gastro esophageal reflux disease (gerd)
TRANSCRIPT

Abdelrahman Alkilani, RN, BSN
Gastro-Esophageal Reflux Disease
Overview
Anatomy and physiology Definition of GERD Phathophysiology Clinical manifistations Diagnostic tests Medical management Nursing management

Anatomy and physiology
Esophagus Mucus-lined, muscular tube that carries food from the
mouth to stomach. Begins at the base of the pharynx and ends about
4cm below the diaphragm. Its ability to transport food and fluid is facilitated by
the upper esophageal sphincter (hypophrengeal) and the lower esophageal sphincter (gastroesophageal).
There is no serosal layer of the esophagus.

GERD
Some degree of esophageal reflux (back-flow of gastric and dudenal contents into the esophagus) is normal in both adults and children.
GERD is the excessive reflux.
Pathophysiology
Normally, Lower Esophageal Sphincter (LES) creates enough pressure around the lower end of the esophagus to close it. So, gastric content don’t back up into the esophagus.
Reflux occurs when LES pressure is deficient or the pressure of the stomach exceed LES pressure
When this happens, the LSE relaxes.
Pathophysiology
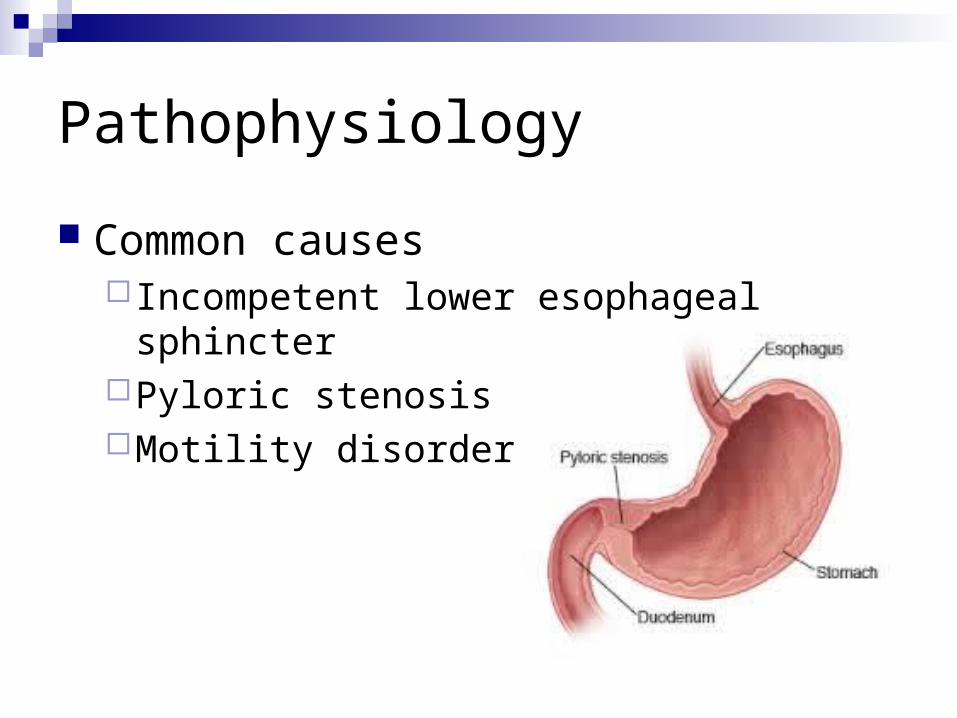
Common causes Incompetent lower esophageal sphincterPyloric stenosisMotility disorder
Pathophysiology
The acidity of gastric content and amount of time in contact with esophageal mucosa are related to the degree of mucosal damage.
Esophageal ulcer and esophagitis may result

Clinical Manifestations
Pyrosis (Burning sensation in the esophagus). Dyspepsia (indigestion). Regurgitation. Dysphagia or odynophagia (pain on swallowing) Hypersalivation. Esophagitis.

Assessment and Diagnostic findings Endoscopy

Assessment and Diagnostic findings Barium swallow
To evaluate the damageto the esophgeal mucosa.

Assessment and Diagnostic findings Ambulatory 12- to 36-hour
esophageal pH monitoring to evaluate the degree of acid reflux
Assessment and Diagnostic findings Bilirubin monitoring (bilitec)
To measure bile reflux patterns

Medical Management
Health EducationDiet
Low fat diet Avoid caffeine, tobacco, beer, milk, foods
containing peppermint or spearmint, and carbonated beverage.
Avoid eating or drinking 2 hours before bed time.

Medical Management
Health EducationMaintain body weight.Avoid tight-fitting clothes.Elevate the head of the bed on 15-20cm
blocks.Elevate the upper body on pillow.

Medical Management
MedicationsAntacids or H2 receptor antagonist.
famotidine, nizatidine, or rantidineProton pump inhibitors
Lanzoprazole, esomeprazole, or rabeprazole.Prokinetic agents
Bethanecol, dompridone, and meetoclopramide.

