transfusion medicine for the internist
TRANSCRIPT

Transfusion Medicine for Internist
By
Hematology/Oncology Division
UAMS

Goals
• Basics of blood grouping and typing
• Recognizing transfusion reactions
• Blood components-Indications and contraindications
• Special blood products
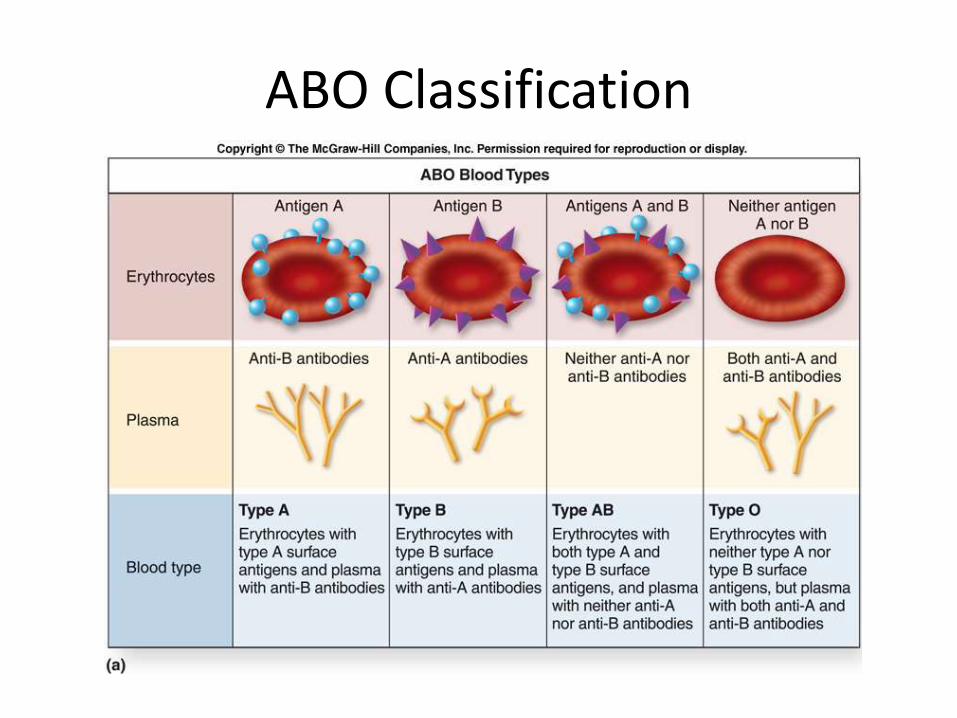
ABO Classification

ABO
• Anti-A and Anti-B antibodies (isohemagglutinins)
– IgM subtype
– Present in plasma
– Present in blood without exposure to A or B antigens
– Efficient at fixing complement
– Intravascular hemolysis with ABO mismatch
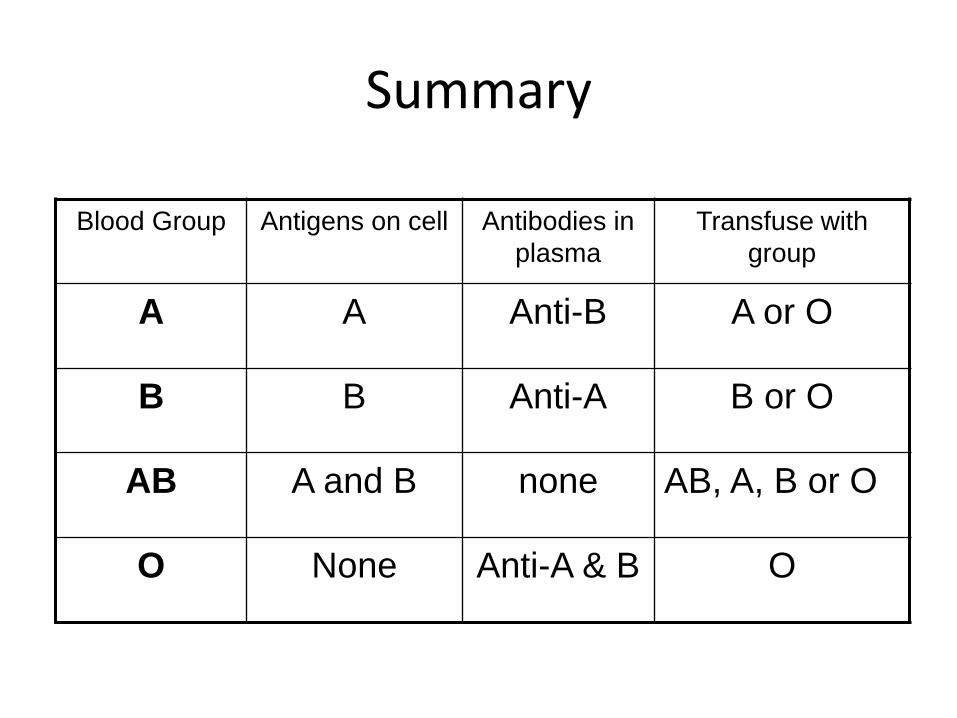
Summary
Blood Group Antigens on cell Antibodies in
plasma
Transfuse with
group
A A Anti-B A or O
B B Anti-A B or O
AB A and B none AB, A, B or O
O None Anti-A & B O

ABO/Rh distribution
ABO Type Rh Percentage
O Positive 37.4%
O Negative 6.6%
A Positive 35.7%
A Negative 6.3%
B Positive 8.5%
B Negative 1.5%
AB Positive 3.4%
AB Negative 0.6%
Stanford School of Medicine Blood Center 2008

