identifying, measuring and managing delerium
TRANSCRIPT

Identifying, measuring and managing delirium
Dr Tizzy TealeSenior Clinical Lecturer and Honorary Consultant Geriatrician
University of Leeds and Bradford Teaching Hospitals NHS Trust

How common is delirium?
• Delirium is the commonest complication of hospitalisation in older people
• Large point prevalence study (Italy)
– 108 acute and 12 rehabilitation wards
– Delirium assessments with the 4AT within a pre-determined 24 hour period (“Delirium Day”)
– 1867 patients assessed
Bellelli G, Morandi A, Santo et al BMC Medicine 2016;14:106
• Overall point prevalence of delirium in hospital inpatients over 65 was 22.9%
• This estimate is consistent across prevalence studies
• Over 50% of patients with delirium have a diagnosis of dementia
Ryan DJ, O’Regan et al BMJOpen 2013;3;e001772

Poorer longer term outcomes following delirium
• Poor cognitive outcomes
– Delirium is associated with incident dementia
• OR 8.7 95%CI: 2.1-35
Davis et al Brain 2012; 135:2809-2816
– Acceleration of cognitive decline
• Two-fold increased rate in the first 12 months
Gross et al 2012; Arch Int Med;2012;172(17):1324-1331
• Institutionalisation
– OR 2.41 95%CI: 1.77-3.29 (average follow up 15 months)
• Mortality
– HR 1.95 95%CI: 1.51-2.52 (average follow up 23 months)Witlox et al JAMA 2010;304(4):443-51
People remember being delirious
• Recall of delirium experiences is common after recovery (>50%)
• Those with more severe delirium and with underlying cognitive impairment less likely to recall
– This doesn’t make their distress any less at the time
• Commonly recalled symptoms are of visual hallucinations
• Misinterpretation of real sensory experiences also common
• Source of fear and anxiety
• Delusions common (often threatening)
• Descriptions of incomprehensible situations / time distortion common
• Trying to make sense of situation
• There may be longer lasting neuropsychiatric sequelaeO’Malley et al J of Psychosomatic Res 2008;65:223-228

