i need connection' city life research paper 2010
TRANSCRIPT

‘I NEED CONNECTION’
CITY LIFE HEALTH & WELLBEING
NEEDS ANALYSIS AND SERVICE PLAN
Authors: Crystal McDonald & Janet Reid
Chisholm TAFE Dec 2010

Page 1 of 24
Executive Summary
Research background
This project was undertaken by two Community Development students of Chisholm TAFE Frankston,
under the auspice of the City Life, a Christian charity that works with the homeless and
disadvantaged who describe themselves as having a mandate to ‘support the dislocated people of
Frankston through empowerment, connection and mercy’. The research supported current projects
by the Frankston Homeless Support Service (FHSS) and the Monash Health and Wellbeing
partnership, both committed to finding solutions to the problems faced by the homeless and
disadvantaged people of Frankston. These projects followed research by the Royal District Nursing
service (RDNS) whom identified through the research paper “I Require Medical Assistance” (Everard,
2008) that a Homeless persons program (HPP) was needed in Frankston.
This research followed observations by the above bodies that many of the people who attended City
Life were of poor health or hygiene and the hypothesis that they may have needed better access to
Health Care.
Objectives
The objectives of this report were:
1. To discover what Health and Wellbeing meant to City Lifes clients and identify what they
needed to acheive this.
2. To discuss the barriers to Health and Wellbeing that clients face.
3. To discover what service could help support clients Health and Wellbeing.
Methodology
Research was undertaken using the method of Participatory Action Research (PAR), a process of
social research that looks to improve a particular situation by working closely with all who have a
stake in the outcome, particularly the Critical Reference Group (CRG) who contribute to defining the
issue and identifying possible solutions through discussion of their experiences. This method was
used because it is particularly suited to projects wanting to understand the experiences of the
participants.
The research activities were conducted over a period of 9 weeks (total project taking 4 months
including preparation and reporting stages) with 35 participants during meal times at City Life’s Cafe.
Survey’s were completed with participants to identify the demographic of the people who access
City Life’s services, and indicate any service needs they may have. Secondly, a focus group was run
over four weeks with 2-5 participants where the above objectives were posed as questions to
participants who discussed their experiences and thoughts with the group. Lastly, a forum was held
with 10 self-selected participants to again discuss the above objectives and crosscheck information
obtained through previous stages.
Participants
The CRG in this research were the clients of City Life which consist of a varied demographic, most of
which are single parents, middle aged and elderly people, and people on disability pensions. A total
of 50 people participated in the research activities.

Page 2 of 24
Frankston
City Life is located in the heart of the city of Frankston which has been identified as the 8th most
disadvantaged Local Government area in Melbourne and was recorded as having 775 homeless
people during the 2006 Census (ABS, 2006).
Results
The findings of this research are summarised below:
Of the CRG 100% of clients reported having either a physical and/or mental illness.
94% reported their main source of income as a government pension
57% fell into the status of insecure housing defined by the federal governments definition of
homeless
74% came to City Life between 1-3 times a week
80% reported having a regular Doctor
Wellbeing means having support spiritually, mentally and physically
The CRG require health services to be more Holistic.
66% of participants expressed that they would access dental services
60% wanted a counselling service at City Life
Peer support is important during difficult times
Social connection greatly improves the Health and Wellbeing of CRG.
Family relationships have a great affect on the CRG’s Wellbeing.
CRG desire greater social connection but don’t know how, or lack the confidence to connect.
City Life is the main provider for social opportunities for the CRG.
Doctors appointment s were rushed and did not always treat the clients varied needs
Although research was born out of observations around the Health of City Life’s clients, research
indicated that participants had good access to health care and in most cases regularly visited a
doctor. The emphasis was in fact not on Health but Wellbeing and on the importance of healthy
relationships and social connections to improve health and wellbeing. Participants expressed that
they needed support in connecting better to their families and the community.
Recommendations
The information obtained throughout research suggests that City Life participants need better social
connections - and support to make these connections- to improve their Health and Wellbeing. Due
to the existing connection City Life has with homeless and disadvantaged demographic, and their
geographical location, it is recommended that City Life provide the following:
1. Support groups- to foster peer support and provide an environment to share information
and experiences
2. Social Groups- to improve confidence and social skills and offer an alternative lifestyle
3. Workshops- To educate participants on topics of need
4. Outreach services- To increase access to services and provide appropriate care.

Page 3 of 24
Acknowledgments
We would like to acknowledge the support and guidance of the following people and organisations:
City Life Health & Wellbeing Partnership. This partnership exemplifies true intragrated practice and
the commitment and passion to help those most vulnerable in our city is inspiring.
We would also especially like to mention Kate Sommerville from Frankston City Council, who has helped guide and educate us in forming the survey and approach to health and wellbeing. Mark & Sue Whitby, founders of City Life, who have opened their doors to us as researchers and allowed us to develop what we felt was a hunch. Mark and Sue are community development personified and make an incredible difference in many people’s lives. Finally, Chisholm Institute for their teaching and support as we endeavour to develop ourselves as workers in the field.

