future ph education - fkm.unair.ac.id · •health public good social goal of many sectors and...
TRANSCRIPT

FUTURE PH EDUCATION
Widodo J. Pudjirahardjo, 2018
Created by:
Widodo J Pudjirahardjo

• Health Public Good Social Goal of many sectors and communities;
• Government and Educational Institutions have fundamental, statutory duty to assure the health of the public, but
• Government and Educational Institutions. cannot do it alone;
• Need for Intersectoral and Community Engagement in partnership with government.
Approach and Rationale
= =
Created by:
Widodo J Pudjirahardjo
TOPIK
Created by:
Widodo J Pudjirahardjo
Bahasan skenario
masa depan Bidang
Kesehatan Masyarakat
Bidang

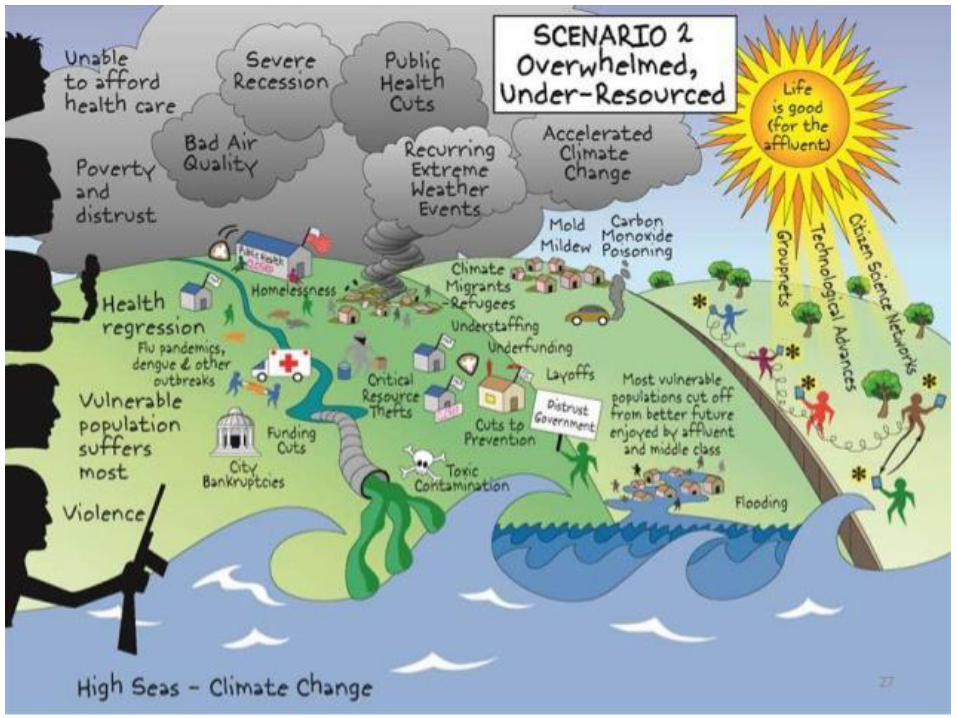
FUTURE PH CHALLENGES• Global Warming and Climate Change;• More frequent Occurrence of Disaster;• High Poluted Environment;• Complexity of Preventing the Spread of
Diseases;• The New Problem of Infectious Diseases; • The Behavior of a Society that is
increasingly Varied and Risky; and• Public Health System in Disarray.

PH System in “Disarray”1. Fragmented Efforts;
2. Fragmented Service Delivery;
3. Confusing Legal Authority;
4. Disjointed Policy Development;
5. Lack of Accountability;
6. Chronic Under Funding;
7. Lack of Trained Resources;
8. A Weakened Public Health Effort; and
9. Outdated Technology.Created by:
Widodo J Pudjirahardjo
TOPIK
Created by:Widodo J Pudjirahardjo
Bahasan skenario
masa depan Bidang
Kesehatan Masyarakat
System;Structure;
Learning Outcome;Curricullum & Content;
Basic Knowledge.
What Public Health Does1. Prevents Epidemics;2. Protect the Environment, Workplace,
Housing, and Food;3. Promote Healthy Behavior;4. Develop Policies to Promote Health;5. Monitors the Health of the Population;6. Mobilizes Communities for Action;7. Assures that Health Care Services are High
Quality, Safe, and Accessible;8. Trains PH Specialists in Investigating and
Preventing Diseases;9. Responds to Disasters; and
10. Build a Big Population Base Data.

