1641–1654.12. Natale A, Akhtar M, Jazayeri MR, Dhala A, Blanck Z, Deshpande S, Krebs
A, Sra JS. Provocation of hypotension during head-up tilt testing in subjects withno history of syncope or presyncope.Circulation 1995;92:54–58.13. Fitzpatrick AP, Theodorakis G, Vardas P, Sutton R. Methodology of head-uptilt testing in patients with unexplained syncope.J Am Coll Cardiol1991;17:125–130.14. Bloomfield D, Maurer M, Bigger JTJ. Effects of age on outcome of tilt-tabletesting.Am J Cardiol1999;83:1055–1058.15. Petersen ME, Sutton R. The normal response to prolonged passive head-uptilt testing.Heart. In press.16. Kurbaan AS, Franze´n AC, Bowker TJ, Williams TR, Kaddoura S, PetersenME, Sutton R. Usefulness of tilt test-induced patterns of heart rate and bloodpressure using a two stage protocol with glyceryl trinitrate provocation in patientswith syncope of unknown origin.Am J Cardiol. 1999;84:665–670.17. Grubb BP, Karas B. Clinical disorders of the autonomic nervous systemassociated with orthostatic intolerance: an overview of classification, clinicalevaluation, and management.PACE Pacing Clin Electrophysiol1999;22:798–810.18. Benditt DG. Neurally mediated syncopal syndromes: pathophysiologicalconcepts and clinical evaluation.PACE Pacing Clin Electrophysiol1997;20:572–584.19. Sutton R, Petersen ME. The economics of treating vasovagal syncope.PACEPacing Clin Electrophysiol1997;20:849–850.20. Low PA, Opfer-Gehrking TL, Textor SC, Benarroch EE, Shen WK, Schon-dorf R, Suarez GA, Rummans TA. Postural tachycardia syndrome (POTS).Neurology1995;45(4, suppl 5):S19–S25.21. Grubb BP, Kosinski DJ, Boehm K, Kip K. The postural orthostatic tachy-cardia syndrome: a neurocardiogenic variant identified during head-up tilt tabletesting.PACE Pacing Clin Electrophysiol1997;20:2205–2212.22. Bloomfield D, Sheldon R, Grubb BP, Calkins H, Sutton R. Putting it together:a new treatment algorithm for vasovagal syncope and related disorders.Am JCardiol 1999;84:33Q–39Q.23. Raviele A, Brignole M, Sutton R, Alboni P, Giani P, Menozzi C, Moya A, forthe Vasovagal Syncope International Study Investigators. Effect of etilefrine inpreventing syncopal recurrence in patients with vasovagal syncope: a double-blind, randomized, placebo-controlled trial.Circulation 1999;99:1452–1457.24. Connolly SJ, Sheldon R, Roberts RS, Gent M. The North American Vaso-vagal Pacemaker Study (VPS): a randomized trial of permanent cardiac pacingfor the prevention of vasovagal syncope.J Am Coll Cardiol1999;33:16–20.25. Petersen ME, Chamberlain-Webber R, Fitzpatrick AP, Sutton R. Reproduc-ibility of the Westminster tilt protocol. (Abstr.)J Am Coll Cardiol1992;19:340.
A SYMPOSIUM: TREATMENT FOR PATIENTS WITH VASOVAGAL SYNCOPE 19Q