Page 4 of 24
Glossary
Acronyms used in this report
CCC Community Care Centre
CD Community Development
CRG Critical Reference Group
CUPSE Community Understanding of Social Exclusion LGA Local Government Area
PAR Participatory Action Research
RDNS Royal District Nursing Service
RDHS HPP Royal District (Nursing Service Homeless Persons Program
SMR Southern Metropolitan Region
Defining Key Concepts
Community Development (CD)
The process of helping a community (or parts of a community) strengthen itself and develop towards
its full potential. Employing techniques and principles such as empowerment, participation &
negotiation.
Royal District Nursing Service (RDNS)
A community nursing service that outreaches to clients in their lived environment. The RDNS
Homeless Persons Program (RDNDHPP) is a specialist unit of this service that seeks to empower
those reciving their care whilst also supporting mainstream healthcare providers to become more
accessible to Homeless people. (2008, p36)
Disadvantaged
People identified as being socially or economically less advantaged than the majority of others in
their community.
Marginalised
People identified as existing on the margins (Outskirts) of mainstream society possibly because they
are possibly disadvantaged in some way or do not follow social norms.

Page 5 of 24
Saturation
The point during research at which you feel you are hearing the same responses or themes often
and therefore can assume this is the most accurate representation of participant’s experiences and
hence may choose to conclude research.
Holistic Care
Acknowledging that there are many elements that influence a persons health and wellbeing and
hence providing care that supports a persons mental, physical and spiritual needs.
Social Inclusion
Social Inclusion is the answer to a problem: Social Exclusion. Exclusion occurs when an individual or
group is “not part of the networks that support most people in ordinary life” (2008).
Homelessness
The Australian Bureau of Statistics define Homelessness in three categories which are summarized
below:
Primary Homeless: People without conventional accommodation i.e.: sleeping on streets (also
known as rough sleeping) or squatting etc.
Secondary Homeless: People who move from one temporary accommodation to another. This
can encompass those staying with friends or family or those in emergency accommodation etc.
Tertiary Homeless: People who live in a boarding or rooming house where they do not have their
own facilities (kitchen or bathroom) and do not have the security of tenure provided by a lease.
All three refer to housing that is insecure and so this report refers to any of these three when using
the term ‘Homeless’.
Need/s
It is the purpose of this research to ascertain participant’s self-defined health and wellbeing needs
and to then identify the services that would best respond to those needs.
The idea of need looks at the kinds of problems that people experience; the requirements for a
particular kind of response; and the relationship between the problems and the responses available
(Everard, 2008 p.8)
Page 6 of 24
Table of Contents
Executive Summary ................................................................................................................................. 1
Acknowledgments ................................................................................................................................... 3
Glossary ................................................................................................................................................... 4
Table of Contents .................................................................................................................................... 6
Introduction ............................................................................................................................................ 8
City Life .................................................................................................................................................... 8
Project Background and History ............................................................................................................. 8
Critical Reference Group ......................................................................................................................... 9
CRG- City Life clients ....................................................................................................................... 9
Frankston City ..................................................................................................................................... 9
Previous Health & Being Research ........................................................................................................ 10
Methodology ......................................................................................................................................... 12
Participatory Action Research (PAR) ................................................................................................. 12
Participation .......................................................................................................................................... 12
Timeline................................................................................................................................................. 13
Stage One: Research Preparation & Collaboration ..................................................................... 13
Preliminary Survey ........................................................................................................................ 13
Stage Two: Research Development (Surveys) and Reflection ..................................................... 13
Stage Three: Research Development (Focus Groups) and Reflection ....................................... 14
Stage Four: Research Development (Forum) and Reflection ....................................................... 15
Stage Five: Analysis and Reporting .............................................................................................. 15
Limitations ............................................................................................................................................ 15
Findings ................................................................................................................................................. 16
General .............................................................................................................................................. 16
Health ................................................................................................................................................ 17
Wellbeing .......................................................................................................................................... 18
Barriers to Health & Wellbeing ......................................................................................................... 18
Solutions for Change ......................................................................................................................... 19
Analysis of Findings ............................................................................................................................... 20
Recommendations ................................................................................................................................ 21
1. Support groups.......................................................................................................................... 21
2. Social groups ............................................................................................................................. 21
3. Workshops ................................................................................................................................ 21

Page 7 of 24
4. Services ..................................................................................................................................... 21
Conclusion ............................................................................................................................................. 22
Bibliography .......................................................................................................................................... 23
References ............................................................................................................................................ 24
Appendicies
One: Survey Results ................................................................................................................. Attached
Two: Focus Group Summaries ................................................................................................. Attached
Three: Evaluation Form ........................................................................................................... Attached
Four: Outdoor Inc .................................................................................................................... Attached
Five: Consent Form .................................................................................................................. Attached
Six: Focus Group Invite ............................................................................................................ Attached
Seven: Blank Survey................................................................................................................. Attached

