tilt table
TRANSCRIPT

TILT TABLE
Lincoln Thio
MOT 1st Year
SVNIRTAR
INTRODUCTION
A padded table with a top capable of being rotated on its transverse axis so that a patient lying on it can be brought into the erect position.
Initially used as a diagnostic tools ‘Tilt Table Test’ for assessment of syncope.
However with repeated use, improvement in upright tolerance was observed. So serial tilt training has came to used as a therapy for the treatment of syncope.

CONTD…
Serves as an integral part of therapy for
physiological accommodation to an
upright position
It also provides an opportunity for early
weight bearing in lower limbs.
IMI No. 1330

PARTS
The padded table top is 24’’ wide , 80’’
long, 34” high and is fitted on heavy
duty 47’’ square steel tube legs.
Mounted on 4 lockable 4’’ diameter
wheels for mobility.
Two wide straps to hold the patient.
(108”)
Crank with handle
180 degree Protractor

CONT..
Footrest ( 17/14’’)
Removable grip bar/Hand rill
(34/28’’)
Adjustable grab bar holder
Side bar with 6 holes

TYPES
Manual Tilt Table
Electric Tilt Table
Pediatric Tilt Table
W/H accessible Hi-lo Tilt
Table
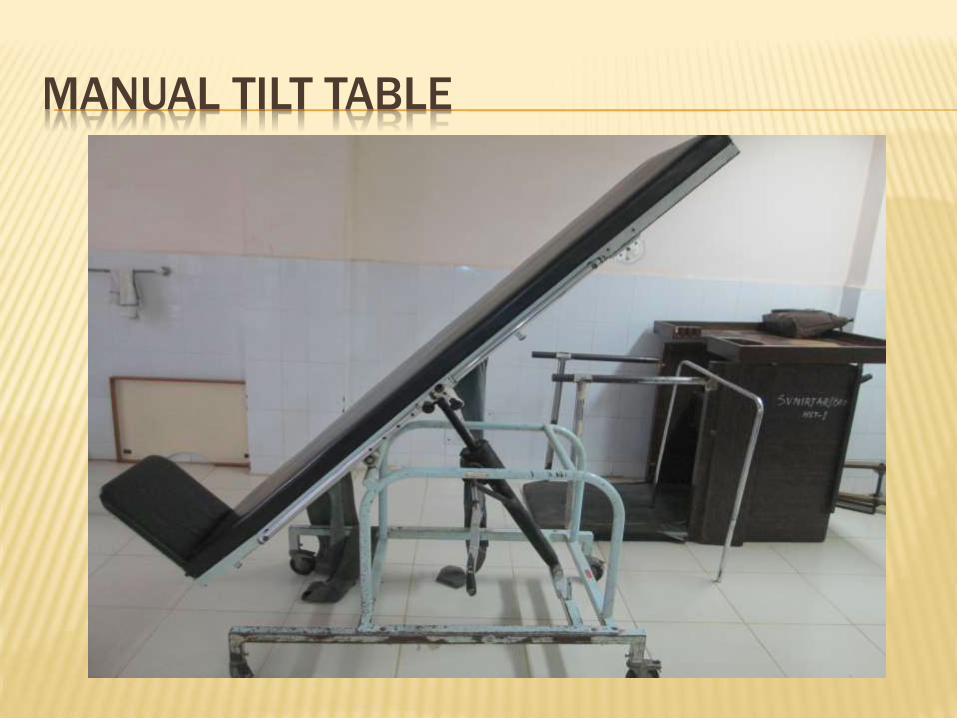
MANUAL TILT TABLE

ELECTRIC TILT TABLE

PEDIATRIC TILT TABLE

WHEEL CHAIR ACCESSIBLE HI- LO TILT TABLE
COMMON SETTINGS
Home
Early intervention centers
Hospitals
Therapy centers
rehabilitation centers
extended centers

PROCEDURE
Before transferring to Tilt Table,
measure the baseline resting BP
and Pulse rate.
Transfer the patient to the Tilt Table.
The patient lies supine on top of
the table with foot flat on the foot
board.

PROCEDURE
Therapist secures the safety straps
over the knee, pelvic and chest.
Secure abdominal binder and
antiembolism stocking/elastic
stocking.
Then gradually elevate the Tilt table to
upright position.


