improving the discharge process in hospitals by reducing ...¥rdsamverkanskaraborg... · gemba walk...
TRANSCRIPT
i
Improving the discharge process in hospitals by reducing the number
of utskrivningsklara dagar
A SIX SIGMA PROJECT IN THE SKARABORG REGION 2015
Louise Axelsson,
Victor Romera de la Fuente
Jeanette Andersson

ii
Abstract
This report presents the outcome of a Six Sigma project performed at Skövde Hospital in Sweden. The Six Sigma project was conducted between January and June 2015, with a team consisting of two students from Chalmers University of Technology and a Social Services Development Manager from Skaraborgs Kommunalförbund. The purpose of the project was to investigate how the discharge process in hospitals could be improved by reducing the number of utskrivningsklara dagar. In order to do so the team had to identify the root causes that could explain why a patient medically pronounced ready to be discharged from the hospital has to wait before being finally discharged. The study reported a series of different causes; most significantly those concerning the availability of short-term accommodation at the municipalities (korttidsboende), the Social Services assistance, and the disparate understanding of the discharge process by the different organizations involved in it. In order to deal with the reasons for these causes the team recommends a series of improvements, specifically the implementation of a Network-Learning Platform, having an early planning at the hospitals, informing the doctors about all the areas in the process, having a person-centered care, having VPL nurse involvement in other parts of the process, improving KLARA - SVPL measurement system and recording the reasons why the patients are waiting at the hospital.

iii
Glossary In this report some Six Sigma and healthcare terms will occur. Below there is a list with a description for each one of these. They have been divided according to their respective area. Six Sigma terminology AIM (Affinity-Interrelationship Method) - Is a problem solving tool for analyzing qualitative data and increasing the understanding behind the problems and their relationship to each other. Big Y - The output delivered by the system that needs to be improved. Cause-and-effect/Fishbone/Ishikawa diagram - Qualitative tools for identifying root causes of problems. DMAIC - cycle - Structured problem solving methodology. Acronym for Define, Measure, Analyze, Improve, Control. Effective scoping - A systematic work of identification of what is being delivered by the system (Y), what related measure to this Y needs to be improved (y) and eventual detection of where changes can be made, what inputs are supplied into the system (x) and from whom. Gemba walk - Gemba is a japanese term for the real place. That, in our case, is where the process takes place. Process mapping - An outline representation that captures the process studied. SIPOC - Is a process snapshot that captures information critical to the project. Acronym for Supplier, Input, Process, Output, Customer. Small y - A measure that should be understood and improved. VOC (Voice of the customer) - Identify what the customer wants and needs. Healthcare terminology AT (Arbetsterapeut) - Occupational therapist. Betalningsansvarslagen - National law that regulates municipal payment liability for the patients in the hospital when they are ready to be discharged. Hemtjänst grupperna - Personal Groups working with Social Care Service. Kallelse - An information message in KLARA - SVPL sent from the hospital to the municipality that triggers the discharge planning process. Karensdagar - Payment-free period of time with a maximum extension of five days that municipalities have to plan for the patient´s takeover and health and care plan.

iv
KLARA - SVPL - IT-communication system in Västra Götalands region. Short-term accommodation (korttidsboende) - Municipal lodging intended for temporary health care, 24 hours a day. Ready to be discharged - The physician will pronounce the patient ready to be discharged when the patient no longer needs the hospital healthcare resources. SG (Sjukgymnast) - Physiotherapist. Socialstyrelsen - The National Board of Health and Welfare is a Government agency in Sweden dependent of the Ministry of Health and Social Affairs. SOL (Social tjänstens insatser) - Social Service Assistance SVPL - Coordinated discharge planning process between the hospital and the municipality. Utskrivningsklara dagar - The number of days the patient stays in hospital after they have been already pronounced ready to be discharged.
Vårdplaneringsmöte - Care plan meeting with the patient, relatives, nurses and social care peoples.

v
Contents
1. Introduction ...................................................................................................................... 1 1.1 Background and problem description .......................................................................... 1
1.1.1 The coordinated discharge planning process ...................................................... 1 1.1.2 Patient ready to be discharged from hospital: The concept ................................ 1
1.2 Purpose ......................................................................................................................... 2 1.3 Delimitations ................................................................................................................ 2
2. Methodology ..................................................................................................................... 2 2.1 Interviews ..................................................................................................................... 2 2.2 Observations ................................................................................................................. 2 2.3 Journal .......................................................................................................................... 3 2.4 Timeline ....................................................................................................................... 3 2.5 Six Sigma approach...................................................................................................... 3
3. Define phase ...................................................................................................................... 3 3.1 Tools used .................................................................................................................... 3 3.2 AIM .............................................................................................................................. 4
3.2.1 AIM session ........................................................................................................ 4 3.2.2 Reflections after the AIM session....................................................................... 4
3.3 Voice Of the Customer ................................................................................................. 5 3.4 Project charter .............................................................................................................. 5 3.5 Effective scoping .......................................................................................................... 5 3.6 Summary of the Define phase ...................................................................................... 6
4. Measure phase .................................................................................................................. 6 4.1 Tools used .................................................................................................................... 6 4.2 Process mapping........................................................................................................... 6 4.3 Data sources ................................................................................................................. 7 4.4 Area of study ................................................................................................................ 8 4.5 Measurement System Analysis .................................................................................... 9
4.5.1 KLARA-SVPL System ....................................................................................... 9 4.5.2 Excel files ........................................................................................................... 9
4.6 Summary of the Measure phase ................................................................................. 10 5. Redifine ........................................................................................................................... 10
5.1 Focus at one hospital .................................................................................................. 10 5.2 Focus at two wards ..................................................................................................... 10 5.3 Reflections after redefine ........................................................................................... 11
6. Analyze phase ................................................................................................................. 11 6.1 Tools used .................................................................................................................. 11 6.2 Analysis of the process flow ...................................................................................... 11 6.3 Analysis of the collected data .................................................................................... 13 6.4 Determination of root causes ..................................................................................... 14
6.4.1 Cause and effect fishbone diagram ................................................................... 14 6.4.2 Identification through semi-structured interviews ............................................ 14 6.4.3 Trial investigation on root causes ..................................................................... 15
6.5 Conclusions of the Analyze phase ............................................................................. 15 6.6 Summary of the Analyze phase .................................................................................. 16
7. Improve phase ................................................................................................................ 16 7.1 Tools used .................................................................................................................. 16 7.2 Improvement proposals .............................................................................................. 16
vi
7.2.1 Implement a network - learning platform ......................................................... 16 7.2.2 Early planning at the hospital ........................................................................... 16 7.2.3 Inform the Doctors about all the areas in the process ....................................... 17 7.2.4 Person-centered care ......................................................................................... 17 7.2.5 VPL-nurse involment in other parts of the discharge process .......................... 17 7.2.6 Improve KLARA-SVPL measure system ........................................................ 17 7.2.7 Mark down the reasons why patients are waiting at the Hospital .................... 17
8. Control phase .................................................................................................................. 18 9. Recommendations .......................................................................................................... 18 10. Conclusion ................................................................................................................. 19 11. Discussion and reflection ......................................................................................... 19
11.1 Reflections upon the project .................................................................................. 19 11.2 Discussion about the near future implications of this research ............................. 20
12. References ................................................................................................................. 21 13. Appendix 1 - Gantt timeline .................................................................................... 22 14. Appendix 2 - SIPOC ................................................................................................ 23 15. Appendix 3 - Improved SIPOC and process map for Ward 73 ........................... 24 16. Appendix 4 - Project Charter.................................................................................. 25

1
1. Introduction
Vårdsamverkan Skaraborg is a coordinated effort between the hospital, primary health center, dental center, and the municipalities in the Skaraborg region. Vårdsamverkan aims to get an effective care collaboration between all parties involved. The goal is that residents and patients receive health care without limits. Skaraborg have 260 000 inhabitants in 15 municipalities. The hospitals are placed in Skövde, Lidköping, Mariestad and Falköping and there are 34 primary health center.
1.1 Background and problem description A major problem is that many patients - often fragile, elderly people – have to remain in hospital for too long time. That means decreased quality of life, health and security. A more efficient discharge process would result in more available hospital beds for patients with greater needs. Residents would also get more health care out of the taxes (Sveriges läkarförbund 2014). Patients who are ready to be discharged but remain in hospitals is a well known problem. Today, about 5 per cent of the hospitals’ beds are occupied by patients who do not need to be there. The national average for this group is of four waiting days after they were pronounced ready to be discharged before they can leave institutional healthcare. There is a real lack of consensus on the issue between the municipalities and County Council. There is neither common understanding nor an immediate solution for the cause of this problem (Statens offentliga utredningar 2015:20).
1.1.1 The coordinated discharge planning process Patients who need coordinated efforts from the municipality have the right to get a coordinated care planning during their time at the hospital (Hälso- och sjukvårdslagen 1982: 763 § 3f). Coordinated health and social care planning should be done when the patient is deemed to be in need of future interventions for continued health and/or care and rehabilitation after being discharged i.e. the transition from hospital care to other forms of health care. Coordinated health and social care planning should be based on patient´s needs, circumstances and preferences. It is a collaboration between representatives from the municipality, hospital and primary health care, together with the patient and his/her relatives when planning for continued health and social care after being discharged from hospital. According to national and regional laws and governing documents, i.e., (SOSFS 2005: 27) by the National Board of Health regulations about the cooperation in the admission and discharge process in hospital care, and the law (SFS 1990: 1404) about municipal liability for certain health care, the coordinated discharge planning process consists of six phases.
1.1.2 Patient ready to be discharged from hospital: The concept In 2003 the concept of finished with medical treatment was changed into ready to be discharged. The attending physician would then decide that the patient is ready to be discharged when the patient no longer needs the hospital healthcare resources (SFS 2003:193). A discharge message is sent to the receiving organization with the date of discharge day. Betalningsansvarslagen regulates the municipal payment liability for the patients in hospital when they are ready to be discharged if the patient has a health care plan established. Municipalities have five payment-free days to make a health care plan for these patients. The purpose of this law is that it should be possible for municipalities to take over the responsibility of patients when they do not longer need hospital care within a reasonable period of time (SFS 1990:1404).

