improving mental health in dorset - … · improving mental health in dorset a public health...
TRANSCRIPT
Improving Mental Health in Dorset
A public health approach
Wessex CPD
29 November 2013
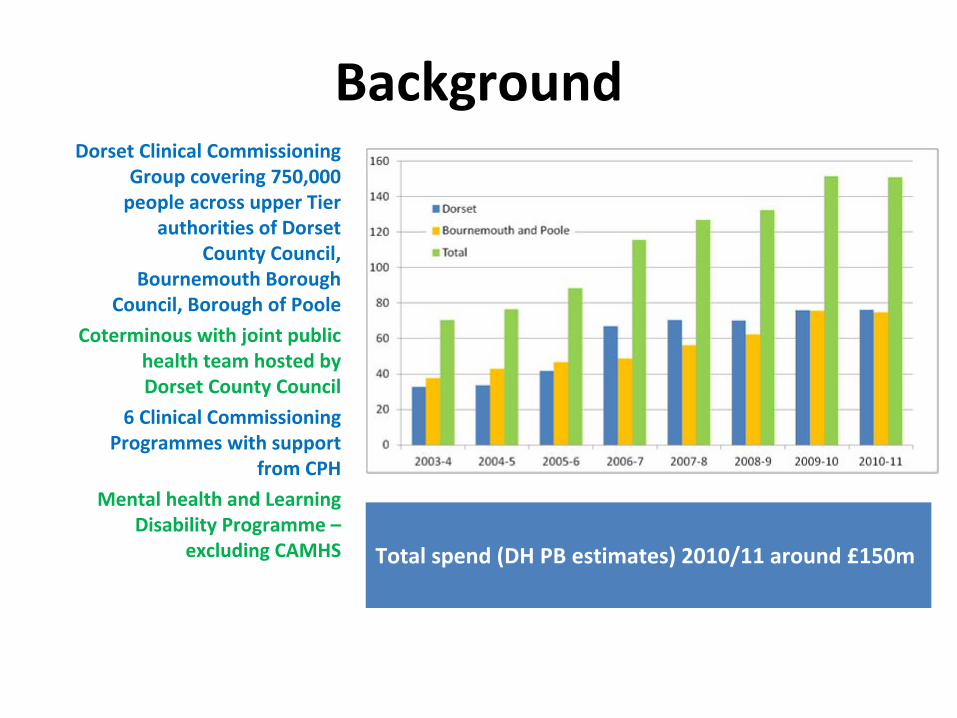
BackgroundDorset Clinical Commissioning
Group covering 750,000
people across upper Tier
authorities of Dorset
County Council,
Bournemouth Borough
Council, Borough of Poole
Coterminous with joint public
health team hosted by
Dorset County Council
6 Clinical Commissioning
Programmes with support
from CPH
Mental health and Learning
Disability Programme –
excluding CAMHS Total spend (DH PB estimates) 2010/11 around £150m

Understanding needs
• Pan‐Dorset Joint Strategic Needs Assessment 2012
• Wide variations in crude admissions to MH services across
localities –
double between East Dorset and Weymouth
• Wide variations in prevalence of SMI as measured by registers
• Access to IAPT very different across Dorset with large waiting
times in the West
• BUT ... No real idea what the commissioners were buying for
£150m a year ... Or why patterns of service use vary so much