Page 8 of 24
Introduction
The World Health Organisation (WHO) defines Health as:
‘...a state of complete physical, mental and social well-being, and not merely the absence of disease
or infirmity (World Health Organization, 1948).
What can be gained from this definition is the recognition of the holistic nature of health, which is certainly a positive thing. But if Health is the state of complete achievement of these elements as the World Health Organisation states, most people are a long way off. Unfortunately those living in poverty or with a mental or physical illness are even further removed from this definition of Health. Many ask the question: Which comes first, poverty or sickness? Do people get sick because of poverty or does illness cause them to live in poverty? It is a complex question and regardless of which came first, the fact remains that poverty and illness go hand in hand. City Life, a charity that works with homeless and the disadvantaged, has long considered this dilema and has requested research be done into the Health and Wellbeing of their clientele. This research project has been a partnership between Chisholm Institute under the auspice of the City Life Health and Wellbeing partnership. This report is intended to support the development of concurrent projects of the partnership by providing current information on the Health and Wellbeing needs of City Life’s clients and to explore what services would assist them.
City Life
City Life is a registered Christian charity located in the heart of Frankston which provides support for
the disadvantaged and marginalised. They are not government funded and relies on the income
from their Op Shop, grants and donations to provide their many services. One of the main areas of
support is providing free hot meals four times a week to around 100 people each meal in their Cafe.
City Life also offers support with referral through their Community Care workers as well as
emergency relief, mainly through food parcels. Free internet access and the opportunity for training
is also provided. City Life have a self imposed ‘mandate to support the dislocated people of
Frankston through empowerment, connection and mercy’ and their ethos is to ‘Help People Dream
Again’ (Whitby, 2010)
Project Background and History
A number of agencies and individuals reported concurring observations on the health needs of both
the homeless and those on very low income in Frankston. The first of these agencies to contact City
Life was the Royal District Nursing Service (RDNS) whom identified through research paper ‘I Require
Medical Assistance’ (Everard, 2008) that a Homeless Persons Program was needed in Frankston. At
around the same time, The Frankston Homeless Support Service (FHSS) were planning to provide a
shower for the homeless. These groups both approached City Life as a possible hub for their projects
and an obvious solution was to create a space both could use. The Community Care Centre (CCC)

Page 9 of 24
was created using a shop front at the City Life Centre consisting of a shower, two consulting rooms
and a reception area.
As the discussion developed between City Life, FHSS & the RDNS regarding a joint project, a number
of volunteers who are nurses and work for Monash University observed a need for health care
among the City Life clients. They, like other organisations, noticed clients had issues of basic care
such as hygiene, medication maintanance, as well as diabetes. These volunteers also approached
the leadership of City Life and Monash University with the idea of linking the resources of Monash, -
specifically their Medicine & Science Faculty- to the CCC to contribute to the vision of supporting the
health and wellbeing of City Life clients.
As all these groups came together to form the City Life Health & Wellbeing Partnership, they
developed two main questions to identify the specific needs of the clients and tailor appropriate
referral and services to these needs:
What do the clients at City Life identify as a need to improve their health and
wellbeing?
What services at City Life could help support clients health and wellbeing?
These question form the basis of this report.
Critical Reference Group
CRG- City Life clients
The Critical reference group for this research consisted entirely of City Life clientele, most of which
reside in Frankston City. City Life’s clientele cover a wide demographic including single parents,
families, middle aged men, elderly women, people on disability pensions. According to our survey
results, almost all of them are on Centrelink support and almost all of them would be on the poverty
line. Note: See on ‘Participation’ for information on the selection of the CRG.
Frankston City
The City of Frankston is made up of the suburbs of Carrum Downs, Frankston, Frankston North,
Frankston South, Langwarrin, Langwarrin South, Sandhurst, Seaford and Skye. (Figure 1, 2) It
stretches across 131 square kilometres, and nestles beside Port Phillip Bay, where the suburbs
interface with the Mornington Peninsula. At the time of the 2006 census, Frankston City was home
to 117,801 people and the population is estimated to be growing at 1.69% per year. (ABS 2006,
2007)
Figure 2: Frankston in Greater Melbourne
Figure 1: City Of Frankston Suburbs