2
1.2 Purpose In 2014 a discussion about the reason why the patients remain in hospital started in Skaraborg, with different perceptions between the municipalities and County. There was also a distrust in the existing data about the number of days that a patient ready to be discharged stays at the hospital. The Steering Committee from Vårdsamverkan gave a mission and the purpose for this Six Sigma project: "Review the variations in utskrivningsklara dagar between the municipalities and the hospitals. Investigate the reason why patients ready to be discharged remain in hospital care despite the fact that they are considered ready to be discharged. This mission will be implemented in a spirit of healthcare collaboration to review the problem from both the hospital and the municipalities´perspective”. The goal should be to shorten waiting times as much as possible.
1.3 Delimitations This Six Sigma project has the following delimitations. The project focuses on elderly people over 65 years old who need help from the municipality when leaving the hospital. Children and patients in the psychiatric wards are excluded because KLARA - SVPL has no access to the data in the psychiatric Ward and the discharge nurses have no jurisdiction over the psychiatric ward. The primary health care centers will not be included in the project because they are not so active in the discharge process today.
2. Methodology
This study has been based on the DMAIC-cycle, which is a structured problem-solving methodology. Before explaining each step in the DMAIC-cycle, this chapter will describe what type of methods/tools that have been used to enhance the project and the steps. The methods included qualitative and quantitative data collections through meetings, interviews, observations and Gemba walks.
2.1 Interviews Semistructured interviews have been used in the project to get information and develop the team's knowledge regarding the discharge process. According to Bryman and Bell (2011) the order of the predefined questions can vary in a semi-structured interview. The researcher has also the possibility of asking questions to the attendants. Three interviews were made with three members from the project group, all three of them on the telephone, with satisfactory results. One of the Swedish members in the group made the interviews in Swedish, since the team did not want to hinder the interviewees by conducting these interviews it in English. The main question was “Why does the hospital have utskrivningsklara dagar?” which was followed by more specific questions. The three interviews were also used as a base when the team started to measure reasons for utskrivningsklara dagar at the hospital. The team also had briefer interviews and discussions with the personnel during the visits that took place there at the hospital. These were conducted in Swedish and face to face with the people involved in the discharge process.
2.2 Observations Observations have been done to understand the process better and to get a deeper insight into the different steps of the discharge process. One of the observations was done together with one of the discharge nurses at Skövde Hospital. The team sat beside the nurse when she administered different discharge cases. Later on she also had the possibility to show the team how the nurses are filling in the Excel files and the documents used for the vårdplaneringsmöten. One important step in the discharge process is the vårdplanering, where all the parts involved have a meeting together with the patient. The team got the opportunity to join a vårdplaneringsmöte at Skövde Hospital to observe how one of these meetings proceed. This was

3
helpful because it showed that in these meetings the patient is in the very focus, a focus that sometimes was lost during the project group discussions that would revolve more around organizational aspects of the process.
2.3 Journal A project journal has been used through the whole project and helped the team to be continually updated when working from different places and with different tasks. The team was very strict having entries after every meeting, since it is easy to forget important information otherwise. The journal was also very helpful when the team came to the improvement phase by having the possibility to search for ideas and tips that were mentioned at the very beginning of the project. All team members have participated in the writing of the journal; the order of this participation has depended on the time availability of the members. The journal will be part of a separate file.
2.4 Timeline A Gantt chart was created to plan the available time. The main phases of the DMAIC-cycle as well as group meetings and sessions (e.g AIM-session) were timetabled to help structuring the project. See Appendix 1.
2.5 Six Sigma approach Six Sigma is about describing and reducing variation in all processes in all parts of the organization (Hammersberg 2015). The purpose is to eliminate the root-causes to errors and failures that are identified by understanding what outputs the customers see as critical. As already mentioned the DMAIC approach has been used. The letters are an acronym for the five phases of the Six Sigma improvement cycle: Define - Measure - Analyze - Improve - Control (George et al. 2005).
3. Define phase
The Define phase is the first step in the DMAIC-cycle. This phase includes identifying what is the Output of this activity (Y). According to George et al. (2005) the purpose with Define is to have the team and the stakeholders reaching an agreement on the scope, goal, financial and performance targets for the project. In Six Sigma,Define together with Measure and Control are regarded as the most important phases (Hammersberg 2015). Since the project involves two major organizations, the hospital and the municipality, it was important to get the perspective and the voice from each one of them to be able to understand the process. This was done by conducting an AIM-session, defining a project charter and through Gemba walks. A time plan was created and data was collected as well.
3.1 Tools used As mentioned above the team employed the Affinity-Interrelationship Method to analyze the problem that they have got. To further increase the team´s understanding of the problem they collected the Voice of the Customer, this was mainly done through meetings and interviews. A project charter was created to keep the team under a shared understanding about the project. Gemba walks helped to further understand the process, but the project´s time limits and the complexity of the organizations made it impossible for the team to walk through the whole process at Skaraborg hospitals.

4
3.2 AIM The Affinity-Interrelationship Method (AIM) is a problem solving tool. According to Alänge (2005) the tool is based on two of the seven management tools: the affinity diagram and the interrelationship diagram. Many scholars and companies have used this approach to analyze complex problems and so the team did with this project. It also serves to increase the understanding behind these problems and their relationships.
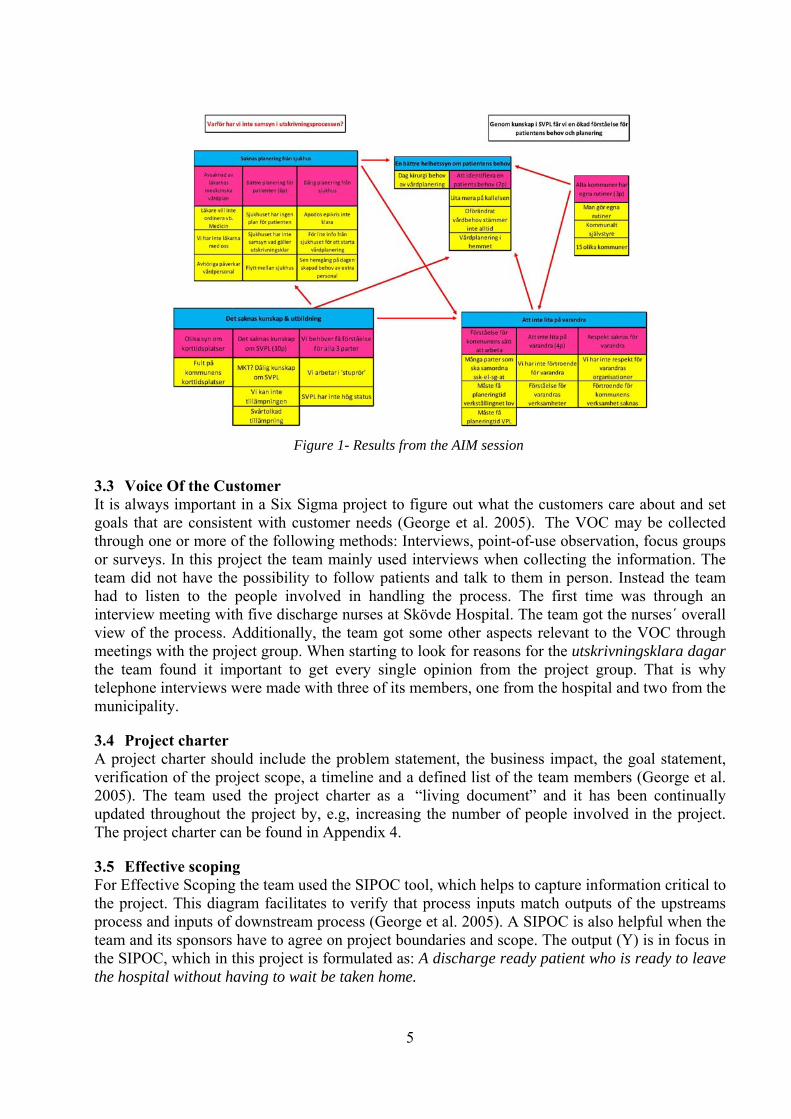
3.2.1 AIM session Before the session took place, some background data were prepared mainly consistent of graphs that showed the actual distribution of utskrivningsklara dagar for the municipalities and some additional information about the Six Sigma methodology. Even though the participants in the session had a fairly good knowledge about the problem, it was important to make sure that everyone had the same understanding. The session was the first meeting with the project group, and it was important to introduce them to the problem. It started with some general discussion where everyone wanted to share their point of view. The group consisted of five people who represented both Hospital and municipality. Not too long into the discussion they ended up agreeing upon that they viewed the problem from different perspectives. That is why the AIM question was formulated in the following way: “Why do we not have the same view of the discharge process?” The session went smoothly and every participant got involved into the brainstorming, grouping and in discussions. Everyone seemed to be satisfied with the results, consisting of five main clusters. The headers for these five groups were: Lack of planning from the hospital, lack of knowledge and education, a better “comprehensive view” of the patients’ view, lack of trust between each other and that every municipality has its own different routines. The voting results highlighted three main issues: First, knowledge is missing about SVPL. Secondly, patient’s needs have to be identified. Third, improve the present planning for the patients. Afterwards the results of the analysis were summarized in one conclusion sentence: “Through knowledge in SVPL we get an increased understanding about the patients’ needs and planning.” The AIM chart can be seen in figure 1.
3.2.2 Reflections after the AIM session Even though the conclusion does not answer the question and did not bring any new information for those participating in the session, it was a good help for the team to increase their understanding of how the problem really looked like. The team saw a clear difference between the participants´ views on the same process. This differences could be explained by their diverse knowledge and education on the various areas. A specially important subsequent realization was that the group had not talked anything about the patients. How are they feeling? Do they actually feel that they are ready to go home? These kind of questions were reflected upon and needed to be addressed.
5
3.3 Voice Of the Customer It is always important in a Six Sigma project to figure out what the customers care about and set goals that are consistent with customer needs (George et al. 2005). The VOC may be collected through one or more of the following methods: Interviews, point-of-use observation, focus groups or surveys. In this project the team mainly used interviews when collecting the information. The team did not have the possibility to follow patients and talk to them in person. Instead the team had to listen to the people involved in handling the process. The first time was through an interview meeting with five discharge nurses at Skövde Hospital. The team got the nurses´ overall view of the process. Additionally, the team got some other aspects relevant to the VOC through meetings with the project group. When starting to look for reasons for the utskrivningsklara dagar the team found it important to get every single opinion from the project group. That is why telephone interviews were made with three of its members, one from the hospital and two from the municipality.
3.4 Project charter A project charter should include the problem statement, the business impact, the goal statement, verification of the project scope, a timeline and a defined list of the team members (George et al. 2005). The team used the project charter as a “living document” and it has been continually updated throughout the project by, e.g, increasing the number of people involved in the project. The project charter can be found in Appendix 4.
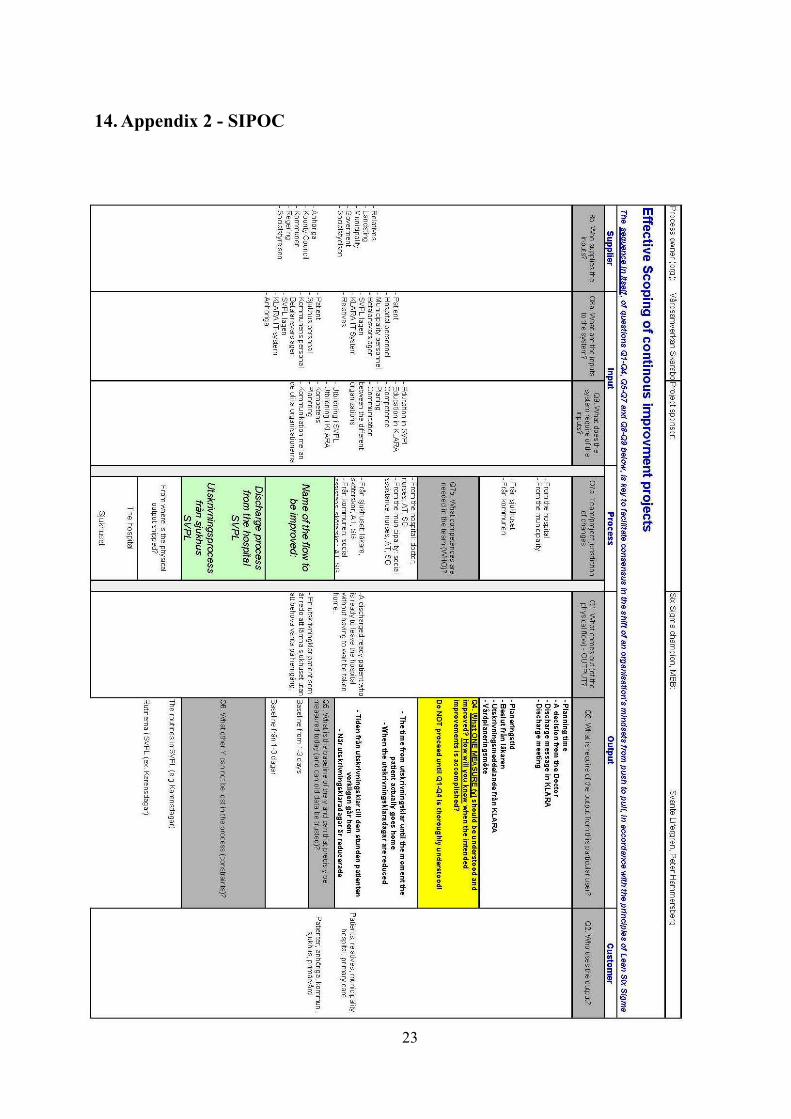
3.5 Effective scoping For Effective Scoping the team used the SIPOC tool, which helps to capture information critical to the project. This diagram facilitates to verify that process inputs match outputs of the upstreams process and inputs of downstream process (George et al. 2005). A SIPOC is also helpful when the team and its sponsors have to agree on project boundaries and scope. The output (Y) is in focus in the SIPOC, which in this project is formulated as: A discharge ready patient who is ready to leave the hospital without having to wait be taken home.
Figure 1- Results from the AIM session

