fmt: can we cure obesity and insulin resistance? max nieuwdorp md phd internist-endocrinologist dept...
TRANSCRIPT

FMT: Can we cure obesity and insulin resistance?
Max Nieuwdorp MD PhD
Internist-endocrinologist
Dept of Vascular Medicine Amsterdam
Wallenberg Laboratory, Gothenberg, Sweden
session Panacea or Pandora’s Box 17th august 2014: 0840-0905am

Disclosure slide
• Scientific advisory board Seres Health
• Founder Caelus pharmaceuticals

Take home message• Decreased butyrate producing bacteria in obesity
associated with malign obesity and insulin resistance
• FMT incudes changes in (small) iIntestinal microbiota and affects insulin resistance (but it is not a panancea)
• Using FMT as a working model can derive novel probiotics on top of current treatment for insulin resistance

Intestinal microbiota in obesity and MetSyn

Benign vs malign obesity• 66% metabolically
healthy obese
• 34% insulin resitance and DM2
• Low grade inflammation involved Samocha-bonet et al, obesity Reviwws 2014.

Gut microbiota and obesity/type 2 diabetes mellitus
Qin, Nature 2012
Le Chatelier, Nature 2013
Karlsson, Nature 2013
Ridaura, Science 2013

Diagnostic and clinical value of gut microbiota composition in Dm2
• Reduced short-chain fatty acid butyrate producers (Roseburia species and Faecalibacterium prausnitzii) in DM2
• Enrichment of Lactobacillus gasseri and Streptococcus mutans in fecal sample has predictive value for developing insulin resistance
Karlsson, Nature 2013

Results of these cohort based studies using fecal samples
Smits/Nieuwdorp, Gastroenterology 2013 [in press]
F prausznitzii lower
Ruminococcus lower

Major disadvantages of current fecal sample centered approach
• 1. Small intestine is more involved
in metabolism than the colon
• 2. Association is not causality!
• 3. Sequencing vs culturing bacteria

Hartstra/nieuwdorp, Diabetes Care 2014. pH dictates bacterial survival and gutmicrobiota composition

Koch’s postulatesfor causality
• The microorganism must be identified/isolated from a diseased organ(ism).
• The microorganism should be associated with
disease (association/intervention).
• The cultured microorganism should induce beneficial or adverse effects when introduced into an organism (inoculation).

Manipulating gut microbiota by fecal transplant

Van Nood, NEJM 2013
Effects of fecal transplantations in clostridium difficile diarroea

Gutmicrobiota Diversity in Cdiff After FMT
Correction of Low Diversity of Patients by Transplantation
Diverse Community Stably Maintained for Over 2 Months

FMT Randomized controlled trials performed at AMC
• Since 1958 casereport by Eiseman, at least 4500 patients treated worldwide with donor feces (since 2007 at AMC),
• RCT superiority of fecal Tx in clostridium difficile diarrhea and MetSyn
• At AMC ongoing/finished RCT’s for:
-IBD (Colitis ulcerosa, TURN trial)
- insulin resistance
-NAFLD/NASH
• Long term side effects not seen yet
Smits/Nieuwdorp, Gastroenterology 2013 [in press]; van Nood/Nieuwdorp, NEJM 2013

• No adverse effects!
• No effect on weight 6 weeks after lean donor FMT
A.Vrieze, Gastroenterology 2012

