gudesblatt et al, mult scler foster city 2014, 2:1 ournal ... · ournal of multiple sclerosis ......
TRANSCRIPT

Volume 2 • Issue 1 • 1000123J Mult Scler (Foster City)ISSN: 2376-0389 JMSO, an open access journal
Gudesblatt et al,. J Mult Scler (Foster City) 2014, 2:1http://dx.doi.org/10.4172/2376-0389.1000123
Research Article Open Access
Journal of Multiple Sclerosis
Outcomes of a Switch to Fingolimod to Treat Relapsing Multiple Sclerosis: A Patient Subgroup Post Hoc AnalysisMark Gudesblatt1*, Neetu Agashivala2, Simrat Randhawa2, Stan Li3, Luigi Barbato2 and Barry Singer4
1South Shore Neurologic Associates, Patchogue, NY, USA2Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA3Minimax Information Services, Belle Mead, NJ, USA4Missouri Baptist Medical Center, St Louis, MO, USA
AbstractObjective: The EPOC study assessed the effects of switching from an injectable disease-modifying therapy
(glatiramer acetate or one of three interferon beta drugs) to once-daily, oral fingolimod 0.5 mg in patients with relapsing MS. Outcomes were assessed in several patient subgroups at 6 months between patients who switched to fingolimod and those who continued on iDMT.
Methods: Differences in study endpoints between those who switched to fingolimod and those who continued on an iDMT were evaluated by age, gender, baseline Expanded Disability Status Scale score, MS duration, number of relapses in the previous year, previous treatment, previous treatment duration, and reason for switching. The primary endpoint was the change from baseline to month 6 in the Treatment Satisfaction Questionnaire for Medication Global Satisfaction score. Secondary endpoints were changes in scores for the TSQM Effectiveness, Side Effects and Convenience subscales, Beck Depression Inventory-II, Fatigue Severity Scale, Patient-Reported Outcome Indices for Multiple Sclerosis Activities subscale and the 36-item Short-Form Health Survey. Physician-assessed Clinical Global Impressions of Improvement score at 6 months was also recorded.
Results: Switching to fingolimod from iDMT significantly improved scores in all subgroups for TSQM Global Satisfaction at month 6 (all comparisons p≤0.001). Switching to fingolimod significantly improved secondary endpoint scores across all scales for most subgroups (p<0.05) with a few exceptions: switching to fingolimod improved PRIMUS Activities scores only in patients with baseline EDSS scores of greater than 2.5 (p<0.05), and did not improve FSS scores in patients who were male, switched for efficacy reasons, received previous glatiramer acetate, or in whom MS symptom onset had occurred less than 3 years ago. For SF-36 scores, the benefit of switching to fingolimod was highly variable.
Conclusion: Switching to fingolimod from iDMT improved outcomes versus continuing on iDMT, including for overall treatment satisfaction, in patients with MS with wide-ranging baseline characteristics.
*Corresponding author: Mark Gudesblatt, MD, South Shore Neurologic Associates, 77 Medford Avenue, Patchogue, NY 11772, USA, Tel: +1 631 758 1910; Fax: +1 631 758 2371; E-mail: [email protected]
Received July 25, 2014; Accepted October 01, 2014; Published October 05, 2014
Citation: Gudesblatt M, Agashivala N, Randhawa S, Li S, Barbato L, et al. (2014) Outcomes of a Switch to Fingolimod to Treat Relapsing Multiple Sclerosis: A Patient Subgroup Post Hoc Analysis. J Mult Scler (Foster City) 2:123. doi:10.4172/2376-0389.1000123
Copyright: © 2014 Gudesblatt M, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Keywords: Beta interferon; Fingolimod; FTY720; Gilenya; Glatiramer acetate; Relapsing multiple sclerosis; Treatment satisfaction questionnaire for medication
IntroductionSymptoms or adverse events experienced by patients with multiple
sclerosis (MS) can affect their health-related quality of life (QOL) and treatment satisfaction, and can be caused by either the disease itself or the disease-modifying therapy (DMT). As the disease progresses and relapses occur, patients may increasingly experience symptoms such as fatigue and depression [1,2]. A reduction in QOL may occur as a result of one or more treatment-related factors, including dissatisfaction with administration route, the need for frequent administration of therapy, the development of side effects or a perceived lack of treatment efficacy [3-6]. In addition, the relative importance assigned to different treatment outcomes may vary among patients. It is of interest to determine what impact changing therapy may have on the experiences of those who are dissatisfied with their current treatment.
Fingolimod, a sphingosine 1-phosphate receptor modulator, is the first, once-daily, oral therapy approved in the USA and Europe for the treatment of relapsing MS. Its efficacy has been demonstrated in two phase 3 trials, showing superiority to both placebo and intramuscular (IM) interferon (IFN) beta-1a in terms of relapse rate and magnetic resonance imaging (MRI)-based endpoints [7,8]. Although these studies provide robust efficacy data across large patient populations, data on health-related QOL and patient-reported outcomes for fingolimod are limited [9]. To address this, the open-label, randomized, multicenter, phase 4 study, Evaluate Patient Out Comes, Safety and Tolerability of Fingolimod (EPOC; NCT01216072), was conducted.