Variations
• Variable strength of expression of ABO
– Weak A (A2)
– can develop antibodies to common A (A1)
– Usually only bind at nonphysiologic temperatures
– If reactive at 37⁰C, patient should only receive type A2 or type O blood
– Variations occur in type B but are rare
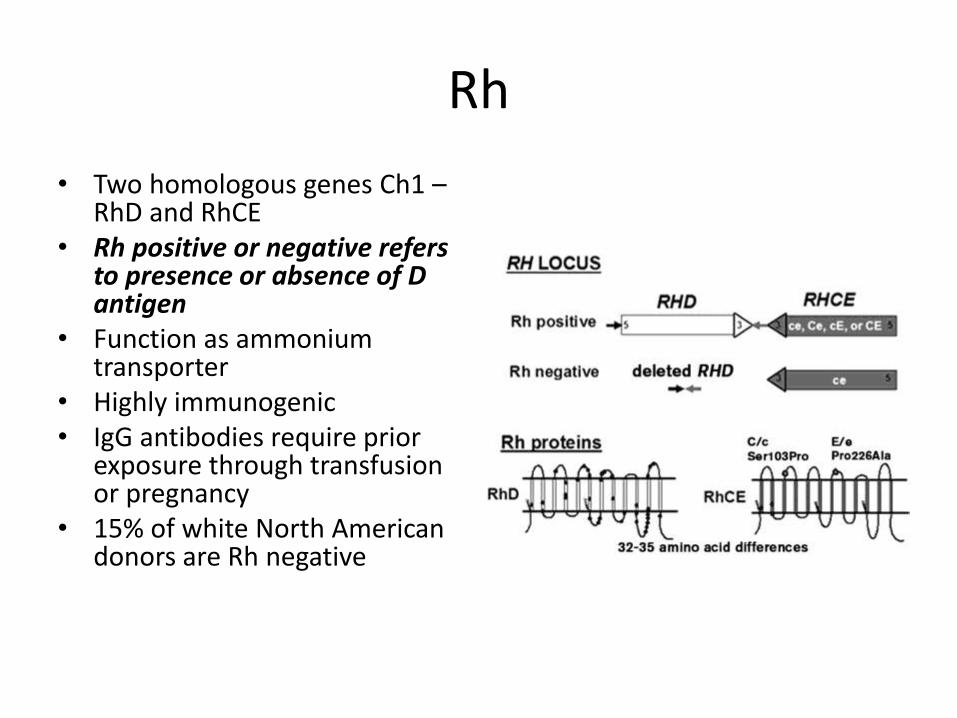
Rh
• Two homologous genes Ch1 –RhD and RhCE
• Rh positive or negative refers to presence or absence of D antigen
• Function as ammonium transporter
• Highly immunogenic• IgG antibodies require prior
exposure through transfusion or pregnancy
• 15% of white North American donors are Rh negative

Rh Variants
• Weak D– Quantitative reduction in D antigen expression– Can be considered Rh positive
• Partial D– Qualitative change in D antigen usually from
recombination with C/E gene locus– Can test as Rh positive but make alloantibodies to D
antigen– Transfuse with Rh negative blood products and give
RhD immune globulin to prevent hemolytic disease of newborn
Other antigen systems
Kell, Kidd, Duffy, and MNS systems
• Duffy glycoprotein also serves as a receptor for the malarial parasite Plasmodium vivax
• Antigens M and N critical to the invasion of RBCs by Plasmodium falciparum
Lewis,P and I antigen system
• P antigen: Donath-Landsteiner antibodies(cold-reacting IgGautoantibodies) directed against the P antigen can fix complement on circulating RBCs resulting in intravascular hemolysis PCH
• The Lewis antigenH pylori receptor
• The I antigen: responsible for IgM-mediated autoimmune hemolytic anemia (AIHA; cold agglutinin disease)
Case 1
A 26-year-old G2P1 woman with blood group O positive gives birth to a healthy term infant with blood group B positive. Antibody screen is negative in the infant and mother. A direct antiglobulin test is positive in the infant, and a follow-up elution test demonstrates reactivity with type B reagent RBCs. From birth to 11 hours post-delivery, the infant's bilirubin level increases from 8.1 mg/dL to 16.7 mg/dL;(predominantly unconjugated)and then to 18.9 mg/dL 21 hours post-delivery.
• Which of the following is the most appropriate blood component to use for exchange transfusion?
• A. Type O, RhD negative or positive whole blood
• B. Type B, RhD negative or positive whole blood
• C. Type O, RhD negative or positive red blood cells, and type AB plasma combined to the desired hematocrit
• D. Type B, RhD negative or positive red blood cells, and type AB plasma combined to the desired hematocrit

Pretransfusion Testing
• Type and Screen performed prior to selecting a compatible unit
• Two tests to determine a patients blood type
– Forward typing
• Patient RBCs mixed with anti-A or anti-B IgM
– Reverse typing
• Patient serum mixed with known type A or type B red cells
• Indirect anti globulin (Coombs) test

Pretransfusion Testing
• Type and Cross performed to ensure compatibility with selected units
• If type and screen is negative and no history of antibodies– Mix patient’s serum with selected PRBC unit prior to transfusion
• If type and screen is positive or history of antibodies– Mix patient’s serum with selected PRBC unit incubate at 37
deg C– Wash and suspend in Coombs reagent( antibody to human
IgG)look for agglutination– Ensures that the antibodies present are not reactive to donor
RBCs
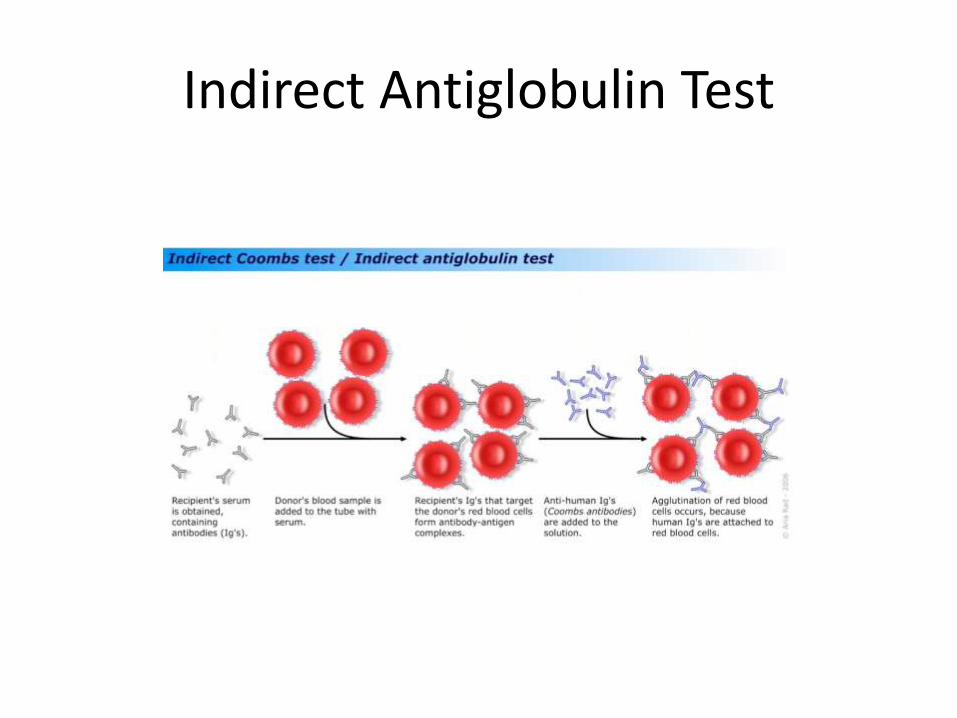
Indirect Antiglobulin Test
Transfusion reactions
• Acute reactions (minutes hours)
– Immunologic
– Non-immunologic
• Delayed reactions (days weeks)
– Immunologic
– Non-immunologic

