friday, july 17 – saturday, july 18, 2015 sheraton wall ... july 17 – saturday, july 18, 2015 ....
TRANSCRIPT

Theme - HIV/Viral Hepatitis: Antiviral Therapy Development and Access
For more information and to register, visit: coinfectionmeeting.com
Friday, July 17 – Saturday, July 18, 2015 Sheraton Wall Centre, Vancouver, Canada
PHOTO BY JAMESZ_FLICKR

www.iasociety.org
Highlights from the Meeting
• Only international meeting that brings together all the stakeholders in HIV/Hepatitis Coinfection to work towards equitable access to Hepatitis therapy globally – Review latest science – Identify barriers – Learn from recent successes in low middle and
high income countries – Engage all partners in constructive solutions

HCV treatment revolution

2.2% have treatment (WHO 2014)

World Hepatitis Alliance

Change the mindset
• Challenge the prevailing mindset such that viral hepatitis joins HIV, malaria and tuberculosis as the most important infectious diseases
• Funders, government officials, NGOs, medical societies, foundations, man-in-the-street
• Advocacy is key - 240 million people who are
chronically infected with HBV (plus 130 million HCV), if only a fraction could be empowered to respond…

Improving the cascade of care
Diagnosis Access
Treated SVR
Modeled data for non-VA US population
Yehia PLoS One 2014
8
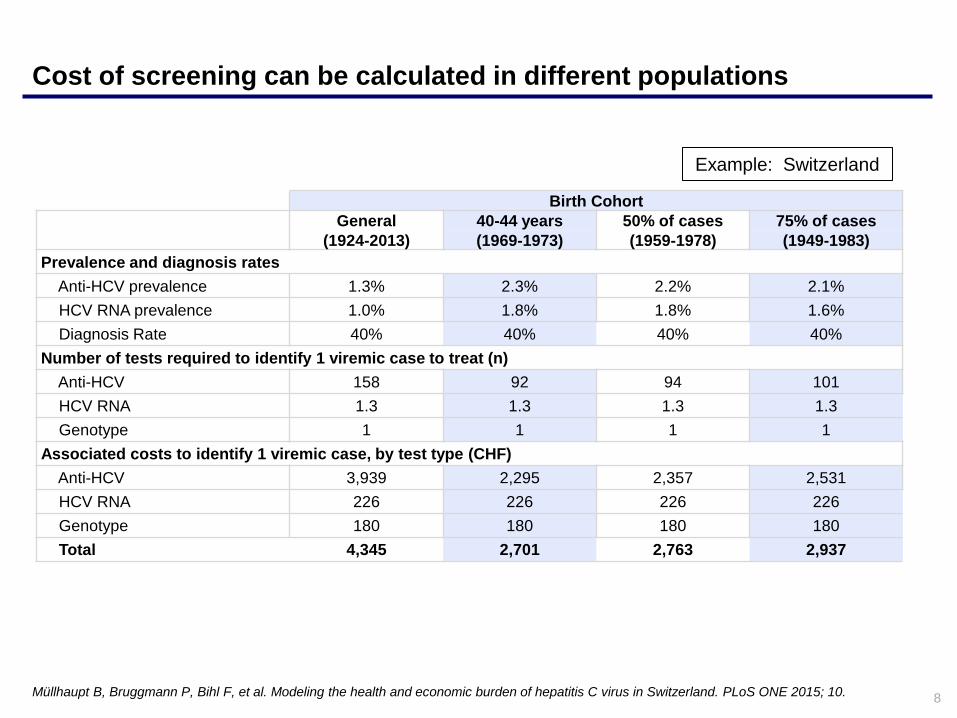
Cost of screening can be calculated in different populations
Müllhaupt B, Bruggmann P, Bihl F, et al. Modeling the health and economic burden of hepatitis C virus in Switzerland. PLoS ONE 2015; 10.
Example: Switzerland
Birth Cohort
General 40-44 years 50% of cases 75% of cases (1924-2013) (1969-1973) (1959-1978) (1949-1983)
Prevalence and diagnosis rates Anti-HCV prevalence 1.3% 2.3% 2.2% 2.1% HCV RNA prevalence 1.0% 1.8% 1.8% 1.6% Diagnosis Rate 40% 40% 40% 40% Number of tests required to identify 1 viremic case to treat (n) Anti-HCV 158 92 94 101 HCV RNA 1.3 1.3 1.3 1.3 Genotype 1 1 1 1 Associated costs to identify 1 viremic case, by test type (CHF) Anti-HCV 3,939 2,295 2,357 2,531 HCV RNA 226 226 226 226 Genotype 180 180 180 180 Total 4,345 2,701 2,763 2,937

