final thesis draft - open...
TRANSCRIPT

Optimizing Anticoagulation Therapy inECMO Patients using Antithrombin III
Item Type text; Electronic Thesis
Authors Oldeen, Molly Elisabeth
Publisher The University of Arizona.
Rights Copyright © is held by the author. Digital access to this materialis made possible by the University Libraries, University of Arizona.Further transmission, reproduction or presentation (such aspublic display or performance) of protected items is prohibitedexcept with permission of the author.
Download date 22/07/2018 23:30:30
Link to Item http://hdl.handle.net/10150/228500
OPTIMIZING ANTICOAGULATION THERAPY FOR ECMO PATIENTS USING
ANTITHROMBIN III
By
Molly Elisabeth Oldeen
_______________________________________________
Thesis Submitted to the Faculty of the
MEDICAL PHARMACOLOGY DEPARTMENT
In Partial Fulfillment of the Requirements
For the Degree of
MASTER OF SCIENCE
In the Graduate College
THE UNIVERSITY OF ARIZONA 2012
STATEMENT BY AUTHOR
This thesis has been submitted in partial fulfillment of requirements for an advanced degree at The University of Arizona and is deposited in the University Library to be made available to borrowers under rules of the Library. Brief quotations from this thesis are allowable without special permission, provided that accurate acknowledgment of source is made. Requests for permission for extended quotation from or reproduction of this manuscript in whole or in part may be granted by the head of the major department or the Dean of the Graduate College when in his or her judgment the proposed use of the material is in the interests of scholarship. In all other instances, however, permission must be obtained from the author.
SIGNED: _________________________________________ Molly Elisabeth Oldeen
APPROVAL BY THESIS DIRECTOR This thesis has been approved on the date shown below:
05/07/12 Douglas F. Larson Date Professor of Pharmacology

3
TABLE OF CONTENTS
LIST OF TABLES ........................................................................................................................5
LIST OF FIGURES.......................................................................................................................6
ABSTRACT ..................................................................................................................................7
BACKGROUND ...........................................................................................................................9
ECMO ...............................................................................................................................................................9
Anticoagulation ........................................................................................................................................................11
Complications Related to ECMO........................................................................................................................14
Coagulation Management....................................................................................................................................17
Previous Research ...............................................................................................................................................19
OBJECTIVES............................................................................................................................. 21
PATIENTS AND METHODS.................................................................................................. 22
Indications for ECMO............................................................................................................................. 22
Anticoagulation and Transfusion Protocols................................................................................ 23
Data Collection and Analysis.............................................................................................................. 23
RESULTS ................................................................................................................................... 25
DISCUSSION............................................................................................................................. 29
CONCLUSIONS......................................................................................................................... 34
Summary..................................................................................................................................................... 34

4
TABLE OF CONTENTS - CONTINUED
Future Directions .................................................................................................................................... 35
APPENDIX ................................................................................................................................ 36
REFERENCES ........................................................................................................................... 44

5
LIST OF FIGURES
Figure 1........................................................................................................................................................ 36
Figure 2 ........................................................................................................................................................................37
Figure 3 ........................................................................................................................................................................38
Figure 4 ........................................................................................................................................................................39
Figure 5 ........................................................................................................................................................................40
Figure 6 ........................................................................................................................................................................41

6
LIST OF TABLES
Table 1 ......................................................................................................................................................... 42
Table 2 ..........................................................................................................................................................................43
7
ABSTRACT
One of the most fundamental aspects of extracorporeal membrane oxygenation
(ECMO) is maintaining proper anticoagulation management in order to prevent
hemorrhagic or thrombotic events. Anticoagulation on ECMO is most commonly
achieved with the use of unfractionated heparin to maintain a minimum
anticoagulation level as monitored by activated clotting time (ACT). Heparin’s main
effect is exerted by binding to and potentiating antithrombin III. Many factors may
contribute to a sub-‐therapeutic ATIII level that may decrease the effectiveness of
heparin. A retrospective record review was performed on all adult ECMO patients
at the University of Arizona Medical Center between 2008 and 2011, in order to
determine optimal ATIII levels for maintaining proper anticoagulation. In addition,
we investigated correlations between ATIII levels and hemorrhagic and/or
thrombotic events. Variables measured include, ACTs, heparin dose, ATIII dose,
ATIII levels, blood product use, and adverse events. Thirty-‐five patients received
ATIII over the course of the ECMO run. Six patients did not receive ATIII and they
were found to have used significantly more blood products than those who did
receive ATIII. Also, heparin dose dropped significantly 24h after the first dose of
ATIII. There is a significant positive correlation between the amount of ATIII given
per day and the amount of packed red blood cells transfused per day. The results