The EPOC study examined the impact of a switch to fingolimod versus remaining on injectable DMT (iDMT; either glatiramer acetate [GA] or one of three IFN beta drugs). In order to reflect real-world clinical practice, patients did not undergo a washout period before the switch in therapy. The impact of the switch was assessed using a series of patient- and physician-reported outcomes, which included treatment satisfaction, side effects, convenience, fatigue and depression, but the primary analysis did not differentiate according to factors such as patient demographics or previous therapy type [10,11].
Subgroup analyses of phase 3 data have been conducted to establish the efficacy of fingolimod versus placebo and IFN beta-1a according to different patient characteristics, including age, gender and disability status [12,13]. The results of these studies revealed that the positive impact of receiving fingolimod applied across a broad range of patients with relapsing MS; however, the studies did not investigate the impact of treatment on patient-reported outcomes or the effect of a therapy

Volume 2 • Issue 1 • 1000123J Mult Scler (Foster City)ISSN: 2376-0389 JMSO, an open access journal
Citation: Gudesblatt M, Agashivala N, Randhawa S, Li S, Barbato L, et al. (2014) Outcomes of a Switch to Fingolimod to Treat Relapsing Multiple Sclerosis: A Patient Subgroup Post Hoc Analysis. J Mult Scler (Foster City) 2:123. doi:10.4172/2376-0389.1000123
Page 2 of 11
switch in the groups that did not receive fingolimod treatment. To address this gap in the literature, the current post hoc study evaluated several patient subgroups within the EPOC study population to determine whether the efficacy gains were mirrored by improvements in patient- and physician-reported outcomes. The results presented here provide evidence of the impact on patient- and physician-reported outcomes of a switch to fingolimod from iDMT in patients stratified into subgroups according to a range of demographic variables.
MethodsStudy design
The EPOC study was a 6-month, randomized, open-label, multicenter, phase 4 study conducted in the USA and Canada. Patients were randomized 3:1 to switch to fingolimod (FTY720; Gilenya®, Novartis Pharma AG, Basel, Switzerland) or to remain on one of four iDMTs for 6 months, with no washout period. The four iDMTs were subcutaneous (SC) IFN beta-1b (Extavia®, Novartis Pharma AG, Basel, Switzerland, or Betaseron®, Bayer AG, Leverkusen, Germany) 0.25 mg every other day, IM IFN beta-1a (Avonex®, Biogen Idec, Cambridge, MA, USA) 30 μg once weekly, SC IFN beta-1a (Rebif®, Merck Serono, Darmstadt, Germany, and Pfizer Inc., New York City, NY, USA ) 22 or 44 μg three times weekly, or SC GA (Copaxone®, Teva Pharmaceutical Industries Ltd, Petah Tikva, Israel) 20 mg once daily. An institutional review board or independent ethics committee at each study center reviewed and approved the protocol and informed consent form. Written informed consent was provided by each patient.
Patients
Men and women aged 18–65 years with relapsing forms of MS, as defined by the 2005 revised McDonald criteria [14], and an Expanded Disability Status Scale (EDSS) score of 0–5.5 were eligible to participate in the study. Patients were required to have received a single iDMT (other than natalizumab) continuously for 6 months or more before study initiation and to have been candidates for therapy change at the start of the study (as determined by the treating physician). In the case of Canadian patients, only those with the relapsing–remitting form of MS and an inadequate response to, or inability to tolerate, one or more therapies for MS were eligible. Patients were also required to have been naïve to fingolimod treatment.
Individuals were excluded from the study if they had: chronic immune system disease other than MS; immunodeficiency; malignancy other than localized basal cell carcinoma within the past Take over years; a history of cardiac arrest, myocardial infarction, ischemic heart disease or coronary spasm within the past 6 months; Mobitz type II second-degree heart block, third-degree atrioventricular block or an increased corrected QT (QTc) interval (>470 ms); undergone a bone marrow transplant; a or history of alcohol abuse within the past 5 years. Further exclusion criteria were presence of the following at the time of screening: macular edema; active systemic infection; a negative test for Varicella zoster immunoglobulin G antibodies; positive tests for Hepatitis B, Hepatitis C or human immunodeficiency virus; tuberculosis; uncontrolled diabetes; uncontrolled or poorly controlled hypertension or asthma; cardiac failure; severe respiratory disease or pulmonary fibrosis; or chronic liver or biliary disease. Patients were also excluded if they had been treated with any of the following medications: immuno suppressants, immunoglobulins or monoclonal antibodies in the 6 months before screening; any live or live attenuated vaccines in the month before screening; cladribine, cyclophosphamide or mitoxantrone at any time; or class Ia or class III antiarrhythmic drugs at the time of screening.
Study enrollment was completed in October 2011, with a total population of 1053 patients. At randomization, 790 patients were randomized to switch to fingolimod and the remaining 263 patients were randomized to remain on iDMT. Patients who switched from one iDMT to another or who were treated prior to randomization with an iDMT other than one of the four study iDMTs were not included in the analysis. The flow of patients through the study is shown in Figure 1.
Assessments
Assessments were carried out at baseline and 6 months after randomization. The primary post hoc study endpoint for all subgroups was the least-squares mean (LSM) change from baseline in Treatment Satisfaction Questionnaire for Medication (TSQM; v1.4) Global Satisfaction score at 6 months (last observation carried forward [LOCF]) [15]. Higher TSQM scores indicate greater satisfaction.
