hiatal closure – new trends in laparoscopic …type-i hiatal hernia is persistent gerd symptoms...
TRANSCRIPT

HIATAL CLOSURE – NEW TRENDS IN LAPAROSCOPIC ANTIREFLUX SURGERY
F. A. Granderath1 • C. T. Frantzides2 • M. A. Carlson3
1 Department of General Surgery, Hospital Zell am See, Austria2 Minimally Invasive Surgery Center, Evanston Northwestern Healthcare, Evanston, Il, USA3 Department of Surgery, University of Nebraska Medical Center, Omaha, NE, USA
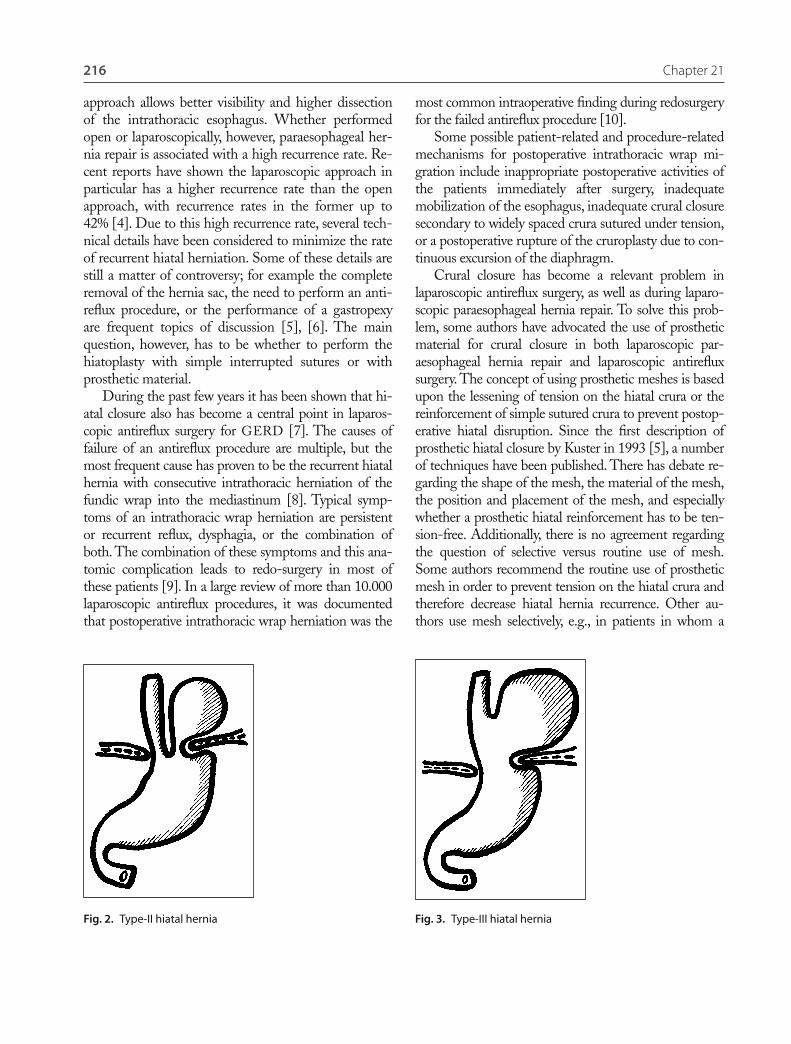
Fig. 1. Type-I hiatal hernia
Chapter 21
Introduction
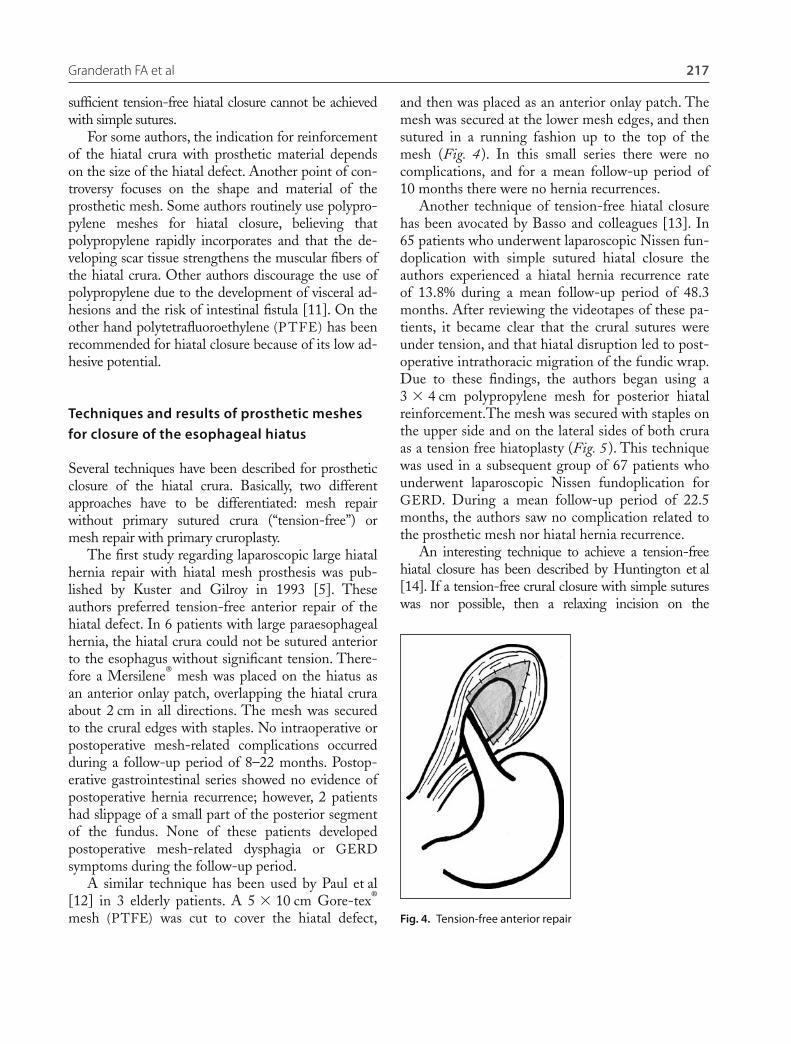
Gastroesophageal reflux disease (GERD) has provento be the most common upper gastrointestinal disord-er in the western world with 10% of patients havingdaily symptoms [1], [2]. In many patients, GERD isassociated with the presence of a hiatal hernia. Thedifferences between the three traditional types of hia-tal hernia regarding their morphological character-istics as well as the symptomatic correlation withGERD have to be considered. The most compre-hensive classification recognizes three types of hiatalhernias. Type-I hiatal hernias, the classical sliding hia-tal hernias, are characterized by transdiaphragmaticmigration of the gastroesophageal junction and theproximal stomach toward the mediastinum. Type-I hi-atal hernias are proven to be most common (80–90%of all types), particularly when the hernia is small. Intype-II hiatal hernias or paraesophageal hernias, thegastroesophageal junction remains below the dia-phragm in its normal position and the gastric fundusherniates alongside the esophagus into the mediasti-num. The type-III hiatal hernias are a combination ofboth type-I and -II hernias. The gastroesophagealjunction is above the diaphragm, and the gastric fundusherniates alongside the esophagus (Figs. 1–3). Morethan 80% of all paraesophageal hernias are consideredto be type-III hiatal hernias.
Depending on these morphological entities, thesethree types show several symptomatic and clinical differ-ences. A type-I hiatal hernia often causes characteristicGERD symptoms such as heartburn and regurgitation.Considerations regarding surgical therapy for this herniatype depends on the presence of GERD symptoms;therefore, the most common indication for surgery intype-I hiatal hernia is persistent GERD symptoms re-calcitrant to medical therapy. A type-II hiatal hernia
also can be accompanied by GERD symptoms, but thishernia type is typically associated with chest pain, dys-phagia, pulmonary problems, nausea or bleeding, whichare caused by the gastric herniation. Although paraeso-phageal hernia is a rare condition, it is associated with arather high incidence of complications.
In case of axial rotation of the gastric fundus, therisk for intrathoracic strangulation and gastric volvuluswith eventual incarceration and necrosis is increased.Therefore, most authors recommend a surgical man-agement of paraesophageal hernia, even in patientswithout symptoms. The minimally invasive approachto paraesophageal hernia repair has become the stan-dard of care for surgical management of this problem.Several studies have shown that laparoscopic para-esophageal hernia repair is associated with a lower incidence of morbidity, a shorter hospital stay, and ashorter recovery period compared to open repair [3].Additionally, most authors agree that the laparoscopic
216 Chapter 21
most common intraoperative finding during redosurgeryfor the failed antireflux procedure [10].
Some possible patient-related and procedure-relatedmechanisms for postoperative intrathoracic wrap mi-gration include inappropriate postoperative activities ofthe patients immediately after surgery, inadequate mobilization of the esophagus, inadequate crural closuresecondary to widely spaced crura sutured under tension,or a postoperative rupture of the cruroplasty due to con-tinuous excursion of the diaphragm.
