iih overview - cdn.ymaws.com
TRANSCRIPT
IIH Overview
Scottsdale Headache Symposium 2016
• Alex Sinclair
• NIHR Clinician Scientist & Honorary
Consultant Neurologist • [email protected]
• No conflicts of interest
Presentation
Diagnosis
Management
Overview
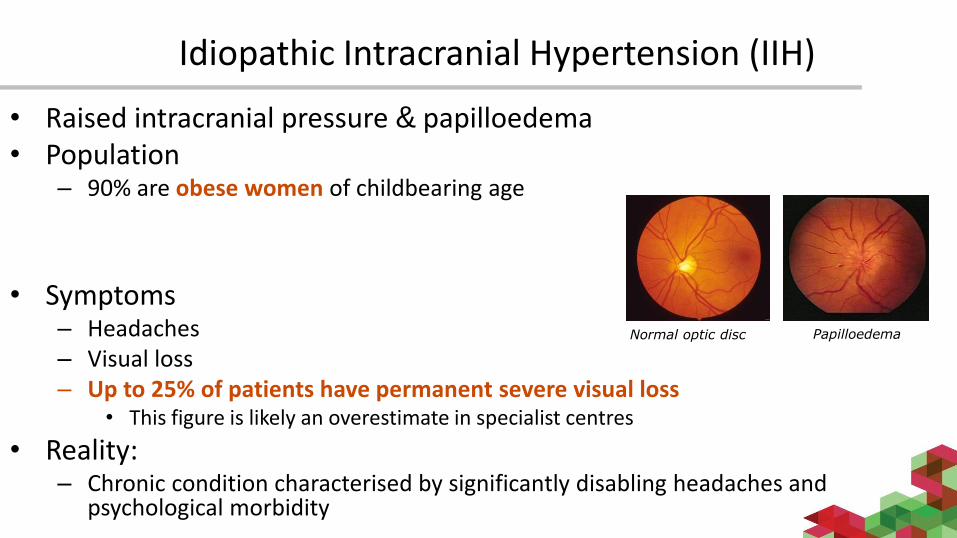
Idiopathic Intracranial Hypertension (IIH)
• Raised intracranial pressure & papilloedema• Population
– 90% are obese women of childbearing age
• Symptoms– Headaches– Visual loss– Up to 25% of patients have permanent severe visual loss
• This figure is likely an overestimate in specialist centres
• Reality:– Chronic condition characterised by significantly disabling headaches and
psychological morbidity
Normal optic disc Papilloedema
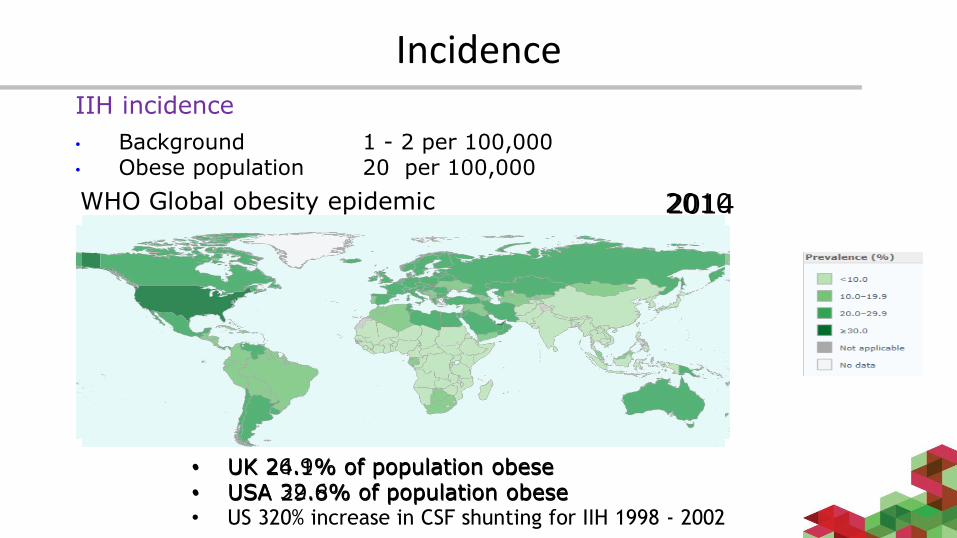
IncidenceIIH incidence
• Background 1 - 2 per 100,000• Obese population 20 per 100,000
WHO Global obesity epidemic
• UK 24.1% of population obese• USA 29.8% of population obese
20102014
• UK 26.9% of population obese• USA 32.6% of population obese• US 320% increase in CSF shunting for IIH 1998 - 2002
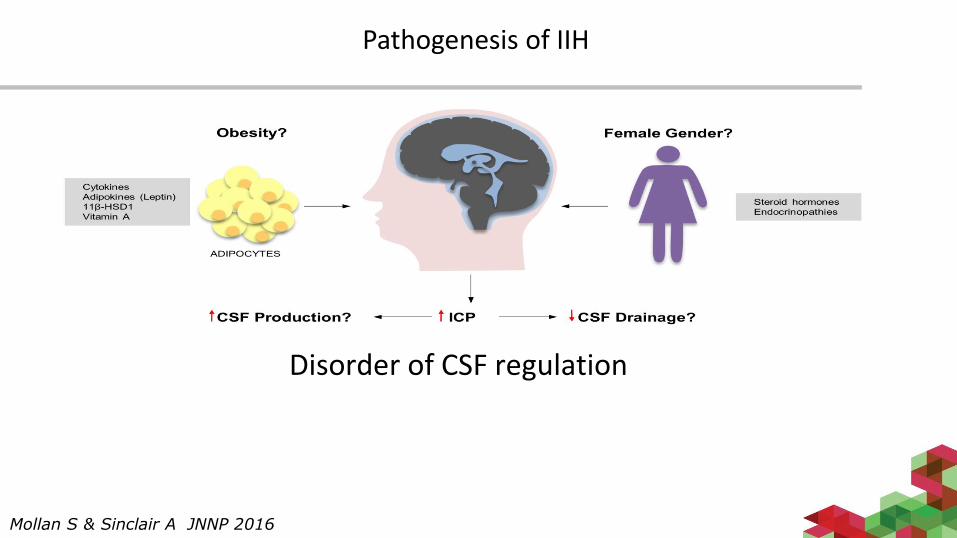
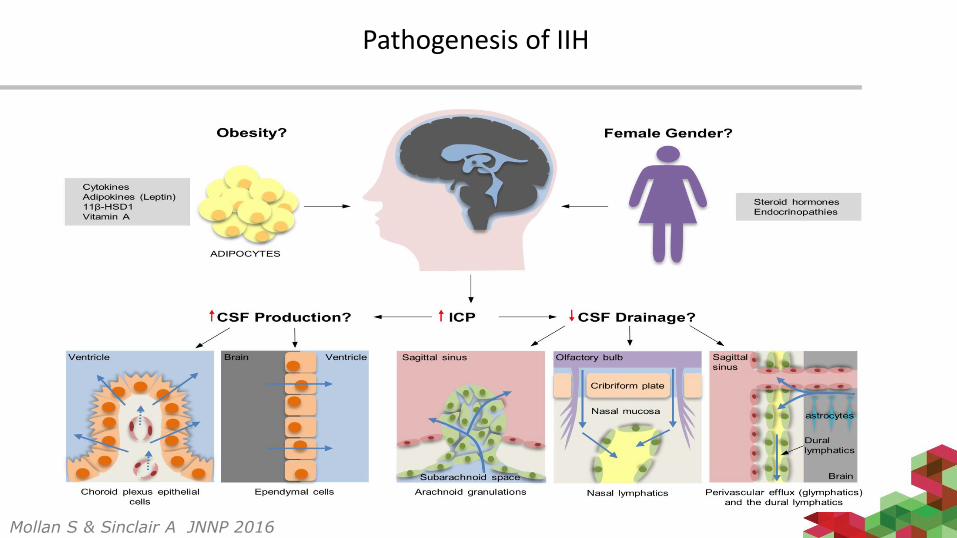
Pathogenesis of IIH
Mollan S & Sinclair A JNNP 2016
Disorder of CSF regulation
Mollan S & Sinclair A JNNP 2016
Pathogenesis of IIH
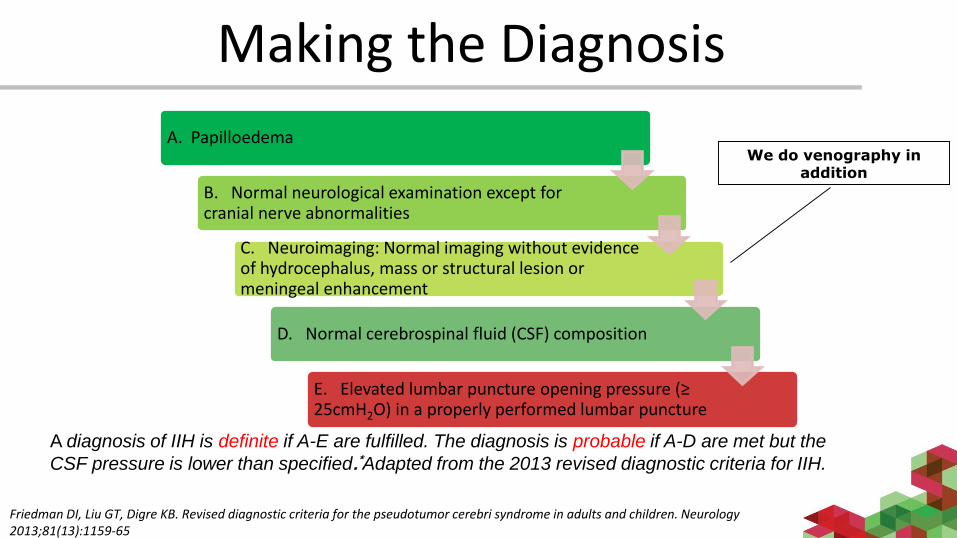
A diagnosis of IIH is definite if A-E are fulfilled. The diagnosis is probable if A-D are met but the
CSF pressure is lower than specified.*Adapted from the 2013 revised diagnostic criteria for IIH.
