increased breath markers of oxidative stress in normal pregnancy and in preeclampsia
TRANSCRIPT
American Journal of Obstetrics and Gynecology (2004) 190, 1184e90
www.elsevier.com/locate/ajog
Increased breath markers of oxidative stress in normalpregnancy and in preeclampsia
Michael Moretti, MD,b,c Michael Phillips, MD, FACP,a,b,* Ahmed Abouzeid, MD,c
Renee N. Cataneo, MA,a Joel Greenberg, BSa
Menssana Research, Inc, Fort Lee, New Jersey,a Department of Medicine, New York Medical College, Valhalla, NewYork,b and Department of Obstetrics and Gynecology, Sisters of Charity Health Care System, St Vincent’s Campus,Staten Island, New Yorkc
––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––Objectives: The purpose of this study was to compare the intensity of oxidative stress in normal
pregnancy, preeclampsia, and nonpregnant women using a breath test.Study design: We studied primiparous women in third trimester pregnancy (38 uncomplicated, 26with preeclampsia) and 60 nonpregnant control subjects. Volatile organic compounds (VOCs) in
alveolar breath were analyzed by gas chromatography/mass spectroscopy to construct the breathmethylated alkane contour (BMAC), a 3-dimensional display of abundance of C4-C20 alkanesand monomethylated alkanes.
Results: The mean volume under curve (VUC) of the BMAC was significantly higher in pre-eclampsia patients than in normal pregnant women (P!.003) and nonpregnant control subjects(P!.005). A predictive model employing 5 VOCs distinguished preeclampsia from uncompli-cated pregnancy (sensitivity=92.3%, specificity=89.7%; cross-validated sensitivity=88.5%,
specificity=79.3%).Conclusion: A breath test significantly demonstrated greater oxidative stress in women with pre-eclampsia than in uncomplicated pregnancy and nonpregnant control subjects. The breath test
accurately identified women with established preeclampsia, but further studies are required to de-termine if this test can predict the onset of disease.� 2004 Elsevier Inc. All rights reserved.
KEY WORDSPreeclampsia
Oxidative stressBreathAlkanesMethylated alkanes
–––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––
Preeclampsia is a complication of pregnancy charac-terized by hypertension, edema, and proteinuria, and nosingle test or combination of tests has yet been shown topredict its onset with accuracy.1 A number of risk fac-tors for preeclampsia have been identified, including in-
Supported by a grant from the Dishe Fund for research.
* Reprint requests: Michael Phillips MD, FACP, Menssana
Research, Inc, 1 Horizon Road, Suite 1415, Fort Lee, NJ 07024.
E-mail: [email protected]
0002-9378/$ - see front matter � 2004 Elsevier Inc. All rights reserved.
doi:10.1016/j.ajog.2003.11.008
creased plasma cellular fibronectin concentrations,2
history of preeclampsia, elevated screening mean arterialpressure, and low unconjugated estriol concentration.3
However, in clinical practice, preeclampsia is definedby its clinical manifestations, and is often discovered latein its course. An objective screening test to predict theonset of preeclampsia would be clinically valuable in or-der to identify women who require closer clinical moni-toring during pregnancy, and also to aid in evaluatingnew preventive therapies before the onset of clinicalsymptoms or signs.4

Moretti et al 1185
Figure 1 Plan of data analysis. Breath tests for the BMAC were performed in three groups of women: healthy control subjects
(nonpregnant females), primiparous women in their third trimester of pregnancy, and primiparous women with preeclampsia. TheBMAC is affected by age, so that statistical comparisons of the BMAC between groups were performed in age-matched subgroupsthat had been selected as shown in this figure.
Because increased oxidative stress has been impli-cated in the etiology of preeclampsia,5 a marker of ox-idative stress could potentially provide such a screeningtest. Oxidative stress originates in the mitochondria asa byproduct of oxidative metabolism. When oxygenaccepts electrons, the main products are water and en-ergy, but a number of other products known collec-tively as reactive oxygen species (ROS) are alsoformed. ROS are highly toxic; they leak into the cyto-plasm and inflict a constant barrage of oxidative dam-age to DNA, proteins, lipids, and other biologicallyimportant molecules.6 This process generates a varietyof metabolic products, including oxidized thiols,7 lipidperoxides,8 and isoprostane,9 which have been em-ployed as biomarkers of increased oxidative stress inpreeclampsia.