Crural closure has become a relevant problem in laparoscopic antireflux surgery, as well as during laparo-scopic paraesophageal hernia repair. To solve this prob-lem, some authors have advocated the use of prostheticmaterial for crural closure in both laparoscopic par-aesophageal hernia repair and laparoscopic antirefluxsurgery. The concept of using prosthetic meshes is basedupon the lessening of tension on the hiatal crura or thereinforcement of simple sutured crura to prevent postop-erative hiatal disruption. Since the first description ofprosthetic hiatal closure by Kuster in 1993 [5], a numberof techniques have been published. There has debate re-garding the shape of the mesh, the material of the mesh,the position and placement of the mesh, and especiallywhether a prosthetic hiatal reinforcement has to be ten-sion-free. Additionally, there is no agreement regardingthe question of selective versus routine use of mesh.Some authors recommend the routine use of prostheticmesh in order to prevent tension on the hiatal crura andtherefore decrease hiatal hernia recurrence. Other au-thors use mesh selectively, e.g., in patients in whom a
approach allows better visibility and higher dissectionof the intrathoracic esophagus. Whether performedopen or laparoscopically, however, paraesophageal her-nia repair is associated with a high recurrence rate. Re-cent reports have shown the laparoscopic approach inparticular has a higher recurrence rate than the openapproach, with recurrence rates in the former up to42% [4]. Due to this high recurrence rate, several tech-nical details have been considered to minimize the rateof recurrent hiatal herniation. Some of these details arestill a matter of controversy; for example the completeremoval of the hernia sac, the need to perform an anti-reflux procedure, or the performance of a gastropexyare frequent topics of discussion [5], [6]. The mainquestion, however, has to be whether to perform thehiatoplasty with simple interrupted sutures or withprosthetic material.
During the past few years it has been shown that hi-atal closure also has become a central point in laparos-copic antireflux surgery for GERD [7]. The causes offailure of an antireflux procedure are multiple, but themost frequent cause has proven to be the recurrent hiatalhernia with consecutive intrathoracic herniation of thefundic wrap into the mediastinum [8]. Typical symp-toms of an intrathoracic wrap herniation are persistentor recurrent reflux, dysphagia, or the combination ofboth. The combination of these symptoms and this ana-tomic complication leads to redo-surgery in most ofthese patients [9]. In a large review of more than 10.000laparoscopic antireflux procedures, it was documentedthat postoperative intrathoracic wrap herniation was the
Fig. 3. Type-III hiatal herniaFig. 2. Type-II hiatal hernia
Granderath FA et al 217
sufficient tension-free hiatal closure cannot be achievedwith simple sutures.
For some authors, the indication for reinforcementof the hiatal crura with prosthetic material dependson the size of the hiatal defect. Another point of con-troversy focuses on the shape and material of theprosthetic mesh. Some authors routinely use polypro-pylene meshes for hiatal closure, believing that polypropylene rapidly incorporates and that the de-veloping scar tissue strengthens the muscular fibers ofthe hiatal crura. Other authors discourage the use ofpolypropylene due to the development of visceral ad-hesions and the risk of intestinal fistula [11]. On theother hand polytetrafluoroethylene (P TFE) has beenrecommended for hiatal closure because of its low ad-hesive potential.
Techniques and results of prosthetic meshes for closure of the esophageal hiatus
Several techniques have been described for prostheticclosure of the hiatal crura. Basically, two differentapproaches have to be differentiated: mesh repairwithout primary sutured crura (“tension-free”) ormesh repair with primary cruroplasty.
The first study regarding laparoscopic large hiatalhernia repair with hiatal mesh prosthesis was pub-lished by Kuster and Gilroy in 1993 [5]. Theseauthors preferred tension-free anterior repair of thehiatal defect. In 6 patients with large paraesophagealhernia, the hiatal crura could not be sutured anteriorto the esophagus without significant tension. There-fore a Mersilene® mesh was placed on the hiatus asan anterior onlay patch, overlapping the hiatal cruraabout 2 cm in all directions. The mesh was securedto the crural edges with staples. No intraoperative orpostoperative mesh-related complications occurredduring a follow-up period of 8–22 months. Postop-erative gastrointestinal series showed no evidence ofpostoperative hernia recurrence; however, 2 patientshad slippage of a small part of the posterior segmentof the fundus. None of these patients developed postoperative mesh-related dysphagia or GERDsymptoms during the follow-up period.
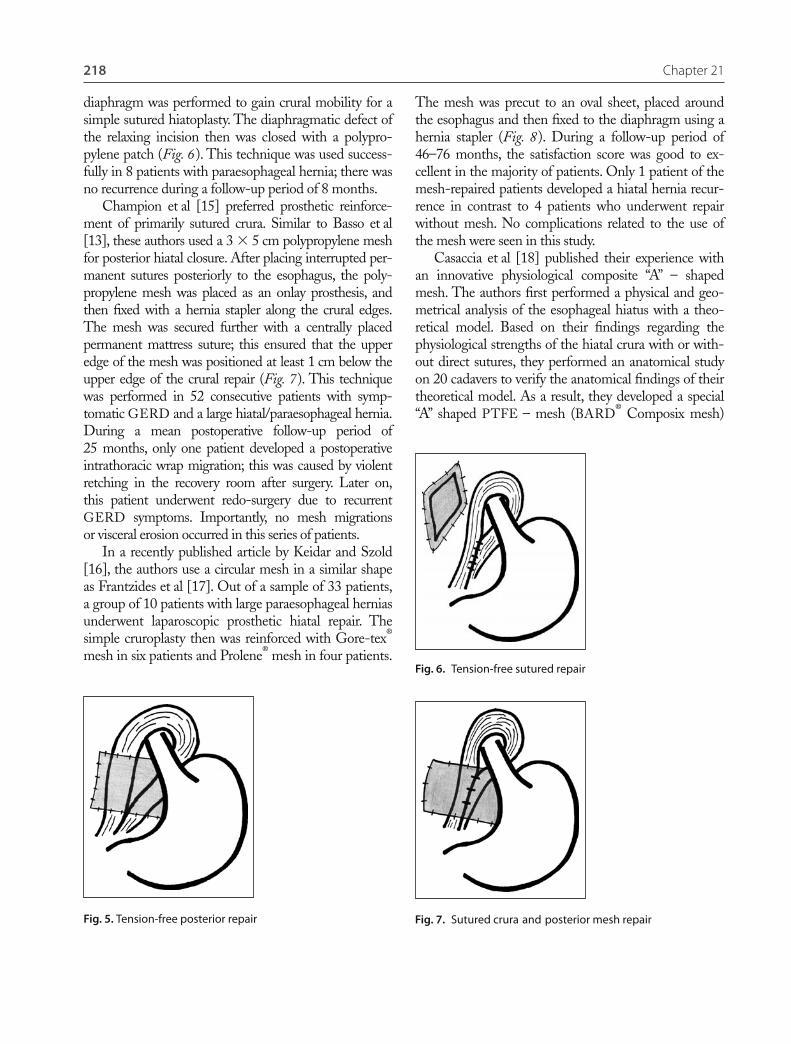
A similar technique has been used by Paul et al[12] in 3 elderly patients. A 5 � 10 cm Gore-tex®
mesh (PTFE) was cut to cover the hiatal defect,
and then was placed as an anterior onlay patch. Themesh was secured at the lower mesh edges, and thensutured in a running fashion up to the top of themesh (Fig. 4 ). In this small series there were nocomplications, and for a mean follow-up period of10 months there were no hernia recurrences.
Another technique of tension-free hiatal closurehas been avocated by Basso and colleagues [13]. In65 patients who underwent laparoscopic Nissen fun-doplication with simple sutured hiatal closure theauthors experienced a hiatal hernia recurrence rateof 13.8% during a mean follow-up period of 48.3months. After reviewing the videotapes of these pa-tients, it became clear that the crural sutures wereunder tension, and that hiatal disruption led to post-operative intrathoracic migration of the fundic wrap.Due to these findings, the authors began using a 3 � 4 cm polypropylene mesh for posterior hiatalreinforcement.The mesh was secured with staples onthe upper side and on the lateral sides of both cruraas a tension free hiatoplasty (Fig. 5 ). This techniquewas used in a subsequent group of 67 patients whounderwent laparoscopic Nissen fundoplication forGERD. During a mean follow-up period of 22.5months, the authors saw no complication related tothe prosthetic mesh nor hiatal hernia recurrence.
An interesting technique to achieve a tension-freehiatal closure has been described by Huntington et al[14]. If a tension-free crural closure with simple sutureswas nor possible, then a relaxing incision on the
Fig. 4. Tension-free anterior repair
218 Chapter 21
diaphragm was performed to gain crural mobility for asimple sutured hiatoplasty. The diaphragmatic defect ofthe relaxing incision then was closed with a polypro-pylene patch (Fig. 6). This technique was used success-fully in 8 patients with paraesophageal hernia; there wasno recurrence during a follow-up period of 8 months.
Champion et al [15] preferred prosthetic reinforce-ment of primarily sutured crura. Similar to Basso et al[13], these authors used a 3 � 5 cm polypropylene meshfor posterior hiatal closure. After placing interrupted per-manent sutures posteriorly to the esophagus, the poly-propylene mesh was placed as an onlay prosthesis, andthen fixed with a hernia stapler along the crural edges.The mesh was secured further with a centrally placedpermanent mattress suture; this ensured that the upperedge of the mesh was positioned at least 1 cm below theupper edge of the crural repair (Fig. 7). This techniquewas performed in 52 consecutive patients with symp-tomatic GERD and a large hiatal/paraesophageal hernia.During a mean postoperative follow-up period of 25 months, only one patient developed a postoperativeintrathoracic wrap migration; this was caused by violentretching in the recovery room after surgery. Later on,this patient underwent redo-surgery due to recurrentGERD symptoms. Importantly, no mesh migrations or visceral erosion occurred in this series of patients.
In a recently published article by Keidar and Szold[16], the authors use a circular mesh in a similar shapeas Frantzides et al [17]. Out of a sample of 33 patients,a group of 10 patients with large paraesophageal herniasunderwent laparoscopic prosthetic hiatal repair. Thesimple cruroplasty then was reinforced with Gore-tex®
mesh in six patients and Prolene® mesh in four patients.