Making the Diagnosis
Friedman DI, Liu GT, Digre KB. Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology 2013;81(13):1159-65
A. Papilloedema
B. Normal neurological examination except for cranial nerve abnormalities
C. Neuroimaging: Normal imaging without evidence of hydrocephalus, mass or structural lesion or meningeal enhancement
D. Normal cerebrospinal fluid (CSF) composition
E. Elevated lumbar puncture opening pressure (≥ 25cmH2O) in a properly performed lumbar puncture
We do venography in addition
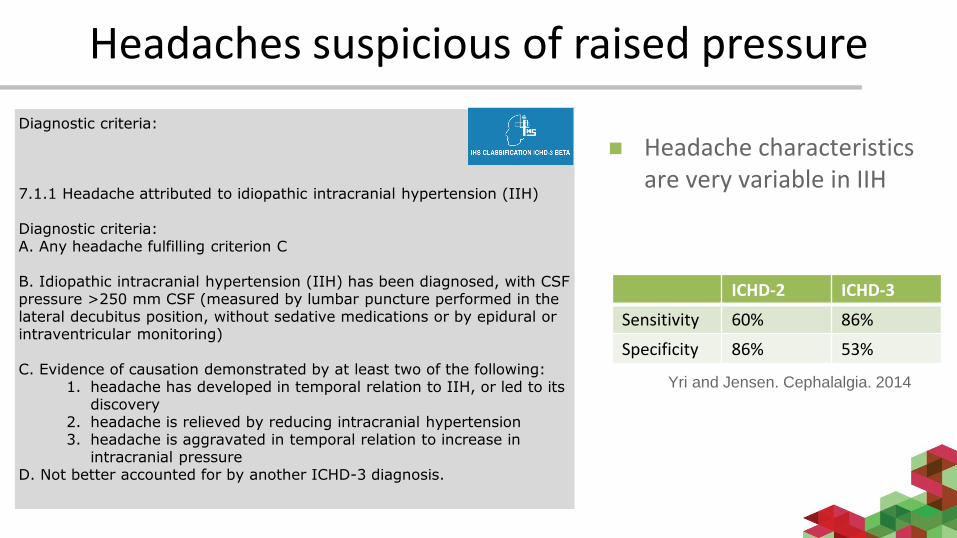
Headaches suspicious of raised pressure
Yri and Jensen. Cephalalgia. 2014
Diagnostic criteria:
7.1.1 Headache attributed to idiopathic intracranial hypertension (IIH)
Diagnostic criteria:A. Any headache fulfilling criterion C
B. Idiopathic intracranial hypertension (IIH) has been diagnosed, with CSF pressure >250 mm CSF (measured by lumbar puncture performed in the lateral decubitus position, without sedative medications or by epidural or intraventricular monitoring)
C. Evidence of causation demonstrated by at least two of the following:1. headache has developed in temporal relation to IIH, or led to its
discovery2. headache is relieved by reducing intracranial hypertension3. headache is aggravated in temporal relation to increase in
intracranial pressure D. Not better accounted for by another ICHD-3 diagnosis.
ICHD-2 ICHD-3
Sensitivity 60% 86%
Specificity 86% 53%
Headache characteristics are very variable in IIH
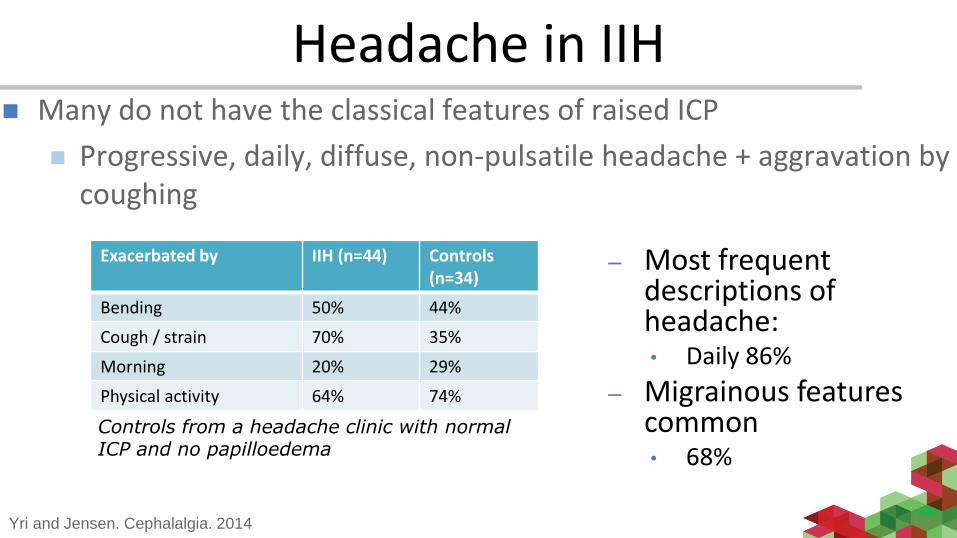
Headache in IIH Many do not have the classical features of raised ICP
Progressive, daily, diffuse, non-pulsatile headache + aggravation by coughing
Exacerbated by IIH (n=44) Controls (n=34)
Bending 50% 44%
Cough / strain 70% 35%
Morning 20% 29%
Physical activity 64% 74%
Yri and Jensen. Cephalalgia. 2014
Controls from a headache clinic with normal ICP and no papilloedema
– Most frequent descriptions of headache:• Daily 86%
– Migrainous features common • 68%
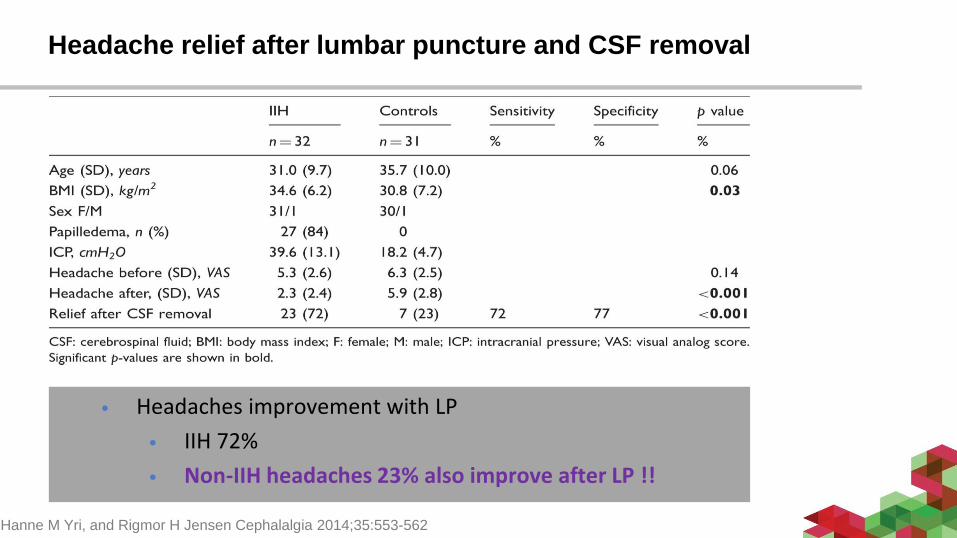
Headache relief after lumbar puncture and CSF removal
Hanne M Yri, and Rigmor H Jensen Cephalalgia 2014;35:553-562
• Headaches improvement with LP
• IIH 72%
• Non-IIH headaches 23% also improve after LP !!