Page 10 of 24
Frankston City has been identified as being the eighth most disadvantaged Local Government Area
(LGA) in Melbourne, and Second highest in the Southern Metropolitan Region (SMR). By
comparison, the City of Greater Dandenong has the highest level of relative social disadvantage of all
Melbourne LGAs, the City of Casey is ranked 11th, while Mornington Peninsula Shire is ranked 15th
and the City of Kingston 17th. (Commonwealth of Australia, 2006)
Frankston City also includes some of the most disadvantaged individual suburbs in Victoria.
‘Frankston has the dubious distinction of being one of Melbourne's three most disadvantaged
suburbs while Frankston North, along with twenty-two other suburbs, experiences the highest level
of relative social disadvantage in all of Victoria.’ (Everard, 2008, p. 17)
Analysis of household income levels in Frankston City in 2006 compared to the Melbourne Statistical
Division shows that there was a smaller proportion of high income households (those earning $1,700
per week or more) but a larger proportion of low income households (those earning less than $500
per week). (Frankston City Council, 2010)
As the data indicates, Frankston has a high level of relative social disadvantage which impacts on the
community and the services available within that community.
Previous Health & Wellbeing Research
As we began the process of exploring the Health and Well Being of the clients who attend City Life,
we realised that we were not alone in wanting answers. Finding out what the barriers to achieving
health and wellbeing were and what services could help them overcome those barriers reflected a
question numerous professionals were asking for both their individual regions as well as on a
national and international level.
Measuring the basic needs of an individual to determine if they are disadvantaged does not
necessarily reflect the general wellbeing of a person. As previously stated, the World Health
Organisation defines health as ‘a state of complete physical, mental and social wellbeing and not
merely the absence of disease or infirmity’ (World Health Organization, 1948). This suggests that to
indicate whether a person has health and wellbeing, other factors outside of their physical health
need to be considered.
Peter Saunders former Director of the Social Policy Research Centre (SPRC) at the University of New
South Wales, has spent years researching poverty, income distribution, household needs and living
standards among the most vulnerable of our society. His paper ‘Experiencing Poverty: The Voices of
Low-Income Australians: Towards New Indicators of Disadvantage’(2006) clearly defines new
parameters for assessing basic wellbeing for people. Using a questionnaire tool titled ‘Community
Understanding of Poverty and Social Exclusion’ (CUPSE), Saunders identifies a process to determine
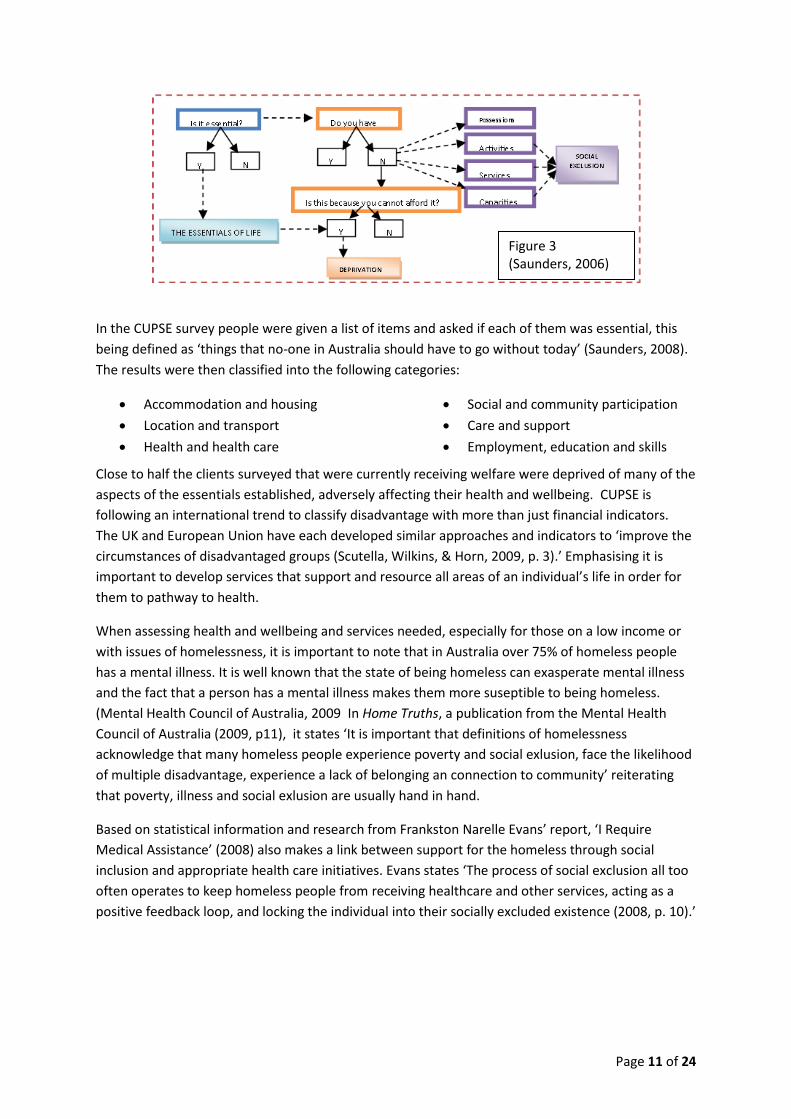
essentials of a person’s life and if they feel they are deprived of those essentials. (see Figure 3)
Page 11 of 24
In the CUPSE survey people were given a list of items and asked if each of them was essential, this
being defined as ‘things that no-one in Australia should have to go without today’ (Saunders, 2008).
The results were then classified into the following categories:
Accommodation and housing
Location and transport
Health and health care
Social and community participation
Care and support
Employment, education and skills
Close to half the clients surveyed that were currently receiving welfare were deprived of many of the
aspects of the essentials established, adversely affecting their health and wellbeing. CUPSE is
following an international trend to classify disadvantage with more than just financial indicators.
The UK and European Union have each developed similar approaches and indicators to ‘improve the
circumstances of disadvantaged groups (Scutella, Wilkins, & Horn, 2009, p. 3).’ Emphasising it is
important to develop services that support and resource all areas of an individual’s life in order for
them to pathway to health.
When assessing health and wellbeing and services needed, especially for those on a low income or
with issues of homelessness, it is important to note that in Australia over 75% of homeless people
has a mental illness. It is well known that the state of being homeless can exasperate mental illness
and the fact that a person has a mental illness makes them more suseptible to being homeless.
(Mental Health Council of Australia, 2009 In Home Truths, a publication from the Mental Health
Council of Australia (2009, p11), it states ‘It is important that definitions of homelessness
acknowledge that many homeless people experience poverty and social exlusion, face the likelihood
of multiple disadvantage, experience a lack of belonging an connection to community’ reiterating
that poverty, illness and social exlusion are usually hand in hand.
Based on statistical information and research from Frankston Narelle Evans’ report, ‘I Require
Medical Assistance’ (2008) also makes a link between support for the homeless through social
inclusion and appropriate health care initiatives. Evans states ‘The process of social exclusion all too
often operates to keep homeless people from receiving healthcare and other services, acting as a
positive feedback loop, and locking the individual into their socially excluded existence (2008, p. 10).’
Figure 3 (Saunders, 2006)