Secondary patient-reported outcome endpoints were the LSM change from baseline in TSQM Effectiveness, Side Effects and Convenience subscale scores (also employing TSQM v1.4). If a patient’s responses to more than one item were missing from a subscale, then that subscale was not considered to be valid.
Fatigue severity was assessed with the 10-item Fatigue Severity Scale (FSS); higher scores indicate greater fatigue severity [16]. The 21-item Beck Depression Inventory-II (BDI-II) was used to evaluate changes in patient-reported depression; higher scores represent more severe depression [17]. For these instruments, the result was stated as ‘missing’ if more than 20% of the total number of items were unanswered.
The 15-item Patient-Reported Outcome Indices for Multiple Sclerosis (PRIMUS) Activities was used to evaluate changes in activities forming part of daily living; higher scores indicate a greater degree of activity limitation [18].
Health-related QOL was evaluated using the 36-item Short-Form Health Survey (SF-36) v2, which is a self-administered survey assessing eight domains of health [19]. These include physical functioning, role limitations due to physical health, bodily pain, general health perceptions, vitality, social functioning, role limitations due to emotional problems and general mental health. Higher scores indicate a better QOL. For any of the eight domains of SF-36, if more than half of the questions were unanswered, the patient score for that domain was stated as ‘missing’. In addition, two summary subscale scores (the Physical Component Summary [PCS] and the Mental Component Summary [MCS]) can be calculated from the eight individual subscale scores, as well as the overall score. If a patient had not completed one or more of the eight scale scores, the PCS and MCS results for that patient were stated as ‘missing’.
As a further secondary endpoint, a physician-rated assessment, the Clinical Global Impressions of Improvement (CGI-I) scale, provided a global evaluation of clinical change over time at month 6. The scale enables the physician to score the patient’s level of improvement from 1 (very much improved since the initiation of treatment) to 7 (very much worse since the initiation of treatment) [20].
Subgroups
Evaluations of differences in patient- and physician-reported outcomes between patient subgroups were based on the following categories: age ≤ 47 years versus >47 years, male versus female, baseline EDSS score ≤ 2.5 versus >2.5, duration of MS symptoms <3 years versus ≥ 3 years, number of relapses in the previous year 0 versus ≥ 1, previous treatment with IFN beta versus GA, duration of previous treatment ≤ 3.7 years versus >3.7 years and reason for a switch being lack of efficacy

Volume 2 • Issue 1 • 1000123J Mult Scler (Foster City)ISSN: 2376-0389 JMSO, an open access journal
Citation: Gudesblatt M, Agashivala N, Randhawa S, Li S, Barbato L, et al. (2014) Outcomes of a Switch to Fingolimod to Treat Relapsing Multiple Sclerosis: A Patient Subgroup Post Hoc Analysis. J Mult Scler (Foster City) 2:123. doi:10.4172/2376-0389.1000123
Page 3 of 11
Figure 1:Study flow diagram.

Volume 2 • Issue 1 • 1000123J Mult Scler (Foster City)ISSN: 2376-0389 JMSO, an open access journal
Citation: Gudesblatt M, Agashivala N, Randhawa S, Li S, Barbato L, et al. (2014) Outcomes of a Switch to Fingolimod to Treat Relapsing Multiple Sclerosis: A Patient Subgroup Post Hoc Analysis. J Mult Scler (Foster City) 2:123. doi:10.4172/2376-0389.1000123
Page 4 of 11
versus other reasons. Cutoffs between categories were based on the median value for each factor, with the exception of duration of MS symptoms for which the 3-year cutoff point was based on the division between early- and late-stage MS.
Statistical analyses
For the primary endpoint, enrollment of 1000 patients (750 fingolimod and 250 iDMT) would provide 90% power to detect a significant difference between treatment groups in the change from baseline, assuming an effect size of 0.25, a significance level of 5% and a 10% rate of invaluable patients. The primary variable was evaluated by analysis of covariance with baseline TSQM Global Satisfaction score as a covariate and treatment group as a main effect. The LSM, LSM difference between the treatment groups and 95% confidence interval (CI) for the difference between the two treatment groups based on the fitted linear model are reported. Missing data were imputed using the LOCF method. Analyses were conducted using SAS software v9.2 (SAS, Cary, NC, USA).
ResultsPrimary endpoint
A switch to fingolimod was associated with significantly improved outcomes for the primary endpoint of TSQM Global Satisfaction score, relative to remaining on iDMT, in all subgroups (all p ≤ 0.001) (Figure 2).