How often is delirium missed?
• Up to 2/3 of cases of delirium are missed or misdiagnosed by acute medical teams
Collins et al Age Ageing 2010; 39(1):131-135
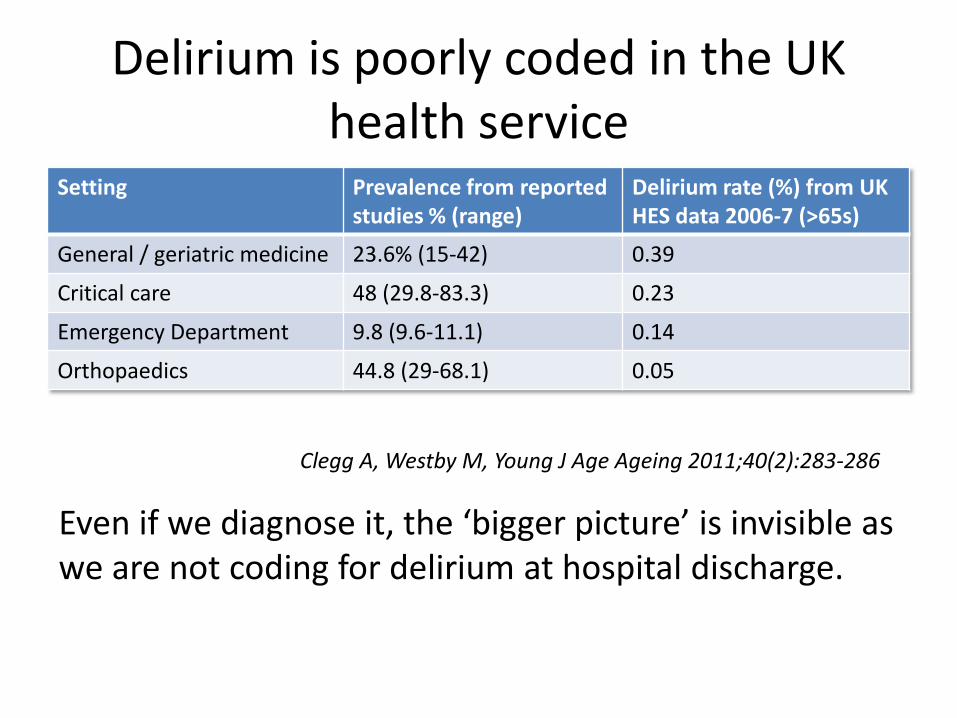
Delirium is poorly coded in the UK health service
Setting Prevalence from reported studies % (range)
Delirium rate (%) from UK HES data 2006-7 (>65s)
General / geriatric medicine 23.6% (15-42) 0.39
Critical care 48 (29.8-83.3) 0.23
Emergency Department 9.8 (9.6-11.1) 0.14
Orthopaedics 44.8 (29-68.1) 0.05
Clegg A, Westby M, Young J Age Ageing 2011;40(2):283-286
Even if we diagnose it, the ‘bigger picture’ is invisible as we are not coding for delirium at hospital discharge.
Recognising delirium
• Based on DSM 5 criteria
• Diagnosis of delirium requires all DSM 5 criteria to be met
• Criteria operationalised into screening or diagnostic algorithms
• A degree of subjectivity / inconsistently applied criteria
• Delirium is a complex syndrome – features can be difficult to spot
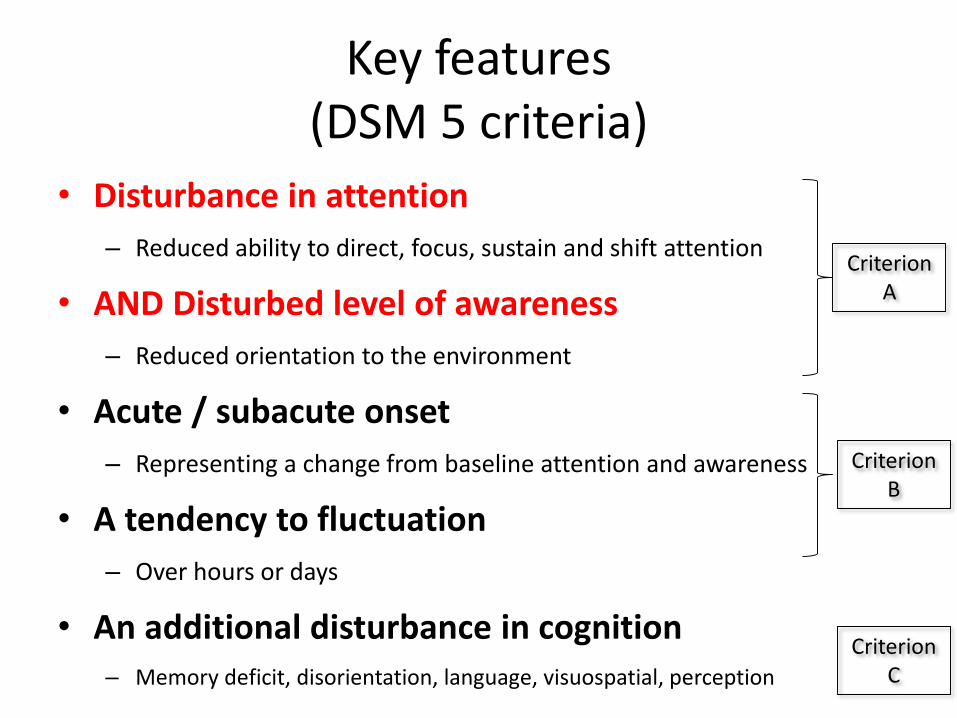
Key features (DSM 5 criteria)
• Disturbance in attention
– Reduced ability to direct, focus, sustain and shift attention
• AND Disturbed level of awareness
– Reduced orientation to the environment
• Acute / subacute onset
– Representing a change from baseline attention and awareness
• A tendency to fluctuation
– Over hours or days
• An additional disturbance in cognition– Memory deficit, disorientation, language, visuospatial, perception
Criterion A
Criterion B
Criterion C

• Not better explained by an existing or evolving neurocognitive disorder
– Not in the context of severely reduced arousal
• e.g. coma
• Physiologically attributable to a medical condition
– History, examination, lab findings
– Substance intoxication or withdrawal
– Exposure to a toxin
– Multiple aetiologies
Criterion D
Criterion E
Key features (DSM 5 criteria)
• Disturbance in attention
– Reduced ability to direct, focus, sustain and shift attention
• AND Disturbed level of awareness
– Reduced orientation to the environment
• Acute / subacute onset
– Representing a change from baseline attention and awareness
• A tendency to fluctuation
– Over hours or days
• An additional disturbance in cognition– Memory deficit, disorientation, language, visuospatial, perception
Criterion A
Criterion B
Criterion C

Inattention
• Difficulty maintaining / shifting focus between tasks
• Easily distracted by sounds, objects, own thoughts
• Perseveration
• May be poor eye contact
• May seem vague

