hospital program for adult patients with intellectual disabilities: improving the patient experience...
TRANSCRIPT

Hospital program for adult patients with intellectual disabilities:
Improving the patient experience July 25, 2011
Sarah Ailey, PH.D. RN APHN-BCRobyn Hart, M.Ed., CCLS
Some information is from research funded by: Center for Clinical Research and Scholarship: Rush University
Gamma Phi Chapter of Sigma Theta Tau

Purpose
• Discuss the program at Rush University Medical Center to improve the hospital experience for adults with intellectual and developmental disabilities (I/DD)

Objectives
• Describe ways in which services to assist persons with I/DD can be implemented using the example of Rush University Medical Center

Scope of Issue
• In a study done in two regions in NY State among adults with ID age 40-79 and living in community residential facilities of 4-15 people– 16% hospitalized in one year– 30% visited the emergency department **Janicki et al., 2002
©2009 Rush University Medical Center

AGENDA• Overview of the Rush Adults with IDD Committee• Origins• Identification of Mission and Goals • Staff and consumer input/involvement• Overview of work• Information gathering
– Survey of Illinois DDNA nurses– Information from chart reviews
• Examples• Plans for the future

Origins of the Committee
• Staff concerns raised at town hall meeting– Felt not prepared well enough - no training– Not sure how to communicate– Safety concerns for patients– Safety concerns for staff- at least few reports of
injury to staff
Overview of committee• Formed in 2007• Multidisciplinary/multi role• Seeks community representation and input

Assembling the team- multidisciplinary/multi-role
• Nursing (neurology, psychiatry, community and mental health nursing)• Child Life• Medicine• Occupational Therapy• Social Work (inpatient & older-adult outpatient)• Special Education Teacher• Employee & Organizational Development• Visitor and Guest Relations• Patient satisfaction• Out-patient Administration• Information Services• Library Services• Representatives from agency serving people with IDD

Mission Statement:
“To foster awareness, sensitivity and skills related to individuals with intellectual and developmental disabilities in order to promote partnership in the healthcare experience. “

Goals• Improve hospital care• Improve outpatient care• (For both)
– Elicit consumer input– Creation of work groups – Gather information– Develop education for staff– Provide improved programming
Input/Involvement• Invited family and agency representatives to serve on committee• Consulted experts in the field
– RRTC at University of Illinois• Coordinated with hospital ADA committee• Representatives from many departments/sectors of medical center
Creation of Three Work Groups
1. Building an administrative structure
2. Gathering data and external support
3. Changing the Rush Culture

Work group 1: Building Administrative Structure
• Identify key players and create partnerships (e.g. ADA taskforce, diversity taskforce, information services. interpreters’ services, unit directors, outpatient services, patient satisfaction)
• Obtain executive leadership support• Address
– Length of stay (LOS) and adverse events – Regulations – Systems issues

Workgroup 2: Gathering data & external support
Gathering data• Survey among staff• Other hospitals• Obtained grant for chart review of adult clients with ID over 2 year period (not psych admissions)*• Survey among DDNA nurses in Illinois
*Funded by: Gamma Phi Chapter Sigma Theta Tau Center for Clinical Research and Scholarship RUMC

Gathering support • Elicited internal and external family input• Collaborated with Autism Resource Center• Conferred with community agencies• Presentations at conferences• AHRQ Innovation Exchange - we have been in contact with
– Other hospitals– Agencies serving people with IDD– Governmental DD agencies– Many others

Changing the culture
Link the program to the ongoing efforts at the medical center to promote
• I CARE (innovation, collaboration, accountability, respect and excellence)/ I CONNECT
• Reinforce the mission statement of the Medical Center
Survey of employees
Contact with adult clients with intellectual and developmental disabilities
• 12% frequent contact (daily or almost daily)• 18% regular contact (at least once per week)• 70% occasional contact (once a month or less)

Employee-identified issues:
• Inadequate social histories• Communication problems• Assessing pain levels• Discharge planning/LOS• Legal issues• Patient safety/staff safety• Calming upset patients

