immediate dental implant placement: technique, part 1 · pdf filecontinuing education...
TRANSCRIPT
Continuing Education
Immediate Dental ImplantPlacement: Technique, Part 1
Authored by Gary Greenstein, DDS, MS, and John Cavallaro, DDS
Course Number: 169
Upon successful completion of this CE activity 2 CE credit hours may be awarded
A Peer-Reviewed CE Activity by
Opinions expressed by CE authors are their own and may not reflect those of Dentistry Today. Mention of
specific product names does not infer endorsement by Dentistry Today. Information contained in CE articles and
courses is not a substitute for sound clinical judgment and accepted standards of care. Participants are urged to
contact their state dental boards for continuing education requirements.
Dentistry Today, Inc, is an ADA CERP Recognized Provider. ADA CERP isa service of the American Dental Association to assist dental professionalsin indentifying quality providers of continuing dental education. ADA CERPdoes not approve or endorse individual courses or instructors, nor does itimply acceptance of credit hours by boards of dentistry. Concerns orcomplaints about a CE provider may be directed to the provider or to ADA CERP at ada.org/goto/cerp.
Approved PACE Program ProviderFAGD/MAGD Credit Approval doesnot imply acceptance by a state orprovincial board of dentistry orAGD endorsement. June 1, 2012 toMay 31, 2015 AGD PACE approvalnumber: 309062

LEARNING OBJECTIVESAfter participating in this CE activity, the individual will learn: • Indications and contraindications for immediate implantplacement.
• Practical suggestions for immediate implant placement.
ABOUT THE AUTHORSDr. Greenstein is a professor in thedepart ment of periodontology at theCollege of Dental Med icine, ColumbiaUniversity, New York, NY. He maintains aprivate practice in surgical implantologyand periodontics in Freehold, NJ. He can
be reached at [email protected].
Disclosure: Dr. Greenstein reports no disclosures.
Dr. Cavallaro is a clinical associateprofessor of the implant fellowshipprogram and prosthodontics of ColumbiaUniversity, NY, and is in private practice ofsurgical implantology and prosthodonticsin Brooklyn, NY. He can be reached at
Disclosure: Dr. Cavallaro reports no disclosures.
INTRODUCTIONImmediate dental implant placement refers to insertion of animplant directly after a tooth is extracted, whereas de layedpositioning occurs at some later time. The concept of placingimplants immediately after tooth removal was introduced inthe 1970s.1 Currently, widespread acceptance of thisprocedure is due to its high survival rate.2,3 However,placement of immediate implants in different regions of themouth and under diverse conditions can be challenging. This2-part article addresses issues relevant to immediate
implants (part 1), and provides practical clinical informationfor positioning immediate implants in different sections of themouth (part 2).
BACKGROUND INFORMATION Classification of Extraction Sockets The following classification system identifies clinicalscenarios related to immediate implant placement4
(classification of socket type is dependent on informationob tained with a periodontal probe, visual, and radiographicassessments):
l Type I: The bony socket is intact, and the soft-tissueform is undisturbed.
l Type II: The bony socket is intact in the coronal aspectof the socket, but a fenestration is present in the apicalarea. The soft tissue remains intact and undisturbed.
l Type III: Bone loss is present in the coronal aspect of thesocket. The soft tissue remains intact and undisturbed.
l Type IV: Bony defects exist in conjunction with soft-tissue deformity.
Indications and Contraindications for ImmediateImplant PlacementThere are a series of decisions that need to be made prior toproceeding with immediate implant placement. First, thesocket type needs to be assessed and categorized as shownabove. Type I and usually Type II (depending on extent of thedefect) sockets are candidates for immediate implantplacement and require preservation of adjacent tissuesaround an immediate implant. Types III and IV socketsfrequently warrant de layed placement and soft- or hard-tissue augmentation prior to implant insertion. This papermainly focuses on surgical management of Type I cases.
Management of cases (immediate versus delayed implantplacement) requires both a surgical and prostheticperspective. Prior to initiating therapy, a patient should be de -fined as having a high or low risk of attaining an excellentesthetic result, especially in the esthetic zone. Table 1 outlinescritical determinants for evaluating patients.5
The main advantages of immediate implant placementare that they save time and there are fewer patient visits.There are numerous indications for tooth replacement withan immediate implant when an adequate amount of bone
Continuing Education
1
Immediate Dental ImplantPlacement: Technique, Part 1Effective Date: 1/1/2014 Expiration Date: 1/1/2017

and soft tissue are available to support it: deciduoustooth, en do don tic failure, caries, deep probing depthsdue to periodontitis, vertical root fracture, andidiopathic root resorption. Con tra dictions to in sertingimmediate implants include inadequate height orwidth of bone, lack of soft tissue, ad verse location ofnerves, proximity of ad jacent teeth, failure to achieveprimary stability, and inability to attain a res torativelyreasonable position, an gulation or sink depth of theimplant.
Immediate Implant Survival Rates Implants immediately placed into fresh extractionsockets and healed ridges have similar survival rates(97.3% to 99%).2,3 Furthermore, im mediate implantsinserted into in fected sites6,7 or locations withperiapical lesions have comparable survival rates toimplants placed into healthy ridges.8 However, thesestudies did not delineate the amount of bone grafting thatwas performed or extent of infections that were present.