Transfusion reactions
Case 2
57 y/o man presents to the ER with 1 day history of BRBPR, colonoscopy reveals a 7x7 cms mass in the rectum. The next day Hb dropped to 6.3, and 2 Units of RBCs are ordered. After 15 minutes of blood transfusion, patient gets fever (39C )and chills ,complains flank pain, starts oozing blood from mouth and peripheral line and soon becomes hypotensive. Labs reveals Hbof 5, low fibrinogen, elevated D dimer and prolong PT and PTT. He has a positive direct antiglobulin test(DAT)
What is the most likely diagnosis?
Case 2
57 y/o man presents to the ER with 1 day history of BRBPR, colonoscopy reveals a 7x7 cms mass in the rectum. The next day Hb dropped to 6.3, and 2 Units of RBCs are ordered. After 15 minutes of blood transfusion, patient gets fever (39C )and chills ,complains flank pain, starts oozing blood from mouth and peripheral line and soon becomes hypotensive. Labs reveals Hbof 5, low fibrinogen, elevated D dimer and prolong PT and PTT. He has a positive direct antiglobulin test(DAT)
What is the most likely diagnosis?
Acute hemolytic transfusion reaction
Case 2
57 y/o man presents to the ER with 1 day history of BRBPR, colonoscopy reveals a 7x7 cms mass in the rectum. The next day Hb dropped to 6.3, and 2 Units of RBCs are ordered. After 15 minutes of blood transfusion, patient gets fever (39C )and chills ,complains flank pain, starts oozing blood from mouth and peripheral line and soon becomes hypotensive. Labs reveals Hbof 5, low fibrinogen, elevated D dimer and prolong PT and PTT. He has a positive direct antiglobulin test(DAT)
What is the most likely diagnosis?
Acute hemolytic transfusion reaction

Acute Hemolytic Transfusion Reaction
• Mechanism– Incompatible donor
RBCs coated with recipient serum IgMantibodies that fix complement leading to intravascular hemolysis.
– Release of cytokines such as TNF results in fever and chills
– DAT is positive for IgGand complement

Acute hemolytic transfusion reaction
• Timing: first 15 minutes, but usually before end of transfusion
• Fever and chills (> 80%)
• Back or infusion site pain
• Hypotension/shock
• Hemoglobinuria
• DIC/increased bleeding
• Sense of “impending doom”

Acute Hemolytic Transfusion Reaction
• Management
– STOP transfusion
– Hydration to maintain urine output >100 cc/hr
– Diuresis with Mannitol to prevent renal failure
– Vasopressors if needed for hypotension
– DIC – FFP, platelets, cryoprecipitate as needed

Case 3
62 y/o woman with AML s/p 7 + 3,on D16WBC 0.3, Hb 8, and plat 5. On call resident ordered platelet transfusion.After a few minutes of the platelet transfusion patient complaints of chills, 1 hour later Temperature is found to be 38.3.BP is 110/90, HR 90, RR 18.On exam,no skin rash, no stridor, no wheezing. Labs: Plat 30, indirect billirubin, LDH, haptoglobin and direct antiglobulintest are negative.
• What is the most likely diagnosis?

Case 3
62 y/o woman with AML s/p 7 + 3,on D16WBC 0.3, Hb 8, and plat 5. On call resident ordered platelet transfusion.After a few minutes of the platelet transfusion patient complaints of chills, 1 hour later Temperature is found to be 38.3.BP is 110/90, HR 90, RR 18.On exam,no skin rash, no stridor, no wheezing. Labs: Plat 30, indirect billirubin, LDH, haptoglobin and direct antiglobulintest are negative.
• What is the most likely diagnosis?
Febrile non-hemolytic transfusion reaction

Febrile non-hemolytic transfusion reactions
• Most frequently reported reaction• Transient fever and chills (+/- rigors) during or up to 2 hours
after transfusion• Cause: Increased pyrogenic substances (e.g., TNF-α, IL-1β,
IL-6), mostly from WBCs• More common in platelet transfusions• Incidence decreased since “universal” leukoreduction (0.1
to <1%)• Differential diagnosis: acute HTR and transfusion-related
sepsis• Labs: negative hemolysis workup (diagnosis of exclusion)

Febrile non-hemolytic transfusion reactions: treatment and prevention
• Treatment
– Antipyretics (acetaminophen)
– Meperidine (Demerol) for more severe chills
• Prevention
– Premedication: Acetaminophen
– Leukocyte reduction works extremely well to prevent vast majority of these reactions.
Case 4
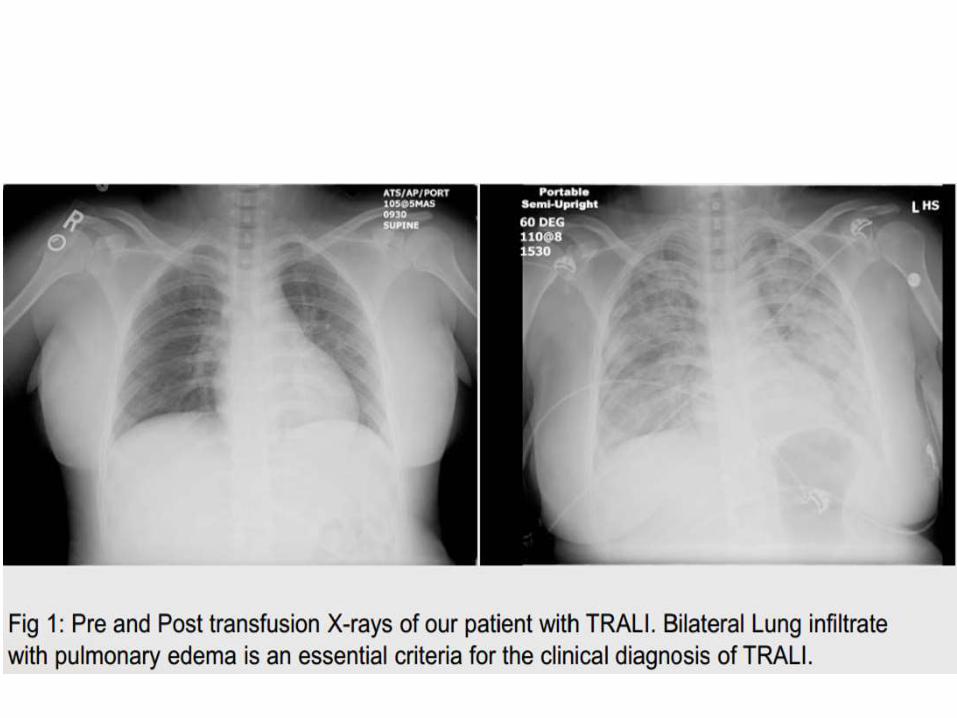
• 50 y/o woman with chronic atrial fibrillation, on coumadin, was admitted for emergent laparoscopic appendectomy.45 minutes after completing the transfusion of 5 units of FFP, the patient developed fever (37.0°C to 38.1°C), relative hypotension (128/60 to 100/50) and severe respiratory distress with RR of 30/min and a SPO2 of 81% requiring intubation and mechanical ventilation.She was treated with a single dose of hydrocortisone. A post-intubation CXR showed bilateral diffuse infiltrates with "white out" of lungs. The fever and hypotension resolved without further treatment.
• What is the most likely diagnosis?