RAISING AND LOWERING THE PATIENT
Slowly elevate to 20*
Take BP/HR
Elevate the pt. To 45*- repeat vitals.
Elevate the pt. To 85*-repeat vitals
Check the BP & HR of the Pt. every 3-5 minutes
Gradually to return to horizontal position and
check vitals signs
Transfer the Pt back.

SPECIAL CONSIDERATION
Let the Pt. determined the tilt angle and
duration of elevation
Avoid prolong upright position because it may
lead to venous stasis
Never leave Pt. unattended because marked
physiological changes such as hypotension
/severe headache etc may occur suddenly
Chest strap should be secured properly and
make sure that it is not too tight so that patient
could breathe comfortably.

CONTD…
Be alert for signs and symptoms of insufficient cerebral circulation like- dizziness, nausea, pallor, diaphoresis, tachycardia, sensation of fainting and edema in L/E .
If the above signs develop, immediately return to the horizontal position.
While transfer from W/C to tilt table and vice versa therapist must take care of his/her proper posture.
If person is elevated beyond 70*, chest strap should be applied.
DURATION FOR TRAINING
Perform once/twice a day regime for up to
10-30 min each session.
One level below where the fainting starts.
Up to 4 weeks, then try a higher level
PHYSIOLOGICAL EFFECTS
Increased circulation in upright position.
Increased urinary drainage
Musculoskeletal: muscle tone increases in antigravity muscle, Increased bones density.
Neurologic: Sensory receptors of the soles of the feet, Joint proprioceptors, muscle spindles, semicircular canals get stimulated.
Respiratory: increased ventilation, gravity drains bronchioles.
Tilt at 60 degree onwards can gives Pt. the physiological effect and sensation of upright standing.

INDICATIONS
Prolonged recumbence.
Generalized weakness
Disturbance in balance , proprioception,
kinesthesia, lower limb circulation
Orthostatic hypotension/ postural hypotension
drop of 10-20mmhg in response to upright
position
CONT…
HEAD INJURY
SCI
CP
SPINA BIFIDA
MUSCULAR DYSTROPHY
STROKE
POST POLIO SYNDROME

THERAPEUTIC BENEFITS
Reintroduce patient to vertical position.
Facilitate early weight bearing
Promote and maintain bone density in L/E
Prevent muscle contracture.
Improve lower limb strength .
Increase arousal.
Cardiovascular conditioning.
Allow to become acclimated to an upright position without rapid changes in BP.
Decrease spasticity

CONT…
Prevention of osteoporosis, hypercalciurea,
pathological fracture.
Postural improvement
Enhance bowel and bladder function
Provide early weight bearing experiences for
patients too weak to stand on their own.
Decreases prolonged bed rest complications.
Improve psychological outlook and also
motivates
Pt. to participate in ambulation program.

CONTRAINDICATIONS
Bone tumors
Fresh fracture
Fresh implant
Neoplastic disease of spine
Pregnancy
Acute inflammatory condition in pelvis or L/L
Patient refusal
Acute spinal or pelvic fractures
Acute cardiac infarctions.

ADAPTATION
Wooden box can be placed under weight
bearing leg if one of the Pt. leg is non weight
bearing
Adjustable and removable table/lapboard can
be attached to Tilt Table for writing, reading,
food, communication devises etc
Adjustable footboard

DIFFERENCE FROM STANDING FRAME
Same goal with same benefits in a more
functional position
Standing Frame is more challenging and
allows more active participation from the
individuals using it
Standing Frame an be used as a progressing
from Tilt Table
DISADVANTAGE
Passive
Cumbersome
Fainting
Edema of L/L
Time consuming

REFERENCES
Abe, H., K. Kohshi, et al. (2003). "Effects of orthostatic self-training on head-up tilt testing and balance in paraplegic patients . J CardiovascPharmacol 41 Suppl 1: S73-6
Standing with assisstance of a tilt table in ICU A survey of Australian Physiotherapy Practise2004 50(1)
Tolerance of a Standing Tilt Table Protocol by Patients an Inpatient Stroke Unit Setting: A Pilot Study
Equipment Designed for Occupational Therapy. Florence M. Stattel, MA, OTR
Tilt table protocol by Mary Egbert.

CONT…
Tilt Training: A new challenge in treating of
neurally mediated syncope- Tony Reybrouk,
Hugo Ector
Benefits of prolonged standing for SCI by
janice j eng stephen m levins
Early mobilization emphasizes upright
positioning and weight bearing By Darin
Trees, DPT, PT, CWS