Oxidative stress can also be estimated with breathtesting because lipid peroxidation of polyunsaturatedfatty acids in membranes generates alkanes such as eth-ane and pentane, which are excreted in the breath as vol-atile organic compounds (VOCs).10 Breath tests forthese VOCs have demonstrated increased oxidativestress in breast cancer,11 rheumatoid arthritis,12 hearttransplant rejection,13 acute myocardial infarction,14
schizophrenia,15 and bronchial asthma.16
However, a biomarker of oxidative stress such asbreath pentane is an inherently nonspecific marker ofdisease because it is increased in a wide variety of con-ditions. We have reported a new index of oxidativestress, the breath methylated alkane contour (BMAC),comprising a 3-dimensional surface plot of the abun-dance in breath of C4 to C20 alkanes and their mono-methylated derivatives.17 The BMAC incorporates 107different VOCs, and their pattern is altered in a distinc-tive fashion in different conditions, including lung can-cer,18 breast cancer,19 unstable angina,20 oxygenbreathing,21 and aging.22 In this study, we employedthe BMAC to compare the intensity of oxidative stress
in 3 groups of women: normal third trimester preg-nancy, women with preeclampsia, and nonpregnantcontrol subjects.
Material and methods
Human subjects
The design of the study is shown in Figure 1. The re-search was approved by the institutional review boardof the Sisters of Charity Health Care System, St Vin-cent’s Campus, Staten Island, New York, and all womengave their signed informed consent to participate. Allsubjects in this study were nonsmokers. This wasa cross-sectional study of 3 groups of women:
Uncomplicated pregnancy (n = 38)All subjects were singleton primigravidas selected fromthe general obstetric population with gestational ageR26 weeks, no chronic medical disorders, and not in la-bor. They were normotensive and nonobese. Patientswith a history of renal disease, diabetes, or significantperinatal complications were excluded.
Preeclampsia (n = 26)All subjects were primigravida with gestational ageO26weeks and no chronic medical disorders (apart from twosubjects with gestational diabetes mellitus) and not in la-bor. Preeclampsia was defined as blood pressureO140/90 mm Hg on 2 separate occasions 4 to 6 hours apartwith concordant proteinuria. Proteinuria was definedas a urinary dipstick valueO1C (30mg/dL), or a 24-hour urine collection with a protein excretion ofO300mg. Patients taking aspirin, antihypertensive medica-tion, or antioxidants (other than traditional prenatal vi-tamins) were excluded, as were those with obesity,history of chronic hypertension, insulin-dependent dia-betes, or renal disease. Only those patients with
1186 Moretti et al
proteinuric hypertension classified as mild preeclampsiaby the American College of Obstetrics and GynecologyCriteria were included.23
Healthy controls (n = 60)The healthy nonpregnant control subjects were recruitedfrom employees of the medical center. All were nonpreg-nant females aged 17 to 40 years, with no chronic med-ical disorders. None of the women had delivered a babyor conceived during the year before the breath test. Clin-ically obese women, and those women taking hormonalcontraception were excluded.
Location and time of breath testsBreath collections were performed in the labor and de-livery unit by a research assistant (AA). In the pre-eclampsia group, breath samples were collected whenthe patient presented for evaluation, and before initia-tion of MgSo4 or antihypertensives. Samples were col-lected from the other patients between 8 a.m. and 4p.m. daily, at least 2 hours after meals.