Medical Management
Surgical interventionNissen fundoplication(wrapping of a portion of the gastric fundus around the
sphincter area of esophagus)

Nursing managementAssessment Nursing
diagnosisObjective Intervention evaluation
Pt complains of pyrosis
Impaired tissue integrity R/T esophageal exposure to gastric acid
- Pt not to have pyrosis for after 8 hrs.- Pt is able to verbalize knowledge of necessity lifestyle changes with 24 hours of discharge from the hospital
Teach patient to avoid foods that cause pain and or can increase acid secretion.
-Pt has no more pyrosis-Pt knows the necessity lifestyle changes

Nursing managementAssessment Nursing
diagnosisObjective Intervention evaluation
- Pt complains of recurrent regurgitation
- Pt shows signs of uncomforting.
Risk of aspiration R/T recurrent regurgitation
Pt won’t show signs of aspiration within 8 hours
Teach the pt to:-Elevate the HOB while in bed -Eat small frequent meals.-Not to eat or drink 2 hours before bed time
-No more regurgitations, according to the pt
Nursing managementAssessment Nursing
diagnosisObjective Intervention evaluation
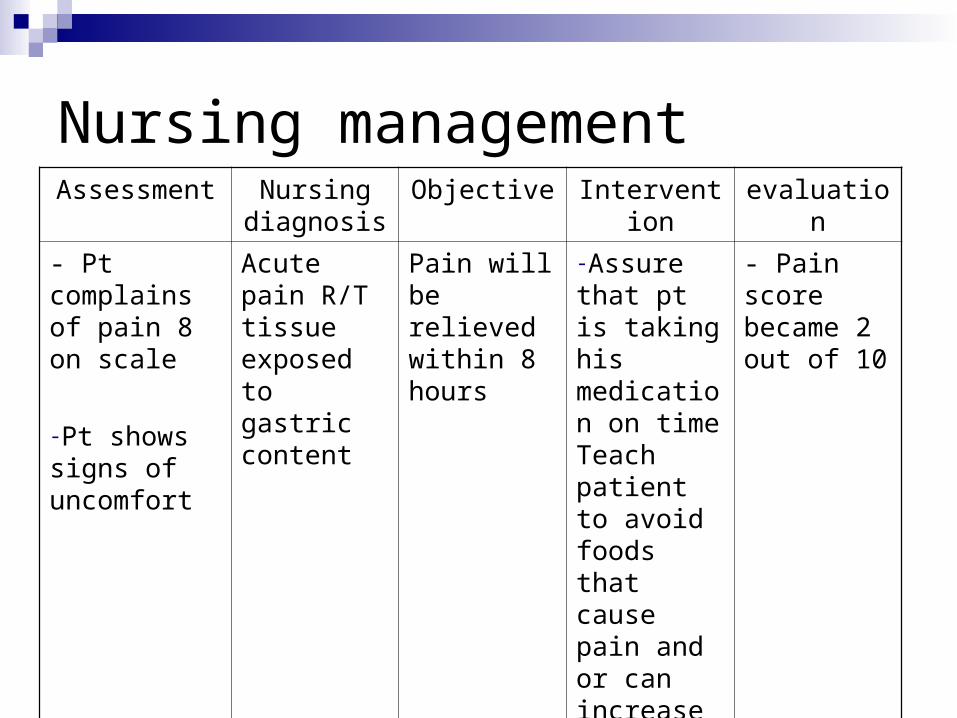
- Pt complains of pain 8 on scale
-Pt shows signs of uncomfort
Acute pain R/T tissue exposed to gastric content
Pain will be relieved within 8 hours
-Assure that pt is taking his medication on timeTeach patient to avoid foods that cause pain and or can increase acid secretion
- Pain score became 2 out of 10

Nursing managementAssessment Nursing
diagnosisObjective Intervention evaluation
-Pt has weight loss-Pt state that he is not eating so he’ll not feel pyrosis.
Imbalance nutrition R/T decrease intake
Pt will achieve adequate caloric and nutritional intake
-Explain the importance of adequate nutrition -Teach the pt about the diet which doesn’t cause esophagus irritation
-No more weigh loss during the daily weighting-Pt receiving and adequate caloric diet as followed by Dietitian
Summary GERD is an excessive reflux may occur because
of a incompetent lower esophageal sphincter, pyloric stenosis, or a motility disorder.
symptoms may include pyrosis, dyspepsia, regurgitation.
Management starts with health education, then medications, and the last option will be the surgical interventions
Nurses play a significant role in providing care for patients with GERD.

Assignment
Write about a diet plan for patient with GERD. What are the recommended food for them and which types of food should be avoided.Date of submission, Monday 12th Oct, 2015.
Reference
Brunner & Suddarth’s Textbook of Medical-Surgical Nursing, 2013.

Thanks