frontal lobe disorders. functional areas right frontal lobe: five functional areas left frontal...
TRANSCRIPT
Frontal Lobe Disorders
Functional Areas
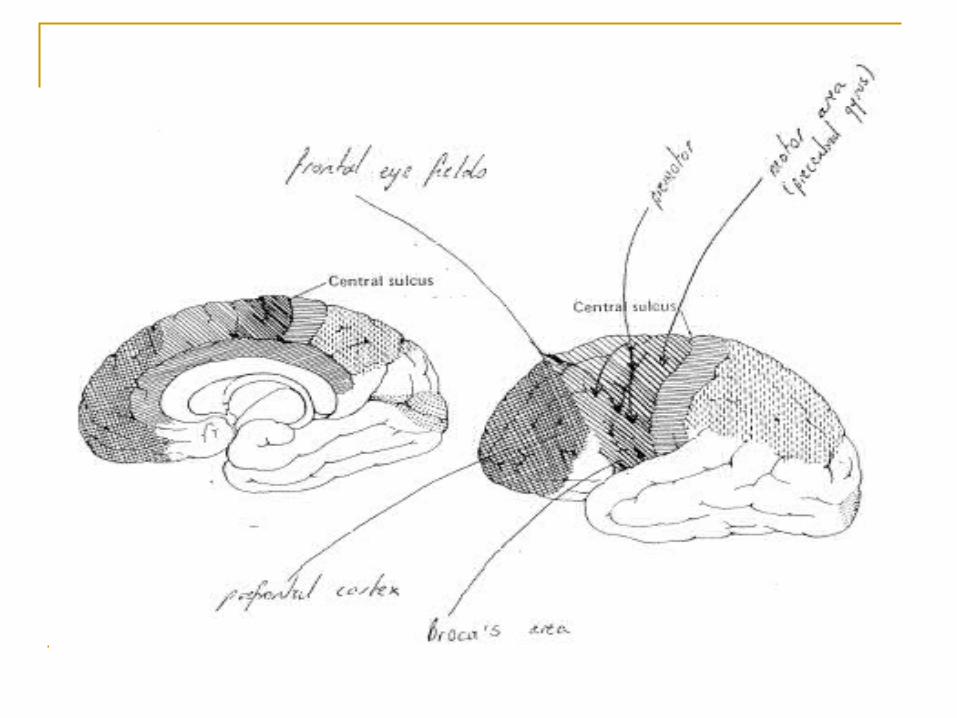
Right frontal lobe: Five functional areas
Left frontal lobe: Six functional areas - motor area - supplementary motor area - premotor area - frontal eye fields - prefrontal cortex - Broca’s area (left)
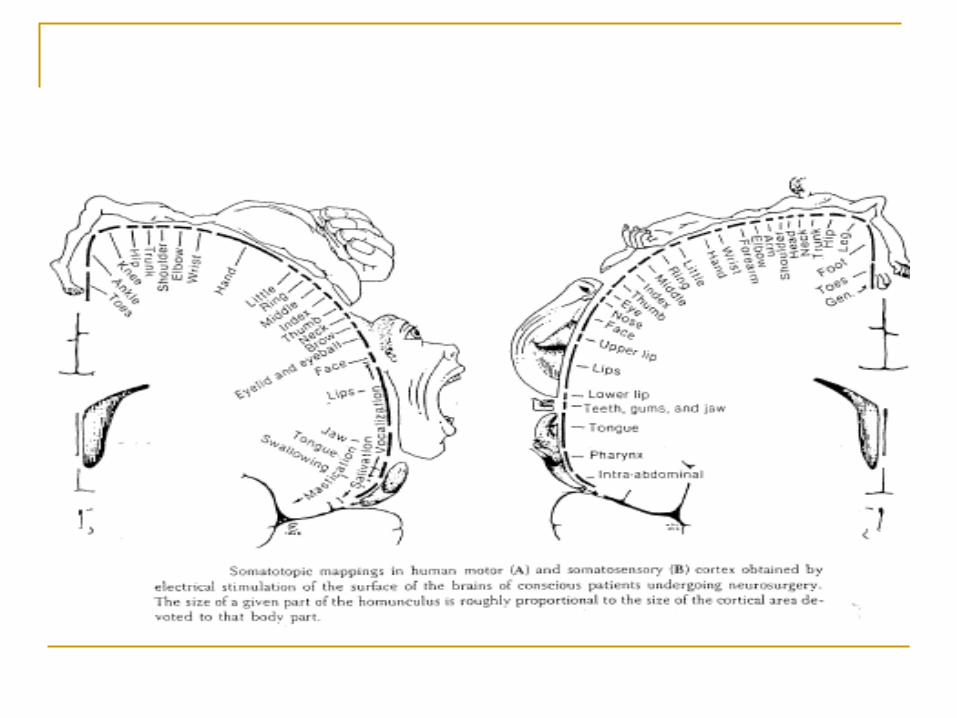
Motor and Supplementary Motor Areas Concerned with the voluntary control of
movement Cells agranular Project to ventral thalamic nuclei Damage: Contralateral hemiparesis
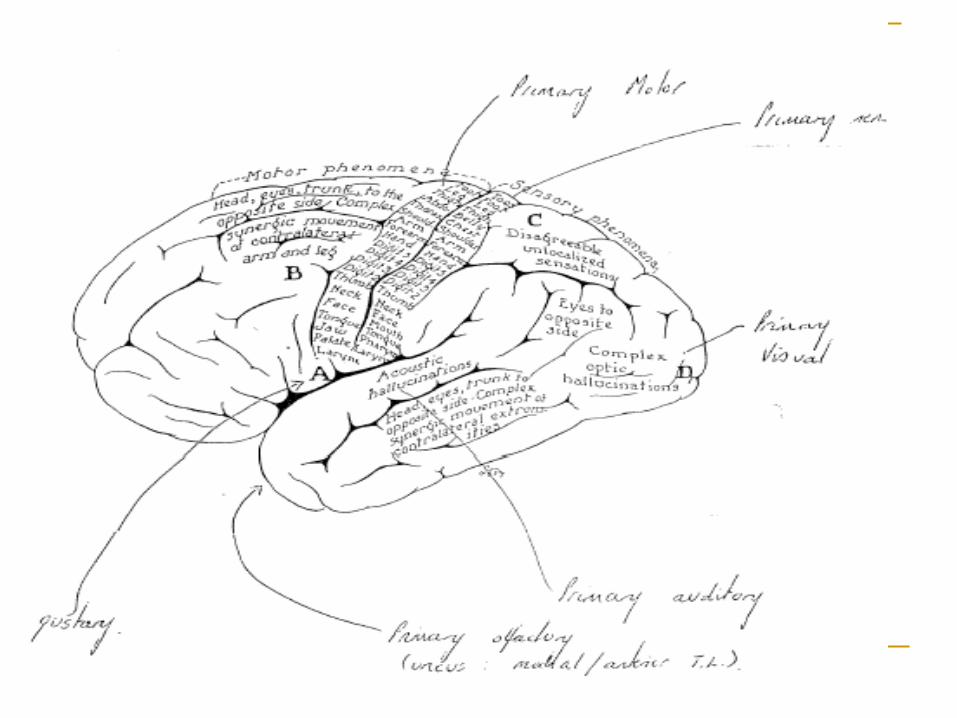
Premotor Cortex
Role in motor organisation, esp. complex movements
Intermediary between ideational aspects of planned action and implementation of movements
Involved in sensorimotor integration and praxis
Damage: Disruption in the organisation of movement
Frontal Eye Fields
Visual attention and saccadic eye movements
Damage: - Difficulty in complex visual scanning- Deviation of the head and eyes towards the
side of the lesion, difficulties with saccadic eye movements away from the side of the lesion
Broca’s Area
Contains the motor programs for the production of speech
Damage: Motor, expressive or non-fluent aphasia
Prefrontal Cortex
A. Structural Features
Undergone far greater development in humans than in other species
Proportion of brain occupied by frontal cortex increases from 3% in cats to 15% in chimpanzees to 30% in humans (rendering it difficult to investigate prefrontal functions using animal subjects)
Cortex – granularStellate cells predominate (layers II & IV). Multipolar, have short
axons that do not leave the cortex. Role: reception of information
Developmentally the prefrontal cortex (together with regions in the tertiary association area) is the last to become fully myelinated. The orbital (basal) areas myelinate before the dorsolateral.