Page 12 of 24
Methodology
This research was conducted following the methodology of Participatory Action Research (PAR), and incorporates elements of Action Research. This method was chosen because of its client-centred focus which was most appropriate to answer the research questions and supports a strengh based approach that considers ‘participant’s as experts in their own situations’ (McCashen, 2005, p. 5)
Participatory Action Research (PAR)
PAR is a process of social research that looks to improve a particular situation by working closely
with all who have a stake in the outcome, particularly the CRG who contribute to defining the issue
and identifying possible solutions through discussion of their experiences. It is the participants who
control the research.
The process of PAR begins with small cycles of planning, acting, observing and reflecting
(Wadsworth, 1991 p79) and continues until the research question has been satisfied. However, it is
common for PAR to be perpetual, constantly evaluating and improving practices.
Through reflection on a current situation, an issue is identified ‘as a hunch’ by Researchers who
begin looking at why it exists and how the situation could be better- it is here that they identify the
research question/s.
Researchers then begin to find out what others think about the issue by identifying 4 conceptual
parties or Stakeholders:
Conceptual Parties Project specific Stakeholders
1) Who or what is to be “researched”? Current City Life ‘clients’ and their Health & Wellbeing needs
2) Who is to be the researcher/s? Students/Employees of City Life, Monash Partnership
3) Who is to benefit? (Referred to as the Critical Reference Group (CRG))
City Life clients
4) Who needs to know? City Life, Monash University, RDNS, Funding bodies
By working collaboratively with other parties involved in the issue, PAR attempts to minimise
‘resistance to change and to also understand where resistance may be rooted in conflicting views
and competing kinds of practice(Wadsworth, 1991 p79.)’. Through this collaboration, researchers
identify a common ground around the interests of the CRG.
Active participation (by the group who’s “issue” is being addressed) is the key to this research and
the input of participants constantly reshapes research direction and outcomes.
Participation
PAR starts with a small group of collaborators, but widens the community of participants so that the
research gradually includes more and more of those affected by the practices (or issue) in question
(Wadsworth, 1991 p79.).

Page 13 of 24
This project has attempted to involved participants incrementally, starting with one group and
widening the scope of participation through various research activities.
Researchers for this project sourced participants by making announcements during meal service at
City Life’s café –at each stage of implementation- requesting to speak with interested people. Their
participation was voluntary and could be withdrawn at any time. See ‘Timeline’ below for more
information on participation at each stage.
Yoland Wadsworth (1991, pg. 81) offers this explanation of PAR, which highlights the focus on active
participation,
‘In order to find out what people think and value, what things mean, to them, we need to
engage fully in a process of immersion of their /our worlds. We observe, read, listen,
interact, participate, question, and listen again, exploring meanings of feedback until we
reach effective understanding. We can ask very open questions at first, gradually refining
them as our hunches get challenged or confirmed.’
Timeline
This research was conducted over a period of 4 months and was implemented over five stages:
Stage One: Research Preparation & Collaboration
Approximately 3 weeks
Stage one of this project focused on planning and collaboration. Researchers from City Life met with
Monash partnership and discussed the aims of the Community Care Centre and the areas in which
further research would benefit the project. Previous observations surrounding clients Health and
Wellbeing were discussed and ‘hunches’ about the cause of the identified issues were explored,
which led to the development of the research question.
To gather further insight into the current situation, a survey was produced that would identify the
demographic of the people who access City Life’s services, and indicate any needs they may have for
further services.
Preliminary Survey
These surveys were trialled in the Café with interested participants, and then small adjustments
were made to improve the relevance and workability of questions.
Stage Two: Research Development (Surveys) and Reflection
Approximately 4 weeks
The final survey was also implemented in the Café during meal times with interested participants to
gain information in the following areas:
Age, Gender & Suburb
Main source of income o If this income was sufficient o In what areas could they benefit from assistance

Page 14 of 24
Employment status
Accommodation situation
Family situation
How often they attend City Life
What City Life services do they use
Health o Frequency of Doctor visits o If they had a regular doctor o Last time they visited Emergency
Where they go to for help/support
Would they use the Shower at City Life
What services they would like City Life to offer Overall, 35 participants completed the surveys with the researcher over several meal times in the
Café. Although a quantitative method, the surveys became a catalyst for conversation around
Health and Wellbeing where qualitative information was also recorded. These ‘interviews’ lasted
between 15-40minutes each.
Surveys were then collated and a Survey Results document (Appendix One) was produced. This data,
along with Qualitative information, was discussed with the Monash Partnership and the appropriate
questions for stage three were designed.
Stage Three: Research Development (Focus Groups) and Reflection
Approx 4 weeks
An announcement was made during meal service and individuals were approached similarly to Stage
Two. After a brief introduction, interested clients were invited to join the Focus group. 5 clients were
listed, however only four arrived for session 1 and only two for sessions 2,3 & 4.
These groups were conducted over 4 weeks and the following questions were used to provoke
discussion about the participant’s experiences:
Phase One: What is Health & Wellbeing?
Focus: Establish the client’s perception of Health & Wellbeing, and what they identify as
needs. Additional to obtaining specific health information of individuals it was important to
allow participants to define what Health & Wellbeing was for them.
Phase Two: What are the Barriers to achieving Health & Wellbeing?
Focus: Discuss what stops clients from fulfilling their identified needs,
Phase Three: What services could be provided (or improved) to overcome these barriers?
Focus: List ideas for new services or service improvements that would help clients achieve
their identified needs.
Evaluation forms (Appendix Three) were also completed during phase three and the participants
were offered a Certificate of Appreciation for their time and effort.
Notes were taken at each of the Focus Groups and were checked by participants for their accuracy.
These session summaries are included in this report (Appendix Two).

