gastro-esophageal reflux disease: new therapeutic … fismad 24-7ok.pdfgastro-esophageal reflux...
TRANSCRIPT

Gastro-esophageal reflux disease:
new therapeutic aspects
Symposium held in Bologna on March 27, 2015,during the 21st National Congress of Digestive Diseases

© Copyright 2015 by Pacini Editore SpA, Pisa, Italy
Publisher and Graphic Design: Pacini Editore S.p.A., Via Gherardesca 1, 56121 Pisa, Italy
The editor remains at the complete disposal of those with rights whom it was impossible to contact, and for any omissiones.
Photocopies, for personal use, are permitted within the limits of 15% of each publication, following payment to SIAE of the charge due, article 68, paragraphs 4 and 5 of the Law April 22, 1941, No 633. Reproductions for professional or commercial use or for any other purpose other than personal use can be made following a written request and specific authorization in writing from AIDRO, Corso di Porta Romana, 108, 20122 Milan, Italy mail to: [email protected] - www.aidro.org.
Published in July 2015

Cong
ress
Rep
ort
Gastro-esophageal reflux disease: new therapeutic aspectsSymposium held in Bologna on March 27, 2015, during the 21st National Congress of Digestive Diseases
1
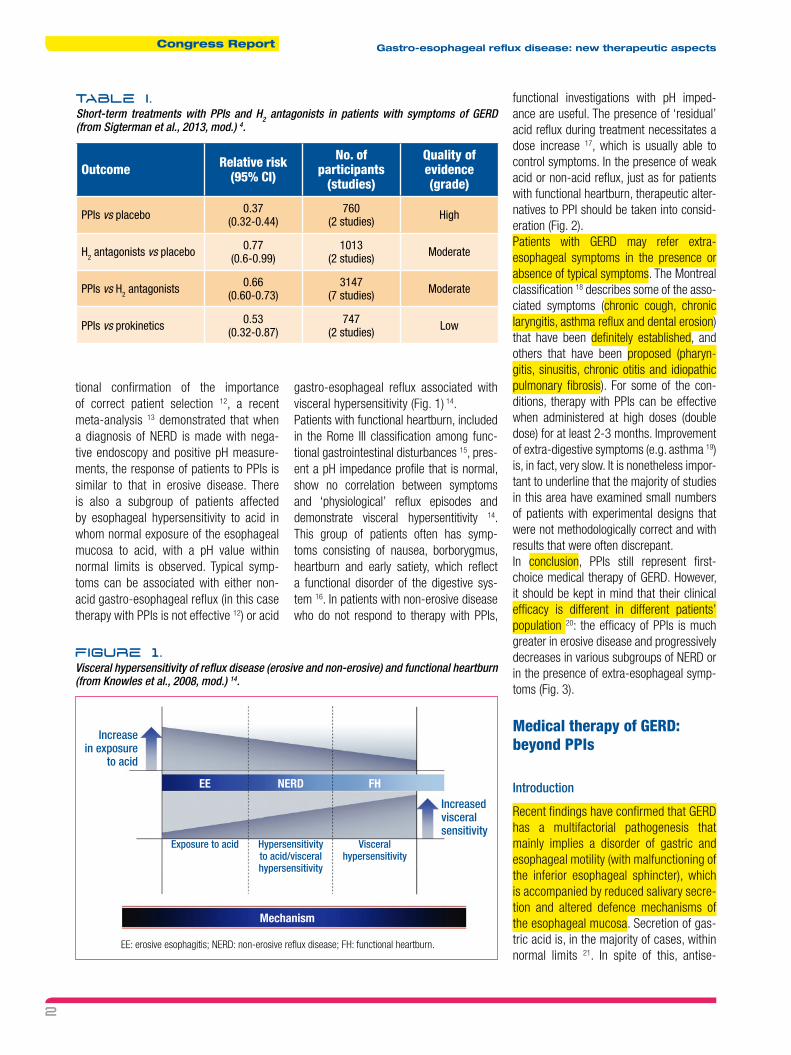
Medical therapy with GERD: the role of PPIs The role of PPIs in the management of GERD is two-fold, namely diagnostic and therapeutic. Presently, in GERD with typical symptoms, an initial treatment with PPIs is of relevance in confirming the “clinical” diagnosis, with good sensitivity and speci-ficity. In management of GERD, PPIs repre-sent the mainstay of medical therapy, just as they are the first-choice in other acid-related pathologies 1. In the 1990s, it was demonstrated that the frequency of symp-toms in GERD is directly correlated with exposure to acid of the distal esophagus 2. Two classes of drugs, aimed to reduce the acid secretion at the gastric level, are nowadays available: H2 receptor antago-nists and PPIs. Both classes of drugs are thereby able to reduce the exposure of the esophageal mucosa to acid. H2 antagonists have a more rapid onset of action than PPIs, which, however, have a longer duration of action 3. PPIs are effec-tive in the resolution of symptoms and the healing of esophageal injuries, and when administered at high or low doses, help maintain patients in long-term remission 3. A recent Cochrane review 4 demonstrated that this class of drugs is more effective in resolving the typical symptoms of GERD than either H2 antagonists or prokinetics (Table I). It is nonetheless important to underline that PPIs reduce the exposure of esophageal mucosa to acid and modify
IntroductionFor many years, gastro-esophageal reflux disease (GERD) was considered to be strictly correlated with the presence of acid reflux, and acid secretory inhibitors were the mainstay of therapy. In recent years, however, several publications and system-atic reviews have highlighted that 20-40% of patients with GERD do not respond (either completely or partially) to proton pump inhibitors (PPIs), thus showing that acid is often not the only pathogenetic fac-tor involved. It is now clear from the medical literature, that the majority of patients with GERD have non-erosive disease, meaning the absence of macroscopic alterations of esophageal mucosa. However, biopsy and histological examination have demonstrat-ed the presence of microscopic esophagitis, which is primarily (but not only) character-ised by altered dilation of intercellular spac-es, which is typical of GERD. In evaluating patients with GERD (especially those who show no benefits from PPIs), it is important to define the type of gastro-esophageal reflux (acid, weak acid, non-acid, liquid, or gaseous) and to identify the presence of microscopic lesions in endoscopically nor-mal mucosa. The therapeutic approach in these ‘difficult’ patients is based on prod-ucts that act on different pathophysiological mechanisms, including those that involve implies the protection of the esophageal mucosa, a therapeutic target that has been largely overlooked.