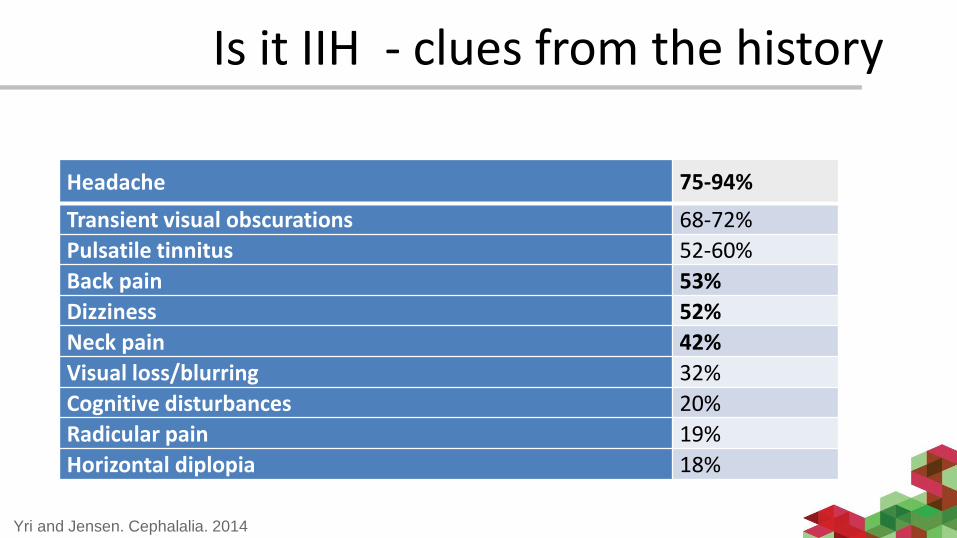
Is it IIH - clues from the history
Headache 75-94%
Transient visual obscurations 68-72%
Pulsatile tinnitus 52-60%
Back pain 53%
Dizziness 52%
Neck pain 42%
Visual loss/blurring 32%
Cognitive disturbances 20%
Radicular pain 19%
Horizontal diplopia 18%
Yri and Jensen. Cephalalia. 2014
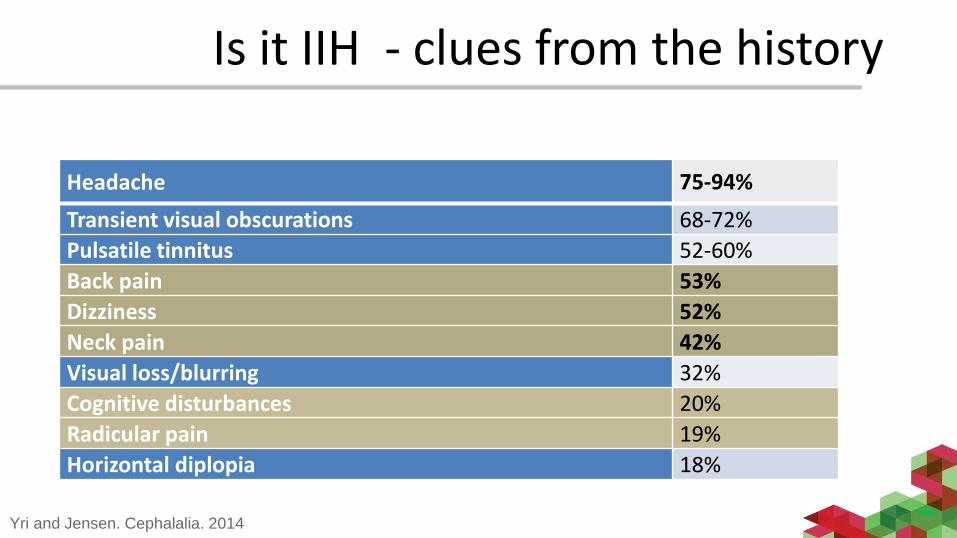
Headache 75-94%
Transient visual obscurations 68-72%
Pulsatile tinnitus 52-60%
Back pain 53%
Dizziness 52%
Neck pain 42%
Visual loss/blurring 32%
Cognitive disturbances 20%
Radicular pain 19%
Horizontal diplopia 18%
Yri and Jensen. Cephalalia. 2014
Is it IIH - clues from the history
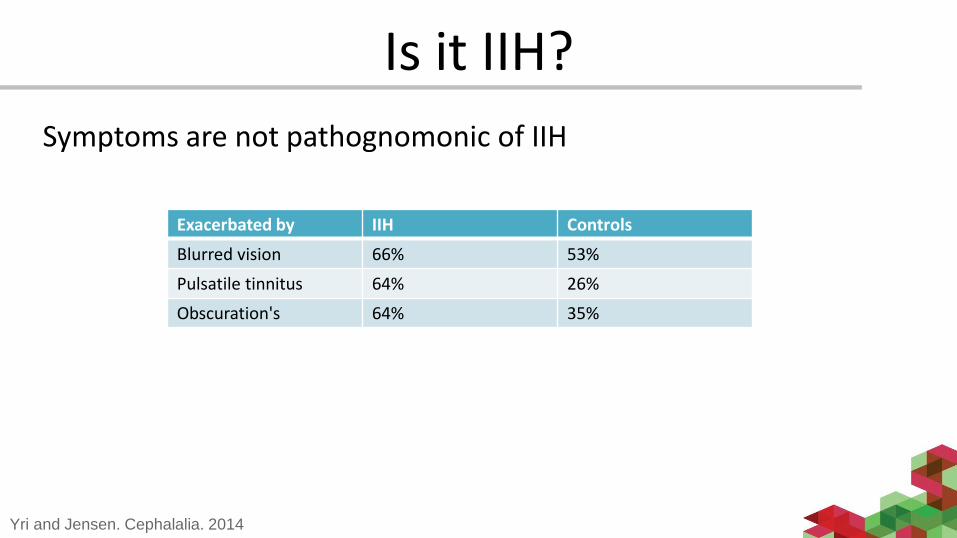
Is it IIH?
Symptoms are not pathognomonic of IIH
Exacerbated by IIH Controls
Blurred vision 66% 53%
Pulsatile tinnitus 64% 26%
Obscuration's 64% 35%
Yri and Jensen. Cephalalia. 2014
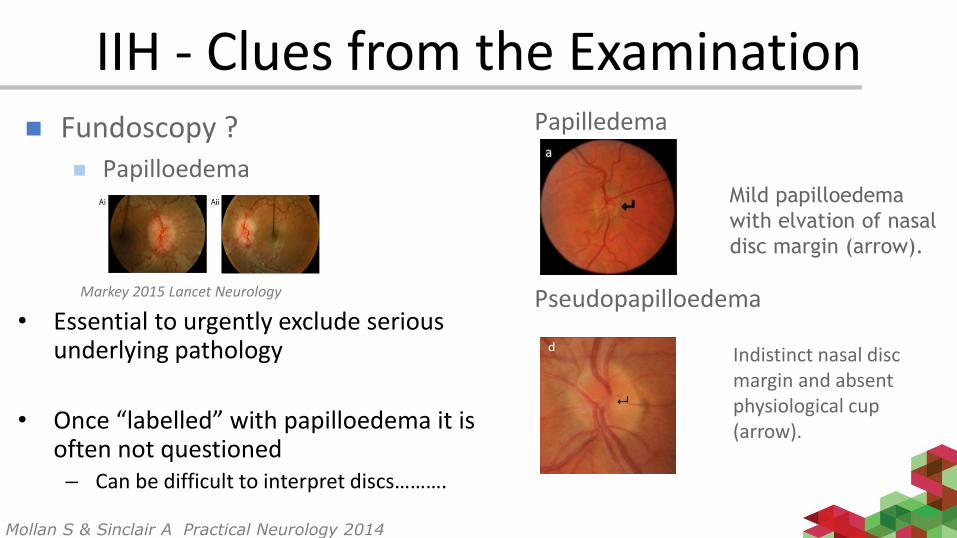
IIH - Clues from the Examination
• Essential to urgently exclude serious underlying pathology
• Once “labelled” with papilloedema it is often not questioned– Can be difficult to interpret discs……….
Markey 2015 Lancet Neurology
Fundoscopy ? Papilloedema
Papilledema
Pseudopapilloedema
Indistinct nasal disc margin and absent physiological cup (arrow).
Mild papilloedema
with elvation of nasal
disc margin (arrow).
Mollan S & Sinclair A Practical Neurology 2014
Diagnostic error in IIH
• 40% of patients labelled with IIH referred to a neuro-ophthalmology clinic don’t have IIH!
• Error is due to inaccurate identification of papilloedema in headache patients
– 79% had a un-necessary LP
– 96% received acetazolamide unnecessarily
– 3% has shunt surgery
Fisayo et AL Neurology 2016
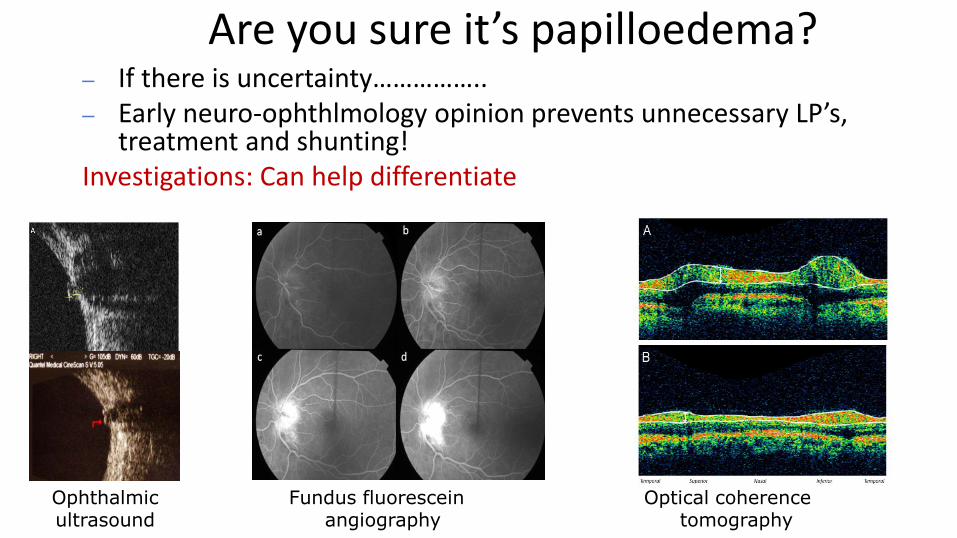
Are you sure it’s papilloedema?– If there is uncertainty……………..– Early neuro-ophthlmology opinion prevents unnecessary LP’s,
treatment and shunting!Investigations: Can help differentiate
Ophthalmic ultrasound
Fundus fluorescein angiography
Optical coherence tomography
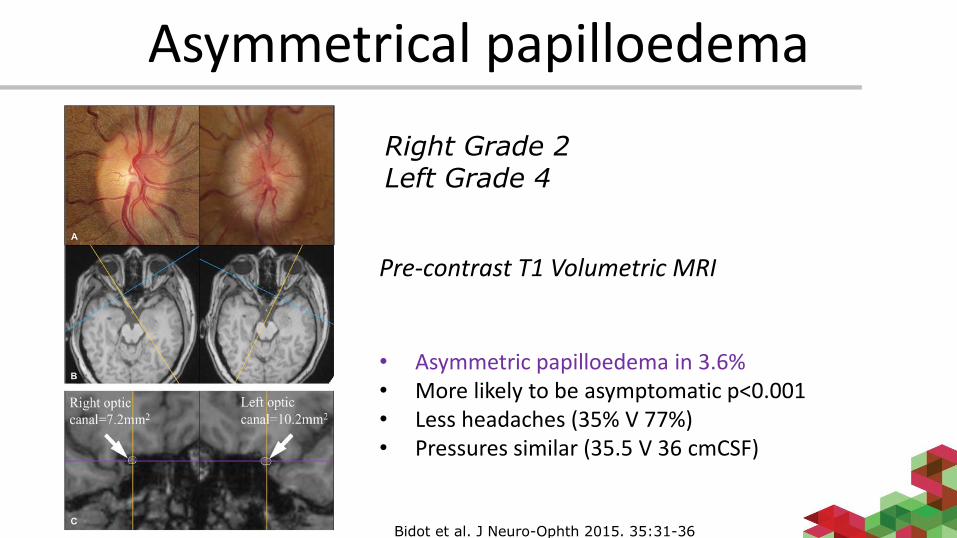
Asymmetrical papilloedema
Right Grade 2Left Grade 4
Pre-contrast T1 Volumetric MRI