6
The Y is shown in connection to suppliers, inputs, process, output and customers, and can be seen in Appendix 2. One of the most important information in the SIPOC is what measure should be understood and improved and whether it is measurable. This is called y and in this project is stated as: The time from utskrivningsklar until the moment the patient actually goes home. The team will know that the intended improvements are accomplished when utskrivningsklara dagar are reduced. Inputs to the process are also presented in the input column of the SIPOC; these are called x´s and need to be identified.
3.6 Summary of the Define phase The Define phase is mainly focused on having the team and the stakeholders reaching an agreement on the scope, goal, financial and performance targets for the project. The main output of the process (Y) was identified. An useful tool to help analyzing the problem was the AIM-session that was conducted with the participation of the project group. The conclusion from this session was: “We get an increased knowledge about the patients’ needs and planning through knowledge in SVPL”. The VOC was identified by conducting interviews, having meetings and observing personnel connected to the problem. Additionally, a project charter was outlined in order to identify sponsors and key persons of the project. Lastly, the SIPOC diagram summarized the information gathered throughout this phase as a way of defining and visualizing the scope of the project.
4. Measure phase
Data on critical-to-quality characteristics (CTQ) will be collected in the measure phase and will be the base of the following phases (Magnusson 2003). The purpose of this phase is to achieve a thorough understanding of the current state of the process and collect trustworthy data that will be used to reveal the underlying causes of the problem (George et al. 2005). Given the current problem of the differences in the utskrivningklara dagar between the four hospitals in the region, and within each hospital between wards, i.e. The amount of days passed from the moment the patient is pronounced dischargeable until he or she is actually collected from the hospital and taken home, the team members discussed and planned what data would be necessary to collect.
4.1 Tools used All medical records for all the discharge processes in the SkaS region are managed through a centralized IT-system called KLARA - SVPL. The system collects all data related to the discharge process, from all the patient's personal data (personnummer, medical case number, etc.) to all the dates in which all the different phases of the discharge process for the patient took place. All three organizations have access to it and each one of them has to fill in the part of the information it is responsible for. At the same time, that very same data are collected manually and stored in Excel files by the discharge nurses practicing at the hospitals in the Skaraborg region. Another tool used was a process map to gain an enhanced understanding of the sequence, connections and dependencies between the different phases in the discharge process. This process map would later on serve as a basis for calculating the lead time for the whole process.
4.2 Process mapping The discharge process for the elderly people is a coordinated effort involving the hospital, primary health centers and municipalities which follows a sequence of phases set by law and is the same for all parties involved within the Skaraborgs region. The team firstly examined all the available
7
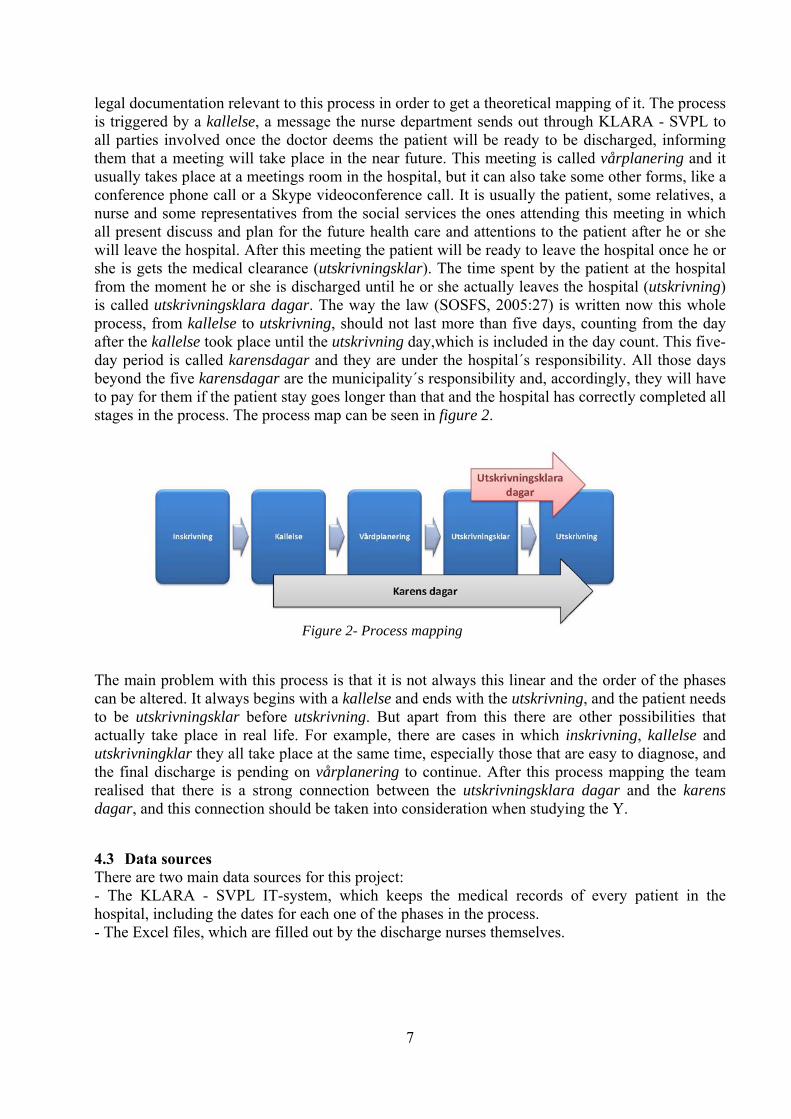
legal documentation relevant to this process in order to get a theoretical mapping of it. The process is triggered by a kallelse, a message the nurse department sends out through KLARA - SVPL to all parties involved once the doctor deems the patient will be ready to be discharged, informing them that a meeting will take place in the near future. This meeting is called vårplanering and it usually takes place at a meetings room in the hospital, but it can also take some other forms, like a conference phone call or a Skype videoconference call. It is usually the patient, some relatives, a nurse and some representatives from the social services the ones attending this meeting in which all present discuss and plan for the future health care and attentions to the patient after he or she will leave the hospital. After this meeting the patient will be ready to leave the hospital once he or she is gets the medical clearance (utskrivningsklar). The time spent by the patient at the hospital from the moment he or she is discharged until he or she actually leaves the hospital (utskrivning) is called utskrivningsklara dagar. The way the law (SOSFS, 2005:27) is written now this whole process, from kallelse to utskrivning, should not last more than five days, counting from the day after the kallelse took place until the utskrivning day,which is included in the day count. This five-day period is called karensdagar and they are under the hospital´s responsibility. All those days beyond the five karensdagar are the municipality´s responsibility and, accordingly, they will have to pay for them if the patient stay goes longer than that and the hospital has correctly completed all stages in the process. The process map can be seen in figure 2.
The main problem with this process is that it is not always this linear and the order of the phases can be altered. It always begins with a kallelse and ends with the utskrivning, and the patient needs to be utskrivningsklar before utskrivning. But apart from this there are other possibilities that actually take place in real life. For example, there are cases in which inskrivning, kallelse and utskrivningklar they all take place at the same time, especially those that are easy to diagnose, and the final discharge is pending on vårplanering to continue. After this process mapping the team realised that there is a strong connection between the utskrivningsklara dagar and the karens dagar, and this connection should be taken into consideration when studying the Y.
4.3 Data sources There are two main data sources for this project: - The KLARA - SVPL IT-system, which keeps the medical records of every patient in the hospital, including the dates for each one of the phases in the process. - The Excel files, which are filled out by the discharge nurses themselves.
Figure 2- Process mapping