After adolescence and through adult life the cyctoarchitecture of the human cortex remains relatively stable.
In the seventh or eighth decade: neuronal involution – size, volume and density of cells tend gradually to decrease. Most of the decrement is due to the shrinkage and disappearance of dendrites. The cortices of the frontal and temporal lobes are the first to show signs of involution with the prefrontal cortex leading most if not all other cortical areas in morphological aging.
*Highlights importance of using age-appropriate norms when assessing the integrity of prefrontal functions in the older patient.
Prefrontal Cortex (con’t)
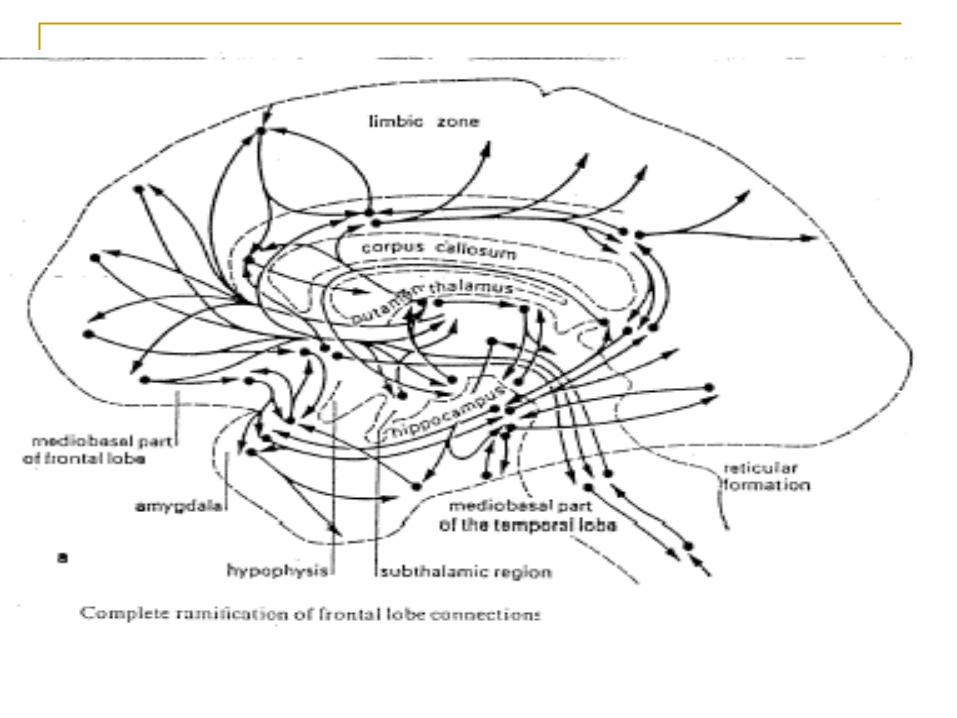
B. Connections
Prefrontal cortex has connections with secondary and tertiary association areas, basal ganglia, thalamus, limbic structures and brainstem nuclei.
Sends fibres to practically every structure from which it receives them with the exception of the basal ganglia (Unidirectional projection to the basal ganglia). Basal ganglia implicated in motor control including eye movements.
Neurological syndromes producing frontal lobe disturbancesWidespread connectivity implies that may diseases of the brain will
impact on the function of the prefrontal cortex.
A. Intrinsic Prefrontal Diseases
1. Dementia of the frontal lobe type (DFT)- Selective atrophy of the fronto-temporal cortex- Personality changes represent one of the earliest
manifestations- Cognitive deficits typically manifest on measures of flexibility,
response inhibition, reasoning and problem-solving- Memory may be relatively intact.