Detecting inattention
• Months of the year backwards (MOTYB)
–Ask to say forwards Jan to Dec.
–Then ask to recite backwards from Dec.
– If able to reach July without error, attention likely intact
• MOTYB in >69yo without dementia
– 84% sensitivity
– 90% specificity for deliriumO’Regan JNNP 2014;85:1122-1131

Detection of delirium superimposed on dementia (DSD) is particularly challenging
• Impaired attention is a key feature of delirium
• May help distinguish delirium from dementia
• But patients with dementia struggle to complete tests of attention
Rutter et al EDA Conference Abstract 2016; #13

• MOTYB in those with dementia
– Poor specificity for delirium
– Patients with dementia may struggle to complete
O’Regan JNNP 2014;85:1122-1131
• Patterns of errors may help to discriminate between delirium and dementia (more work needed)
– omissions / repetitions / self-correction Rutter et al EDA Conference Abstract 2016; #13
Duncan et al EDA Conference Abstract 2016 # 35
• Use of informant instruments can help to identify pre-existing dementia (e.g. the IQCODE-SF)
Jackson et al Age Ageing 2016;45(4):505-11

Consciousness, arousal and attention
• Altered consciousness (DSM-IV) changed to disturbance in attention and awareness in DSM-5
• Consciousness is a hierarchical construct
– Level of consciousness = arousal
– Content of consciousness = attention
• Consciousness therefore includes implicit assessment of arousal
– Removed in DSM-5

• It is important not to miss delirious patients in whom attention cannot be assessed due to alterations in arousal (e.g. too sleepy)
• Those with sudden onset of altered arousal (over, or underactive) not attributable to existing or evolving condition (e.g. stroke) should be considered to meet DSM-5 criterion A for delirium
• EDA and ADS BMC Medicine 2014; 12:141
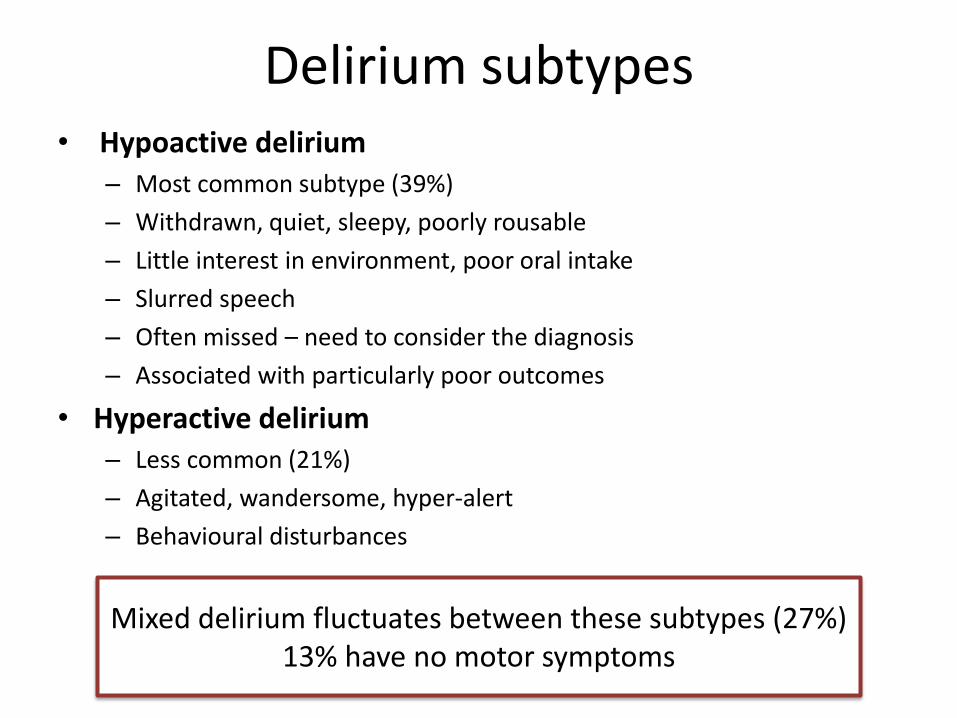
• Hypoactive delirium– Most common subtype (39%)
– Withdrawn, quiet, sleepy, poorly rousable
– Little interest in environment, poor oral intake
– Slurred speech
– Often missed – need to consider the diagnosis
– Associated with particularly poor outcomes
• Hyperactive delirium – Less common (21%)
– Agitated, wandersome, hyper-alert
– Behavioural disturbances
Mixed delirium fluctuates between these subtypes (27%)13% have no motor symptoms
Delirium subtypes