Page 15 of 24
Stage Four: Research Development (Forum) and Reflection
Approx 1 week
Clients of City Life were asked to stay behind after their meal to participate in a forum on Health &
Wellbeing. Approximately 10 people of varying age and gender participated.
The purpose of this one-off session was to extend the research questions to a wider audience by
providing an alternative platform in which clients might feel more comfortable participating. Being
the third research activity of the project, this stage provided the opportunity for researchers to
‘crosscheck’ the information previously provided by clients to find areas of similarity or difference.
After reflecting on the outcome of stage two, questions were simplified and presented to the Forum
as follows:
1. What is Health & Wellbeing? 2. What stops us? (from achieving it) 3. What services could help? (to achieve this)
For the purpose of keeping to time constraints, examples from previous stages were offered with
each question to get conversation going. All responses were brainstormed on the whiteboard.
The information gained at every stage was recorded and reviewed before the commencement of the
following stage, with alterations made where necessary. In this way, researchers ensured the
research was driven by the participant’s experiences and not by the preconceived ideas of the
facilitators.
Stage Five: Analysis and Reporting
Approx 4 weeks
At the completion of each Research activity, findings were reviewed and discussed by project
workers to ascertain the level of saturation achieved and to set the goals for further activities. These
incremental findings were also provided to committee members at committee meetings where
possible.
All information obtained over the course of this research was collated and analysed over a period of
two weeks and a final findings summary was provided to all stakeholders.
Limitations
This research project was undertaken by two project workers over a four month time frame. These
workers were also employed and volunteering at City Life respectively. It is possible that this
involvement with City Life created some personal bias for the workers.
This also effected the time available to the workers to undertake research activities within working
hours. Further research would benefit from a full time project worker who was employed solely for
the purpose of undertaking the research thereby allowing them ample time to dedicate to research
activities and more opportunity to carry them out with a wider clientele base.

Page 16 of 24
Additionally, this project was undertaken to support current projects by two existing committees,
surrounding the Health & Wellbeing of City Life’s clientele and the homeless people of Frankston
respectively. These two committees each consist of representatives from several organisations,
including City Life. For the research project to be a useful tool in the implementation of their
projects, the research had to satisfy the needs of their many stakeholders, thus creating some
limitation to the project workers’ freedom and the PAR process.
Random sampling was not a feature of this study. Participants in this research were invited to
participate and then they self selected into each activity. Due to the varied nature of client’s health
issues, a more private approach to gaining information may have been more beneficial.
Furthermore, it became increasingly difficult to gain interested participants for research activities
during the course of this project contributing to a relatively small sample size which limits the ability
of the results to be generalised to a larger community.
Literacy skills varied between participants but more often than not, participants were unable to
either read the survey or write their answers. This increased the time necessary to complete each
survey and this consequently affected the amount of surveys researchers were able to complete in
the allowed time frame which also contributed to a smaller sample size than hoped.
Finally, throughout the focus groups it became apparent that participants were not attending to
simply participate in research; they were attending for the value of being a group and connecting as
individuals. The research activities were for them, an exercise in social inclusion which gave them
great satisfaction. In reflection this aspect was not sufficiently taken into account by facilitators and
may have influenced the outcome.
Note: This observation was confirmed during the evaluation session when participants disclosed the
value of group participation for them and the process they went through personally to achieve this
level of connection with others.
Findings
Note: Please see Appendices One and Two for a full record of Findings
General Clients of City Life consist of a varied demographic. Those who participated in research were equally
represented by each gender and almost all of them had children. Income was mostly from
government pension and in most cases was not sufficient to meet their needs.
Average age of 46
68% lived in Frankston Council
86% of those with children did not live with them
43% were on a disability pension
94% reported their main source of income as a government pension
57% fell into the status of insecure housing defined by the federal governments definition of homeless

Page 17 of 24
When participants were asked if they were in a situation of stress or harm (where they needed some
support or going through a rough time) where would they go for help, the most common response
was they would not speak to anyone but try and deal with the crisis themselves. As a last resort they
would go to family followed by their Doctor. When discussing why they would not seek assistance
they gave the following responses:
“I don’t trust anyone”
“It’s a pride thing, you just don’t go to others for help, you sort it out yourself”
Although most felt their issues were private, it was observed and often directly stated that
participants came to City life for the social connection and peer support it provided more
than any other reason.
74% came to City Life between 1-3 times a week
89% came for the café
63% accessed emergency relief food parcels
Health
Of the CRG 100% of clients reported having either a physical and/or mental illness. The below chart
displays the health issues reported by the CRG:
80% reported having a regular Doctor
77% had visited a Doctor in the last 3 months
23% had been to the Hospital Emergency in the last 3 months
Though many clients regularly visit their medical professional, it was stated that visits were short and
not necessarily holistic in their approach especially when dealing special or varied needs.
The most significant health service request was dental care with 66% of participants expressed that
they would access dental services if provided at City Life.
Health Issues
Depression
Dental
Arthritis
Asthma
Blood pressure
Diabetes
Heart Disease
Other

