general approach to the pediatric patient rosen’s chapt. 164 march 29, 2007 martin hellman m.d....
TRANSCRIPT
General Approach to the General Approach to the Pediatric PatientPediatric Patient
Rosen’s Chapt. 164March 29, 2007
Martin Hellman M.D.
Slides byScott Gunderson PGYIII

EpidemiologyEpidemiology
30% of ED visits are pediatrics
Most critically ill patients present to community ED’s not pediatric hospitals
Well established support network for definitive care is essential

EpidemiologyEpidemiology
Fever, Respiratory, & Trauma most common reasons for visits
Trauma is the most common reason for serious morbidity and mortality

PathophysiologyPathophysiology
Anatomic & Physiologic Anatomic & Physiologic DifferencesDifferencesLarge head:body ratio increases head
injuries
Flexible ribs transmit blunt force w/o fractures
Ligaments stronger than physeal plates so fx. more common than sprains

Anatomic & Physiologic Anatomic & Physiologic DifferencesDifferencesSmaller airways more prone to obstruction
Infants often nose breathers and nasal congestion can cause significant distress
Vital SignsVital Signs
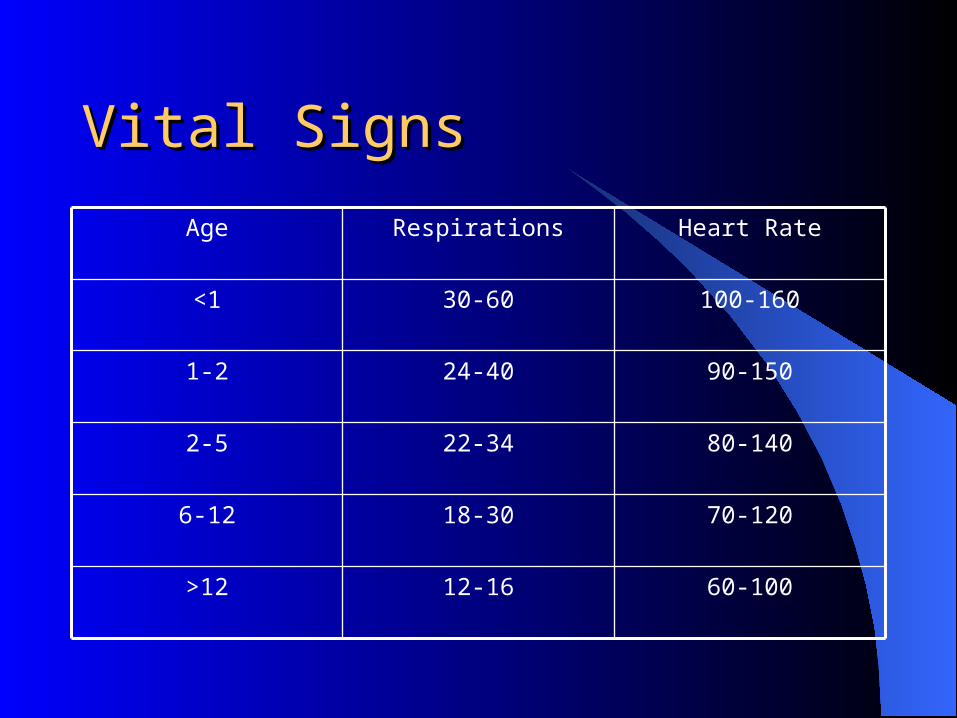
60-10012-16>12
70-12018-306-12
80-14022-342-5
90-15024-401-2
100-16030-60<1
Heart RateRespirationsAge

Vital SignsVital Signs
Tachycardia may be shock, but more commonly d/t fever, anxiety, or fear
Blood pressure difficult to obtain without child cooperation
Lower limit of SBP is 70 + (2 x age)

Vital SignsVital Signs
Respiratory rate– Infants may have apnea up to 20 seconds
normally
– Increased by 5/min per degree (C) fever
Developmental MilestonesDevelopmental Milestones
Neonates– Discomfort is nonspecific– Little interaction
Infants– Social smile, tracts lights – 2-3 months– Stranger anxiety – 6 months

Developmental MilestonesDevelopmental Milestones
Toddlers (13 – 36 months)– Walks alone– Language develops
Preschool (4 – 5 yrs)– Many fantasizes may play a role in irrational
thoughts

Developmental MilestonesDevelopmental Milestones
School Age children (6 – 12 yrs)– Reasoning matures– Explain and include child in conversations
Adolescents (13 – 19 yrs)– Independence and autonomy– Peer pressure– Risk taking behaviors