Key features (DSM 5 criteria)
• Disturbance in attention
– Reduced ability to direct, focus, sustain and shift attention
• AND Disturbed level of awareness
– Reduced orientation to the environment
• Acute / subacute onset
– Representing a change from baseline attention and awareness
• A tendency to fluctuation
– Over hours or days
• An additional disturbance in cognition– Memory deficit, disorientation, language, visuospatial, perception
Criterion A
Criterion B
Criterion C

Acute onset and fluctuating course
• Aim to identify a change from baseline
• SQiD (single question in delirium)– “Do you think [patient] has been more confused lately”?– 80% sensitivity for delirium– 71% specificity
• Have there been fluctuations over the course of days or hours?
Sands et al. Palliat Med 2010; 24: 561-565

Key features (DSM 5 criteria)
• Disturbance in attention
– Reduced ability to direct, focus, sustain and shift attention
• AND Disturbed level of awareness
– Reduced orientation to the environment
• Acute / subacute onset
– Representing a change from baseline attention and awareness
• A tendency to fluctuation
– Over hours or days
• An additional disturbance in cognition– Memory deficit, disorientation, language, visuospatial, perception
Criterion A
Criterion B
Criterion C

Additional cognitive disturbance
• Disorganised thinking, incoherent speech, perceptual problems, disorientation
• Problems making sense of what is going on
• Misinterpreting the environment
• Asking abstract questions can help identify
• May be hallucinations or persecutory ideas
– Do you feel frightened by anything or anyone?
– Are you concerned about anything going on here?Health Improvement Scotland Delirium toolkit 2014
• Mumbling, slurred or rambling speech which may be difficult to understand

4AT (the4at.com)
• 4AT can be used in those untestable with other methods
– e.g. stupor
• Does not rely on skilled assessment of attention
• Previous validation study (Italy)
– Sensitivity 89.7%
– Specificity 84.1%Bellelli Age Ageing 2014;43(4):496-502
• Utility in non-English speaking patients
– Sensitivity 91%
– Specificity 71%De et al Int J Geriatr Psych 2016; epub ahead of print
Alertness (normal / abnormal)
AMT4 (Age, DOB, Place, Current Year)
Attention (MOTYB)
Acute change or fluctuating course (yes / no)
Who gets delirium ?
• Strong predictors:
– Frailty
– Dementia
– Visual impairment
– Dehydration
– Severe illness
• Modifiable vs non-modifiable risk factors

Delirium prevention strategies:
• Up to one third of delirium is preventable through multicomponent delirium prevention interventions
Siddiqi et al Cochrane Review 2016 DOI: 10.1002/14651858.CD005563.pub3
• Personalised care delivered in a ward environment geared for delirium prevention
• What don’t we know? – Which are the most important / effective components of a
multicomponent intervention and how should these best be delivered ?
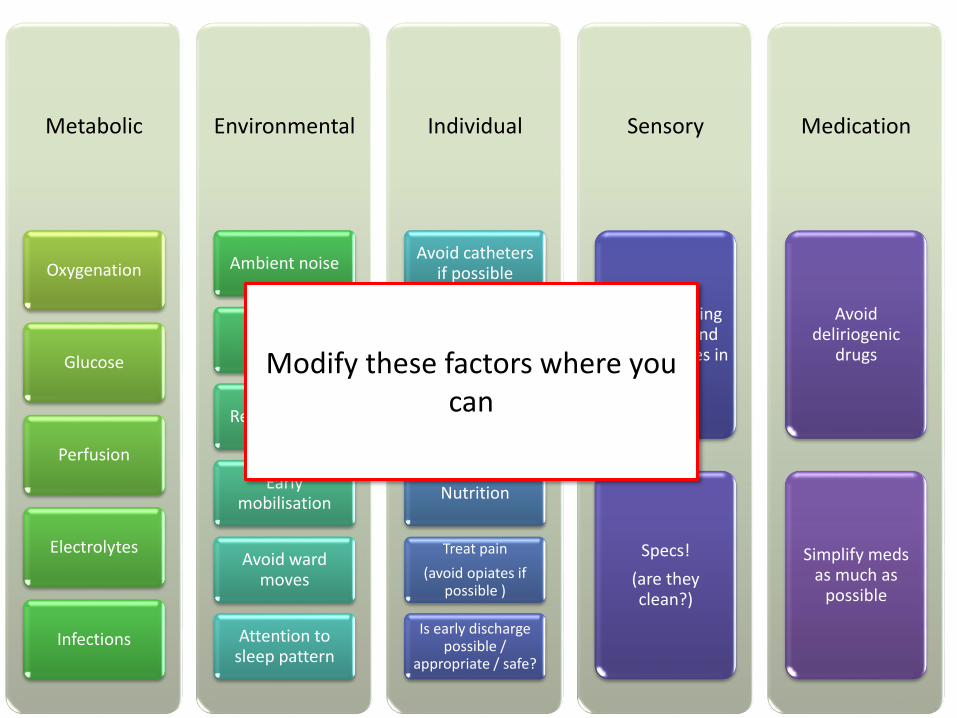
Metabolic
Oxygenation
Glucose
Perfusion
Electrolytes
Infections
Environmental
Ambient noise
Signage
Re-orientation
Early mobilisation
Avoid ward moves
Attention to sleep pattern
Individual
Avoid catheters if possible
Bowel Care
Hydration
Nutrition
Treat pain
(avoid opiates if possible )
Is early discharge possible /
appropriate / safe?
Sensory
Ensure hearing aids work and
have batteries in
Specs!
(are they clean?)
Medication
Avoid deliriogenic
drugs
Simplify meds as much as
possible
Modify these factors where you can