8
suggest an ideal therapeutic range of ATIII dosing, where lack of or too much ATIII
administration can lead to excessive bleeding.

9
BACKGROUND
ECMO
Extracorporeal membrane oxygenation (ECMO) is a form of mechanical
circulatory support that is used in the management of life threatening pulmonary or
cardiac failure. It is often utilized in emergent situations and only for temporary
support. A requirement for extracorporeal membrane oxygenation is systemic
anticoagulation. This happens to be a limitation as well due to bleeding
complications. ECMO controls the gas exchange and perfusion, while stabilizing the
patient physiologically and reducing the risk of iatrogenic injury. Gas exchange can
be dependent on the thickness of the blood film, membrane material, fraction of
inspired oxygen (FIO2), and hemoglobin concentration1. Simultaneously, it allows
time for diagnosis, treatment, and most importantly, recovery from injury or
disease2. Circulation through the device occurs by draining right atrial blood from
the venous circulation through a cannula to an artificial lung device and returning it
to the patient through another cannula to the aorta (veno-‐arterial) or the right
atrium (veno-‐venous). Veno-‐arterial cannulation may provide support for both the
heart and lungs. Veno-‐venous oxygenation is used in series to the native lungs to
assist in oxygenation for those in isolated respiratory failure.
The specific vessel cannulation for both modes of ECMO can vary depending
on the needs of the patient. Veno-‐venous cannulation can be achieved multiple

10
ways through cannulation of the femoral vein and/or internal jugular vein. Veno-‐
arterial cannulation is most commonly through cannulation of the femoral vein and
femoral artery. For infants, with femoral vessels that are too small or difficult to
reach, cannulation is most often via the internal jugular and carotid.
The overall purpose of veno-‐venous cannulation is to return oxygenated
blood to the venous circulation, thereby increasing oxygen content and lowering
CO2 content in the right atrial blood. This blood is pumped through the functionally
preserved cardiac system where the heart is solely responsible for systemic
perfusion and blood flow. Patients remain both sedated and immobile while on this
device. In addition, the lungs are still being ventilated on minimal settings despite
their inability to oxygenate adequately in order to prevent additional damage.
Veno-‐arterial cannulation may provide full or partial cardiac support
depending on the needs of the patient and the underlying function of the heart.
Oxygen and carbon dioxide levels in the blood are a reflection of blood flow that is a
combination of pumping from the heart as well as flow from the circuit. If the lungs
are functioning poorly, then blood leaving the heart from the left ventricle will be
similar to that entering the right atrium. The best location to determine optimal
ECMO flow and measure cerebral perfusion is to take a blood gas from the right
upper extremity. This is because the innominate is the last aortic arch vessel to
11
receive flow from the ECMO circuit when returned retrograde through the femoral
artery.
Clinical syndromes indicated for ECMO include both cardiac and respiratory.
ECMO is reserved for the most medically compromised patients that have exhausted
all optimal care resources and present as a high mortality risk. Acute cardiac failure
occurs when the heart cannot produce adequate cardiac output to supply the body
with oxygenated blood. Acute respiratory failure occurs when the lungs can no
longer efficiently oxygenate the blood and remove carbon dioxide.
Anticoagulation A primary requirement for ECMO is systemic anticoagulation. The most
common drug used to achieve this effect is unfractionated heparin. Heparin is one
of the oldest anticoagulation drugs that is still in clinical use. It did not enter clinical
trials, however, until 1935, for its use as a blood anticoagulant3. Today, it is
commonly used for conditions such as acute coronary syndrome, atrial fibrillation,
deep vein thrombosis, pulmonary embolism, cardiopulmonary bypass for heart
surgery, as well as ECMO4. It continues to dominate anticoagulation therapy for
ECMO because it is rapid acting, easily controllable, inexpensive and widely
available. In addition, it is well tolerated by both adult and pediatric patients5.