8
4.4 Area of study There are four hospitals within Skaraborg´s region: Lidköping, Mariestad, Skövde and Falköping. Only the first three will be the object of this study. Falköping hospital will not be considered because as of now records of the discharge process are not being kept. Based on the data collected by the nurses in the Excel files, the team went on to study the first task entrusted to the team: to review the differences in utskrivningsklara dagar between municipalities within each hospital. Skövde The different mean values for each municipality range from 2 days (Vara, Grästorp) to 4,6 days (Falköping). See figure 3. Lidköping The different mean values for each municipality range from to 3 days (Mariestad) to 4,6 days (Skövde). Notice the important variation for Skövde. See figure 4. Mariestad The different mean values for each municipality range from to 2,5 days (Gullspång) to 4,2 days (Mariestad). See figure 5. As it can be seen, the differences between hospitals are not that dramatic. These results were collected in the following charts:
Figure 3- Skövde 2014
Figure 5- Mariestad 2014
Figure 4- Lidköping 2014
9
4.5 Measurement System Analysis The team studied the possibility of conducting an MSA, but the efforts were unsuccessful. - Gauge R&R: The team could not measure the same item more than once. Each case is unique and a measure on it can only be performed once. - Evaluating Bias: There is not a master value for utskrivningsklara dagar yet. - Measuring Stability: Loss of stability can be due to (George et al. 97): Deterioration of measurement devices: not in this case; the nurses are using a permanently
maintained and supported IT system. Increase in variability of operator actions: there is an undetermined number of nurses working
concurrently on the same file, so at this stage it is very difficult to set them apart and monitor each one of them separately; doing this would have required too many resources in terms of time and manpower from the team but it is suggested having this task performed by a follow-up team.
- Evaluating discrimination: The measuring system does not detect variation in the data, it only records it. - Kappa analysis: The team is not dealing with attribute data, but using continuous data. The team proceeded to ensure the accuracy, consistency and reliability of the data (George et al. 2005). In order to do so both data sources were examined separately.
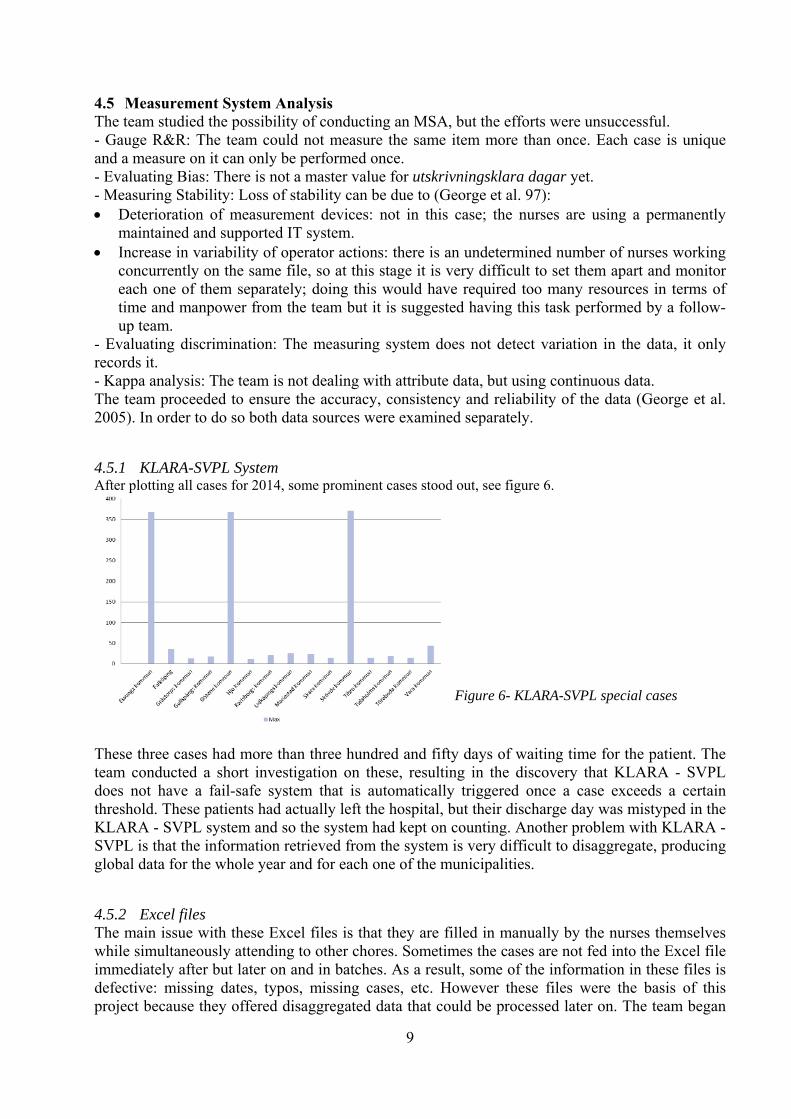
4.5.1 KLARA-SVPL System After plotting all cases for 2014, some prominent cases stood out, see figure 6.
These three cases had more than three hundred and fifty days of waiting time for the patient. The team conducted a short investigation on these, resulting in the discovery that KLARA - SVPL does not have a fail-safe system that is automatically triggered once a case exceeds a certain threshold. These patients had actually left the hospital, but their discharge day was mistyped in the KLARA - SVPL system and so the system had kept on counting. Another problem with KLARA - SVPL is that the information retrieved from the system is very difficult to disaggregate, producing global data for the whole year and for each one of the municipalities.
4.5.2 Excel files The main issue with these Excel files is that they are filled in manually by the nurses themselves while simultaneously attending to other chores. Sometimes the cases are not fed into the Excel file immediately after but later on and in batches. As a result, some of the information in these files is defective: missing dates, typos, missing cases, etc. However these files were the basis of this project because they offered disaggregated data that could be processed later on. The team began
Figure 6- KLARA-SVPL special cases

