identifying and addressing market access challenges
TRANSCRIPT
Supplement to May/June 2018
PART 1 OF 2
A continuing medical education (CME) activity provided by Evolve Medical Education LLC and distributed with Retina Today.
This CME activity is supported through an educational grant from Regeneron Pharmaceuticals, Inc.
Distributed with
David Eichenbaum, MD, Moderator
Larry Halperin, MD
Pamela Pautler JD, MBA
Jonathan L. Prenner, MD
Winston Wong, PharmD
IDENTIFYING AND ADDRESSING MARKET ACCESS CHALLENGESWITH ANTI-VEGF THERAPIES FOR PATIENTS WITH RETINAL DISEASE

CONTENT SOURCEThis continuing medical education (CME) activity captures
content from a roundtable discussion.
ACTIVITY DESCRIPTIONThe use of anti-VEGF therapies for retinal diseases raises
numerous issues in today’s health care environment when the cost of treatment is often as much a consideration as the efficacy and safety. Thus, payers have become more involved in managing the use of these agents, potentially interfering with clinical deci-sion making. The following roundtable brings together thought leaders in the retina field to discuss the challenges they face in obtaining access to anti-VEGF medications for their patients and how they overcome those challenges.
TARGET AUDIENCEThis certified CME activity is designed for ophthalmologists
and retina specialists involved in the treatment and management of patients with retinal disorders.
LEARNING OBJECTIVESUpon completion of this activity, the participant should be
able to:• Identify and implement algorithms, decision-making tools,
and patient communication approaches that can be used to determine the most appropriate treatment for the patient.
• Identify opportunities to advocate against prior authoriza-tions and step policies and appeal them.
• Discuss the potential impact of the Drug Quality and Security Act and opportunities to advocate for continued access to compounded ophthalmologic drugs.
• Describe the impact of the Medicare Access and CHIP Reauthorization Act (MACRA) on ophthalmology and its potential impact on the prescribing of anti-VEGF agents.
2 SUPPLEMENT TO RETINA TODAY | MAY/JUNE 2018
Identifying and Addressing Market Access Challenges With Anti-VEGF Therapies for Patients With Retinal Disease Release Date: May 2018
Expiration Date: May 2019
DAVID EICHENBAUM, MD, MODERATOR
Clinical Assistant Professor, Department of OphthalmologyUniversity of South Florida College of Medicine
Retina Vitreous Associates of FloridaTampa, Florida
JONATHAN L. PRENNER, MD Associate Clinical Professor, Chairman,
Department of Ophthalmology Robert Wood Johnson Medical School
Rutgers UniversityNJRetina
New Brunswick, New Jersey
LARRY HALPERIN, MD Clinical Professor of Surgery, Ophthalmology,
Florida Atlantic University College of MedicineRetina Group of FloridaFort Lauderdale, Florida
WINSTON WONG, PharmD President, W-Squared Group
Longboat Key, Florida
PAMELA PAUTLER JD, MBA Practice Administrator
Retina Vitreous Associates of Florida St. Petersburg, Clearwater, and Tampa, Florida
FACULTY

GRANTOR STATEMENTSupported through an educational grant from Regeneron
Pharmaceuticals, Inc.
ACCREDITATION STATEMENTEvolve Medical Education LLC (Evolve) is accredited by
the Accreditation Council for Continuing Medical Education (ACCME) to provide CME for physicians.
CREDIT DESIGNATION STATEMENTEvolve designates this enduring material for a maximum of 1 AMA
PRA Category 1 Credit™. Physicians should claim only the credit com-mensurate with the extent of their participation in the activity.
TO OBTAIN AMA PRA CATEGORY 1 CREDIT™To obtain AMA PRA Category 1 Credit™ for this activity, you must
read the activity in its entirety and complete the Pretest/Posttest/Activity Evaluation/Satisfaction Measures Form, which consists of a series of multiple choice questions. To answer these questions online and receive real-time results, please visit evolvemeded.com and click “Online Courses.” Upon completing the activity and self-assessment test, you may print out a CME certificate awarding 1 AMA PRA Category 1 Credit™. Alternatively, please complete the Pretest/Posttest/Activity Evaluation/Satisfaction Measures Form and mail or fax to Evolve Medical Education LLC, 353 West Lancaster Avenue, Second Floor, Wayne, PA 19087; Fax: (215) 933-3950.
DISCLOSURE POLICY It is the policy of Evolve that faculty and other individuals
who are in the position to control the content of this activ-ity disclose any real or apparent conflict of interests relating to the topics of this educational activity. Evolve has full policies in place that will identify and resolve all conflicts of interest prior to this educational activity.
The following faculty/staff members have the following finan-cial relationships with commercial interests:
David Eichenbaum, MD, has had a financial agreement or affiliation during the past year with the following commercial interests in the form of Consultant: Alimera Sciences; Allergan plc; Notal Vision; and Regeneron Pharmaceuticals, Inc. Grant/Research Support: Alcon; Allergan plc.; Clearside Biomedical; Genentech; Novartis; and Opthotech. Speaker’s Bureau: Allergan plc; Genentech; and Notal Vision. Stock/Shareholder: BIRC, Clearside Biomedical; Humera; and US Retina.
Jonathan L. Prenner, MD has had a financial agreement or affiliation during the past year with the following commercial interests in the form of Consultant: Alcon; Genentech; and Regeneron Pharmaceuticals, Inc.
Larry Halperin, MD, has had a financial agreement or affilia-tion during the past year with the following commercial inter-ests in the form of Consultant: Regeneron Pharmaceuticals, Inc.
Pamela Pautler JD, MBA; and Winston Wong, PharmD, have no financial relationships with commercial interests.
EDITORIAL SUPPORT DISCLOSURESErin K. Fletcher, MIT, director of compliance and education,
Susan Gallagher-Pecha, director of client services and project management, Evolve; and Debra Gordon, writer, have no financial relationships with commercial interests. Jaya Kumar, MD, peer reviewer, has no financial relationships with commercial interests.
OFF-LABEL STATEMENTThis educational activity may contain discussion of published
and/or investigational uses of agents that re not indicated by the FDA. The opinions expressed in the educational activity are those of the faculty. Please refer to the official prescribing infor-mation for each product for discussion of approved indications, contraindications, and warnings.
DISCLAIMER
The views and opinions expressed in this educational activ-ity are those of the faculty and do not necessarily represent the views of Evolve, Retina Today, or Regeneron Pharmaceuticals, Inc.
DIGITAL EDITIONTo view the online version of the material, please visit go to
evolvemeded.com/online-courses/.
MAY/JUNE 2018 | SUPPLEMENT TO RETINA TODAY 3

1. RATE YOUR LEVEL OF CONFIDENCE IN IDENTIFYING FINANCIAL ASSISTANCE PROGRAMS FOR PATIENTS WHO REQUIRE TREATMENT WITH A BRANDED ANTI-VEGF COMPOUND:
a. Not at all confidentb. Not very confidentc. Neutrald. Confidente. Very confident
2. RATE YOUR LEVEL OF CONFIDENCE IN PROACTIVELY AVOIDING CLAIM DENIALS OR LATE REIMBURSEMENT:
a. Not at all confidentb. Not very confidentc. Neutrald. Confidente. Very confident
3. RATE YOUR LEVEL OF CONFIDENCE IN DISCUSSING BRANDED AND OFF-LABEL DRUGS WITH PATIENTS:
a. Not at all confidentb. Not very confidentc. Neutrald. Confidente. Very confident
FOR THE FOLLOWING QUESTIONS (4-6) RATE HOW OFTEN YOU ENGAGE IN THE FOLLOWING ACTIVITIES: 5 = ALWAYS, 1 = NEVER
4. I USE DECISION SUPPORT TOOLS IN DISCUSSING THERAPY SELECTION WITH MY PATIENTS: _____
5. I USE SAMPLES WHEN INITIATING THERAPY: _____
6. I INITIATE THERAPY WITH BRANDED AGENTS: ______
7. A PATIENT WITH DIABETIC MACULAR EDEMA (DME) HAS A VISIT THAT INVOLVES THE SELECTION OF AN ANTIANGIOGENIC TREATMENT. ALL OF THE FOLLOWING TASKS SHOULD BE IMMEDIATELY CONDUCTED BY THE OFFICE TEAM, EXCEPT:
a. Verification of insurance benefits to confirm active coverage and patient coinsurance amounts.
b. Review of the insurance carrier clinical policy guidelines on the treat-ment of DME using antiangiogenic medications.
c. Process of a benefits investigation with all of the pharmaceutical companies offering DME medications.
d. Completion of a copay assistance application with the patient.