Community Agency/Family Identified Issues:
Inpatient• Patient/staff communication• Negative attitudes from caregivers• Sensitivity to unique emotional & physical needs • Preserving patient dignity• Agency staff not able to stay with patients - therefore
hospital staff can not just rely on them
Community Agency/Family Identified Issues:
Outpatient• Lengthy waiting times for appointments• Need for written orders and instructions-
misconceptions that staff with person can transmit orders/instructions
• Staff at times do not talk to client (when able)• Need areas for repositioning/personal care

Programs developed: I CARE/I CONNECT Patient/Family Education Resources
• Development of step-by-step pictorial preparation materials for visual learners
• Provision of prehospitalization tourshttp://www.rush.edu/rumc/page-1234554423845.html
• Creation of personalized communication boards• Information for families on Rush web page• Help Line• Special Needs Buddies

Special Needs BuddiesNew program: Student volunteers buddy with
patients• Student volunteers volunteer with patients with special needs• Medical students, nursing students, OT students• Act as advocate and friend
• Answer questions• Familiarize them with medical personnel• Teach to use phone, TV or bed• Help fill out forms, meal card• Spend time
• Students gain experience with patients with IDD

Changing the Rush culture: Identified Staff Training Opportunities
• Disability Awareness Month programs• Unit-specific inservices• New employee orientation• Patient-care technician training• Individual consultation services• Special Needs Buddies

Changing the Rush Culture: Staff Training Topics
• Understanding autism and other developmental disabilities
• Fostering family-centered, respectful interactions
• Promoting positive health-care encounters
• Non-verbal or behavioral communication techniques
• Procedural preparation• De-escalation techniques• Illinois state services• Open-forum discussions:
participant identified topics

Consultation ServiceExamples:• Mark: 40 year old patient with Down syndrome
and deafness diagnosed with cancer
• Annie: 22 year old patient with a developmental disability diagnosed with leukemia

Additional information in EPIC admissionCommunication Issues
Expressive• Verbal/Non-verbal• Complex/simple communication• Alternate communication means
• Signs• Gestures • Other
• How do they communicate• Hunger• Thirst• Stop• Fear• Need for bathroom• Pain

Communicaton (cont.)Receptive
• Verbal/Non-verbal• Complex/simple communication• Alternate communication means
• Signs• Gestures• Other
• How do they receive communication• Hunger• Thirst• Stop• Fear• Need for bathroom• Pain

Additional information in EPIC admission Behavioral issues; Self-injurious; Wanderer
Antecedents to behavior/What is provoking for patient?• Light/Firm touch• Noise/Quiet• Light/No light• Disruption of routine• Other
What is calming for patient? What is provoking for patient?

Care plans
• Starting with existing care plans and deciding whether to revise/ develop some new
• Determining whether issues that should have a care plan are covered

Two year chart review*
• Describe results of a two year chart review of adult patients with intellectual disabilities and controls and discuss implications
* Funded by: Center for Clinical Research and Scholarship RUMC
Gamma Phi Chapter Sigma Theta Tau
Previous research on hospital experiences of adults with ID • Length of stay (LOS) longer, including longer than
individuals with other disabilities*• Patients with ID report feelings of
– Vulnerability– loss of control– fear of what was going to happen to them**– difficulty communicating their needs to hospital staff**** (Walsh, Kastner, & Criscione, 1997). ** (Parkes, Samuels, Hassiotis, Lynggaard, & Hall, 2007)***(Iacono & Davis, 2003).
©2009 Rush University Medical Center

Demographics
• Information collected on 217 adult admissions individuals with ID– 85% insured by Medicare or Medicaid
– Mean age 41.1 (15.7) Range18-82
– Mean LOS 7.16 (12.1) Range 1-113
– 49% male/ 51 % female

Demographics (cont.)– 30% of patients went to a neuroscience unit
– 20% to medical units
– 15% to intensive care units- of these 45% went to PICU
– 14% to surgical units
– 11% to pediatric units (including PICU)
– 4% to oncology units.

