steroid dependent/frequently relapsing minimal change disease
TRANSCRIPT

Steroid dependent/frequently Relapsing
Minimal Change disease
Irfana Soomro
9.11.12
CASE 22 y.o chinese male diagnosed with Hepatitis B and minimal change disease in 2009 presented to renal clinic for follow up. Initial presentation in 09: Presented with complaints of bilateral lower extremity swelling, frothy urine, rash on extensor surfaces of his upper extremities, diarrhea for 1 week, diffuse muscle aches and a feeling of his throat being “hot”
PHYSICAL EXAM
Vital signs: T 97.5 BP 144/85 HR 71 RR
HEENT: Sclera anicteric, EOMI
Resp: Clear breath sounds bilaterally
CVS: RRR, normal S1S2
Abd: Soft, mildly tender in the RUQ, non distended, liver edge palpable 2cm below costal margin
Ext: Significant for 3+ pitting edema in upper and lower extremities
Skin: multiple papules and pustules measuring about 1-2 mm in diameter scattered across the extensor surfaces of the arms with few excoriations

LABS ON ADMISSION 2009 BMP: Na 128 K 5.2 Cl 97 HCO3 26 BUN 63 Cr 2.3 Ca 7.6 CPK: 6960 CBC: WBC 7.8 Hgb 15.3 hct 45.2 plt 236 LFTs: AST 151 ALT 108 Alk phos 76 T.bili 0.2 Albumin 2.4 PT/INR 12.2/0.87 PTT 42.2 Lipid panel: HDL 123 Chol 437 TG 449 LDL unable to calculate as UA: blood 3+, protein >300mg/dl, RBC 10-15 WBC 0-2, granular cast 5-10 Uprot/cr 6.4g

LABS…
ASO: 39
C3 85
C4 28.6
ANA negative
Anti dsDNA negative
C-ANCA negative
P-ANCA negative
Hep B s Ag Reactive Hep B s Ab non reactive Hep B e Ag Reactive HepBcAb Ig M non reactive Hep C Ab non reactive HIV non reactive

Patient was started on diuretics while awaiting renal biopsy
Rash was evaluated by dermatology and he was found to have folliculitis not related to systemic disease and treated with topical clindamycin. Improved before discharge

RENAL BIOPSY Minimal Change disease superimposed on IgA
mesangial deposits LM: 18 glomeruli per level, one of which is obsolescent. Capillary walls are normal in thickness and contour and the mesangial areas are normally expanded. Podocytes are markedly hypertrophic but not hyperplastic. Tubulointerstitial compartment is remarkable for very patchy interstitial fibrosis and tubular atrophy involving approximately 5% of the surface area studied IF: IgG and IgM shows 1+ staining in the mesangium. IgA, C3, kappa and lambda light chains positive in the mesangium EM: GBM are normal in thickness and contour. Mesangial areas are normal in cellularity but numerous electron dense depositis are senn in mesangium and paramesangial locations. Podocytes are acutely injured abd reveal extensive effacement foot process effacement. Podocyte effacement involves 100% of the surface area studied

TREATMENT
Patient was started on prednisone 60 mg/day and entecavir for hepatitis B.
He was discharged to follow up in renal clinic after 15 days of hospitalization on prednisone 60 mg qday, lasix 40 mg q day, Entecavir 0.5 mg Q48h
His lower extremity edema had improved and creatinine trended down to 1.5 on the day of discharge