Secondary endpoints
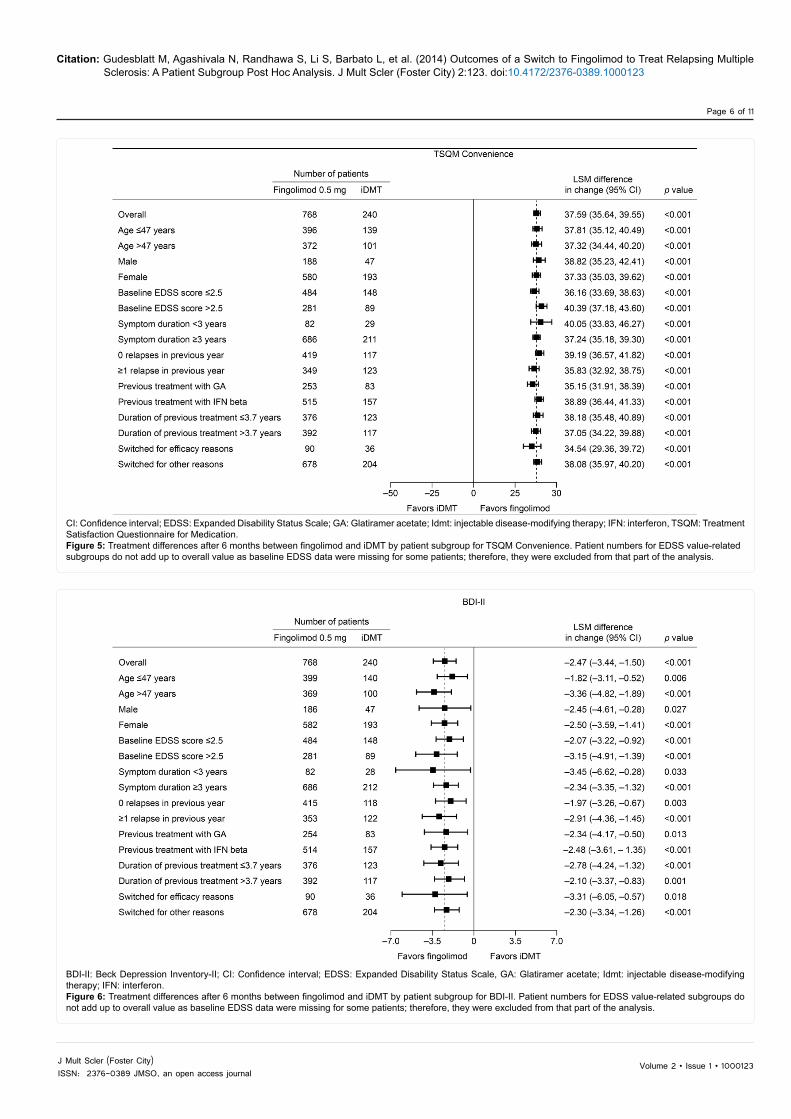
A switch to fingolimod was associated with significantly better outcomes for all subgroups, relative to remaining on iDMT, for TSQM Effectiveness (all p ≤ 0.01), TSQM Side Effects (all p<0.001, except previous treatment with GA [p=0.009]) and TSQM Convenience (all p<0.001) (Figures 3–5).
Superior BDI-II scores were observed following a switch to fingolimod across all subgroups (all p<0.05), relative to remaining on iDMT (Figure 6). For FSS scores, a switch to fingolimod was associated with significantly better outcomes, relative to remaining on iDMT, across several subgroups (all p<0.05) with the exceptions of male gender (p=0.128), duration of symptoms of less than 3 years (p=0.774), previous treatment with GA (p=0.236) and a switch for efficacy reasons (p=0.452) (Figure 7). For PRIMUS Activities, a switch to fingolimod was associated with superior scores, compared with continuing on iDMT, for patients with baseline EDSS scores of more than 2.5 (p<0.05); all other subgroup comparisons showed no significant differences resulting from a switch (Figure 8).
Change in mean score for the MCS of the SF-36 was significantly greater following a switch to fingolimod, compared with continuing on iDMT, for patients who were aged over 47 years, were female, had a baseline EDSS score of more than 2.5, had experienced MS symptoms for 3 years or more, had no relapses in the previous year, had been on their previous treatment for longer than 3.7 years, had previously been treated with IFN beta and had switched for efficacy reasons (all p<0.05);
CI: Confidence Interval; EDSS: Expanded Disability Status Scale; GA: Glatiramer Acetate; Idmt: Injectable Disease-modifying Therapy; IFN: Interferon; TSQM: Treatment Satisfaction Questionnaire for Medication. Figure 2: Treatment differences after 6 months between fingolimod and iDMT by patient subgroup for TSQM Global Satisfaction. Patient numbers for EDSS value-related subgroups do not add up to overall value as baseline EDSS data were missing for some patients; therefore, they were excluded from that part of the analysis.

Volume 2 • Issue 1 • 1000123J Mult Scler (Foster City)ISSN: 2376-0389 JMSO, an open access journal
Citation: Gudesblatt M, Agashivala N, Randhawa S, Li S, Barbato L, et al. (2014) Outcomes of a Switch to Fingolimod to Treat Relapsing Multiple Sclerosis: A Patient Subgroup Post Hoc Analysis. J Mult Scler (Foster City) 2:123. doi:10.4172/2376-0389.1000123
Page 5 of 11
CI: Confidence interval; EDSS: Expanded Disability Status Scale; GA: Glatiramer acetate; Idmt: injectable disease-modifying therapy; IFN: interferon, TSQM: Treatment Satisfaction Questionnaire for Medication.Figure 3:Treatment differences after 6 months between fingolimod and iDMT by patient subgroup for TSQM Effectiveness. Patient numbers for EDSS value-related subgroups do not add up to overall value as baseline EDSS data were missing for some patients; therefore, they were excluded from that part of the analysis.
