hypoglycemia, electrolyte disturbances and acid-base...
TRANSCRIPT
Hypoglycemia,Electrolyte disturbances and acid-base
imbalances
Pediatric emergency – PICU division
Pediatric department
Medical faculty, University of Sumatera Utara –
H. Adam Malik Hospital
1

Hypoglycemia
Def : Plasma glucose < 45 mg/dL
sweating, trembling, feeling of warmth, palpitations,anxiety, nausea, hunger, blurred or double vision,weakness
Neuroglycopenic sypmtoms with prolonged hypoglycemiaNeuroglycopenic sypmtoms with prolonged hypoglycemia� dizziness, confusion, tiredness, difficulty speaking,
headache, inability to concentrate, nightmares,bizzare behaviour
Criteria diagnostic for insulinoma (Whipple triad):- Hypoglycemic symptoms in fasting or exercising state- Low plasma glucose level- Relief of symptoms through correction of hypoglycemia2

Insulin and C-peptide levels may help determine cause
In nondiabetic hospitalized patients common etiologiesinclude :- Renal insufficiency- Malnutrition- Liver disease- Liver disease- Infection- Sepsis
Other causes : alcoholism, adrenal insufficiency, medications(insulin, sulfonylurea, pentamidine, trimethroprim –sulfamethoxazole, salycilates, beta-blocking agents),insulin-secreting tumors.
3
Differential Diagnosis :
o Deliriumo Pheochromocytomao Factitious hypoglycemiao Liver failureo Psychoneurosiso Sepsis syndromeo Sepsis syndromeo Myxedema coma
4

Treatment :
- Glucose IV or orally (if awake & alert)Glucose 10% � 5 ml/KgBW
- Monitor blood glucose closely as patients may need continousdextrose infusion until precipitating cause removed- Glucagon & hydrocortisone can be given for refractoryhypoglycemia- Identify & treat underlying disease or remove causative agent
5
Electrolyte disturbances
6
• Normal plasma level:133–144 mmol/l
Hypernatraemia (greater than 150 mmol/l)
• Causes: vomiting/diarrhoea, excess water loss (e.g. diabetes
insipidus, osmotic diuretics, burns), high sodium intake, iatrogenic
SODIUM
insipidus, osmotic diuretics, burns), high sodium intake, iatrogenic
fluid restriction (often combined with drugs containing sodium, near
drowning (seawater)
• Presentation: lethargy, irritability, coma, seizures
7
Hypernatremia cont’..
• Treatment
• treat underlying cause
• slow rehydration using sodium containing fluid, e.g.
0.45% saline with dextrose (over at least 48 h). May
need 0.9% saline.
• reduction of sodium level slowly 0.5–1 mmol/l/h• reduction of sodium level slowly 0.5–1 mmol/l/h
• desmopressin (DDAVP) can be used in diabetes
insipidus to reduce water loss
8

Hyponatraemia
• Causes
• Inappropriate ADH secretion – decreased water clearance
• Water overload, e.g. iatrogenic, nephrotic syndrome
• Excessive sodium loss (e.g. diuretics, renal tubular dysfunction,
diarrhoea and vomiting)
• Fluid sequestration, e.g. sepsis, burns
• Symptoms: range from non-symptomatic through lethargy to coma, • Symptoms: range from non-symptomatic through lethargy to coma,
nausea and vomiting, seizures usually below 125 mmol/l
• Therapy
• fluid restriction as therapy
• if symptomatic, 3% NaCl to return plasma sodium to 125 mmol/l
6 ml/kg of 3% saline increases body sodium by about 5 mmol/l
9
POTASSIUM
Normal serum level is 3.5–5.5 mmol/l
Hypokalemia
• common causes: diarrhoea, alkalosis, diuretics, volume depletion,
hyperaldosteronism, beta adrenergic agonists in asthma
• signs: ECG changes:T wave inversion, ST depression, predisposition to
dysrhythmias, skeletal and smooth muscle excitability and weakness
• treatment: the cause, oral or IV replacement
10