Proteinuria Treatment
Sep-Dec 2009
6.2 gm-127 mg Prednisone 60 mg up until december. Started on taper, decrease by 5mg/week
March 2010 Completed steroid taper
25 March 2010
9.8gm (24 hr)
p/w recurrence of LE swelling started a day after finishing the taper. Restarted on prednisone 60 mg
April- July 2010
4gm-60 mg Prednisone 60mg. Started on taper in july , decrease by 5mg/week
Sep 2010 1.2gm Started on MMF 500 mg bid & continued on prednisone 30 mg qday
Oct 2010 8.9 gm MMF dose increased to 1gm bid, continued on prednisone 30 mg qday
Dec 2010 457 mg Prednisone taper started 20 mg qday. MMF 1gm bid
Jan 2011 3.77g Prednisone increased back to 30 mg qday. MMF 1500 mg bid
Feb 2011 1.13 gm Continued on prednisone 30 mg and MMF 1500 mg bid
March – 2011 Jan 2012
29 mg-102 mg Prednisone slow taper started . MMF 1500 mg bid Prednisone stopped in January
Feb 2012 1.6g Restarted on prednisone 20 mg qay, MMF 1500 mg bid
March 2012 2.18 g MMF stopped. Started on cyclosporine 50 mg q12(but pt took 25 mg q12). Continued on prednisone 20 mg
April 2012 4.7 gm Cyclosporine increased to 75 mg Q12 (T < 50). Prednisone iQ12 ncreased to 60 mg qday
May 2012 40 mg Cyclosporine increased to 100mg Q12 (T <50)Prednisone taper started 50 mg qday for 2 weeks and then 10 mg every 2 weeks until 20 mg is reached
August 2012 108 mg Prednisone decreased to 15 mg qday. Cyclosporine 100mg

• I N C H I L D R E N , M C N S I S T H E M O S T C O M M O N F O R M O F N E P H R O T I C S Y N D R O M E A C C O U N T I N G F O R 9 0 % O F C A S E S I N Y O U N G C H I L D R E N A N D 5 0 % O F C A S E S I N A D O L E S C E N T S
• I N A D U L T S , M C N S I S T H E T H I R D M O S T C O M M O N F O R M O F N S , N E X T T O M E M B R A N O U S N E P H R O P A T H Y A N D F S G S , A C C O U N T I N G F O R 1 0 - 1 5 % O F T H E C A S E S O F T H E A D U L T N S
• M C N S I S M O R E C O M M O N I N H I S P A N I C S , A S I A N S A N D C A U C A S I A N S T H A N I N A F R I C A N A M E R I C A N S
BACKGROUND
PATHOLOGY
Normal appearing glomeruli on light microscopy
Diffuse effacement of foot processes on electron microscopy
Absence of electron dense deposits or thickening of GBM
Negative Immunofluorescence staining
Absence of segmental sclerosis
VARIANTS
Mild mesangial hypercellularity is an infrequent finding (3% to 5%)
Small amounts of mesangial IgG, complement C3, and occasionally IgA may be observed in patients whose clinical course is indistinguishable from classic MCD

PATHOGENESIS
Pathogenesis still not understood very well
At present, it is proposed that MCNS is a disorder of lymphocyte function with increased levels of lymphocyte derived “Permeabilty factor”, which could induce podocyte injury and increased glomerular permeability to plasma proteins.
Following observations support the possibilty that circulating permeability factor may be of immune origin
Induction of albuminuria in rats upon injection of a
factor produced by human T-cell hybridomas derived from a patient with MCD
Two kidneys from a patient with MCD were transplanted into two recipients without significant proteinuria. In both recipients proteinuria was present at the time of grafting but diminished rapidly and was within the normal range within 6 weeks
Koyoma A, Kidney Int 1991 Ali AA Transplantation 1994

ROLE OF IMMUNE SYSTEM IN THE PATHOGENESIS OF NEPHROTIC SYNDROME
T cell dysfunction appears to play a major role. First proposed by Shalhoub in 1974. Following observations are consistent with the hypothesis Association of MCNS with lymphoproliferative disease, in particularly
Hodgkin’s, disease, T-cell lymphoma and thymoma and the induction of remission by removal of the tumor.
Favorable response of nephrotic syndrome to immunosuppressive drugs Atopic individuals are at a high risk for the development of MCD Active measles infection (depresses cell mediated immunity ) can induce
remission Some studies have also implicated interleukin (IL)–13 released from T cells in causing the proteinuria, as T-cell production of IL-13 is elevated and overexpression of IL-13 can induce nephrotic syndrome in rats. Mechanism involved is the induction of CD80 expression on podocytes. Shalhoub RJ, Lancet 1974
Ishimoto T, Semin Nephrol 2011