• Asymmetric papilloedema in 3.6%• More likely to be asymptomatic p<0.001• Less headaches (35% V 77%)• Pressures similar (35.5 V 36 cmCSF)
Bidot et al. J Neuro-Ophth 2015. 35:31-36
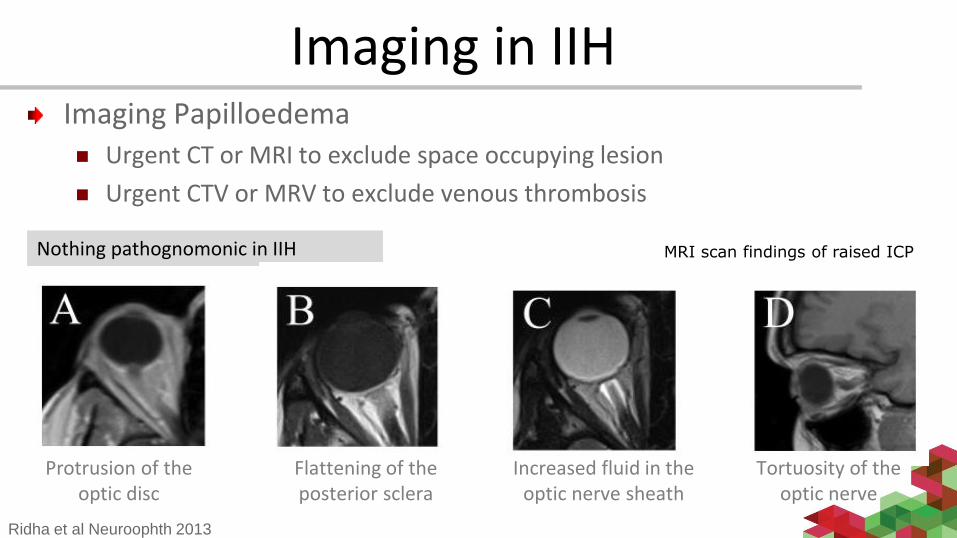
Imaging in IIH
Ridha et al Neuroophth 2013
MRI scan findings of raised ICP Nothing pathognomonic in IIH
Imaging Papilloedema Urgent CT or MRI to exclude space occupying lesion
Urgent CTV or MRV to exclude venous thrombosis
Protrusion of the optic disc
Flattening of the posterior sclera
Increased fluid in the optic nerve sheath
Tortuosity of the optic nerve
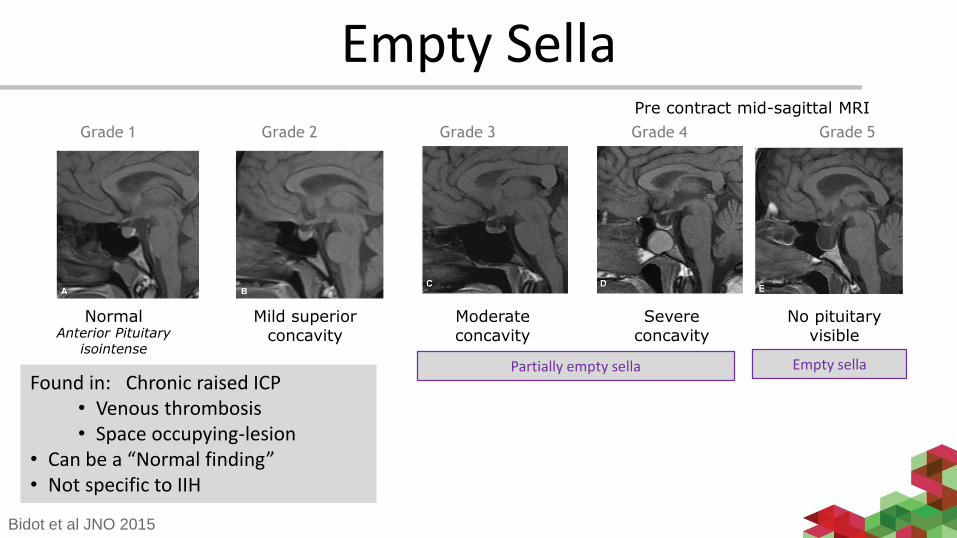
Empty Sella
Normal Mild superior concavity
Moderate concavity
Severe concavity
No pituitary visible
Grade 4Grade 2 Grade 3Grade 1 Grade 5
Partially empty sella Empty sella
Pre contract mid-sagittal MRI
Anterior Pituitary isointense
Bidot et al JNO 2015
Found in: Chronic raised ICP• Venous thrombosis • Space occupying-lesion
• Can be a “Normal finding”• Not specific to IIH
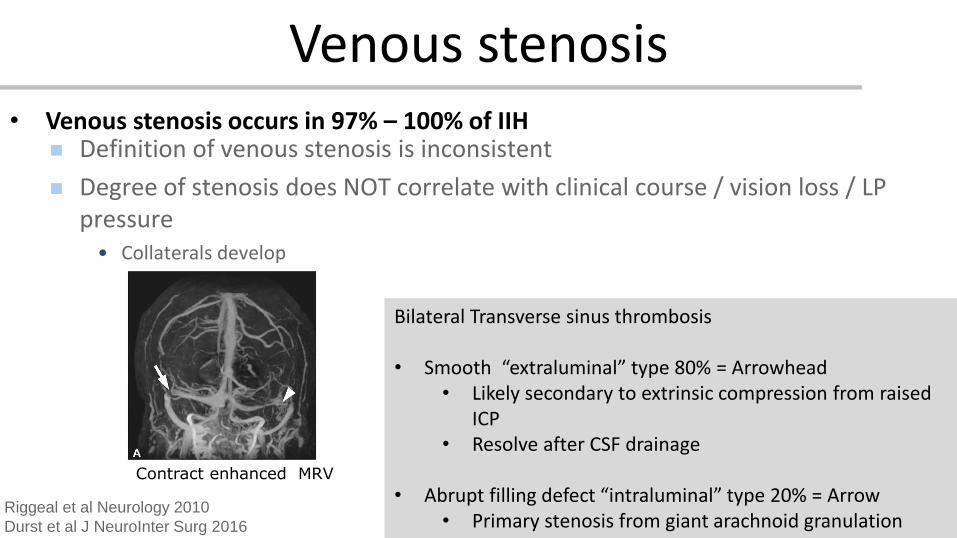
Venous stenosis• Venous stenosis occurs in 97% – 100% of IIH
Riggeal et al Neurology 2010
Durst et al J NeuroInter Surg 2016
Contract enhanced MRV
Bilateral Transverse sinus thrombosis
• Smooth “extraluminal” type 80% = Arrowhead• Likely secondary to extrinsic compression from raised
ICP• Resolve after CSF drainage
• Abrupt filling defect “intraluminal” type 20% = Arrow• Primary stenosis from giant arachnoid granulation
Definition of venous stenosis is inconsistent
Degree of stenosis does NOT correlate with clinical course / vision loss / LP pressure
• Collaterals develop
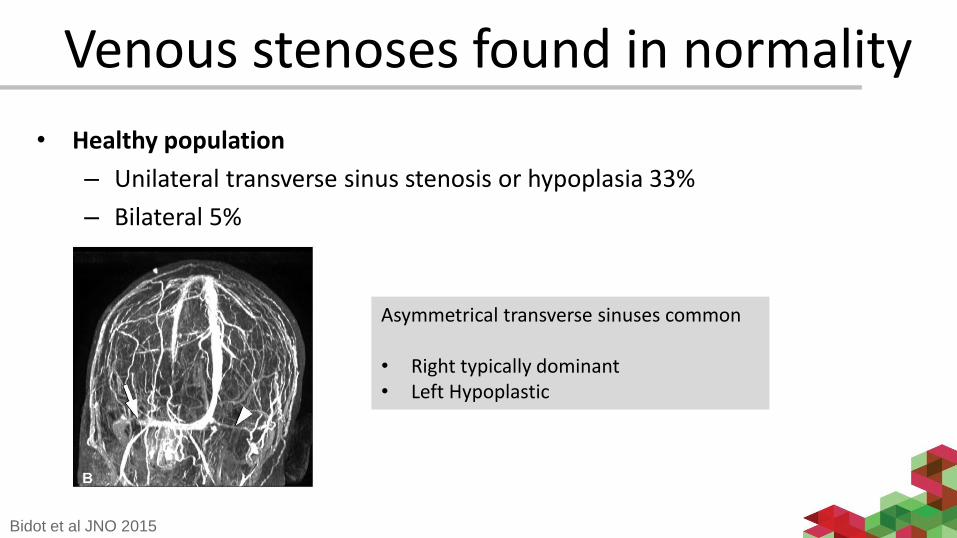
Venous stenoses found in normality
Asymmetrical transverse sinuses common
• Right typically dominant• Left Hypoplastic
Bidot et al JNO 2015
• Healthy population
– Unilateral transverse sinus stenosis or hypoplasia 33%
– Bilateral 5%
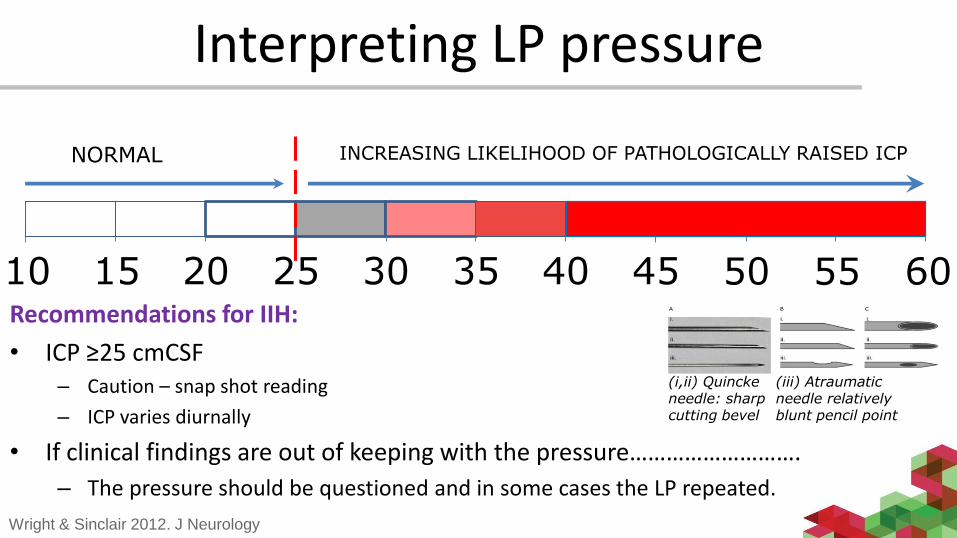
NORMAL INCREASING LIKELIHOOD OF PATHOLOGICALLY RAISED ICP
15 20 25 30 35 40 4510 50 55 60
Interpreting LP pressure
Recommendations for IIH:
• ICP ≥25 cmCSF– Caution – snap shot reading
– ICP varies diurnally
• If clinical findings are out of keeping with the pressure……………………….