Breath collection and assayThis method has been previously described.24,25 In sum-mary, a portable breath collection apparatus was em-ployed to capture the VOCs in 1.0 l breath and in 1.0 lroom air onto separate sorbent traps. Each subject worea nose clip while breathing in and out of the disposablemouthpiece of the apparatus for 2.0 minutes. Breathsamples could be collected without discomfort because
Table I Characteristics of the normal pregnant women andpatients with preeclampsia
Characteristics
Normalpregnancy(n = 38)
Preeclampsia(n = 26)
Maternal age (y) 24.8 (4.7) 28.1 (6.2)Gestational age (wks) 33.5 (4.0) 35.5 (4.67)Blood pressure
(mm Hg)Systolic 110 (7) 160.7 (19.4)Diastolic 63 (8) 94.6 (5.3)
Maternal weight (lb) 158 (29.3) 178 (42.5)Proteinuria (mg/24h) d 2246 (566)Urine dipstickO1C (No.) d 26Race (No.)White 22 17Hispanic 3 3African American 13 6Asian 0 0
Gestational age atdelivery (wks)
39.2 (1.2) 36.3 (4.67)
Birth weight (g) 3407 (220) 2361.3 (1085)NICU admissions 1 75 min Apgar !7 0 4
Values are mean and (SD)
NICU, Neonatal intensive care unit.
light flap valves in the mouthpiece presented low resis-tance to respiration. VOCs captured in sorbent trapswere analyzed by automated thermal desorption, gaschromatography, and mass spectroscopy.
Derivation of BMACsThis method has been previously described.17 Data fromthe assays of breath and air VOCs were employed togenerate 3-dimensional surface plots of C4 to C20 n-al-kanes and their monomethylated derivatives. For eachbreath VOC, Vb denotes the area under the curve asso-ciated with the chromatogram peak, and Ib denotes theanalogous area associated with the internal standardused to normalize the data (0.25 mL 2 ppm 1-bromo-4-fluoro-benzene; Supelco, Bellefonte, Pa). Va and Ia de-note corresponding areas derived from the associatedsample of room air. The alveolar gradient25 of eachVOC was then determined as:
alveolar gradient ¼ Vb=Ib � Va=Ia:
The mean alveolar gradients of these VOCs werecomputed for each group of subjects and displayed insurface plots showing the carbon chain length on thex-axis, the methylation site on the z-axis, and the meanalveolar gradient on the y-axis.
Analysis of dataThe volume under curve (VUC) of each BMAC was de-termined, and VUC values in the 3 groups were com-pared. Forward step-wise discriminant analysis26 wasused to identify the combination of VOCs that providedthe best discrimination between women with preeclamp-
Table II Laboratory investigations in patients with pre-eclampsia
Serum creatinine (mg/dL) 0.7 (0.9)Uric acid (mg/dL) 5.7 (5.8)Platelet count (thous/mcL) 158,000 (27)AST (u/L) 35.7 (26)ALT (u/L) 34.9 (19)LDH (uU/L) 197.7 (48.3)Total bilirubin (mg/dL) 0.5 (0.14)Direct bilirubin (mg/dL) 0.2 (0.35)Fibrinogen (mg/dL) 413.8 (71.8)Prothrombin time (ratio) 12.3 (1.9)Partial thromboplastintime (sec)
27.8 (2.3)
WBC 10.86 (2.74)Hemoglobin (g/dL) 12.08 (1.02)Hematocrit (%) 34.8 (3.2)
Values are mean and (SD)
AST, Aspartate amino transferase; ALT, alanine aminotransferase; LDH,
lactate dehydrogenase; WBC, White blood cell count.