the composition of the reflux, but do not reduce the total number of gastro-esopha-geal reflux events. Moreover, their efficacy on belching reduction is clearly inferior to that on heartburn resolution, with a thera-peutic gain that is less than 50% 5.By endoscopy, patients with typical symp-toms of GERD may show erosive esophagi-tis (with or without complications, stenosis, or Barrett’s esophagus) or normal mucosa, which is seen more frequently (about 65% of cases). Patients with this latter pheno-type are referred to as being affected with non-erosive reflux disease (NERD). Several systematic reviews 6 7 and meta-analyses 8 9 have documented that the clinical efficacy of PPIs is generally less than 50% in patients with NERD. The reason of this low efficacy is related to the complexity in the definition of NERD patients which can be classified in at least four subgroups with negative endos-copy and reflux symptoms 10. Studies using PH impedance test have allowed for identi-fication of the following populations:• patients with NERD;• patients with an esophagus that is
hypersensitive to acid;• patients with an esophagus that is
hypersensitive to non-acid;• patients with functional heartburn. Obviously, the first two groups of patients (in which acid has a predominant patho-genetic role) adequately respond to PPIs, while there is practically no clinical effi-cacy in the other two groups 11. As addi-
Congress Report Gastro-esophageal reflux disease: new therapeutic aspects
2
tional confirmation of the importance of correct patient selection 12, a recent meta-analysis 13 demonstrated that when a diagnosis of NERD is made with nega-tive endoscopy and positive pH measure-ments, the response of patients to PPIs is similar to that in erosive disease. There is also a subgroup of patients affected by esophageal hypersensitivity to acid in whom normal exposure of the esophageal mucosa to acid, with a pH value within normal limits is observed. Typical symp-toms can be associated with either non-acid gastro-esophageal reflux (in this case therapy with PPIs is not effective 12) or acid
gastro-esophageal reflux associated with visceral hypersensitivity (Fig. 1) 14.Patients with functional heartburn, included in the Rome III classification among func-tional gastrointestinal disturbances 15, pres-ent a pH impedance profile that is normal, show no correlation between symptoms and ‘physiological’ reflux episodes and demonstrate visceral hypersentitivity 14. This group of patients often has symp-toms consisting of nausea, borborygmus, heartburn and early satiety, which reflect a functional disorder of the digestive sys-tem 16. In patients with non-erosive disease who do not respond to therapy with PPIs,
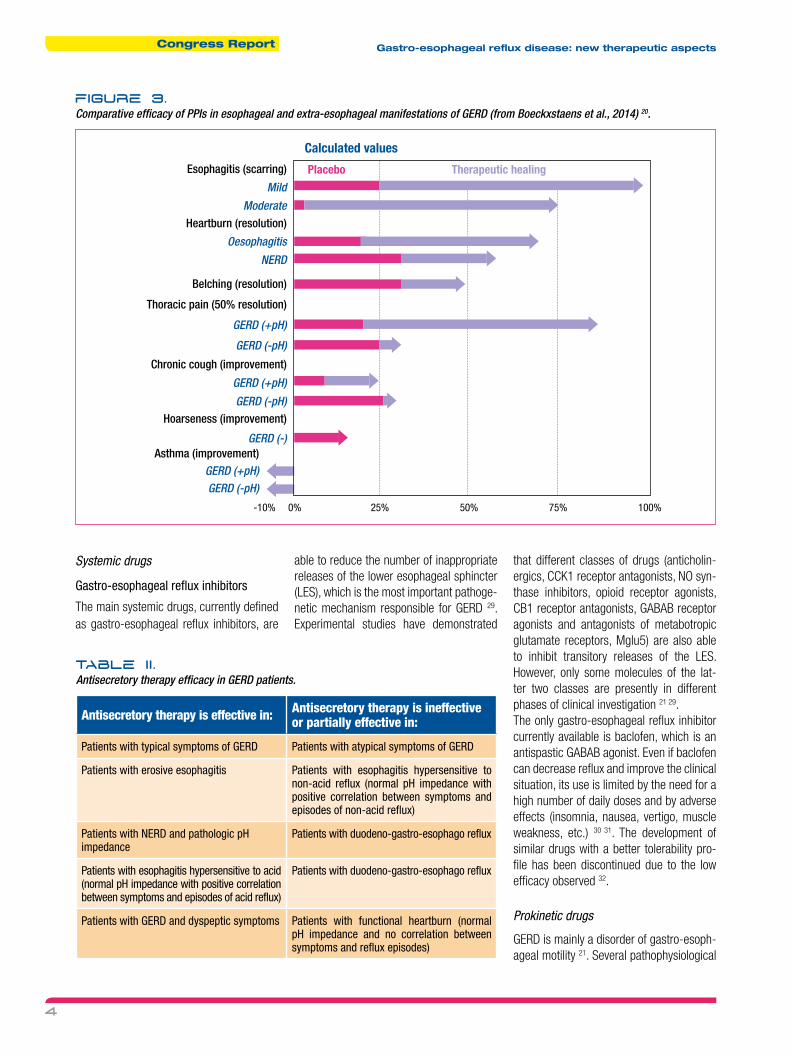
functional investigations with pH imped-ance are useful. The presence of ‘residual’ acid reflux during treatment necessitates a dose increase 17, which is usually able to control symptoms. In the presence of weak acid or non-acid reflux, just as for patients with functional heartburn, therapeutic alter-natives to PPI should be taken into consid-eration (Fig. 2). Patients with GERD may refer extra-esophageal symptoms in the presence or absence of typical symptoms. The Montreal classification 18 describes some of the asso-ciated symptoms (chronic cough, chronic laryngitis, asthma reflux and dental erosion) that have been definitely established, and others that have been proposed (pharyn-gitis, sinusitis, chronic otitis and idiopathic pulmonary fibrosis). For some of the con-ditions, therapy with PPIs can be effective when administered at high doses (double dose) for at least 2-3 months. Improvement of extra-digestive symptoms (e.g. asthma 19) is, in fact, very slow. It is nonetheless impor-tant to underline that the majority of studies in this area have examined small numbers of patients with experimental designs that were not methodologically correct and with results that were often discrepant.In conclusion, PPIs still represent first-choice medical therapy of GERD. However, it should be kept in mind that their clinical efficacy is different in different patients’ population 20: the efficacy of PPIs is much greater in erosive disease and progressively decreases in various subgroups of NERD or in the presence of extra-esophageal symp-toms (Fig. 3).