CI: Confidence interval; EDSS: Expanded Disability Status Scale; GA: Glatiramer acetate; Idmt: injectable disease-modifying therapy; IFN: interferon, TSQM: Treatment Satisfaction Questionnaire for Medication.Figure 4: Treatment differences after 6 months between fingolimod and iDMT by patient subgroup for TSQM Side Effects. Patient numbers for EDSS value-related subgroups do not add up to overall value as baseline EDSS data were missing for some patients; therefore, they were excluded from that part of the analysis.
Volume 2 • Issue 1 • 1000123J Mult Scler (Foster City)ISSN: 2376-0389 JMSO, an open access journal
Citation: Gudesblatt M, Agashivala N, Randhawa S, Li S, Barbato L, et al. (2014) Outcomes of a Switch to Fingolimod to Treat Relapsing Multiple Sclerosis: A Patient Subgroup Post Hoc Analysis. J Mult Scler (Foster City) 2:123. doi:10.4172/2376-0389.1000123
Page 6 of 11
CI: Confidence interval; EDSS: Expanded Disability Status Scale; GA: Glatiramer acetate; Idmt: injectable disease-modifying therapy; IFN: interferon, TSQM: Treatment Satisfaction Questionnaire for Medication.Figure 5: Treatment differences after 6 months between fingolimod and iDMT by patient subgroup for TSQM Convenience. Patient numbers for EDSS value-related subgroups do not add up to overall value as baseline EDSS data were missing for some patients; therefore, they were excluded from that part of the analysis.
BDI-II: Beck Depression Inventory-II; CI: Confidence interval; EDSS: Expanded Disability Status Scale, GA: Glatiramer acetate; Idmt: injectable disease-modifying therapy; IFN: interferon.Figure 6: Treatment differences after 6 months between fingolimod and iDMT by patient subgroup for BDI-II. Patient numbers for EDSS value-related subgroups do not add up to overall value as baseline EDSS data were missing for some patients; therefore, they were excluded from that part of the analysis.

Volume 2 • Issue 1 • 1000123J Mult Scler (Foster City)ISSN: 2376-0389 JMSO, an open access journal
Citation: Gudesblatt M, Agashivala N, Randhawa S, Li S, Barbato L, et al. (2014) Outcomes of a Switch to Fingolimod to Treat Relapsing Multiple Sclerosis: A Patient Subgroup Post Hoc Analysis. J Mult Scler (Foster City) 2:123. doi:10.4172/2376-0389.1000123
Page 7 of 11
CI: Confidence interval; EDSS: Expanded Disability Status Scale; FSS: Fatigue Severity Scale: GA: Glatiramer acetate; Idmt: injectable disease-modifying therapy; IFN: interferon.Figure 7:Treatment differences after 6 months between fingolimod and iDMT by patient subgroup for FSS. Patient numbers for EDSS value-related subgroups do not add up to overall value as baseline EDSS data were missing for some patients; therefore, they were excluded from that part of the analysis.
CI: Confidence Interval, EDSS: Expanded Disability Status Scale, GA: Glatiramer acetate, Idmt: injectable disease-modifying therapy, IFN: interferon, PRIMUS=Patient Reported Outcome Indices for Multiple Sclerosis. Figure 8: Treatment differences after 6 months between fingolimod and iDMT by patient subgroup for PRIMUS Activities. Patient numbers for EDSS value-related subgroups do not add up to overall value as baseline EDSS data were missing for some patients; therefore, they were excluded from that part of the analysis.

Volume 2 • Issue 1 • 1000123J Mult Scler (Foster City)ISSN: 2376-0389 JMSO, an open access journal
Citation: Gudesblatt M, Agashivala N, Randhawa S, Li S, Barbato L, et al. (2014) Outcomes of a Switch to Fingolimod to Treat Relapsing Multiple Sclerosis: A Patient Subgroup Post Hoc Analysis. J Mult Scler (Foster City) 2:123. doi:10.4172/2376-0389.1000123
Page 8 of 11
the remaining subgroups showed no significant differences as a result of a switch (Figure 9).
For the PCS of the SF-36, a switch to fingolimod was associated with significantly better scores than continuing on iDMT in patients who were aged 47 years or younger, were male, had a baseline EDSS score of more than 2.5, had experienced MS symptoms for 3 years or more, had no relapses in the previous year, had been previously treated with IFN beta, had been on their previous treatment for 3.7 years or less and had switched for reasons other than efficacy (all p<0.05); the remaining subgroups showed no significant differences as a result of a switch (Figure 10).
Physician evaluation of overall improvement in patients 6 months after a switch, as measured by mean CGI-I score, significantly favored a switch to fingolimod across all subgroups versus iDMT (all p<0.02) (Figure 11).
DiscussionThis analysis shows that a switch to fingolimod from iDMT
significantly enhances patient- and physician-reported outcomes across a broad patient population when compared with remaining on iDMT, and provides additional detail to the findings reported in the primary analysis [11]. Several of the outcome measures in this study showed improvement across the entire range of patient subgroups following a switch to fingolimod treatment from iDMTs. This finding is consistent with previous results showing that fingolimod is an effective and generally well-tolerated therapy [7,8].