Moretti et al 1187
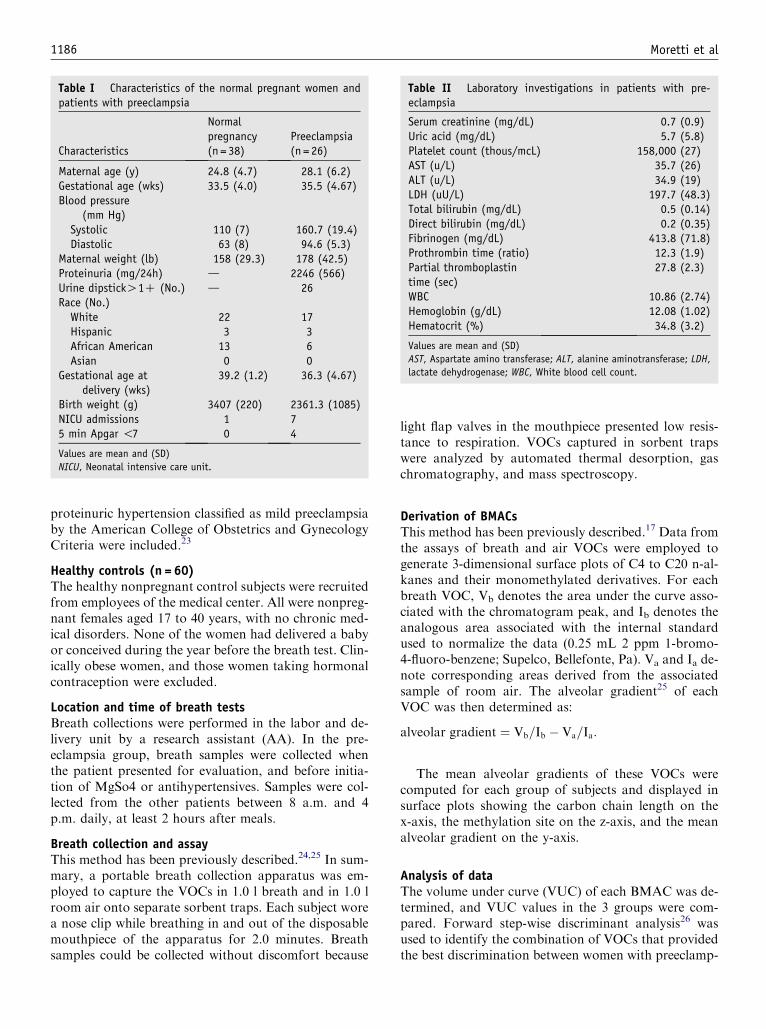
Figure 2 BMACs in 3 groups of women. The BMAC is a display of the abundance (alveolar gradients) of C4 to C20 alkanes and
monomethylated alkanes in breath. The alveolar gradient (y-axis) is the concentration in breath minus the concentration in roomair, and varies with the rate of synthesis minus the rate of clearance. The x-axis displays the chain length of straight chain n-alkanesmethylated at one site, and the z-axis displays the methylation site. This figure includes n-alkanes, showing them as methylated at
C1. For example, an alkane with carbon chain length=4 (butane) becomes the C5 alkane pentane when methylated at C1. BMACsare shown for the healthy control subjects (nonpregnant females), primiparous women in their third trimester of pregnancy, andprimiparous women with preeclampsia. The mean value for each of the age-matched subgroups selected in Figure 1 is shown. It is
apparent that peaks are predominantly negative in the nonpregnant females and predominantly positive in preeclampsia group, andintermediate in the normal pregnant women.
sia and primiparous women in the third trimester of un-complicated pregnancy, in order to construct a predictivemodel. The accuracy of this predictive model was firsttested by cross-validation using a leave-one-out tech-nique, in which each subject was classified using anequation derived from all other subjects.27 A receiveroperating characteristic (ROC) curve28 was constructedto display the sensitivity and specificity of the breathtest.
Results
Human subjects
Table I shows demographic and clinical data for the pre-eclampsia and normal pregnancy groups. No significantperinatal complications developed in the normal preg-nancy group. Table II shows the laboratory data inthe preeclampsia group. No cases of HELLP Syndrome,eclampsia, or abruption developed. There were no ma-ternal or neonatal deaths. All patients in the preeclamp-sia group received MgSo4 before delivery and for 24hours postpartum.