Page 18 of 24
Other health services participants would like to access at City Life were:
60% wanted a counselling service
40% wanted nutritional support/education
31% wanted a podiatry service
31% wanted a physiotherapy service
Wellbeing
Participants were very open to discussing their experiences and needs and described health and
wellbeing as follows:
‘To have a healthy life, to be happy and well and be good to others’
‘To be able to ask for help, not to dwell on the past but look to the future’
‘Happy and be able to help other people. Hope for the future. Have a good life and then
contribute to others people’s good life.’
It was identified that positive family relationships was the most significant contributor to their
health and wellbeing. It was also stated that to experience wellbeing meant having support
spiritually, mentally and physically.
Participants stated the following places they seek support from:
City Life
Church
Frankston Information and Community Support
Medical Professionals
Life-partner
Centrelink
Barriers to Health & Wellbeing
In defining the barriers participants experienced, four key areas were identified:
Physical Health:
Finances- effects nutrition and food choices
Unhealthy Habits
Lack of Motivation
Exercise- inability to exercise due to mental and physical illness
Mental Health:
Stress
Injury
“Medication prescribed for one condition can cause issues in another area”
Motivation
Losing hope – due to lack of control
Family disconnection/breakdown
Inappropriate diagnosis/care
Page 19 of 24
Social Health:
Isolation- “thinking you’re the only one in that situation.”
Lack of knowledge about services
Inability to articulate
“When you’re paranoid from past experiences” General Barriers affecting all Health and Wellbeing:
Family disconnection
Shyness/”A phobia of asking for help”
Communication – “can’t explain what’s wrong with you”.
Negative/unhealthy communication
Lack of control over personal situations
Feeling your powerless to change situation
Complicated forms
Solutions for Change
Participants provided the following suggestions for the improvement or provision of services to
improve Health and Wellbeing:
Physical Health:
Education on healthy food on a budget
Doctor can only do so much, need specialist access
More bulk-billing doctors needed locally – can’t afford transport to existing doctors.
Happy with own (full fee) Doctor but need financial assistance to pay for it.
Need ongoing self care advice
Meals on wheels
Somebody to steer in right direction to get right services
Dietician- (participant has used before and found really helpful but ran out of money)
Having someone to exercise with, get you up. –Personal trainer/motivator
Having a dog to walk (companionship, responsibility)
Discussed walking group/ daunting in a group. Different ability levels
Mental Health:
Psychologist /Counsellors-It was stressed by participants that the worker need to be the right person for the job and needed to understand clients perspective and provide a safe, private, comfortable environment
Referral service to appropriate care
Education on alternative health options
Education about your condition/s
Drug education /discussion group.
Social Health:
More small groups
6- 8 people is comfortable
Mix of Sexes
Supply food Ideas for groups
Divorce/Separation support group
‘People with similar problems’
Walking

Page 20 of 24
Craft
Community Kitchens
Participants discussed the importance of peer support during difficult times and as a catalyst for
better social connection.
“You look for comfort, attention and understanding.”
“Group sessions to discuss personal hardships with other people with similar problems and
situations in a controlled environment.”
Analysis of Findings
Participant’s responses to the survey were limited to the questions asked, however the qualitative
information obtained from this process proved consistence with the themes that arose during later
stages:
Social connection greatly improves the Health and Wellbeing of CRG.
Family relationships have a great affect on the CRG’s Wellbeing.
CRG desire greater social connection but don’t know how, or lack the confidence to connect.
City Life is the main provider for social opportunities for the CRG.
‘Mental and Dental’ are the greatest health care needs of CRG.
The CRG require health services to be more Holistic.
Due to this research being born out of an observation that the clients of City Life were in poor
health, there was expectation that research would uncover gaps in health care. It is important to
note that this assumption was not validated due to clients reporting good health care access. This
instead suggests that the issue is the standard of the health care being provided.
A common response from participants is that appointments were ‘rushed’ and that the doctors don’t
ask the appropriate questions or only treat them for the obvious issue and don’t look at the larger
picture such as the cause of the issues. This identifies a need for Holistic care.
There was a strong emphasis on the importance of healthy relationships and social connections to
improve health and wellbeing. Participants expressed that they need support in developing skills
and pathways to help them connect better to their families and the community.
The enjoyment and benefit participants reported from participating in focus groups, was a good
indication that groups improve people’s social connection skills.

Page 21 of 24
Recommendations
The suggestions offered by participants, and the information obtained throughout this research have
been combined to make the following recommendations:
1. Support groups
Run by/at City Life- To foster peer-support and provide an environment to share information and experiences.
Parents with part time or no access to their children
Parenting groups
Divorced/separated people
Living with a mental illness
2. Social groups
Run by/at City Life in partnership with other community groups- To improve confidence and social skills and offer an alternative lifestyle
Craft
Day outings
Outdoor recreation
Walking
Arts Programs
3. Workshops Run at City Life in partnership with other service providers.- To educate participants on particular topics of need
What to do when things get tough: Housing options and process
Building healthier/stronger relationships
Being assertive and in control
Increasing motivation and confidence
Healthy food on a budget
4. Services
Run as an outreach service by Monash University and other service providers from the CCC.- To increase access to services and provide appropriate care
Financial counsellor
RDNS Nurse
Community Dentist
Mental Health worker
Referrals (Including connection to other services above) Due to the frequency of CRG’s attendance at City Life, the Community Care Centre would be an ideal
location for the provision of services. City Life also have ample space within premises to house
Workshops and support groups. Depending on the level of expertise required, these groups could be
run by volunteers or by linking in with other service providers to share facilitation.
Social groups should ideally be provided firstly from City Life, and then branch out further as
participants confidence improves. Utilising other service providers for outings such as Outdoor Inc.
(Appendix Four) would provide a specialist service to participants whilst not requiring too many
resources from City Life.