CORE PH FUNCTION
Created by:
Widodo J Pudjirahardjo
• Assessment (Collection Data and Analysis foInformation to Identify important problems):– Surveillance, Monitor and Collect Data; and
– Diagnose and Investigate.
• Policy Analysis and Policy Development (Based on Health Needs)– Inform, Educate, and Empower People about Health Issues;
– Mobilize Community Partnership to Identify and Solve Health Problems;
– Develop Policies and Plans that support Individual and Community Health Efforts.
Essential Public Health Functions

Essential Public Health Functions• Assurance (Assuring that Appropriate Services are
Available and Assessible to meet the Needs of the Population):– Enforce Laws and Regulations that Protect Health and
Ensure Safety;
– Link People to Needed Personal Health Servives and Assure the Provision of Health Care when otherwise Unavailable;
– Assure a Competence Public Health and Personal Healthcare Workforce;
– Evaluate Effectiveness, Accessibility, Quality and Safety of Personal and Pulation-Based Health Services; and
– Research New Insight and Innovative Solutions to Health Problems.
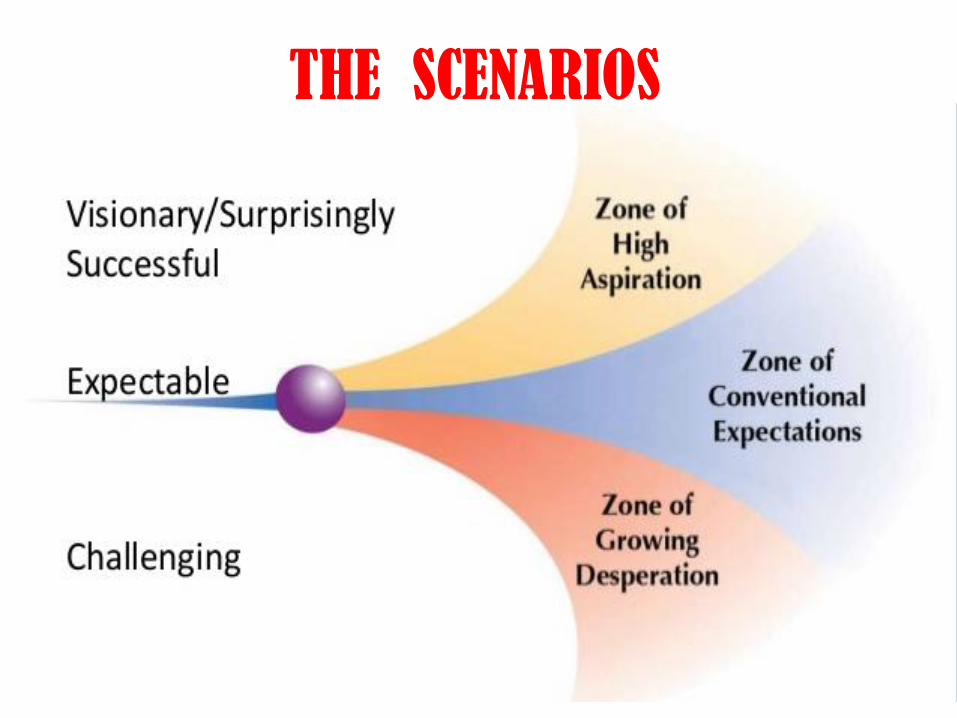
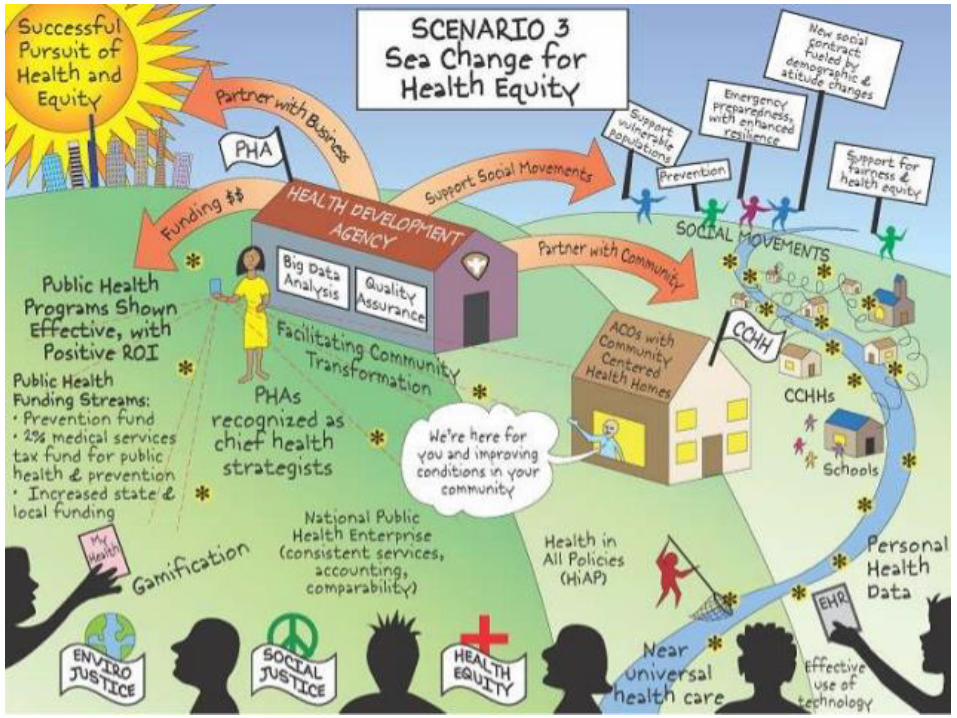
THE SCENARIOS