Hyperkalemia
• causes: renal failure, metabolic acidosis, adrenal insufficiency, cell lysis,
high intake
• hyperkalemia can be accompanied by hypovolaemia in sepsis
• Signs and symptoms:
• risk of arrhythmias particularly levels above 7.5 mmol/l – can proceed to • risk of arrhythmias particularly levels above 7.5 mmol/l – can proceed to
cardiac arrest
• peaked T waves, decreased R waves, widened QRS complex
• muscle weakness
11
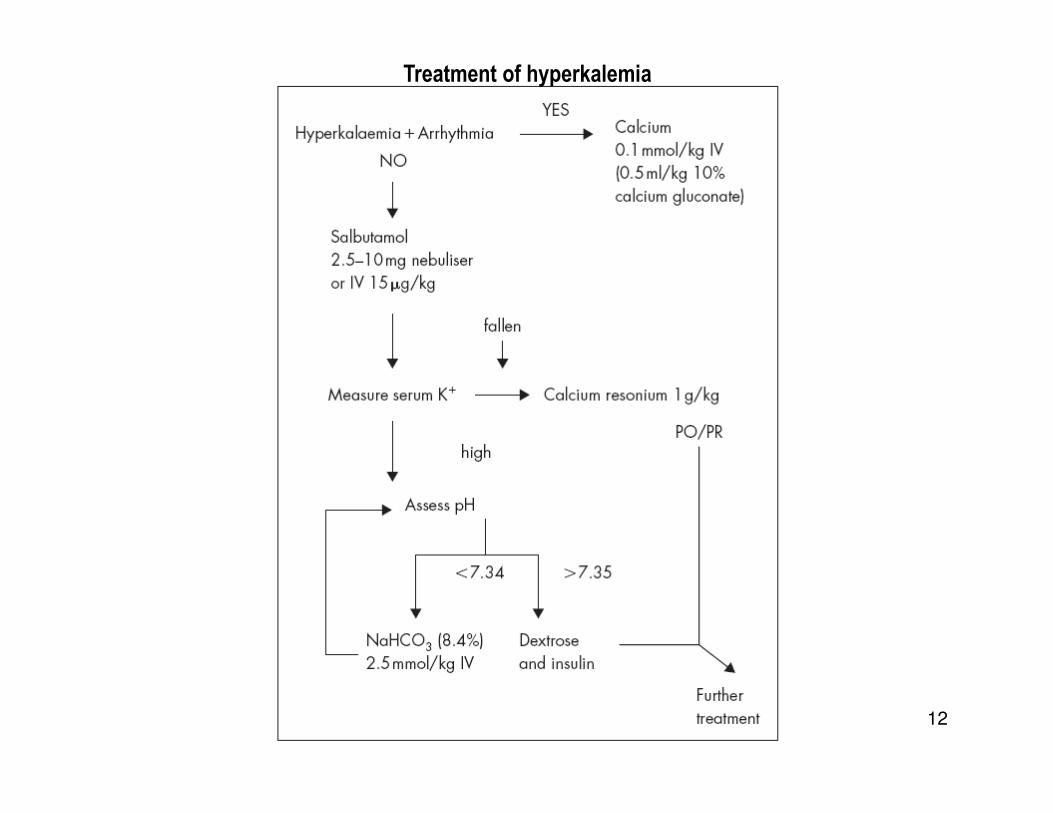
Treatment of hyperkalemia
12

CALCIUMNormal level 2.1–2.56 mmol/l
Hypercalcemia• rare
• causes: childhood malignancy, hyperparathyroidism, iatrogenic administration
• effects: polyuria, kidney stone formation, hypertension, shortened QT interval and
dysrhythmias
treatment: hydration with or without diuretics, reduce Ca intake, phosphate infusion
13
Hypocalcemia• causes: severe septicaemia, rickets, hypoparathyroidism, pancreatitis rhabdomyolysis,
citrate infusion (massive blood transfusion), acute and chronic renal failure
• treatment: IV calcium,may need infusion via central line, high phosphate (especially in
renal failure) may prevent rise