Initial AssessmentInitial Assessment
Hands-off– Appearance– Work of breathing– Circulation
Gives initial assessment of sick or well

AppearanceAppearance
Interaction with environment– CNS Hypoperfusion
Initially irritableProgress to alternating irritability and lethargyProgress to lethargy and coma

Work of BreathingWork of Breathing
Assess from a distance– Once a cry is started difficult to interpret
– Listen from a distance for audible soundsGrunting - self-induced PEEP to open alveoliStridor - upper airway obstructionMuffled voice - larynx trauma or abscessWheezing - airway narrowing, assess degree
Work of BreathingWork of Breathing
Positioning– Sniffing position - trying to overcome
obstruction– Tripoding - maximizes accessory muscles
Effortless tachypnea– Think compensation of shock and metabolic
acidosis
CirculationCirculation
Visual inspection of perfusion– Pallor - shunting to vital organs in shock– Mottling - worsening shock– Cyanosis - late shock and respiratory failure

Clinical InterviewClinical Interview
Remember and respect parents perception that their child has an emergency
Obtain SAMPLE history involving the child as much as possible

Physical ExaminationPhysical Examination
Not stepwise
Painful or frightening components last (ears)
Examine infants mostly in caretakers lap

TraumaTrauma
Attentions to C-spine precautions– Cervical spine injuries without radiographic
abnormalities (SCIWORA)More common in infants due to elasticityDon’t ignore ridiculer symptoms because
radiographs are negativeUp to 36% of traumatic cervical mylopathies in
children are SCIWORA
ABC’s

Intentional TraumaIntentional TraumaChild abuse
– Usually blunt injuries– Consult child protective services– Look for characteristic bruises
Bruise of different agesHand printsBelt/cord marksLinear marksBitesLocation - neck, groin, thigh, wrists and ankles

