healthrelatedqualityoflife* in*romanian*cochlear* implantedpaents · ·...
TRANSCRIPT

Health-‐related quality of life in Romanian cochlear implanted pa6ents
M COSGAREA, Violeta NECULA “Iuliu Ha6eganu” University of Medicine and Pharmacy Cluj-‐Napoca, ROMANIA ENT Department – Head of Dept Prof Dr Marcel COSGAREA

Introduc6on • Cochlear implant -‐ the best solu3on for severe to profound sensorineural hearing
loss • improves hearing thresholds • the pa3ent learns to understand speech sounds • achieve language • promotes communica3on, influencing posi3vely the pa3ent’s quality of life -‐ an
important impact on the pa3ent psyche, confidence, daily and social ac3vi3es

• HRQoL -‐ the pa3ent’s percep3on about his disease and treatment impact -‐ from physical, psychological and social point of view -‐ the individual’s ability to enjoy daily life normal ac3vi3es, including func3onal capacity and well being
• Nijmegen Cochlear Implant Ques3onnaire -‐ a disease-‐specific ques3onnaire for hearing loss and cochlear implant, assessing three main areas, which characterize the pa3ent’s subjec3ve health status -‐ six sub-‐domains – Physical status -‐ three sub-‐domains that reflect the pa3ent’s auditory and verbal func3on -‐
sound percep3on (basal and advanced level) and speech produc3on – Psychological domain -‐ self assessment, self-‐confidence and social func3onality -‐ self-‐esteem/
self-‐confidence – Social domain -‐ degree of ac3vity limita3on and socializa3on ability -‐ daily ac3vi3es and social
interac3on sub-‐domains
Introduc6on

Materials and methods • Study group -‐ 84 children, cochlear implanted in a ter3ary ENT Department in
Romania, between 2003 and 2009. • Unilateral MedEl devices, more than 6 months of experience • The cochlear implanted group was divided into two subgroups, according the age
of implanta3on – G1 subgroup of children implanted before the age of 5 years (less than 60 months) – G2 subgroup of children implanted aYer the age of 5 years (more than 60 months).
• Control group -‐ 50 hearing aided children (less than 18 years old) with severe or profound bilateral sensorineural hearing loss, congenital or acquired prelingually -‐ Some of these children were subsequently cochlear implanted.

• 84 families of 102 responded to the ques3onnaire and gave their acceptance for the study.
• The ques3onnaire was filled out by parents or child’s proxy. • Items related to child hearing loss (onset, e3ology), addi3onal disabili3es,
about family, educa3onal environment and ques3ons related to the quality of life.
• HRQL -‐ The physical, psychological and social domains consist of six subdomains -‐ 10 ques3ons each with 6 answers on the Lickert scale, from 0 to 5, 0-‐unfavorable responses, and 5-‐excellent situa3on. For each subdomain a percentage score was calculated.
• CAPr (revised category of auditory performance) and SIR (speech intelligibility ra3ng) – for speech percep3on and produc3on assessment
Materials and methods

Results Sta6s6cal data
• Study group -‐ 84 cochlear implanted children – Age between 19 and 219 months (mean 91.42±49.83 months) – 35.7% female, 64.3% male – Hearing loss onset: 1.26( SD 3.36) months – Age at implanta3on – 12months to 191 months (mean 62.86±41.59 months) – Processor use – 6 to 92 months (27.07±21.82 months)
• Control group – 50 hearing aided children – age between 15 and 134 months (mean 66.36 27.47 months), – 44% females and 56% male – hearing aids use -‐ between 6 and 96 months (33.46 22.692 months). – hearing loss onset -‐ 0.85(SD 2.30 )months.