10
by not considering those cases that did not have either a utskrivningsklar or an utskrivning date, because without any of these it is not possible to calculate the utskrivningsklara dagar, and thus, 12% of the total aggregated data for the three hospitals was not usable. However, a closer look into the data showed that these incomplete entries were unevenly distributed: for Lidköping it was the 10%, for Mariestad the 1% and for Skövde 20%. This was explained by the relative size of each hospital: Mariestad being the smaller one has hardly any problems filling in the files while Skövde being the biggest one of the three has to deal with a heavier workload that affects the way information is recorded.
4.6 Summary of the Measure phase An initial process mapping helped the team to get a better understanding of the whole discharge process. Two data sources were used to obtain temporal data for each one of the phases in the process and this data was used to review the differences in utskrivningsklara dagar between municipalities within each hospital. While conducting this study several issues relating to the measurement systems surfaced: one of them was found to be unreliable and the other produced unusable data because it was either missing or defective; the relative proportion of this data varied depending on the size of the hospital.
5. Redifine
As mentioned above, one of the goals of the project was to investigate how the number of utskrivningsklara dagar vary between the different municipalities in the Skaraborg region. But also which root-causes are behind this variation. The team started working with data from all municipalities and three different hospitals. When studying this data, the team realized that it would be difficult to work with this amount of data. The decision was made to narrow down the scope of the project and delimit the amount of data that would be examined.
5.1 Focus at one hospital The team arranged a meeting with the project group where the team presented the average and standard deviation of the utskrivningsklara dagar for all wards at the three hospitals. In consultation with the project group they decided to focus on Skövde Hospital. The reason behind this decision was that the project group had more information and knowledge about Skövde Hospital than about the other two.
5.2 Focus at two wards When the decision about focusing on Skövde Hospital had been taken, the team wanted to dig deeper into the data. The team in consultation with the project group wanted to identify one good and one bad performing ward. They identified ward 73 (Hematology) and ward 81(Orthopedics) as the ones with highest mean, and thus considered as two bad performing wards, see figure 7.
21 22 31 32 41
41-42 42 51 52 54 55 56 63
63-64 64 65 71 72 73 74 81 82 83 84
21 22 31 32 41
41-42 42 51 52 54 55 56 63
63-64 64 65 71 72 73 74 81 82 83 84
Figure 7- Wards at Skövde Hospital
11
A further analysis of these wards revealed that even though ward 81 had a higher mean, the standard deviation was 2,63 which is lower than ward 73´s 3,35. The team had to decide whether they should further investigate ward 73, that had a lower mean but higher standard deviation, or ward 81, that had a higher mean but lower standard deviation. This decision was easier when realizing that ward 81 is an orthopedic ward. Vårdplanering is frequently deferred for patients who had just had surgery because they often feel more recovered after three or four days after the procedure, resulting in an increased number of utskrivningsklara dagar. This helped identifying the reason for the high amount of utskrivningsklara dagar at ward 81. Additionally, ward 73 is already working on a process mapping and improvement measures. When studying a process, not only the worse cases should be reflected upon, but also the good performing ones should be considered; this contrast view will help us realize what makes the good ones good (Hammersberg 2015). Ward 32 was considered as a good performing ward since it has a low mean and at the same time a low standard deviation 1,69.
5.3 Reflections after redefine After making this decision, Ingela Morgan at ward 73 was contacted and a further analysis of the ward was conducted. The goal was to plot a p-mapping for ward 73, but once there the team was informed that another study had been conducted on this ward, resulting in an patient-centered process mapping and a patient-centered SIPOC. The team was also informed that from the starting of 2015 both wards 73 and 74 would work together as a single unit. Based on this information, the team decided that from there on both wards would be considered as a sole one. Another issue that arose directly after this decision was if the wards actually have something to do with the number of utskrivningsklara dagar; there might some be other factors affecting the utskrivningsklara dagar not specifically ward related.
6. Analyze phase
According to George et al. (2005) the purpose of the define phase is to "pinpoint and verify causes affecting the key input and output variables" tied to the goals of the project. For this Six Sigma project the aim was to find the root causes for the stated problem, i.e. why do some patients stay in hospital more than two days even though they are already discharged and ready to go, with the help of the chosen analysis tools.
6.1 Tools used All the data collected during the Measure phase were the points in time at which each phase in the process took place, i.e. dates. However, due to the complexity of the discharge process itself and its non-linear flow it was problematic to determine whether the unwanted variation in the duration of the discharge process could be related to any cause belonging to the process itself, to the hospital, to the municipality, to none, to some or to all of them just by solely looking into this chronological data. This is why several additional tools were used in order to help the team to push beyond symptoms to uncover potential root causes.
6.2 Analysis of the process flow An initial analysis of the structure of the discharge process revealed that the variation in the utskrivningsklara dagar for the patient could not be exclusively related to the utskrivningsklar and the utskrivning phases, but also it should be examined for all upstream phases leading up to them and for the whole discharge process as well. Based on the process mapping previously performed, lead time calculations were made for the most significant phases in the process and globally for the whole process both at ward 32 and ward 73-74.

12
In order to make these new calculations, all the data collected in the Measure phase had to be reviewed again to ensure their integrity, because previously only the completeness of the data for utskrivningsklar and the utskrivning phases was secured. The results are shown in the following figures: Ward 32 - Kallelse - Utskrivning (NB: Neither kallelse day nor weekend days are included) Mean: 5,36 - Standard Deviation: 3,87 - Kallelse - Utskrivningsklar (NB: Neither kallelse day nor weekend days are included) Mean: 4,36 - Standard Deviation: 3,88 - Kallelse - Vårdplanering (NB: Vårdplanering day is included but neither kallelse day nor weekend days are). Mean: 2,49 - Standard Deviation: 1,24 - Vårdplanering - Utskrivningsklar (NB: Both days are included. Weekends are not) Mean: 2,63 - Standard Deviation: 4,20 - Utskrivningsklar - Utskrivning (y in the SIPOC) (NB: Both days are included. Weekends are not. Also no negative values were considered, as this would imply that the patient would have left the hospital without being discharged. This day computation is congruent with the criteria employed by the KLARA - SVPL system). The following figure shows the histogram for this measure, see figure 8.
Ward 73-74 - Kallelse - Utskrivning (NB: Neither kallelse day nor weekend days are included) Mean: 5,51 - Standard Deviation: 3,97 - Kallelse - Utskrivningsklar (NB: Neither kallelse day nor weekend days are included) Mean: 3,37 - Standard Deviation: 4,20 - Kallelse - Vårdplanering (NB: Vårdplanering day is included but neither Kallelse day nor weekend days are). Mean: 2,5 - Standard Deviation: 1,46 - Vårdplanering - Utskrivningsklar (NB: Both days are included. Weekends are not) Mean: 1,44 - Standard Deviation: 4,37 - Utskrivningsklar - Utskrivning (y in the SIPOC) (NB: Both days are included. Weekends are not. Also no negative values were considered, as this would imply that the patient would have left the hospital without being discharged. This day computation is congruent with the criteria employed by the KLARA - SVPL system). The following figure shows the histogram for this measure, see figure 9.
Figure 8- Histogram for Ward 32

13
All these values were collected in the following lead time process mapping for both wards, see figure 10.
The analysis of this two process maps revealed some thought-provoking points for further investigation. Interestingly enough the total lead time for both wards is very similar. It was already known that both wards differed mainly in their utskrivningsklara dagar; however, these results showed that the time between vårdplanering and utskrivningklar for ward 73-74 is about double that same time for ward 32.
6.3 Analysis of the collected data As it has been previously mentioned, a certain amount of cases could not be used because they did not include information about one or more phases in the process. This meant that any case which had been stored in the files without recording the date of either kallelse, vårdplanering, utskrivningklar or utskrivning was removed from the data set. The team had a closer look on how this process of discarding could affect the integrity of the collected data and so a histogram was plotted. It showed that these incomplete entries were evenly distributed during the year, see figure 11.
Figure 9- Histogram for Ward 73-74
Ward 32 Ward 73-74 Figure 10- Lead times for the process
Figure 11- Distribution of the missing data
14
6.4 Determination of root causes The team decided that three complementary qualitative tools would be used in order to expose possible root causes for the variation of the utskrivningsklara dagar.
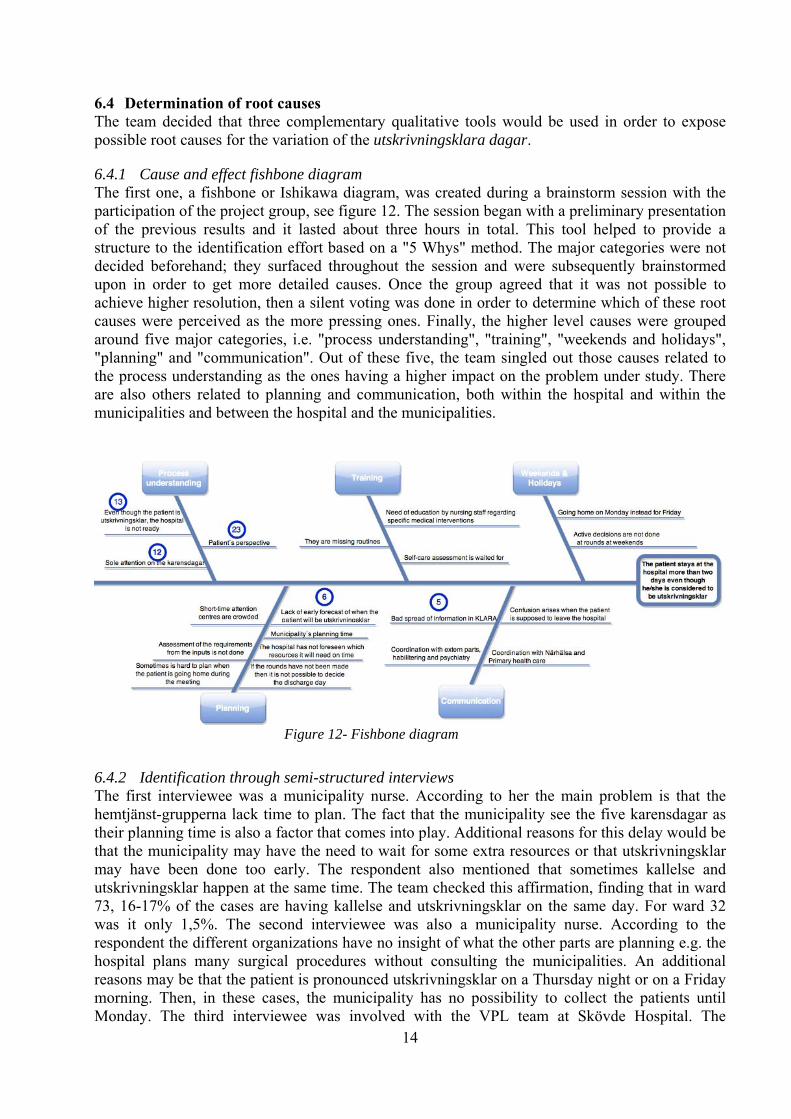
6.4.1 Cause and effect fishbone diagram The first one, a fishbone or Ishikawa diagram, was created during a brainstorm session with the participation of the project group, see figure 12. The session began with a preliminary presentation of the previous results and it lasted about three hours in total. This tool helped to provide a structure to the identification effort based on a "5 Whys" method. The major categories were not decided beforehand; they surfaced throughout the session and were subsequently brainstormed upon in order to get more detailed causes. Once the group agreed that it was not possible to achieve higher resolution, then a silent voting was done in order to determine which of these root causes were perceived as the more pressing ones. Finally, the higher level causes were grouped around five major categories, i.e. "process understanding", "training", "weekends and holidays", "planning" and "communication". Out of these five, the team singled out those causes related to the process understanding as the ones having a higher impact on the problem under study. There are also others related to planning and communication, both within the hospital and within the municipalities and between the hospital and the municipalities.
6.4.2 Identification through semi-structured interviews The first interviewee was a municipality nurse. According to her the main problem is that the hemtjänst-grupperna lack time to plan. The fact that the municipality see the five karensdagar as their planning time is also a factor that comes into play. Additional reasons for this delay would be that the municipality may have the need to wait for some extra resources or that utskrivningsklar may have been done too early. The respondent also mentioned that sometimes kallelse and utskrivningsklar happen at the same time. The team checked this affirmation, finding that in ward 73, 16-17% of the cases are having kallelse and utskrivningsklar on the same day. For ward 32 was it only 1,5%. The second interviewee was also a municipality nurse. According to the respondent the different organizations have no insight of what the other parts are planning e.g. the hospital plans many surgical procedures without consulting the municipalities. An additional reasons may be that the patient is pronounced utskrivningsklar on a Thursday night or on a Friday morning. Then, in these cases, the municipality has no possibility to collect the patients until Monday. The third interviewee was involved with the VPL team at Skövde Hospital. The
Figure 12- Fishbone diagram