Effect donor faeces on periferal insulin sensitivity
A.Vrieze, Gastroenterology 2012
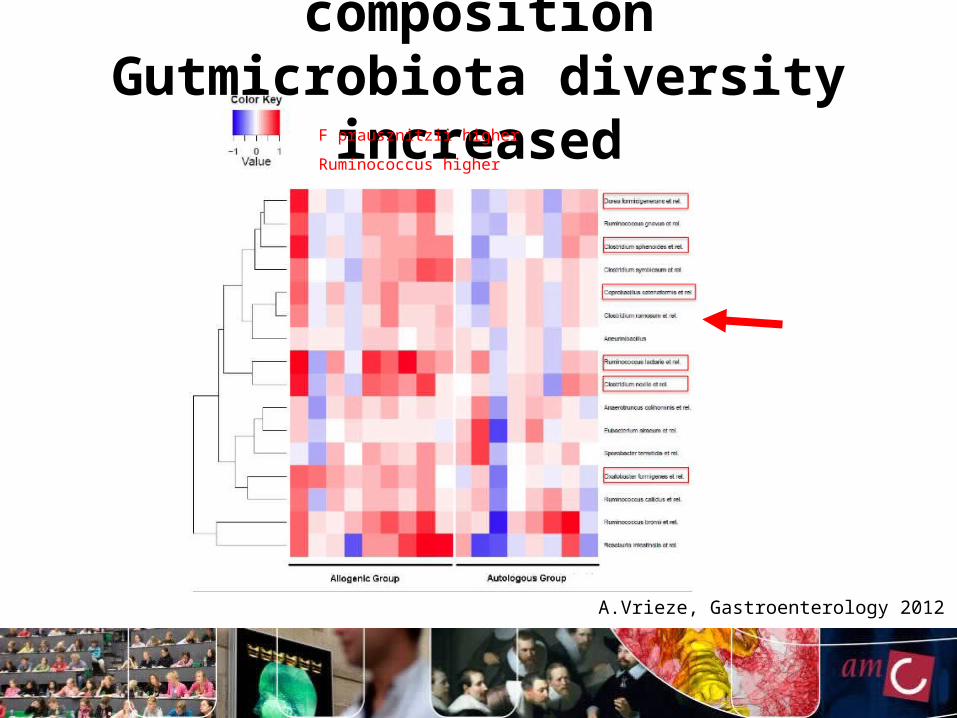
Fecal gut microbiota compositionGutmicrobiota diversity increased
A.Vrieze, Gastroenterology 2012
F prausznitzii higher
Ruminococcus higher
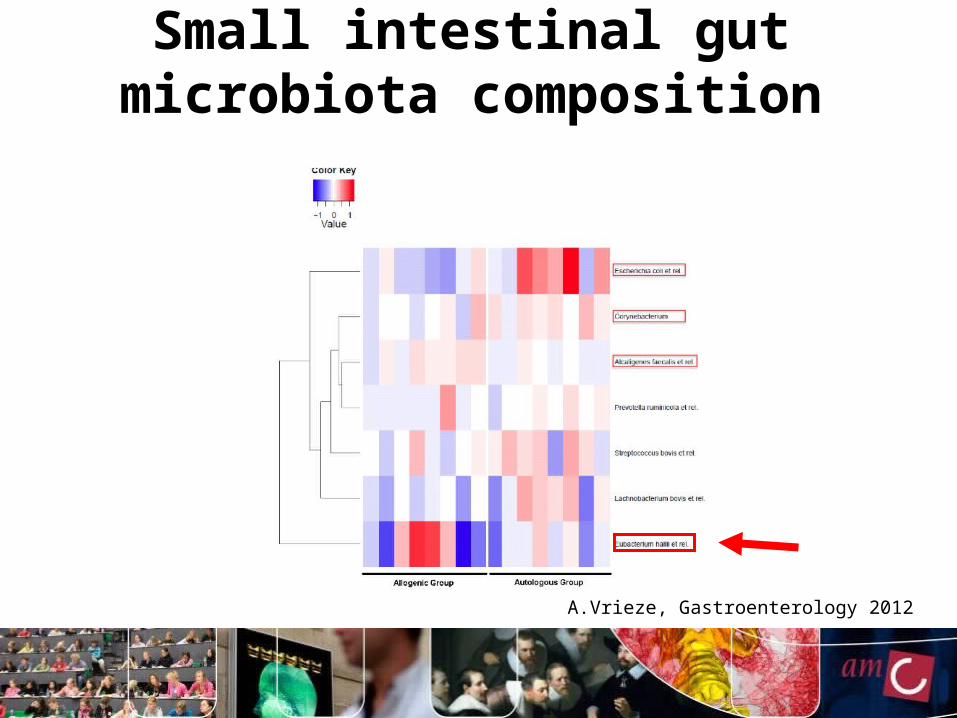
A.Vrieze, Gastroenterology 2012
Small intestinal gut microbiota composition

Koch’s postulates
Eiseman (Surgery 1958)
• Fecal transplant doesn’t induce a definate cure!
• The cultured microorganism should induce beneficial or adverse effects when introduced into a healthy organism (3rd postulate)
• Concentrations of Eubacterium hallii in small intestinal biopsies correlated significantly with improved insulin sensitivity upon lean donor Fecal Tx

Manipulating gutmicrobiota by Eubacterium hallii : effect on
insulin resistance

Eubacterium hallii• belongs to Firmicutes phylum (spore
former)• Anaerobic gram positive lactate-utilizing
SCFA butyrate- producing bacterial strain
• Can produce butyrate at pH 5-6 (small intestine) as well as at pH 6-7 (colon)
• Sensitive to vancomycine

