gore-tex synthetic ligament
TRANSCRIPT
GORE-TEX SYNTHETIC LIGAMENT
DON JOHNSON, MD
The evolution of the Gore-Tex synthetic knee ligament is described. The original graft, introduced in 1982, was braided and implanted by an open procedure. The initial indication was for failure of autogenous grafts in young athletes. The early results were encouraging, but soon the failure rate was found to be unacceptable. The results were encouraging, but soon the failure rate was found to be unacceptable. The results of the compact diameter graft dramatically improved with more rigid patient selection. At the same time, the technique improved, ie, better notchplasty and tunnel placement. In this series of 202 patients, the failure rate was 5% at 5 years. The effusion rate was minimal because the wrapped intra-articutar portion of the graft. This experience taught us many lessons that may be applicable to the next synthetic graft. KEY WORDS: anterior cruciate ligament, Gore-Tex, reconstruction, synthetic ligament
BACKGROUND
A synthetic replacement ligament was developed by W. L. Gore and associates in the 1970s. This material had previously been shown to have good biocompatibil- ity in vascular grafts. Gore-Tex was also porous, and would allow bony ingrowth. The initial graft was made from a single strand of expanded polytetraflouroethylene that was braided into suitable lengths with eyelets at both ends. The eyelets proved to be the best method of fix- ation (Fig 1).
BIOMECHANICS
The material underwent extensive testing, both mechan- ical and biological. The ultimate tensile strength was 2.8 times the normal anterior cruciate ligament. The cyclical creep tests showed only 3% elongation over 30 million cycles. The bending fatigue tests were also acceptable.
rate. When the graft was implanted in animals into fem- oral intra-articular tunnels they all failed.
CLINICAL TRIALS
Based on these encouraging results, multicenter clinical trials were started in October 1982. The first operations were performed by open arthrotomy, minimal notch- plasty, and an "over the top" position to an extra- articular femoral tunnel. No immobilization was re- quired postoperatively.
When it was noticed that some of the cases were loose early on in follow up, a change in tensioning was pro- posed. The graft was preconditioned by pulling on the distal end of the graft while putting the knee through a range of motion. The tibial screw was tensioned and set at 20 ° of flexion. The 2-year results had 10% effusion and a 12% failure rate. The graft was approved by the Food and Drug Administration (FDA) for limited use in failures of autogenous grafts.
ANIMAL STUDIES
The graft was implanted in 17 goats to test the safety in a biological environment. The main objective was to eval- uate stability and safety over a prolonged period. The graft was found to be safe with no synovial reaction up to 1 year. There was good bone ingrowth around the cir- cumference of the graft in the tunnels. There was no graft failure at I year. It was believed that "the over the top" position into a femoral tunnel decreased the amount of bending of the graft and thus decreased the failure
THE EVOLUTION
The next major change that occurred was the arthroscop- ically aided insertion of the graft. This also allowed a better notchplasty. The tibial tunnel was moved more
From the University of Ottawa, Ottawa, Ontario, Canada. Address reprint requests to Don Johnson, MD, Sports Medicine
Clinic, Carleton University, Ottawa, Ontario, KlS 5B6, Canada. Copyright © 1995 by W. B. Saunders 1060-1872/95/0303-0006505.00/0 Fig 1. The original braided graft.