TH17/TREG IMBALANCE IN ADULT PATIENTS WITH MINIMAL CHANGE NEPHROTIC SYNDROME
Treg and Th17 cells are two new important subsets of T helper cells
Th17/Treg balance controls autoimmunity and inflammation
Treg cells express transcription factor (Foxp3) have an anti-inflammatory role and maintain tolerance to self components through direct contact with cells or by releasing anti-inflammatory cytokines such as Il-10 and TGFB-1
Li-li Liu , Clinical Immunology 2011

Th17 cells express RORᵧt play role in induction of autoimmune tissue injuries and inflammation by producing cytokines such as IL-17, TNF-alpha and IL-6

Li-li Liu , Clinical Immunology 2011

Berre et al reported that a rapid and complete normalization of proteinuria in buffalo/Mna rats, could be achieved by promoting or transferring functional Treg cells.
All these findings suggest T reg cells may be a new target for NS treatment
L.L Berre, J.AM. Soc. Nephrol 2009.

B CELL DYSFUNTION
Few case series have shown rituximab to induce remission in steroid dependent/resistant MCNS suggesting that permeability factor could be produced by B-cells or T cells through pathways regulated or stimulated by B-cells
Yang, Nephrol Dial transplant 2008


ETIOLOGY
Primary or Idiopathic Secondary: MCD is associated with the following Drugs- Gold, NSAIDs, lithium, penicillamine, pamidronate,
probenecid, antimicrobials(ampicillin, rifampin, cefepime)
Neoplasms- Hodgkin disease, Non-Hodgkin lymphoma, leukemia
Allergy – Bee stings, pollen, poison ivy Infections – syphillis, tuberculosis, ehrlichiosis,
echinococcus, mycoplasma

RESPONSE TO THERAPY
Complete remission: reduction of proteinuria to <0.3 g/day
with disappearance of edema and normalization of serum albumin level
Partial remission: >50% reduction of proteinuria with absolute values between 0.3 to 3.5g/day
Relapse: return of proteinuria to approximately >3 g in a patient who had previously undergone complete or partial remission
Frequent relapser: Two relpases within 6 months or 4 or more relapses within a year

RESPONSE…
Steroid dependence: relapse on tapering the steroid therapy or within 4 weeks of discontinuing steroids and need for long term maintenance steroids
Steroid resistance: failure to achieve remission despite at least 16 wks of prednisone

TREATMENT
Treatment for MCD in adults is challenging for several reasons Many patients respond to initial therapy, MCD is believed to
have “benign” course, no controlled treatment trials in adults
Pathogenesis remains unkown
Variability in response patterns and course of the disease

Glucocorticoids are the mainstay of initial therapy leading to complete remission in 80 -97% of adults with MCD
Several reports of adult onset MCNS have shown response rate to corticosteroids in adults was slower compared with that in children; adults with MCNS have been reported to enter remission at rates 37% to 50% within 4 weeks, 51 to 76% within 8 weeks and 76 to 97% within 16 weeks.
Approximately 50 to 75% of glucocorticoid responsive adults will have a relapse and frequent relapse occur in 10-25%. Steroid dependence is seen in 25 to 30%
…