Medical therapy of GERD: beyond PPIs
Introduction
Recent findings have confirmed that GERD has a multifactorial pathogenesis that mainly implies a disorder of gastric and esophageal motility (with malfunctioning of the inferior esophageal sphincter), which is accompanied by reduced salivary secre-tion and altered defence mechanisms of the esophageal mucosa. Secretion of gas-tric acid is, in the majority of cases, within normal limits 21. In spite of this, antise-
Table I.
Short-term treatments with PPIs and H2 antagonists in patients with symptoms of GERD (from Sigterman et al., 2013, mod.) 4.
Outcome Relative risk(95% CI)
No. of participants
(studies)
Quality of evidence(grade)
PPIs vs placebo 0.37(0.32-0.44)
760(2 studies) High
H2 antagonists vs placebo 0.77(0.6-0.99)
1013(2 studies) Moderate
PPIs vs H2 antagonists 0.66(0.60-0.73)
3147(7 studies) Moderate
PPIs vs prokinetics 0.53(0.32-0.87)
747(2 studies) Low
FIgure 1.
Visceral hypersensitivity of reflux disease (erosive and non-erosive) and functional heartburn (from Knowles et al., 2008, mod.) 14.
EE: erosive esophagitis; NERD: non-erosive reflux disease; FH: functional heartburn.
Increase in exposure
to acid
Increased visceral sensitivity
Exposure to acid Hypersensitivity to acid/visceral hypersensitivity
Mechanism
EE NERD FH
Visceral hypersensitivity

Congress ReportGastro-esophageal reflux disease: new therapeutic aspects
3
cretory drugs (and PPIs in particular) are widely utilised for medical therapy of GERD and can be considered as the first thera-peutic choice with the aim of reducing the lesions caused by acid gastric reflux in the esophagus 22. The clinical efficacy of PPIs 22 23 and the availability of intraluminal pH measure-ments in past years 24 primarily focused attention on the acid component of the reflux. As a consequence, gastro-esopha-geal reflux and acid reflux have become synonymous. However, aberrant sphinc-ter function allows not only acid to reflux in the esophagus, but the entire gastric content including food and bile with vari-able pH. Studies with pH impedance have clearly demonstrated that the reflux can be acid, weakly acid, or non-acid, as well as gaseous or mixed, both before and dur-ing therapy 21. PPIs, which decrease both volume and concentration of gastric juice, can reduce the exposure of the distal esophagus to acid, but do not influence other types of reflux. Considering this,
there is thus the need for additional drugs that can act on GERD through mecha-nisms that are different from inhibition of acid secretion. Moreover, PPIs have an effect on reflux disease that is only pallia-tive as they do not act on the underlying physiological alterations 26. Both literature data and clinical experience suggest that at least 20% of patients with GERD do not respond adequately to therapy with PPIs 27. The clinical efficacy of PPIs, compared to that observed in patients with esopha-geal lesions, is lower in NERD 13 28. The main reason for this is due to the fact that NERD is a heterogeneous group that can be divided into several subgroups; in some of these subgroups, acid reflux does not play a pathogenetic role. In such patients, there is almost no response to PPIs 13 28. The response to PPIs is often suboptimal even in patients with atypical symptoms and extra-esophageal manifestations of GERD 5 and in those with functional heart-burn 13 28 (Table II).
Management of patients with partial response to PPIs
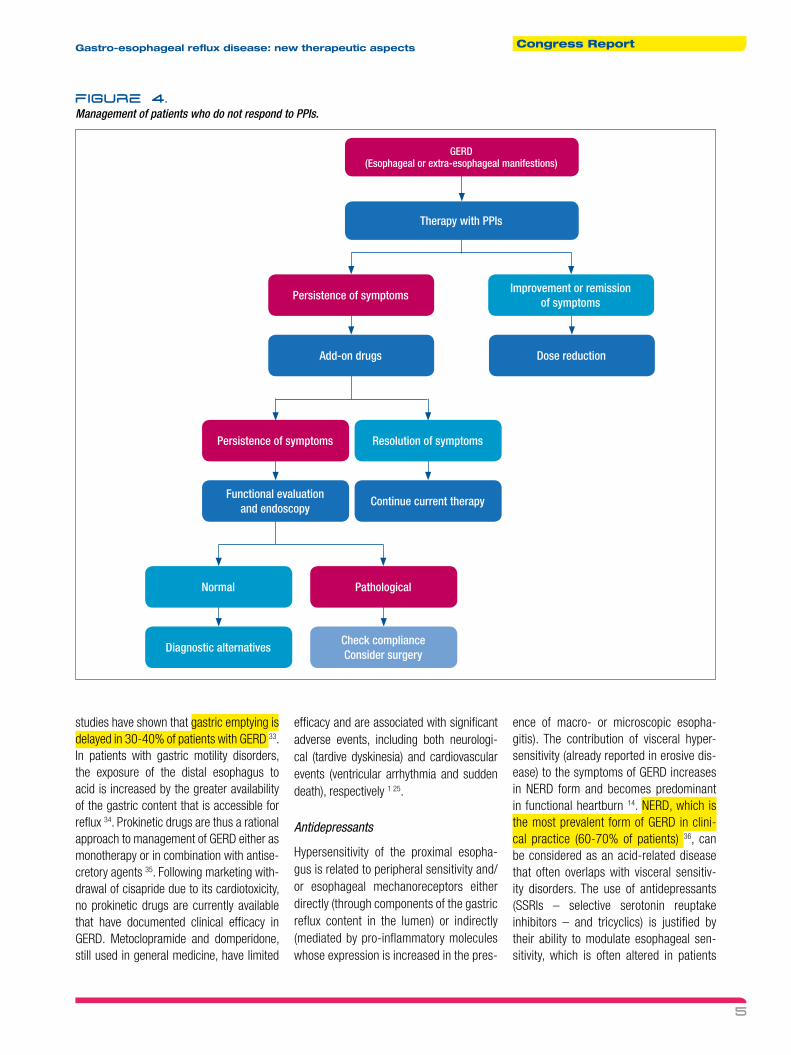
Management of patients with symp-toms (typical or atypical, which do not adequately respond to PPIs) requires a gradual approach, initially based on the use of add-on treatments in addition to antisecretory therapy. In the case of failure, an esophago-gastro-duodenoscopy with biopsy should be performed (even on mac-roscopically normal esophageal mucosa), together with functional exploration using 24-hour pH impedance (Fig. 4). Esophageal manometry and dynamic radiological exam of the esophagus are needed only in the presence of dysphagia or thoracic non-car-diac pain or in planning antireflux surgical intervention.