The favorable safety profiles of new DAA combinations suggest that minimal laboratory monitoring will be necessary to assess safety during treatment. Diagnostics and monitoring could be limited to: - two HCV antigen tests to confirm chronic infection before treatment and clearance after treatment (detection limit HCV RNA >2000 IU/mL: US$34 for two tests - two full blood counts + clinical chemistry tests (ALT / creatinine): US$22 - genotyping if necessary: US$90 (not needed if treatment is pan-genotypic)
Simplified diagnostic testing for HCV
10
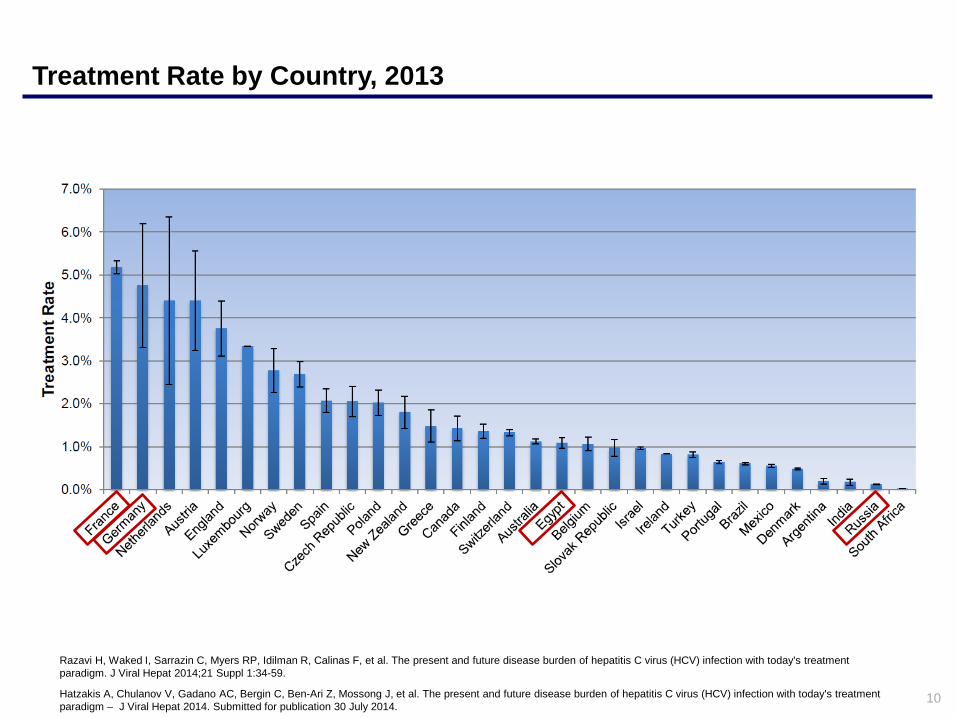
Treatment Rate by Country, 2013
Razavi H, Waked I, Sarrazin C, Myers RP, Idilman R, Calinas F, et al. The present and future disease burden of hepatitis C virus (HCV) infection with today's treatment paradigm. J Viral Hepat 2014;21 Suppl 1:34-59.
Hatzakis A, Chulanov V, Gadano AC, Bergin C, Ben-Ari Z, Mossong J, et al. The present and future disease burden of hepatitis C virus (HCV) infection with today's treatment paradigm – J Viral Hepat 2014. Submitted for publication 30 July 2014.