– The pressure should be questioned and in some cases the LP repeated.
(i,ii) Quinckeneedle: sharp cutting bevel
(iii) Atraumatic needle relatively blunt pencil point
Wright & Sinclair 2012. J Neurology
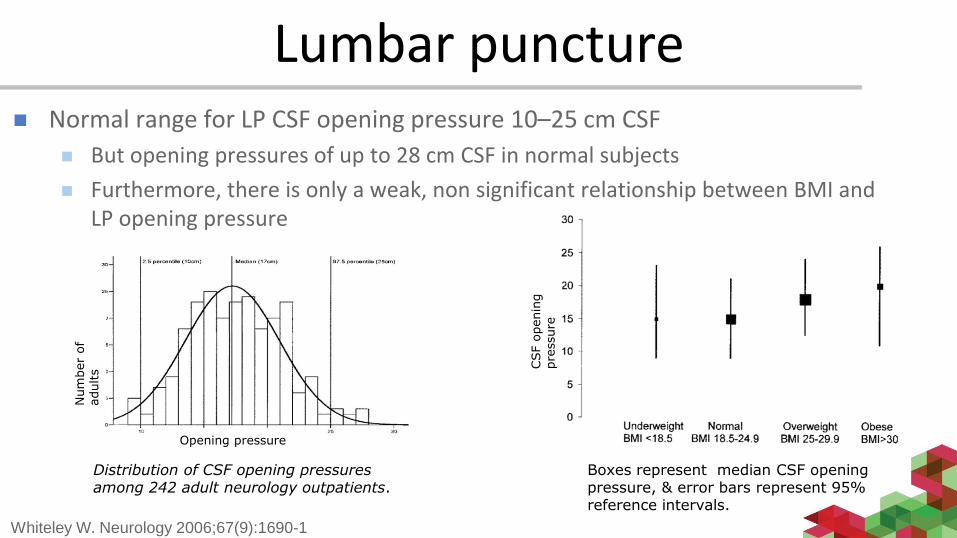
Lumbar puncture Normal range for LP CSF opening pressure 10–25 cm CSF
But opening pressures of up to 28 cm CSF in normal subjects
Furthermore, there is only a weak, non significant relationship between BMI and LP opening pressure
Whiteley W. Neurology 2006;67(9):1690-1
Boxes represent median CSF opening pressure, & error bars represent 95% reference intervals.
Distribution of CSF opening pressures among 242 adult neurology outpatients.
Num
ber
of
adults
CSF o
penin
g
pre
ssure
Opening pressure
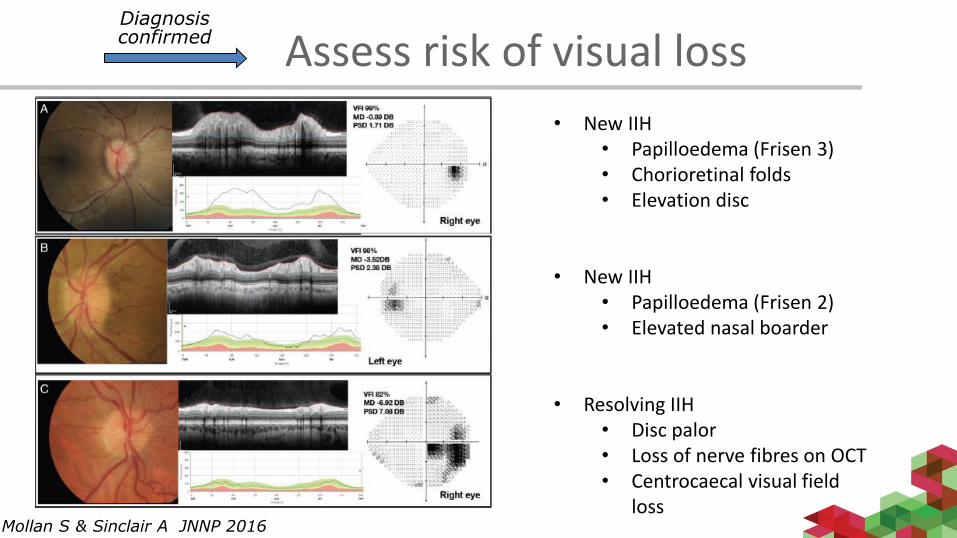
Mollan S & Sinclair A JNNP 2016
• New IIH• Papilloedema (Frisen 3)• Chorioretinal folds• Elevation disc
• New IIH • Papilloedema (Frisen 2)• Elevated nasal boarder
• Resolving IIH• Disc palor• Loss of nerve fibres on OCT• Centrocaecal visual field
loss
Assess risk of visual lossDiagnosis confirmed
Management of IIH
Surgical
Weight loss
Medical
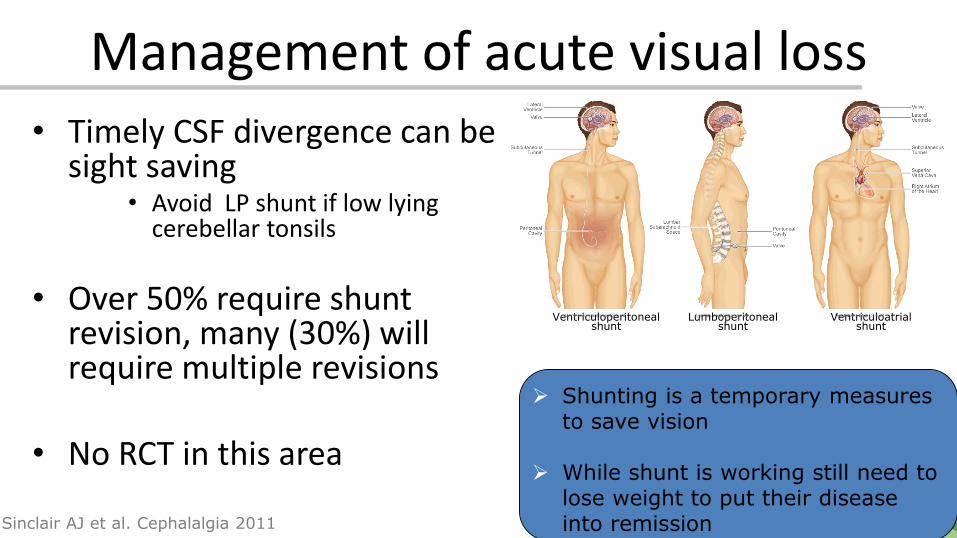
Management of acute visual loss• Timely CSF divergence can be
sight saving• Avoid LP shunt if low lying
cerebellar tonsils
• Over 50% require shunt revision, many (30%) will require multiple revisions
• No RCT in this area
Shunting is a temporary measures to save vision
While shunt is working still need to lose weight to put their disease into remissionSinclair AJ et al. Cephalalgia 2011
Lumboperitoneal shunt
Ventriculoperitoneal shunt
Ventriculoatrial shunt
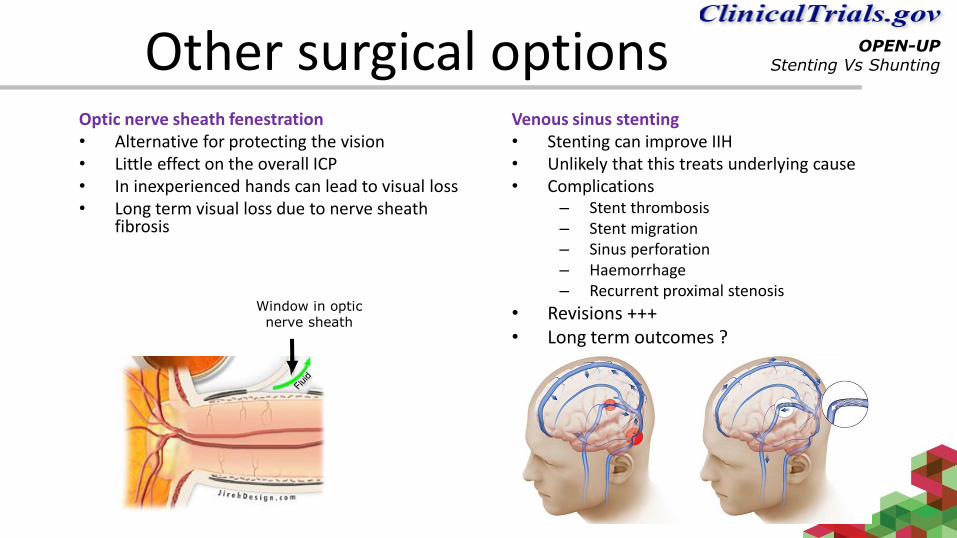
Other surgical optionsOptic nerve sheath fenestration• Alternative for protecting the vision• Little effect on the overall ICP • In inexperienced hands can lead to visual loss• Long term visual loss due to nerve sheath
fibrosis
Venous sinus stenting• Stenting can improve IIH• Unlikely that this treats underlying cause• Complications
– Stent thrombosis– Stent migration– Sinus perforation– Haemorrhage– Recurrent proximal stenosis
• Revisions +++• Long term outcomes ?