Healing Phase and Bone LossTypical Healing of an Extraction Socket—Six months aftertooth removal, which includes flap elevation, the extractionsockets manifest a mean 1.24 mm vertical bone loss (range0.9 to 3.6 mm). Usually there is approximately 3.79 mmhorizontal bone decrease (range 2.46 to 4.56 mm).9
In contrast, extractions of teeth with no flap demonstrate areduced amount of horizontal10-12 and vertical bone loss.13-16
However, others suggest there is no difference in the amount ofvertical osseous resorption if procedures are done flapless orwith a flap when placing implants, but these studies did notnecessarily address immediate im plants.17-21 Bone reductionafter flapless extractions may be due to elimination of the bloodsupply from the periodontal ligament (PDL). Differences inosseous resorption rates in the above studies may also beattributed to buccal plate thickness (thicker plates resorb less).22
Nevertheless, especially in the esthetic zone, it is suggested thatimmediate implants be placed without elevating a buccal flap topreserve bone and avoid soft-tissue recession.Socket Healing After Immediate Placement—Many
studies verified that immediate implant placement isaccompanied by bone loss. This was corroborated in
dogs23-25 and human clinical trials.26-27 Commonly, there isa reduction of vertical bone height and even a greateramount of horizontal bone loss.23,27 The quantity of boneresorption is larger on the buccal than the lingual side of anim plant, since the buccal plate is usually thinner.28,29 Thedegree of bone re duction is related to numerous factors(Table 2).12-15,21,30-37
Immediate Implants Help Preserve Vertical BoneHeight—Among patients who receive immediate implants,the amount of bone resorption during the first year after toothextraction38-41 ap pears to be less than when teeth areremoved and no implants are placed.42-44 This is based oninvestigations that did not directly compare patients that hadboth therapies. For instance, 1.0 to 1.5 mm vertical boneheight is usually lost after an extraction, when a flap iselevated42-44; however, vertical bone loss noted the first yearafter immediate placement was 0.6 mm with Tioblastfixtures,38 0.4 mm for Astra Tech (DENTSPLY Im plants),39
0.37 for Nano Tite Prevail (Biomet 3i),40 and 1.1 mm of boneloss occurred after nonocclusal and early loading withOsseotite (Biomet 3i) implants.41
Other data also support the contention that immediatelyplaced im plants preserve bone. When the amount ofosseous resorption that occurs after im mediate and delayedimplant placement is compared, the data demonstrate thatthere are no differences in the quantity of bone lost.45-47
Continuing Education
2
Immediate Dental Implant Placement: Technique, Part 1
Table 1. Diagnostic Assessment in Determining High and Low Risk of Attaining an Excellent Esthetic Result5
Clinical Feature Low Risk High Risk
1. Level of the free Coronal to cemento- Even or apical to CEJgingival margina enamel junction (CEJ)
2. Gingival formb Flat scalloped High scalloped
3. Biotypec Thick Thin
4. Tooth shaped Square Triangular
5. Position of High crest Low crestosseous creste
6. Facial lingual Lingual Facialplane of toothf
aA coronal free gingival margin provides a margin of error for some minor recession that may occur.bFlap scalloped gingival contours recede less than high scalloped contours.cThin biotype will manifest more recession than thick biotypes.dTriangular teeth manifest more recession than square teeth.eIf the bone crest is > 3 to 4 mm apical to the free gingival margin perform delayed implant placement.fTeeth in lingual position have thicker bone and thicker gingiva, if prominent buccally the bone isthinner and recession occurs more often.
However, these investigations made evaluations with respectto the amount of bone reduction several months afterimmediate or delayed placement. The baseline for evaluatingthe preliminary bone height was as sessed on the day ofimplant insertion. Researchers did not consider that withdelayed placement, bone loss occurred postextraction andbefore delayed insertion of an im plant. Therefore, it can bededuced that de layed placement resulted in a larger degreeof bone loss than immediate implant insertion.