8. A PATIENT WITH DME HAS A VISIT THAT INVOLVES THE SELECTION OF AN ANTI-ANGIOGENIC TREATMENT. ALL OF THE FOLLOWING WOULD IMPACT THE SELEC-TION OF THE AGENT, EXCEPT:
a. Discussion of FDA-approved versus repackaged agents.b. Clinical evidence and experience with available antiangiogenic
treatments.c. Availability of a manufacturer-supported free drug program and/or
copay assistance for uninsured or underinsured patients.d. Phakic or pseudophakic patient status.
9. THE ASRS HAS SUPPORT FOR RETINA SPECIALISTS AVAILABLE WHEN DOC-TORS ARE CONFRONTED BY STEP THERAPY OR PRESSURE TO UTILIZE CERTAIN AGENTS FROM THIRD-PARTY PAYERS.
a. Trueb. False
10. AN ESTABLISHED PATIENT WITH A MEDICARE ADVANTAGE PLAN IS SCHEDULED FOR AGE-RELATED MACULAR DEGENERATION (AMD) TREATMENT, BUT THE PATIENT IS NOT RESPONDING TO THE CURRENT MEDICATION, AND THE PHYSI-CIAN WOULD LIKE TO INJECT WITH A DIFFERENT MEDICATION ON THIS VISIT. WHAT IS THE BEST APPROACH TO ENSURE APPROPRIATE TREATMENT FOR THE PATIENT AS WELL AS REIMBURSEMENT FOR THE NEW MEDICATION? ADD A CHECK MARK TO THE ITEMS BELOW THAT ARE CONSISTENT WITH YOUR CURRENT CLINICAL PRACTICE.
PRETEST QUESTIONS
Action Consistent Not Consistent
Treat the patient with a sample medication, and perform a benefits investigation for the new medication for future treatments.
Treat the patient with the currently approved medication and schedule for a medication change once a ben-efits investigation is complete.
Treat the patient with the newly rec-ommended medication from inven-tory, bill for it, and perform a benefits investigation before next treatment.
Treat the patient with a sample of newly recommended medication, and bill the drug as stock to see if the car-rier will pay for services rendered.
Reschedule and perform a benefits investigation with the pharmaceuti-cal company’s practice support pro-gram for the new medication.
Ask the staff to contact the insurance carrier immediately to confirm, and document that the new medication is covered, and then proceed with treatment.
Request that the patient signs an Advance Beneficiary Notice for the new medication, and collect from the patient the full allowable rate on the medication after treatment.
Check the carrier’s published clinical policy to confirm the medication is covered for that diagnosis and the patient's plan type does not require an authorization or referral for the change in medication.
Please complete prior to accessing the material and submit with Posttest/Activity Evaluation Instructions for CME Credit.
4 SUPPLEMENT TO RETINA TODAY | MAY/JUNE 2018

MAY/JUNE 2018 | SUPPLEMENT TO RETINA TODAY 5
IDENTIFYING AND ADDRESSING MARKET ACCESS CHALLENGES WITH ANTI-VEGF THERAPIES FOR PATIENTS WITH RETINAL DISEASE
Action Consistent Not Consistent
Treat the patient with a sample medication, and perform a benefits investigation for the new medication for future treatments.
Treat the patient with the currently approved medication and schedule for a medication change once a ben-efits investigation is complete.
Treat the patient with the newly rec-ommended medication from inven-tory, bill for it, and perform a benefits investigation before next treatment.
Treat the patient with a sample of newly recommended medication, and bill the drug as stock to see if the car-rier will pay for services rendered.
Reschedule and perform a benefits investigation with the pharmaceuti-cal company’s practice support pro-gram for the new medication.
Ask the staff to contact the insurance carrier immediately to confirm, and document that the new medication is covered, and then proceed with treatment.
Request that the patient signs an Advance Beneficiary Notice for the new medication, and collect from the patient the full allowable rate on the medication after treatment.
Check the carrier’s published clinical policy to confirm the medication is covered for that diagnosis and the patient's plan type does not require an authorization or referral for the change in medication.
INITIAL TREATMENT Q DAVID EICHENBAUM, MD: We use antiangiogenic
injections in common retinal diseases such as neovascular macular degeneration, diabetic macular edema (DME), and RVO. When we’re considering using these injections, we have three commercially available products to choose from: bevacizumab, ranibizumab, and aflibercept. There is also an expanding array of investigative products. When treating a patient with a common retinal disease, what do you consider when deciding on an initial treatment for that patient, including efficacy and the medical and financial burden of treatment?
LARRY HALPERIN, MD: There are a variety of factors, including, but not limited to, the disease entity and the patient’s insurance, including whether or not the patient can be placed on a copay assistance pro-gram (which most can). A discussion with the patient then takes place concerning branded and off-label drugs, which I try to help direct because most patients will follow whatever we recommend. It results in a conversation around shared decision making (Figure 1).
JONATHAN L. PRENNER, MD: I echo Dr. Halperin’s sentiment. We always attempt to provide patients with as much information as they can handle, but it depends on who the patient is and often what the practice setting is like. For some patients, I’ll present a brief narrative about disease pathology and how you can intervene with any of the three biologics, as there is absent product differentiation, in terms of efficacy. That leads me into a discussion about potential safety issues for branded and nonbranded drugs.
My practice in Princeton, New Jersey, includes a highly educated patient population. For more sophisticated patients, I find myself discussing pharmacodynamics and pharmacokinetics in great detail. I attempt to match the detail of the discussion to what the patient wants to receive and then proceed from there.
DR. EICHENBAUM: Some patients start on FDA-approved anti-VEGF agents, and we have the discussion about cost and coverage at the outset of therapy, while some patients start on bevacizumab. When a decision is made to convert a patient from bevacizumab to an FDA-approved agent, or from one FDA-approved agent to anoth-er, the protocols of most published studies offer lack of efficacy of the initial agent as the indication for converting to a new drug. The decision to convert is often prompted by disease activity, lack of efficacy, or lack of durability,7-11 which is when we convert in clinical practice as well. At that point, we often discuss the financial burden of the FDA-approved agents.
In your practice, Dr. Halperin, what is the next step a patient takes when the decision is made to start with or convert to a higher cost FDA-approved therapy to achieve a better outcome?
DR. HALPERIN: The next step is to have a direct conversation with the patient, which is when I l like to show the patient their OCT to demonstrate where we started and where we are currently. I use the OCT to explain our goal, whether there is subretinal fluid or intra-retinal fluid, or if there is still a hemorrhage in the eye and the vision hasn’t moved.
Identifying and Addressing Market Access Challenges With Anti-VEGF Therapies for Patients With Retinal Disease
The introduction of anti-VEGF agents for the treatment of age-related macular degeneration (AMD), diabetic retinopathy (DR), and retinal vein occlusion (RVO), transformed the management of these conditions. While the clinical benefits of these compounds are well documented, their use brings up other issues for ophthalmologists, namely, cost.1-5 Thus, payers have become more involved in managing the use of these agents, potentially interfering with clinical decision making.6 The following roundtable brings together thought leaders in the retina field to discuss the challenges they face in obtaining access to anti-VEGF medications for their patients and how they overcome those challenges.