Case 4
• 50 y/o woman with chronic atrial fibrillation, on coumadin, was admitted for emergent laparoscopic appendectomy.45 minutes after completing the transfusion of 5 units of FFP, the patient developed fever (37.0°C to 38.1°C), relative hypotension (128/60 to 100/50) and severe respiratory distress with RR of 30/min and a SPO2 of 81% requiring intubation and mechanical ventilation.She was treated with a single dose of hydrocortisone. A post-intubation CXR showed bilateral diffuse infiltrates with "white out" of lungs. The fever and hypotension resolved without further treatment.
• What is the most likely diagnosis?
Transfusion-related acute lung injury (TRALI)
Case 4
• 50 y/o woman with chronic atrial fibrillation, on coumadin, was admitted for emergent laparoscopic appendectomy.45 minutes after completing the transfusion of 5 units of FFP, the patient developed fever (37.0°C to 38.1°C), relative hypotension (128/60 to 100/50) and severe respiratory distress with RR of 30/min and a SPO2 of 81% requiring intubation and mechanical ventilation.She was treated with a single dose of hydrocortisone. A post-intubation CXR showed bilateral diffuse infiltrates with "white out" of lungs. The fever and hypotension resolved without further treatment.
• What is the most likely diagnosis?
Transfusion-related acute lung injury (TRALI)
TRALI
• Incidence varies widely: 1:1200 to 1:190,000 transfusions• Currently the #1 cause of transfusion-related fatality in the
US! • Occurs within 6 hours of transfusion, most commonly
within 2 hours• Mortality 6-10%• Mechanism
– Antineutrophil antibodies or anti HLA antibodies between donor and patient react in lung vasculature
– Donor antibodies most common particularly from multiparouswomen
– Alternative: Primed leukocytes in recipient due to underlying illness react to cytokines or lipids from donor

TRALI
• Definition: – New acute lung injury within 6 hours of a transfusion,– Hypoxemia with PaO2/FiO2 < 300 mm Hg (or O2 sat
<90%) and bilat CXR infiltrates– Lack of other risk factors for pulmonary edema– No pre-existing acute lung injury– Usually also with fever, chills, transient hypertension
then hypotension
• Platelets/plasma transfusions most often implicated with TRALI, but also with RBCs/whole blood

TRALI: Differential diagnosis
• ARDS: TRALI may look exactly like ARDS, but TRALI usually resolves in 24-48 hours
• TACO: -TRALI is usually associated with fever (unlike TACO)-No evidence of volume overload (no JVD, normal
wedge pressure, normal BNP levels)-No response to diuretics-May become hypotensive-Positive anti-HLA and/or anti-neutrophil antibodies
• Anaphylactic reactions (generally afebrile)• Acute pulmonary edema due to other causes
TRALI: Treatment/Prevention
• Treatment:– Supportive care (O2 , intubation)– Mortality reported between 5 and 25%– 80% recover quickly
• Prevention– Implicated donors (with antibodies found) should be
deferred from donation– Use of male plasma has been shown to decrease the risk
of TRALI (females have more anti-HLA and anti-neutrophil antibodies because of pregnancy).
– Some centers have begun testing multiparous female PLT donors for anti-HLA +/- neutrophil antibodies and deferring those who have antibodies

TACO: treatment
• Treatment:
– Stop the transfusion, evaluate, sit patient up
– Supplemental oxygen
– Diuretics to decrease blood volume
• Prevention in at-risk patients
– Control infusion rates (1 mL/Kg/hour).
– Consider lower volume units.
– Diuretics in between units
Case 5
• 24 year-old woman is admitted for abnormal uterine bleeding. Hb was found to be 5.5 and so two units of packed RBC's were ordered. She developed urticarial rash and soon developed hoarseness of voice and facial edema.BP remained stable.She was immediately treated with 25 mg of IV Benadryl with resolution of her symptoms.
• What is the most likely diagnosis?