ACID-BASE DISORDERS
• pH is normally within the range of 7.35–7.45
• Normal pH is maintained by buffers in the body � solutions which contain
a weak acid and its conjugate base and are relatively resistant to changes
in pH
• Two main categories are bicarbonate and non-bicarbonate
• The non-bicarbonate forms almost 50% of the buffering capacity of whole
blood �haemoglobin, plasma proteins and organic and inorganic
phosphates
• However, the bicarbonate buffer system along with plasma proteins are
able to form the immediate response to an increase in acid or base
14
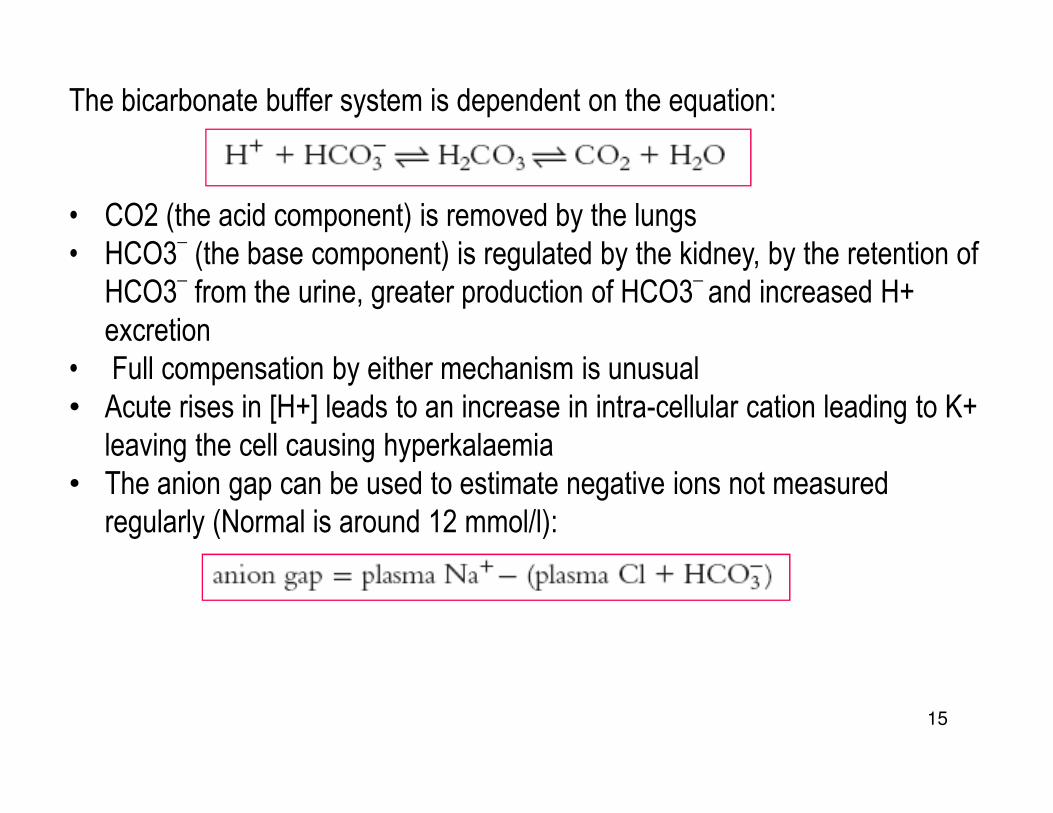
The bicarbonate buffer system is dependent on the equation:
• CO2 (the acid component) is removed by the lungs
• HCO3_(the base component) is regulated by the kidney, by the retention of
HCO3_from the urine, greater production of HCO3
_ and increased H+
excretion
• Full compensation by either mechanism is unusual
• Acute rises in [H+] leads to an increase in intra-cellular cation leading to K+
15
• Acute rises in [H+] leads to an increase in intra-cellular cation leading to K+
leaving the cell causing hyperkalaemia
• The anion gap can be used to estimate negative ions not measured
regularly (Normal is around 12 mmol/l):
Respiratory acidosis
• Characterised by raised PaCO2
• Causes:
• Hypoventilation due to respiratory depression, obstructive and
restrictive respiratory disease, neuro-muscular weakness causing
respiratory failure, inadequate mechanical ventilation
• Increased CO2 production; seizures, malignant hyperpyrexia
• Chronic respiratory acidosis is associated with a partially compensated
16
• Chronic respiratory acidosis is associated with a partially compensated
picture with raised PaCO2 and bicarbonate
• Treatment:
• Improve respiratory function by ventilatory support
• Need to be careful in patients with chronic respiratory acidosis

Respiratory alkalosis
• Characterised by lowered PaCO2
• Causes: Hyperventilation:
– Salicylate poisoning
– Fever, sepsis
– Encephalopathy
– Hypoxic and acidotic patients may hyperventilate
– Overventilated by mechanical ventilation
17
– Overventilated by mechanical ventilation
•Treatment:
–Treat cause in order to reduce respiratory rate and depth
– Reduction of ventilation or increase in dead space may help if
ventilated
Metabolic acidosis
• Characterised by a rise in serum H+
• Causes:
Normal anion gap – HCO3-lost:
– From GI tract, e.g. diarrhoea, fistulae
– From renal tract, e.g. proximal renal tubular acidosis
Increased anion gap acidosis:
– Renal failure
18
– Renal failure
– Ingestion, e.g. salicylates, methanol
– Ketoacidosis, e.g. diabetic ketoacidosis
– Lactic acidosis

•Causes of lactic acidosis:
Association with hypotension and/or severe tissue hypoxia
– Shock from any cause
– Respiratory failure
– Cyanide or carbon monoxide poisoning
– Severe anaemia
Associated with impaired mitochondrial respiration and increased
lactate production
– Diabetes mellitus
19
– Diabetes mellitus
– Hepatic failure
– Severe infection
– Drugs (e.g. salicylates)
– Toxins (e.g. ethanol)
– Inborn errors of metabolism
• Sign of metabolic acidosis: stimulation of respiration, may become deep
and sighing (Kussmaul’s respiration), myocardial depression, reduced
cardiac output, peripheral vasodilatation leading to hypotension, confusion
and drowsiness, reduced activity of inotropic agents
• Treatment:
–Treatment of the cause
20
–Treatment of the cause
–Intra-venous fluids
–Sodium bicarbonate, but beware due to the left shift of the oxygen
dissociation curve, inhibition of oxygen release from Hb may occur
–Renal replacement therapy

Metabolic alkalosis
• Characterised by gain of HCO3- or loss of H+
• Causes:
• Loss of H+: Vomiting, Gastric losses from nasogastric tube, Renal
losses e.g. diuretic therapy, Increased mineralocorticoids, Post-
hypercapnia
• Increased HCO3-– administration• Increased HCO3-– administration
• Large citrate load, e.g. massive blood transfusion
• Treatment: Treat cause if possible (e.g. stop diuretics)
21
Thank You
22