Dorset’s public health approach
• Improve equity in use of services– Esp. IAPT and earlier recognition in primary care
• Understand and tackle inequalities –
including those related to mental health
• Improve effectiveness and efficiency through mapping of resource allocation in MH
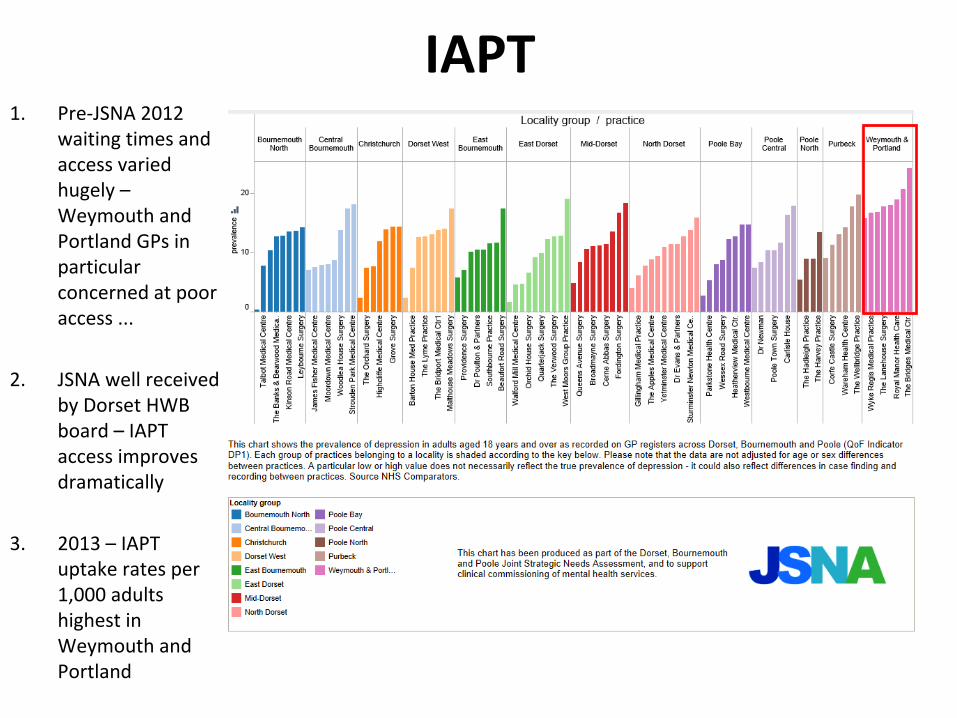
IAPT1.
Pre‐JSNA 2012
waiting times and
access varied
hugely –
Weymouth and
Portland GPs in
particular
concerned at poor
access ...
2.
JSNA well received
by Dorset HWB
board – IAPT
access improves
dramatically
3.
2013 – IAPT
uptake rates per
1,000 adults
highest in
Weymouth and
Portland

Inequalities
• Health theme group – meets 6 times per year
• Over‐arching target to close gap in life expectancy from 10.3 years (M) to
below average for England
• Stakeholder from providers, GPs, housing, Members, early years – meet in a
select committee style to challenge delivery

Why mental health?
• Boscombe
West had highest under 65 mortality rate of all wards – twice
rate of the Town
London Health Observatory
gap tools used to produce
scarf charts show suicide
and injury undetermined
plus cirrhosis of the liver
among top five causes of
death contributing to the
gap in life expectancy ...
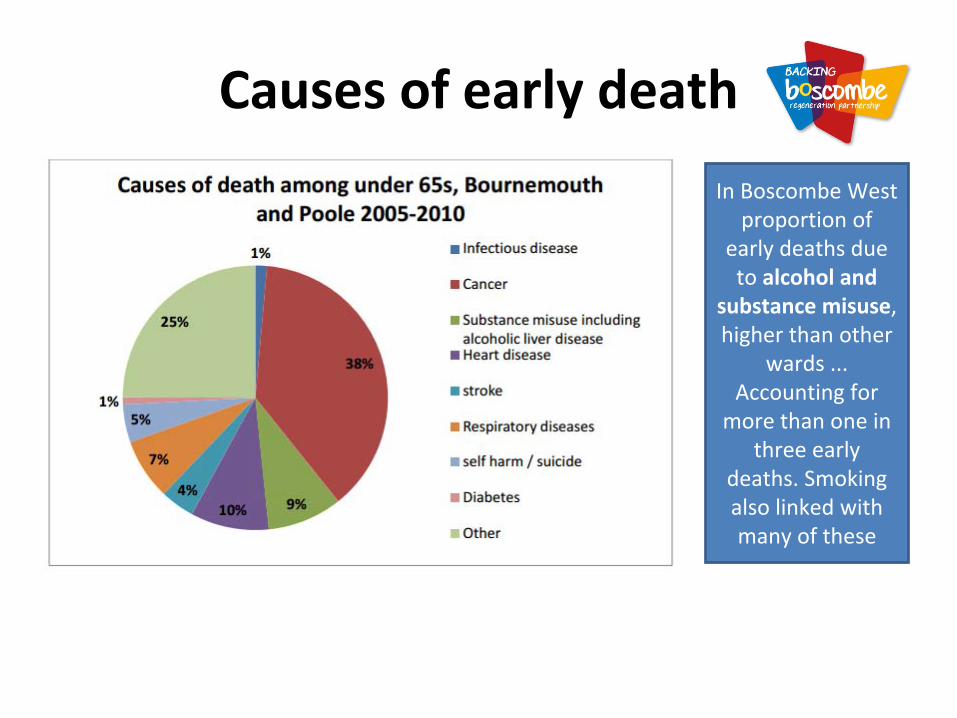
Causes of early death
In Boscombe
West
proportion of
early deaths due
to alcohol and
substance misuse,
higher than other
wards ...
Accounting for
more than one in
three early
deaths. Smoking
also linked with
many of these