15
interviewee indicated that the definition of utskrivningsklar is unclear. The different stakeholders have different views on the process and a distrust has been created between the hospital and municipalities. This distrust has resulted in the hospital pronouncing the patient utskrivningsklar too early. The reason is the belief that the municipalities will not come to fetch these patients right away. The respondent also explains that the municipalities seem to have poor preparedness. Once vårdplanering is already done it should not be a problem to take the patient home even though it is Friday.
6.4.3 Trial investigation on root causes Additionally to the two previous tools, the team decided it would conduct a trial investigation during two weeks to determine the root causes for the deferred departure of the patients. Together with the manager of the VPL team at Skövde Hospital it was agreed that the file which recorded all the cases would contain an extra column in which the actual reason for the delay would be registered. In order to facilitate this extra workload, the team initially devised a coded system with some standard reasons; this code was later refined and updated with some of the root causes detected during the fishbone session plus some additional ones that were brainstormed by the team. The data collected during the aforementioned period was the basis for the following Pareto chart, see figure 13.
6.5 Conclusions of the Analyze phase Employing three complementary techniques for determining the root causes for the deferred departure of the patients, i.e. Fishbone chart, direct interviews with nurses and a trial investigation on root causes, helped the team to get a more comprehensive picture of the reasons behind this problem. Through the fishbone session it was detected that some of these were related to the understanding of the discharge process itself. The interviews with the nurses confirmed this and also contributed with some other reasons: the lack of time for planning, the misuse of the five karensdagar, the deficient communication and mistrust between hospital and municipalities, or the obscure definition for some of the legal terms involved in the process. Finally the trial investigation on root causes produced a Pareto chart which clearly points towards areas that are beyond the hospital boundaries and related to the municipalities, more specifically to how the short-term accommodation centers are being managed.
Figure 13- Pareto chart of the trial investigation

16
6.6 Summary of the Analyze phase The analyze phase began by examining the data collected through the measure face and using it as the foundation for a lead time process mapping for two of the wards at Skövde Hospital: a good performing and a bad performing ward. The comparison of these two mappings revealed that the differences in the discharge process was not only related to the utskrivningsklara dagar but also to other phases in the process, like the time between vårdplanering and utskrivningklar. Based on this preliminary findings and with the help of a fishbone diagram session, personal interviews and a trial two-week investigation that led to a Pareto diagram the team pushed beyond symptoms to uncover potential root causes.
7. Improve phase
The purpose of the improve phase is to learn from pilots of the selected solutions and execute full-scale implementation (George et al. 2005). This project focused the improvement efforts on the main root-causes found in the Analyze phase. As the root-causes in this Six Sigma project are interacting with each other in many ways, it was more useful to develop improvement suggestions that cover more than one causes.
7.1 Tools used The tools that were used when making suggestions for improvement were mainly brainstorming and discussions at group meetings. The main focus was on root causes in which the project group could make a significant impact.
7.2 Improvement proposals Below seven improvement proposals are stated. They are all based on the findings from the fishbone diagram, the trial intervention and also on findings from the measurement phase.
7.2.1 Implement a network - learning platform A recurring factor all throughout the project has been that different organizations have different view at the discharge process. This was already evident at the AIM session. To create a better understanding about each other's work the suggestion is to develop a network. This network will consist of VPL-nurses in the hospitals, VPL-teams in the municipalities and representatives from each primary health care centres in Skaraborg. The network will be divided into three areas in Skaraborg: west, north and south. The action plan that is going to be used is based on the root causes that were found in the analyze phase. But before the implementation and startup of this network a decision from SVPL is required. Additionally, it is suggested having the Managers of the Social Assistance Office at the municipalities trained on KLARA - SVPL to help them increasing their understanding about the discharge process.
7.2.2 Early planning at the hospital Early planning at the hospital is going to be implemented within the near future at Skövde hospital. The idea, as mentioned above, is to get the planning of the discharge process started earlier. This will be already done by issuing an expected date for discharge at the kallelse. An early plan would benefit the hospital by making the discharge process less time consuming; also the municipality will benefit by having an earlier indication on what patient needs will have to be considered first.
17
7.2.3 Inform the Doctors about all the areas in the process The analyze phase showed that both personnel at the hospital and municipality feel that many Doctors do not have a comprehensive perspective of the discharge process and neither of what happens to the patients once they leave hospital. A suggestion is to inform them about how the municipalities work and how they are affected by the Doctor's discharge decision. A further improvement suggestion is to have a study trip to Södra Älvsborgs Hospital, where they are working with planning boards beside each patient´s bed. On each board there is a prognosis of the discharge day. In order to start planning the discharge process earlier this idea could be used at Skaraborg Hospitals as well.
7.2.4 Person-centered care To improve the person-centred care and at the same time decrease the number of utskrivningsklara dagar, it is suggested to devise a continuous staff shift schedule for the hospital. This would implicate that personnel would be working the same shift during the running week with the advantage of having the possibility to follow the same patients through the week and get a better understanding about their situation.
7.2.5 VPL-nurse involment in other parts of the discharge process Today, the discharge nurses at the hospital are involved in the process from kallelse to vårdplanering. Afterwards it is up to the ward to manage the process. A proposal is to involve discharge nurses after the discharge meeting or to select the patients who really need the additional support from the discharge nurse.
7.2.6 Improve KLARA-SVPL measure system As described in the measure phase, KLARA-SVPL is not always a reliable source. The team found cases with over 350 utskrivningsklara dagar, which makes the statistics unreliable. The improvement suggestion is to have a threshold limit that triggers an alarm when a case passes a certain number of utskrivningsklara dagar. Additionally the team believes that a more friendly-user graphic user interface for KLARA-SVPL would make the personnel more interested in using it.
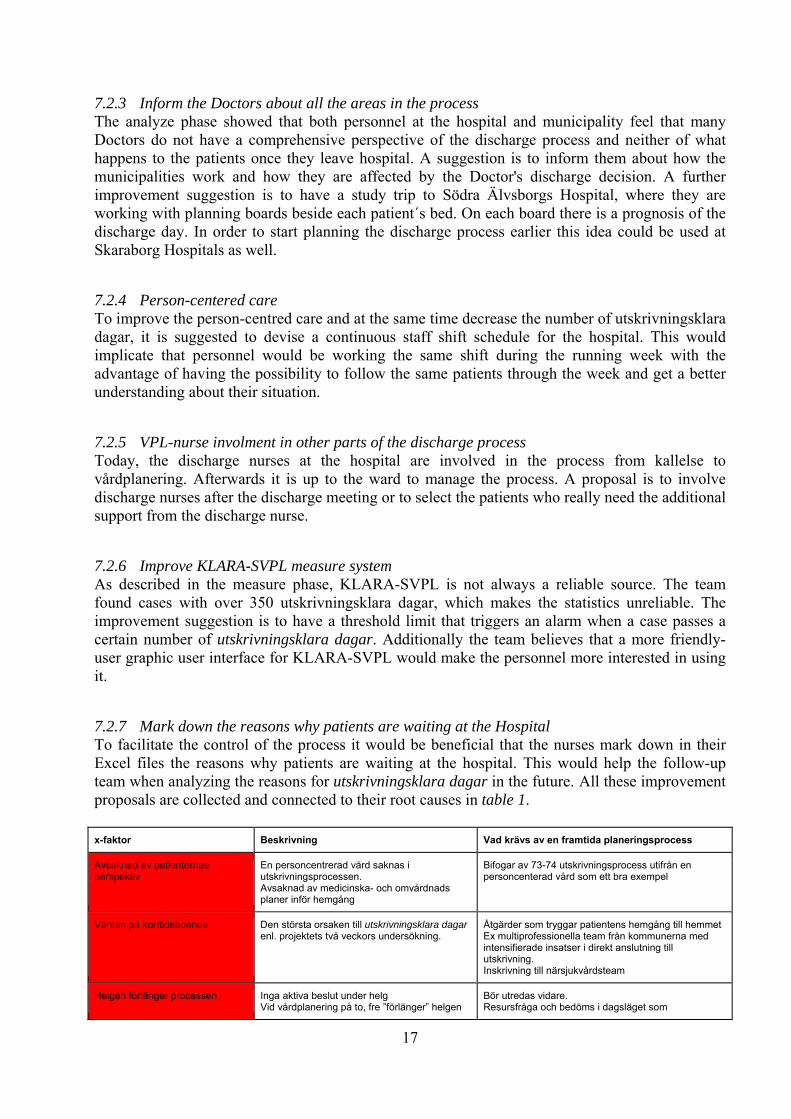
7.2.7 Mark down the reasons why patients are waiting at the Hospital To facilitate the control of the process it would be beneficial that the nurses mark down in their Excel files the reasons why patients are waiting at the hospital. This would help the follow-up team when analyzing the reasons for utskrivningsklara dagar in the future. All these improvement proposals are collected and connected to their root causes in table 1. x-faktor Beskrivning Vad krävs av en framtida planeringsprocess
Avsaknad av patienternas perspektiv
En personcentrerad vård saknas i utskrivningsprocessen. Avsaknad av medicinska- och omvårdnads planer inför hemgång
Bifogar av 73-74 utskrivningsprocess utifrån en personcenterad vård som ett bra exempel
Väntan på korttidsboende Den största orsaken till utskrivningsklara dagar enl. projektets två veckors undersökning.
Åtgärder som tryggar patientens hemgång till hemmetEx multiprofessionella team från kommunerna med intensifierade insatser i direkt anslutning till utskrivning. Inskrivning till närsjukvårdsteam
Helgen förlänger processen Inga aktiva beslut under helgVid vårdplanering på to, fre ”förlänger” helgen
Bör utredas vidare. Resursfråga och bedöms i dagsläget som