Two year chart review
– Advanced directives – Admission source– ER/ambulance– Admitting/final
diagnosis– Other health hx– Level of ID– In hospital events
– Standards of care initiated
– In patient referrals– Post discharge referrals– sitter – And other data– Discharge location
In depth review of 70 charts

Two year chart review
• In depth reviews on 70 records– 33% of patients came through ER
– Approximately 43% came by ambulance
– 60% had a decision maker noted on chart

Admission source*
• Home- 41.2%• Community Living facility – 25%• Nursing home – 5.9%• Other hospital – 25%
• *From 70 intensive review charts
©2009 Rush University Medical Center

Previous health history
• Seizures – 70.6%• Cerebral palsy – 36.8%• GI - 39.7%• Respiratory – 30.9%• Autism spectrum – 10.3%• Aggressive behaviors – 7.4%
©2009 Rush University Medical Center

In hospital events
• Hospital Acquired(HA) decubitus ulcer 4.4%• HA infection 7.4%• Post-op complications – 4.4%• Medication reactions – 5.9%• Fall – 2.9%
©2009 Rush University Medical Center

Other hospital events
• Pulled IV or other tubing – 5.9%• Medicated for agitation or aggression –
14.7%
©2009 Rush University Medical Center

Common precautions initiated• Fall precautions• Seizure precautions• Aspiration precautions• Skin integrity• 4 side rails up

Common referrals• Nutrition -64.7%• Neuro - 39.7%• Case management 26.5%• Surgical -29.4%• Pain/Palliative care – 5.9%• Social work 13.2%• PT/OT/ST 19.1%• GI -20.6%• Pulmonary – 20.6%• Psych 10.3%• Child life - 4.4%• Chaplain 7.4%• Other 27.9%

Two year chart review (cont)
• Information collected on adults similar diagnoses but without ID over same period.

Comparison data Neuroscience Adults with ID – N=68 (14)
• Age – 39.6 (13.5)• LOS – 3.5 (3.6)• Decision maker – 57.1%• ER – 14.3%• Ambulance- 28.6%• Admission source
– Home 28.6%– Community facility – 35.7%– Other hospital -21.4%– Nursing home – 14.3%
Adults without ID N=640 (13)• Age- 38.5 (14.2)• LOS 3.1 (2.2)• Decision maker – 0%• ER – 46.2%• Ambulance – 7.7%• Admission Source
– Home – 85%
©2009 Rush University Medical Center

Previous health history
Adults with ID N=14– CP - 21.4%– GI – 14.3%%– Respiratory -14.3%– Autism spectrum- 14.3%– Aggressive behavior -
14.3%
Adults without ID N=13• CP – 0%• GI – 23.1%• Respiratory – 30.8%• Autism spectrum – 0%• Aggressive behavior –
15.4%
©2009 Rush University Medical Center