Breath test
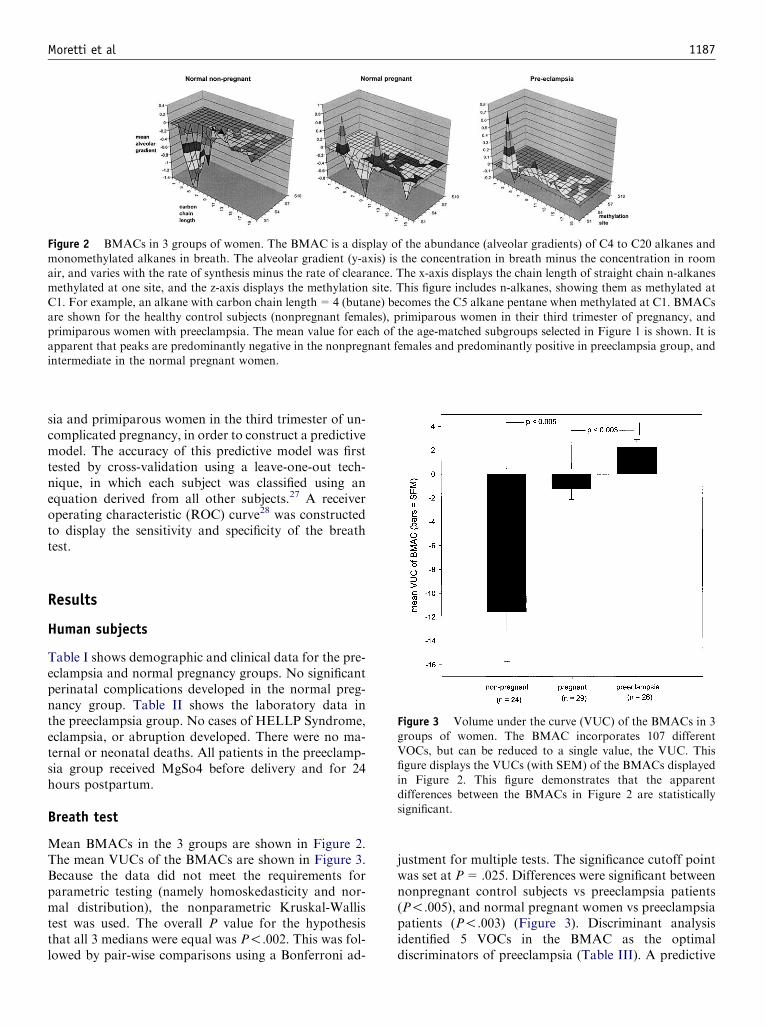
Mean BMACs in the 3 groups are shown in Figure 2.The mean VUCs of the BMACs are shown in Figure 3.Because the data did not meet the requirements forparametric testing (namely homoskedasticity and nor-mal distribution), the nonparametric Kruskal-Wallistest was used. The overall P value for the hypothesisthat all 3 medians were equal was P!.002. This was fol-lowed by pair-wise comparisons using a Bonferroni ad-
justment for multiple tests. The significance cutoff pointwas set at P=.025. Differences were significant betweennonpregnant control subjects vs preeclampsia patients(P!.005), and normal pregnant women vs preeclampsiapatients (P!.003) (Figure 3). Discriminant analysisidentified 5 VOCs in the BMAC as the optimaldiscriminators of preeclampsia (Table III). A predictive
Figure 3 Volume under the curve (VUC) of the BMACs in 3
groups of women. The BMAC incorporates 107 differentVOCs, but can be reduced to a single value, the VUC. Thisfigure displays the VUCs (with SEM) of the BMACs displayed
in Figure 2. This figure demonstrates that the apparentdifferences between the BMACs in Figure 2 are statisticallysignificant.

1188 Moretti et al
model employing these VOCs identified women withpreeclampsia with sensitivity=92.3% and specific-ity=89.7% (cross-validated sensitivity=88.5% andspecificity=79.3%). The ROC curve is shown inFigure 4.