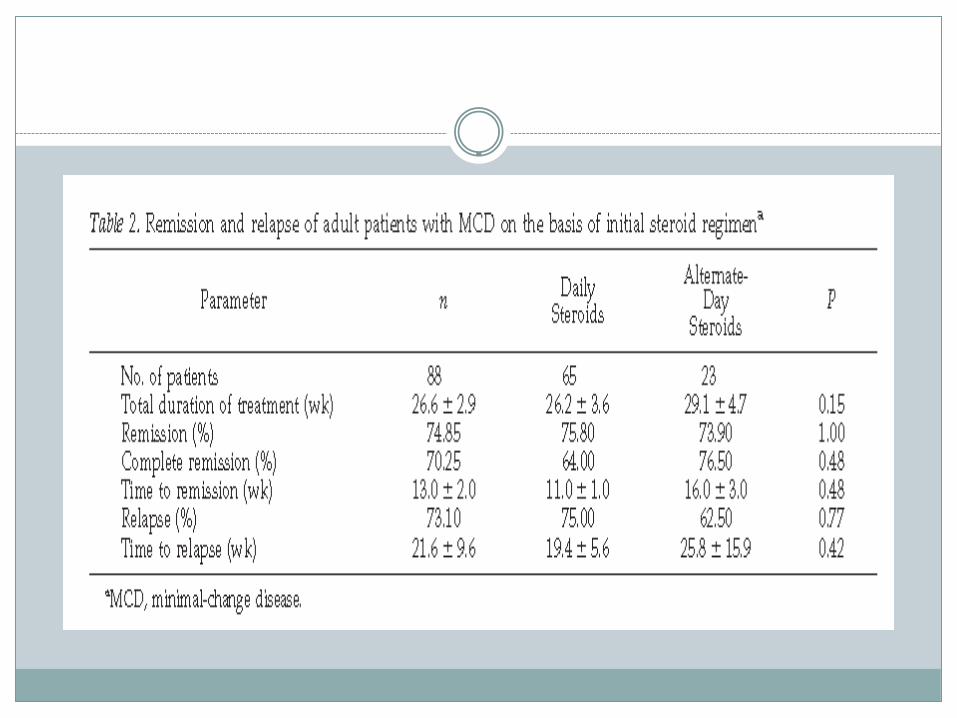

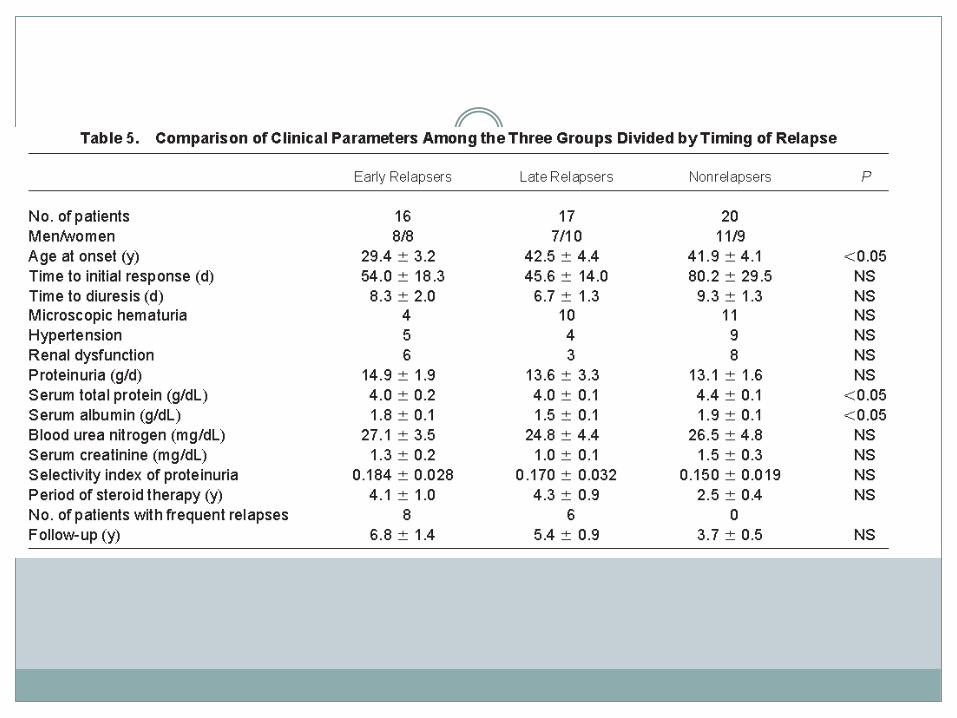
Initial steroid dosage for the daily treatment group was 1mg/kg/day tapered gradually over 26.2 ± 3.6 wk
Initial steroid dosage in the alternate day treatment group was 2mg/kg qod for 6-
8 wk, then decreased by 20 mg at 2 wk intervals until 40 mg qod, followed by a slow taper based on cliniical improvement
28.6% of patients met the criteria for frequent relapsers with a mean of 4.1±0.5
relapses per patient per year.
Frequent relapsers tended to be younger than those who did not relapse frequently (38.6±3.4 vs 46.7 ±1.8 yr, respectively; P=0.043)
27% patients were resistant to initial trial of steroid treatment
Responders tended to have a slightly lower creatinine at presentation compared with non responders, but this was not significant (1.30 vs 1.61 P=0.066)
Waldman, CJN 2007
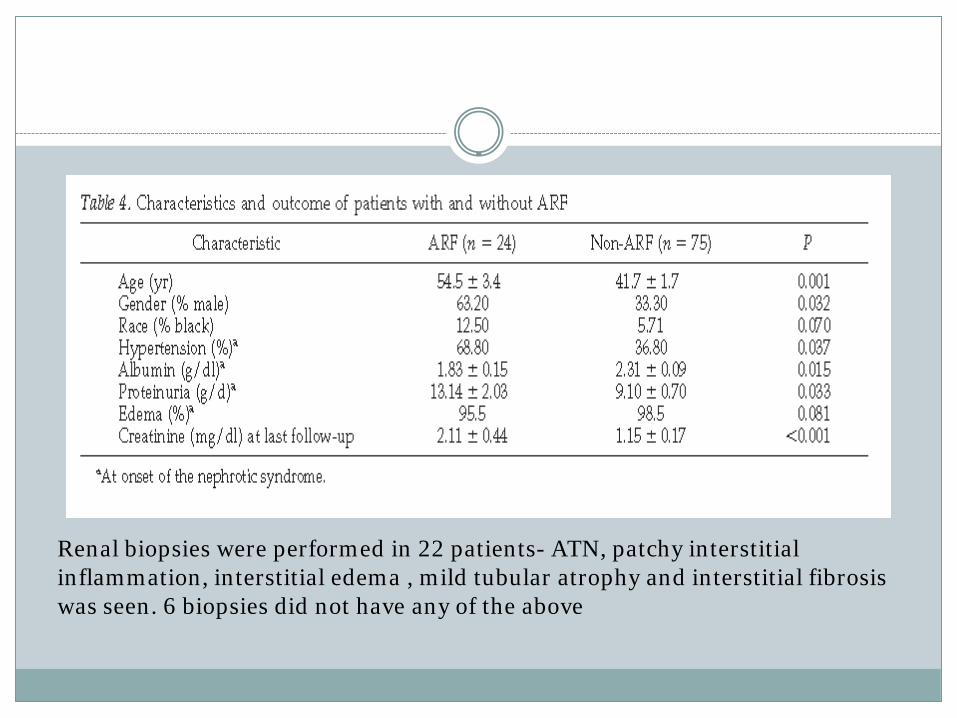
Renal biopsies were performed in 22 patients- ATN, patchy interstitial inflammation, interstitial edema , mild tubular atrophy and interstitial fibrosis was seen. 6 biopsies did not have any of the above
Nakayama, American Journal of kidney disease 2002