45.8
30.6 36
0
10
20
30
40
50
CI Group 1 CI Group 2 Control group
Unknown
Hereditary
Ototoxic
Birth trauma
Congenital rubella
Meningi3s
Prematurity
CMV infec3on
Results E6ology

Results Sta6s6cal data
CI group 1 CI group 2 Control group
Parents educa6onal level -‐ medium degree -‐ high degree
33.33% 66.67%
33.33% 66.67%
90.0% 10.0%
Daily use of device -‐ Intermiient -‐ Permanent
6.3% 93.7%
27.8% 72.2%
44.0% 56.0%
Communica6on mode -‐ Verbal -‐ Mixed -‐ Sign
35.4% 64.6% 0
44.4% 52.8% 2.8%
26.0% 36.0% 38.0%
Associated diseases -‐ Gluten intolerance -‐ CleY palate -‐ Oesophageal atresia -‐ Hypotyroidism -‐ Asthma -‐ Myopia -‐ Re3nal detachment -‐ Re3ni3s pigmentosa -‐ Squint -‐ Learning disturbances, ADHD
N=8 1 1 1 1 1 3
N=9 4 2 3
N=13 2 1 2 1 2 5
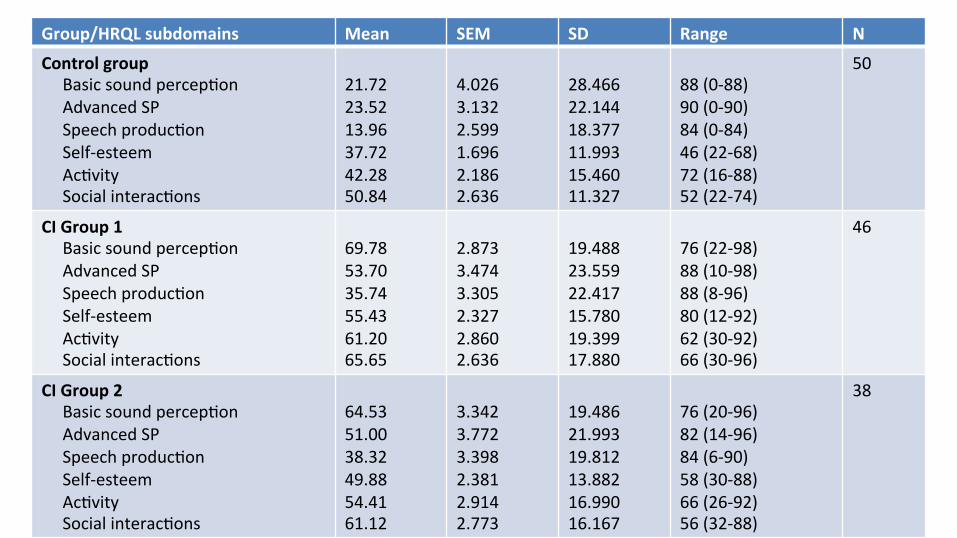
Group/HRQL subdomains Mean SEM SD Range N
Control group Basic sound percep3on Advanced SP Speech produc3on Self-‐esteem Ac3vity Social interac3ons
21.72 23.52 13.96 37.72 42.28 50.84
4.026 3.132 2.599 1.696 2.186 2.636
28.466 22.144 18.377 11.993 15.460 11.327
88 (0-‐88) 90 (0-‐90) 84 (0-‐84) 46 (22-‐68) 72 (16-‐88) 52 (22-‐74)
50
CI Group 1 Basic sound percep3on Advanced SP Speech produc3on Self-‐esteem Ac3vity Social interac3ons
69.78 53.70 35.74 55.43 61.20 65.65
2.873 3.474 3.305 2.327 2.860 2.636
19.488 23.559 22.417 15.780 19.399 17.880
76 (22-‐98) 88 (10-‐98) 88 (8-‐96) 80 (12-‐92) 62 (30-‐92) 66 (30-‐96)
46
CI Group 2 Basic sound percep3on Advanced SP Speech produc3on Self-‐esteem Ac3vity Social interac3ons
64.53 51.00 38.32 49.88 54.41 61.12
3.342 3.772 3.398 2.381 2.914 2.773
19.486 21.993 19.812 13.882 16.990 16.167
76 (20-‐96) 82 (14-‐96) 84 (6-‐90) 58 (30-‐88) 66 (26-‐92) 56 (32-‐88)
38

Results Quality of life assessment
Mean values of HRQoL subdomains in the two study groups (G1 and G2) and in the control group; asterisks indicate a sta3s3cally significant difference between groups (p < 0.05).