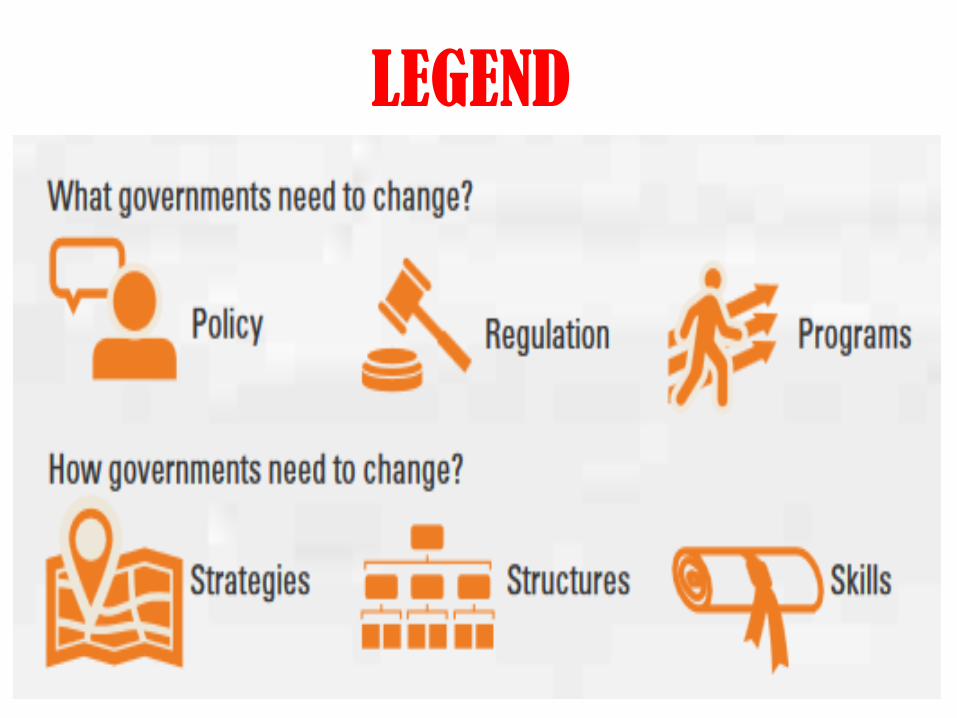
LEGEND

Professional Competencies in Public Health, Adapted From the Report of
The Faculty/Agency Forum
1. Universal Competencies:2. Public Health Administration and
Policy;3. Epidemiology and Biostatistics:
Individual Competencies in Epidemiology;
Individual Competencies in Biostatistics.
4. Behavioral Sciences; and
5. Environmental and Workplace Public Health.