— David Eichenbaum, MD, moderator
Figure 1. A Shared Decision Making chart, courtesy of the Agency for Healthcare Research and Quality.

IDENTIFYING AND ADDRESSING MARKET ACCESS CHALLENGES WITH ANTI-VEGF THERAPIES FOR PATIENTS WITH RETINAL DISEASE
6 SUPPLEMENT TO RETINA TODAY | MAY/JUNE 2018
The next step is to discuss other options. Some insurance payers demand the use of a specialty pharmacy, in which case we might have the opportunity to use a sample of a branded drug to initiate treatment and then work through the specialty pharmacy for future treatments. If we don’t have that constraint, we typically will have the patient sign the forms to start engagement with a copay assistance program then initi-ate the change at that visit. We create a schedule to assess the benefit of the change and the time frame for reevaluation.
DR. EICHENBAUM: Who initiates copay assistance or benefits veri-fication, or looks for financial support through a foundation or other organization that provides assistance?
DR. HALPERIN: The technicians involved in seeing the patient, along with myself, will have a brief conversation. Then our front desk and back office staff confirm the insurance and connect patients with enti-ties that provide assistance. We ask most patients to register with those entities as a precaution. It may appear that the patient is covered with Medicare and that they have a good secondary, but there are still issues with copays, whether it’s through deductibles or other costs. Those assistance programs and funds can be very helpful to patients.
DR. EICHENBAUM: What do you do in your practice, Dr. Prenner?
DR. PRENNER: We start many of our patients on branded drugs. Thus, our decision-making process is a bit different as we are commonly going to have to face the issue of cost and financial exposure for our patients up front. When we do convert from one drug to another, I’m less worried about anatomic response than visual response. If patients are seeing well, the presence of a bit of fluid doesn’t concern me enough to convert to another drug.
When we have a new patient come in with exudative AMD, DME, or RVO, and the patient elects to be treated with a branded drug, we immediately perform a benefits investigation. That process is carried out by our front desk and back office staff who assist the patient to determine what their exposure may be. If they are underinsured or uninsured, one of the assistance programs/foundation support pro-grams available may help.
We don’t use samples in our practice; we typically ask patients to return for their initial injection unless there is real pressure to perform the injection the first day, at which point we’ll use bevacizumab.
DR. EICHENBAUM: That’s an important point. Like your practice, Dr. Prenner, I start most patients on a branded drug after a conversa-tion regarding efficacy and safety. We often use samples to initiate treatment, either at that visit or at a visit shortly following the initial diagnosis before the benefits investigation is completed.
Dr. Prenner, why does your practice choose not to use samples?
DR. PRENNER: I think it's uncommon to find a case where there is substantial pressure to treat someone within 48 hours of diagnosis. First, I don’t desire to convert patients back and forth between agents. If I deliver a sample and then discover that they’re not going to be covered
by insurance, I have to then switch them to bevacizumab. The reverse is also true if the patient's preference is to use the branded drug, but we started with bevacizumab.
Second, I want to identify why we are attempting to treat patients on the first day of diagnosis. Important considerations are patient convenience, particularly if you practice in a rural environment. I live in the most populated part of the country, and most of our patients live within 10 miles of our offices. In our location, returning to the office is not a major problem.
Third, when we consider our clinical registration trials of aflibercept and ranibizumab, patients were not treated immediately, and results were excellent.3,4,12,13 Many days passed prior to initiation of treatment, as patients required screening, imaging, and validation/grading of the imaging prior to randomization and treatment.
This should give you confidence that we shouldn’t lose our thera-peutic window if we don’t start treatment immediately. In cases where there is a submacular hemorrhage or a monocular patient, particularly if there was a bad outcome in the fellow eye, I start them on bevaci-zumab. Most patients will do well with their first injection, and I will typically not change their agent at that point.
DR. EICHENBAUM: I agree. There was an abstract from 2017 that looked post hoc at the patients in HARBOR who had treatment initi-ated in window but at different times following screening, and there was no difference in visual outcomes between patients treated at the earliest quartile and the latest quartile (Figure 2). This analysis suggests that patients do not need to be injected the same day as diagnosis to get good results.14
The primary reason we treat the same day in our practice is patient convenience. It comes down to the patient having a general burden of coming back. I think our patients in Florida may be more elderly and more infirm than your patients, Dr. Prenner.
Ms. Pautler, what systems are in place for when we decide to do branded FDA-approved higher cost treatment on a patient, whether as additional therapy or as a conversion? What roles do we have in the
Figure 2. BCVA over time according to the HARBOR Trial.
MAY/JUNE 2018 | SUPPLEMENT TO RETINA TODAY 7
IDENTIFYING AND ADDRESSING MARKET ACCESS CHALLENGES WITH ANTI-VEGF THERAPIES FOR PATIENTS WITH RETINAL DISEASE
offices to ensure that the patient’s exposure is limited and that the practice’s exposure is limited? How can we be as sure as possible that there is coverage for the selection of agents?
PAMELA PAUTLER JD, MBA: At every visit, whether new or established, we verify the insurance information is up to date by checking the insurance benefits. We identify patient copayments, insurance deductibles, and coinsurance amounts. If we know the patient is going to be treated with a specific drug, one of our technicians performs a benefits investigation, and we enroll the patient into a copay assistance program. Once this benefits process is completed we know the patient’s treatment will be fully covered.
The process is disrupted when the physician examines the patient and decides to change the medication from one drug previously autho-rized by the insurance carrier to another. Insurance authorizations are issued for a specific drug CPT code. In this case, we have to pause and use a sample medication; this requires us to redo the whole process to ensure we have an authorization on file for the new drug. Our techni-cians are intimately involved in the process with the patient, so they are well-versed on the insurance benefits, the copay assistance, and the patient’s treatment plan.
DR. EICHENBAUM: Dr. Wong, as a member of the insurance industry, how does this look from the other side of the payer equation? Say a patient comes in and an FDA-approved drug is selected for an on-label indication. Either a sample is used, or the patient is requested to return after the benefits investigation, possibly using one of the support pro-grams from the pharmaceutical company. How does it look from the payer side when that benefits investigation comes through?
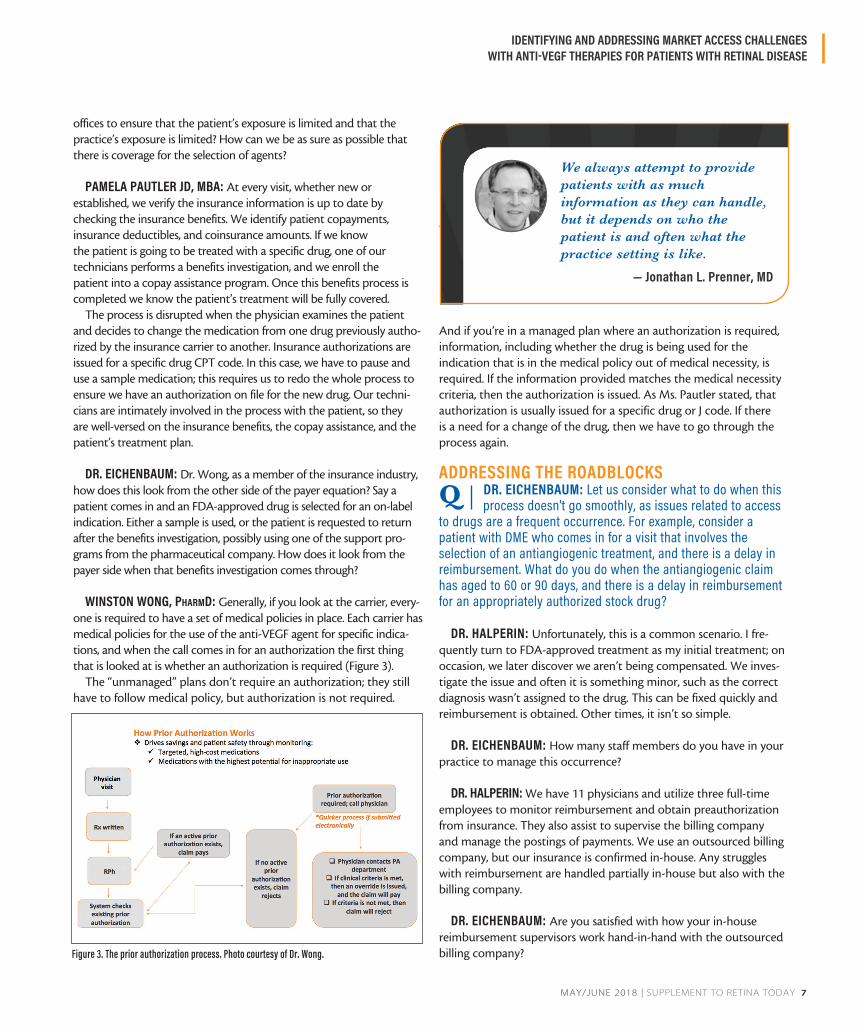
WINSTON WONG, PharmD: Generally, if you look at the carrier, every-one is required to have a set of medical policies in place. Each carrier has medical policies for the use of the anti-VEGF agent for specific indica-tions, and when the call comes in for an authorization the first thing that is looked at is whether an authorization is required (Figure 3).