18
processen Helgen blir en transportsträcka Resursfråga
okontrollerbar och är beroende av nuvarande lagstiftning.
Saknad av tidig prognos när patienten är utskrivningsklar
Kommunen hinner inte planera insatser innan patienten är utskrivningsklar Det finns ingen plan för patienten i ett tidigare skede. Följer inte rutinen, utskrivningsmeddelandet skickas i stor utsträckning samma dag som utskrivningsklar datum. Lever här och nu, kort framförhållning ”Guldfiskplanering”
Vid inskrivning bedöma en prognos kring planerat utskrivningsklarsdatum. Att redan i ”kallelsen” skriva in prognostiserad utskrivningsdatum. Utbildning krävs inför införandet. En mötesarena, lärplattform, där berörda professioner träffas för att skapa en gemensam målbild, utreda avvikelser, utbyta erfarenheter och utveckla vårdprocessen. Ansvarar också för utbildning/information till sin organisation. Förslagsvis: Vpl sjuksköterskor från slutenvården, läkare VPL team från kommunerna och ansvarig vårdplaneringsansvarig från Primärvården
Tittar blint på karensdagar Ekonomi går före patientperspektivet En mötesarena, lärplattform där berörda professioner träffas se förslag ovan.
Palliativa patienter med öppen retur
Patienter som vill kvarstanna på sjukhuset i den sena fasen i sin palliativa fas kan aldrig bli utskrivningsklara enligt Regional tillämpning –Gemensam rutin i Västra Götaland
Utbildning/information inom sjukhuset: Följa rutinen med avbrott i processen i KLARA-SVPL så att dessa patienter inte räknas in i statistiken för utskrivningsklara patienter.
Dålig kunskap/spridning/användning av KLARA IT-system
Kommunerna saknar förvaltare i SkaraborgTid och resurs för utbildning saknas
Mer utbildning behövs, både i KLARA-SVPL systemet men också en utbildning i SVPL generellt. Utbildning för kontaktombud har pågår.
8. Control phase
The purpose of the control phase is to complete the project work and hand off improved process to process owner, with procedures to maintaining the gains (George et al. 2005). A presentation and hand-over of the project to the process owners is scheduled for the 8th of June 2015, with the participation of the project group, the Manager of the Vårdsamverkan group of Skaraborg and the Developer Manager of the Hospital and Skaraborgs kommunalförbund. The team has also been invited to report back to the Vårdsamverkan steering group in September 2015. The team came up with a series of future recommendations for this stage with the possibility of this follow-up in mind. It began with the team reporting to the group the findings made in the analyze phase and reviewing the improvement proposals in the improve phase. After examining them the team agreed upon the following procedure: First, in two months time, it needs to be verified whether the early discharge prognosis is already being written in the kallelse. From then on the follow-up team should check out whether the utskrivningsklara dagar are decreasing by checking on KLARA -SVPL.
9. Recommendations
- A careful planning of the hand-over to the follow-up group is strongly advised. - In order to structure and start the improvement works to reduce the number of days the patients ready to be discharged have to wait in hospital, municipalities, hospitals and primary health centers should come up with a common understanding of the discharge process. - A priority suggestion would be to start a learning platform where care planning staff from the Hospital, municipalities and primary health centers can work together. It is suggested that Skaraborgs Närvårdsområden would create this group. This movement would be a good strategy and support structure for further development. In a complex, large organization as Vårdsamverkan the interaction within the network is a vital support structure for reflection and new learning.
Table 1- Root causes and improvement proposals
19
- The improvement proposals listed in Table 1 could be the starting point of an action plan for the proposed learning platform. - An early planning for the discharge date and its entering into the kallelse through KLARA - SVPL is a relatively simple improvement to start with, but it will require coaching for many employees in Skaraborg and a written routine should be developed for it. - The team recommends to continue measuring utskrivningsklara dagar in Skaraborg Hospitals and have this data included in other measurements system in Vårdsamverkan. It also recommends to continue collecting data in KLARA - SVPL during the aforementioned period to investigate the reason why patients are staying at the hospital even though they are ready to be discharged. Both Siemens and Västra Götalands Region analysis support should be contacted and briefed concerning the concept of utskrivningsklara dagar, because the way these are counted now is misleading.
10. Conclusion
This study has investigated the variations in utskrivningsklara dagar between the municipalities and the hospitals in Skaraborg. After reviewing Skövde, Mariestad and Lidköping hospitals, a redefining of the scope of the project was needed to be done. The focus was then directed toward Skövde Hospital; the reason for this was that the project group had more information about this hospital than the other two. The next step the team had to take was to study the reason why patients, ready to be discharged, remain in hospital care despite the fact that they are considered ready to be discharged. The Ishikawa diagram showed that some of the reasons were related to the understanding of the process itself. Interviews contributed with further reasons like the lack of time planning, the misuse of the five karensdagar, the deficient communication and mistrust between hospital and municipality, or the obscure definition for some of the legal terms involved in the process. An investigation was made at Skövde Hospital, where the causes for delayed discharge were collected during a certain period of time. The main causes found for a delayed discharge process were that the patient is waiting for a short-time accommodation or because the lack of SOL assistance. The team and the group came up with seven main improvement suggestion built upon the root-causes discovered throughout this project. These recommendations might help the two organization to get a common view of the process which might result in an eventual decrease of utskrivningsklara dagar. Out of these, the team would emphasize starting a learning platform and having an early prognosis for the discharge date included as part of the kallelse.
11. Discussion and reflection
This report will conclude with some reflections upon the project itself and having a discussion on the near future implication of this research.
11.1 Reflections upon the project The transportations between Gothenburg and Skövde required a lot of time from the team. In order to have gained a better understanding of the process it would have been better if the team could have stayed for longer periods of time in Skövde. Additionally, the working language in the Swedish health care system is obviously Swedish, a language that is not mastered by every member in the team, something that at some points complicated communications. Regarding the

20
health care system and the process, its complexity needs to be stressed. This process should be thoroughly analyzed before conducting a full Six Sigma project on it. After working in this project the team had the shared opinion that hospitals, municipalities and county council should allocate more resources into improvement projects. Not mere monetary resources, but time and human resources should be allocated as well.
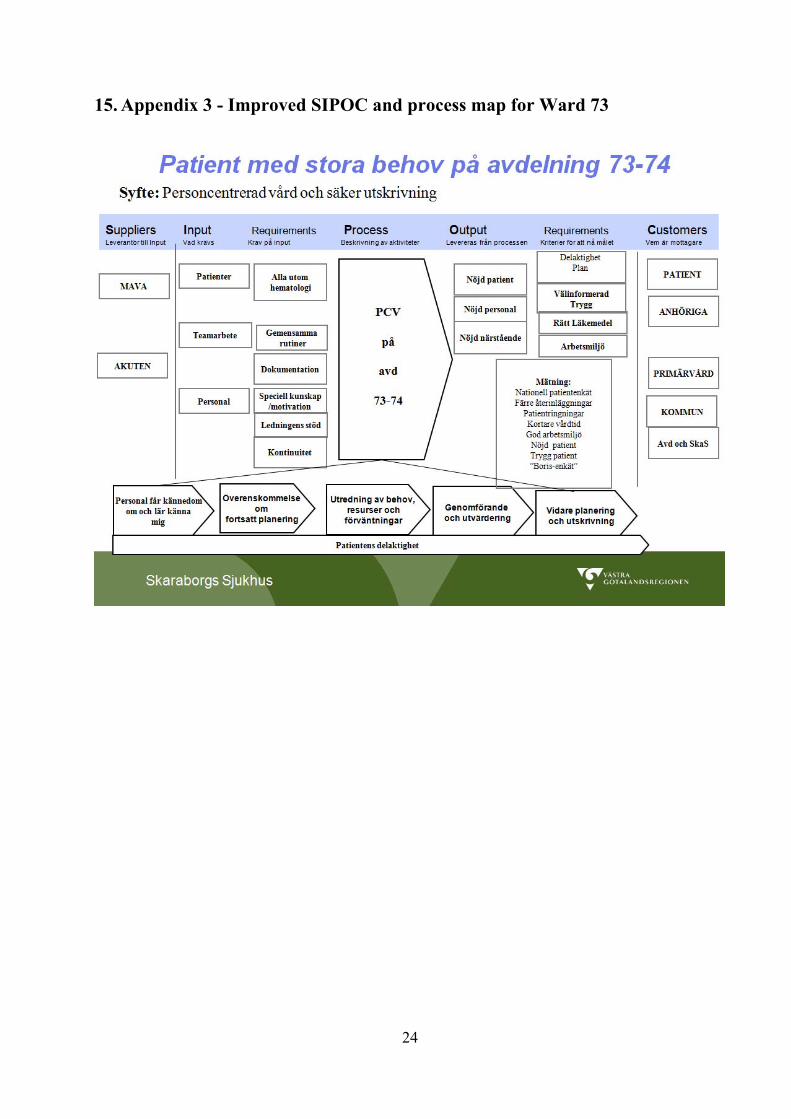
11.2 Discussion about the near future implications of this research In recent years, the average length of hospital stay has been radically reduced. This, in turn, has resulted in greater demands of a more efficient and coordinated planning time. Municipalities should have an opportunity to start the planning earlier than they do today. Studies show that this planning is often deficient, resulting in patients staying more days in hospital, an increased risk of readmissions and an inadequate attention at their homes. Having a person-centered approach, in which patients and families are involved in the discharge planning at the hospital and where the patient is considered as a partner in the care team, the number of days at the hospital can be shortened. This is shown by a recent study from researchers at Sahlgrenska Academy conducted at Sahlgrenska University Hospital Östra, Gothenburg (Ulin, 2015). During 2015, ward 73-74 at Skövde Hospital has designed the discharge process based on a person-centered approach (see Appendix 3). In this Six Sigma project the team found that during 2014, 73-74 was a ward with a high number of utskrivningsklara dagar and variation. It is now essential to continue investigating the variation in the number of utskrivningsklara dagar at this ward to monitor whether this person-centered approach is improving its performance. This Six Sigma project has detected that one of the main reasons for patients staying at hospital even though they are ready to be discharged is that they are waiting for a short-term accommodation at their respective municipality. Many elderly people and their relatives often feel insecure when they are leaving hospital, and therefore desire to stay at a short-term accommodation center. Several municipalities in Sweden have developed Trygg hemgång (Feel safe to go home after being discharged from hospital). It involves a multidisciplinary team from the corresponding municipality that will meet up directly at the patient's home after being discharged and provide an increased intensive support for some weeks. During 2014, some trial testing of this trygg hemgång in Ronneby (Trygg hemgång i Ronneby 2014) came up with some promising results: a markedly increased sense of security for the patients and the professionals, a reduction of 80% in the number of readmissions and a dramatic decrease in costs for short-term accommodation. In the spring of 2015 a new proposal for a new law was presented by the Swedish government with the name "Safe and Effective discharge from hospital" (Swedish Government Official Reports SOU 2015: 20). The goal of this proposal is to provide satisfactory health care while keeping the time spent by the patient going from hospital to municipality healthcare at their own homes or at nursing homes as short as possible. Some studies report that the way the currently applicable laws are written is inadequate for current and future needs. The new law proposes to make some changes in the discharge process; the physician will be required to notify all relevant units concerned through a "registration statement" in which an expected date of discharge should be indicated and which will be issued within 24 hours after the patient entered the hospital. The studies also suggest a reduction in the municipality's planning days from the present five to three, and these including weekend days. On May 18, a conference was organized in Skaraborg where Göran Stiernsted, government advisor, was invited to present the new law proposal. The results from our Six Sigma project were shown at this conference.