PRACTICAL SUGGESTIONS FOR IMMEDIATEIMPLANT PLACEMENT Atraumatic Tooth Removal Prior to Implant InsertionTeeth need to be removed atraumatically to preserve themaximum amount of bone before immediate implantplacement. The clinical situation will dictate if the toothshould be removed flaplessly (eg, if it is broken subgingi-
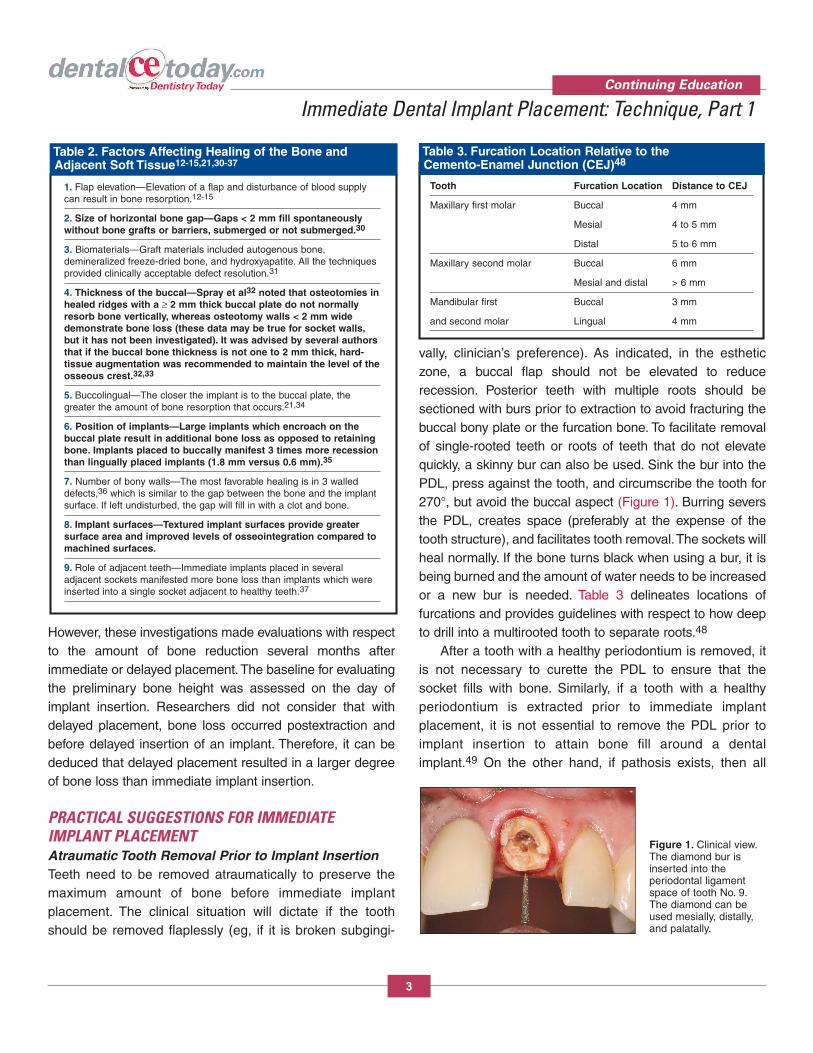
vally, clinician’s preference). As indicated, in the estheticzone, a buccal flap should not be elevated to reducerecession. Posterior teeth with multiple roots should besectioned with burs prior to extraction to avoid fracturing thebuccal bony plate or the furcation bone. To facilitate removalof single-rooted teeth or roots of teeth that do not elevatequickly, a skinny bur can also be used. Sink the bur into thePDL, press against the tooth, and circumscribe the tooth for270°, but avoid the buccal aspect (Figure 1). Burring seversthe PDL, creates space (preferably at the expense of thetooth structure), and facilitates tooth removal. The sockets willheal normally. If the bone turns black when using a bur, it isbeing burned and the amount of water needs to be increasedor a new bur is needed. Table 3 delineates locations offurcations and provides guidelines with respect to how deepto drill into a multirooted tooth to separate roots.48
After a tooth with a healthy periodontium is removed, itis not necessary to curette the PDL to ensure that thesocket fills with bone. Similarly, if a tooth with a healthyperiodontium is extracted prior to immediate implantplacement, it is not essential to remove the PDL prior toimplant insertion to attain bone fill around a dentalimplant.49 On the other hand, if pathosis exists, then all
Continuing Education
3
Immediate Dental Implant Placement: Technique, Part 1
Table 2. Factors Affecting Healing of the Bone and Adjacent Soft Tissue12-15,21,30-37
1. Flap elevation—Elevation of a flap and disturbance of blood supplycan result in bone resorption.12-15
2. Size of horizontal bone gap—Gaps < 2 mm fill spontaneously without bone grafts or barriers, submerged or not submerged.30
3. Biomaterials—Graft materials included autogenous bone, demineralized freeze-dried bone, and hydroxyapatite. All the techniquesprovided clinically acceptable defect resolution.31
4. Thickness of the buccal—Spray et al32 noted that osteotomies inhealed ridges with a ≥ 2 mm thick buccal plate do not normallyresorb bone vertically, whereas osteotomy walls < 2 mm widedemonstrate bone loss (these data may be true for socket walls,but it has not been investigated). It was advised by several authorsthat if the buccal bone thickness is not one to 2 mm thick, hard-tissue augmentation was recommended to maintain the level of theosseous crest.32,33
5. Buccolingual—The closer the implant is to the buccal plate, thegreater the amount of bone resorption that occurs.21,34
6. Position of implants—Large implants which encroach on thebuccal plate result in additional bone loss as opposed to retainingbone. Implants placed to buccally manifest 3 times more recessionthan lingually placed implants (1.8 mm versus 0.6 mm).35
7. Number of bony walls—The most favorable healing is in 3 walleddefects,36 which is similar to the gap between the bone and the implantsurface. If left undisturbed, the gap will fill in with a clot and bone.
8. Implant surfaces—Textured implant surfaces provide greatersurface area and improved levels of osseointegration compared tomachined surfaces.
9. Role of adjacent teeth—Immediate implants placed in several adjacent sockets manifested more bone loss than implants which wereinserted into a single socket adjacent to healthy teeth.37
Table 3. Furcation Location Relative to the Cemento-Enamel Junction (CEJ)48
Tooth Furcation Location Distance to CEJ
Maxillary first molar Buccal 4 mm
Mesial 4 to 5 mm
Distal 5 to 6 mm
Maxillary second molar Buccal 6 mm
Mesial and distal > 6 mm
Mandibular first Buccal 3 mm
and second molar Lingual 4 mm
Figure 1. Clinical view.The diamond bur isinserted into theperiodontal ligamentspace of tooth No. 9.The diamond can beused mesially, distally,and palatally.

granulomatous tissue should be removed. Atpresent, no studies have compared the healingresponse of bone around immediately placedimplants with respect to bone fill related to theab sence or presence of the PDL.