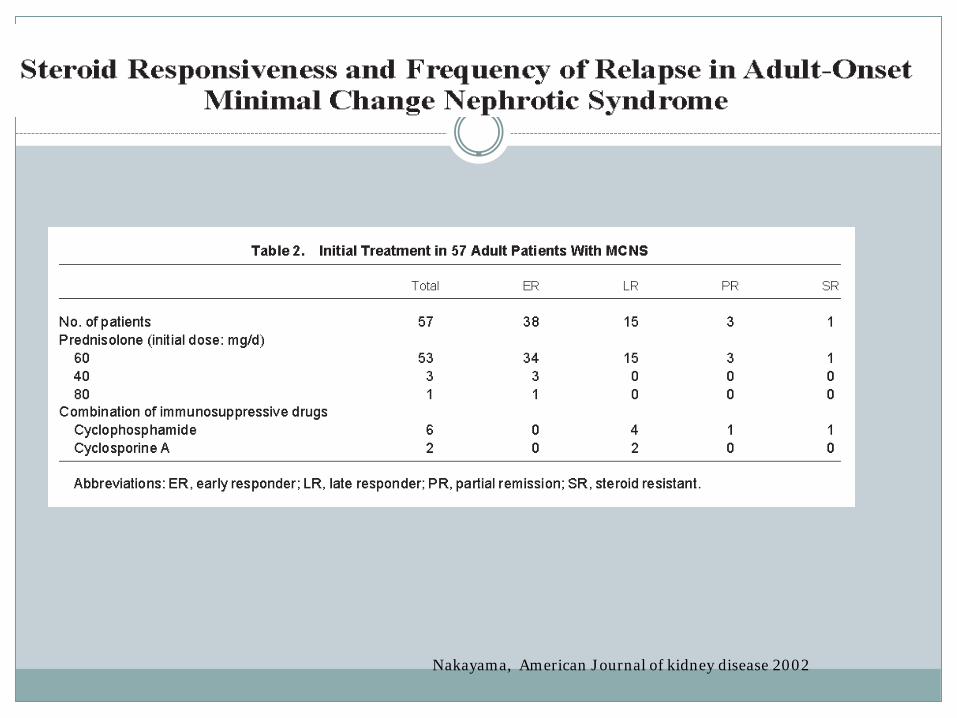
Nakayama, American Journal of kidney disease 2002
TREATMENT OF STEROID DEPENDENT /FREQUENTLY RELAPSING MCD
Continous low dose prednisone
Alkylating agents - cyclophosphamide
Calcineurin Inhibitor -Cyclosporine or tacrolimus
Antimetabolites – azathioprine or mycophenolate mofetil
Levamisole
Rituxan