Comment
The abundance of breath markers of oxidative stresswas significantly higher in preeclampsia than in thethird trimester of uncomplicated pregnancy or in non-pregnant control subjects. A predictive model employ-ing 5 VOCs in the BMAC was sensitive and specificfor preeclampsia. Although the pathogenesis of pre-eclampsia remains poorly understood, these findingsare consistent with previous reports that oxidative stressplays an important role.29-32 Various mechanisms forthe increase in oxidative stress have been proposed, in-cluding the promotion of free radical reactions by‘‘cross-talk’’ between the diseased placenta and mater-nal dyslipidemia.5
Figure 4 Receiver operating characteristic (ROC) curvedpreeclampsia vs normal pregnancy. The probability of pre-
eclampsia was determined in 2 groups of women (normalpregnancy and preeclampsia) using a predictive model derivedfrom the differences between their BMACs. The ROC curvedemonstrates the continuum of sensitivity and specificity
encountered as the cutoff point (predicted probability ofdisease) was varied. The optimal combination (observed at the‘‘shoulder’’ of the curve at top left) was sensitivity=92.3%
and specificity=89.7% (cross-validated sensitivity=88.5 andspecificity=79.3%). This ROC curve describes the perfor-mance of the breath test in women with established disease,
and additional studies need to be performed at earlier stages ofpregnancy to determine if the breath test can predict the onsetof preeclampsia.
Several studies have employed different markers to es-timate oxidative stress, and there is agreement that thelevel of lipid peroxides in blood is generally higher inpregnant women than in nonpregnant women.33 How-ever, comparisons between normal pregnancy and pre-eclampsia have yielded conflicting results with differentmarkers. Studies employing plasma F(2)-isoprostanes34
and the ratios of free-to-oxidized cysteine, homocysteine,and cysteinylglycine7 found significant increases in pree-clampsia.compared with normal pregnancy. However,studies employing lipid hydroperoxides, malondialde-hyde,35 and breath ethene36 found no difference betweenthe 2 groups. The central difficulty in interpreting theseapparent disparities is that there are no studies compar-ing the sensitivity and specificity of the different markersof oxidative stress. One possible explanation is thatmarkers such as the BMAC and F(2)-isoprostanes aremore sensitive to increased oxidative stress in preeclamp-sia than lipid hydroperoxides and breath ethene. In sup-port of the sensitivity of the BMAC, it has demonstratedsignificant increases in oxidative stress in normal breath-ing oxygen21 and in aging,22 and has provided a sensitiveand specific marker of lung cancer,18 breast cancer,19
heart transplant rejection,37 and unstable angina.20 Thestrength of the BMAC, compared with most othermarkers, is that it comprises the aggregate of 107 differ-ent end products of oxidative stress.
The physiologic role of oxidative stress during nor-mal pregnancy is poorly understood; it may result fromthe maternal response to pregnancy when spiral arteriesare transformed into low resistance vessels around theinvading trophoblast.38 However, increased oxidativestress may also originate in the fetus because ROS actas signal transducers during normal growth and devel-opment. ROS are essential regulators of cell prolifera-tion and differentiation; eg, in the central andperipheral nervous system, ROS initiate the establish-ment of neuronal patterns and promote subsequent neu-rogenesis.39 The process may be mediated by growthfactor or cytokine stimulation, which causes a rapid in-crease in intracellular ROS.40
Table III Breath test discriminators between preeclampsiaand normal pregnancy
Undecane6-methyltridecane2-methylpentane5-methyltetradecane2-methylnonane
Discriminant analysis of the BMACs (shown in Fig 2) identified these 5
components of the BMAC as optimal discriminators between
uncomplicated pregnancy and preeclampsia (P!10�4 for each VOC).
These VOCs were incorporated into a predictive model that accurately
discriminated between the 2 groups. The sensitivity and specificity of
this model are shown in Fig 4.

Moretti et al 1189
This was a cross-sectional study performed in womenwith established preeclampsia. Consequently, the clini-cal value of this breath test as a predictor of preeclamp-sia is unknown because it is not known whetherincreased oxidative stress precedes the onset of disease.41
Future longitudinal studies are required to determine ifincreased breath markers of oxidative stress during ear-lier stages of pregnancy can predict the onset of pre-eclampsia. In addition, it would be of great interest todetermine if increased oxidative stress in preeclampsiaand normal pregnancy resolves after delivery.