Width and Length of an Implant to AttainPrimary StabilityDepending on the size of the extracted toothand the implant to be placed, somewherealong the root surface, the implant willusually exceed the diameter of the root andprovide mechanical retention of the implant.This retention and/or extension of theosteotomy and placement of the im plantbeyond the apex of the ex tracted tooth provideprimary im plant stability. It is advisable to place an implant aminimum of 3 to 5 mm into bone to attain primary stability ifmechanical retention cannot be achieved laterally (Figures2a and 2b). Occasionally, it is possible to place a taperedimplant into an extraction socket with minimal to noosteotomy preparation, thereby relying on the threads’engagement of the bone lateral to the socket walls.
Apicocoronal and Horizontal Placement of Immediate Dental ImplantsIn general, immediate implants should be placed one mmsubcrestally as viewed from the midpoint of the labial plateto account for vertical bone height resorption (the implantoften will be deeper interproximally).50,51 If the buccal orlingual plates of bone are thin, the implants should be placed
more subcrestally, since there may be an increased amountof bone resorption. The amount of vertical bone loss can bedecreased with platform switching. Atieh et al52 reported thatbone loss with versus without platform switching after im mediate implant placement was re spectively, 0.05 mm to0.99 mm versus 0.19 mm to 1.67 mm.
As a general rule, platforms of immediate implantsshould be placed 2 to 3 mm below the gingival margin(Figures 3a to 3e).53 This may or may not correlate withbeing 2 to 3 mm below the cemento-enamel junction (CEJ)of the adjacent teeth. Therefore, if recession occurred onthe adjoining teeth, using the CEJ as a guide will provide apoor esthetic result.
Horizontally, implants should not touch the buccal plate ofbone29 because there is a horizontal zone of influence, and if
Continuing Education
4
Immediate Dental Implant Placement: Technique, Part 1
Figure 2a. Radiograph of structurally unsound tooth No. 4. The tooth reaches the sinus.Figure 2b. Radiograph demonstrating insertion of an implant with a diameter wider than thesocket. In addition, aggressive apical threads engage the bone lateral to the socket walls.
a b
Figure 3a. Radiograph of structurally unsound toothNo. 12 to be extracted.
Figure 3b. Clinical view ofan immediately placedimplant at site No. 12. Thesink depth is approximately4 mm apical to the freegingival margin.
Figure 3c. Radiographicview of implant at site No. 12.
Figure 3d. Intraoral clinical view ofthe definitive restoration at insertion atsite No. 12.
Figure 3e.Radiograph of thedefinitive restorationat site No. 12.
a b c d e

an implant encroaches upon the buccal plate of bone, it willinduce resorption (Figure 4).54 This is particularly true in theesthetic zone. In this regard, when large implants are placedin molar sites and engage the buccal or lingual plate of bone,they may induce some bone loss.
Maxillary Canine TiltAlways check the radiograph to as sess angulations ofadjacent teeth and possible dilacerations of roots beforedrilling an osteotomy. This is particularly critical when placinga maxillary first premolar implant, because maxillary ca ninesare often angled 11° distally and the root curves distally 32%
of the time.55 When necessary, place the im plant in the firstbicuspid alveolus parallel to the canine, not parallel to thesecond premolar. Minor parallelism discrepancies can be
Continuing Education
5
Immediate Dental Implant Placement: Technique, Part 1
Table 4. Possible Therapies Available to Treat the Buccal Gap After Immediate Implant Placement: With and Without Flap Elevation56
A. WITH FLAP ELEVATION ADVANTAGE DISADVANTAGE
1. NO ADDITIONAL TREATMENT (NO BONE GRAFT OR BARRIER USED)a. Flap placed over the defect Covers defect This may require flap advancement
Increased morbidity (edema and ecchymosis)Soft tissue may invade gap
b. Flap positioned at bone crest leaving the gap exposed Easier Plaque and food may get trapped in voidif clot is not retained
2. BONE GRAFT PLACED INTO THE DEFECT WITH OR WITHOUT GROWTH FACTORSa. Flap placed over the defect Covers defect This may require flap advancement
Increased morbidity (edema and ecchymosis)Soft tissue may invade bone graft
b. Flap positioned at bone crest, leaving the gap exposed Easier Plaque and food may get trapped in voidif clot is not retained
3. BARRIER PLACED OVER DEFECTa. Flap advancement is usually necessary to attain primary closure Covers barrier Increased morbidity (edema and ecchymosis)
b. No flap advancement and use of nonresorbable Easier Nonresorbable barrier-exposure/infectionor resorbable barrier or connective tissue graft Resorbable barrier-rapid dissolution in mouth
4. BARRIER PLACED OVER BONE GRAFTa. Flap advancement is usually necessary to attain primary closure Covers barrier Increased morbidity (edema and ecchymosis)
Nonresorbable barrier-exposure/infection
b. No flap advancement and use of nonresorbable or resorbable barrier Easier Nonresorbable barrier-exposure/infectionor connective tissue graft Resorbable barrier-rapid dissolution in mouth
5. TEMPORIZATION OF IMPLANT AND ABUTMENT Supports Additional work at time of surgerysoft tissue Sufficient primary stability required
Reasonable restorative position required
B. NO FLAP ELEVATION (FLAPLESS IMPLANT INSERTION) ADVANTAGE DISADVANTAGE
1. THE GAP IS LEFT OPEN WITH NO ADDITIONAL THERAPY Easier Plaque and food may get trapped in voidif clot is not retained
2. BONE IS PLACED WITHIN THE GAP Bone particles may be displaced
3. TEMPORIZATION OF IMPLANT AND ABUTMENT WITH EITHER OF THE ABOVE Supports soft tissue Additional work at time of surgery
Figure 4. Intraoralocclusal view of an immediately placedimplant at site No. 5. Itis positioned to remaindistant from the labialplate of bone. Primarystability is achievedapically andinterproximally.