Waldman, CJN 2007

Mean dosage Duration steroids Mean time to remission
Relapse
Cyclophosphamide 123.6 mg/day 11.5 ± 7.9wk yes 6.4 wk 35%
cyclosporine 220 mg/day 49.5 ± 14.8 wk yes 5 wk 41%
Tacrolimus 2-4 mg bid (T 5-10)
yes
MMF 1-2g/day 36.1 ± 7.9wk yes 20 wk± 2.7 wk
Waldman, CJN 2007

Repeat biopsies were performed in 11 patients because of difficulties with management or because they followed an “atypical course”
6 biopsies revealed a diagnosis that was consistent with FSGS. All these patients had been steroid resistant, 4 were also resistant to both cyclosporine and cyclophosphamide.
Waldman, CJN 2007

Steroid responders were more likely than steroid non responders to be in remission at follow up(62.7% vs 17.4% respectively (P <0.001) and less likely to progress to ESRD compared with non responders
4 patients progressed to ESRD. Time from initial diagnosis of MCD to ESRD ranged from 120 wk to 6 yr. 3 of the patients who progressed to ESRD were black/steroid resistant and found to have FSGS on repeat biopsy

Prospective randomized study
73 patient with idiopathic nephrotic syndrome were randomly assigned to Cyclophosphamide group and CsA group
Cyclophosphamide- 2.5 mg/kg/day for 8 weeks
CsA – 5mg/kg/day in adults, 6mg/kg/day in children
7 patients lost to follow up
Remaining 66 patients were followed up for 3-24 months after randomization
Ponticelli, Nephrology dialysis tranplantation 1993

Ponticelli, Nephrology dialysis tranplantation 1993


At 9 month, 26 of 25 patients assigned to CsA(74%) were
still in remission and 5 (12%) were in partial remission
Of the 28 patients given cyclophosphamide,
18 (64%) were in complete remission and 1 (4%)
were in partial remission
9 patients on CsA had relapses of NS or non nephrotic proteinuria because of intercurrent infections and subsequent reductions on the dose of CsA
After the 9th month when CsA was gradually tapered off, most patients had relapses of NS
Ponticelli, Nephrology dialysis tranplantation 1993

CsA: white columns
Cyclophosamide: Shaded columns
Ponticelli, Nephrology dialysis tranplantation 1993

Open prospective cohort study Tac cohort received oral TAC (target trough blood level
4-8ng/ml) for 24 weeks CYC cohort received IV CYC(750/m2) once every 4 weeks
for 24 weeks CR after the 24 week period was 76.9% in the CYC group
and 90.9% in the TAC group 60% of the CYC patients and the 50% of TAC patients
maintained remission during the follow up period 23.0 + 10.1 months
40% CYC patients and 50% of TAC patients experienced relapses
Li, Nephrology dialysis tranplantation 2002

Li, Nephrology dialysis tranplantation 2002
THANK YOU