We conclude that a breath test for oxidative stress ac-curately identified women with established preeclamp-sia. Further studies are required to determine ifa breath test for oxidative stress performed earlier inpregnancy can identify women at increased risk of devel-oping preeclampsia.
Acknowledgments
We thank Eugene Sersen, PhD, and James J. Grady,DrPH, for statistical consultation and review.
References
1. Higgins JR, Brennecke SP. Pre-eclampsiadstill a disease of
theories? Curr Opin Obstet Gynecol 1998;10:129-33.
2. Chavarria ME, Lara-Gonzalez L, Gonzalez-Gleason A, Sojo I,
Reyes A. Maternal plasma cellular fibronectin concentrations in
normal and preeclamptic pregnancies: a longitudinal study for
early prediction of preeclampsia. Am J Obstet Gynecol 2002;187:
595-601.
3. Stamilio DM, Sehdev HM, Morgan MA, Propert K, Macones GA.
Can antenatal clinical and biochemical markers predict the
development of severe preeclampsia? Am J Obstet Gynecol 2000;
182:589-94.
4. Forest JC, Masse J, Moutquin JM, Radouco-Thomas M. Pre-
eclampsia: physiopathology and prospects for early detection. Clin
Biochem 1989;22:483-9.
5. Hubel CA. Oxidative stress in the pathogenesis of preeclampsia.
Proc Soc Exp Biol Med 1999;222:222-35.
6. Butterfield DA, Koppal T, Howard B, et al. Structural and
functional changes in proteins induced by free radical-mediated
oxidative stress and protective action of the antioxidants N-
tert-butyl-alpha-phenylnitrone and vitamin E. Ann N Y Acad Sci
1998;854:448-62.
7. Raijmakers MT, Zusterzeel PL, Roes EM, Steegers EA, Mulder
TP, Peters WH. Oxidized and free whole blood thiols in
preeclampsia. Obstet Gynecol 2001;97:272-6.
8. Mutlu-Turkoglu U, Aykac-Toker G, Ibrahimoglu L, Ademoglu E,
Uysal M. Plasma nitric oxide metabolites and lipid peroxide levels
in preeclamptic pregnant women before and after delivery.
Gynecol Obstet Invest 1999;48:247-50.
9. Walsh SW, Vaughan JE, Wang Y, Roberts LJ II. Placental
isoprostane is significantly increased in preeclampsia. Faseb J 2000;
14:1289-96.
10. Kneepkens CM, Lepage G, Roy CC. The potential of the
hydrocarbon breath test as a measure of lipid peroxidation. Free
Radic Biol Med 1994;17:127-60.
11. Hietanen E, Bartsch H, Bereziat JC, et al. Diet and oxidative stress
in breast, colon and prostate cancer patients: a case-control study.
Eur J Clin Nutr 1994;48:575-86.
12. Humad S, Zarling E, Clapper M, Skosey JL. Breath pentane
excretion as a marker of disease activity in rheumatoid arthritis.
Free Radic Res Commun 1988;5:101-6.
13. Sobotka PA, Gupta DK, Lansky DM, Costanzo MR, Zarling EJ.
Breath pentane is a marker of acute cardiac allograft rejection. J
Heart Lung Transplant 1994;13:224-9.
14. Weitz ZW, Birnbaum AJ, Sobotka PA, Zarling EJ, Skosey JL.
High breath pentane concentrations during acute myocardial
infarction. Lancet 1991;337:933-5.
15. Phillips M, Sabas M, Greenberg J. Increased pentane and carbon
disulfide in the breath of patients with schizophrenia. J Clin Pathol
1993;46:861-4.
16. Olopade CO, Zakkar M, Swedler WI, Rubinstein I. Exhaled
pentane levels in acute asthma. Chest 1997;111:862-5.
17. Phillips M, Cataneo RN, Greenberg J, Gunawardena R, Naidu A,
Rahbari-Oskoui F. Effect of age on the breath methylated alkane
contour, a display of apparent new markers of oxidative stress. J
Lab Clin Med 2000;136:243-9.