Results HRQL -‐ associated diseases
• The presence of associated diseases -‐ a nega3ve impact on auditory-‐verbal performances, also on health-‐related quality of life, regardless the type of device.
• Children with associated diseases -‐ poorer results than those without problems regardless of hearing device (conven3onal or implantable).
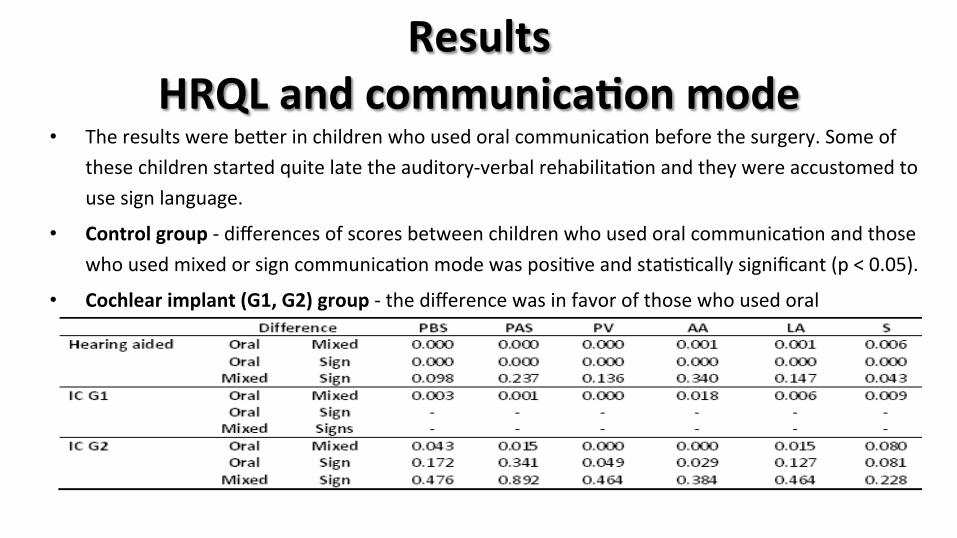
Results HRQL and communica6on mode
• The results were beier in children who used oral communica3on before the surgery. Some of these children started quite late the auditory-‐verbal rehabilita3on and they were accustomed to use sign language.
• Control group -‐ differences of scores between children who used oral communica3on and those who used mixed or sign communica3on mode was posi3ve and sta3s3cally significant (p < 0.05).
• Cochlear implant (G1, G2) group -‐ the difference was in favor of those who used oral communica3on, with sta3s3cal significance for all six sub-‐domains.

HRQL, auditory performance score (CAPr) and speech intelligibility rates (SIR)
• CI group -‐ the two scores, CAPr and SIR, were posi3ve and moderate-‐strongly correlated – CAPr and SIR correlated (acceptable-‐G1 and moderate-‐G2) with dura3on of
cochlear implant use.
• Speech intelligibility and CAPr were posi3ve and sta3s3cally significant correlated with all subdomains of HRQoL for all three groups.
G1 G2 CG
BAP AAP SP BAP AAP SP BAP AAP SP
CAPr 0.538 0.564 0.793 0.769 0.612 0.624
SIR 0.820 0.722 0.597

Results • HRQoL was posi3vely correlated with
auditory performance and speech intelligibility and nega3vely with implanta3on age.
• The correla3on coefficient, R = 0.78 indicates that between the three variables, age at implanta3on, SIR and CAPr scores and quality of life is a very good linear and directly propor3onal correla3on.