Operative Techniques in Sports Medicine, Vol 3, No 3 (July), 1995:173-176 173
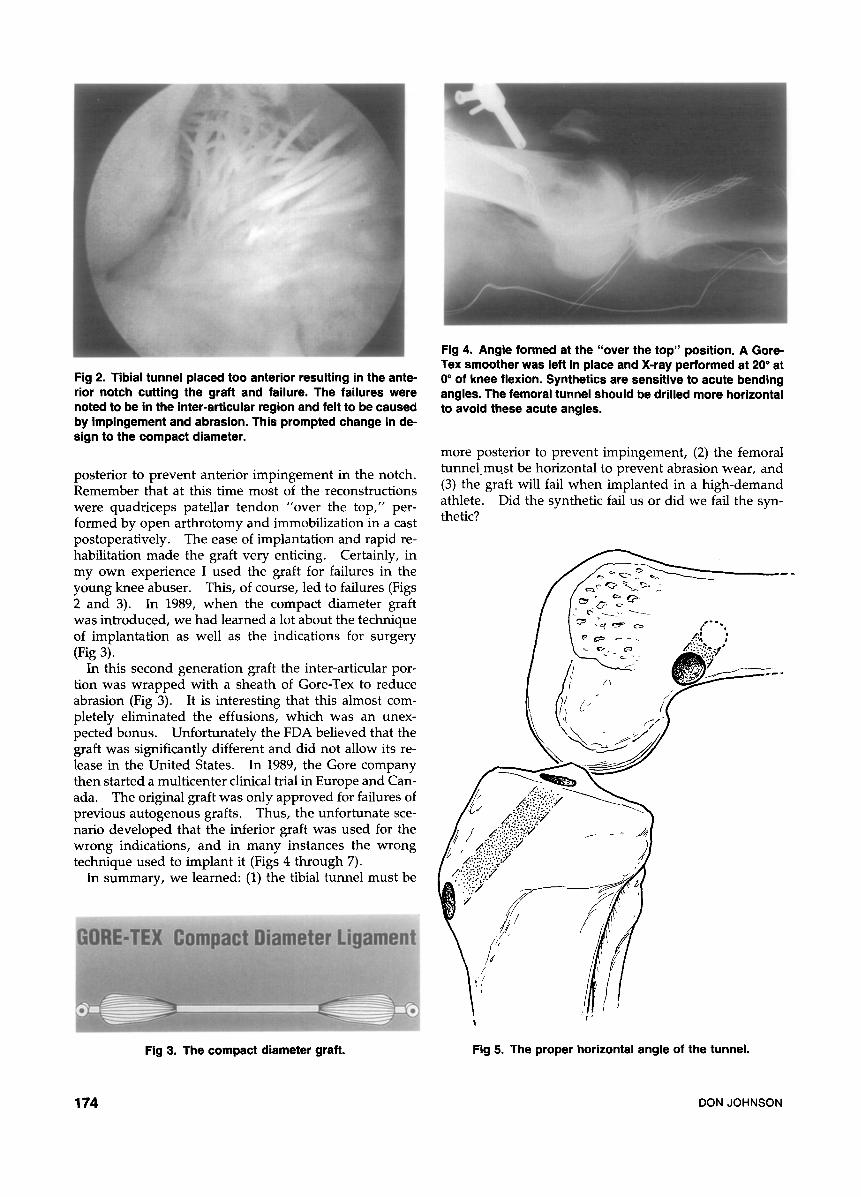
Fig 2. Tibial tunnel placed too anterior resulting in the ante- rior notch cutting the graft and failure. The failures were noted to be in the inter-articular region and felt to be caused by impingement and abrasion. This prompted change in de- sign to the compact diameter,
posterior to prevent anterior impingement in the notch. Remember that at this time most of the reconstructions were quadriceps patellar tendon "over the top," per- formed by open arthrotomy and immobilization in a cast postoperatively. The ease of implantation and rapid re- habilitation made the graft very enticing. Certainly, in my own experience I used the graft for failures in the young knee abuser. This, of course, led to failures (Figs 2 and 3). In 1989, when the compact diameter graft was introduced, we had learned a lot about the technique of implantation as well as the indications for surgery (Fig 3).
In this second generation graft the inter-articular por- tion was wrapped with a sheath of Gore-Tex to reduce abrasion (Fig 3). It is interesting that this almost com- pletely eliminated the effusions, which was an unex- pected bonus. Unfortunately the FDA believed that the graft was significantly different and did not allow its re- lease in the United States. In 1989, the Gore company then started a multicenter clinical trial in Europe and Can- ada. The original graft was only approved for failures of previous autogenous grafts. Thus, the unfortunate sce- nario developed that the inferior graft was used for the wrong indications, and in many instances the wrong technique used to implant it (Figs 4 through 7).
In summary, we learned: (1) the tibial tunnel must be
Fig 3. The compact diameter graft.
Fig 4, Angle formed at the "over the top" position. A Gore- Tex smoother was left in place and X-ray performed at 20 ° at 0 ° of knee flexion. Synthetics are sensitive to acute bending angles. The femoral tunnel should be drilled more horizontal to avoid these acute angles,
more posterior to prevent impingement, (2) the femoral tunnel must be horizontal to prevent abrasion wear, and (3) the graft will fail when implanted in a high-demand athlete. Did the synthetic fail us or did we fail the syn- thetic?
/ I ~ " ~ > ~ ~ , " ' " ,
-'- ~ ; : '~,.