The “unmanaged” plans don’t require an authorization; they still have to follow medical policy, but authorization is not required.
And if you’re in a managed plan where an authorization is required, information, including whether the drug is being used for the indication that is in the medical policy out of medical necessity, is required. If the information provided matches the medical necessity criteria, then the authorization is issued. As Ms. Pautler stated, that authorization is usually issued for a specific drug or J code. If there is a need for a change of the drug, then we have to go through the process again.
ADDRESSING THE ROADBLOCKSQ DR. EICHENBAUM: Let us consider what to do when this
process doesn't go smoothly, as issues related to access to drugs are a frequent occurrence. For example, consider a patient with DME who comes in for a visit that involves the selection of an antiangiogenic treatment, and there is a delay in reimbursement. What do you do when the antiangiogenic claim has aged to 60 or 90 days, and there is a delay in reimbursement for an appropriately authorized stock drug?
DR. HALPERIN: Unfortunately, this is a common scenario. I fre-quently turn to FDA-approved treatment as my initial treatment; on occasion, we later discover we aren’t being compensated. We inves-tigate the issue and often it is something minor, such as the correct diagnosis wasn’t assigned to the drug. This can be fixed quickly and reimbursement is obtained. Other times, it isn’t so simple.
DR. EICHENBAUM: How many staff members do you have in your practice to manage this occurrence?
DR. HALPERIN: We have 11 physicians and utilize three full-time employees to monitor reimbursement and obtain preauthorization from insurance. They also assist to supervise the billing company and manage the postings of payments. We use an outsourced billing company, but our insurance is confirmed in-house. Any struggles with reimbursement are handled partially in-house but also with the billing company.
DR. EICHENBAUM: Are you satisfied with how your in-house reimbursement supervisors work hand-in-hand with the outsourced billing company? Figure 3. The prior authorization process. Photo courtesy of Dr. Wong.
We always attempt to provide patients with as much information as they can handle, but it depends on who the patient is and often what the practice setting is like.
— Jonathan L. Prenner, MD

IDENTIFYING AND ADDRESSING MARKET ACCESS CHALLENGES WITH ANTI-VEGF THERAPIES FOR PATIENTS WITH RETINAL DISEASE
8 SUPPLEMENT TO RETINA TODAY | MAY/JUNE 2018
DR. HALPERIN: Given the system that we all live in, yes. Ideally, every patient would have an insurance card when they walk in and you would be confident you would be compensated, but that is not our reality. We really do need these people, and they work efficiently.
DR. EICHENBAUM: Many retina specialists, comprehensive oph-thalmologists, and other medical doctors use outsourced billing companies. The companies are often paid based on a percentage of the gross reimbursement. In my experience with outside billing companies, this would essentially eliminate any margin for buy-and-bill drugs and could even create a loss with every drug, unless those drugs are carved out from the billing company as a separate pool of revenue not subject to the same percentage as clinical services. Is that how your billing company works?
DR. PRENNER: You identified a couple of key points. One is that the profitability of using branded drugs is very small. This panel has identified some of the features leading to the somewhat surpris-ing economics involved. One consideration is the human capital required to manage the process of using these agents and limiting loss rate. The second is that many of us use a billing services to man-age our overall billing. Those work quite well for the majority of our work. However, there are going to be claims that don’t rise to the threshold set for automated systems to trigger, which require addi-tional full-time employees to work on those claims. The profitability of using branded drugs appears significant on first inspection, but as you look deep into data surrounding branded drug use, the margins are quite small.
In my practice, we have 18 retina specialists in 15 offices, and we use a publicly traded, independent billing company. It’s very efficient and effective for us. Using these services works well at scale; the exper-tise helps interface with the systems and manage the liabilities of a nonhuman billing process.
DR. EICHENBAUM: Dr. Prenner, how does your practice handle a reimbursement aging 60 to 90 days or an inadequate or incomplete reimbursement for an FDA-approved drug? Does that meet the threshold that you set for these automated claims with regards to financial significance for your practice?
DR. PRENNER: We have three full-time employees who are in charge of billing who manage this process. They determine what the breakdown in the process is and work to solve the problem.
DR. EICHENBAUM: Our practice faces the same issues, but we have five retina specialists and five offices. We frequently have delayed reimbursement or inadequate reimbursement. We have an in-house billing system and use three full-time employees who are devoted completely to billing who also work with these types of claims and delayed reimbursement.
Ms. Pautler, please elaborate on how our practice handles delayed reimbursement or inadequate or underreimbursement.
MS. PAUTLER: We have a robust practice management system, including an electronic health record system. We transmit clean claims within a day and a half of the date of service. In Florida, we have a prompt pay-or-deny statute requiring the carriers to pay or deny a claim within 18 days. If a payment delay occurs because a referral or an authorization wasn’t linked correctly to the claim, this can be quickly corrected and resubmitted to the carrier. We’re seeing insurance carriers deny claims until additional medical information is submitted. We respond quickly and submit those medical records for review. Despite our attempts, the carriers can extend out the number of days they have to process the claim. We typically main-tain an average day of accounts receivable to 20 days.
It becomes a challenge with some insurance carriers making exces-sive requests for medical records or proof of medical necessity. These requests extend the window of time they have to pay the claim even though the claim is clean and well supported. We have a process to follow up 15 to 20 days and document every call made to the carrier. We don’t have many claims denied or delayed, which is proof that our process is working.
DR. PRENNER: If you are efficient on the front end, you shouldn’t see a volume of denials on the back end, but it still occurs. When it does occur, you are best served by an infrastructure in place to deal with it. When you’re completing the volume of treatments that a typical retina practice does, while the incidence rate will be low, the prevalence rate is still going to be fairly high.
DR. HALPERIN: We work hard to manage trends in our billing errors, because the key is to get it right the first time. If we know there’s a payer that is always asking for medical information, we provide that medical information along with the bill, so we can avoid the initial denial. If we don’t get it right on the first try, we look at why and try to determine trends so we can prevent them in the future.
Everyone has a prompt-pay requirement for clean claims in which all required information is provided and no additional information is needed to process the claim. If there’s something missing, it falls out of that prompt-pay time frame. Ensuring that the prior authorization has been obtained in advance helps ensure a 'clean' claim.