Discussions • 85% of children were using the CI all the day – in agreement with other studies – Kersall et all (1995), Summerfield
and Marshall (1995), Hinderink et all (2000) • The quality of life increase as the cochlear implant is used and improves communica3on. The situa3on is even
beier as the child is implanted at a younger age with the opportunity to grow like hearing children. • In both groups were pa3ents who wear hearing aids or cochlear implant intermiient, not all the day long.
– more common in the control group of hearing aided children, some3mes they refuse to wear the device, because of headache, ear fullness or feedback.
– Rarer in cochlear implant groups (in G2) -‐ a small number of children wear the implant only at school or at speech therapy classes (accusing headache)
• Associated diseases were some3mes a cause of delay in the auditory-‐verbal development of children regardless they were implanted or hearing aided and the difference between the two categories was sta3s3cally significant. Although their evolu3on was slower, the cochlear implant had a beneficial effect for them.
Discussion • The communica3on mode is highly dependent on the environment – the family
has the major role in the rehabilita3on process. Some of implanted children were enrolled in special deaf schools and although they carried out intensive auditory training they missed the family environment, a hearing environment, and these children are more likely to use mixed language than children raised at home, in a hearing environment.
• The values obtained for HRQoL domains correlate with auditory percep3on and speech produc3on scores in both hearing aided and implanted children.
• The best performances were achieved by children who used oral communica3on, in both hearing aid group and implanted group. In addi3on, good performances were achieved by those who were using hearing aids or cochlear implant permanent, all day long.

Conclusions • Cochlear implant improves auditory performance and speech produc3on
much beier than hearing aids. • Cochlear implanted children with addi3onal diseases have a slower and
poorer auditory-‐verbal evolu3on but, if we look from the perspec3ve of quality of life, these children enjoy a lot of advantages that cannot be offered by conven3onal hearing aids.
• It is well known that children implanted at a younger age evolve beier than older, but we should consider that even older children can get good results, good performances, if they are well trained and sustained.