Hospital incidents
Adults with ID N=14 • Fall – 7.1% (N=1)• HA decubitus 7.1%• Pulled IV/other tubing 7.1%• Medicated for
agitation/aggression 7.1%
Adults without ID N=13• Medicated for
agitation/aggression 7.7% (N=1)
©2009 Rush University Medical Center
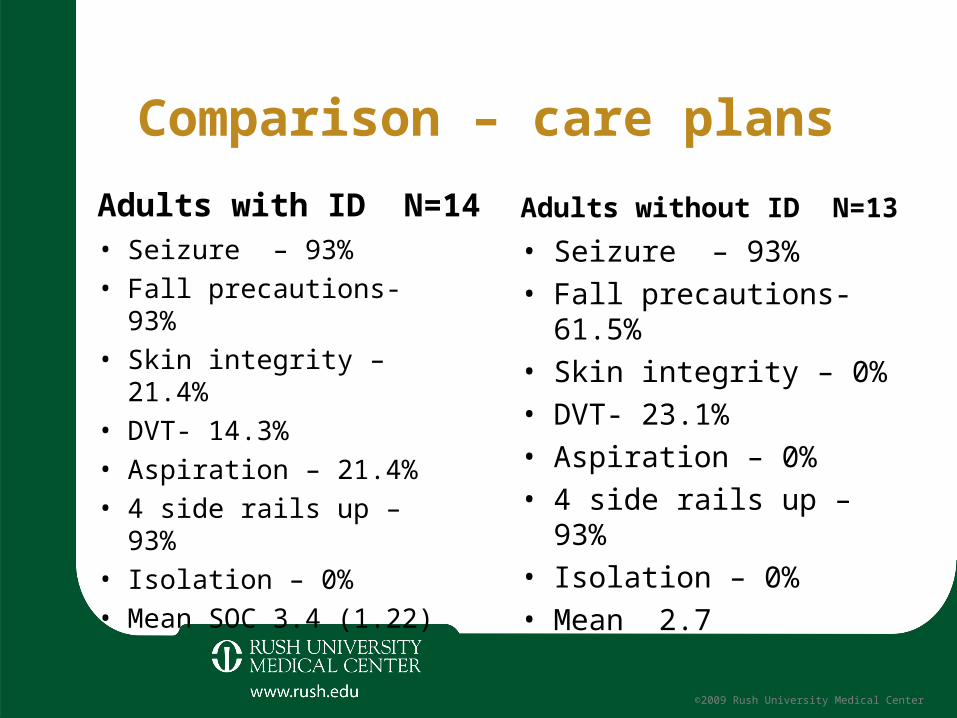
Comparison – care plans
Adults with ID N=14• Seizure – 93%• Fall precautions- 93%• Skin integrity – 21.4%• DVT- 14.3%• Aspiration – 21.4%• 4 side rails up – 93%• Isolation – 0%• Mean SOC 3.4 (1.22)
Adults without ID N=13• Seizure – 93%• Fall precautions- 61.5%• Skin integrity – 0%• DVT- 23.1%• Aspiration – 0%• 4 side rails up – 93%• Isolation – 0%• Mean 2.7
©2009 Rush University Medical Center

Pediatric units – General PediatricAdults with ID N=9 (7)
• Age 22.2 (3.5)• LOS 16.8 (32.5 N=9 )• Decision maker – 71.4%• ER – 71.4%• Ambulance – 28.6%• Admission Source
– Home – 57.1%– Community facility 14.3%– Nursing home 14.3%– Other hospital 14.3%
Adults without ID N=356 (9)• Age 22.9 (5.1)• LOS 5.5 (7.8)• Decision maker – 44.4%• ER – 12.5%• Ambulance – 12.5%• Admission Source
– Home – 66.7%– Other hospital 22.2%
©2009 Rush University Medical Center

Previous history – General Pediatrics
Adults with ID N=7• Seizures -57.1%• CP 85.7%• GI 57.1%• Respiratory 42.9%%• Autism spectrum 14.3%
Adults without ID N=9• Seizures 11.1%• CP- 11.1%• GI- 100%• Respiratory -33.3%
©2009 Rush University Medical Center

Hospital incidents
Adults with ID N=7• Post- op complications –
14.3% (N=1)• HA infection 14.3% (N=1)
Adults without ID N=9• None noted
©2009 Rush University Medical Center
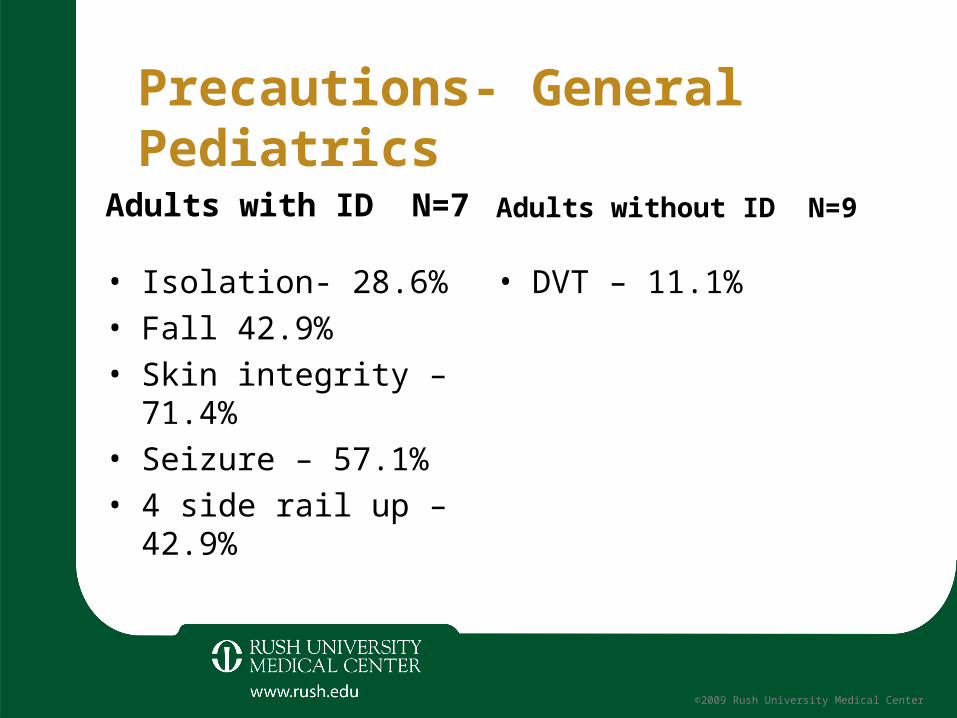
Precautions- General Pediatrics
Adults with ID N=7
• Isolation- 28.6%• Fall 42.9%• Skin integrity – 71.4%• Seizure – 57.1%• 4 side rail up – 42.9%
Adults without ID N=9
• DVT – 11.1%
©2009 Rush University Medical Center