What drugs in addition to PPIs?
The available pharmacological options include systemic and topical therapies.
FIgure 2.
Therapeutic options in patients with NERD or functional heartburn (from Savarino et al., 2013, mod.) 25.
Non-erosive disease (NERD) Functional heartburn
NERD Esophagus hypersensitive
to acid
Esophagus hypersensitive
to non-acid
Response to PPIs Partial response to PPIs No response to PPIs No response to PPIs
40-45% of patients 15-20% of patients 12-17% of patients 25-30% of patients
Altered esophageal exposure to acid
Normal exposure to acid and positive correlation
between symptoms and episodes of acid reflux
Normal exposure to acid and positive correlation
between symptoms and episodes
of non-acid reflux
Normal esophageal exposure to acid and non-acid and no correlation between symptoms
and reflux episodes
• Single or double dose PPIs
• Inhibitors of TRIOS (baclofen)
• Surgical therapy (fundoplication acc. to Nissen or Toupet)
• Double dose PPIs• Inhibitors of TRIOS
(baclofen)• Surgical therapy
(fundoplication acc. to Nissen or Toupet)
• Double dose PPIs• Inhibitors of TRIOS
(baclofen)• Surgical therapy
(fundoplication acc. to Nissen or Toupet)
• Tricyclic antidepressants (amitriptyline, desipramine, nortriptyline)
• Selective inhibitors of serotonin and noradrenaline uptake (citalopram, escitalopram, fluoxetine, paroxetine, sertraline)
• Reuptake inhibitors of serotonin and noradrenaline (duloxetine, venlafaxine, desvenlafaxine)
NERD: non-erosive reflux disease; TRIOS: transient release inferior esophageal sphincter.
Congress Report Gastro-esophageal reflux disease: new therapeutic aspects
4
FIgure 3.
Comparative efficacy of PPIs in esophageal and extra-esophageal manifestations of GERD (from Boeckxstaens et al., 2014) 20.
Esophagitis (scarring)
Mild
ModerateHeartburn (resolution)
Oesophagitis
NERD
Belching (resolution)
Thoracic pain (50% resolution)
GERD (+pH)
GERD (-pH)
Chronic cough (improvement)
GERD (+pH)
GERD (-pH)Hoarseness (improvement)
GERD (-)Asthma (improvement)
GERD (+pH)GERD (-pH)
Calculated values
-10% 0% 25% 50% 75% 100%
Systemic drugs
Gastro-esophageal reflux inhibitors
The main systemic drugs, currently defined as gastro-esophageal reflux inhibitors, are
able to reduce the number of inappropriate releases of the lower esophageal sphincter (LES), which is the most important pathoge-netic mechanism responsible for GERD 29. Experimental studies have demonstrated
that different classes of drugs (anticholin-ergics, CCK1 receptor antagonists, NO syn-thase inhibitors, opioid receptor agonists, CB1 receptor antagonists, GABAB receptor agonists and antagonists of metabotropic glutamate receptors, Mglu5) are also able to inhibit transitory releases of the LES. However, only some molecules of the lat-ter two classes are presently in different phases of clinical investigation 21 29.The only gastro-esophageal reflux inhibitor currently available is baclofen, which is an antispastic GABAB agonist. Even if baclofen can decrease reflux and improve the clinical situation, its use is limited by the need for a high number of daily doses and by adverse effects (insomnia, nausea, vertigo, muscle weakness, etc.) 30 31. The development of similar drugs with a better tolerability pro-file has been discontinued due to the low efficacy observed 32.
Prokinetic drugs
GERD is mainly a disorder of gastro-esoph-ageal motility 21. Several pathophysiological
Placebo Therapeutic healing
Table II .
Antisecretory therapy efficacy in GERD patients.
Antisecretory therapy is effective in: Antisecretory therapy is ineffective or partially effective in:
Patients with typical symptoms of GERD Patients with atypical symptoms of GERD
Patients with erosive esophagitis Patients with esophagitis hypersensitive to non-acid reflux (normal pH impedance with positive correlation between symptoms and episodes of non-acid reflux)
Patients with NERD and pathologic pH impedance
Patients with duodeno-gastro-esophago reflux
Patients with esophagitis hypersensitive to acid (normal pH impedance with positive correlation between symptoms and episodes of acid reflux)
Patients with duodeno-gastro-esophago reflux
Patients with GERD and dyspeptic symptoms Patients with functional heartburn (normal pH impedance and no correlation between symptoms and reflux episodes)
Congress ReportGastro-esophageal reflux disease: new therapeutic aspects
5
studies have shown that gastric emptying is delayed in 30-40% of patients with GERD 33. In patients with gastric motility disorders, the exposure of the distal esophagus to acid is increased by the greater availability of the gastric content that is accessible for reflux 34. Prokinetic drugs are thus a rational approach to management of GERD either as monotherapy or in combination with antise-cretory agents 35. Following marketing with-drawal of cisapride due to its cardiotoxicity, no prokinetic drugs are currently available that have documented clinical efficacy in GERD. Metoclopramide and domperidone, still used in general medicine, have limited
efficacy and are associated with significant adverse events, including both neurologi-cal (tardive dyskinesia) and cardiovascular events (ventricular arrhythmia and sudden death), respectively 1 25.