— Winston Wong, PharmD

MAY/JUNE 2018 | SUPPLEMENT TO RETINA TODAY 9
IDENTIFYING AND ADDRESSING MARKET ACCESS CHALLENGES WITH ANTI-VEGF THERAPIES FOR PATIENTS WITH RETINAL DISEASE
DR. WONG: In Florida, are most of your issues with commercial plans or with Medicare?
MS. PAUTLER: With the age of our patients and the age-related diseases treated in our practice, the issues are with the Medicare replacement plans. We are also seeing patients with state plans that require special handling. For instance, some plans require that we obtain the drugs through a specialty pharmacy, which adds an addi-tional step in the process.
DR. WONG: Everyone has a prompt-pay requirement for clean claims in which all required information is provided and no addition-al information is needed to process the claim. If there’s something missing, it falls out of that prompt-pay time frame. Ensuring that the prior authorization has been obtained in advance helps ensure a 'clean' claim.
Looking back to the mid-2000s when these therapies first came around, I can see plans being a little more cautious. It’s a costly therapy, especially at that time, and I can see them wanting to have the information to be sure the drugs are being used appropriately. Today, with the open authorizations and medical policies available, if an authorization is required, that information’s already been col-lected. Payment should be made if the claim was submitted clean. If there’s information missing, then you should provide the informa-tion and get paid promptly.
Yes, there may be plans that are more stringent or try to push things through their specialty pharmacy, which should also be con-veyed with the authorization—that you’ll be paid for the drug—but you have to get the drug from a specific pharmacy. This usually occurs to manage the distribution channel to obtain the most cost-effective product versus going on the free market.
DR. EICHENBAUM: To summarize, to reduce the rate of delayed reimbursement or inadequate or underreimbursement by submitting clean claims, use appropriate on-label diagnoses, investigate benefits prior to using a stock medication, check the authorization if required, and comply with specialty pharmacy requirements from certain pay-ers so the stock drug is not tied up in this type of situation.
THE STEP THERAPY DILEMMA Q DR. EICHENBAUM: Let us consider the DME patient, for
whom FDA-approved therapy is recommended. How do you handle a call from the insurance company’s medical director benchmarking off-label treatments or step therapy? Dr. Prenner, do you have any step therapy plans in your practice?
DR. PRENNER: We don’t currently. I think there’s a bit of debate about the validity of those step policies. At the ASRS level there has been an aggressive attempt to reduce these policies by highlighting the importance of physician choice. The ASRS has been very clear that our ability to have physician choice is critical.15
DR. EICHENBAUM: In the absence of step therapy, how often do
you get a phone call from a medical director discussing off-label treatment or asking you to consider off-label treatment?
DR. PRENNER: I have never received one.
DR. HALPERIN: We have this sort of activity in Florida; it comes in a variety of forms, from seemingly inquisitive to more confronta-tional meetings and conversations where you’re asked to explain why bevacizumab is not the first-line drug for all types of macular prob-lems. We ascribe to the ASRS stance that step therapy is a form of forced medical decision making from payers and that the choice of drug should be made between the physician and the patient. Some payers can be quite aggressive.
DR. EICHENBAUM: I agree. In Florida, we have had payers come to our practice with various aggressive tactics to influence the choice of drug. I think that the ASRS does provide appropriate guidance. The ASRS has a series of points that any retina specialist confronted with these discussions can use.16 Additionally, the FDA approves only two commercially-available therapies for common retinal diseases. Between the FDA label and the ASRS guidance, it’s important for retina specialists to know that there is ammunition they can easily access when confronting this type of problem.
Dr. Halperin, how do you handle reauthorization requests or other onerous requests or appeals that are very time intensive for your full-time employees? Do you provide some information up front, or have you looked for trends in your payer environment? Do you outsource that type of work to the billing company? Or do you do that in-house with your billing supervisors?
DR. HALPERIN: I agree that it’s time intensive. Copying paper charts was actually faster. Now that we have electronic records, you have to make sure that all the different parts of the record are included. And it’s not always straightforward.
Certain payers will want documentation to ensure on a very consis-tent basis that we’re following their guidelines and medical decisions,
Certain payers will want documentation to ensure on a very consistent basis that we’re following their guidelines and medical decisions, both as a quality measure for medical care and for any other type of billing issue.
— Larry Halperin, MD
IDENTIFYING AND ADDRESSING MARKET ACCESS CHALLENGES WITH ANTI-VEGF THERAPIES FOR PATIENTS WITH RETINAL DISEASE
10 SUPPLEMENT TO RETINA TODAY | MAY/JUNE 2018
both as a quality measure for medical care and for any other type of billing issue.
When it becomes egregious, it’s a frustrating problem, and we have conversations directly with payers. We have an outsourced consultant we use who will communicate with the payer about these medical information requests. We try and get the medical directors on the phone and take us off their so-called audit list to get the requests down to a reasonable level.
DR. PRENNER: Unfortunately, I think these are becoming more common, and you have to accept that aggressive communication may be required. You are respecting the patient’s wishes for a treat-ment course, and I am confident that by doing so you are in good standing. While there is some paperwork, usually you’ll wind up being approved. I haven’t lost one of those battles yet.
DR. HALPERIN: I agree 100%. We generally don’t lose because we’re always right with what we’re doing on behalf of the patient. But that doesn’t stop the insurer from asking over and over again; it reaches the point of harassment. You may need to engage an attorney to communicate with the payer that their requests are approaching breach of contract and that they’re not entitled to ask for extensive medical information on every patient you see. We are happy to provide an appropriate and reasonable amount of medical documentation.
SWITCHING AGENTSQ DR. EICHENBAUM: Let us consider a patient with wet
AMD who has had a series of treatments with any of the three commercially-available agents. The patient returns after a second attempt at extension to 6 weeks from 4 or 5 weeks. This patient presents with fluid and has now failed two attempts at extension to 6 weeks on agent A. The decision is made to use an FDA-approved agent, whether switching from one FDA-approved agent to the other or switching from bevacizumab to an approved agent. Do any of your situations differ significantly from the following step-by-step fashion?
In our practice, if a patient with a failed extension with drug A is going to be switched to FDA-approved drug B, the patient usu-ally receives an injection with a sample of that drug that day for his or her convenience. Then, the patient discusses options for copay assistance or foundation support with a technician and signs a ben-efits investigation form. We enroll the patient in the manufacturer’s patient support program and have a fairly quick turnaround regard-ing the patient’s insurance benefits.
The patient returns at the next prescribed visit. In this particular scenario, it would probably be 6 weeks or sooner. The patient then often receives stock medication with patient support as provided by the pharmaceutical company. If the patient is on a commercial managed care plan or a Medicare Advantage plan that requires a specialty pharmacy, we’ve obtained the drug, and it’s administered at this visit. The patient is charged for the out-of-pocket coinsurance or copay. We usually settle that charge at the time of service at the
front desk, so we can go on with treatment with this FDA-approved agent, hopefully with further extension and better anatomic and visual outcome for the course of the disease.
DR. PRENNER: Because we prefer not to use samples, our process is to consider changing the therapy the day before implementing the change. If patient responds suboptimally on drug A, at the next visit we would consider additional treatment with drug A or perhaps switching to drug B based on the exam findings. Then, as the patient checks out, we make sure they go through the benefits investigation process for the new drug. That way, we’ll be able to change drugs at the next visit if the findings demand that. And the rest of the process is very similar to what you described.
DR. HALPERIN: Our process is similar for the vast majority of patients treated with a stock drug on the first day. We even make the diagnosis or make a decision to change that day because they have Medicare and a secondary insurance, and we’re very familiar with the secondary and know that everything is going to be fine. We are not using hundreds of samples because many patients can be treated on the day of diagnosis without a problem.
DR. PRENNER: Dr. Halperin, do you treat patients who have not had a benefits investigation if they have Medicare and a supplemental insurance?