Fig. 7. Sutured crura and posterior mesh repair
Fig. 6. Tension-free sutured repair
Fig. 5. Tension-free posterior repair
The mesh was precut to an oval sheet, placed aroundthe esophagus and then fixed to the diaphragm using ahernia stapler (Fig. 8). During a follow-up period of46–76 months, the satisfaction score was good to ex-cellent in the majority of patients. Only 1 patient of themesh-repaired patients developed a hiatal hernia recur-rence in contrast to 4 patients who underwent repairwithout mesh. No complications related to the use ofthe mesh were seen in this study.
Casaccia et al [18] published their experience withan innovative physiological composite “A” – shapedmesh. The authors first performed a physical and geo-metrical analysis of the esophageal hiatus with a theo-retical model. Based on their findings regarding thephysiological strengths of the hiatal crura with or with-out direct sutures, they performed an anatomical studyon 20 cadavers to verify the anatomical findings of theirtheoretical model. As a result, they developed a special“A” shaped PTFE – mesh (BARD® Composix mesh)

Granderath FA et al 219
which, when positioned over the hiatal defect, was in-tended to effect closure similar to the physiological con-dition (Fig. 9). In 8 patients with large type-II andtype-III hiatal hernia, laparoscopic repair was per-formed with this composite “A” shaped P TFE mesh.Intraoperatively, the authors found that the mesh fitwell in the hiatal region, with good handling and easyplacement on the diaphragm. Postoperative dysphagiaoccurred in 2 patients for up to 3 months after surgery,but no recurrence was observed during an average follow-up period of 8 months.
Based on the possibility of mesh-related complica-tions such as esophageal stricture, mesh migration, orvisceral erosion, Oelschlager et al [19] advocated the useof a new type of mesh made from porcine small intes-tine submucosa (SIS) for laparoscopic repair of par-aesophageal hernias. The authors closed the hiatal crurawith interrupted 2�0 silk sutures, and then positioned aU-shaped 7 � 10 cm four-ply Surgisis® mesh posteri-orly so that the mesh covered the crural repair. Themesh was secured with interrupted silk sutures to thediaphragm (Fig. 10). This technique has been used in 9patients with large paraesophageal hernias that couldnot be closed without tension. In 8 patients who wereavailable for follow-up, only 1 had a small (2 cm) recurrent hiatal hernia on barium esophagram; thisrecurrence was asymptomatic. Another patient had toundergo pneumatic dilatation for persistent mild dysphagia, but without signs of anatomic failure onendoscopy or barium swallow. There were no othercomplications in this series.
Another approach to crural closure with biomaterial hasbeen described by Varga et al [20]. In this study, the hi-atoplasty was performed with the ligamentum teres inaddition to simple sutures. After closing the hiatal crurawith nonabsorbable interrupted sutures, the mobilizedligamentum teres was pulled between the closed cruraand posterior esophagus, and then sutured to the crura.This created a U-shaped hiatal onlay reinforcement(Fig. 11). This technique was performed in 4 patientswith type-III hiatal hernia. There were no perioperativecomplications related to this kind of hiatoplasty. Onepatient had minor episodic epigastric pain postopera-tively; otherwise, all patients relieved of symptoms. Norecurrent hiatal hernia occurred during follow-up of 3–11 months.
Fig. 8. Simple cruroplasty and circular mesh repair
Fig. 9. Simple cruroplasty and “A”-shaped mesh repair
Fig. 10. Simple cruroplasty and SIS® mesh repair

220 Chapter 21
number of sutures depended on the size of hiatal her-nia; in these patients, the crura were approximated with2–4 interrupted nonbasorbable polyfilament sutures(Figs. 12 and 13).
In the cruroplasty and mesh group, the crura wereapproximated with simple interrupted sutures as above.Additionally, a 1 � 3 cm section of polypropylene mesh(cut from a 10 � 15 Prolene® mesh for groin hernia re-pair) was placed on the sutured crura as a posterior on-lay and sutured with one stitch on the lateral sides ofboth the right and the left crus (Figs. 14 and 15).
Follow-up examinations were performed 6 weeks, 3months and 1 year after surgery. After 1 year of follow-up, a significant difference in the postoperative occur-rence of intrathoracic wrap migration was found. In theinitial group with non-mesh hiatoplasty, a postoperativeintrathoracic wrap migration occurred in 6.1% of pa-tients compared to 0.6% of patients who underwent cru-
Fig. 11. Simple cruroplasty and ligamentum teres repair
Own experience
The high rate of postoperative intrathoracic wrap mi-gration after laparoscopic antireflux surgery promptedus to use prosthetic meshes for crural closure in Decem-ber 1998. In all patients who underwent laparoscopicantireflux surgery at our surgical unit, hiatal hernia re-currence with intrathoracic wrap migration was themost common cause of anatomic failure after primarylaparoscopic antireflux surgery. In over 70% of patientswho underwent laparoscopic refundoplication after pri-mary failed antireflux surgery, intrathoracic wrap migra-tion was found as the reason for failure.
In a prospective non-randomized trial [21] we com-pared 361 patients with GERD who underwent lapa-roscopic Nissen or Toupet fundoplication with simplecrural closure to 170 GERD patients who underwentlaparoscopic antireflux surgery with simple hiatal clo-sure reinforced with polypropylene mesh. In the groupof patients who underwent primary cruroplasty, the
Fig. 12. Simple cruroplasty
Fig. 13. Simple cruroplasty

Granderath FA et al 221
ral closure with polypropylene mesh onlay. A significantdifference also occurred in the incidence of postoperativedysphagia. Patients with mesh-cruroplasty had a dys-phagia rate of 35.3% compared to 19.8% in the non-mesh group 3 months after surgery; however, thedysphagia rate resolved at the 1 year visit and was notdifferent between the two groups.
These findings were re-evaluated in another non ran-domized trial [22], in which 100 GERD patients withsimple crural closure were compared to 100 GERD pa-tients with simple closure reinforced with the 1 � 3 cmpolypropylene mesh hiatoplasty. The postoperative dys-phagia rate and its impact on quality of life was evaluatedfor a period of 12 months after surgery. The postopera-tive dysphagia rate was significantly higher in the mesh-group at 3 month follow-up, but again decreased to
comparable values at 1 year follow-up. Apart from theseresults, patients quality of life (GQLI) significantly im-proved after surgery in both groups. This improvementremained stable up to one year postoperatively, was com-parable between the two groups, and similar to valuesfrom a healthy control group.
To verify these findings, a prospective randomizedstudy was performed on 100 GERD patients scheduledfor laparoscopic Nissen fundoplication [23]. Fifty pa-tients were prospectively randomized to laparoscopic360� floppy Nissen fundoplication with simple hiato-plasty, and fifty were randomized to laparoscopic 360�floppy Nissen fundoplication with 1 � 3 cm polypro-pylene mesh onlay. Follow-up of 12 months was obtained in all patients. Three months after surgery, asignificant difference in postoperative intrathoracic wrapmigrations was observed. Five patients (10%) of thenon-mesh group had a recurrence compared to 1 patient(2%) of the mesh-group. Twelve months after surgery,the recurrence rates increased to 4 patients (8%) in themesh-group and 13 patients (26%) in the non-mesh-group. In addition, patients with prosthetic hiatal closureagain had a higher dysphagia rate at the 3 months visit,as previously observed.
A different type of prosthetic mesh was used in 24patients who underwent laparoscopic refundoplicationin our surgical unit for a failed primary antireflux sur-gery. The cause of failure in all of these patients was asymptomatic intrathoracic wrap mig-ration [24]. Thefailed hiatal repair was primarily approximated with in-terrupted nonabsorbable sutures and then reinforcedwith a circular precut polypropylene mesh. The meshwas cut out with a 3–4 cm “keyhole” as described by
Fig. 14. Simple cruroplasty and posterior 1 � 3 cm polypropyl-ene mesh repair
Fig. 15. Simple cruroplasty and posterior 1 � 3 cm polypropylenemesh repair
222 Chapter 21
the mesh and secured with staples on the lateral side ofthe mesh (Figs. 18 and 19). The advantages of thismesh type have been ascribed to the combination oftwo clinically proven materials: BARD® mesh on theone side for maximum tissue ingrowth and eP TFE onthe other side for minimal visceral adhesions.