Window in optic nerve sheath
OPEN-UPStenting Vs Shunting
Weight loss
– Weight loss as a treatment of IIH
• 90% of patients with IIH are obese women• Commonly advocated treatment in IIH
• Evidence for efficacy of weight loss ?
– Prospective, multicentre, two stage cross-over study
– Primary outcome was change in ICP as measured by LPSinclair et al. 2010 . BMJ;341:c2701
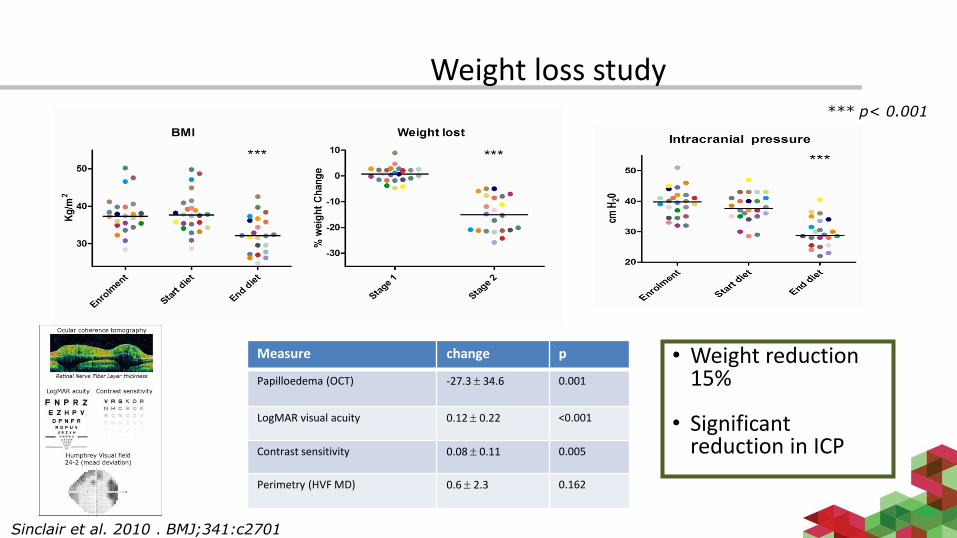
Weight loss study*** p< 0.001
Sinclair et al. 2010 . BMJ;341:c2701
Measure change p
Papilloedema (OCT) -27.3 34.6 0.001
LogMAR visual acuity 0.12 0.22 <0.001
Contrast sensitivity 0.08 0.11 0.005
Perimetry (HVF MD) 0.6 2.3 0.162
• Weight reduction 15%
• Significant reduction in ICP
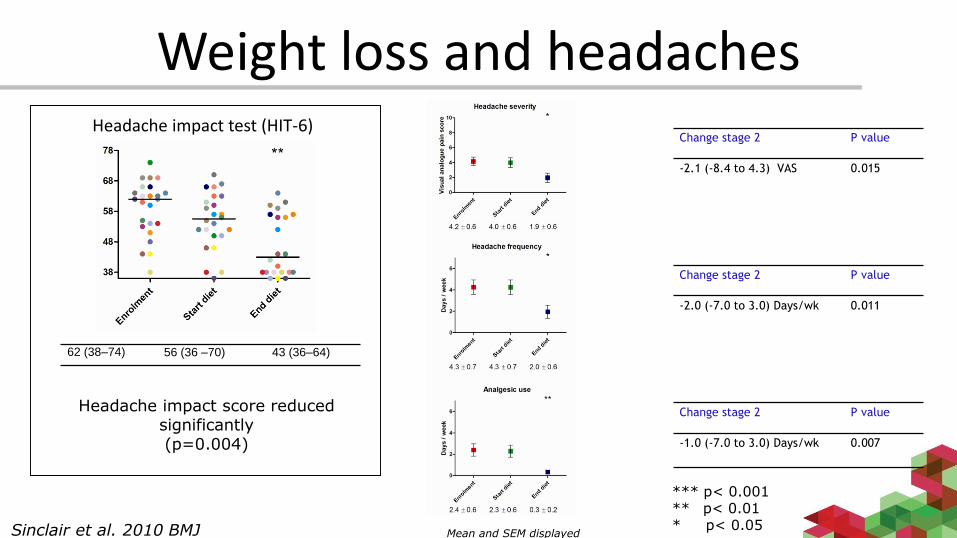
Weight loss and headaches
Headache impact score reduced significantly(p=0.004)
Change stage 2 P value
-2.1 (-8.4 to 4.3) VAS 0.015
Change stage 2 P value
-2.0 (-7.0 to 3.0) Days/wk 0.011
Change stage 2 P value
-1.0 (-7.0 to 3.0) Days/wk 0.007
*** p< 0.001** p< 0.01* p< 0.05
62 (38–74) 56 (36 –70) 43 (36–64)
Mean and SEM displayedSinclair et al. 2010 BMJ
Headache impact test (HIT-6)
IIH and weight
• Long-term weight loss is difficult to achieve and maintain
– Typically as little as 2–4 kg at 2 years irrespective of the dietary regime followed
– Orlistat, (reduce weight by 2.89kg) - these drugs do not achieve sufficient weight loss to significantly modify IIH
• Bariatric surgery is recommended by NICE for patients with a BMI over 40, or over 35 with a co-morbidity
– Women suffering from IIH have an average BMI of 38
• IIH is not currently recognised as a co-morbidity for bariatric surgery in UK

The IIH Weight Trial• Phase III
• UK multi-centre, randomised controlled trial recruiting for 3 years
• Outcome measures:– LP
– Visual function
– Headache
Community weight loss
program
Bariatric surgery
IIHN=60
Follow-up 12 months
Follow-up 24,60months
Primary outcome
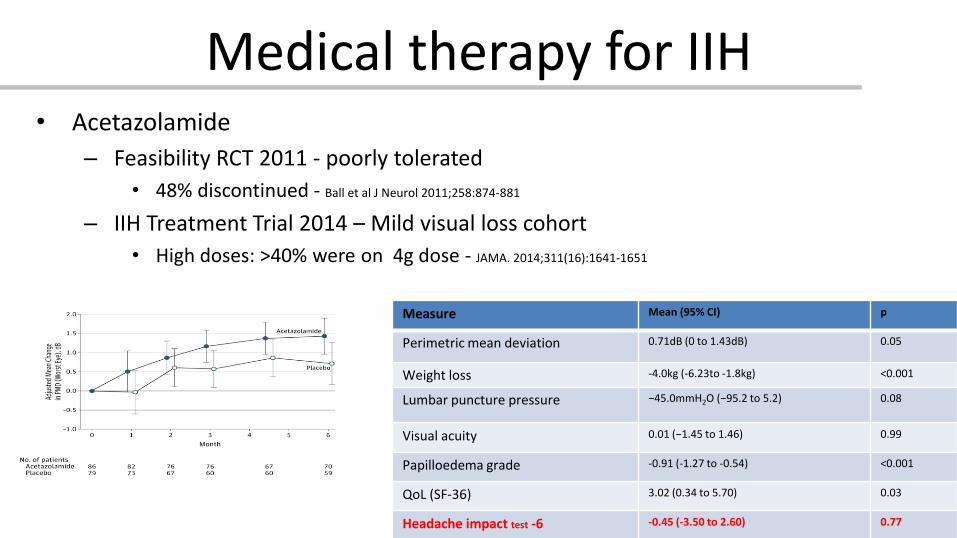
Medical therapy for IIH• Acetazolamide
– Feasibility RCT 2011 - poorly tolerated
• 48% discontinued - Ball et al J Neurol 2011;258:874-881
– IIH Treatment Trial 2014 – Mild visual loss cohort
• High doses: >40% were on 4g dose - JAMA. 2014;311(16):1641-1651
Measure Mean (95% CI) p
Perimetric mean deviation 0.71dB (0 to 1.43dB) 0.05
Weight loss -4.0kg (-6.23to -1.8kg) <0.001
Lumbar puncture pressure −45.0mmH2O (−95.2 to 5.2) 0.08
Visual acuity 0.01 (−1.45 to 1.46) 0.99
Papilloedema grade -0.91 (-1.27 to -0.54) <0.001
QoL (SF-36) 3.02 (0.34 to 5.70) 0.03
Headache impact test -6 -0.45 (-3.50 to 2.60) 0.77
Medical treatment for IIH
• Cochrane review IIH updated August 2015
• Two included RCTs included: “showed modest benefits for acetazolamide for some outcomes”
• “Insufficient evidence to recommend or reject the efficacy of acetazolamide for treating IIH”.