Case 5
• 24 year-old woman is admitted for abnormal uterine bleeding. Hb was found to be 5.5 and so two units of packed RBC's were ordered. She developed urticarial rash and soon developed hoarseness of voice and facial edema.BP remained stable.She was immediately treated with 25 mg of IV Benadryl with resolution of her symptoms.
• What is the most likely diagnosis?
Allergic reaction
Case 5
• 24 year-old woman is admitted for abnormal uterine bleeding. Hb was found to be 5.5 and so two units of packed RBC's were ordered. She developed urticarial rash and soon developed hoarseness of voice and facial edema.BP remained stable.She was immediately treated with 25 mg of IV Benadryl with resolution of her symptoms.
• What is the most likely diagnosis?
Allergic reaction(Mild)
Allergic reactions
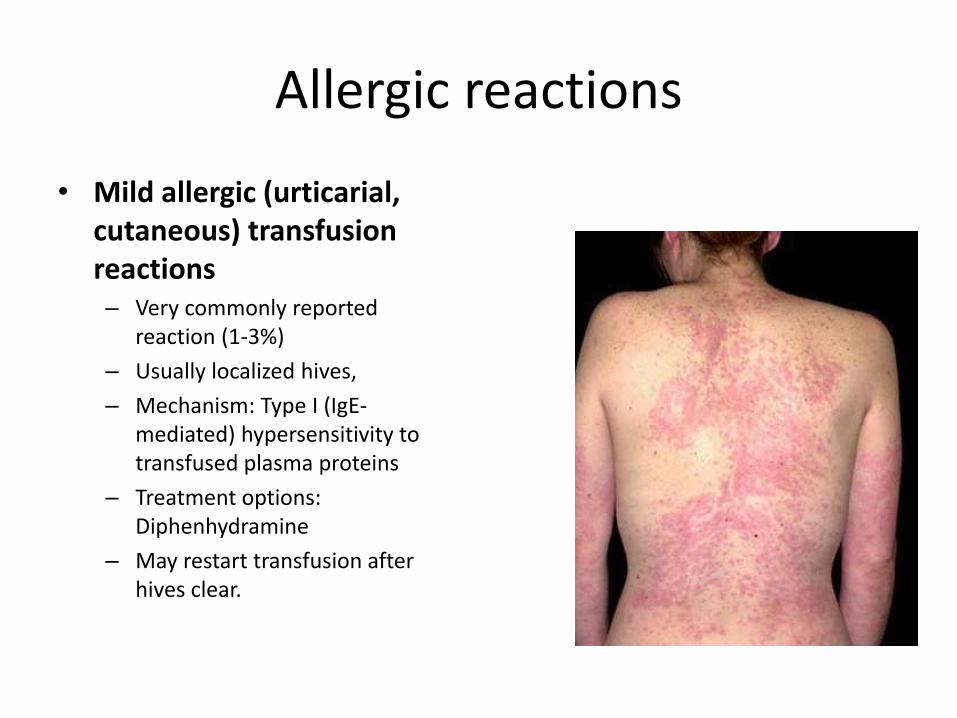
• Mild allergic (urticarial, cutaneous) transfusion reactions– Very commonly reported
reaction (1-3%)
– Usually localized hives,
– Mechanism: Type I (IgE-mediated) hypersensitivity to transfused plasma proteins
– Treatment options: Diphenhydramine
– May restart transfusion after hives clear.

Allergic reactions
• Moderate allergic (anaphylactoid) transfusion reactions– May present with upper/lower airway obstruction +/–
cutaneous manifestations (Stridor, hoarseness, “lump” in throat, Wheezing, chest tightness, dyspnea)
• Severe allergic (anaphylactic) transfusion reactions– Uncommon (1:20,000 to 50,000 transfusions)– Anaphylactic shock very early in the transfusion– Lower airway obstruction– Most patients have skin findings (urticaria, angioedema,
generalized pruritis)– Classic history: IgA deficient recipient who has formed an anti-
IgA of the IgE class – Latex, drugs, foods in donors can lead to severe reactions in
susceptible recipients.

Case 6
A 74 yo patient with leukemia received 2 units of RBCs. Approximately 1 hour after transfusion, he developed chills, and a temperature of 102.9ºF (39.4ºC) and became hypotensive.Thepatient's blood cultures grew Yersinia enterocolitica. The same organism was cultured from the leftover RBC unit bag.
What is this?

Case 6
A 74 yo patient with leukemia received 2 units of RBCs. Approximately 1 hour after transfusion, he developed chills, and a temperature of 102.9ºF (39.4ºC) and became hypotensive.Thepatient's blood cultures grew Yersinia enterocolitica. The same organism was cultured from the leftover RBC unit bag.
What is this?
Transfusion-related sepsis

Transfusion-related sepsis
• More often seen with RBC transfusions (occur within the first few minutes of transfusion)
• Rapid onset high fever (often greater than 4F/2C)
• Shaking chills• Abdominal cramping,
nausea/vomiting• Hypotension/shock• DIC• Differential diagnosis: acute HTR ,
anaphylactic transfusion reaction, and febrile nonhemolytictransfusion reaction

Transfusion-related sepsis
• Most contaminated products that cause reactions are closer to their expiration date
• Organisms identified depend on product.
– Red cells: Gram-negative rods (endotoxin-makers that like growing in cold temperatures) Yersinia enterocolitica (most common historically), E. coli, Enterobacter/Pantoea sp, Serratia marcescens and liquifaciens, Pseudomonas species. Gram-positive cocci (much less commonly) Staph. Epidermidis, Staph aureus
– Platelets: Vast majority are gram-positive cocci, Gram negative rods can also contaminate and are much more likely to cause fatalities.
– Plasma products: Uncommonly contaminated

Transfusion Associated Infections
• Donated blood is tested for– HIV
– Hepatitis B and C
– HTLV I and II
– West Nile Virus
– Syphilis
– Chagas (Trypanosoma cruzi)
• Donors are screened by questionnaire for– CJD, Malaria, Babesiosis, Lyme disease

Transfusion Associated Infections
Virus Risk Per Transfusion
HIV 1 and 2 1:2,000,000-3,000,000
Hepatitis C 1:2,000,000-3,000,000
Hepatitis B 1:200,000-500,000
HTLV I and II 1:2,000,000
West Nile Virus Seasonal and regional variability, none since 2005

Case 7
21 yo woman presents to the ED with abdominal pain, nausea, and vomiting 7 days after spinal fusion surgery. The recent surgery had been complicated by blood loss requiring 8 units of PRBCs. On preoperative testing, the patient's blood type was A positive, with a negative antibody screen. PE in the ED reveals a HR of 120 and Temp of 100.6° F. Her hemoglobin dropped to 8.9 g/dL (post-op day seven) and 6.8 g/dL (post-op day nine) from 11.2 g/dL(prior discharge HGB)with no evidence of bleeding on imaging studies of the abdomen and pelvis. Reticulocyte count was 4.2%. Total bilirubin increased to 2.4 mg/dL and LDH elevated at 593 U/L (reference range: 100-220 U/L).A new type and screen on post-op day eight was A positive with a positive antibody screen or indirect antiglobulin test (IAT).
What is the most likely diagnosis?