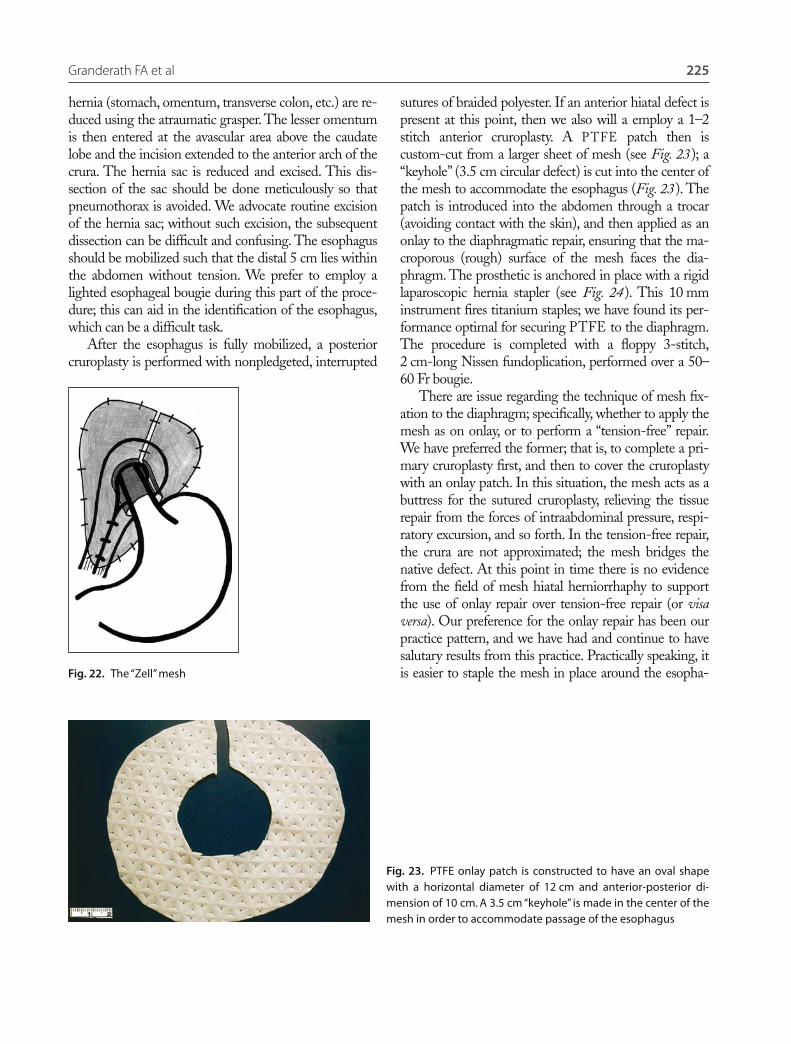
In addition, we are participating in a multicenterstudy regarding the use of PARIETEX®, a newer mesh,which, similar to the Composix mesh, combines two dif-ferent materials. Parietex® composite mesh has a three-dimensional weave of polyester on the one side with ahydrophilic collagen material on the other side. The re-sorbable collagen side has been designed for the preven-tion of intrabdominal adhesions to the mesh in the earlypostoperative period. The polyester side guarantees rapidtissue ingrowth with permanent reinforcement. In con-junction with the participating colleagues and the man-ufacturer, we have designed a special “V” shape of thismesh particularly for laparoscopic closure of the hiatalcrura. The mesh is used both for tension-free hiatal clo-sure (Figs. 20 and 21) and as an additional reinforcementof primary sutured hiatal crura. Positioned as a posterioronlay prosthesis, the mesh is secured to the diaphragmwith a hernia stapler.
Based on our previous findings and experiences, weare developing a new kind of prosthetic mesh whichspecifically will be for hiatal closure. During laparo-scopic refundoplication for primary failed hiatal clo-sure, the fundic wrap often does not slip posterior tobut also anterior to the esophagus. Therefore, in addi-tion to posterior closure, the mesh should also coverthe anterior diaphragmatic region to prevent postope-rative anterior slippage. Circular meshes have proven
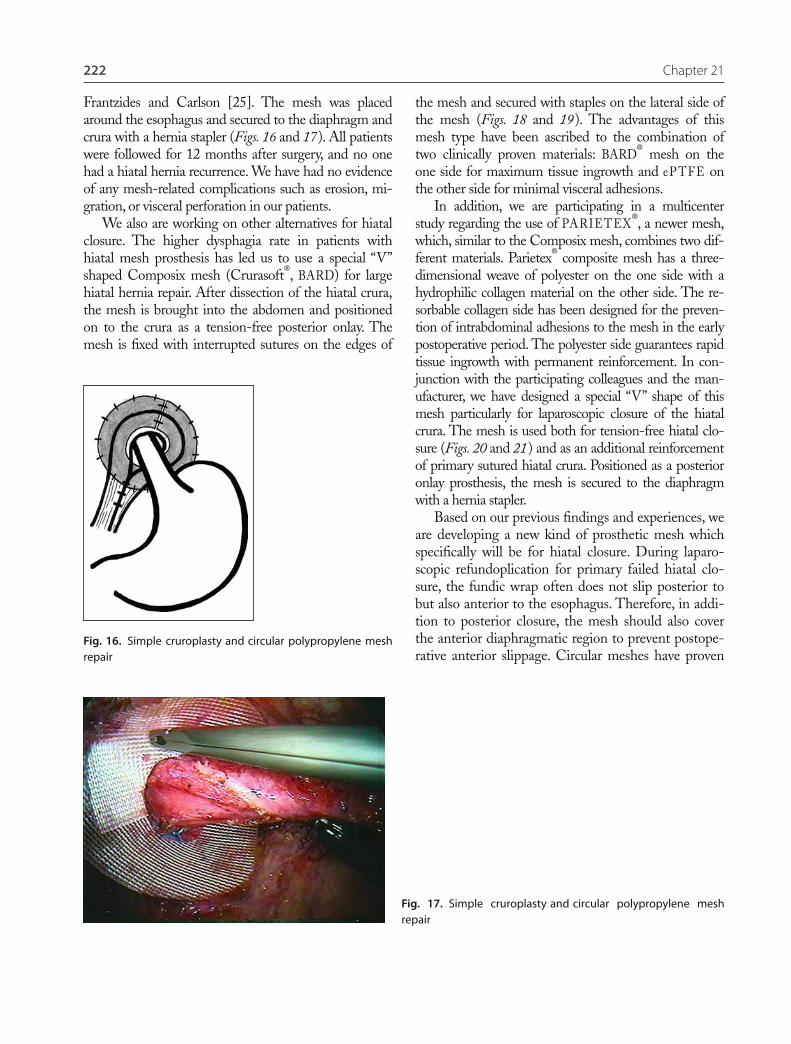
Frantzides and Carlson [25]. The mesh was placedaround the esophagus and secured to the diaphragm andcrura with a hernia stapler (Figs. 16 and 17). All patientswere followed for 12 months after surgery, and no onehad a hiatal hernia recurrence. We have had no evidenceof any mesh-related complications such as erosion, mi-gration, or visceral perforation in our patients.
We also are working on other alternatives for hiatalclosure. The higher dysphagia rate in patients with hiatal mesh prosthesis has led us to use a special “V”shaped Composix mesh (Crurasoft®, BARD) for largehiatal hernia repair. After dissection of the hiatal crura,the mesh is brought into the abdomen and positionedon to the crura as a tension-free posterior onlay. Themesh is fixed with interrupted sutures on the edges of
Fig. 16. Simple cruroplasty and circular polypropylene meshrepair
Fig. 17. Simple cruroplasty and circular polypropylene meshrepair

Granderath FA et al 223
to be an effective method to prevent hiatal hernia re-currence in some studies. We have employed a “heart”shaped modification of this mesh with large anteriorand posterior portions which completely cover the hi-atal crura behind the esophagus. The esophagus lies ina 3–4 cm central keyhole, which is protected by aPTFE collar to prevent esophageal erosion by themesh (Fig. 22).
Experience of Drs. Frantzides and Carlson
Our initial results with laparoscopic mesh-reinforced diaphragmatic hernia repair
To our knowledge, Dr. Robert Condon of the MedicalCollege of Wisconsin (Milwaukee, Wisconsin, USA)
was the first to address the problem of unacceptablyhigh recurrence rate after (open) sutured hiatal hernior-rhaphy by using a mesh-reinforced cruroplasty. Begin-ning in the latter 1970’s, this surgeon (who was ourmentor) instituted a policy of polypropylene onlay tothe diaphragm for patients with large hiatal hernia withintrathoracic stomach [26]. His technique consisted ofa sutured posterior cruroplasty onto which a sheet ofMarlex® was placed, followed by a gastrostomy. In orderto accommodate passage of the esophagus, a “keyhole”was cut in the center of the mesh. Over a fifteen yearperiod, 44 patients with intrathoracic stomach weretreated in such a manner. After a mean follow-up period of 52 months (range 2 months to 15 years), theclinical recurrence rate was zero [26]. At the time of itspublication in 1998, this manuscript represented one ofthe largest series of prosthesis-reinforced diaphragmatichernia repairs, either open or laparoscopic.
Encouraged with the result of open mesh repair ofdiaphragmatic hernia, we elected to perform the repairwith a minimally invasive approach. We did have a con-cern with using a stiff prosthetic mesh (such as Marlex®)at the hiatus, because this mesh did erode into theesophagus in one patient from the open series [26].Polypropylene mesh erosion into exposed bowel hasbeen a frequent enough problem in mesh repair of an-terior abdominal wall defects, especially in the presenceof acute inflammation [27]. We believed that the use ofP TFE at the hiatus might lessen the risk for erosivecomplications, since only a handful of cases have beenpublished documenting P TFE as the cause or suspect-ed cause of a bowel fistula (at the time we were contem-plating such repairs, no reports of erosive complicationsFig. 18. Tension-free posterior Crurasoft® mesh repair
Fig. 19. Tension-free posterior Crurasoft® mesh repair
224 Chapter 21
patients with gastroesophageal reflux disease and largedefect hiatal hernia were enrolled into this trial [25]. Thestudy population consisted of a subset of all patients (� 600) undergoing primary minimally invasive antire-flux surgery under the care of Dr. Frantzides. The deci-sion whether to enroll a patient into the study was madeafter intraoperative measurement of the hiatal defect. Ifthe defect diameter was � 8 cm, then the subject wasrandomized, and a simple posterior cruroplasty with orwithout P TFE onlay reinforcement (see below) followedby a floppy Nissen fundoplication was performed. After amean follow-up period of 3.3 years, the recurrence rate inthe cruroplasty-only group was 22% (i.e., 8 of 36), andthe rate in the cruroplasty plus P TFE group was zero.There were no mesh-related complications. We con-cluded that P TFE reinforcement of posterior cruroplastywas indicated for hiatal defects � 8 cm.