11
HCV Diagnosis Rate, Treatment Rate and Prevalence
Wedemeyer H, Dore GJ, Ward JW. Estimates on HCV disease burden worldwide - filling the gaps. J Viral Hepat 2015;22 Suppl 1:1-5.

12
HCV burden among PWID in LMICs
10 out of 16 million PWIDs have anti-HCV antibodies (Nelson, Lancet, 2011) more than 5% of the HCV+ are PWIDs globally
PWID-HCV+: 26% live in East/SouthEast Asia and 23.5% in Eastern Europe (Nelson, Lancet, 2011)
25.6% PWIDs
21.5% PWIDs
40.4% PWIDs
5.6% PWIDs
2.7% PWIDs
0.14 million
1.1 million
4.1 million
0.64 million
1.4 million
PWID Not PWID Number of adults with HCV antibodies % of PWIDs
Georgia
Ukraine
Russia
Myanmar
Indonesia
Vietnam
(adapted from Luhmann et al. IJDP. forthcoming)
2.7 million 9.2% PWIDs
2nd International HIV/Viral Hepatitis Co-infection Meeting IAS Vancouver 2015

13
Use of non-sterile equipment needs to be eliminated
Hutin YJ, Hauri AM, Armstrong GL. Use of injections in healthcare settings worldwide, 2000: literature review and regional estimates. BMJ 2003;327:1075.

Potential role of addiction care
Testing, awareness and counseling
Evaluation, retention and adherence
Prevention of reinfection

15
Increasing treatment and SVR can significantly reduce the number of viremic infections
-
50,000
100,000
150,000
200,000
250,000
300,000
Total Infected Cases (Viremic) - Germany
Basecase Increased Efficacy Only Increased Efficacy & Treatment
-
50,000
100,000
150,000
200,000
250,000
Total Infected Cases (Viremic) - France
Basecase Increased Efficacy Only Increased Efficacy & Treatment
-
1,000,000
2,000,000
3,000,000
4,000,000
5,000,000
6,000,000
7,000,000
Total Infected Cases (Viremic) - Egypt
Basecase Increased Efficacy Only Increased Efficacy & Treatment
-
1,000,000
2,000,000
3,000,000
4,000,000
5,000,000
6,000,000
7,000,000
Total Infected Cases (Viremic) - Russia
Base Case Increased Efficacy Only Increased Efficacy & Treatment