Case 7
21 yo woman presents to the ED with abdominal pain, nausea, and vomiting 7 days after spinal fusion surgery. The recent surgery had been complicated by blood loss requiring 8 units of PRBCs. On preoperative testing, the patient's blood type was A positive, with a negative antibody screen. PE in the ED reveals a HR of 120 and Temp of 100.6° F. Her hemoglobin dropped to 8.9 g/dL (post-op day seven) and 6.8 g/dL (post-op day nine) from 11.2 g/dL(prior discharge HGB)with no evidence of bleeding on imaging studies of the abdomen and pelvis. Reticulocyte count was 4.2%. Total bilirubin increased to 2.4 mg/dL and LDH elevated at 593 U/L (reference range: 100-220 U/L).A new type and screen on post-op day eight was A positive with a positive antibody screen or indirect antiglobulin test (IAT).
What is the most likely diagnosis?
Delayed hemolytic transfusion reactions (DHTRs)

Case 7
21 yo woman presents to the ED with abdominal pain, nausea, and vomiting 7 days after spinal fusion surgery. The recent surgery had been complicated by blood loss requiring 8 units of PRBCs. On preoperative testing, the patient's blood type was A positive, with a negative antibody screen. PE in the ED reveals a HR of 120 and Temp of 100.6° F. Her hemoglobin dropped to 8.9 g/dL (post-op day seven) and 6.8 g/dL (post-op day nine) from 11.2 g/dL(prior discharge HGB)with no evidence of bleeding on imaging studies of the abdomen and pelvis. Reticulocyte count was 4.2%. Total bilirubin increased to 2.4 mg/dL and LDH elevated at 593 U/L (reference range: 100-220 U/L).A new type and screen on post-op day eight was A positive with a positive antibody screen or indirect antiglobulin test (IAT).
What is the most likely diagnosis?
Delayed hemolytic transfusion reactions (DHTRs)

Delayed hemolytic transfusion reactions (DHTRs)
• Hemolysis occurring >24 hours but < 28 days after transfusion.
• Physiopathology
– Patient exposed to non-ABO red cell antigen not present on own RBCs
– Antibody is formed but fades from detection over time
– Patient is re-exposed to antigen in a future transfusion
– Anamnestic rapid production of IgG antibody vs. target antigen
– IgG antibodies coat red cells and lead to their removal in the liver/spleen
– Peripheral smear will commonly show spherocytes
– This mechanism is typical for Kidd, Duffy, Kell antibodies

Transfusion-associated graft-vs-host disease (TA-GVHD)
• A nearly-always fatal transfusion complication resulting from an attack on recipient cells by viable T-lymphocytes in a transfused blood product

TA-GVHD: The normal response
• Transfused T- lymphocytes (CD4, CD8, and NK cells) mount an immune response against foreign HLA host tissues
• Normally, host lymphocytes counterattack and neutralize the response
• Lack of host neutralization may lead to TA-GVHD, with continued T-lymphocyte attack on host tissues

TA-GVHD: signs and symptoms
• Almost uniformly fatal, but thankfully rare
• Patients present with:
– Fever 7-10 days post-transfusion
– Face/trunk rash that spreads to extremities
– Mucositis, nausea/vomiting, watery diarrhea
– Hepatitis
– Pancytopenia and subsequent marrow aplasia → most patients dying from overwhelming infections


Patients at-risk for TA-GVHD
• Immunosuppressed patient:
– DiGeorge’s, SCID, Wiskott-Aldrich.
– Stem cell transplant recipients
– Patients receiving chemo that attack T-cells (Fludarabine, purine analogs)
– Aplastic anemia patients
– Hodgkins seems to have an inherent cellular immune defect
– Patients with solid tumors getting intensive chemotherapy/radiation
• Intrauterine transfusions, premature neonatal transfusions, and neonatal exchange transfusions
• Granulocyte transfusion recipients (Viable, fresh T-lymphocytes)
• Patients probably NOT at risk: Solid organ transplant recipients, term neonates, AIDS, patients getting FFP or cryo.

TA-GVHD: prevention
• Radiation is used to deactivate the T-lymphocytes in transfused blood products (2500 cGy )
• Leukocyte reduction may not work.
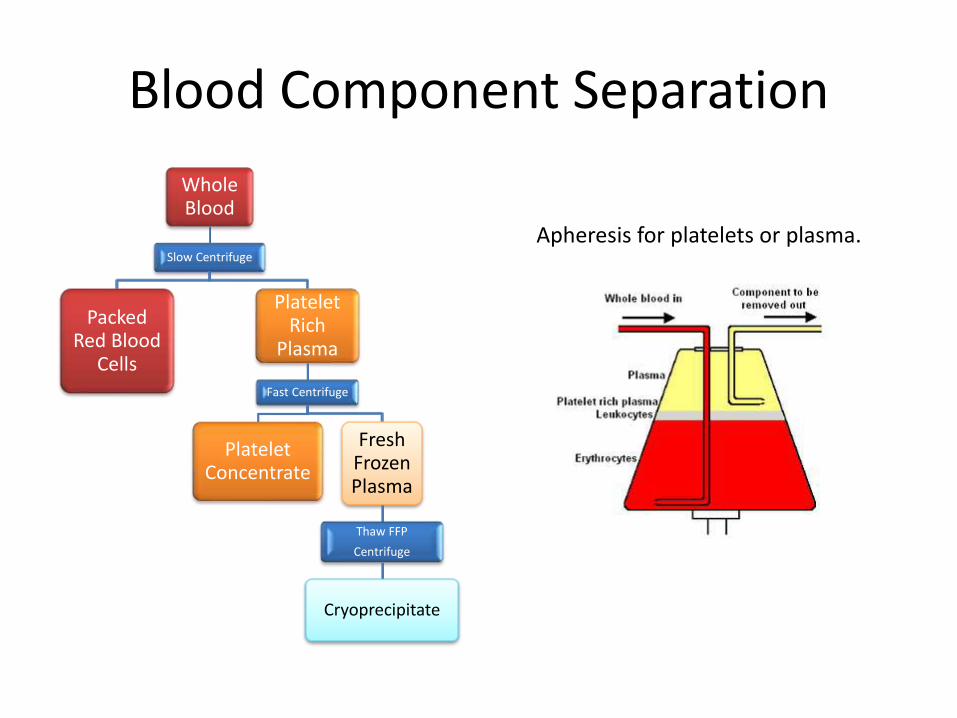
Blood Component Separation
Whole Blood
Slow Centrifuge
Packed Red Blood
Cells
Platelet Rich
Plasma
Fast Centrifuge
Platelet Concentrate
Fresh Frozen Plasma
Thaw FFP
Centrifuge
Cryoprecipitate
Apheresis for platelets or plasma.