DR. HALPERIN: Yes. I’ve always treated the patient on the day of diagnosis, which is the first time I see them. I find patients are appre-ciative because they don’t have to return to the office, and they like knowing we have initiated treatment for their condition. That’s why samples are helpful when we’re skeptical of payment, but, most of the time, we’re not skeptical of payment so we don’t have to use samples frequently.
DR. EICHENBAUM: We do the same. We treat them with stock medication on the day of diagnosis if the patient is a Medicare patient and carries a known secondary. We do verify that secondary is active when the patient checks in.
DR. HALPERIN: I have found that I am less likely to switch between drugs and more likely to work with the interval. I definitely change drugs, but frequently I don't see that it makes a huge difference.
DR. EICHENBAUM: I agree. When looking at the FDA-approved agents, especially in wet AMD, there is more of an interval consider-ation than a product consideration in the vast majority of patients.14 But I do think that the FDA-approved agents probably have some-what more potency, better safety and predictability, and certainly more data than the off-label agent, which is primarily why we use a lot of FDA-approved drugs in our practice.1,17-19
From the provider’s perspective, what do you have at stake in this individual clinical scenario for a wet AMD patient for whom you’re recommending FDA-approved therapy?

MAY/JUNE 2018 | SUPPLEMENT TO RETINA TODAY 11
IDENTIFYING AND ADDRESSING MARKET ACCESS CHALLENGES WITH ANTI-VEGF THERAPIES FOR PATIENTS WITH RETINAL DISEASE
DR. PRENNER: I think the goals are to allow for fair assessment of the pathology, review the relevant data for efficacy and safety, and then allow the patient to make an educated decision in partnership with the doctor. As Dr. Halperin pointed out earlier, many patients will follow what the doctor recommends. Having the flexibility to not be influenced by forces other than data and patient and doctor preference is key. We try to design a process that makes sure there is as little friction as possible so we can spend our time doctoring and as little time as possible on nonpatient care.
DR. EICHENBAUM: From the perspective of the insurance plan, Dr. Wong, what stake do you have when an FDA-approved drug is being recommended for wet AMD? What do you want to see happen in this scenario with the patient?
DR. WONG: Our goal, as stakeholders, in health care is to see the patient treated optimally and receiving the best outcomes they can. As a payer, we also want to see that the optimal clinical outcome is reached in the most cost-effective way. In discussions that I’ve had with colleagues over the past few years, I don’t see this class being managed as tightly as it once was. As I look at the national payers and their policies, they are all covering the branded products. They’re not really showing any preferences one way or another.
However, I’m looking at national commercial products that are paid by employers and individual benefits. That may not necessarily be the same scenario when you get to a more price-sensitive or cost-sensitive line of business, such as Medicare and Medicaid. It may be in those instances that payers are trying to manage more aggressively.
Listening to the discussion for the reauthorization, I would agree that if you have to photocopy the entire chart, as well as possibly have a discussion with a medical director, that is a little onerous. But, using an analogy with oncology, not every health plan has an oncologist on their staff. We don’t have an oncologist as a medi-cal director, so I doubt that the plans are going to have a retinal specialist as a medical director, either. What you may be viewing as an onerous request is really part of a more generic reauthorization process requesting information to determine if the initial regimen has been effective. As a result, the reauthorization request may seem onerous in this disease state, but in other disease states, it may not actually be.
Not to defend the payers, but I don’t believe that any payer is going to intentionally try to overburden you with the reauthoriza-tion process. It’s really designed to be more of a checkpoint in that you received the initial authorization for reimbursement for services. Payers will check in again to confirm it’s a valid indication or it’s medically necessary to continue your patient on that treatment. A payer’s main objective is to see that patients have the best outcomes and to leave the decision making to the retinal specialists.
DR. EICHENBAUM: Ms. Pautler, from the practice administrator view, what should the practice do to achieve the best clinical out-come in this scenario?
MS. PAUTLER: We’re going to do whatever is necessary to sup-port the physician and their decision to treat the patient regardless of the carrier and specific drug. But at the end of the day, there must be a full accounting of all the stock drug inventory and fully sup-ported clean claims submitted in a timely manner to the carrier for reimbursement. We also keep the patient informed and try to limit their potential financial exposure by checking benefits and enrolling eligible patients into copay assistance programs.
DR. EICHENBAUM: To take the perspective of the patient, the patient wants to be better. This sentiment has been shown in the published literature; patient perceptions of their general health and quality of life are profoundly affected by wet AMD.20 If improving vision takes a few more visits or costs somewhat more, our best data imply that patients believe that effort is worthwhile as long as they are getting the best outcome they can for their vision. As a patient, I want to get better, and I want to have trust in my doctor. I want my doctor to be my advocate.
As practice owners or practice administrators, we do have to think of the logistics of delivering care, but when we make decisions as physicians we have to remember that the patients want to trust us, and they want to get better.
From the perspective of the manufacturer, what does the pharma-ceutical company want to do in this scenario?
DR. PRENNER: Pharmaceutical companies believe in their branded products and the efficacy, safety, and track record associated. They want to make sure patients have access to their drugs in a timely fashion, so they are motivated to do what they can within the confines of the regulatory processes in place to assist patients and physicians in retaining the freedom to choose therapeutic direction.
It’s interesting that, as providers, we’re suspicious of the motiva-tions of nonproviders in this process. It’s good to hear Dr. Wong’s commentary suggesting we’re probably more aligned than we think. Some of it may just be certain processes or logistics that we could probably all improve on.
Our goal, as stakeholders, in health care is to see the patient treated optimally and receiving the best outcomes they can. As a payer, we also want to see that the optimal clinical outcome is reached in the most cost-effective way.
— Winston Wong, PharmD

IDENTIFYING AND ADDRESSING MARKET ACCESS CHALLENGES WITH ANTI-VEGF THERAPIES FOR PATIENTS WITH RETINAL DISEASE
12 SUPPLEMENT TO RETINA TODAY | MAY/JUNE 2018
DR. HALPERIN: We may see the payers as this sort of monolithic enti-ty, but they are very large, if not enormous, bureaucracies. While there are parts of these entities that fall in line with some of the notions Dr. Wong said this evening, I would question whether all aspects and all people in the entity fall in line. I would argue that they don’t.
Some medical directors and people involved in helping expedite patient care are really caring and concerned for patient outcomes and patient experience. However, we struggle to convince others in the bureaucracy of these extremely large payers that what we’re doing is right only to find out that another group of people at a level above them don’t respect the opinion of their coworkers. This requires us to go through the whole process again.
DR. WONG: I agree with you from the standpoint that whenever you have more than one person in the room, you are going to have a difference of opinion, and you will have a difference in philoso-phy. And the bigger the organization, the more diversity of opinion and philosophy. You will always find someone in the organization in which everything is a black-and-white situation, and they’re not taking anything in from the clinical aspect or even the opinion of the physician.
From the payer’s side, I could almost say the same thing of physi-cians we’ve talked to. You will find physicians who are genuinely interested in their patients, and they will talk to us and give us their rationale for the treatment regimen, and it’s a very civil, educational discussion. And you have other physicians who say, 'I want to give this regimen because I want to give this regimen,' without any justifi-cation. It’s a give and take on both sides.
As Ms. Pautler stated, you know which payers have the most requirements. Proactive preparation is your best way to work with payers. If you’re proactive and you can provide that clean claim up front, then you’ll reduce the amount of denials and delays down the line. It’s all in that preparation.
DR. EICHENBAUM: What can we do to optimize the outcome
when we select an agent we think the patient will do best with? One with extensive evidence and experience in that retinal dis-ease state? There are a couple of points we discussed that focus on collaboration and efficiency and driving home the best clinical outcome for this patient that we can obtain with commercially available drugs in 2018.