reconciled at the abutment level by utilizing angulatedabutments (Figures 5a to 5d).
Flap Versus Flapless Implant InsertionA clinician has multiple therapeutic options regardingimmediate im plant placement: flap versus flapless surgery,bone grafting, and barrier utilization (Table 4).56 Commentsin Table 4 relate to circumstances where the bony plate isundamaged and does not need a re generative procedure torestore bone contour. If implant insertion is performedflaplessly, a cover screw or short healing abutment can beplaced and the implant can be submerged, but this usuallyentails flap advancement if only one tooth was removed.Some times submergence is desirable if the implant isplaced under a provisional partial or full denture, or if theimplant was a spinner, or if it was inserted in soft qualitybone and it is questionable how well initial stability wouldwithstand occlusal stresses. Alternately, a healing, interim,or definitive abutment can be placed with or without aprovisional crown that is not in occlusal function. Recentdata indicate that when an immediate implant was placedflaplessly in the esthetic zone in conjunction with anabutment, a provisional crown, and a bone graft placed inthe buccal gap that extended coronally from the crest of thebone to the gingival margin (referred to as dual-zonetherapy), the amount of bone loss and recession wereminimal.57,58
CONCLUDING REMARKS Placement of immediate implants is a predictableprocedure and attention to detail is essential to ensuresuccess when placing these implants. Type 1 and usuallyType 2 sockets are candidates for immediate implantplacement and require preservation of ad jacent tissuesaround the implant. Part 1 of this article has discussed in dications/contraindications for im mediate implant place-ment, healing phase and bone loss after extraction, andpractical suggestions for immediate implant placement. Part2 will pro vide practical information for positioning immediateimplants in different sections of the mouth.
Continuing Education
6
Immediate Dental Implant Placement: Technique, Part 1
Figure 5a. Radiograph after extraction of the maxillary left firstpremolar (No. 12). Note the distaltilt of the adjacent canine tooth root.
a
Figure 5b. Radiograph of immediately placed postplacement of the implant into theextraction socket of No. 12. Theimplant has been placed to avoidencroachment on the canine root.
b
Figure 5c. Clinical view of implantlevel transfer coping demonstratingthe need to use an angled abutment to correct implant trajectory at site No. 12.
c
Figure 5d. Clinical view of an angulated abutment torqued toplace at site No. 12. A line of drawhas been created that enables therestoration to be seated.
d

REFERENCES1. Schulte W, Kleineikenscheidt H, Lindner K, et al. The
Tübingen immediate implant in clinical studies [inGerman]. Dtsch Zahnarztl Z. 1978;33:348-359.
2. Lang NP, Pun L, Lau KY, et al. A systematic review onsurvival and success rates of implants placedimmediately into fresh extraction sockets after at least1 year. Clin Oral Implants Res. 2012;23(suppl 5):39-66.
3. Ortega-Martínez J, Pérez-Pascual T, Mareque-Bueno S,et al. Immediate implants following tooth extraction. Asystematic review. Med Oral Patol Oral Cir Bucal.2012;17:e251-e261.
4. Evian CI, Waasdorp JA. Evaluating extraction sockets inthe esthetic zone for immediate implant placement.Compend Contin Educ Dent. 2011;32:e58-e65.
5. Kois JC. Predictable single-tooth peri-implant esthetics:five diagnostic keys. Compend Contin Educ Dent.2004;25:895-907.
6. Waasdorp JA, Evian CI, Mandracchia M. Immediateplacement of implants into infected sites: a systematicreview of the literature. J Periodontol. 2010;81:801-808.
7. Crespi R, Capparè P, Gherlone E. Immediate loading ofdental implants placed in periodontally infected and non-infected sites: a 4-year follow-up clinical study. JPeriodontol. 2010;81:1140-1146.
8. Crespi R, Capparè P, Gherlone E. Fresh-socket implantsin periapical infected sites in humans. J Periodontol.2010;81:378-383.
9. Tan WL, Wong TL, Wong MC, et al. A systematic reviewof post-extractional alveolar hard and soft tissuedimensional changes in humans. Clin Oral Implants Res.2012;23(suppl 5):1-21.
10. Vera C, De Kok IJ, Chen W, et al. Evaluation of post-implant buccal bone resorption using cone beamcomputed tomography: a clinical pilot study. Int J OralMaxillofac Implants. 2012;27:1249-1257.
11. Degidi M, Daprile G, Nardi D, et al. Buccal bone plate inimmediately placed and restored implant with Bio-Osscollagen graft: a 1-year follow-up study. Clin OralImplants Res. 2012 Aug 13. [Epub ahead of print]
12. Brownfield LA, Weltman RL. Ridge preservation with orwithout an osteoinductive allograft: a clinical,radiographic, micro-computed tomography, and histologicstudy evaluating dimensional changes and new boneformation of the alveolar ridge. J Periodontol.2012;83:581-589.
13. Job S, Bhat V, Naidu EM. In vivo evaluation of crestalbone heights following implant placement with ‘flapless’and ‘with-flap’ techniques in sites of immediately loadedimplants. Indian J Dent Res. 2008;19:320-325.