Packed Red Blood Cells
• 250-300 ml
• Hct 60%
• Stored at 4⁰C for up to six weeks
• One unit expected to raise Hgb by 1g/dL in average size adult

Packed Red Blood Cells
• Indication: symptomatic anemia
• Common triggers
– Hgb < 8 mg/dL or symptomatic
– Hgb < 10 mg/dL for cardiac or pulmonary disease
– Hemorrhage with >30% total blood loss
– Sickle cell anemia
• Transfusion or exchange to decrease Hgb S <30%
Transfusion in Critical Care Trial
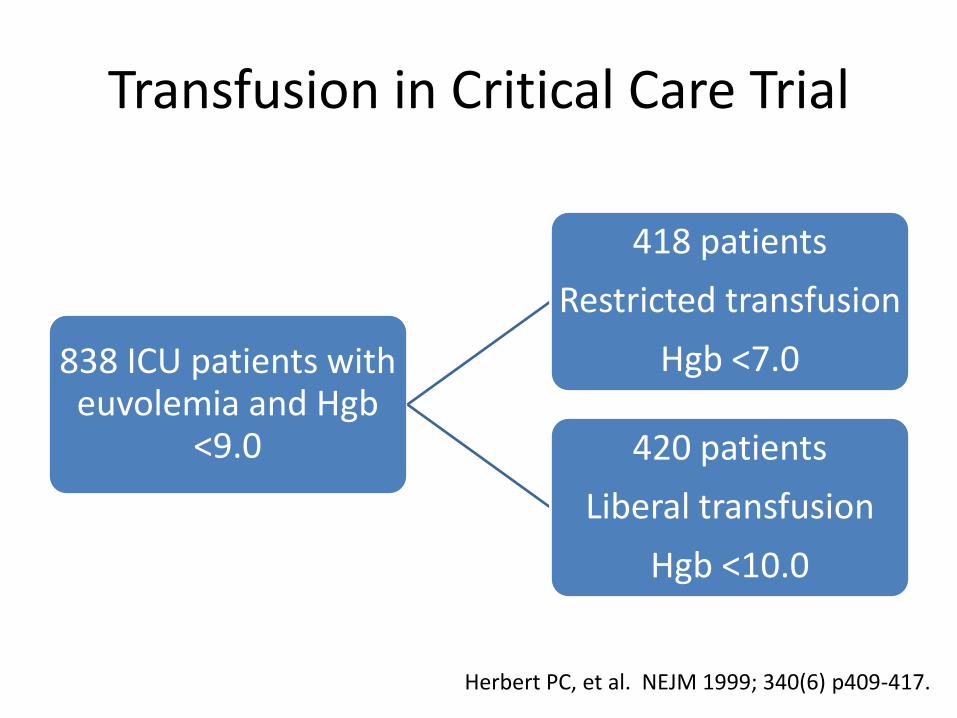
838 ICU patients with euvolemia and Hgb
<9.0
418 patients
Restricted transfusion
Hgb <7.0
420 patients
Liberal transfusion
Hgb <10.0
Herbert PC, et al. NEJM 1999; 340(6) p409-417.
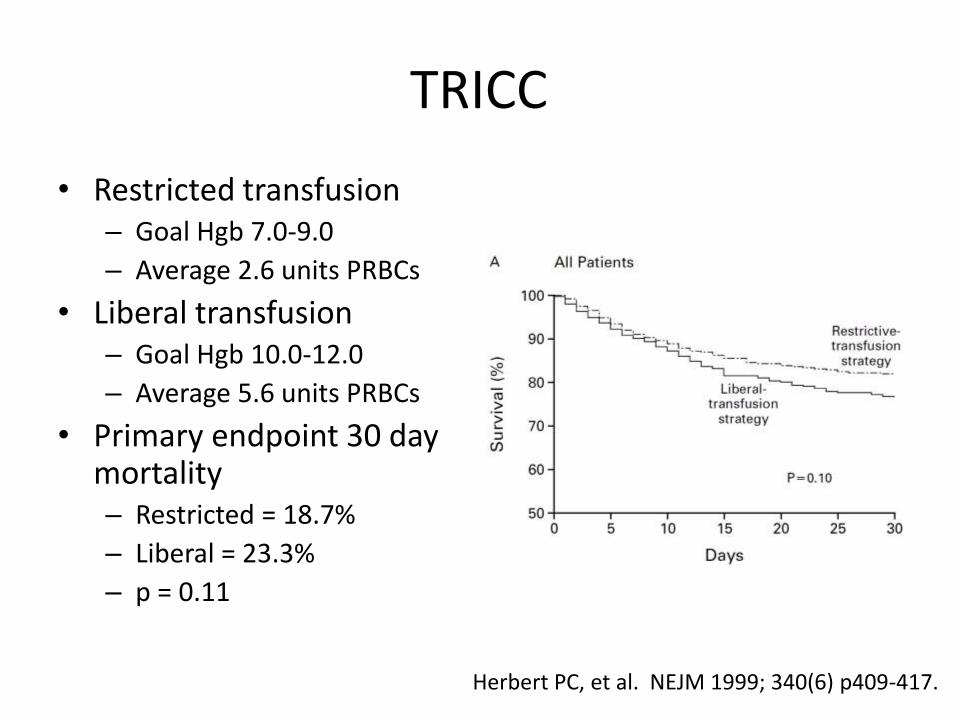
TRICC
• Restricted transfusion– Goal Hgb 7.0-9.0
– Average 2.6 units PRBCs
• Liberal transfusion– Goal Hgb 10.0-12.0
– Average 5.6 units PRBCs
• Primary endpoint 30 day mortality– Restricted = 18.7%
– Liberal = 23.3%
– p = 0.11
Herbert PC, et al. NEJM 1999; 340(6) p409-417.

Packed Red Blood Cells
• Contraindications
– Volume expansion
– Bleeding with <20-30% blood loss
– Nutritional deficiency
– Rarely indicated for Hgb > 10 mg/dL

Platelets
• Random donor– 4-6 units of platelets from multiple
donors
• Apheresis– Single donor
• Stored at room temperature for up to 5 days– Cold storage decreases platelet function– Long storage time increases infection
risk
• Raise plate count by 20,000-30,000/µL
• Platelets express ABO antigens and HLA class I Ag on their surface.Theydo not express Rh or HLA class II antigens
• ABO compatibility testing- not done routinely for plt transfusions

Platelets
• Indications: decreased platelet count and/or function
• Common triggers– Plts < 10,000
– Plts < 20,000 with fever or sepsis
– Plts < 50,000 prior to major surgery
– Plts < 100,000 prior to neurosurgery or opthalmologic surgery
– Active bleeding with known platelet dysfunction

Platelet Refractoriness
• Informal (bedside) definition: 2 consecutive post transfusion platelet count increments <10,000/µL
• Formal definition: Corrected Count Increment < 5,000/µL
• CCI = (Post transfusion platelet count –Pretransfusion platelet count) x BSA/Number of platelets transfused– Post transfusion platelet count 15 min – 1 hour after
transfusion– Number of platelets transfused expressed as multiples
of 1 x 10¹¹ - typically 3 x 10¹¹ for random donor platelet six pack or one apheresis unit
CCI Example
• Pre transfusion plt = 10,000
• Post transfusion plt = 15,000
• BSA = 2.0
• One unit apheresis
• CCI = (15,000 – 10,000) x 2.0/3 = 3,333
– <5,000 = platelet refractory