Page 22 of 24
Conclusion
If Health is the state of ‘complete physical, mental and social well-being...’ (WHO), we must pay
equal consideration to our mental state and level of wellbeing as we do to our physical. This
research has indicated that not only is a holistic appraoch to health crucial, but that the other
elements of this holistic approach (mental health and wellbeing) rely heavily on the individuals level
of social connection. It is therefore imperitive that social inclusion is a key consideration to all health
providers, and that the mental and social aspects of a persons situation are acknowledged with the
physical.
Although this report acknowledges the links between poverty and illness, the findings reflect that it
is social inclusion that can mitigate the effects caused by these conditions and therefore greatly
increase a person’s wellbeing.
City Life, with its strong existing connections to the homeless and disadvantaged people of
Frankston, and partnerships with leading community organisations, is the most suitable location at
which to implement socially inclusive programs and services. Being located in the second most
disadvantaged community in the Southern Metropolitan Region, suggests that there is a great
opportunity to connect with some of the region’s most disadvantaged, thus improving the Health
and Wellbeing of the community. A continued partnership with the FHSS, Monash university, and
RDNS would greatly benifit the outcomes of such programs.
The people of City Life have shared thier needs and voiced thier wishes. They want services that give
them appropriate care, and connection to the community around them. In other words:
‘The I in Illness is isolation and the crucial letters in wellness are we.’ (Guarneri, 2007)
Page 23 of 24
Bibliography
AustralianBureau of Statistics 2006, 1301.0-Year Book Australia, 2006, Retrieved April 14, 2009, from
http://www.abs.gov.au/ausstats/[email protected]/46d1bc47ac9d0c7bca256c470025ff87/bfdda1ca
506d6cfaca2570de0014496e!OpenDocument
Australian Institute of Health and Welfare 2010, Mental health services in Australia 2007–08,
Retrieved November 8, 2010, from Australian Institute of Health and Welfare:
http://www.aihw.gov.au/publications/hse/88/11415.pdf
Commonwealth of Australia 2006, Socio-Economic Indexes for Areas (SEIFA), Retrieved Oct 15, 2010,
from Australian Bureau of Statistics: http://www.abs.gov.au/AUSSTATS/[email protected]
/DetailsPage/2033.0.55.0012006?OpenDocument
Cooper, L 2004, Dilemmas in Working with Women with Complex Needs, Retrieved on 15 Oct, 2010
from: Department of Family and Community Services:
http://www.facs.gov.au/sa/housing/pubs/homelessness/saap_er_publications/dilemmas_w
omen_complex/Pages/default.aspx
Everard, N 2008, I Require Medical Asistance, Royal District Nursing Service, Melbourne
Frankston City Council 2010, Frankston City- What is our weeklyhousehold income?, Retrieved Oct
2010, from Frankston City Council:
http://profile.id.com.au/Default.aspx?id=111&pg=107&gid=10&type=enum
Guarneri, M 2007, The Heart Speaks: A Cardiologist Reveals the Secret Language of Healing, Simon &
Schuster,New York.
McCashen, W 2005, The Strengths Approach, St Luke's Innovative Resources, Bendigo.
Mental Health Council of Australia 2009, Home Truths: Mental Health, Housng and Homelessness in
Australia, Mental Health Council of Australia.
Saunders, P & Sutherland, K 2006, Experiencing Poverty: The Voices of Low-Income Australians,
Towards New Indicators of Disadvantage Project Stage I: Focus Group Outcomes. University
of New South Wales: Social Policy Research Centre, Sydney.
Page 24 of 24
Saunders, P Naidoo, Y & Griffiths, M 2007, Towards New Indicators of Disadvantage: Deprivation and
Social Exclusion in Australia, Social Policy Research Centre, Sydney
Scutella, R, Wilkins, R, & Horn, M 2009, Measuring Poverty and Social Exclusion in Australia: A
Proposed Multidimensional Framework for Identifying Socio-Economic Disadvantage,
Melbourne University: Melbourne Institute of Applied Economic and Social Research,
Melbourne Retrieved 10 Oct 2010 from:
http://papers.ssrn.com/sol3/papers.cfm?abstract_id=1639867
United Nations 2010, The Universal Decleration of Human Rights, Retrieved Oct 30, 2010, from
United Nations: http://www.un.org/en/documents/udhr
Whitby, Mark. Personal Interview. 9TH October, 2010. World Health Organization 1948, WHO Definition of Health, Retrieved Sept 10, 2010, from World
Health Organization: http://www.who.int/about/definition/en/print.html
References
Everard, N 2008. I Require Medical Asistance. Royal District Nursing Service p.10., Melbourne
Fleuret, S & Atkinson, S 2007, Wellbeing, Health and Geography: A critical review and research
agenda, New Zealand Geographer, vol 63, pages 106-118
Saunders, P 2008, Measuring Wellbeing Using Non-Monetary Indicators, Family Matters, No.78, pp.
8-17.
Saunders, P 2010, Identifying the Material and Non-Material Ingredients of the Good Life, Australian
Journal of Social Issues, Vol. 45 (1), 53-69.
Wadsworth, Y 1991, Everyday Evaluation on the run 2nd Ed. Action Research Issues Association Inc.,
Melbourne. p.79.