Our technique of laparoscopic mesh-reinforced hiatal hernia repair
Our technique of minimally invasive hiatal hernia repairhas been described in detail elsewhere [28]. The patientis placed in a modified lithotomy position with 15–20�of reverse-Trendelenburg tilt, and the surgeon stands be-tween the patient’s legs. We employ five 10 mm ports;this gives us maximum flexibility in instrument choice,including atraumatic 10 mm tissue graspers (atraugripgrasper – Pilling and Weck Surgical, Ft. Washington,PA). The liver is retracted with an inflatable non-traumatic balloon retractor (Soft Wand atraumatic bal-loon, Southborough, MA). The contents of the hiatal
from P TFE could be found). Another theoretical con-cern we had was whether the use of mesh actually wouldbe of benefit in the repair of diaphragmatic hernia. Ourretrospective series suggested that utilization of meshdecreased hernia recurrence rate, but we did not haveany controlled data that confirmed this. Therefore, aftera small number of cases to demonstrate the feasibility ofminimally invasive hiatal herniorrhaphy with P TFE on-lay reinforcement [17], we embarked on a randomizedcontrolled trial to test whether mesh placement reducedthe recurrence rate after laparoscopic diaphragmatic hernia repair.
We hypothesized that a benefit from mesh placementmost likely would be seen in patients with a large hiataldefect (which we defined as � 8 cm). Seventy-two
Fig. 21. Parietex® mesh repair
Fig. 20. Parietex® mesh repair
Granderath FA et al 225
hernia (stomach, omentum, transverse colon, etc.) are re-duced using the atraumatic grasper. The lesser omentumis then entered at the avascular area above the caudatelobe and the incision extended to the anterior arch of thecrura. The hernia sac is reduced and excised. This dis-section of the sac should be done meticulously so thatpneumothorax is avoided. We advocate routine excisionof the hernia sac; without such excision, the subsequentdissection can be difficult and confusing. The esophagusshould be mobilized such that the distal 5 cm lies withinthe abdomen without tension. We prefer to employ alighted esophageal bougie during this part of the proce-dure; this can aid in the identification of the esophagus,which can be a difficult task.
After the esophagus is fully mobilized, a posteriorcruroplasty is performed with nonpledgeted, interrupted
sutures of braided polyester. If an anterior hiatal defect ispresent at this point, then we also will a employ a 1–2stitch anterior cruroplasty. A P TFE patch then iscustom-cut from a larger sheet of mesh (see Fig. 23); a“keyhole” (3.5 cm circular defect) is cut into the center ofthe mesh to accommodate the esophagus (Fig. 23). Thepatch is introduced into the abdomen through a trocar(avoiding contact with the skin), and then applied as anonlay to the diaphragmatic repair, ensuring that the ma-croporous (rough) surface of the mesh faces the dia-phragm. The prosthetic is anchored in place with a rigidlaparoscopic hernia stapler (see Fig. 24). This 10 mminstrument fires titanium staples; we have found its per-formance optimal for securing PTFE to the diaphragm.The procedure is completed with a floppy 3-stitch,2 cm-long Nissen fundoplication, performed over a 50–60 Fr bougie.
There are issue regarding the technique of mesh fix-ation to the diaphragm; specifically, whether to apply themesh as on onlay, or to perform a “tension-free” repair.We have preferred the former; that is, to complete a pri-mary cruroplasty first, and then to cover the cruroplastywith an onlay patch. In this situation, the mesh acts as abuttress for the sutured cruroplasty, relieving the tissuerepair from the forces of intraabdominal pressure, respi-ratory excursion, and so forth. In the tension-free repair,the crura are not approximated; the mesh bridges thenative defect. At this point in time there is no evidencefrom the field of mesh hiatal herniorrhaphy to supportthe use of onlay repair over tension-free repair (or visaversa). Our preference for the onlay repair has been ourpractice pattern, and we have had and continue to havesalutary results from this practice. Practically speaking, itis easier to staple the mesh in place around the esopha-Fig. 22. The “Zell” mesh
Fig. 23. PTFE onlay patch is constructed to have an oval shapewith a horizontal diameter of 12 cm and anterior-posterior di-mension of 10 cm. A 3.5 cm “keyhole” is made in the center of themesh in order to accommodate passage of the esophagus

226 Chapter 21
The actual firing of the stapler can be a “tricky”maneuver, because unfortunate stapler deployment caninjure the heart, which can result in fatal outcomes [31].The precise technical details in stapling P TFE to thediaphragm with proximity of the heart are difficult toconvey in written form. The surgeon must use enoughpressure on the stapler to ensure that the staple pene-trates the prosthesis and secures an adequate tissue bite,but not so much pressure that the staple penetrates thediaphragm and breaches the pericardium. The attain-ment of this skill is facilitated with training, anatomicknowledge, and experience.
Recent results with laparoscopic mesh-reinforced diaphragmatic hernia repair
Since the conclusion of our randomized trial [25] wehave routinely employed P TFE mesh reinforcementduring minimally invasive repair of large hiatal hernia.We have decreased our threshold for mesh usage to hiataldefects whose diameter is in the range of 5–6 cm. Ouroriginal indication for the utilization of P TFE re-inforcement during hiatal herniorrhaphy was a defect sizeof � 8 cm; this cut-off size is relatively large. Since we had an impressive difference in outcome between the control and mesh groups in our randomized trial [25]we felt justified in broadening the indication for meshusage. Since 2000, we have performed 63 minimally invasive hiatal hernia repairs; P TFE was employed in28 (44%) of these herniorrhaphies. Since 1992 sixty fourpatients have undergone laparoscopic large hiatal herniarepairs with placement of P TFE prosthesis. We have yet
gus when it is surrounded by the sutured crura. In asmall number of cases, it will be impossible to suture thecrura together secondary to excessive tension, poor tis-sue, or other reasons. In these situations a tension-freeapplication of the prosthetic should be employed. In thefinal analysis, it likely is the presence of the mesh itself(and not whether it is applied as an onlay or a bridge)which prevents hernia recurrence.
We believe that in order for the mesh to have an op-timal effect (i.e., producing the lowest possible recur-rence rate), the mesh should cover the repair with alarge “overlap”. That is, the mesh should extend beyondthe crural margins by as much as the local anatomy willallow (see Fig. B). Practically speaking, extension of themesh in this location is limited to the right by the infe-rior vena cava, anteriorly by the left lobe of the liver,posteriorly by retroperitoneal structures and to the leftby the spleen. Thus caution should be taken to avoidinjury to any of these structures. The importance of sev-eral centimeters of mesh extension beyond the entirecircumference of a hernial defect has been borne out bya large amount of retrospective data from underlay re-pair of ventral herniorrhaphy, both open and laparo-scopic [29], [30] For example, if a surgeon is faced witha 4 cm round-shaped ventral hernia, then the diameterof the mesh used in an underlay repair typically shouldbe 8–10 cm, which permits a 2–3 cm extension of themesh beyond the entire circumference of the defect.While it is difficult to satisfy these same criteria formesh coverage of a hiatal defect, the precept of meshoverlap of the hernial defect should be kept in mindwhen applying this technique to a hiatal hernia.
Fig. 24. Completed mesh repair of a hiatal hernia. The crura firstwere closed with simple sutures of 2�0 braided polyester, andthen a patch as shown in the previous figure was applied to thecruroplasty (i.e., as an onlay) and stapled circumferentially inplace. Note the extensive overlap of the repair by the mesh

Granderath FA et al 227
to document a recurrence after mesh reinforcement ofminimally invasive hiatal hernia repair with our tech-nique described above. In addition, no patient has beendocumented to have mesh infection, erosion, or contrac-tion (“mesh shrinkage” [32]). We have noted in the lit-erature a few reported cases reports of PF TE erosion intoa gastrointestinal lumen (see below), but this has not dis-suaded us from using P TFE-onlay reinforcement of su-tured cruroplasty for the repair of the large hiatal defect.
Complications of prosthetic hiatal repair
The use of prosthetic materials in surgery for gastro-esophageal reflux disease and/or large hiatal hernia re-pair is accompanied by alow incidence of foreign bodycomplications. For instance, the use of Teflon-pledgetsin fundoplication has been associated with visceral ero-sion, foreign body migration, or gastroesophageal fistulaafter surgery [33]–[35].
In particular, a risk for complications related to theuse of prosthetic materials for closure of the hiatalcrura has been predicted by some authors. The focus ison the possibility of erosion or migration of the meshinto the esophagus or stomach, as well as compli-cations due to severe mesh adhesions, infection, or thedevelopment of fibrotic strictures in the hiatal area. Ina study by Carlson et al [26], one patient (2.3%) out of44 who underwent open prosthetic hiatal closure forlarge hiatal hernia repair developed a mesh erosioninto the esophagus 29 months after surgery. Edelmanet al [36] reported one patient out of 5 who had to un-dergo revisional surgery after primary laparoscopic pa-raesophageal hernia repair with mesh. This patientshad severe dysphagia due to esophageal stenosis sec-ondary to mesh-induced fibrosis. Likewise, Trus et al[37] also saw one patient who had undergone primarylaparoscopic mesh repair for paraesophageal herniawho then suffered from refractory postoperative dys-phagia. During re-laparotomy the authors found a cir-cular scar at the distal esophagus caused by the hiatalmesh. The mesh had to be excised, a myotomy wasperformed, and then the crura were approximated.Persistent postoperative dysphagia refractory to dilata-tions was reported by Van der Peet et al [38]. One pa-tient who underwent laparoscopic hiatal hernia repairwith Dacron mesh reinforcement had a significant fi-brotic reaction to the mesh; This had to be removed
during a reoperation. Another two patients withmesh-related complications were reported byCasabella et al [39]. One patient developed fibroticdamage at the hiatus postoperatively; the other patienthad a mesh erosion into the esophagus. Both of thesepatients underwent redo-surgery and required distalresection of the esophagus because of the mesh intru-sion into the lumen. Coluccio et al [40] also reportedabout one case who required resection of the distalesophagus due to a mesh-related complication. Thispatient underwent large hiatal hernia repair with theuse of a P TFE prosthesis which subsequently migrat-ed into the cardial lumen. During reoperation themesh had to be removed, and the patient required adistal esophageal resection. A fatal complication wasdescribed by Kemppainen et al [31]. This patient hada large paraesophageal hernia with acute thoracicherniation and incarceration of the stomach, and underwent laparoscopic hiatal hernia repair withtension-free hiatoplasty using P TFE. Fixation of themesh was undertaken with a hernia stapler. Aftersurgery, this patient developed a cardiac tamponadecaused by a stapler laceration of a coronary vein.