Non-pharmacological treatment of delirium
• It is important to be aware of, and modify potential triggers in non-delirious patients, as well as targeting contributing factors in those who are delirious
• Delirium episodes shorter and less severe if occur in the context of a multicomponent delirium prevention intervention
Marcantonio JAMA 2001;49(5):516-22O’Hanlon et al JNNP 2014;85(2):207-213
• No convincing evidence that multicomponent interventions are beneficial for the treatment of established delirium
Drugs and delirium
• Drugs implicated in development of delirium
• Drugs for delirium prevention
• Drugs for delirium treatment
• Drugs for management of delirium symptoms

Drugs implicated in delirium
• In general avoid– Drugs with anticholinergic properties
• Antihistamines
• TCAD
• Treatments for OAB
– Benzodiazepines
– Opioids (but treat pain)
• Medication review is a key aspect of delirium prevention / management
• Pay attention to the number, and type of medication

Drugs to prevent delirium (outside ICU)
• Drugs investigated for prophylaxis– Antipsychotics
– Melatonin / melatonin agonists
– Acetylcholinesterase inhibitors
– Citicoline
– Gabapentinoids
• No evidence to support the use of any of these drugs for prevention of delirium
Siddiqi et al Cochrane Review 2016 DOI: 10.1002/14651858.CD005563.pub3
Pharmacological treatment of delirium
• Evidence remains limited
• No convincing benefit for pharmacological therapies for treatment or prevention of delirium in non-ICU settings
• There is a need for further trials to identify agents that are safe for older people, and that have efficacy in the treatment / prevention of delirium
Management of delirium symptoms
• Identify and manage the underlying cause
• Symptoms should be managed through verbal and non-verbal de-escalation techniques
• If a person with delirium is distressed or considered a risk to themselves or others and verbal and non-verbal de-escalation techniques are ineffective or inappropriate, consider giving short-term (usually for 1 week or less) haloperidol or olanzapine
• Start at the lowest clinically appropriate dose and titrate cautiously according to symptoms
• Use antipsychotic drugs with caution or not at all for people with conditions such as Parkinson's disease or dementia with Lewy bodies
• No drugs have a UK license for treatment or prevention of delirium https://www.nice.org.uk/guidance/cg103/chapter/1-Guidance#treating-delirium

Delirium recovery
• Persistence of delirium beyond hospital discharge is common
– Discharge 44.7% (half of these will have recovered by 3/12)
– 1 month 32.8%
– 3 months 25.6%
– 6 months 21%Cole et al Age Ageing 2009; 38:19-26
• Outcomes for people with persistent delirium are worse than for those who recover
• Those with dementia are more likely to develop persistent delirium
• 38% of people presenting with delirium have undiagnosed cognitive impairment
Jackson et al Age Ageing 2016;45(4):493-499

Follow up
• People who have had delirium are more likely to develop incident dementia
• Follow up after an episode of delirium is useful:
– For education / give the opportunity for patients to make sense of their experience if they want to
– To identify features of persistent delirium
– To identify / signpost those with incident dementia
Bradford Teaching Hospitals NHS Foundation Trust delirium patient information leaflethttp://johnscampaign.org.uk/docs/external/bradford-teaching-hospitals-delirium-prevention.pdf
• Please contact BTHFT for copyright permissions if you wish to use / adapt
Resources

NICE Delirium: Diagnosis, Prevention and Management of delirium guidelines (CG103) July 2010http://www.nice.org.uk/guidance/cg103
The 4AThttp://www.the4at.com/
The Scottish Delirium Association “Delirium Management Comprehensive Pathway” Dec 2013http://www.scottishdeliriumassociation.com
Healthcare Improvement Scotlandhttp://www.healthcareimprovementscotland.org• E-modules• Information for patients and carers• TIME delirium care bundle