14. Fickl S, Zuhr O, Wachtel H, et al. Tissue alterations aftertooth extraction with and without surgical trauma: avolumetric study in the beagle dog. J Clin Periodontol.2008;35:356-363.
15. Barros RRM, Novaes AB Jr, Papalexiou V. Buccal boneremodeling after immediate implantation with a flap orflapless approach: a pilot study in dogs. Titanium.2009;1:45-51.
16. Blanco J, Nuñez V, Aracil L, et al. Ridge alterations followingimmediate implant placement in the dog: flap versus flaplesssurgery. J Clin Periodontol. 2008;35:640-648.
17. Maló P, Nobre M. Flap vs. flapless surgical techniques atimmediate implant function in predominantly soft bone forrehabilitation of partial edentulism: a prospective cohortstudy with follow-up of 1 year. Eur J Oral Implantol.2008;1:293-304.
18. De Bruyn H, Atashkadeh M, Cosyn J, et al. Clinicaloutcome and bone preservation of single TiUniteimplants installed with flapless or flap surgery. ClinImplant Dent Relat Res. 2011;13:175-183.
19. Caneva M, Botticelli D, Salata LA, et al. Flap vs. “flapless”surgical approach at immediate implants: ahistomorphometric study in dogs. Clin Oral Implants Res.2010;21:1314-1319.
20. Araújo MG, Lindhe J. Ridge alterations following toothextraction with and without flap elevation: anexperimental study in the dog. Clin Oral Im plants Res.2009;20:545-549.
21. Becker W, Wikesjö UM, Sennerby L, et al. Histologic eval-uation of implants following flapless and flapped surgery: astudy in canines. J Periodontol. 2006;77:1717-1722.
22. Ferrus J, Cecchinato D, Pjetursson EB, et al. Factorsinfluencing ridge alterations following immediate implantplacement into extraction sockets. Clin Oral ImplantsRes. 2010;21:22-29.
23. Araújo MG, Wennström JL, Lindhe J. Modeling of thebuccal and lingual bone walls of fresh extraction sitesfollowing implant installation. Clin Oral Implants Res.2006;17:606-614.
24. Vignoletti F, de Sanctis M, Berglundh T, et al. Earlyhealing of implants placed into fresh ex traction sockets:an experimental study in the beagle dog. II: ridgealterations. J Clin Periodontol. 2009;36:688-697.
25. De Santis E, Botticelli D, Pantani F, et al. Boneregeneration at implants placed into extraction sockets ofmaxillary incisors in dogs. Clin Oral Implants Res.2011;22:430-437.
26. Botticelli D, Berglundh T, Lindhe J. Hard-tissue alterationsfollowing immediate implant placement in extraction sites.J Clin Periodontol. 2004;31:820-828.
Continuing Education
7
Immediate Dental Implant Placement: Technique, Part 1

27. Sanz M, Cecchinato D, Ferrus J, et al. A prospective,randomized-controlled clinical trial to evaluate bonepreservation using implants with different geometryplaced into extraction sockets in the maxilla. Clin OralImplants Res. 2010;21:13-21.
28. Araújo MG, Lindhe J. Dimensional ridge alterationsfollowing tooth extraction. An experimental study in thedog. J Clin Periodontol. 2005;32:212-218.
29. Caneva M, Salata LA, de Souza SS, et al. Hard tissueformation adjacent to implants of various size andconfiguration immediately placed into extraction sockets:an experimental study in dogs. Clin Oral Implants Res.2010;21:885-890.
30. Paolantonio M, Dolci M, Scarano A, et al. Immediateimplantation in fresh extraction sockets. A controlledclinical and histological study in man. J Periodontol.2001;72:1560-1571.
31. Chen ST, Wilson TG Jr, Hämmerle CH. Immediate orearly placement of implants following tooth extraction:review of biologic basis, clinical procedures, andoutcomes. Int J Oral Maxillofac Implants.2004;19(suppl):12-25.
32. Spray JR, Black CG, Morris HF, et al. The influence ofbone thickness on facial marginal bone response: stage1 placement through stage 2 uncovering. AnnPeriodontol. 2000;5:119-128.
33. Juodzbalys G, Wang HL. Soft and hard tissueassessment of immediate implant placement: a caseseries. Clin Oral Implants Res. 2007;18:237-243.
34. Favero G, Botticelli D, Favero G, et al. Alveolar bony crestpreservation at implants installed immediately after toothextraction: an experimental study in the dog. Clin OralImplants Res. 2013;24:7-12.
35. Evans CD, Chen ST. Esthetic outcomes of immediateimplant placements. Clin Oral Implants Res. 2008;19:73-80.
36. Kim CS, Choi SH, Chai JK, et al. Periodontal repair insurgically created intrabony defects in dogs: influence ofthe number of bone walls on healing response. JPeriodontol. 2004;75:229-235.
37. Favero G, Lang NP, Favero G, et al. Role of teethadjacent to implants installed immediately into extractionsockets: an experimental study in the dog. Clin OralImplants Res. 2012;23:402-408.
38. Collaert B, De Bruyn H. Immediate functional loading ofTiOblast dental implants in full-arch edentulous maxillae:a 3-year prospective study. Clin Oral Implants Res.2008;19:1254-1260.
39. Norton MR. A short-term clinical evaluation ofimmediately restored maxillary TiOblast single-toothimplants. Int J Oral Maxillofac Implants. 2004;19:274-281.