Although there has been a limited number ofcomplications related to prosthetic mesh after lapa-roscopic antireflux surgery or large hiatal herniarepair, some authors recommend the use of bioma-terials or autologous tissue to avoid any risk of com-plication secondary to prosthetic mesh. Varga et al[20] advocated the use of ligamentum teres for reinforcement of the hiatal crura in four patientswith a hiatal hernia � 6 cm. In a similar way, thesuccessful use of biomaterial has been described byOelschlager et al [19]. Nine patients underwent lap-aroscopic paraesophageal hernia repair with the useof a porcine small intestine submucosa (SIS) meshfor crural closure to avoid mesh-related esophagealor gastric injury.
Conclusion and future perspectives
In general, hiatal reinforcement with the use pros-thetic meshes has proven to be a safe and effectiveprocedure to prevent postoperative hiatal hernia re-currence and/or postoperative intrathoracic migra-tion of the fundic wrap in both laparoscopic surgeryfor hiatal or paraesophageal hernia repair as well as

228 Chapter 21
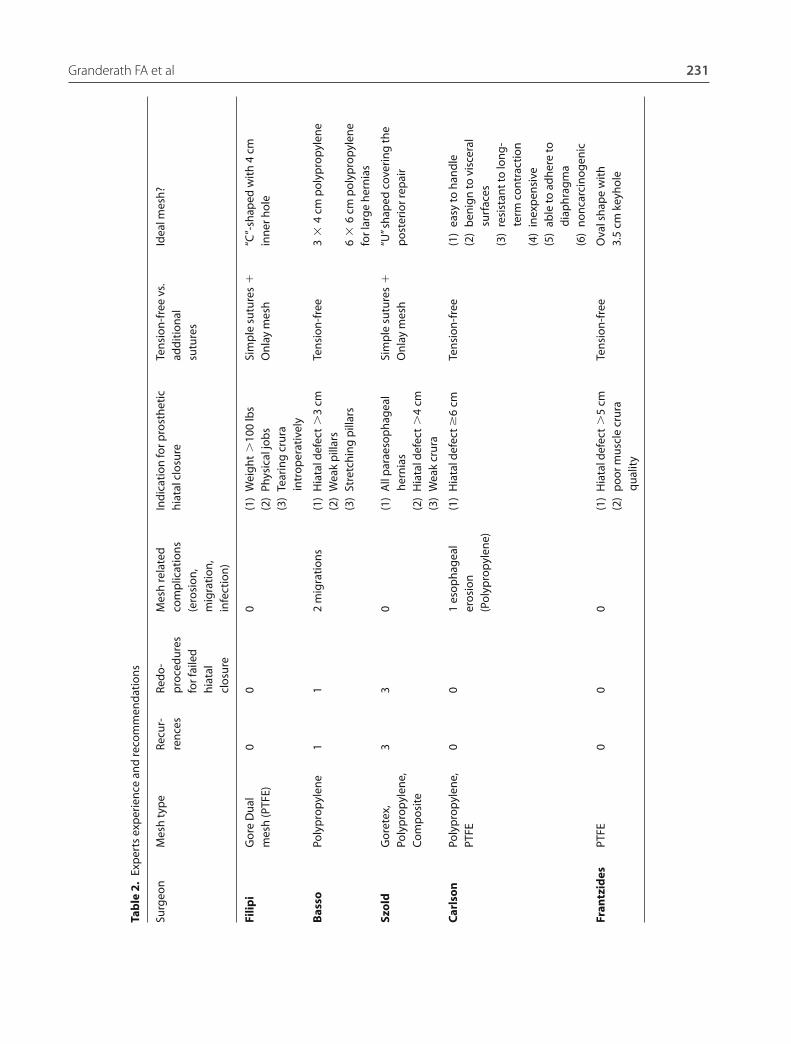
Carlson (Omaha, USA) have reduced their originalindication of hiatal defect � 8 cm to a typical cut-offpoint of 5–6 cm. Other factors like body mass indexor sociodemographic aspects may influence the indi-cation somewhat, but the primary indication forthem has remained the size of the hiatus. Dr. Szold(Tel Aviv, Israel) recommends the use of meshes inall patients with paraesophageal hernias, in all hiatalhernias � 4 cm, or in patients in whom the cruraseem weak or damaged.
Regarding the characteristics of the mesh, mostauthors agree that the ideal mesh has to be easy tohandle during laparoscopy, able to adhere to thediaphragmatic surface on the one side, and bebenign to the visceral surface on the other side. Itshould be resistant to infection and to long-termcontraction.
The shape of the mesh is still a matter of con-troversy. Most authors recommend a posterior onlayrepair; others have advocated the use of circular pros-theses with good results. This topic will be a matter offuture research, especially when long-term results ofpublished series are available. An overview of expertsrecommendations is shown in Table 2.
in laparoscopic antireflux surgery for gastroesopha-geal reflux disease. A few comparative studies andtrials of laparoscopic hiatal closure with simple su-tures versus mesh-hiatoplasty have shown, that pa-tients with a prosthetic hiatal closure had a lower rateof postoperative hiatal hernia recurrences in compar-ison to patients with simple hiatal repair. Some pa-tients with prosthetic hiatal closure, however, sufferfrom prolonged postoperative symptoms like dyspha-gia or chest pain; Fortunately, this resolves in mostof the patients without further treatment. A truecomplication related to the use of prosthetic mate-rial for hiatal closure is a rare condition when theprocedure is performed properly.
A consensus regarding a standard indication forthe use of prosthetic mesh for hiatal closure does notexist at this time. Some authors advocate the use ofprosthetic meshes empirically only in patients inwhom a tension-free crural closure with simple su-tures seems impossible. Some authors, however, em-ploy prosthetic hiatoplasty in a more liberal matter.These authors agree that the primary indication forprosthetic hiatal closure should be the size of the hi-atal defect. Dr. Frantzides (Chicago, USA) and Dr.
Granderath FA et al 229
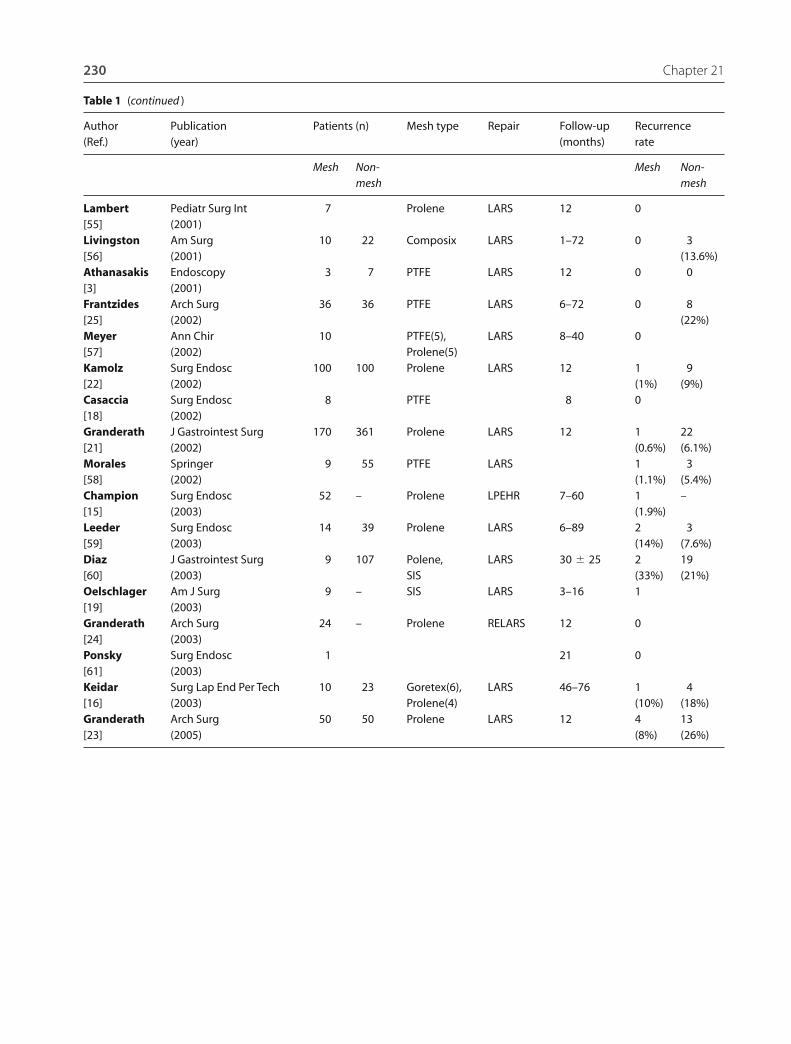
Table 1. Results of laparoscopic hiatal hernia repair with mesh prosthesis
Author Publication Patients (n) Mesh type Repair Follow-up Recurrence (Ref.) (year) (months) rate
Mesh Non- Mesh Non-mesh mesh
Kuster J Laparoendosc Surg 6 – Mersilene LPEHR 8–22 0 –[5] (1993)Pitcher Arch Surg 2 10 PTFE LPEHR(4), – 0 0[42] (1995) LARS(8)Odsdottir Surg Endsoc 10 – LARS 8.9 0[43] (1995)Edelman Surg Laparosc Endosc 5 – Surgipro LARS – 0[37] (1995)Behrns J Laparoendosc Surg 2 10 LPEHR(5), 6 0 0[44] (1996) LARS(7)Trus J Gastrointest Surg 1 75 LPEHR(5), � 16 5(7%)[38] (1997) LARS(71)Huntington J Am Coll Surg 8 – Prolene 8 0[14] (1997)Paul Surg Endosc 3 – PTFE LPEHR(2), 10 0[12] (1997) LARS(1)Willekes Ann Surg 30 PTFE LARS 0[45] (1997)Frantzides Surg Endosc 3 – PTFE LARS � 11 0[17] (1997)Medina JSLS 2 18 Goretex LPEHR(6), 6–48 0 0[46] (1998) LARS(14)Hawasli Am Surg 27 Prolene LARS 1–56 0[47] (1998)Carlson J Am Coll Surg 44 – Prolene PEHR 52 0 –[36] (1998)Simpson Am Surg 38 – Dacron LARS 15 0[48] (1998)Schulz Abstract 161 157 Prolene LARS 2 12[49] (1998) (1.2%) (7.1%)Horgan Am J Surg 5 36 LARS 0 0[50] (1999)Wu Surg Endosc 6 – Marlex LARS[51] (1999)Carlson Dig Surg 15 16 PTFE LARS 12–36 0 3[52] (1999) (18.8%)Frantzides Surg Endosc 17 18 PTFE LARS 36 0 3[53] (1999) (16.6%)Basso Surg Endosc 67 65 Prolene LARS 22.5–48.3 0 9[13] (2000) (13.8%)Hui Am Surg 12 12 Goretex(8), LARS 24–48 0 0[54] (2001) Marlex(2),
Prolene(2)
(continued )
230 Chapter 21
Table 1 (continued )
Author Publication Patients (n) Mesh type Repair Follow-up Recurrence (Ref.) (year) (months) rate
Mesh Non- Mesh Non-mesh mesh
Lambert Pediatr Surg Int 7 Prolene LARS 12 0[55] (2001)Livingston Am Surg 10 22 Composix LARS 1–72 0 3[56] (2001) (13.6%)Athanasakis Endoscopy 3 7 PTFE LARS 12 0 0[3] (2001)Frantzides Arch Surg 36 36 PTFE LARS 6–72 0 8[25] (2002) (22%)Meyer Ann Chir 10 PTFE(5), LARS 8–40 0[57] (2002) Prolene(5)Kamolz Surg Endosc 100 100 Prolene LARS 12 1 9[22] (2002) (1%) (9%)Casaccia Surg Endosc 8 PTFE 8 0[18] (2002)Granderath J Gastrointest Surg 170 361 Prolene LARS 12 1 22[21] (2002) (0.6%) (6.1%)Morales Springer 9 55 PTFE LARS 1 3[58] (2002) (1.1%) (5.4%)Champion Surg Endosc 52 – Prolene LPEHR 7–60 1 –[15] (2003) (1.9%)Leeder Surg Endosc 14 39 Prolene LARS 6–89 2 3[59] (2003) (14%) (7.6%)Diaz J Gastrointest Surg 9 107 Polene, LARS 30 � 25 2 19[60] (2003) SIS (33%) (21%)Oelschlager Am J Surg 9 – SIS LARS 3–16 1[19] (2003)Granderath Arch Surg 24 – Prolene RELARS 12 0[24] (2003)Ponsky Surg Endosc 1 21 0[61] (2003)Keidar Surg Lap End Per Tech 10 23 Goretex(6), LARS 46–76 1 4[16] (2003) Prolene(4) (10%) (18%)Granderath Arch Surg 50 50 Prolene LARS 12 4 13[23] (2005) (8%) (26%)