21
12. References
Alänge, S. (2009). The Affinity-Interrelationship Method AIM. A Problem Solving Tool for Analysing Qualitative Data Inspired by the Shiba “Step by Step” Approach. Technology Management and Economics, Division of Quality Sciences, Chalmers University of Technology. Gothenburg, Sweden. Bryman, A., Bell, E. (2011). Business Research Methods. Oxford University Press George, M. L., Rowlands, D., Price, M., & Maxey, J. (2005). The Lean Six Sigma pocket toolbok: A quick reference guide to nearly 100 tools for improving process quality, speed, and complexity. 5th ed. McGraw-Hill.
Trygg hemgång i Ronneby: utvärdering och ekonomisk analys av ett tjänstekoncept, SKL/HCM, 2014.
Samordnad vård- och omsorgsplanering. Regionala och nationella styrprogram. Västra Götaland www.vgregionen.se/SVPL
Svensk författningssamling 1982:763. Hälso- och sjukvårdslag (1982:763 3f §).
Svensk författningssamling 1990:1404. Lag om kommunernas betalningsansvar för viss hälso- och sjukvård SFS 1990:1404 ändrad SFS 2003:193, SFS 2010:247.
Socialstyrelsen 2005, Socialstyrelsens föreskrifter om samverkan vid in- och utskrivning av patient i sluten vård SOSFS 2005:27 .
Statens offentliga utredningar, Trygg och effektiv utskrivning från slutenvården. Betänkande utredning om betalningsansvarslagen. Stockholm 2015. (SOU 2015:20).
Sveriges läkarförbund 2014 Rapport: Utskrivningsklara patienter 2014.
Ulin K. Person-centred care – An approach that improves the discharge process Eur J Cardiovasc Nurs 1474515115569945,first published on February 3, 2015.
PP - Peter Hammersberg (2015), Session1, Introduction to Lean Six Sigma
PP - Peter Hammersberg (2015) - BB15.4.1, Problem characterization and p-map.
www.vgregion.se/SVP
22
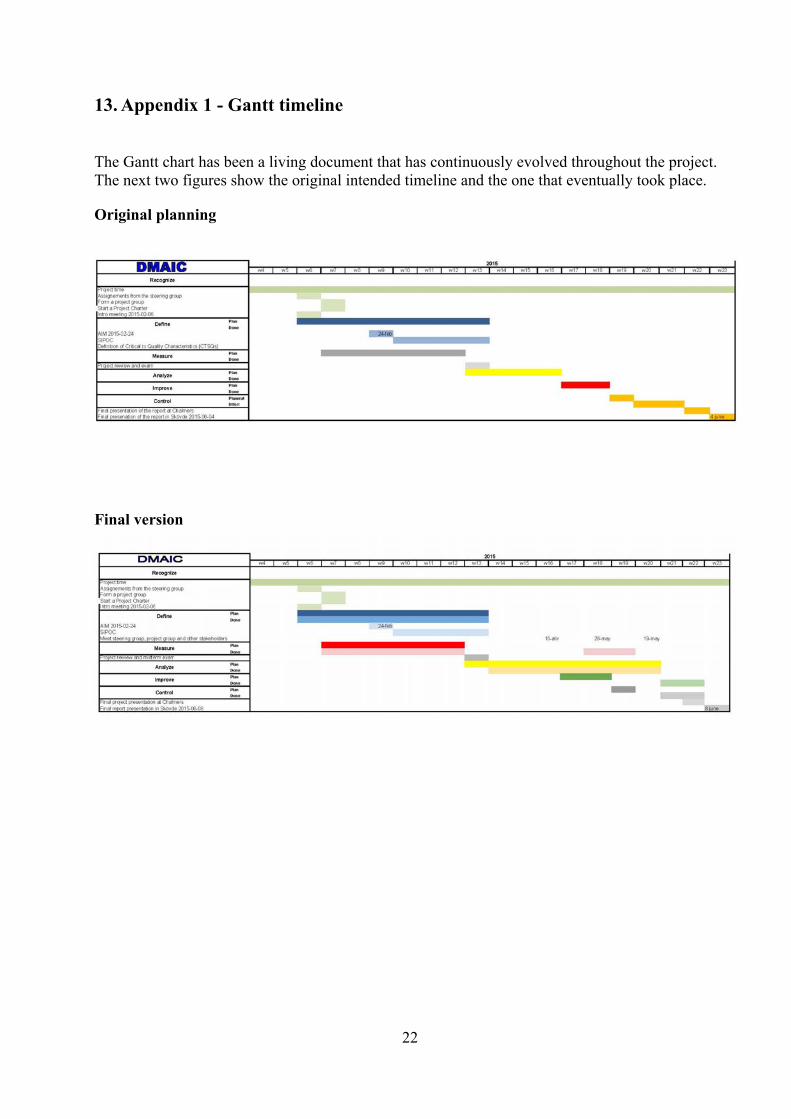
13. Appendix 1 - Gantt timeline
The Gantt chart has been a living document that has continuously evolved throughout the project. The next two figures show the original intended timeline and the one that eventually took place.
Original planning
Final version
23
14. Appendix 2 - SIPOC
24
15. Appendix 3 - Improved SIPOC and process map for Ward 73

25
Element Description
1. Delivery affected A short description of what is affected
2. Benefit to customersDefine internal and external customers (most
critical) and their requirements
3. Benefit to the businessDescribe the expected improvement in
business performance
Actual value (baseline)
Realistic goal by project end date
Best case goal
1-3 days
Visualization of the variation, its reasons
and its relation to municipalities and
hospitals.
Not identified
5. Impacted processThe specific processes involved in the project
where changes can be implemented
6. Team members Names of the participants in the project
(area of competence)
7. Other people involvedList technical experts and other people who
will be part of the team (area of competence)
8. Project delimitations What will be excluded from the project
9. Required support Support in terms of resources (human and
financial) required for implementing changes
10.Project summary A short description of the project
The organisation of Vårdsamverkan.The SVPL-group in Skaraborg.
The study reported a series of different causes for these delays; most significantly those concerning the availability of short-term
accommodation at the municipalities (korttidsboende ), a delayed planning of the discharge process at the hospital, and the disparate
understanding of the discharge process by the different organizations involved in it
A increased understanding of the reason why patients who are ready to be discharged are still staying at the hospital.
4. Measure to improve
Ingela Morgan, Nurse ward 73-74Peter Wiman, Siemens
Patients from the Psychiatric ward and children.
The coordinated discharge process
Margareta Liljegren, Manager of the Discharge NursesAnna Joelsson, Social Assistance Officer, Skövde municipality
Sandra Carlqvist, Discharge Nurse, SkaSLouise Samuelsson, Manager of the Social Assistance Office, SkaS
Marijana Psag, Nurse, Vara municipalityErik Backhaus, Medical Doctor, SkaS
Cost savings, better quality and higher patient safety.
Define the baselines, your realistic goals for the project and the best case targets for
improvement.
Charter
A reduced waiting time for the patient at the Hospital once they are ready to be discharged.
Executive Lars Johansson Senior Deployment Champion
Deployment ChampionPia Jonsson Axelsson
Mia GustavssonProject Champion Svante Lifvergren
Master Black Belt Peter Hammersberg Finance Champion
IT ChampionCatarina Karlberg
RegionkanslietHR Champion
Responsible Black Belt Louise Axelsson
Víctor Romera de la FuenteJeanette Andersson
Telephone/e-mail 073-4618045
Sponsor & process owner
Vårdsamverkan Skaraborg Site or location Skövde
Project Start Date 20/01/2015 Project completion Date 15/06/2008
Expected impact level
Survey of the number of “utskrivningsklara” days for patients in hospital and the
reason.
Expected financial impact (savings/revenues)
Not applicable
16. Appendix 4 - Project Charter
DEFINE phase completion date 27/03/2015 MEASURE phase completion date 11/05/2015
ANALYZE phase completion date 17/05/2015 IMPROVE phase completion date 30/05/2015
CONTROL phase completion date 30/05/2015 PROJECT results presentation date 08/06/2015
Project Title Improving the discharge process in hospitals by reducing the number of utskrivningsklara dagar Unit Department: Skaraborgs Sjukhus, Skövde and Vara Municipalities