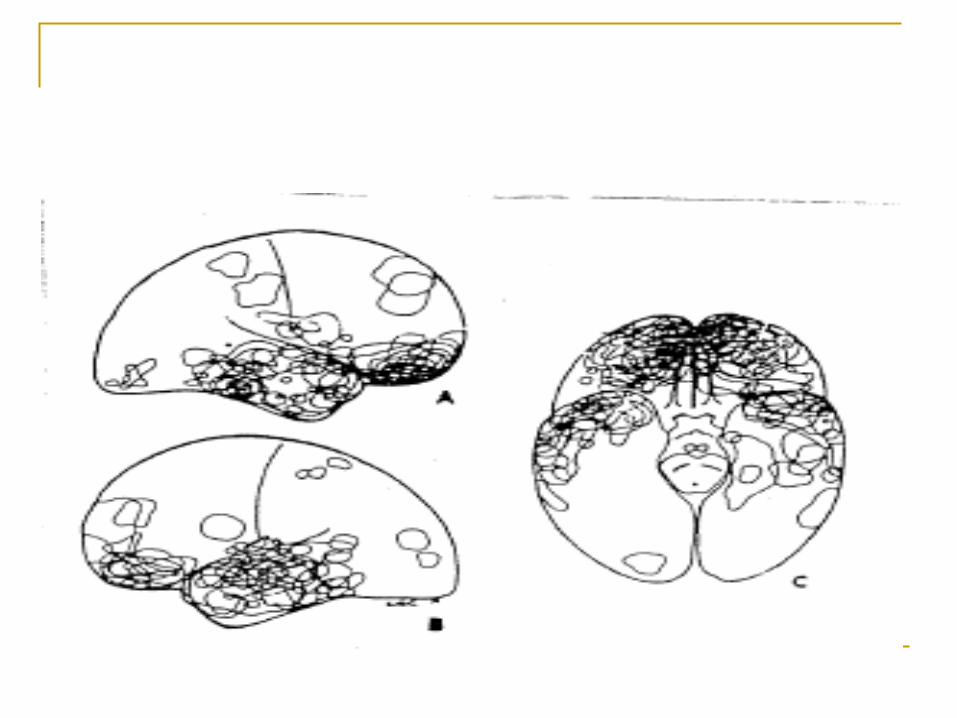
2. Traumatic Brain Injury (TBI)
Reflects the vulnerability of the frontal lobes to damage following rapid acceleration and deceleration of the head
Post-traumatic (TBI) deficits include cognitive impairments and neurologically determined personality changes.
Such patients may be impulsive, emotionally labile, disinhibited, aggressive, irresponsible and insightless.
Lezak: The characterologically altered brain injured.
3. Frontal Tumours
Clinical features will vary according to their anatomical position
Later may become nonspecific as intracranial pressure rises affecting neighbouring limbic tracts and other parts of the brain
Those more medially located may cause a profound global amnesia as they exert pressure on basal forebrain structures and anterior columns of the fornix
Patients with orbital tumours may show disinhibited behaviour.
4. Frontal Lobe Epilepsy
May be treated via frontal lobe resection.
B. Diseases primarily extrinsic to the frontal lobes.
1. Parkinson’s Disease
2. Huntington’s Disease
3. Chronic Alcohol Abuse
4. Multiple Sclerosis
5. Normal Pressure Hydrocephalus
Etc, etc.
Neuropsychological disorders seen in association with frontal damage Neuropsychological descriptions of the role of the prefrontal
cortex vary.
Agreed that frontal lobe damage typically will not result in a loss of knowledge or an inability to perform basic functions. However, when choice, alternatives, control, goal selection and monitoring are required (i.e. when new information must be processed or old information analysed in new ways) involvement of the frontal lobes is required.
Prefrontal cortex: attends, integrates, formulates, executes, monitors, modifies and judges all nervous system activities.
Application of intellect.
Luria: Man not only reacts passively to incoming information but creates intentions, forms plans and programs of action, inspects their performance and regulates his behaviour so that it conforms to these plans and programs. Finally, he verifies his conscious activity, comparing the effects of his actions with the original intentions and correcting any mistakes he has made.