Granderath FA et al 231
Tab
le 2
.Ex
per
ts e
xper
ien
ce a
nd
reco
mm
end
atio
ns
Surg
eon
Mes
h t
ype
Recu
r-Re
do
-M
esh
rela
ted
Ind
icat
ion
for p
rost
het
icTe
nsi
on
-fre
e vs
.Id
eal m
esh
?re
nce
sp
roce
du
res
com
plic
atio
ns
hia
tal c
losu
read
dit
ion
alfo
r fai
led
(ero
sio
n,
sutu
res
hia
tal
mig
rati
on
,cl
osu
rein
fect
ion
)
Filip
iG
ore
Du
al
00
0(1
)W
eig
ht
�10
0lb
sSi
mp
le s
utu
res
�“C
”-sh
aped
wit
h 4
cmm
esh
(PTF
E)(2
)Ph
ysic
al jo
bs
On
lay
mes
hin
ner
ho
le(3
)Te
arin
g c
rura
in
tro
per
ativ
ely
Bas
soPo
lyp
rop
ylen
e1
12
mig
rati
on
s(1
)H
iata
l def
ect
�3
cmTe
nsi
on
-fre
e3
�4
cm p
oly
pro
pyl
ene
(2)
Wea
k p
illar
s(3
)St
retc
hin
g p
illar
s6
�6
cm p
oly
pro
pyl
ene
for l
arg
e h
ern
ias
Szo
ldG
ore
tex,
33
0(1
)A
ll p
arae
sop
hag
eal
Sim
ple
su
ture
s�
“U”s
hap
ed c
over
ing
th
ePo
lyp
rop
ylen
e,h
ern
ias
On
lay
mes
hp
ost
erio
r rep
air
Co
mp
osi
te(2
)H
iata
l def
ect
�4
cm(3
)W
eak
cru
ra
Car
lso
nPo
lyp
rop
ylen
e,0
01
eso
ph
agea
l (1
)H
iata
l def
ect
�6
cmTe
nsi
on
-fre
e(1
)ea
sy to
han
dle
PTFE
ero
sio
n(2
)b
enig
n to
vis
cera
l(P
oly
pro
pyl
ene)
surf
aces
(3)
resi
stan
t to
lon
g-
term
co
ntr
acti
on
(4)
inex
pen
sive
(5)
able
to a
dh
ere
tod
iap
hra
gm
a(6
)n
on
carc
ino
gen
ic
Fran
tzid
esPT
FE0
00
(1)
Hia
tal d
efec
t�
5cm
Ten
sio
n-f
ree
Ova
l sh
ape
wit
h
(2)
po
or m
usc
le c
rura
3.5
cm k
eyh
ole
qu
alit
y
232 Chapter 21
References
[1] Dent J, Jones R, Kahrilas P, Talley NJ (2001) Manage-ment of gastro-oesophageal reflux disease in general prac-tice. BMJ 322: 344
[2] Spechler SJ (1992) Epidemiology and natural history ofgastro-oesophageal reflux disease. Digestion 51: 24
[3] Athanasakis H, Tzortzinis A, Tsiaoussis J, Vassilakis JS,Xynos E (2001) Laparoscopic repair of paraesophagealhernia. Endoscopy 33: 590–594
[4] Hashemi M, Peters JH, DeMeester TR, Huprich JE,Quek M, Hagen JA, Crookes PF, Theisen J, DeMeesterSR, Sillin LF, Bremner CG (2000) Laparoscopic repairof large type-III hiatal hernia: objective followup revealshigh recurrence rate. J Am Coll Surg 190(5): 553–560;Discussion 560–561
[5] Kuster GG, Gilroy S (1993) Laparoscopic technique forrepair of paraesophageal hiatal hernias. J LaparoendoscSurg 3: 331–338
[6] Perdikis G, Hinder RA, Filipi CJ, Walenz T, McBridePJ, Smith SL, Katada N, Klingler PJ (1997) Laparosopicparaesophageal hernia repair. Arch Surg 132: 586–590
[7] Hunter JG, Smith CD, Branum GD et al (1999) Lap-aroscopic fundoplication failures: patterns of failure andresponse to fundoplication revision. Ann Surg 230:595–604
[8] Soper NJ, Dunnegan D (1999) Anatomic fundoplicationfailure after laparoscopic antireflux surgery. Ann Surg229: 669–677
[9] Granderath FA, Kamolz T, Schweiger UM, Pointner R(2004) Quality of life, patients satisfaction and surgi-cal outcome after laparoscopic refundoplication: experi-ences with 100 laparoscopic redo-procedures. SurgEndosc (Suppl 18): O212
[10] Carlson MA, Frantzides CT (2001) Complications andresults of primary minimally invasive antireflux proce-dures: a review of 10,735 reported cases. J Am Coll Surg193: 428–439
[11] Ponce JF, Barriga R, Martin I, Morales Conde S,Morales S (1998) Prosthetic materials in incisionalhernia. Experimental study. Cir Esp 63: 189–194
[12] Paul MG, De Rosa RP, Petrucci PE, Palmer ML,Danovitch SH (1997) Laparoscopic tension-free repair oflarge paraesophageal hernias. Surg Endosc 11: 303–307
[13] Basso N, DeLeo A, Genco A et al (2000) 360� laparo-scopic fundoplication with tension – free hiatoplasty inthe treatment of symptomatic gastroesophageal refluxdisease. Surg Endosc; 14: 164–169
[14] Huntington TR (1997) Laparoscopic mesh repair ofthe oesophageal hiatus. J Am Coll Surg 184: 399–401
[15] Champion JK, Rock D (2003) Laparoscopic mesh cru-ro plasty for large paraesophageal hernias. Surg Endosc17: 551–553
[16] Keidar A, Szold A (2003) Laparoscopic repair of para-esophageal hernia with selective use of mesh. Surg Lap-arosc Endosc 13: 149–154
[17] Frantzides CT, Carlson MA (1997) Prosthetic reinforce-ment of posterior cruroplasty during laparoscopic hiatalherniorraphy. Surg Endosc 11: 769–771
[18] Casaccia M, Torelli P, Panaro F, Cavaliere D, Ventura A,Valente U (2002) Laparoscopic physiologic hiatoplastyfor hiatal hernia: new composite “A” shaped mesh. SurgEndosc 16: 1441–1445
[19] Oelschlager BK, Barreca M, Chang L, Pellegrini CA(2003) The use of small intestine submucosa in the re-pair of paraesophageal hernias: initial observations of anew technique. Am J Surg 186(1): 4–8
[20] Varga G, Cseke L, Kalmar K, Horvath OP (2004) Pre-vention of recurrence by reinforcement of hiatal closureusing ligamentum teres in laparoscopic repair of largehiatal hernias. Surg Endosc 18: 1051–1053
[21] Granderath FA, Schweiger UM, Kamolz T et al (2002)Laparoscopic antireflux surgery with routine mesh-hiato-plasty in the treatment of gastroesophageal reflux disease.J Gastrointest Surg 6: 347–353
[22] Kamolz T, Granderath FA, Bammer T, Pasiut M,Pointner R (2002) Dysphagia and quality of life afterlaparoscopic Nissen fundoplication in patients with andwithout prosthetic reinforcement of the hiatal crura.Surg Endosc 16(4): 572–577
[23] Granderath FA, Schweiger UM, Kamolz T, Asche KU,Pointner R (2005) Laparoscopic Nissen fundoplicationwith prosthetic hiatal closure reduces postoperative in-trathoracic wrap herniation: Preliminary results of a pro-spective randomized functional and clinical study. ArchSurg 140: 40–48
[24] Granderath FA, Kamolz T, Schweiger UM et al (2003)Laparoscopic refundoplication with prosthetic hiatalclosure for recurrent hiatal hernia after primary failedantireflux surgery. Arch Surg 138: 902–907