Pediatric units – PICU
Adults with ID N=17 (12)• Age 24.6 (6.4)• LOS 9.6 (9.1)• Decision maker – 41.6%• ER – 33.3%• Ambulance – 66.7%• Admission Source
– Home – 50%– Community facility – 25%– Other hospital 25%
Adults without ID N=97(9)• Age 22.9 (5.1)• LOS 5.5 (7.8)• Decision maker – 42.9%• ER – 57.1%• Ambulance – none
noted 0%• Admission Source
– Home – 100%
©2009 Rush University Medical Center
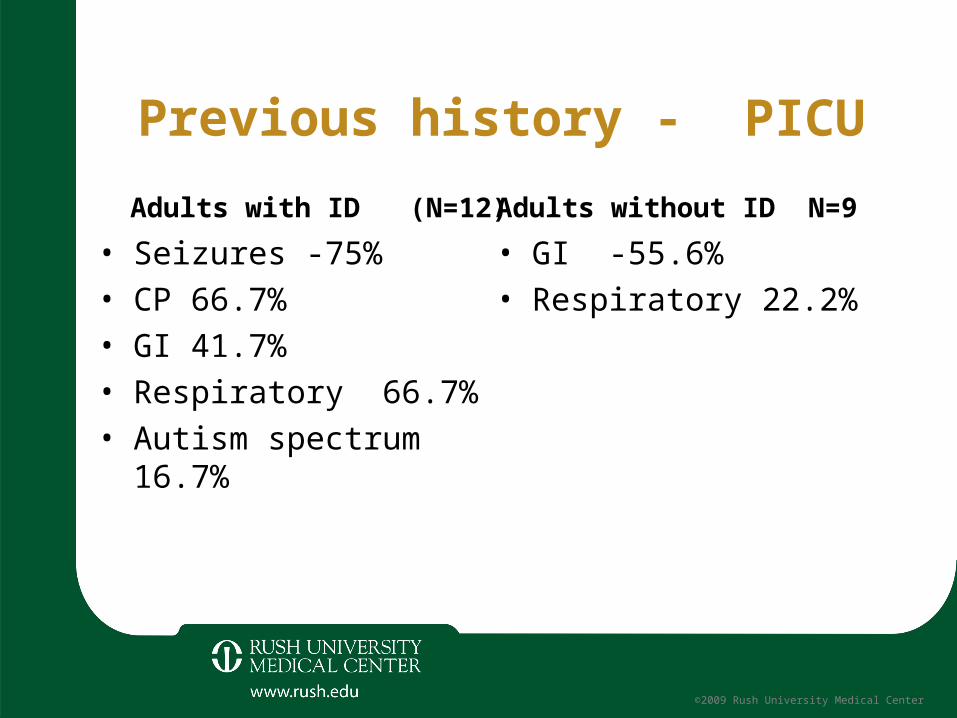
Previous history - PICU
Adults with ID (N=12)• Seizures -75%• CP 66.7%• GI 41.7%• Respiratory 66.7%• Autism spectrum 16.7%
Adults without ID N=9• GI -55.6%• Respiratory 22.2%
©2009 Rush University Medical Center