References
[1] B.L. Feierman, E.H. Domico, Speech recogni3on in background noise of cochlear implant pa3ents, Otolaryngol. Head Neck Surg. 126 (3) (2002) 257–263. [2] C. Loeffler, A. Aschendorff, T. Burger, S. Kroeger, R. Laszig, S. Arndt, Quality of life measurements aYer cochlear implanta3on, Open Otorhinolaryngol. J. 4 (2010)47–54. [3] D.M. Tait, Video analysis: a method for assessing changes in preverbal and early linguis3c communica3on aYer cochlear implanta3on, Ear Hear. 14(1993) 378–389. [4] M. Tait, M.E. Lutman, Comparison of early communica3ve behavior in young children with cochlear implants and with hearing aids, Ear Hear. 15 (1994) 352–361. [5] Y. Bat-‐Chava, D. Mar3n, J.G. Koswic, Longitudinal improvements in communica3on and socializa3on of deaf children with cochlear implants and hearing aids: evidence from parental reports J. Child
Psychol. Psychiatry 46 (12) (2005) 1287–1296. [6] G.H. Guyai, D.H. Feeney, D.L. Patrick, Measuring health related quality of life, Ann.Intern. Med. 118 (1993) 622–623. [7] R. Fitzpatrick, C. Davey, M.J. Buxton, D.R. Jones, Evalua3ng pa3ent-‐based outcome measures for use in clinical trials, Health Technol. Assess. (Winchester, England) 2 (14) (1998), i–iv, 1–74. [8] W.L. Stone, K.L. Lemanek, Developmental issues in children’s self-‐reports, in: A. La Greca (Ed.), Through the Eyes of the Child: Obtaining Selfreports from Children and Adolescents, Allyn and Bacon,
Boston, 1990. [9] J.B. Hinderink, P.F.M. Krabbe, P. van den Broek, Development and applica3on of a health-‐related quality-‐of-‐life instrument for adults with cochlear implants: The Nijmegen Cochlear Implant
Ques3onnaire, Otolaryngol. Head Neck Surg. 123 (6) (2000) 756–757. [10] T.H. Sach, G.R. Barton, Interpre3ng parental proxy reports of (health-‐related) quality of life for children with unilateral cochlear implants, Int. J. Pediatr. Otorhinolaryngol. 71 (2007) 435–445. [11] J.G. Nicholas, A.E. Geers, Personal, social, and family adjustment in school aged children with a cochlear implant, Ear Hear Suppl. 24 (1) (2003) 692–780. [12] S.B. Waltzman, N.L. Cohen, J. Green, J.T. Roland Jr., Longterm effects of cochlear implants in children, Otolaryngol. Head Neck Surg. 126 (5) (2002) 505–511. [13] E.A.R. Beadle, A.A. Shores, E.J. Wood, Parental percep3ons of the impact upon family of cochlear implanta3on in children, Ann. Otol. Rhinol. Laryngol. 185 (Suppl.) (2000) 105–109. [14] S. Khan, L. Edwards, D. Langdon, The cogni3on and behavior of children with cochlear implants, children with hearing aids and their hearing peers: a comparison, Audiol. Neurootol. 10 (2005) 117–126. [15] P.C. Stacey, H. Fortnum, G.R. Barton, A.Q. Summerfield, Hearing-‐impaired children in the United Kingdom, I: auditory performance, communica3on skills, educa3onal achievements, quality of life, and
cochlear implanta3on, Ear Hear. 27 (2006) 161–186. [16] M.C. Allen, T.P. Nikopoulos, G.M. O’Donoghue, Speech intelligibility in children aYer cochlear implanta3on, Am. J. Otol. 19 (1998) 742–746. [17] E.A. Tobey, A.E. Geers, C. Brenner, D. Altuna, G. Gabbert, Factors associated with development of speech produc3on skills in children implanted by age five, Ear Hear. 24 (Suppl.) (2003) 36S–45S. [18] A.E. Geers, J.G. Nicholas, A.L. Sedey, Language skills of children with early cochlear implanta3on, Ear Hear. 24 (Suppl.) (2003) 46S–58S. [19] Geers A.E. Feb, Predictors of reading skill development in children with early cochlear implanta3on, Ear Hear. 24 (Suppl.) (2003) 59S–68S. [20] A. Sharma, M.F. Dorman, Central auditory development in children with cochlear implants: clinical implica3ons, Adv. Otorhinolaryngol. 64 (2006) 66–88. [21] M. Manrique, F.J. Cervera-‐Paz, A. Huarte, I. Mar3nez, A. Gomez, F. Vazquez de la Iglesia, Hearing and speech in children under 2 years of age with a cochlear implant, An. Sist. Sanit. Navar. 27 (2004)
305–317. [22] N. Loundon, D. Busquet, G. Roger, L. Moav, E.N. Garabedian, Audiophonological results aYer cochlear implanta3on in 40 congenitally deaf pa3ents: preliminary results, Int. J. Pediatr. Otorhinolaryngol.
56 (2000) 9–21. [23] L.S. Kim, S.-‐W. Jeong, Y.-‐M. Lee, J.-‐S. Kim, Cochlear implanta3on in children, Auris Nasus Larynx 37 (2010) 6–17. [24] S.R. Saeed, R.T. Ramsden, P.R. Axon, Cochlear implanta3on in the deaf blind, Am. J. Otol. 19 (1998) 774–777. [25] H.K. El-‐Kashlan, A. Boerst, S.A. Telian, Mul3channel cochlear implanta3on in visually impaired pa3ents, Otol. Neurotol. 22 (2001) 53–56.