[25] Frantzides CT, Madan AK, Carlson MA et al (2002) A prospective, randomized trial of laparoscopic poly-tetraflouroethylene (PTFE) patch repair vs simple cruro-plasty for large hiatal hernia. Arch Surg 137: 649–653
[26] Carlson MA, Condon RE, Ludwig KA, Schulte WJ(1998) Management of intrathoracic stomach withpolypropylene mesh prosthesis reinforced transabdominalhiatus hernia repair. J Am Coll Surg 187(3): 227–230
[27] Voyles CR, Richardson JD, Bland KI et al (1981) Emer-gency abdominal wall reconstruction with polypropylene
Granderath FA et al 233
mesh: short-term benefits versus long-term compli-cations. Ann Surg 194(2): 219–223
[28] Frantzides CT, Carlson MA (2001) Paraesophagealherniation. In: Mastery of surgery, vol. 1 (Baker RJ,Fischer JE, eds). Philadelphia: Lippincott Williams &Wilkins, pp 721–736
[29] Wantz GE (1991) Atlas of hernia surgery. New York:Raven Press
[30] Heniford BT, Park A, Ramshaw BJ, Voeller G (2003)Laparoscopic repair of ventral hernias: nine years’experience with 850 consecutive hernias. Ann Surg238(3): 391–399; Discussion 399–400
[31] Kemppainen E, Kiviluoto T (2000) Fatal cardiac tam-ponade after emergency tension-free repair of a largeparaesophageal hernia. Surg Endosc 14(6): 593
[32] Amid PK (2004) Shrinkage: Fake or Fact? In: Meshes:benefits and risks (Schumpelick V, Nyhus LM, eds).Berlin: Springer, pp 198–206
[33] Baladas HG, Smith GS, Richardson MA, DempseyMB, Falk GL (2000) Esophagogastric fistula secondaryto teflon pledget: a rare complication following laparo-scopic fundoplication. Dis Esophagus 13: 72–74
[34] Arendt T, Stuber E, Monig H, Folsch UR, Katsoulis S(2000) Dysphagia due to transmural migration of sur-gical material into the esophagus nine years after Nissenfundoplication. Gastrointestinal Endosc 51: 607–610
[35] Dally E, Falt GL (2004) Teflon pledget reinforcedfundoplication causes symptomatic gastric and esophageallumenal penetration Am J Surg 187: 226–229
[36] Carlson MA, Condon RE, Ludwig KA, Schulte WJ(1998) Management of intrathoracic stomach with poly-propylene mesh prosthesis reinforced transabdominal hi-atus hernia repair. J Am Coll Surg 187: 227–230
[37] Edelman DS (1995) Laparoscopic paraesophageal herniarepair with mesh. Surg Laparosc Endosc 5: 32–37
[38] Trus TL, Bax T, Richardson WS, Branum GD,Mauren SJ, Swanstrom LL, Hunter JG (1997) Com-plications of laparoscopic paraesophageal hernia repair.J Gastrointest Surg 1: 221–228
[39] Van der Peet DL, Klinkerberg-Knol EC, Alonso A,Sietses C, Eijsbouts QAJ, Cuesta MA (2000) Laparo-scopic treatment of large paraesophageal hernias. SurgEndosc 14: 1015–1018
[40] Casabella F, Sinanan M, Horgan S, Pellegrini CA(1996) Systematic use of gastric fundoplication in lap-aroscopic repair of paraesophageal hernias. Am J Surg171: 485–489
[41] Coluccio G, Ponzio S, Ambu V, Tramontano R,Cuomo G (2000) Dislocation into the cardial lumen ofa PTFE prosthesis used in the treatment of volumin-
ous hiatal sliding hernia, a case report. Minerva Chir55: 341–345
[42] Pitcher DE, Curet MJ, Vogt DM, Mason J, Zucker KA(1995) Successful repair of praesophageal hernia. ArchSurg 130: 590–596
[43] Oddsdottir M, Franco AL, Laycock WA, Waring JP,Hunter JG (1995) Laparoscopic repair of paraesophagealhernia. New access, old technique. Surg Endosc 9: 164–168
[44] Behrns KE, Schlinkert RT (1996) Laparoscopicmanagement of paraesophageal hernia: early results.J Laparoendosc Surg 6: 311–317
[45] Willekes CL, Edoga JK, Freeza EE (1997) Laparoscopicrepair of paraesophageal hernia. Ann Surg 225: 31–38
[46] Medina L, Peetz M, Ratzer E, Fenoglio M (1998) Lapa-roscopic paraesophageal hernia repair. JSLS 2: 269–272
[47] Hawasli A, Zonca S (1998) Laparoscopic repair ofparaesophageal hiatal hernia. Am Surg 64: 703–710
[48] Simpson B, Ricketts RR, Parker PM (1998) Prostheticpatch stabilization of crural repair in antireflux surgeryin children. Am Surg 64: 67–70
[49] Schulz HG (1998) Rezidivrate nach laparoskopischerAntirefluxoperation mit und ohne Prolenenetzplastikbei 318 Fällen – erste Ergebnisse. 7. Jahreskongress derGesellschaft für Gastroenterologie Westfalen
[50] Horgan S, Eubanks TR, Jacobsen G, Omelanczuk P,Pellegrini CA (1999) Repair of paraesophageal hernias.Am J Surg 177: 354–358
[51] Wu JS, Dunnegan DL, Soper NJ (1999) Clinical andradiologic assessment of laparoscopic paraesophagealhernia repair. Surg Endosc 13: 497–502
[52] Carlson MA, Richards CG, Frantzides CT (1999)Laparoscopic prosthetic reinforcement of hiatal her-niorrhaphy. Dig Surg 16: 407–410
[53] Frantzides CT, Richards CG, Carlson MA (1999)Laparoscopic repair of large hiatal hernia with poly-tetrafluoroethylene. Surg Endosc 13: 906–908
[54] Hui TT, David T, Spyrou M, Phillips EH (2001) Meshcrural repair of large paraesophageal hiatal hernias. AmSurg 67: 1170–1174
[55] Lambert AW, Huddart SN (2001) Mesh hiatal re-inforcement in Nissen funduplication. Pediatr Surg Int17: 491–492
[56] Livingston CD, Lamar Jones H, Askew RE, VictorBE, Askew RE (2001) Laparscopic hiatal hernia repairin patients with poor esophageal motility or para-esophageal herniation. Am Surg 67: 987–991
[57] Meyer C, Bufffler A, Rohr S, Lima MC (2002) Letraitement laparoscopique des hernies hiatales de grantaille avec mise en place d’une prothese. A propos dedix cas. Ann Chir 127: 257–261

234 Chapter 21
[58] Morales Conde S, Ponce JF, Morales Mendez S(2002) Paraesophageal hernia: technique and methodof fixation a mesh by laparoscopy. In: Laparoscopicventral hernia repair (Morales-Conded S, ed).Springer
[59] Leeder PC, Smith G, Dehn TC (2003) Laparoscopicmanagement of large paraesophageal hiatal hernia.Surg Endosc 17: 1372–1375
[60] Díaz S, Brunt M, Klingensmith ME, Frisella PM, So-per NJ (2003) Laparoscopic paraesophageal hernia re-pair, a challenging operation: medium-term outcome of116 patients. J Gastroint Surg 7: 59–67
[61] Ponsky J, Rosen M, Fanning A, Malm J (2003) An-terior gastropexy may reduce the recurrence after lapa-roscopic paraesophageal hernia repair. Surg Endosc 17:1036–1041