Walsh
For behaviour to be adaptive it must meet environmental demands. It must be appropriate, modifiable, energised and free from disruptive internal influences. Effective behaviour requires an anticipatory relationship to the goal in the form of planning. It requires the ability to monitor ongoing actions so as to effect change should deviations from the plan occur and the effectiveness of action must finally be checked against the anticipated outcome and any necessary adjustments made. Most, if not all, of the necessary conditions for effective behaviour are dependent on the integrity of the frontal lobes.
Nature of the cognitive disturbance
Determined by lesion characteristics. Laterality, location within the frontal lobes and extent of the damage.
David (1992). “The frontal lobes constitute approximately one-third of the brain, therefore localising a disturbance to this region is rather like a person directing a visitor to an address marked Europe.
Descriptions of prefrontal functions typically identify at least three major areas of frontal cortex and their connections.
Damage to each will produce a different neuropsychological profile.
A. Orbitobasal Surface
Responsible for the flexible control of excitation and inhibition.
Damage will produce a disorder of control – an inability to inhibit inappropriate responses
Frequently evident in the head injured individual. Initially manifest as aggressive, uncontrolled behaviour. More subtle version (seen in later stages of recovery) evident as heightened irritability and a shortness of temper. These patients tend to speak their mind, act on impulse without consideration of the consequences of their behaviour and to be verbally and sexually disinhibited.
Damage characterised by
- Lack of restraint- Disinhibition- Tactlessness- Impulsivity- Puerility, childishness- Emotional lability
Disorder of Control (con’t)
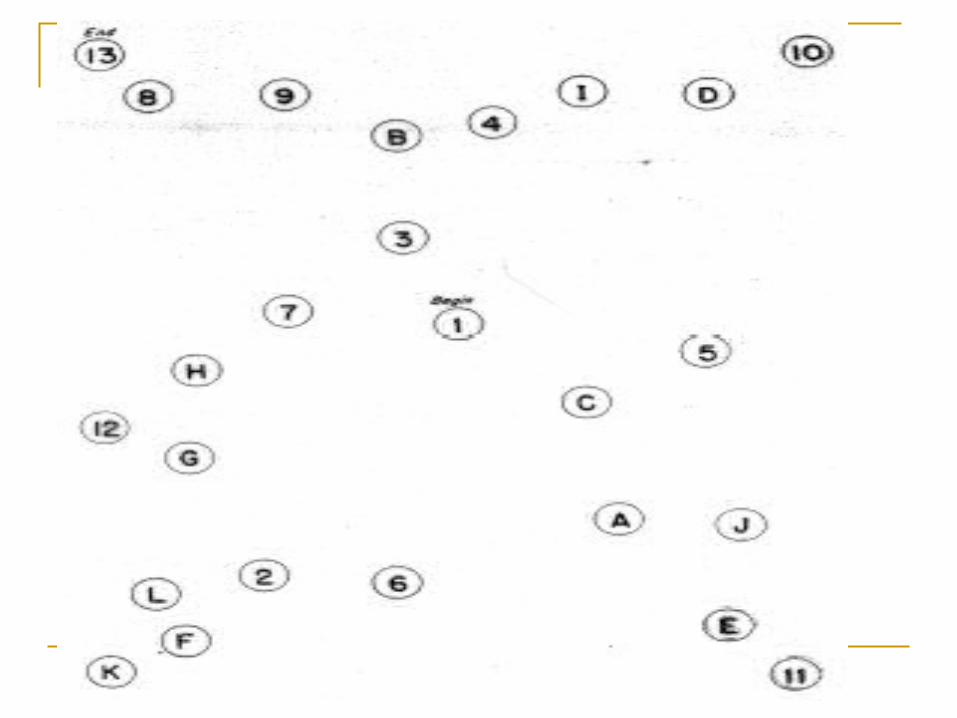
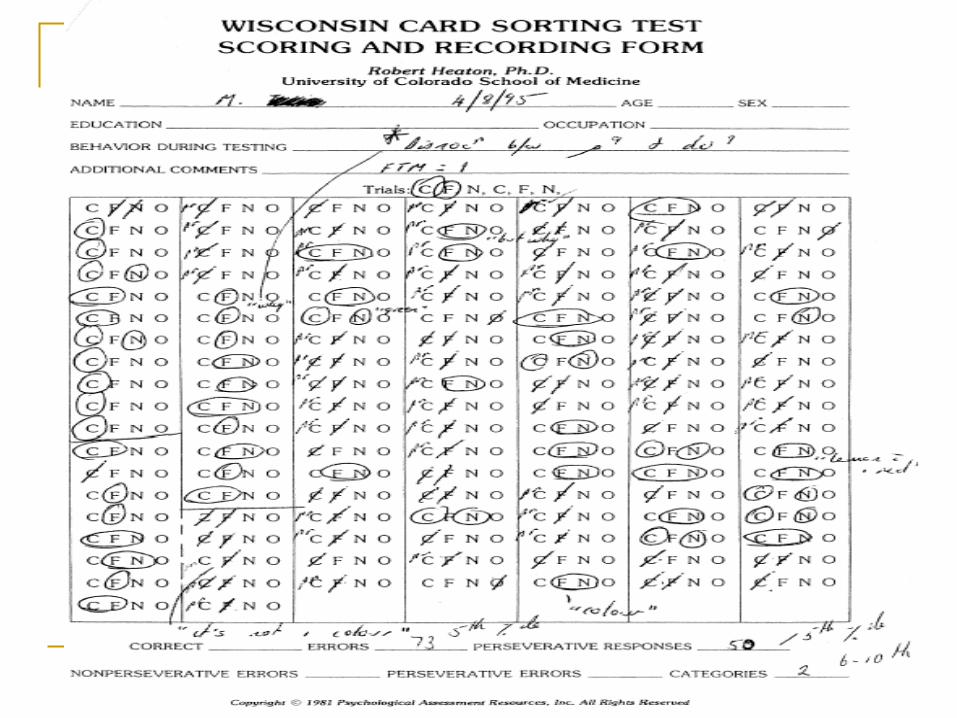
Tests that may be of use.
Those that require the subject to exercise control over their responses, to inhibit well-established though inappropriate response tendencies.
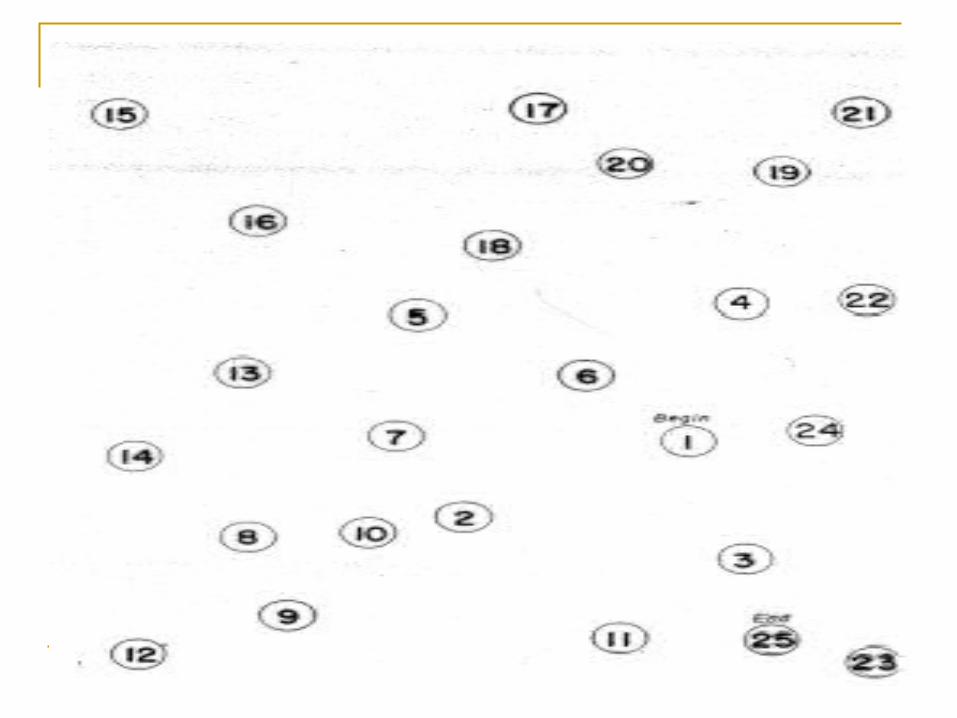
EG- Trial Making Test- Wisconsin Card Sorting Test- Controlled Oral Word Association Test- Booklet Category Test- Stroop Reading Test
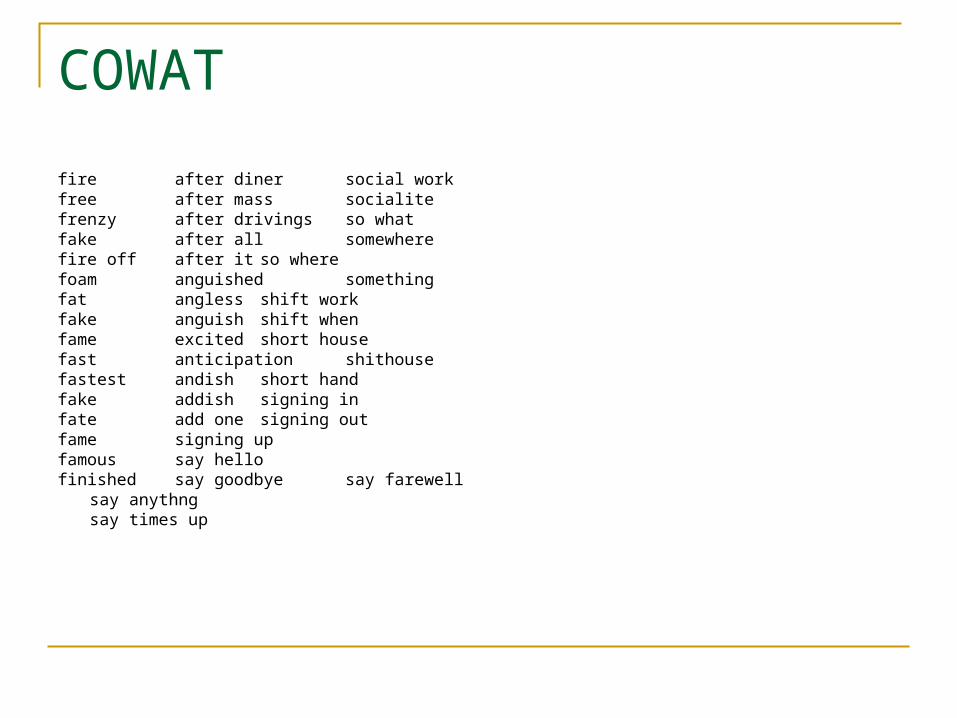
COWAT
fire after diner social workfree after mass socialitefrenzy after drivings so whatfake after all somewherefire off after it so wherefoam anguished somethingfat angless shift workfake anguish shift whenfame excited short housefast anticipation shithousefastest andish short handfake addish signing in fate add one signing outfame signing upfamous say hellofinished say goodbye
say farewellsay anythngsay times up
B. Medial Surface
Important in the initiation of drive/activity
Damage to the medial surfaces will produce apathy and a generalised decrease in activity
Such patients are either incapable of or slow to initiate movements
Closely allied with drive are motivation and will – each reflect a greater degree of intellectual control
Represent site of damage in the other major form of personality change following frontal lobe damage.
Damage characterised by
- Apathy- Aspontaneity- Adynamia- An inability to initiate and sustain behaviour- Reduced verbal output- Lack of initiative
Crystallised v’s Fluid Intelligence
VIQ v’s PIQ
C. Dorsolateral Surface
Damage leads to a disturbance of the application of intellect – Difficult to taxonomise
1. Impaired concept formation and/or conceptual flexibility- Thinking concrete and inflexible- Extreme example: Utilisation Behaviour
2. Inability to use knowledge or verbal mediation to regulate behaviour- Dissociation between knowing and doing.
3. Inability to monitor output - Difficulty in evaluating errors, using this information to effect
change in their behaviour.