SMI prevalence highest
Excess deaths in mental health service users: audit results in 2011/12
• Overall death rate is 3.6 times higher among MH service users c.f.
Population• Death rate from mental and behavioural disorders 12 x higher• BUT – also increased risk of death from:
– Respiratory disease (4‐fold increase)– Ischaemic
heart disease (2.5‐
fold increase)– Digestive system inc. Liver disease (4‐fold increase)
• These are lifestyle
related diseases
• Bournemouth UA has second highest
excess under 75 mortality
rate among adults with SMI among 7 comparator UAs
Source: Mental Health Bulletin: Sixth report from Mental Health Minimum Dataset returns – England 2011/12, initial national figures

What next?• Tackle lifestyle issues among people on SMI registers (see PH15 – could
we audit whether people on SMI registers are also being managed for CVD
risks if appropriate –
linking secondary MH checks with NHS Healthcheck• Offer NHS Healthcheck
preferentially to people on SMI registers if not
already on a CVD register
• Audit take up of IAPT service by small area and judge whether this
matches need –
completed – no concerns over access in Boscombe• Change lifestyle services for people with mental health issues –
reasonable adjustments – what is the evidence base for this
• Public mental health interventions – e.g. Campaign Against Living
Miserably
• Suicide awareness training for primary care professionals – jointly with
social care and voluntary sector workers in Boscombe
–
currently being
considered with CCG locality (ASSIST – see Knapp et al.)

Priorities for public health in Bournemouth
Public health induction to Bournemouth Borough
Council 9 April 2013
7 stages of PBMA
• Aim and scope of exercise
• Compile a programme budget map (activity, expenditure)
• Form marginal analysis advisory panel with stakeholders
• Determine local criteria for decision making
• Identify options– Growth areas
– Resource release – through efficiency or stopping or scaling back service
• Recommendations– Growth areas– Moving resources released from productivity
– Trade offs between services if relative value is higher
• Sense checking / validity

Priorities for public health in Bournemouth
Public health induction to Bournemouth Borough
Council 9 April 2013
Stage one: aim and scope
• Agreed at July 2013 meeting
• Use spend in financial year 13/14, linked to PbR
clusters
• Consider NHS, LA and other spend where possible
• Agree service descriptions and map £ activity by service and
sector
• Reconcile with provider view
• Based on persons, not episodes of care, and identify
proportions treated / untreated (penetration)
• Assess interventions, outcomes and impact in QALYs
where
possible
• Validate and share with stakeholders at each stage

Priorities for public health in Bournemouth
Public health induction to Bournemouth Borough
Council 9 April 2013
In my simple mind ... Service
area
Numbers
accessing
Combined
spend
Interventions Outcomes
Community
Primary care
Intermediate
Secondary

Then develop pathways for PbR
main clusters
Recovery
Reality ...
• Steering group and method agreed –
July
• DHUFT found in breach of FT license
– CEO and chair removed
Taken 5 months to locate right information and compile
initial mapping of provider services ... None reflect
pathways!!

Best guess to date ...

Next steps
• Define patient journeys for typical PbR clusters
• Re‐organise services along these pathways• Add activity / cohorts to the map
• Work with clinicians to agree outcomes /goals
• Assess effectiveness and value• Convene marginal analysis group ...