18. Phillips M, Cataneo R, Cummin A, et al. Detection of lung
cancer with volatile markers in the breath. Chest 2003;123:
2115-23.
19. Phillips M, Cataneo R, Ditkoff B, et al. Volatile markers of breast
cancer in the breath. Br J 2003;9:184-91.
20. Phillips M, Cataneo R, Greenberg J, Grodman R, Salazar M.
Breath markers of oxidative stress in patients with unstable angina.
Heart Dis 2003;5:95-9.
21. Phillips M, Cataneo R, Greenberg J, Grodman R, Gunawardena
R, Naidu A. Effects of oxygen on breath markers of oxidative
stress. Eur Respir J 2003;21:48-51.
22. Phillips M, Cataneo R, Greenberg J, Gunawardena R, Rahbar-
i-Oskoui F. Increased oxidative stress in younger as well as in older
humans. Clinical Chimica Acta 2003;328:83-6.
23. ACOG practice bulletin. Diagnosis and management of pre-
eclampsia and eclampsia. Clinical management guidelines for
obstetrician-gynecologists. 2002;33:312-20.
24. Phillips M. Method for the collection and assay of volatile organic
compounds in breath. Anal Biochem 1997;247:272-8.
25. Phillips M, Herrera J, Krishnan S, Zain M, Greenberg J, Cataneo
RN. Variation in volatile organic compounds in the breath of
normal humans. J Chromatogr B Biomed Sci Appl 1999;729:
75-88.
26. SPSS. Chicago, IL: SPSS, Inc; 1998.
27. Efron B. The jackknife, the bootstrap, and other resampling plans.
Philadelphia: Society for Industrial and Applied Mathematics;
1982.
28. Fletcher R, Fletcher S, Wagner E. Clinical epidemiology: the
essentials. Baltimore: Williams & Wilkins; 1996.
29. Patrick T, Roberts JM. Current concepts in preeclampsia. MCN
Am J Matern Child Nurs 1999;24:193-200.
30. Hubel CA. Dyslipidemia, iron, and oxidative stress in preeclamp-
sia: assessment of maternal and feto-placental interactions. Semin
Reprod Endocrinol 1998;16:75-92.
31. Homzova M, Ostro A. Current views on the etiopathogenesis of
preeclampsia. Ceska Gynekol 2001;66:276-80.
32. Davidge ST. Oxidative stress and altered endothelial cell function
in preeclampsia. Semin Reprod Endocrinol 1998;16:65-73.
33. Little RE, Gladen BC. Levels of lipid peroxides in uncomplicated
pregnancy: a review of the literature. Reprod Toxicol 1999;13:
347-52.
34. Barden A, Ritchie J, Walters B, et al. Study of plasma factors
associated with neutrophil activation and lipid peroxidation in
preeclampsia. Hypertension 2001;38:803-8.

1190 Moretti et al
35. Morris JM, Gopaul NK, Endresen MJ, et al. Circulating markers
of oxidative stress are raised in normal pregnancy and pre--
eclampsia. BJOG 1998;105:1195-9.
36. Zusterzeel PL, Steegers-Theunissen RP, Harren FJ, et al. Ethene
and other biomarkers of oxidative stress in hypertensive disorders
of pregnancy. Hypertens Pregnancy 2002;21:39-49.
37. Phillips M, Boehmer J, Cataneo R, et al. Heart allograft rejection:
detection with breath alkanes in low levels (the HARDBALL
study). J Am Coll Cardiol 2002;1:12-3.
38. Jaffe R. First trimester utero-placental circulation: maternal-fetal
interaction. J Perinat Med 1998;26:168-74.
39. Verity MA. Oxidative damage and repair in the developing
nervous system. Neurotoxicology 1994;15:81-91.
40. Finkel T. Reactive oxygen species and signal transduction.
IUBMB Life 2001;52:3-6.
41. Henriksen T. The role of lipid oxidation and oxidative lipid
derivatives in the development of preeclampsia. Semin Perinatol
2000;24:29-32.