Dr. Wong, you noted the importance of getting things right on the front end when submitting claims. I would submit that prior to that first claim, the initial step when utilizing buy-and-bill drugs is performing the benefits investigation. As discussed, the pharmaceutical companies have services that help with this. They’re easily accessible. Use them; it can take some of the burden off the practice. Always keep the patient’s best interest at heart. We have the ability to manage retinal diseases better today than when I finished my fellowship 10 years ago. And between the agents that we have available and the processes we can put in place to make sure they are accessible, we can get predictable, good outcomes.
CONCLUSIONQ DR. EICHENBAUM: What are the main takeaways from
today’s discussion?
MS. PAUTLER: Once a physician determines the treatment plan, the next step is to identify the insurance carrier and the plan benefits. The practice needs a well-defined process with everyone involved from the front desk to the physician. Every visit requires insurance verification and possibly a new preauthorization, referral, or a specialty pharmacy medication. Communication and coordina-tion are key to clinical efficiency and prompt claim payment.
DR. PRENNER: There is a great deal of synergy between all stake-holders. Working through some of those processes together can be really effective going forward. At the end of the day, everybody wants to do what’s best for each patient, and I think that requires patient and physician choice.
DR. HALPERIN: The patient always comes first. We are obsessed
with patient care, outcome, and experience as well as protecting vision. The reality of the situation is that these medications are not free, and they’re not cheap. But you could argue that the value in a dose of the medication is incredible because we all know what happened to patients before these drugs were available—they lost their vision. We’re fortunate to live in a time of incredible medical advancements, but the advancements cost money. We have to work with the insurance carriers, with our patients, and with our col-leagues to determine how to provide the best care.
DR. WONG: The goals that we all have are very similar. I can’t emphasize enough that it’s crucial to be proactive and have the necessary information readily available, so a clean claim can be sub-mitted. If there is a payer out there who is being difficult, don’t stop voicing your concern. The squeaky wheel will eventually result in someone taking a closer look at your situation and finding a solution. Have an open discussion in terms of what you’re experiencing, and what you see. Payers are not unreasonable. They just have a lot of people they’ve got to talk to.
Whenever you have more than one person in the room, you are going to have a difference of opinion, and you will have a difference in philosophy. And the bigger the organization, the more diversity of opinion and philosophy.
— Winston Wong, PharmD

MAY/JUNE 2018 | SUPPLEMENT TO RETINA TODAY 13
IDENTIFYING AND ADDRESSING MARKET ACCESS CHALLENGES WITH ANTI-VEGF THERAPIES FOR PATIENTS WITH RETINAL DISEASE
DR. EICHENBAUM: Thank you for the discussion. n
1. Martin DF, Maguire MG, Fine SL, et al. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degenera-tion: two-year results. Ophthalmology. 2012;119(7):1388-1398.2. Brown DM, Kaiser PK, Michels M, et al. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1432-1444.3. Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1419-1431.4. Thach AB, Yau L, Hoang C, Tuomi L. Time to clinically significant visual acuity gains after ranibizumab treatment for retinal vein occlusion: BRAVO and CRUISE trials. Ophthalmology. 2014;121(5):1059-1066.5. Diabetic Retinopathy Clinical Research Network, Wells JA, Glassman AR, et al. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema. N Engl J Med. 2015;372(13):1193-1203.6. Allergan, National Association of Managed Care Physicians. Allergan Eye Care Trend Report: Volume 2. www.amcp.org/WorkArea/DownloadAsset.aspx?id=21599. Published 2017. Accessed April 23, 2018. 7. Ashraf M, Banaee T, Silva FQ, Singh RP. Switching Anti-Vascular Endothelial Growth Factors in Refractory Neovascular Age-Related Macular Degeneration. Ophthalmic Surgery, Lasers & Imaging Retina. 2018;49(3):166-170.8. Curry B, Bylsma G, Hewitt AW, Verma N. The VEGF Treatment of AMD Switch Study (The vTAS Study). Asia-Pacific Journal of Ophthalmology (Philadelphia). 2017;6(6):481-487.9. Neves Cardoso P, Pinheiro AF, Meira J, et al. Switch to Aflibercept in the Treatment of Neovascular AMD: Long-Term Results. Journal of Ophthalmology. 2017;2017:6835782.
10. Ricci F, Parravano M, Regine F, et al. Aflibercept in persistent neovascular AMD: comparison of different treatment strategies in switching therapy. Eye (London). 2016;30(8):1077-1083.11. Waizel M, Todorova MG, Masyk M, et al. Switch to aflibercept or ranibizumab after initial treatment with bevacizumab in eyes with neovascular AMD. BMC Ophthalmol. 2017;17(1):79.12. Brown DM, Campochiaro PA, Singh RP, et al. Ranibizumab for macular edema following central retinal vein occlusion: six-month primary end point results of a phase III study. Ophthalmology. 2010;117(6):1124-1133 e1121.13. Heier JS, Clark WL, Boyer DS, et al. Intravitreal Aflibercept Injection for Macular Edema Due to Central Retinal Vein Occlusion. Ophthalmology.121(7):1414-1420.e1411.14. Goldberg RA, et al. Impact of delayed time to treatment on visual outcomes in the HARBOR trial. Paper presented at: ASRS 2017; Boston, Mass.15. Hassan TS. Step Therapy Undermines Physician Choice of AMD Treatment. Retina Today. 2013.16. ASRS. Physician Choice of Medication. 2018; https://www.asrs.org/advocacy/physician-choice-of-medication. Accessed April 28, 2018.17. Yannuzzi NA, Klufas MA, Quach L, et al. Evaluation of compounded bevacizumab prepared for intravitreal injection. JAMA Ophthalmology. 2015;133(1):32-39.18. Goldberg RA, Flynn HW, Jr., Isom RF, Miller D, Gonzalez S. An outbreak of streptococcus endophthalmitis after intravitreal injection of bevacizumab. Am J Ophthalmol. 2012;153(2):204-208 e201.19. Stewart MW. Aflibercept (VEGF Trap-eye): the newest anti-VEGF drug. Br J Ophthalmol. 2012;96(9):1157-1158.20. Submacular Surgery Trials Research G. Patients’ perceptions of the value of current vision: Assessment of preference values among patients with subfoveal choroidal neovascularization—the submacular surgery trials vision preference value scale: sst report no. 6. Arch Ophthalmol. 2004;122(12):1856-1867.

IDENTIFYING AND ADDRESSING MARKET ACCESS CHALLENGES WITH ANTI-VEGF THERAPIES FOR PATIENTS WITH RETINAL DISEASE, PART 1 OF 2
INSTRUCTIONS FOR CME CREDITTo receive AMA PRA Category 1 Credit™, you must complete the attached Pretest/Posttest/Activity Evaluation/Satisfaction Measures Form and mail
or fax to Evolve Medical Education LLC; 353 West Lancaster Avenue, Second Floor, Wayne, PA 19087; Fax: (215) 933-3950. To answer these questions online and receive real-time results, please visit evolvemeded.com and click “Online Courses.” If you are experiencing problems with the online test, please email us at [email protected]. Certificates are issued electronically; please be certain to provide your email address below.
Please type or print clearly, or we will be unable to issue your certificate.
Name ____________________________________________________________________________________ o MD/DO participant o non-MD participant
Phone (required) ______________________________ o Email (required) _________________________________________________________________
Address _______________________________________________________________________________________________________________________
City _____________________________________________________________________ State ____________ Zip ____________________________
License Number ________________________________________________________________
DEMOGRAPHIC INFORMATIONProfession
___ MD/DO
___ NP
___ Nurse/APN
___ PA
___ Other
Years in Practice
___ >20
___ 11-20
___ 6-10
___ 1-5
___ <1
Patients Seen Per Week(with the disease targeted in this activity)
___ 0
___ 1-5
___ 6-10
___ 11-15
___ 15-20
___ 20+
Region
___ Northeast
___ Northwest
___ Midwest
___ Southeast
___ Southwest
Setting
___ Solo Practice
___ Community Hospital
___ Government or VA
___ Group Practice
___ Other
___ I do not actively
practice
Models of Care
___ Fee for Service
___ ACO
___ Patient-Centered
Medical Home
___ Capitation
___ Bundled Payments
___ Other
Training of Fellows ___ Yes ___ No
Release Date: May 2018 Expiration Date: May 2019
DID THE PROGRAM MEET THE FOLLOWING EDUCATIONAL OBJECTIVES? AGREE NEUTRAL DISAGREE
_____ _____ _____
_____ _____ _____
_____ _____ _____
_____ _____ _____
Identify and implement algorithms, decision-making tools, and patient communication approaches that can be used to determine the most appropriate treatment for the patient.