40. Ostman PO, Wennerberg A, Albrektsson T. Immediateocclusal loading of NanoTite PREVAIL implants: aprospective 1-year clinical and radiographic study. ClinImplant Dent Relat Res. 2010;12:39-47.
41. Galli F, Capelli M, Zuffetti F, et al. Immediate non-occlusalvs. early loading of dental implants in partially edentulouspatients: a multicentre randomized clinical trial. Peri-implant bone and soft-tissue levels. Clin Oral ImplantsRes. 2008;19:546-552.
42. Lekovic V, Camargo PM, Klokkevold PR, et al. Preservationof alveolar bone in extraction sockets using bioabsorbablemembranes. J Periodontol. 1998;69:1044-1049.
43. Lekovic V, Kenney EB, Weinlaender M, et al. A boneregenerative approach to alveolar ridge maintenancefollowing tooth extraction. Report of 10 cases. JPeriodontol. 1997;68:563-570.
44. Camargo PM, Lekovic V, Weinlaender M, et al. Influenceof bioactive glass on changes in alveolar processdimensions after exodontia. Oral Surg Oral Med OralPathol Oral Radiol Endod. 2000;90:581-586.
45. Crespi R, Capparè P, Gherlone E, et al. Immediateocclusal loading of implants placed in fresh sockets aftertooth extraction. Int J Oral Maxillofac Implants.2007;22:955-962.
46. Liñares A, Mardas N, Dard M, et al. Effect of immediateor delayed loading following immediate placement ofimplants with a modified surface. Clin Oral Implants Res.2011;22:38-46.
47. Younis L, Taher A, Abu-Hassan MI, et al. Evaluation of bonehealing following immediate and delayed dental implantplacement. J Contemp Dent Pract. 2009;10:35-42.
48. Greenstein G, Caton J, Polson A. Trisection of maxillarymolars: a clinical technique. Compend Contin Educ Dent.1984;5:624-632.
49. Botticelli D, Berglundh T, Lindhe J. Resolution of bonedefects of varying dimension and configuration in themarginal portion of the peri-implant bone. Anexperimental study in the dog. J Clin Periodontol.2004;31:309-317.
50. Chen ST, Darby IB, Reynolds EC. A prospective clinicalstudy of non-submerged immediate implants: clinicaloutcomes and esthetic results. Clin Oral Implants Res.2007;18:552-562.
51. Araújo MG, Lindhe J. Dimensional ridge alterationsfollowing tooth extraction. An experimental study in thedog. J Clin Periodontol. 2005;32:212-218.
52. Atieh MA, Ibrahim HM, Atieh AH. Platform switching formarginal bone preservation around dental implants: asystematic review and meta-analysis. J Periodontol.2010;81:1350-1366.
Continuing Education
8
Immediate Dental Implant Placement: Technique, Part 1

53. Sorni-Bröker M, Peñarrocha-Diago M, Peñar rocha-DiagoM. Factors that influence the position of the peri-implantsoft tissues: a review. Med Oral Patol Oral Cir Bucal.2009;14:e475-e479.
54. Vela X, Méndez V, Rodríguez X, et al. Crestal bonechanges on platform-switched implants and adjacent teethwhen the tooth-implant distance is less than 1.5 mm. Int JPeriodontics Restorative Dent. 2012;32:149-155.
55. Misch CE. Root form surgery in the edentulousmandible: stage I implant insertion. In: Misch CE, ed.Contemporary Implant Dentistry. 2nd ed. St Louis, MO:Mosby; 1999:347-370.
56. Greenstein G, Cavallaro J. Managing the buccal gap andplate of bone: immediate dental implant placement. DentToday. 2013;32:70-79.
57. Tarnow D. Immediate vs. delayed socket placement: whatwe know, what we think we know and what we don’tknow. Presented at: American Academy ofPeriodontology; November 14, 2011; Miami Beach, FL.
58. Chu SJ, Salama MA, Salama H, et al. The dual-zonetherapeutic concept of managing immediate implantplacement and provisional restoration in anteriorextraction sockets. Compend Contin Educ Dent.2012;33:524-534.
Continuing Education
9
Immediate Dental Implant Placement: Technique, Part 1

POST EXAMINATION INFORMATION
To receive continuing education credit for participation inthis educational activity you must complete the programpost examination and receive a score of 70% or better.
Traditional Completion Option:You may fax or mail your answers with payment to DentistryToday (see Traditional Completion Information on followingpage). All information requested must be provided in orderto process the program for credit. Be sure to complete your“Payment,” “Personal Certification Information,” “Answers,”and “Evaluation” forms. Your exam will be graded within 72hours of receipt. Upon successful completion of the post-exam (70% or higher), a letter of completion will be mailedto the address provided.
Online Completion Option:Use this page to review the questions and mark youranswers. Return to dentalcetoday.com and sign in. If youhave not previously purchased the program, select it fromthe “Online Courses” listing and complete the onlinepurchase process. Once purchased the program will beadded to your User History page where a Take Exam linkwill be provided directly across from the program title.Select the Take Exam link, complete all the programquestions and Submit your answers. An immediate gradereport will be provided. Upon receiving a passing grade,complete the online evaluation form. Upon submitting the form, your Letter of Completion will be providedimmediately for printing.
General Program Information:Online users may log in to dentalcetoday.com any time inthe future to access previously purchased programs andview or print letters of completion and results.