Treatment satisfaction was superior in all patient subgroups assessed following a switch to fingolimod compared with those
continuing on iDMT.Similarly, patient perceptions of effectiveness, side effects and convenience showed significant improvement in all subgroups following a switch from iDMT to fingolimod. Depressive symptoms were reduced significantly in all subgroups of patients who switched to fingolimod, compared with those continuing iDMT.
Patient-reported symptoms of fatigue were also significantly improved as a result of such a switch to fingolimod, relative to remaining on iDMT, in some but not all of the subgroups assessed. Mental and physical health self-evaluation scores were found to be superior in several subgroups who switched to fingolimod, versus remaining on iDMT, with some overlap in the subgroups showing improvement for these measures; results were divergent for other subgroups. This highlights the need to assess both the mental and physical impact of MS. As noted by previous researchers [21], certain commonly used outcome measures (such as the EDSS) are weighted towards physical aspects of the disease, and hence may fail to capture mental or psychological changes that are also of significance to patients.
The results of this study support previous findings that fingolimod improves patient-reported outcomes relative to placebo [9]; however, this is the first subgroup analysis to focus on fingolimod versus an active comparator, and to assess both patient- and physician-reported outcomes. This study also employs a broader range of outcome measures than earlier patient-reported outcomesresearch. In addition, the results presented here complement those of previous efficacy studies, which showed that a switch to fingolimod from iDMT is associated with superior outcomes in terms of relapse rate and MRI endpoints relative to continuing on iDMT [7,8,12,13]. Furthermore, the results reflect a real-world scenario, whereas previous data were from controlled clinical trials.
CI: Confidence interval; EDSS: Expanded Disability Status Scale; GA: glatiramer acetate; iDMT=injectable disease-modifying therapy; IFN: interferon; MCS: Mental Component Summary; SF-36: 36-item Short-Form Health Survey.Figure 9: Treatment differences after 6 months between fingolimod and iDMT by patient subgroup for SF-36 MCS. Patient numbers for EDSS value-related subgroups do not add up to overall value as baseline EDSS data were missing for some patients; therefore, they were excluded from that part of the analysis.

Volume 2 • Issue 1 • 1000123J Mult Scler (Foster City)ISSN: 2376-0389 JMSO, an open access journal
Citation: Gudesblatt M, Agashivala N, Randhawa S, Li S, Barbato L, et al. (2014) Outcomes of a Switch to Fingolimod to Treat Relapsing Multiple Sclerosis: A Patient Subgroup Post Hoc Analysis. J Mult Scler (Foster City) 2:123. doi:10.4172/2376-0389.1000123
Page 9 of 11
CI: Confidence interval; EDSS: Expanded Disability Status Scale; GA: Glatiramer acetate; Idmt: Injectable disease-modifying therapy; IFN: interferon; PCS: Physical Component Summary; SF-36: 36-item Short-Form Health Survey.Figure 10: Treatment differences after 6 months between fingolimod and iDMT by patient subgroup for SF-36 PCS.Patient numbers for EDSS value-related subgroups do not add up to overall value as baseline EDSS data were missing for some patients; therefore, they were excluded from that part of the analysis.
CGI-I: Clinical Global Impression of Improvement; CI: Confidence interval; EDSS: Expanded Disability Status Scale; GA: Glatiramer acetate: Idmt: Injectable disease-modifying therapy, IFN: interferon.Figure 11: Treatment differences after 6 months between fingolimod and iDMT by patient subgroup for CGI-I. Patient numbers for EDSS value-related subgroups do not add up to overall value as baseline EDSS data were missing for some patients; therefore, they were excluded from that part of the analysis.

Volume 2 • Issue 1 • 1000123J Mult Scler (Foster City)ISSN: 2376-0389 JMSO, an open access journal
Citation: Gudesblatt M, Agashivala N, Randhawa S, Li S, Barbato L, et al. (2014) Outcomes of a Switch to Fingolimod to Treat Relapsing Multiple Sclerosis: A Patient Subgroup Post Hoc Analysis. J Mult Scler (Foster City) 2:123. doi:10.4172/2376-0389.1000123
Page 10 of 11
A minority of the comparisons did not demonstrate improvement in patients who switched to fingolimod. These exceptions were restricted to outcomes relating to fatigue, the ability to carry out daily activities, and mental and physical health self-evaluations. It is interesting that the therapy switch had a beneficial effect on fatigue in some patient subgroups but not others. Fatigue and depression have been shown to be correlated in MS, but it seems that this is not the case for all patients, given the positive effect of a switch to fingolimod on depressive symptoms across all subgroups. Other investigators have shown that GA can reduce fatigue [22] and is superior to IFN beta in this respect. Consistent with this, it was found that a switch from GA to fingolimod did not alter self-reported fatigue in the current study, but improvements in fatigue were reported by patients who switched from IFN beta to fingolimod. PRIMUS Activities scores were comparable for fingolimod and iDMTs in almost all subgroups, suggesting that these MS therapies offer similar improvements in the ability to carry out daily tasks. Previous studies have shown strong correlations between fatigue and PRIMUS Activities [23], which is consistent with some subgroups in this analysis showing no improvement in either of these two patient-reported outcomes as a result of switching therapy.