Hospital incidents
Adults with ID• HA decubitus – 8.3% (N=1)• HA infection – 8.3%• Pulled IV/other tubing -
8.3%• Medicated for
agitation/aggression -25%
Adults without ID• None noted
©2009 Rush University Medical Center

Care plans
Adults with ID• Isolation – 33.3%• Fall 83.3%• Skin – 66.7%• Seizures – 50%• DVT – 16.7%• Aspiration – 33.3%• 4 side rails up -50%
Adults without ID• DVT 14.3 % (N=1)• Risk of bleeding 14.3 %
(N=1)• Risk of injury 14.3 % (N=1)
©2009 Rush University Medical Center

University Healthsystem Consortium data
• Patients with IDSeizures- 8.8% of total– LOS 3.92– Expected LOS 3.44– % ICU stay 19.09%– ICU days 3.59– % deaths 0.40%
• Patients without IDSeizures– LOS 3.50– Expected LOS 3.38– % ICU stay 16.18%– ICU days 2.91– % deaths 0.41%

University Healthsystem Consortium data
• Patients with IDPneumonia- 3.8% total– LOS 4.57– Expected LOS 4.31– % ICU stay 17.29%– ICU days 3.40– % deaths 1.28%
• Patients without IDPneumonia– LOS 4.34– Expected LOS 4.38– % ICU stay 10.27%– ICU days 2.95– % deaths 1.64%

University Healthsystem Consortium data
• Patients with IDRespiratory infections-
3.2% of total– LOS 6.87– Expected LOS 7.31– % ICU stay 20.63%– ICU days 4.38– % deaths 2.41%
• Patients without IDRespiratory Infections– LOS 8.14– Expected LOS 8.50– % ICU stay 14.43%– ICU days 3.62– % deaths 5.62%

University Healthsystem Consortium data
• Patients with IDDigestive disease- 2.7%
total– LOS 4.42– Expected LOS 3.52– % ICU stay 4.38%– ICU days 2.73– % deaths 0.24%
• Patients without IDDigestive disease– LOS 3.40– Expected LOS 3.31– % ICU stay 3.87%– ICU days 2.57– % deaths 0.27%

University Healthsystem Consortium data
• Patients with IDSepticemia- 2.6% total– LOS 7.74– Expected LOS 7.76– % ICU stay 46.72%– ICU days 4.05– % deaths 11.37%
• Patients without IDSepticemia– LOS 6.98– Expected LOS 7.71– % ICU stay 41.96%– ICU days 3.34– % deaths 19.90%

Important issues• Longer LOS than patients without IDD who have similar
diagnoses• Greater percentage using ICUs• Longer LOS in ICUs• Higher rates of adverse events• High rate of ER as entrance to hospital• At our Medical Center, 25% coming from community
facilities
©2009 Rush University Medical Center

Opinions of nurses specializing in ID
• Survey conducted among more than 60 nurses with varying educational/professional backgrounds (APRNs, BSNs, RNs, LPNs) who specialize in working with individuals with ID.

Opinions of nurses specializing in IDModerate to major problems with hospital staff understanding:
– 77.8% client living situation– 85.7% client level of functioning– 87.2% client communication patterns– 76.2% what is frightening – 84.2% what is calming– 77.8% environmental over-stimulation – 50.8% appropriate patient case conferences– 58.8% discharge orders transmission

Opinions of nurses specializing in ID
• Restraints used too frequently• Skin breakdown on discharge• Misunderstanding guardianship issues

Opinions of nurses specializing in ID• Hospital staff reluctance to receive transfer report from
community facility caregivers• Clients unable to express their symptoms leading to lack of
appropriate care• Clients/family/caregivers not included in plan of care• Client functional level unknown/not assessed
Future plans:
• Where do we go from here?