hypertension dr. stella yiu staff emergency physician
TRANSCRIPT

HypertensionDr. Stella YiuStaff Emergency Physician

LMCC objectives: Hypertension
Diagnose and determine severity
Investigate target organ damage and 2nd causes
List medical management (po and iv)

1. Diagnosis

Cdn 2012 guidelines
> 160 or > 100 x 3 Or> 140 or > 90 x 5

Most HTN = Essential HTN
5-10% 2nd – curable
More demand on pump or
Stiff pipes

2. 2nd causes

2nd Causes: Cardiac output (pump demand)
Renal failure + fluid overload++ aldosteroneAortic coarctation

2nd Causes: Vascular resistance (stiff pipes)
Renal artery stenosisPheochromocytomaDrugs Brain (CVA, ICH, SAH)

MCQ 8: What is the most common treatable 2nd cause for HTN?A. HyperaldosteronismB. Renal artery stenosisC. PheochromocytomaD. Aortic coarctationE. Sympathomimetic use

CDMQ: What are the clinical clues and investigations for 2nd causes?

Cardiac output (pump stress)Renal failure + fluid overload++ AldosteroneAortic coarctation

Vascular resistance (stiff pipes)Renal artery stenosisPheochromocytomaDrugs Brain (CVA, ICH, SAH)

Investigations
Renal failure + fluid overload
Creatinine, CXR

Investigations
++ aldosterone
High Na, Low K
Cushingoid on exam

Investigations
Aortic coarctation
HTN in Upper extremitySystolic murmur over backDelayed Femoral Pulse
Echo, Angio

Vascular resistance (stiff pipes)Renal artery stenosis
Young female + fibromuscular dysplasiaResistant to HTN medsMost common treatable cause
Abdo bruits, low K, Abdo US

Vascular resistance (stiff pipes)Pheochro-mocytoma
Episodes of HTN + HA + palp +diaphoresis
Urine catecholamines, metanephrines

Vascular resistance (stiff pipes)Drugs
Amphetamines, sympathomimeticsMAOI
Clinical exam: toxidromeUrine toxECG

Vascular resistance (stiff pipes)Brain (CVA, ICH, SAH)
CT head

3. Manage HTN emergency

What are the target organs?

What are the target organs?

MCQ 9: Which is not an HTN emergency?
A. 35 M 220/140, dizzy, normal neuro exam
B. 50 M 200/120, chest pain, CXR wide mediastinum
C. 25 F 28 wks pregnant, 150/80, seizure
D. 80 F 220/120, left arm weaknessE. 45 F 200/120, crackles to apex,
JVP 6cm

ACS
Pulmonary
edema
Aortic Dissectio
n

Bleeds, seizures Encephalopathy (not just headache,
dizzy)
Acute renal failure

CDMQ: List Investigations for HTN emergency

Investigations for HTN emergency
ACS
Pulmonary edema
Aortic Dissection
Bleeds, seizure,
encephalopathy
ARF

Treat HTN emergency: GeneralBP: Reduce MAP by 25%
Iv medications:LabetololNitroprussideHydralazine
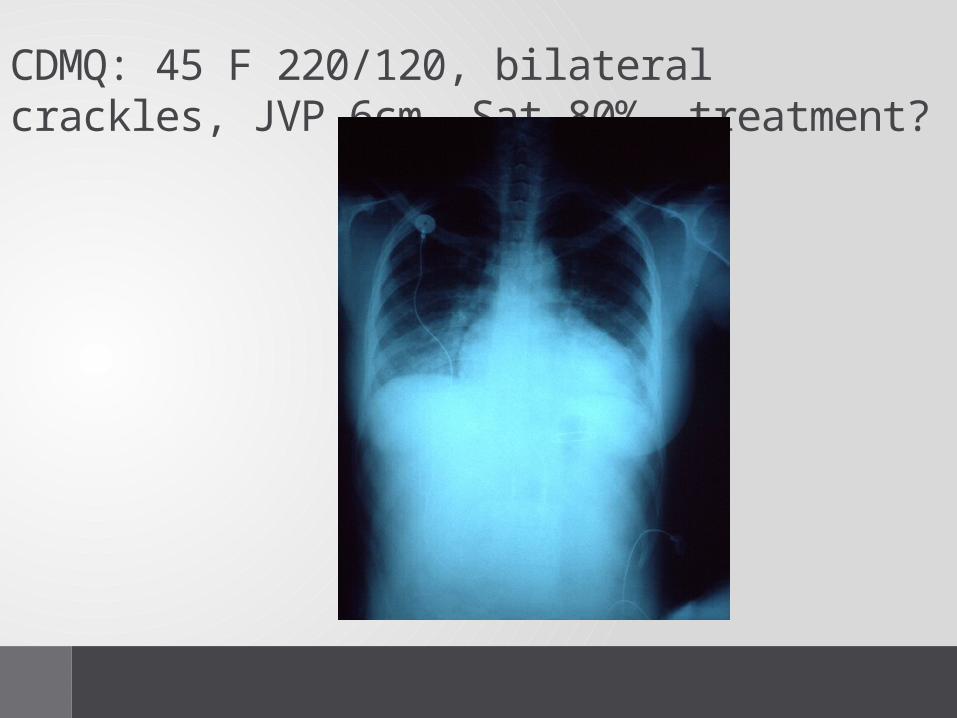
CDMQ: 45 F 220/120, bilateral crackles, JVP 6cm, Sat 80%, treatment?

Specific Treatment: Pulmonary EdemaBiPAPNitrates ivFurosemide iv

Specific Treatment: ACS
ASANTGBeta-blockers

Specific Treatment: DissectionIv Nitroprusside + beta-blocker
Iv labetolol
Surgery if ascending aorta
Specific Treatment: Seizure+ preg (Eclampsia)
MgSO4
Iv Hydralazine
Delivery

3. Manage HTN in Ambulatory setting

Diagnosis
> 160 or > 100 x 3 or> 140 or > 90 x 5

MCQ 10: What test is not needed in ambulatory testing for HTN?
A. Urine, urine albumin (DM)B. Lytes + creatinineC. Fasting glucose +
cholesterolD. CBC + diff E. ECG

Treatment HTN ambulatoryNon-pharmacological management

First line med, dosage and side effects?
No other comorbidities?CAD?Diabetes?Asthma?Renal failure?

No co-morbid – 1st line
Thiazide (HCTZ 251)Beta-blocker (Metoprolol 252)CCB (Amlodipine 51)ARB (Losartan 25mg )

DM
+ Renal: ACEI/ARBCCBThiazide

Asthma
Avoid beta-blocker

CRF (non-DM)
ACEI/ARBThiazide

CAD
ACEI /ARB Angina/recent MI: Beta-blocker

Improving compliance
Fit daily routine
Once daily dosing
Single pill combination
Dosette

LMCC objectives: Hypertension
Diagnose and determine severity
Investigate target organ damage and 2nd causes
List medical management (po and iv)