16
Increasing treatment and SVR can significantly reduce the disease burden
-
200
400
600
800
1,000
1,200
1,400
1,600
1,800
Liver-related Deaths - Germany
Basecase Increased Efficacy Only Increased Efficacy & Treatment
-
200
400
600
800
1,000
1,200
1,400
1,600
1,800
Liver-related Deaths - France
Basecase Increased Efficacy Only Increased Efficacy & Treatment
-
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
Liver-related Deaths - Egypt
Basecase Increased Efficacy Only Increased Efficacy & Treatment
-
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
Liver-related Deaths - Russia
Base Case Increased Efficacy Only Increased Efficacy & Treatment
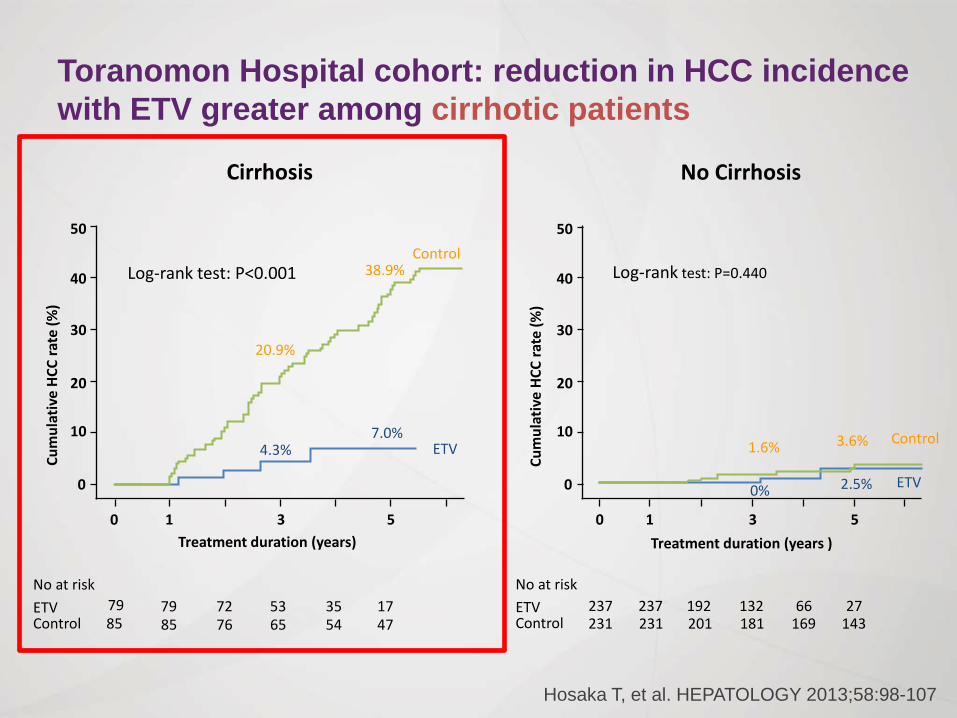
Toranomon Hospital cohort: reduction in HCC incidence with ETV greater among cirrhotic patients
Hosaka T, et al. HEPATOLOGY 2013;58:98-107
1 3 5 Treatment duration (years)
50
40
30
20
10
0
0
Cum
ulat
ive
HCC
rate
(%)
Cirrhosis
Log-rank test: P<0.001
79 85 85
79 72 76 65
53 35 54 47
17 ETV Control
No at risk
50
40
30
20
10
0
0 1 3 5
Log-rank test: P=0.440
No Cirrhosis
1.6% 3.6%
2.5% 0%
237 231 231
237 192 201 181
132 66 169 143
27
Control
ETV
ETV Control
No at risk
Treatment duration (years ) Cu
mul
ativ
e HC
C ra
te (%
)
20.9%
4.3%
38.9%
7.0%
Control
ETV

18
Barriers to HCV treatment
(Wolfe et al. Special issue on HCV and drug use. IJDP. forthcoming)
2nd International HIV/Viral Hepatitis Co-infection Meeting IAS Vancouver 2015

Data from Global Burden of Disease report, 2013. Lancet January 10th 2015, 385: 117-171 FDA Orange Book. http://www.accessdata.fda.gov/scripts/cder/ob/default.cfm. Infographic by TAG.

5g of daclatasvir 12 weeks of treatment, 60mg/day Cost = $53,000 (UK price)
5g of diamonds 25 1-carat ($1900 each) Cost = $48,000