CGI-I scores, which are physician-assessed, showed consistent improvement across subgroups following a switch to fingolimod from iDMTs. CGI-I is reflective of many of the patient-reported outcomesused in this study because it assesses overall patient well-being. This scale contrasts somewhat with traditional physician-assessed measures that often contain a slant towards biomedical or physical factors, such as MRI outcomes or mobility. The CGI-I provides physicians with a method that is consistent with patient self-reported measures, enabling alignment between the two groups’ assessments to increase the likelihood of optimal treatment decisions.
One limitation and bias of this study is that the patients were all candidates for therapy change; the results of this study therefore cannot offer guidance on a therapy switch in patients who are satisfied with their current treatment. Although it would be of interest to assess the effect of a switch to fingolimod in these patients, strong justification would be needed for treatment change if current therapy is deemed satisfactory. Mode of administration may also have impacted on the results; many patients with MS express a dislike of needles or difficulty with injections [3,4]. The use of an open-label study design may also have influenced the results, because the lack of concealment might have led to increased estimates of treatment effects [24]. Finally, it is possible that differences not captured in this study may have impacted on outcomes in some of the subgroups.
It would be interesting to determine whether the effects seen in this trial are similar to those observed after a switch from other MS therapies to fingolimod, especially as studies have recently been completed comparing fingolimod with natalizumab for a series of efficacy endpoints. As yet, there are no comparative data on patient-reported outcomes for these two agents; however, some researchers have reported that natalizumab has a positive impact on fatigue [25,26], including when compared with IFN beta and GA [27].
Overall, the findings of the post hoc analyses suggest that a switch to fingolimod has the potential to enhance treatment outcomes significantly in most patients with MS who are candidates for therapy change from iDMTs. It is highly likely that the improvements seen in the range of secondary outcomes contribute to patients’ increased overall satisfactionwith treatment. The results of this study provide additional support for the use of fingolimod in clinical practice to help improve patient outcomes.
Acknowledgments
All authors made substantial contributions to the conception and design of the study, the acquisition of data, or the analysis and interpretation of data, they were involved in drafting the manuscript and revising it critically for important intellectual content, and had final approval of the version to be published.
Declaration of Funding
Novartis Pharmaceuticals Corporation funded the study and editorial support for the preparation of this manuscript, which was provided by Robert M. Gillies, PhD, and Harriet Crofts, PhD, from Oxford Pharma Genesis™ Ltd.
Conflicts of Interest
M Gudesblatt has received consulting and/or speaking fees from Biogen-Idec, Medtronic, Teva, Genzyme, Novartis, and Sanofi. B Singer has received honoraria for consulting and/or speaking from Acorda Therapeutics, Bayer, Biogen-Idec, EMD Serono, Genzyme, Novartis, Pfizer, and Teva, and has received research support from Acorda Therapeutics, Biogen-Idec, EMD Serono, Genzyme, Roche, and Sanofi. N Agashivala, S Randhawa, and L Barbato are employees and stockholders of Novartis Pharmaceuticals Corporation. S Li is a consultant to Celgene, Novartis, and TechData.
References
1. Chwastiak L, Ehde DM, Gibbons LE, Sullivan M, Bowen JD, et al. (2002) Depressive symptoms and severity of illness in multiple sclerosis: epidemiologic study of a large community sample. Am J Psychiatry 159: 1862-1868.
2. Kale N, Agaoglu J, Tanik O (2010) Neuropsychiatric manifestations in multiple sclerosis: correlation of fatigue and depression with disease progression. Neurol Res 32: 221-223.
3. Cox D, Stone J (2006) Managing self-injection difficulties in patients with relapsing-remitting multiple sclerosis. J Neurosci Nurs 38: 167-171.
4. Lesaux J, Jadbäck G, Harraghy CE (1999) Improving the convenience of home-based interferon beta-1a therapy for multiple sclerosis. J Neurosci Nurs 31: 174-179.
5. Fallowfield L, Atkins L, Catt S, Cox A, Coxon C, et al. (2006) Patients’ preference for administration of endocrine treatments by injection or tablets: results from a study of women with breast cancer. Ann Oncol 17: 205-210.
6. Osborne RH, De Abreu Lourenço R, Dalton A, Houltram J, Dowton D, et al. (2007) Quality of life related to oral versus subcutaneous iron chelation: a time trade-off study. Value Health 10: 451-456.
7. Kappos L, Radue EW, O’Connor P, Polman C, Hohlfeld R, et al. (2010) A placebo-controlled trial of oral fingolimod in relapsing multiple sclerosis. N Engl J Med 362: 387-401.
8. Cohen JA, Barkhof F, Comi G, Hartung HP, Khatri BO, et al. (2010) Oral fingolimod or intramuscular interferon for relapsing multiple sclerosis. N Engl J Med 362: 402-415.
9. Montalban X, Comi G, O’Connor P, Gold S, de Vera A, et al. (2011) Oral fingolimod (FTY720) in relapsing multiple sclerosis: impact on health-related quality of life in a phase II study. MultScler 17: 1341-1350.
10. Cascione M, Wynn D, Barbato LM, Pestreich L, Schofield L, et al. (2013) Randomized, open-label study to evaluate patient-reported outcomes with fingolimod after changing from prior disease-modifying therapy for relapsing multiple sclerosis: EPOC study rationale and design. J Med Econ 16:859-865.