Platelet Refractoriness
• Non-immune causes– Fever, infection, splenomegaly, DIC, massive bleeding,
medications that enhance platelet destruction– More likely to affect 24 hour rather than 1 hour post
transfusion platelet count
• Immune causes– Commonly due to alloantibodies to HLA class I
antigens HLA-A and HLA-B– HLA class II antigens (HLA-DR, HLA-DP, HLA-DQ) are
insignificant for platelet transfusion– Detected by 1 hour post transfusion platelet count
Case 8
66 yo man with sepsis and DIC admitted in ICU received 1 unit of platelets for significant bleeding as her Plt count was 18K.Her platelet count increased appropriately to 40K after transfusion. Over next few days her sepsis improved and she is now on floor bed anticipating discharge.on day 8, her platelet count dropped to 12K.Labs showed no e/of DIC.
What is the likely diagnosis?
Post transfusion purpura

Post Transfusion Purpura
• Profound thrombocytopenia after transfusion of any blood component
• Mechanism– Antibodies against donor platelet antigens (HPA-1a)
results in autologous platelet destruction
• Clinical presentation– Abrupt decline in platelets usually 5-10 days to 2-3
weeks after transfusion
• Management– Usually self limited and resolves in 2-3 weeks– IVIg in severe cases

FFP
• Frozen within 8 hours of collection at -18⁰C
• Stored up to 1 year
• Volume = 200 ml
• 1 IU/ml of each factor
• To increase factor levels by 20-30% - give 10 to 20 ml/kg (4 to 6 units)

ABO typing for plasma
• Plasma contains antibodies, including antibodies to red blood cell (RBC) antigens
• Donor plasma must be either ABO-identical or ABO-compatible with the recipient
E.g,:• A patient with type A blood can accept plasma from donors
who are type A (identical) or type AB (compatible)• A patient with type B blood can accept plasma from donors
who are type B (identical) or type AB (compatible)• A patient with type O blood can accept plasma from donors
who are type O (identical) or types A, B, or AB (compatible)• A patient with type AB blood can only accept plasma from
donors who are type AB (identical)

FFP
• Indications: decreased levels of clotting factors or plasma protein not yet purified
• Common triggers:– PT or PTT 1.5x ULN with active bleeding or scheduled for
invasive procedure– DIC– Reversal of coumadin toxicity– Plasma exchange for TTP– Massive transfusion– Liver disease– Congenital factor deficiencies when specific factor
concentrate is not available (II, V, X, XI)
FFP
• Contraindications
– Volume expansion
– Mildly prolonged PT/PTT
– Protein replacement in nutritional deficiency
– Wound healing

Cryoprecipitate
• Cold-insoluble portion of plasma containing high molecular weight glycoproteins
• Stored at -18⁰C for 1 year• 25 ml for one unit• ≥ 150 mg fibrinogen• ≥ 80 IU of Factor VIII• 30% of factor XIII of
original plasma• 10 units to raise
fibrinogen 100 mg/dL
Cryoprecipitate
• Indications: decreased or dysfunctional fibrinogen, vWF, Factor XIII, Factor VIII, fibronectin
• Common triggers– Fibrinogen < 100 mg/dL
– Dysfibrinogenemia
– Factor XIII deficiency
– Uremic platelet dysfunction with bleeding
– vWD if DDAVP contraindicated (type 2B or type 3) and active bleeding

Leukoreduction
• Process: filtration of RBCs or platelets after collection to obtain 3 log (99.9%) reduction in WBCs to ≤5 x 10⁶
• Does not shorten shelf life• Indications
– Reduction of febrile nonhemolytic transfusion reactions• History of febrile nonhemolytic transfusion reaction
– Reduction of HLA alloimunization– Alternative to CMV negative blood products
• Leukoreduced is equivalent to CMV negative components
Leukoreduction
• Indications for transfusion of CMV negative components– CMV negative (both donor and recipient) organ or
bone marrow transplant
– Immunocompromised CMV negative patients• HIV
• Hematologic malignancy
• Congenital immunodeficiency
– Pregnant CMV negative patients
– Fetus and neonate
Irradiation
• Process: Gamma irradiation of RBCs or platelets with 2500 cGy to inactivate viable lymphocytes
• Shortens shelf life of RBCs to 28 days
• Indications
– Prevention of transfusion associated graft versus host disease – almost always fatal
Irradiation
• Immunocompromised– Recipients of bone marrow or stem cell transplant
– Hematologic malignancy
– Purine analogs (fludarabine, cladrabine)
– Congenital immunodeficiency
– NOT for solid organ transplant
• Fetal/Neonate– Intrauterine transfusion
– Premature infants, especially those undergoing extracoporeal membrane oxygenation
Washing
• Process: washing RBCs with normal saline to remove >98% of plasma proteins, electrolytes, and antibodies
• Shortens shelf life or RBCs to 24 hours• Indications
– Prevention of allergic transfusion reactions for patients with recurrent severe transfusion reactions unresponsive to premedication
– IgA deficient patients when IgA deficient component is not available
– Reduction of hyperkalemia in newborns and neonates

Massive Transfusion
• Transfusion of one blood volume (about 10 units PRBCs) in ≤ 24 hours
• Dilution of hemostatic constituents of blood• Transfusion goals
– Plts ≥ 50,000 (100,000 for neurosurgery, opthalmologic surgery, or cardiac bypass)
– PT/PTT ≤ 1.5x ULN– Fibrinogen ≥ 100 mg/dL
• Complications– Bleeding, hypothermia, acidosis, hypocalcemia
(citrate)


Apheresis
Procedure
• Leukopheresis
• Plateletpheresis
• Therapeutic Plasma Exchange
• Red Cell Exchange
• Stem Cell Collection
Indications• Leukemia (Blasts > 100,000)
leukostasis• Thrombocytosis (plt > 1,000,000),
symptomatic• TTP, cryoglobulinemia,
hyperviscosity in monoclonal gammopathies, myasthenia gravis , Guillan-Barre, Goodpasturesyndrome, CIDP, paraproteinemicpolyneuropathy, humoral renal transplant rejection
• Acute chest syndrome or stroke in sickle cell disease (goal Hb S <30%), malaria, babesiosis
• Stem cell transplant

The End