Antidepressants
Hypersensitivity of the proximal esopha-gus is related to peripheral sensitivity and/or esophageal mechanoreceptors either directly (through components of the gastric reflux content in the lumen) or indirectly (mediated by pro-inflammatory molecules whose expression is increased in the pres-
ence of macro- or microscopic esopha-gitis). The contribution of visceral hyper-sensitivity (already reported in erosive dis-ease) to the symptoms of GERD increases in NERD form and becomes predominant in functional heartburn 14. NERD, which is the most prevalent form of GERD in clini-cal practice (60-70% of patients) 36, can be considered as an acid-related disease that often overlaps with visceral sensitiv-ity disorders. The use of antidepressants (SSRIs – selective serotonin reuptake inhibitors – and tricyclics) is justified by their ability to modulate esophageal sen-sitivity, which is often altered in patients
FIgure 4.
Management of patients who do not respond to PPIs.
GERD(Esophageal or extra-esophageal manifestions)
Persistence of symptoms
Persistence of symptoms
Add-on drugs
Functional evaluation and endoscopy
Continue current therapy
Dose reduction
Improvement or remission of symptoms
Resolution of symptoms
Normal
Diagnostic alternatives
Pathological
Check complianceConsider surgery
Therapy with PPIs

Congress Report Gastro-esophageal reflux disease: new therapeutic aspects
6
with GERD. Antidepressants can also act on gastrointestinal secretions and motility. In particular, a meta-analysis showed as SSRIs, in contrast to tricyclic agents, are effective in refractory disease 2. Their use, however, is limited by adverse effects that are associated with high rates of treatment discontinuation, which was reported to be 31% in a recent meta-analysis 3.
Topical agents
Alginate-containing formulation
A large number of studies documented the ability of formulations containing algi-nate combined with antacids to generate a mechanical barrier against reflux at the level of the cardias. It should be under-lined, however, that most of these studies were performed with Gaviscon, and that given the different compositions of com-mercial formulations it is not possible to extend these results to other formulations. Scintigraphic studies and magnetic reso-nance with three-dimensional image recon-struction has shown how the alginate raft, floating on the gastric content, is localised at the level of the gastro-esophageal junc-tion below the gaseous bubble 4 37. The abil-ity to reduce the proximal extension of the reflux and exposure of the esophagus to acid, confirmed by 24-hour pH impedance studies 5, is useful in supra-esophageal
manifestations of GERD where the inhibitory activity of alginate on peptic activity is also important. A phenomenon that explains the high efficacy of these preparations and that also clarifies why reflux symptoms are par-ticularly prominent following a meal, when the gastric pH is highest due to the buff-ering effect of food, invokes the so-called post-prandial ‘acid pocket’, or the collection of not buffered acid juice that floats above swallowed food 28 38. Considering its locali-sation at the level of the gastro-esophageal junction, the alginate raft can neutralise the content of the acid pocket or move it away from the gastro-esophageal junction, as documented in a clinical study 39. For these reasons, the addition of alginate-containing formulations to PPIs provides significant benefit in patients with both typical and atypical symptoms.
ESOXX® ONE
Gastro-esophageal reflux is present in all individuals, especially after an abundant meal rich in fats. Indeed, this is a physi-ological phenomenon, generally asymptom-atic, which due to efficient clearance and defence mechanisms of the esophageal mucosa does not cause mucosal damage 40. The integrity of the esophageal mucosa depends on a delicate equilibrium between aggressive factors (acid, pepsin, biliary and pancreatic secretions) and protec-
tive mechanisms (e.g. salivary secretions, secretion of mucus and bicarbonates and the impermeable nature of the mucosa) 41. The resistance of the esophageal mucosa does not depend on any single factor, but rather on several structures and the func-tion of the mucosa that interact in a synergic manner to create an integrated system of defence. Protective mechanisms are gen-erally grouped in three distinct categories: pre-epithelial (salivary secretion, secretion of mucus and bicarbonates), epithelial (cells layering the squamous epithelium that limit the retro-diffusion of H+ ions favouring their neutralisation) and post-epithelial (primarily mucosal blood flow that provides additional bicarbonate for neutralisation in addition to oxygen and nutrients, favouring cellular repair mechanisms) (Fig. 5) 42.Some studies have demonstrated that pre-epithelial defence mechanisms are defec-tive in patients with GERD: both salivary secretion 43 and frequent swallowing 44 are significantly reduced, which leads to a decrease in esophageal clearance. Dilation of intercellular spaces, which is corre-lated to transepithelial resistance, and the reduced basal impedance of the esopha-geal mucosa in patients with reflux disease (erosive and non-erosive), reflects a reduc-tion in epithelial defence mechanisms 45.Despite evidence for reduced mucosal integrity, stimulation of defence mecha-
FIgure 5.
Integrity of esophageal mucosa: an equilibrium between aggressive factors and protective mechanisms.
• HCl
• Pepsin
• Biliary acids
• Trypsin
• Lysolecithin
• HCO3-
• Mucin
• Growth factors
• Prostaglandin
• Mechanisms of selective
permeability
• Carbonic anhydrase
• Mucosal blood flow
• Pre-epithelial• Epithelial• Post-epithelial
Aggressive factors
Protective mechanisms

Congress ReportGastro-esophageal reflux disease: new therapeutic aspects
7
nisms and/or protection of the mucosa, with the exception of the initial attempts with sucralfate 46, have been only rarely considered as a therapeutic target in the treatment of GERD 47. The recent availability of ESOxx® ONE, specifically developed to protect esophageal mucosa, has provided a novel therapeutic approach, which is undoubtedly more appealing from a patho-physiological standpoint than inhibition of acid secretion.ESOxx® ONE, a product developed for pro-tection of the esophageal mucosa, contains two naturally-occurring compounds, hyal-uronic acid (HA) and chondroitin sulphate (CS) distributed in a highly bio-adhesive carrier, poloxamer 407 48, which ensures an extended contact time with the esophageal mucosa following oral ingestion:
• HA has an important role is processes that involve the extracellular matrix (repair of lesions, regeneration, mor-phogenesis), thus favouring healing of mucosal lesions (even microscopic) 49;
• CS has a protective effect on the muco-sa, reducing the damage induced by acid and pepsin present in the gastric content that refluxes in the esophagus 50;
• Poloxamer 407 binds to both compo-nents to generate a macromolecular complex that forms physical barrier against various types of harmful agents (liquid or solid) and fluids (acids, weak acids, alkaline).