4. Poor planning and organisation5. Poor problem-solving skills6. Poor memory
- Not a primary disturbance of memory but FL lesions do interfere with mnestic activity. - Difficulty organising information, following instructions, temporally discriminating items in memory, using external cues to guide learning, comparing results with original intentions, retrieving information.
6 a) Prospective memory - Patients may ‘forget to remember’. Intended act unavailable but may be retrieved later (when the system is cued appropriately)b) Increased susceptibility to the effects of interference (evident on tests such as the RAVLT). c) Metamemory. Knowledge and effectiveness of strategies
7. Inability to handle sequential elements and to serially organise behaviour.
Measures
Wisconsin Card Sorting Test Trail Making Test Controlled Oral Word Association Test Rey Complex Figure Booklet Category Test Tower of London Stroop Reading Test
Difficulties inherent in assessing FL disorders1. Tests themselves are multidimensional
2. Test situation is highly structuredShallice: Typically the patient has a single problem to tackle at any one time, the trials tend to be relatively short, task initiation is strongly prompted by the examiner and what constitutes task completion is clearly characterised. The patient is rarely required to plan behaviour over longer time periods or to set priorities in the face of two or more competing tasks or to make use of prospective memory.
3. Repeated assessment. Novelty crucial to notion of adaptation of intellect.
4. Accurate estimates of premorbid level of functioning difficult to obtain.
5. Normative data. S.D.’s typically large.
Neurological signs
Anosmia- Loss of smell discrimination- Common concomitant of damage to the orbital surface of the frontal lobes (orbital cortex received direct connections from the olfactory tract)- shearing of the olfactory nerve will result in complete anosmia
Utilization Behaviour- Patient compelled to grasp and use objects.
Alien Hand Syndrome- Lesions involving the corpus callosum or supplementary motor area. - Apparently purposeful movements that are dissociated from conscious volition
On examination:- Tendency for the arm to drift off and assume odd postures
especially when the eyes are closed or attention is diverted- Intermanual conflict or competition- Pts report that they can not will or command the limb to act- Tendency to attempt to control the unwanted activity by restrainign
the arm physically- May be observed in the left or right hand- Patients retain the ability to execute a new movement with resulting
inhibition of the aberrant movement. - Deficit of the voluntary inhibition of movement.
Gait Disturbances
- eg.Difficulty initiating movement
Shuffling with very small steps
Unilateral neglect (spatial, motor)
Implication for Rehabilitation
1. Lack of insightIn order for a program to be effective, awareness needs to be
present
2. Emotional/behavioural problemsVaried, range from adynamism to disinhibited, antisocial behaviour
3. Poor generalisation
4. Memory Problems
5. Impaired motivation
Every day life failures
1. Unable to cope at school – academically or interpersonally2. Unable to maintain employment – can not report on time,
misses out important steps, can not learn from experience3. Unable to deal with finances4. Unable to maintain relationships
Frontal lobe syndrome (cognitive plus personality changes) is often particularly distressing for family and associates of the sufferer.
Disorders of Self-Awareness
Decreased insight common following frontal lobe damage – differentiate from denial.
Associated Syndromes
1. Confabulation
Production of incorrect, sometimes bizarre responses to routine questions.
Range from momentary or provoked to fantastic or spontaneous
2. Reduplicative Paramnesia
A delusional condition is which a patient believes that two or more locations exist with nearly identical attributes.
Right hemisphere and frontal system dysfunction common
3. Capgras Syndrome
Reduplication of a person in which the patient believes that someone close has been replaced by a similar substitute
Patient will misidentify familiar figures (usually a family member) as impersonating the real person, usually with sinister intent
Will be convinced that this person is from a ‘second’ family. Cognitively, they recognise the impossibility of the situation. Yet they remain convinced that it is other than the ‘real’ person.