SeizuresSeizures
Most benign and self-limited
Assess airway and ventilation– Nasal airways can greatly assist
Look for focal findings
Consider fever, CNS infections, and brain injury
Difficult Airway & ObstructionDifficult Airway & Obstruction
Recognition is key
Mallamptai grades not well studied
Clinical croup score and asthma severity scores are very reproducible
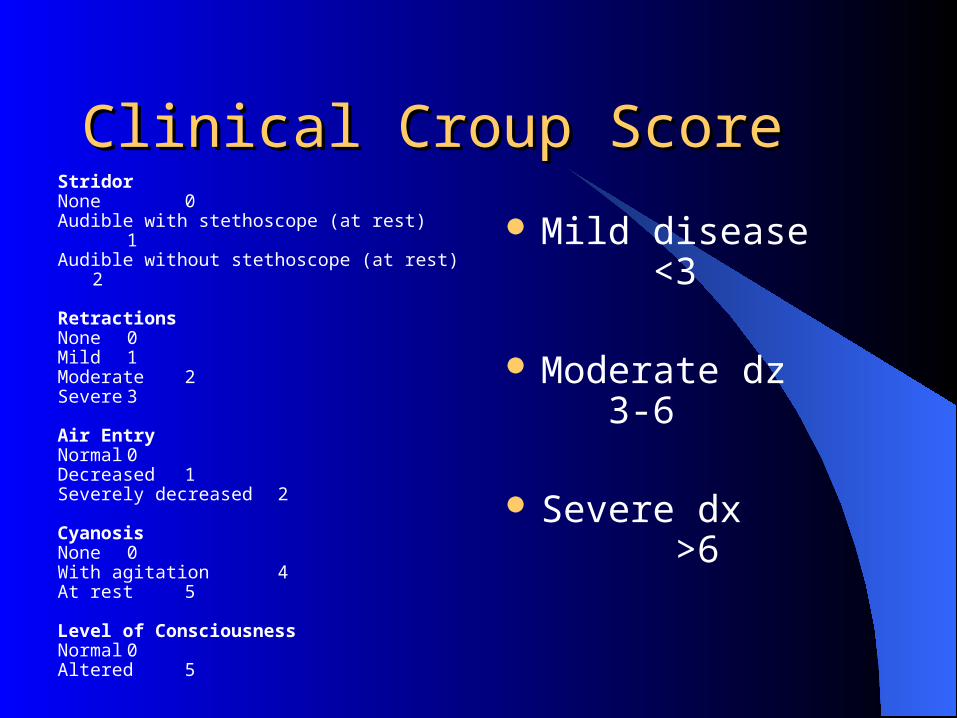
Clinical Croup ScoreClinical Croup ScoreStridor None 0Audible with stethoscope (at rest) 1Audible without stethoscope (at rest) 2
RetractionsNone 0Mild 1Moderate 2Severe 3
Air EntryNormal 0Decreased 1Severely decreased 2
CyanosisNone 0With agitation 4At rest 5
Level of ConsciousnessNormal 0Altered 5
Mild disease <3
Moderate dz 3-6
Severe dx >6
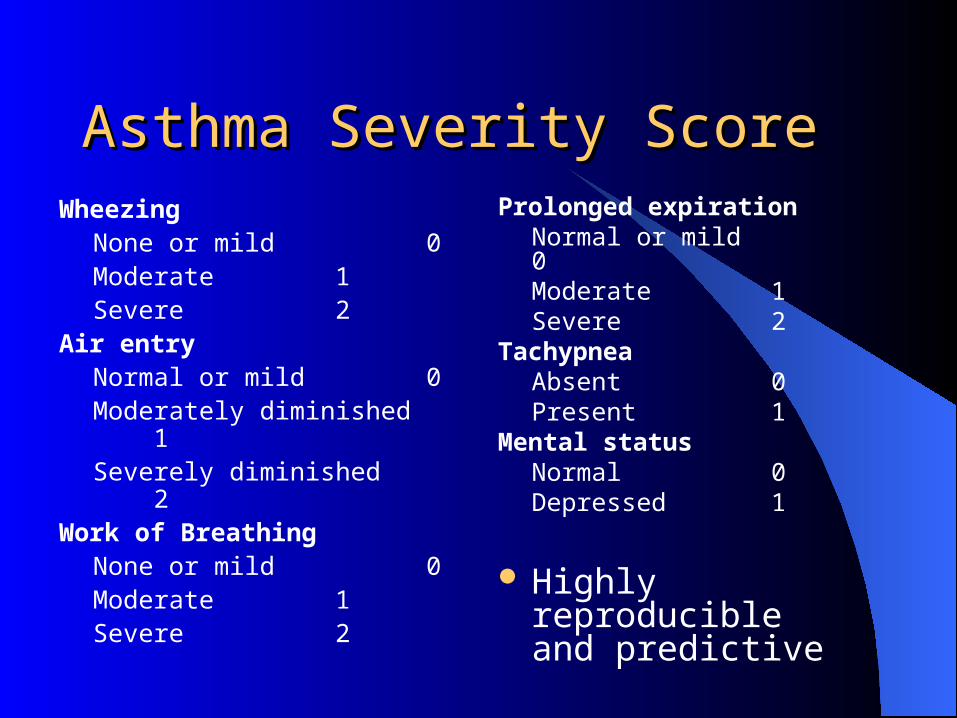
Asthma Severity ScoreAsthma Severity ScoreWheezing
None or mild 0Moderate 1Severe 2
Air entryNormal or mild 0Moderately diminished 1Severely diminished 2
Work of BreathingNone or mild 0Moderate 1Severe 2
Prolonged expirationNormal or mild 0Moderate 1Severe 2
TachypneaAbsent 0Present 1
Mental statusNormal 0Depressed 1
Highly reproducible and predictive
Altered Level of ConsciousnessAltered Level of Consciousness Respirations
– Cheyne-Stokes - increased ICP– Regular tachypnea - midbrain dysfunction
Pupils– Fixed - serious CNS pathology– Unilaterally nonreactive - focal increased ICP
causing uncal compression
Posturing

ShockShock
4 organ approach– Heart - tachycardia occurs first, but can be absent in
last stages
– Skin - shunts blood away Assess where extremities go from cool to warm
– Should move peripherally with resuscitation
– Brain Irritability first then decreased mental status
– Lungs Tachypnea to overcome acidosis

Special NeedsSpecial Needs
Utilize guardian to assess baseline mental function
Behavioral changes can be a V-P shunt malfunction

Noninvasive MonitoringNoninvasive Monitoring
Pulse oximetry– Real-time assessment of respiratory status
End-tidal CO2– Real-time assessment of respirations,
peripheral perfusion, and airway– Helps to avoid repeated blood gas analysis

OMTOMT
OMT in children– There are no specific contraindications for
OMT in children
Otitis media– Numerous studies have shown benefit to OMT
in OM course and reoccurrences
SummarySummary
Understand developmental stages and issues
Remember normal vitals for agesInitial “hands-off” observation is keyBeware of the pale child - early shockSCIWORAAssessment of difficult airways