(, 6" / [ ' f
./... '.:7!~.~;:,?~,Y
7!!" U"
i I
Fig 5. The proper horizontal angle of the tunnel.
174 DONJOHNSON

In 1989, I started to implant the compact diameter liga- ment using the above indications.
Fig 6. Late tunnel enlargement. Unknown clinical signifi- cance at present.
PERSONAL EXPERIENCE
In 1986, I started to implant the original Gore-Tex graft for failure of autologous grafts. My initial enthusiasm was tempered by inter-articular failure of the graft. I be- lieved that this material was failing in the high-demand young knee abuser and we should change the patient selection to an older, less active recreational athlete.
RESULTS
I was fortunate to have the above information when I started my second series of Gore-Tex grafts. When I compared my 2-year results of the two grafts, I found the effusion rate was 0 and the failure rate was half (5%). These improved results have continued for 5 years. The reasons are better technique, better patient selection, and a better graft. The patients rated their knee on a visual analog scale from 1 to 10. Eighty-three percent rated their knee a 7 or better. When asked if they would have the operation again the patients responded as fol- lows: 87% said yes; 6% said no; 7% said not sure. It is obvious that most patients are satisfied with the proce- dure. The sports level of the patients is as follows: equal, 38%; same but lower, 26% active in different sports, 21%; significantly limited, 11%; no sports, 4%.
The patients' range of motion postoperatively is as fol- lows: normal, 60%; limited, 40%. Ten patients (5%) failed KT-1000 measurement standards. The failure was defined by positive Lachman, positive pivot shift, KT- 1000 arthrometer measurements greater than 5 mm, and a symptomatic patient who underwent revision. Sev-
A PAIN 79%
I / 60% I
40% f
Pre
B LAC_____HMAN
Post
lOO lOO
8 o
~ 18
Pre Post KT-IO00 S i d e - t o - s i d e d i f f e r e n c e -30 # preoperatively
C'° t 3O 27
~ I 0 9 2 1 S 2O ~ 111 1
1Q
== 0 . . . . .
~ 0 1 2 3 4 5 6 7 S 9 10 >10
Pre
SWELLING GIVING ,WAY
Pre Pos, Pre Post
PIVOT SHIFT
lOO
,oo i U ~ 6 0
40 10
Pre Post 4o KT-IO00 Side-to-side difference -30#
[ postop~atively 30 23 26
20 15 17
0 1 1 1 0 0 -
~ 0 1 2 3 4 5 8 7 ~ 9 10 >10
Post
Fig 7. (A) Subjective results. Comparing the preoperative versus the postoperative. The patients rated their knee on a visual analog scale from I to 10. (B) Objective results, Comparing the Lachman and pivot shift preoperatively and postoperatively,(C) KT-IO00.
GORE-TEX SYNTHETIC LIGAMENT 175

eral patients suffered adverse events. They are listed as follows: infection, 2; synovitis, 1; failures, 10; deep ve- nous thrombophebitis, 2; late femoral fracture, 2; neuro- vascular, 0; and late tunnel enlargement, 7.
Study description. 1. 202 ligaments implanted in 183 patients; 2. Implant dates 2/89 to 5/92 (2 to 5 year follow up); 3. Average age 37 years; 4. 95% follow up (9% by phone, 86% by direct contact); 5. Single center:single surgeon.
CONCLUSIONS
I believe that the bad results that were initially reported were caused by all of the above: poor technique, poor patient selection, and poor graft. In other words, the synthetic graft did not fail us, but we failed the synthetic graft.
The benefit of the faster rehabilitation that the synthetic had in 1986 was lost in 1993 because of the aggressive rehabilitation programs. Therefore, the ideal older rec- reational patient will do well with an arthroscopicaUy im- planted semitendonosis. The need for a synthetic has been greatly reduced.
Another long-term complication of tibial tunnel en- largement has recently been reported. I have seen this on several occasions, but the patient has been asymptom- atic and no treatment was necessary. The problem will obviously show up at the time of revision and may re- quire bone graft to fill the defect.
I have had experience in revising the Gore-Tex to an- other Gore-Tex, to a patellar tendon, to semi-tendonosis, all with very little problem. Despite the improved re- sults, the Gore company has stopped production of the graft as of July 1993.
With the experience of this synthetic I should be well prepared for the next one. I believe that the future holds a better material and we will look back on our experience of harvesting patellar tendon as somewhat barbaric.
176 DONJOHNSON