Universal Competencies:
• Analytical Skills;
• Communication skills;
• Policy Development/Program Planning Skills;
• Cultural Skills;
• Basic Public Health Sciences Skills; and
• Financial Planning and Management Skills.
Professional competencies in public health, adapted from the report of
the Faculty/Agency Forum

Professional competencies in public health, adapted from the report of
the Faculty/Agency ForumPublic Health Administration and Policy:
• Communication Skills;
• Leadership and Team Leadership;
• Policy Analysis/Strategic Planning;
• Organizational Management/Positioning;
• Program Planning And Administration;
• Human Resources Management;
• Building Management Information Syst; and
• Political and Economic Analysis.

Individual Competencies in Epidemiology:• Situation and Community Health
Analysis; • Surveillance and Study Design;• Surveillance Implementation;• Data Management and Analysis; and• Providing of Health Information.
Professional competencies in public health, adapted from the report of
the Faculty/Agency Forum

Individual Competencies in Biostatistics:• Data Requirements;• Database Management;• Building Health Information System;• Descriptive Statistics;• Inferential Statistics; and• Developing Reporting & Providing
Population Information.
Professional competencies in public health, adapted from the report of
the Faculty/Agency Forum
Behavioral Sciences:
• Knowledge of the Public Health System and Policy and Regulation Development;
• Communication and Persuation Skills;
• Advocative Skills;
• Ability to Conduct an Ongoing Community Health Needs & Behavior Assessment, Individually or as Part of a Team;
Professional competencies in public health, adapted from the report of
the Faculty/Agency Forum
Behavioral Sciences:
• Awareness and ability to implement behavior change strategies for primary, secondary, and tertiary health promotion/disease prevention activities in the public health setting;
• Networking Skills; and
Professional competencies in public health, adapted from the report of
the Faculty/Agency Forum
Behavioral Sciences:
• Ability to disseminate knowledge of be-havior and social concepts and methods cultural sensitivity and understanding of how culture affects behavior and health status.
Professional competencies in public health, adapted from the report of
the Faculty/Agency Forum
Environmental and Workplace Public Health:• Basic Environmental and Workplace Science;• Risk Management Skills;• Epidemiology of Acute and Chronic Diseases
associated with Environmental and Workplace Stresses;
• Economic Considerations in Public Health; and
• Environmental and Workplace Law.
Professional competencies in public health, adapted from the report of
the Faculty/Agency Forum

PUBLIC HEALTH EDUCATION TODAY
1. Purpose of Report;
2. Organization;
3. Educational Goals;
4. Curriculum;
5. Practice Links;
6. Students;
7. Research;
8. Continuing Education;
9. Relation to Medical School;
10.Relation to other Schools;
11.Role of Government;
12.Role of professional Associations.

Public Health Training Pathway

• ST1 – ST5 refer to the years of training after Foundation, Training is continuous across the five years. (indicative)
• Entry into specialty training for medical graduates is normally straight from Foundation. Medical graduates may also be able to apply for competitive entry from fixed term specialty training posts and from career posts. Successful applicants from these routes will be assessed on an adperson am basis for transferable competence but will be required to pass both parts of the MFPH before adjustment of the training pathway. If successful, entry will be considered to have been at ST2 or ST3 as appropriate.
Notification:

• Entry into specialty training for other graduates requires a good (2:1 or above) first degree or a higher degree in a subject relevant to public health plus a minimum of three years post first degree health related and relevant work experience. Individuals will be assessed for transferable competence.
• Other graduates apply for entry into specialty training through the same portal as medical applicants. There is no national quota applied to either group.
• Entry for an individual from either group with Part A MFPH will lead to a reduction in training time.
• Entry from either group who has completed an appropriate postgraduate degree in Public Health will lead to a reduction in training time provided the appropriate competencies in Phase 1 can be evidenced.