Identify opportunities to advocate against prior authorizations and step policies and appeal them.
Discuss the potential impact of the Drug Quality and Security Act and opportunities to advocate for continued access to compounded ophthalmologic drugs.
Describe the impact of the Medicare Access and CHIP Reauthorization Act (MACRA) on ophthalmology and its potential impact on the prescribing of anti-VEGF agents.
LEARNING OBJECTIVES

1. AFTER REVIEWING THIS ACTIVITY, RATE YOUR LEVEL OF CONFIDENCE IN IDENTI-FYING FINANCIAL ASSISTANCE PROGRAMS FOR PATIENTS WHO REQUIRE TREAT-MENT WITH A BRANDED ANTI-VEGF COMPOUND:
a. Not at all confidentb. Not very confidentc. Neutrald. Confidente. Very confident
2. AFTER REVIEWING THIS ACTIVITY, RATE YOUR LEVEL OF CONFIDENCE IN PROAC-TIVELY AVOIDING CLAIM DENIALS OR LATE REIMBURSEMENT:
a. Not at all confidentb. Not very confidentc. Neutrald. Confidente. Very confident
3. AFTER REVIEWING THIS ACTIVITY, RATE YOUR LEVEL OF CONFIDENCE IN DIS-CUSSING BRANDED AND OFF-LABEL DRUGS WITH PATIENTS:
a. Not at all confidentb. Not very confidentc. Neutrald. Confidente. Very confident
FOR THE FOLLOWING QUESTIONS (4-6) RATE HOW OFTEN YOU ENGAGE IN THE FOLLOWING ACTIVITIES: 5 = ALWAYS, 1 = NEVER
4. I USE DECISION SUPPORT TOOLS IN DISCUSSING THERAPY SELECTION WITH MY PATIENTS: _____
5. I USE SAMPLES WHEN INITIATING THERAPY: _____
6. I INITIATE THERAPY WITH BRANDED AGENTS: ______
7. A PATIENT WITH DIABETIC MACULAR EDEMA (DME) HAS A VISIT THAT INVOLVES THE SELECTION OF AN ANTIANGIOGENIC TREATMENT. ALL OF THE FOLLOWING TASKS SHOULD BE IMMEDIATELY CONDUCTED BY THE OFFICE TEAM, EXCEPT:
a. Verification of insurance benefits to confirm active coverage and patient coinsurance amounts.
b. Review of the insurance carrier clinical policy guidelines on the treat-ment of DME using antiangiogenic medications.
c. Process of a benefits investigation with all the pharmaceutical com-panies offering DME medications.
d. Completion of a copay assistance application with the patient.
8. A PATIENT WITH DME HAS A VISIT THAT INVOLVES THE SELECTION OF AN ANTI-ANGIOGENIC TREATMENT. ALL OF THE FOLLOWING WOULD IMPACT THE SELEC-TION OF THE AGENT, EXCEPT:
a. Discussion of FDA-approved versus repackaged agents.b. Clinical evidence and experience with available antiangiogenic
treatments.c. Availability of a manufacturer-supported free drug program and/or
copay assistance for uninsured or underinsured patients.d. Phakic or pseudophakic patient status.
9. THE ASRS HAS SUPPORT FOR RETINA SPECIALISTS AVAILABLE WHEN DOC-TORS ARE CONFRONTED BY STEP THERAPY OR PRESSURE TO UTILIZE CERTAIN AGENTS FROM THIRD-PARTY PAYERS.
a. Trueb. False
10. AN ESTABLISHED PATIENT WITH A MEDICARE ADVANTAGE PLAN IS SCHEDULED FOR AGE-RELATED MACULAR DEGENERATION (AMD) TREATMENT BUT THE PATIENT IS NOT RESPONDING TO THE CURRENT MEDICATION, AND THE PHYSI-CIAN WOULD LIKE TO INJECT WITH A DIFFERENT MEDICATION ON THIS VISIT. WHAT IS THE BEST APPROACH TO ENSURE APPROPRIATE TREATMENT FOR THE PATIENT AS WELL AS REIMBURSEMENT FOR THE NEW MEDICATION? ADD A CHECK MARK TO THE ITEMS BELOW THAT ARE CONSISTENT WITH YOUR CURRENT CLINICAL PRACTICE.
POSTTEST QUESTIONS
Action Consistent Not Consistent
Treat the patient with a sample medication, and perform a benefits investigation for the new medication for future treatments.
Treat the patient with the currently approved medication, and schedule for a medication change once a ben-efits investigation is complete.
Treat patient with the newly recommended medication from inventory, bill for it, and perform a benefits investigation before the next treatment.
Treat the patient with a sample of the newly recommended medication, and bill the drug as stock to see if the car-rier will pay for services rendered.
Reschedule and perform a benefits investigation with the pharmaceuti-cal company’s practice support pro-gram for the new medication.
Ask the staff to contact the insurance carrier immediately to confirm and document that the new medication is covered, and then proceed with treatment.
Request that the patient signs an Advance Beneficiary Notice for the new medication, and collect from the patient the full allowable rate on the medication after treatment.
Check the carrier’s published clinical policy to confirm the medication is covered for that diagnosis and the patient's plan type does not require an authorization or referral for the change in medication.

Your responses to the questions below will help us evaluate this continuing medical education (CME) activity. They will provide us with evidence that improvements were made in patient care as a result of this activity as required by the Accreditation Council for Continuing Medical Education (ACCME).
Rate your knowledge/skill level prior to participating in this course: 5 = High, 1 = Low __________
Rate your knowledge/skill level after participating in this course: 5 = High, 1 = Low __________
This activity improved my competence in managing patients with this disease/condition/symptom ____ Yes ____ No
I plan to make changes to my practice based on this activity. _____ Yes _____ No
The design of the program was effective for the content conveyed. ___ Yes ___ No
The content supported the identified learning objectives. ___ Yes ___ No
The content was free of commercial bias. ___ Yes ___ No
The content was relative to your practice. ___ Yes ___ No
The faculty was effective. ___ Yes ___ No
You were satisfied overall with the activity. ___ Yes ___ No
Would you recommend this program to your colleagues? ___ Yes ___ No
Please check the Core Competencies (as defined by the ACCME) that were enhanced through your participation in this activity:
____ Patient Care
____ Practice-Based Learning and Improvement
____ Professionalism
____ Medical Knowledge
____ Interpersonal and Communication Skills
____ System-Based Practice
Additional comments:________________________________________________________________________________________________________________________ I certify that I have participated in this entire activity.
Please identify any barriers to change (check all that apply):
____ Cost ____ Lack of consensus or professional guidelines
____ Lack of administrative support ____ Lack of experience
____ Lack of time to assess/counsel patients ____ Lack of opportunity (patients)
____ Reimbursement/insurance issues ____ Lack of resources (equipment)
____ Patient compliance issues ____ No barriers
____ Other. Please specify: ____________________________________________________________________________________
This information will help evaluate this CME activity. May we contact you by email in 3 months to see if you have made this change? If so, please provide your email address below._____________________________________________________________________________________________________________________
ACTIVITY EVALUATION/SATISFACTION MEASURES