Daclatasvir: generic prices
Cost of API = $10,000/kg
API per 12 weeks = $50
Formulated drug = $70
Packaged drug = $71
Final generic Price = $107
API needed per person = 5g (60mg x 84 days)
Formulation = 40%
Packaging = $0.35/month
Profit margin = 50%
For mid 2015, Prices falling rapidly
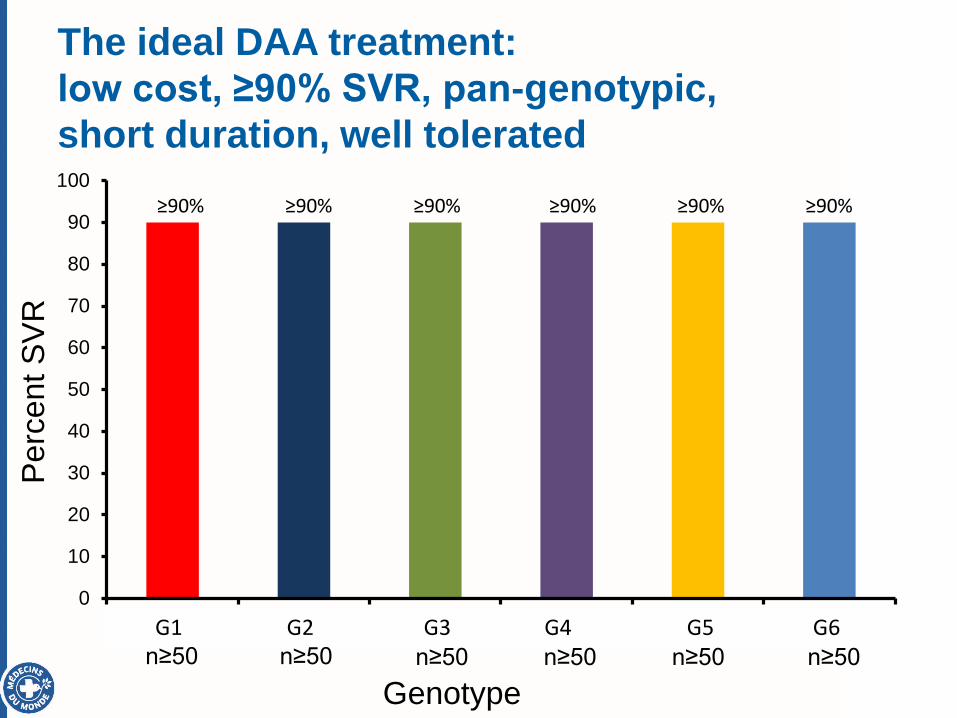
The ideal DAA treatment: low cost, ≥90% SVR, pan-genotypic, short duration, well tolerated
0
10
20
30
40
50
60
70
80
90
100
1 2 3 4 5 6
Genotype
Perc
ent S
VR
≥90% ≥90% ≥90% ≥90% ≥90% ≥90%
n≥50 n≥50 n≥50 n≥50 n≥50 n≥50 G1 G2 G3 G4 G5 G6

Sofosbuvir + Daclatasvir ± RBV (12 or 24 weeks)
Sources: A1444040 trial; ALLY-1; ALLY-2; ALLY-3; 3 French EAPs
525/556 193/216 47/50 1/1 1/1 52/56

Registration status worldwide of Sovaldi® and Daklinza®
High income countries
Countries where Sovaldi® is registered
Countries where Daklinza® is registered
Countries where Daklinza® & Sovaldi® are registered

BUT G3 Remains a Concern in the Real World TRIO: 24 Wks SOF + RBV for GT3 HCV in Real-World Settings
18 academic and 17 community practices in US TRIO network 24 wks sofosbuvir + RBV (N = 96)
ITT population: n = 96; PP population (completed therapy with SVR12 data): n = 77
Key baseline characteristics Male: 56%
HCV RNA > 6 x 106 IU/mL: 15%
Cirrhosis: 30%
Previously treated: 39%
2/96 pts died from causes not related to treatment
Kowdley K, et al. EASL 2015. Abstract P0867.
SVR
12 (%
)
Overall
Tx-Naive, Noncirrhotic
Tx-Expd, Cirrhotic
PP
100 80 60 40 20
0 ITT
70 87
100 80 60 40 20
0 ITT
73 94
PP
100 80 60 40 20 0
ITT
57 80
PP
77 N = 96
34 N = 44
10 N = 14

Selection of RAVs in Patients who Failed after LDV (no SOF)
16% (12/76)
84% (64/76)
Before LDV Treatment
99% (72/73)
1%
At Virologic Failure With LDV Treatment
Patients without NS5A RAVs Patients with NS5A RAVs
Patients who failed after a ledipasvir-containing treatment
(without sofosbuvir)
(Dvory-Sobol et al., EASL 2015)