The “barrier” effect of ESOxx® ONE has been ex vivo studied in a pig esophagus model perfused with hydrochloric acid solutions (with and without pepsin) 51. The mucosal damage, evaluated by histology, is followed by an increase in permeability, which is observable by an Evans Blue stain-ing of the mucosa that is directly proportion-al to the damage extension. Pre-treatment with ESOxx® ONE completely prevent the alterations in mucosal permeability induced by both types of harmful agents (Fig. 6). The protective effects of ESOxx® ONE per-sisted even after washing the esophageal mucosa before acid-peptic perfusion, thus confirming its elevated adhesion to complex macromolecules and the long-lasting per-sistence of the barrier effect 52.In a pilot study 52 with a cohort of unselected patients with acid-related symptoms (heart-burn, belching, epigastric pain and dyspep-sia), ESOxx® ONE administration was shown to be significantly more effective and faster
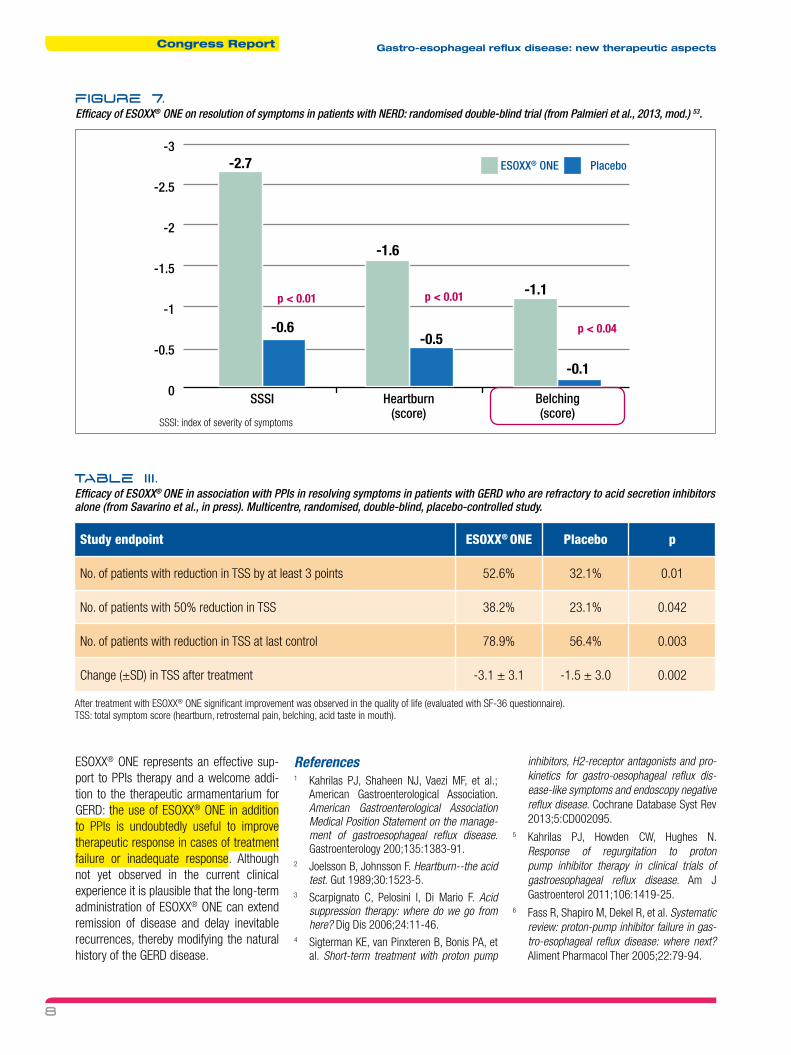
than placebo in improvement of global symp-tom scores. A randomised, double-blind, placebo-controlled trial was later carried out in patients with NERD in which ESOxx® ONE was administered in crossover with placebo for 2 weeks 53. Significant improvement was observed on global symptoms, heartburn and belching (Fig. 7). This latter finding is particularly interesting considering the lim-ited efficacy of PPIs on belching in GERD, which is very difficult to control 5. This data thus support the use of ESOxx® ONE in GERD that was refractory to PPIs, which is unfortunately common in clinical practice 27. The results of this double-blind, placebo-controlled, multicentre study demonstrated that ESOxx® ONE was more significantly effective in the resolution of symptoms than placebo, with a consequent improvement in the quality of life (Table III). In all these stud-ies, the safety profile of ESOxx® ONE was similar to placebo, as expected with a prod-uct with no systemic absorption.
Conclusions
Even if the protective mechanisms of the esophageal mucosa have been identi-fied and studied in detail, they have rarely been considered as therapeutic targets in clinical practice. The recent availability of
FIgure 6.
Permeability of porcine esophageal mucosa after perfusion with Evans Blue and different solutions (from Di Simone et al., 2012, mod. ) 51.
Physiological solution (60 min)
Solution with pepsin at pH 2 (60 min)
Acid solutionat pH 1.5 (90 min)
Solution with pepsin (90 min) + ESOxx® ONE
No damage (no staining)
Severe damage (strong staining)
Moderate damage (weak staining)
No damage (no staining)
Congress Report Gastro-esophageal reflux disease: new therapeutic aspects
8
ESOxx® ONE represents an effective sup-port to PPIs therapy and a welcome addi-tion to the therapeutic armamentarium for GERD: the use of ESOxx® ONE in addition to PPIs is undoubtedly useful to improve therapeutic response in cases of treatment failure or inadequate response. Although not yet observed in the current clinical experience it is plausible that the long-term administration of ESOxx® ONE can extend remission of disease and delay inevitable recurrences, thereby modifying the natural history of the GERD disease.
References1 Kahrilas PJ, Shaheen NJ, Vaezi MF, et al.;
American Gastroenterological Association. American Gastroenterological Association Medical Position Statement on the manage-ment of gastroesophageal reflux disease. Gastroenterology 200;135:1383-91.