• Most trainees undertake a course of formal academic study leading to Pt A MFPH. The course may be taken over one or two years. Part A may be taken at any time during phase 1.
• Some trainees may apply successfully for time during phase 3 to undertake a PhD (outside the Walportinitiative). Two years of this may count towards a CCT provided all core competencies are also met.
• Time out of training, for example to gain experience abroad, may be granted at the discretion of the local Dean. Experience abroad during training can be counted towards training provided that it is part of an approved programme, is supervised and has prospective GMC approval

Three Dimensional Model of Learning
LEARNING OUTCOME
Ethical Management of SelfPublic Health SettingEthical Management of Self
Phases of LearningSu
rve
illan
ce a
nd
Ass
ess
me
nt
Ass
ess
ing
Effe
ctiv
en
ess
Lead
ers
hip
an
d N
etw
ork
ing
Po
licy
& S
trat
egy
Dev
’t
He
alth
& S
oci
al S
erv
eic
eQ
ual
He
alth
Pro
tect
ion
He
alth
Imp
rove
me
nt
Pu
blic
He
alth
Inte
llege
nce
Aca
de
mic
Pu
blic
He
alth
EGDELWONK
sllikS
yciloP-nimdA
cE-lo P-coS
noitam tr so yf SnI
x Des a e s iD
h dc oa he ts ee MR
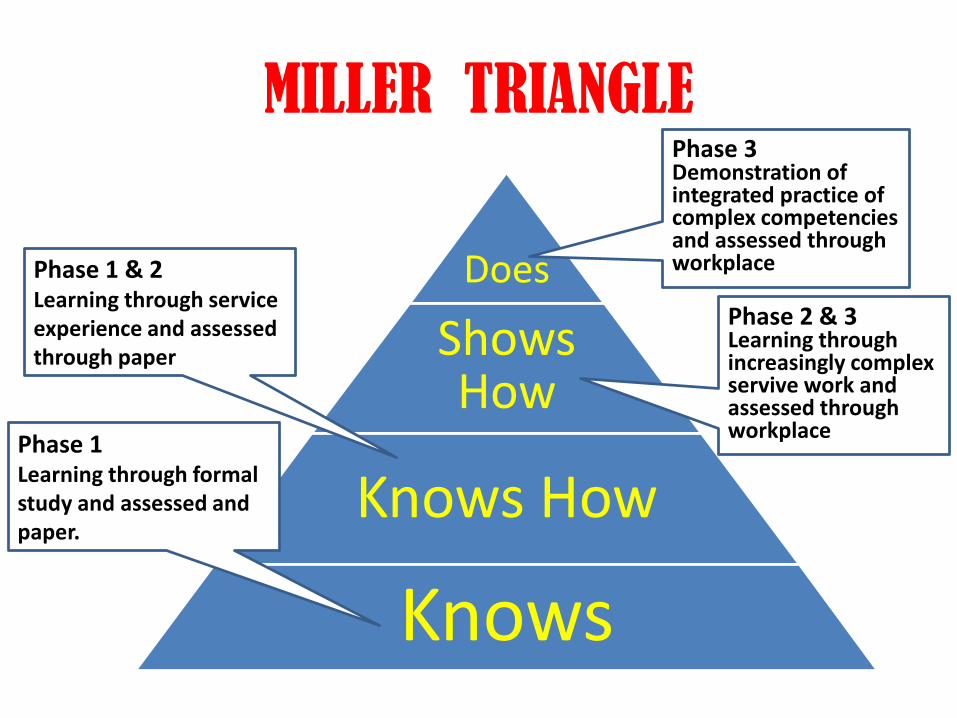
MILLER TRIANGLE
Does
Shows How
Knows How
Knows
Phase 1Learning through formal study and assessed and paper.
Phase 1 & 2Learning through service experience and assessed through paper
Phase 3Demonstration of integrated practice of complex competencies and assessed through workplace
Phase 2 & 3Learning through increasingly complex servive work and assessed through workplace