Studyprotocol I • Db/db male mice (8 weeks old), n=8 per group
• Daily gavage (100ul/mouse) with E. Hallii (stored in 10% glycerol at -80C), gavage within 1 hour after thawing for 4 weeks with: -10^6 CFU/ml
- 10^8 CFU/ml
- 10^10 CFU/ml
- placebo (dissolvens = 10% glycerol)
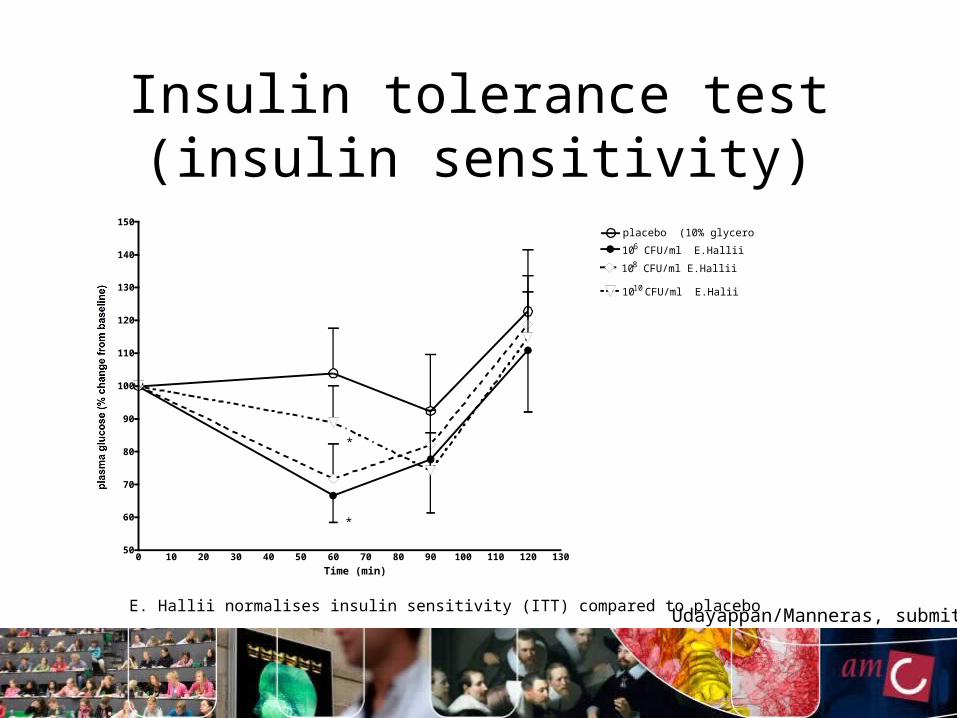
Insulin tolerance test (insulin sensitivity)
E. Hallii normalises insulin sensitivity (ITT) compared to placebo
0 10 20 30 40 50 60 70 80 90 100 110 120 13050
60
70
80
90
100
110
120
130
140
150placebo (10% glycerol)
106 CFU/ml E.Hallii
1010 CFU/ml E.Halii
108 CFU/ml E.Hallii
*
*
Time (min)
Udayappan/Manneras, submitted

Gutmicrobiota analyses: Ehallii treatment significantly increases
Ehallii in cecum
Mean ±SEM

Studyprotocol II • Db/db male mice (8 weeks old), n=7-9 per group
(Gothenborg university, Sweden)
• Daily gavage (100ul/mouse) with alive or heat inactivated E. Hallii 10x6CFU/ (stored in 10% glycerol at -80C), gavage within 1 hour after thawing for 4 weeks followed by:
• -48h in Metabolic cages (Somedic cages)
- hyperinsulinemic normoglycemic clamp

Effect E. Halli on food intake and bodyweight
Udayappan/Manneras, submitted

10^8 E.hallii treatment significantly increases E.halli in cecum
P<0.05
Udayappan/Manneras, submitted

Active E. Hallii treatment significantly increases verruco bacteria, cyanobacteria, deferribacteres and fusobacteria
* Significant p<0.05Mann Whitney UCyanobacteria: p=0.015(2-
tailed), .007 (1-tailed)
Deferribacteres: p=0.028 (2-tailed), .0014 (1-tailed)
Fusobacteria: p=0.028 (2-tailed), .0014 (1-tailed)
Verrucomicrobia: p=0.028 (2-tailed), .0014 (1-tailed)
Red: E hallii 10x8CUF
Green: plaecbo

Resting energy increased upon E. hallii
Mean ±SEM
Udayappan/Manneras, submitted

*
Per
iphe
ral i
nsul
in s
ensi
tivity
Udayappan/Manneras, submitted
Insulin sensitivity (clamp) increased upon E. hallii

Mean ±SEM
E. hallii increases fecal secondary bile acids

Mean ±SEM
Ehallii treatment: effect on fecal SCFA
P<0.05

E.Halli as novel therapeutic in in insulin resistance?
• Has beneficial effects on insulin sensitivity
• Potential mechanism via bileacids and brown fat (Increased Energy Expenditure)
• Human intervention phase 1 dosefinding trial with E.hallii curently ongoing at AMC
•
De Vos WM and Nieuwdorp M. Nature 2013; 498(7452):48-9
Eubacterium hallii

Take home message• Decreased butyrate producing bacteria in obesity
associated with malign obesity and insulin resistance
• FMT incudes changes in (small) iIntestinal microbiota and affects insulin resistance (but it is not a panancea)
• Using FMT as a working model can derive novel probiotics on top of current treatment for insulin resistance

Acknowledgments
Willem de Vos WUR/Helsinki
Mireille Serlie MD PhD AMC
Ruud Kootte MDFleur van der Valk, MDPim Gilijamse, MDLoek Smits, MDSophie Bernelot Moens, MDMara Sandberg, MDKristien Bouter, MScPieter de Groot, MDAnnick Hartstra MD
Han Levels PhDGeesje Dallinga, PhDAlinda Schimmel, Bsc
Anne Vrieze MD PhD
AMC
Fredrik backhedGothenborg
Louise Manneras
Shanti Udayappan
Erik Stroes AMCHans Romijn
AMC