Piper et al. Cochrane Database Syst Rev 2015 Aug 7;8
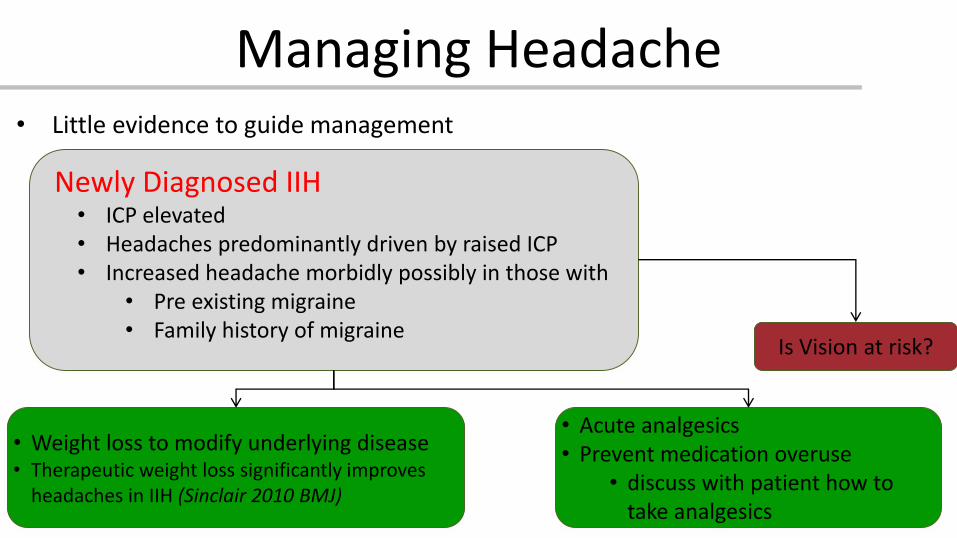
Managing Headache• Little evidence to guide management
Newly Diagnosed IIH• ICP elevated• Headaches predominantly driven by raised ICP• Increased headache morbidly possibly in those with
• Pre existing migraine• Family history of migraine
• Weight loss to modify underlying disease • Therapeutic weight loss significantly improves
headaches in IIH (Sinclair 2010 BMJ)
• Acute analgesics• Prevent medication overuse
• discuss with patient how to take analgesics
Is Vision at risk?
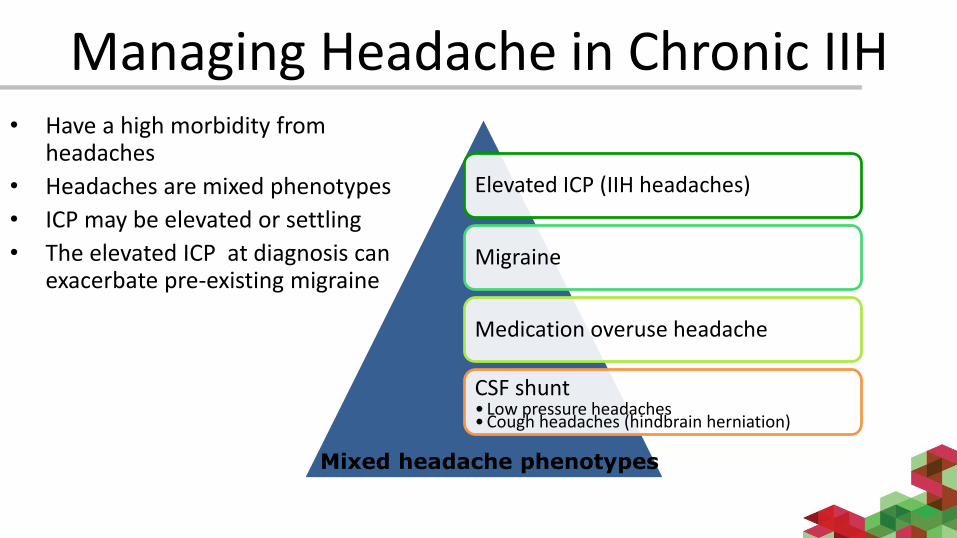
Managing Headache in Chronic IIH• Have a high morbidity from
headaches
• Headaches are mixed phenotypes
• ICP may be elevated or settling
• The elevated ICP at diagnosis can exacerbate pre-existing migraine
Elevated ICP (IIH headaches)
Migraine
Medication overuse headache
CSF shunt• Low pressure headaches • Cough headaches (hindbrain herniation)
Mixed headache phenotypes
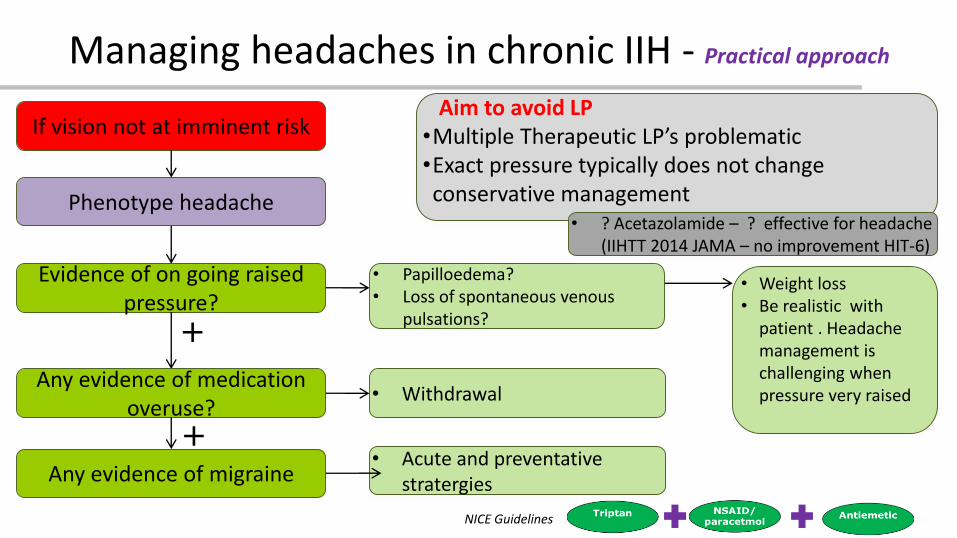
Managing headaches in chronic IIH - Practical approach
Phenotype headache
Aim to avoid LP•Multiple Therapeutic LP’s problematic•Exact pressure typically does not change conservative management
Evidence of on going raised pressure?
• Papilloedema?• Loss of spontaneous venous
pulsations?
If vision not at imminent risk
• Weight loss• Be realistic with
patient . Headache management is challenging when pressure very raised
Any evidence of medication overuse?
• Withdrawal
Any evidence of migraine• Acute and preventative
stratergies
+
+
• ? Acetazolamide – ? effective for headache (IIHTT 2014 JAMA – no improvement HIT-6)
NICE Guidelines
Shunting to treat IIH headache?• Evidence base lacking• Debated area• Cases need to be evaluated individually
– Careful assessment– Discussion of pros and cons
• Work up is patient specific– ± Evaluate imaging for evidence of raised ICP– ± LP – ± ICP monitoring– MDT– Discussion on shunt type
Stenting for headaches…….very contentiousNo RCT’s or long term data.
Shunting to treat IIH headache?
• Headache continues in the majority of patients post-operatively (68% at 6 months and 79% at 2 years).
• De-novo post-operative low-pressure headache occurred in 28%
• We recommend programmable shunts – lower headache morbidity
Sinclair AJ et al. Cephalalgia 2011 Dec;31(16):1627-33

Headaches in Shunted IIH patients
“Shunt series & CT head ” in A&E • NOT helpful • Don’t change management
If concern about shunt infection
Consider LP or shunt tap
Liu A 2015 Clin Neurol Neurosurg
Liu A 2015 Worl Neurosury
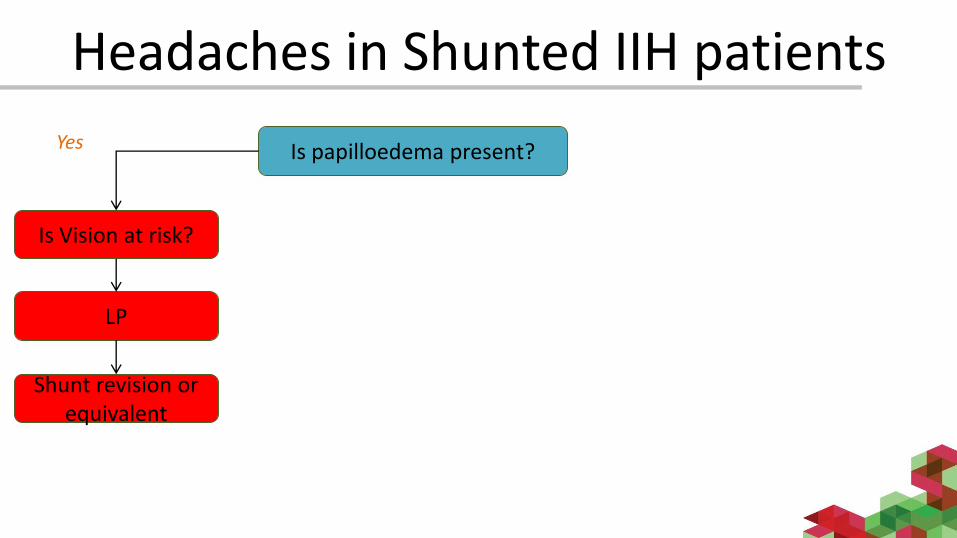
Headaches in Shunted IIH patients
Is papilloedema present?Yes
Is Vision at risk?