11. Fox E, Edwards K, Burch G, Wynn DR, LaGanke C, et al. (2014) Outcomes of switching directly to oral fingolimod from injectable therapies: results of the randomized, open-label, multicenter, Evaluate Patient Out Comes (EPOC) study in relapsing multiple sclerosis. MultScler Relat Disord.
12. Cohen JA, Barkhof F, Comi G, Izquierdo G, Khatri B, et al. (2013) Fingolimod versus intramuscular interferon in patient subgroups from Transforms. J Neurol 260: 2023-2032.
13. Devonshire V, Havrdova E, Radue EW, O’Connor P, Zhang-Auberson L, et al. (2012) Relapse and disability outcomes in patients with multiple sclerosis treated with fingolimod: subgroup analyses of the double-blind, randomised, placebo-controlled Freedoms study. Lancet Neurol 11: 420-428.
14. Polman CH, Reingold SC, Edan G, Filippi M, Hartung HP, et al. (2005) Diagnostic criteria for multiple sclerosis: 2005 revisions to the “McDonald Criteria”. Ann Neurol 58: 840-846.
15. Atkinson MJ, Sinha A, Hass SL, Colman SS, Kumar RN, et al. (2004) Validation

Volume 2 • Issue 1 • 1000123J Mult Scler (Foster City)ISSN: 2376-0389 JMSO, an open access journal
Citation: Gudesblatt M, Agashivala N, Randhawa S, Li S, Barbato L, et al. (2014) Outcomes of a Switch to Fingolimod to Treat Relapsing Multiple Sclerosis: A Patient Subgroup Post Hoc Analysis. J Mult Scler (Foster City) 2:123. doi:10.4172/2376-0389.1000123
Page 11 of 11
of a general measure of treatment satisfaction, the Treatment Satisfaction Questionnaire for Medication (TSQM), using a national panel study of chronic disease. Health Qual Life Outcomes 2:12.
16. Krupp LB, LaRocca NG, Muir-Nash J, Steinberg AD (1989) The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch Neurol 46: 1121-1123.
17. Beck AT, Steer RA, Brown GK (1996) Manual for the Beck Depression Inventory-II. Psychological Corporation, San Antonio, TX.
18. Doward LC, McKenna SP, Meads DM, Twiss J, Eckert BJ. (2009) The development of patient-reported outcome indices for multiple sclerosis (PRIMUS). MultScler 15:1092-1102.
19. Ware JE, Sherbourne CD (1992) The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 30:473-483.
20. Guy W (1976) ECDEU assessment manual for psychopharmacology. Rockville, MD: US Department of Health, Education, and Welfare Public Health Service Alcohol, Drug Abuse, and Mental Health Administration.
21. Nortvedt MW, Riise T, Myhr KM, Nyland HI (1999) Quality of life in multiple sclerosis: measuring the disease effects more broadly. Neurology 53: 1098-1103.
22. Ziemssen T, Hoffman J, Apfel R, Kern S (2008) Effects of glatiramer acetate on fatigue and days of absence from work in first-time treated relapsing-remitting multiple sclerosis. Health Qual Life Outcomes 6: 67.
23. Twiss J, Doward LC, McKenna SP, Eckert B (2010) Interpreting scores on multiple sclerosis-specific patient reported outcome measures (the PRIMUS and U-FIS). Health Qual Life Outcomes 8: 117.
24. Schulz KF, Chalmers I, Hayes RJ, Altman DG (1995) Empirical evidence of bias. Dimensions of methodological quality associated with estimates of treatment effects in controlled trials. JAMA 273: 408-412.
25. Iaffaldano P, Viterbo RG, Paolicelli D, Lucchese G, Portaccio E, et al. (2012) Impact of natalizumab on cognitive performances and fatigue in relapsing multiple sclerosis: a prospective, open-label, two years observational study. PLoS One 7: e35843.
26. Svenningsson A, Falk E, Celius EG, Fuchs S, Schreiber K, et al. (2013) Natalizumab treatment reduces fatigue in multiple sclerosis. Results from the TYNERGY trial; a study in the real life setting. PLoS One 8: e58643.
27. Yildiz M, Tettenborn B, Putzki N (2011) Multiple sclerosis-associated fatigue during disease-modifying treatment with natalizumab, interferon-beta and glatiramer acetate. Eur Neurol 65:231-232.
Submit your next manuscript and get advantages of OMICS Group submissionsUnique features:
• User friendly/feasible website-translation of your paper to 50 world’s leading languages• Audio Version of published paper• Digital articles to share and explore
Special features:
• 350 Open Access Journals• 30,000 editorial team• 21 days rapid review process• Quality and quick editorial, review and publication processing• Indexing at PubMed (partial), Scopus, EBSCO, Index Copernicus and Google Scholar etc• Sharing Option: Social Networking Enabled• Authors, Reviewers and Editors rewarded with online Scientific Credits• Better discount for your subsequent articles
Submit your manuscript at: http://www.omicsonline.org/submission/
Citation: Gudesblatt M, Agashivala N, Randhawa S, Li S, Barbato L, et al. (2014) Outcomes of a Switch to Fingolimod to Treat Relapsing Multiple Sclerosis: A Patient Subgroup Post Hoc Analysis. J Mult Scler (Foster City) 2:123. doi:10.4172/2376-0389.1000123