2 Joelsson B, Johnsson F. Heartburn--the acid test. Gut 1989;30:1523-5.
3 Scarpignato C, Pelosini I, Di Mario F. Acid suppression therapy: where do we go from here? Dig Dis 2006;24:11-46.
4 Sigterman KE, van Pinxteren B, Bonis PA, et al. Short-term treatment with proton pump
inhibitors, H2-receptor antagonists and pro-kinetics for gastro-oesophageal reflux dis-ease-like symptoms and endoscopy negative reflux disease. Cochrane Database Syst Rev 2013;5:CD002095.
5 Kahrilas PJ, Howden CW, Hughes N. Response of regurgitation to proton pump inhibitor therapy in clinical trials of gastroesophageal reflux disease. Am J Gastroenterol 2011;106:1419-25.
6 Fass R, Shapiro M, Dekel R, et al. Systematic review: proton-pump inhibitor failure in gas-tro-esophageal reflux disease: where next? Aliment Pharmacol Ther 2005;22:79-94.
FIgure 7.
Efficacy of ESOxx® ONE on resolution of symptoms in patients with NERD: randomised double-blind trial (from Palmieri et al., 2013, mod.) 53.
SSSI: index of severity of symptoms
-2.7
-1.6
-1.1
-0.5-0.6
-0.1
p < 0.04
p < 0.01p < 0.01
-3
-2.5
-2
-1.5
-1
-0.5
0SSSI Heartburn
(score)Belching(score)
ESOxx® ONE Placebo
Table II I .
Efficacy of ESOxx® ONE in association with PPIs in resolving symptoms in patients with GERD who are refractory to acid secretion inhibitors alone (from Savarino et al., in press). Multicentre, randomised, double-blind, placebo-controlled study.
Study endpoint ESOxx® ONE Placebo p
No. of patients with reduction in TSS by at least 3 points 52.6% 32.1% 0.01
No. of patients with 50% reduction in TSS 38.2% 23.1% 0.042
No. of patients with reduction in TSS at last control 78.9% 56.4% 0.003
Change (±SD) in TSS after treatment -3.1 ± 3.1 -1.5 ± 3.0 0.002
After treatment with ESOxx® ONE significant improvement was observed in the quality of life (evaluated with SF-36 questionnaire).TSS: total symptom score (heartburn, retrosternal pain, belching, acid taste in mouth).

Congress ReportGastro-esophageal reflux disease: new therapeutic aspects
9
7 Dean BB, Gano AD Jr, Knight K, et al. Effectiveness of proton pump inhibitors in nonerosive reflux disease. Clin Gastroenterol Hepatol 2004;2:656-64.
8 van Pinxteren B, Numans ME, Lau J, et al. Short-term treatment of gastroesopha-geal reflux disease. J Gen Intern Med 2003;18:755-63.
9 van Pinxteren B, Sigterman KE, Bonis P, et al. Short-term treatment with proton pump inhibitors, H2-receptor antagonists and pro-kinetics for gastro-oesophageal reflux dis-ease-like symptoms and endoscopy negative reflux disease. Cochrane Database Syst Rev 2010;(11):CD002095.
10 Savarino E, Zentilin P, Savarino V. NERD: an umbrella term including heterogeneous sub-populations. Nat Rev Gastroenterol Hepatol 2013;10:371-80.
11 Weijenborg PW, Cremonini F, Smout AJ, et al. PPI therapy is equally effective in well-defined non-erosive reflux disease and in reflux esophagitis: a meta-analysis. Neurogastroenterol Motil 2012;24:747-57.
12 Watson RG, Tham TC, Johnston BT, et al. Double blind cross-over placebo controlled study of omeprazole in the treatment of patients with reflux symptoms and physi-ological levels of acid reflux--the “sensitive oesophagus”. Gut 1997;40:587-90.
13 Scarpignato C. Poor effectiveness of proton pump inhibitors in non-erosive reflux disease: the truth in the end! Neurogastroenterol Motil 2012;24:697-704.
14 Knowles CH, Aziz Q. Visceral hypersen-sitivity in non-erosive reflux disease. Gut 2008;57:674-83.
15 Jones R, Galmiche JP. Review: what do we mean by GERD?--definition and diagnosis. Aliment Pharmacol Ther 2005;22:2-10.
16 Savarino E, Pohl D, Zentilin P, et al. Functional heartburn has more in common with func-tional dyspepsia than with non-erosive reflux disease. Gut 2009;58:1185-91.
17 Becker V, Bajbouj M, Waller K, et al. Clinical trial: persistent gastro-oesophageal reflux symptoms despite standard therapy with proton pump inhibitors - a follow-up study of intraluminal-impedance guided therapy. Aliment Pharmacol Ther 2007;26:1355-60.
18 Vakil N, van Zanten SV, Kahrilas P, et al.; Global Consensus Group. The Montreal definition and classification of gastroesoph-ageal reflux disease: a global evidence-based consensus. Am J Gastroenterol 2006;101:1900-20.
19 Chan WW, Chiou E, Obstein KL, et al. The efficacy of proton pump inhibitors for the treatment of asthma in adults: a meta-analy-sis. Arch Intern Med 2011;171:620-9.
20 Boeckxstaens G, El-Serag HB, Smout
AJ, et al. Symptomatic reflux disease: the present, the past and the future. Gut 2014;63:1185-93.
21 Scarpignato C, Savarino V. Novità in tema di fisiopatologia della malattia da reflusso gastro-esofageo. Quale ruolo per gli alginati nell’era degli inibitori della pompa protonica? Ther Perspectives 2011;14:1-37.
22 Savarino V, Di Mario F, Scarpignato C. Proton pump inhibitors in GORD. An overview of their pharmacology, efficacy and safety. Pharmacol Res 2009;59:135-153.
23 Galmiche JP, Letessier E, Scarpignato C. Treatment of gastro-oesophageal reflux dis-ease in adults. Br Med J 1998;316:1720-3.
24 Galmiche JP, Scarpignato C. Esophageal pH monitoring. Front Gastrointest Res 1994;22:71-108.
25 Savarino E, Zentilin P, Savarino V. NERD: an umbrella term including heterogeneous sub-populations. Nat Rev Gastroenterol Hepatol 2013;10:371-80.