LP
Shunt revision or equivalent
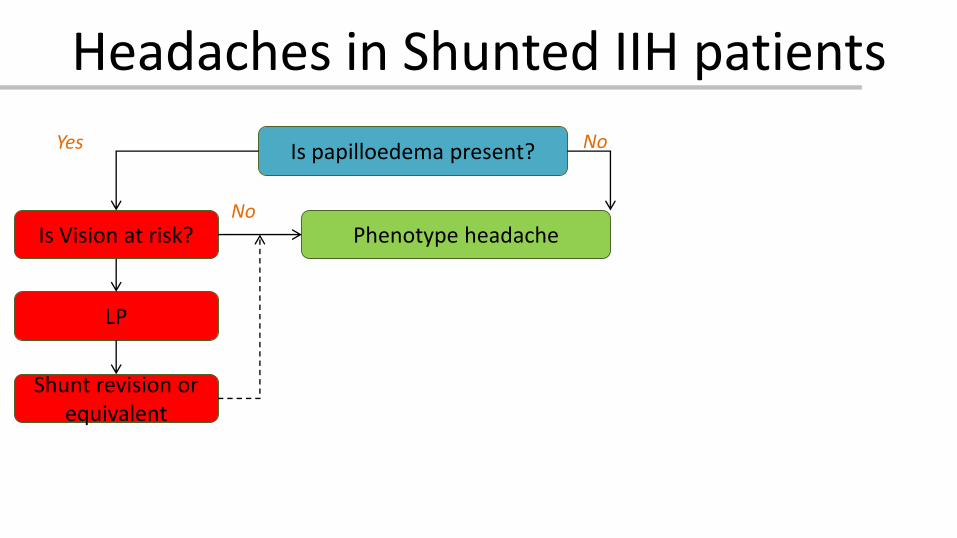
Headaches in Shunted IIH patients
Is papilloedema present?Yes
Is Vision at risk?
LP
Phenotype headache
Shunt revision or equivalent
No
No
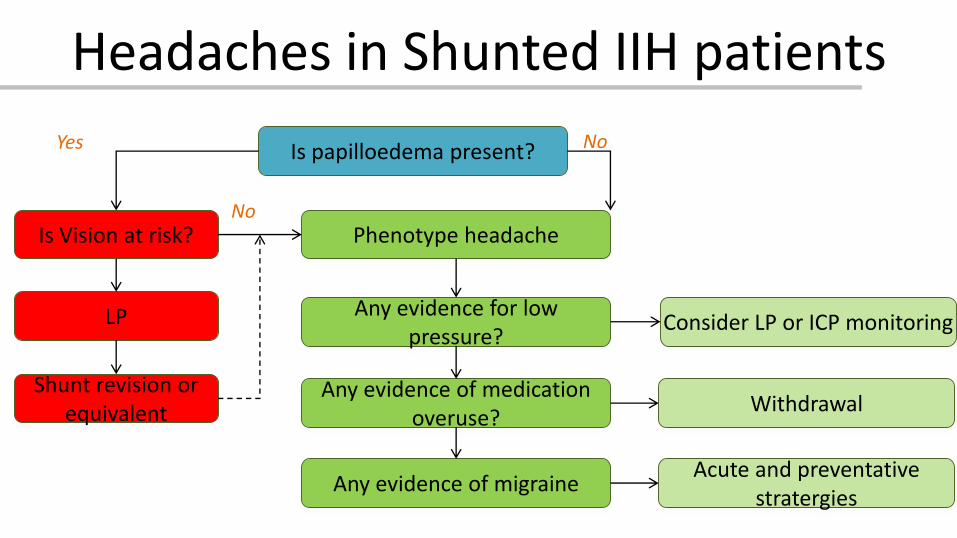
Headaches in Shunted IIH patients
Is papilloedema present?Yes No
Is Vision at risk?
LP
Phenotype headache
Any evidence for low pressure?
Consider LP or ICP monitoring
Any evidence of medication overuse?
Withdrawal
Any evidence of migraineAcute and preventative
stratergies
Shunt revision or equivalent
No
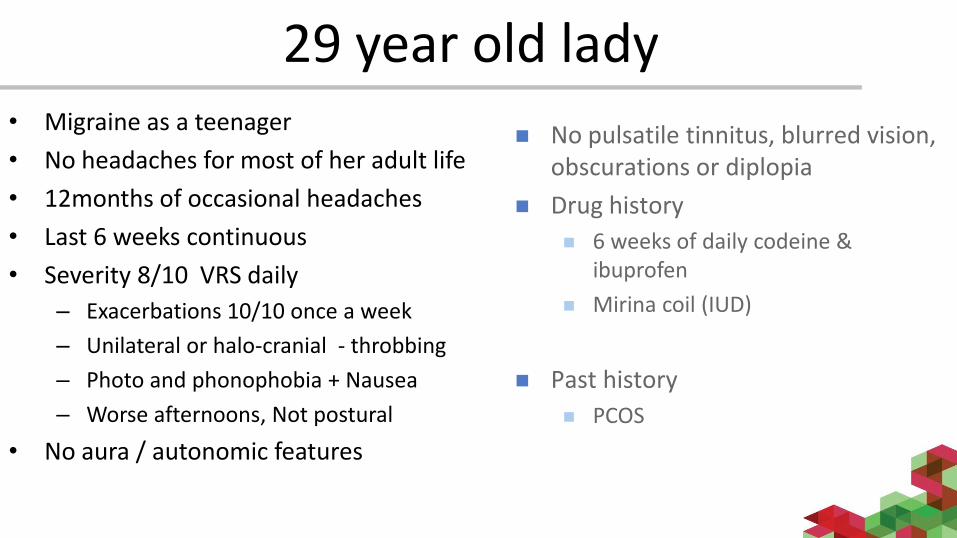
29 year old lady• Migraine as a teenager
• No headaches for most of her adult life
• 12months of occasional headaches
• Last 6 weeks continuous
• Severity 8/10 VRS daily
– Exacerbations 10/10 once a week
– Unilateral or halo-cranial - throbbing
– Photo and phonophobia + Nausea
– Worse afternoons, Not postural
• No aura / autonomic features
No pulsatile tinnitus, blurred vision, obscurations or diplopia
Drug history
6 weeks of daily codeine & ibuprofen
Mirina coil (IUD)
Past history
PCOS
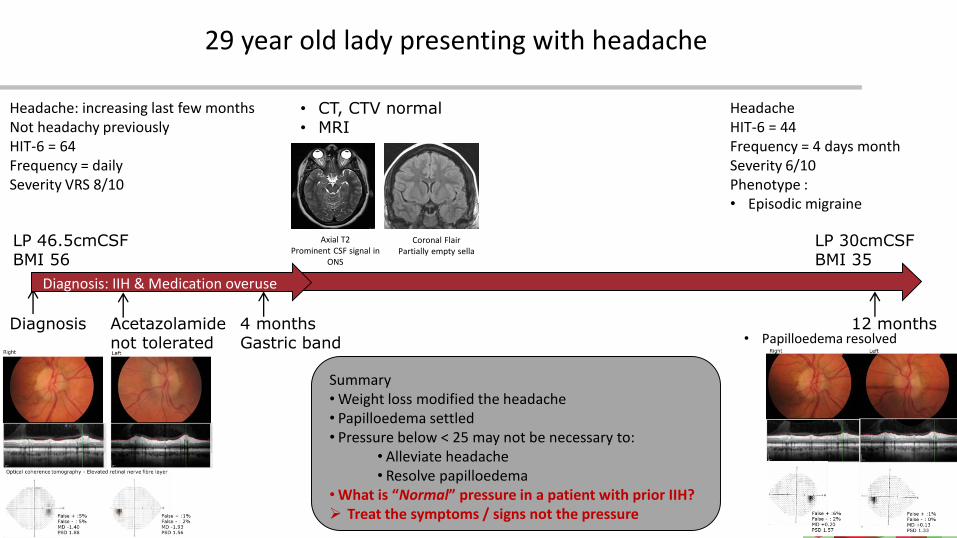
4 monthsGastric band
Headache: increasing last few monthsNot headachy previously HIT-6 = 64Frequency = dailySeverity VRS 8/10
LP 46.5cmCSFBMI 56
Summary• Weight loss modified the headache• Papilloedema settled• Pressure below < 25 may not be necessary to:
• Alleviate headache• Resolve papilloedema
• What is “Normal” pressure in a patient with prior IIH? Treat the symptoms / signs not the pressure
29 year old lady presenting with headache
• CT, CTV normal• MRI
Axial T2Prominent CSF signal in
ONS
Coronal FlairPartially empty sella
Acetazolamide not tolerated
Diagnosis
Diagnosis: IIH & Medication overuse
12 months
LP 30cmCSFBMI 35
Headache HIT-6 = 44Frequency = 4 days monthSeverity 6/10Phenotype :• Episodic migraine
• Papilloedema resolved

Key final messages
IIH– Papilloedema is over diagnosed
– Could it be pseudo-papilloedema?
– Headache improvement post LP not exclusive to IIH– Improvement can occur in non-IIH headaches
– Treat the signs and symptoms not the exact pressure
– Caution diagnosing IIH if pressure <25cmCSF