The NS5A RAVs are Persistent 24 Wks LDV/SOF After Failure of LDV/SOF-Based Therapy: Effect of Baseline RAVs
NS5B variants emerged during retreatment in 33% of pts (4/12) with virologic failure – S282T: n = 2; L159F: n = 1; S282T + L159F: n = 1
Lawitz E, et al. EASL 2015. Abstract O005.
SVR12 by Baseline NS5A RAVs, n/N (%) LDV/SOF for 24 Wks Number of RAVs 0 11/11 (100) 1 11/16 (69) ≥ 2 7/14 (50)
Single NS5A RAV Q30R or M28T 5/5 (100) L31M 4/5 (80) Y93H/N 2/6 (33)

Treatment volumes increasing
Liver Clinic
Make sure you have the capacity to treat & follow everyone

Clinic Issues • Matching needs of your population
– Setting (hospital vs clinic vs the street) – Support services (social work, addiction
counseling) • Triage
– Who gets treated first? • Paper work
– Without systems in place…you will drown! • Following patients on treatment
– Capacity (MD/RN/other), frequency, liver disease

30
HCV in Mongolia
• Genotype 1b (98%) • Anti-HCV average 9.8-15% (285,700-450,000 people)
» Elder people up to 33%
» Health workers >50% co-infected HCV and HBV
» 82% reported needle-stick injuries in 2008
• Viremic 6.8-11% (210,000-330,000 people) • Diagnosed ever: 60,000 (1300 new diagnoses 2013)
» Liver biopsy: 40-60/year (mainly for HCC); Fibroscans: >3000
• Treated (PEG/RBV): 200; DAAs: happy few • Liver transplants: 8 (of which 3 due to HCV) • LC >>350/100,000 many undiagnosed • 15% of all mortality due to LC/HCC (2nd cause of death, esp. in 40-65 age
group) • HCC mortality: 63.2/100,000; world record, 8x world average
18/07/2015 Mongolia - how to stop the HCV epidemic?
30
Mongolia

31
Mongolia - latest actions
• New guidelines for treatment of HCV approved
• 100 “Hep-C frontline” doctors trained (in capital & 21 provinces)
» SOF + LDP roll-out expected Nov 2015 ($400/month)
» Generic tenofovir now available $25/m for HBV+ pregnant women
• Dialogue on financing options for hepatitis care & treatment
» Standard package of services for hep C and B?
» Economic analysis of hep C and B care and treatment
• Discussing new National programme on viral hepatitis (not only HCV)
• Website to link providers, patients, labs and the NCCD for hepatitis screening, care and treatment patients.
18/07/2015 Mongolia - how to stop the HCV epidemic? 31

• Team building & teamwork – Ministry of Health Brazilian Health Surveillance Agency (Anvisa) Secretariat of Health Surveillance (SVS/MS) Secretariat of Science, Technology and Strategic Inputs (SCTIE/MS) – Organized Civil Society, – Healthcare providers
GOAL
TREAT 60,000 PEOPLE IN THE NEXT TWO YEARS.
Lessons Learned in Decision Making

Perspectives July 2015 Onward
Sustained Virological Response (SVR)
Population with Treatment Recommended
Treatments/year
PR/PR+BOC/TEL (2013-2015)
INTERFERON-FREE SOF+DAC/SIM
(2015-) 40%
15.000
F3/F4 (F2)*
>90%
F3/F4 (F2), HIV, Pr/P Tx... 30.000

1. New funding for HCV treatment to be established at either national or international level, to allow large drug orders to be made, and these economies of scale to be achieved.
2. Clear and transparent treatment access policies with voluntary licensing, from all companies making DAAs (BMS, Merck, AbbVie)
3. Feasibility studies of DAA combinations in LMICs to prove this can be done cheaply
4. Low cost point of care tests to monitor viral load or antigen
What needs to happen?

Cycle of Action
ADVOCACY
Action
Awareness
Priority
Funding
Response & Data

36
In the next 25 years, HCV can be eliminated
New HCV Infections
Cured Mortality
New HCV Infections
Cured Mortality
Today Future