POST EXAMINATION QUESTIONS
1. According to Evian et al, Type I sockets requirewhich of the following?
a. Soft-tissue augmentation.
b. Hard-tissue augmentation.
c. Soft- and hard-tissue preservation.
d. Soft-tissue preservation and hard-tissue augmentation.
2. When the bony socket is intact in the coronal aspectbut a fenestration is present apically, what is thesocket classification according to Evian et al?
a. Type I.
b. Type II.
c. Type III.
d. Type IV.
3. After an extraction, the average amount of verticalbone height that is lost if a flap is elevated is:
a. 1.24 mm.
b. 3.79 mm.
c. 2.46 mm.
d. 3.56 mm.
4. When a tooth is extracted, which is usually thethinnest plate of bone?
a. Buccal.
b. Lingual.
c. Proximal.
d. Buccal and lingual are the same thickness.
5. After removing a tooth with a healthy periodontium itis not necessary to curette the periodontal ligament.If pathosis exists, then all granulomatous tissueshould be removed.
a. The first statement is true, the second is false.
b. The first statement is false, the second is true.
c. Both statements are true.
d. Both statements are false.
Continuing Education
10
Immediate Dental Implant Placement: Technique, Part 1

6. After tooth extraction, it is advisable to place theimmediate implant ______ into bone to attain primarystability if mechanical retention cannot be achievedlaterally.
a. 1 to 3 mm.
b. 3 to 5 mm.
c. 5 to 7 mm.
d. 7 to 9 mm.
7. Atieh et al reported that bone loss using platformswitching after immediate implant placement was:
a. 0.05 mm to 0.99 mm.
b. 0.19 mm to 1.67 mm.
c. 0.37 mm to 2.66 mm.
d. 0.77 mm to 3.56 mm.
8. To avoid inducing recession in the maxillary estheticzone, it is preferable to do the following:
a. Avoid raising a buccal flap.
b. Extrude teeth.
c. Bone grafts should be placed to a crestal level.
d. Abutments should be removed and replaced severaltimes.
9. As a general rule, platforms of immediate implantsshould be placed ____ below the gingival margin.
a. 1 mm to 2 mm.
b. 2 mm to 3 mm.
c. 3 mm to 4 mm.
d. 4 mm to 5 mm.
10. Maxillary canine teeth are often angled 11° distally.The roots of maxillary canine teeth curve distally32% of the time.
a. The first statement is true, the second is false.
b. The first statement is false, the second is true.
c. Both statements are true.
d. Both statements are false.
Continuing Education
11
Immediate Dental Implant Placement: Technique, Part 1
PROGRAM COMPLETION INFORMATION
If you wish to purchase and complete this activitytraditionally (mail or fax) rather than online, you mustprovide the information requested below. Please be sure toselect your answers carefully and complete the evaluationinformation. To receive credit you must answer at least 7 ofthe 10 questions correctly.
Complete online at: dentalcetoday.com
TRADITIONAL COMPLETION INFORMATION:Mail or fax this completed form with payment to:
Dentistry TodayDepartment of Continuing Education100 Passaic AvenueFairfield, NJ 07004
Fax: 973-882-3622
PAYMENT & CREDIT INFORMATION:
Examination Fee: $40.00 Credit Hours: 2.0
Note: There is a $10 surcharge to process a check drawn on any bank other than a US bank. Should you have additionalquestions, please contact us at (973) 882-4700.
o I have enclosed a check or money order.
o I am using a credit card.
My Credit Card information is provided below.
o American Express o Visa o MC o Discover
Please provide the following (please print clearly):
Exact Name on Credit Card
Credit Card # Expiration Date
Signature
PROGRAM EVAUATION FORMPlease complete the following activity evaluation questions.
Rating Scale: Excellent = 5 and Poor = 0
Course objectives were achieved.
Content was useful and benefited your clinical practice.
Review questions were clear and relevant to the editorial.
Illustrations and photographs were clear and relevant.
Written presentation was informative and concise.
How much time did you spend reading the activity and completing the test?
What aspect of this course was most helpful and why?
What topics interest you for future Dentistry Today CE courses?
Continuing Education
Immediate Dental Implant Placement: Technique, Part 1
ANSWER FORM: COURSE #: 169Please check the correct box for each question below.
1. o a o b o c o d 6. o a o b o c o d
2. o a o b o c o d 7. o a o b o c o d
3. o a o b o c o d 8. o a o b o c o d
4. o a o b o c o d 9. o a o b o c o d
5. o a o b o c o d 10. o a o b o c o d
PERSONAL CERTIFICATION INFORMATION:
Last Name (PLEASE PRINT CLEARLY OR TYPE)
First Name
Profession / Credentials License Number
Street Address
Suite or Apartment Number
City State Zip Code
Daytime Telephone Number With Area Code
Fax Number With Area Code
E-mail Address
/
Dentistry Today, Inc, is an ADA CERP RecognizedProvider. ADA CERP is a service of the AmericanDental Association to assist dental professionals inindentifying quality providers of continuing dentaleducation. ADA CERP does not approve or endorseindividual courses or instructors, nor does it implyacceptance of credit hours by boards of dentistry.Concerns or complaints about a CE provider may bedirected to the provider or to ADA CERP atada.org/goto/cerp.
Approved PACE Program ProviderFAGD/MAGD Credit Approval doesnot imply acceptance by a state orprovincial board of dentistry or AGDendorsement. June 1, 2012 to May 31, 2015 AGD PACE approvalnumber: 309062
12