26 Contini S, Scarpignato C. Endoscopic treat-ment of gastro-oesophageal reflux disease (GORD): a systematic review. Dig Liver Dis 2003;35:818-38.
27 Bytzer P, van Zanten SV, Mattsson H, et al. Partial symptom-response to proton pump inhibitors in patients with non-erosive reflux disease or reflux oesophagitis - a post hoc analysis of 5796 patients. Aliment Pharmacol Ther 2012;36:635-43.
28 Richter JE, Kahrilas PJ, Johanson J, et al.; Esomeprazole Study Investigators. Efficacy and safety of esomeprazole compared with omeprazole in GERD patients with erosive esophagitis: a randomized controlled trial. Am J Gastroenterol 2001;96:656-65.
29 Bruley des Varannes S, Scarpignato C. Relaxations transitoires du sphincter inférieur de l’oesophage: contrôle pharmacologique et perspectives thérapeutiques. In: Bruley S, des Varannes S, Tack J, editors. Reflux Gastro-oesophagien de l’Adulte. Doin Èditeurs, Rueil-Malmaison 2005, pp. 84-100.
30 Pace F, Pace M. The proton pump inhibitor test and the diagnosis of gastroesophageal reflux disease. Expert Rev Gastroenterol Hepatol 2010;4:423-7.
31 Dent J, Vakil N, Jones R, et al. Accuracy of the diagnosis of GORD by question-naire, physicians and a trial of proton pump inhibitor treatment: the Diamond Study. Gut 2010;59:714-21.
32 Numans ME, Lau J, de Wit NJ, et al. Short-term treatment with proton-pump inhibitors as a test for gastroesophageal reflux disease: a meta-analysis of diagnostic test character-istics. Ann Intern Med 2004;140:518-27.
33 Scarpignato C. Gastric emptying in gas-troesophageal reflux disease and other
functional esophageal disorders. Front Gastrointest Res 1994;22:223-59.
34 Scarpignato C, Franzé A. Esophageal expo-sure to acid in GERD patients with and without delayed gastric emptying. Effect of cisapride. Hepato-Gastroenterology 1992;39:91-2.
35 Heading RC, Baldi F, Holloway RH, et al. Prokinetics in the treatment of gas-tro-oesophageal reflux disease. Eur J Gastroenterol Hepatol 1998;10:87-93.
36 Sharma P, Schmelzle K, McElhinney C, et al. Non erosive reflux disease: prevalence, epidemiology and associated features. Gastroenterology 2000;122(4 Suppl 1):A-584.
37 Vela MF, Camacho-Lobato L, Srinivasan R, et al. Simultaneous intraesophageal impedance and pH measurement of acid and nonacid gastroesophageal reflux: effect of omepra-zole. Gastroenterology 2001;120:1599-606.
38 Edwards SJ, Lind T, Lundell L, et al. Systematic review: standard- and double-dose proton pump inhibitors for the heal-ing of severe erosive oesophagitis -- a mixed treatment comparison of randomized controlled trials. Aliment Pharmacol Ther 2009;30:547-56.
39 Moayyedi P, Santana J, Khan M, et al. Medical treatments in the short term management of reflux oesophagitis. Cochrane Database Syst Rev 2011;(2):CD003244.
40 Kahrilas PJ. GERD pathogenesis, pathophysi-ology, and clinical manifestations. Cleve Clin J Med 2003;70(Suppl 5):S4-19.
41 Orlando RC. The integrity of the esophageal mucosa. Balance between offensive and defensive mechanisms. Best Pract Res Clin Gastroenterol 2010;24:873-82.
42 Orlando RC. Review article: oesophageal mucosal resistance. Aliment Pharmacol Ther 1998;12:191-7.
43 Campisi G, Lo Russo L, Di Liberto C, et al. Saliva variations in gastro-oesophageal reflux disease. J Dent 2008;36:268-71.
44 Bremner RM, Hoeft SF, Costantini M, et al. Pharyngeal swallowing. The major factor in clearance of esophageal reflux episodes. Ann Surg 1993;218:364-9.
45 Farré R. Pathophysiology of gastro-esophageal reflux disease: a role for mucosa integrity? Neurogastroenterol Motil 2013;25:783-99.
46 Scarpignato C. Sucralfate and other muco-sal protective compounds: pharmacol-ogy and potential in the treatment of esophageal lesions. Front Gastrointest Res 1992;20:317-46.
47 Woodland P, Sifrim D. Oesophageal mucosal barrier: a key factor in the pathophysiol-ogy of non-erosive reflux disease (NERD) and a potential target for treatment. Gut 2014;63:705-6.

Congress Report Gastro-esophageal reflux disease: new therapeutic aspects
10
48 Dumortier G, Grossiord JL, Agnely F, et al. A review of poloxamer 407 pharmaceutical and pharmacological characteristics. Pharm Res 2006;23:2709-2728.
49 Voigt J, Driver VR. Hyaluronic acid derivatives and their healing effect on burns, epithe-lial surgical wounds, and chronic wounds: a systematic review and meta-analysis of randomized controlled trials. Wound Repair Regen 2012;20:317-331.
50 Levey S, Sheinfeld S. The inhibition of the proteolytic action of pepsin by sulfate-con-taining polysaccharides. Gastroenterology 1954;27:625-628.
51 Di Simone MP, Baldi F, Vasina V, et al. Barrier effect of Esoxx® on esophageal mucosal damage: experimental study on ex-vivo swine model. Clin Exp Gastroenterol 2012;5:103-7.
52 Palmieri B, Corbascio D, Capone S, et
al. Preliminary clinical experience with a new natural compound in the treatment of oesophagitis and gastritis: symptomatic effect. Trends Med 2009;9:219-25.
53 Palmieri B, Merighi A, Corbascio D, et al. Fixed combination of hyaluronic acid and chondroi-tin-sulphate oral formulation in a randomized double blind, placebo controlled study for the treatment of symptoms in patients with non-erosive gastroesophageal reflux. Eur Rev Med Pharmacol Sci 2013;17:3272-8.

Gastro-esophageal reflux disease:
new therapeutic aspects
Symposium held in Bologna on March 27, 2015,during the 21st National Congress of Digestive Diseases