12
Heparin is naturally produced by basophils and mast cells. Commercially, it
is most often derived from porcine or bovine sources. Commercial preparations
typically include a wide range of molecular weights from 3,000 to 40,000 Daltons,
with a mean molecular weight of 15,000 Daltons6. The structure of heparin is a
heavily sulfated glycoaminoglycan polymer, making it strongly acidic and negatively
charged. Heparin dosing is primarily dependent on its indication for use.
Cardiopulmonary bypass requires a dose of 300-‐400 U/kg. ECMO requires between
20 and 70 u/kg/h. A unit of heparin is measured as a unit of activity. More
specifically, activity is defined as the “amount of heparin that maintains the fluidity
of 1mL of citrated sheep plasma for 1 hour after recalcification”6. This measurement
technique is used to maintain consistency in dosing as different manufacturers vary
the number of USP units per milligram of drug. Heparin exerts its main effect on the
coagulation cascade. The plasma coagulation cascade is the process of fibrin clot
formation in response to both intrinsic and extrinsic activation. Intrinsic activation
results from contact of blood with foreign surfaces, whereas extrinsic activation
results from injury of the vasculature. Both pathways converge to form the common
pathway, beginning with the activated factor X, which converts prothrombin to
thrombin. Thrombin converts fibrinogen into fibrin, resulting in the formation of a
strong clot after fibrin cross-‐linking. In addition to activating fibrinogen, thrombin

13
also stimulates platelet activation, which results in further platelet aggregation and
adherence to endogenous surfaces forming a strong platelet plug.
Alternatively, in order to prevent excessive clot formation and dissolve clots,
the body has various negative feedback systems. Factors involved include, proteins
C and S, antithrombin III, tissue factor inhibitor and tissue plasminogen activator. It
is here that heparin exerts its main effects.
Heparin specifically provides its pharmacological effects by binding to and
amplifying the enzymatic fuction of antithrombin III (ATIII) by more than 1,000
fold6. Antithrombin III primarily inhibits thrombin, as well activated factor X. It
also inhibits factors IX, XII, and XI, to a lesser extent. The site on heparin that binds
to ATIII is found on about 30% of heparin molecules. In the common pathway,
factor Xa activated the conversion of prothrombin to thrombin which heparin
blocks by binding to antithrombin III. Heparin does have minimal non-‐ATIII
dependent anticoagulation effects. It can bind to and activate cofactor II, a natural
thrombin inhibitor. Biologic activity varies between 30 minutes and 6 hours
depending on systemic heparin concentrations5. Heparin is metabolized by the
reticuloendothelial system in addition to the liver. Up to 50% can be excreted
unchanged by the kidneys. Due to heparin’s half-‐life, patients must be kept on a
constant heparin infusion to maintain anticoagulation, with bolus infusions given as
needed.
14
Some patients may exhibit heparin resistance, which tends to be those who
have had prior heparin therapy or an ATIII deficiency. Small amounts of heparin
may bind to plasma proteins such as vitronectin and fibronectin thereby decreasing
its effectiveness and availability for ATIII7. ATIII levels may also be decreased in
those that have been pretreated with heparin6. If this is the case, it has been shown
that “purified ATIII even in small doses, significantly prolongs the ACT response to
heparin”8. Heparin resistance is also often related to certain clinical conditions such
as sepsis, liver disease, or any condition that exerts stress on the body that may
deplete ATIII levels. Given that many of the critically compromised patients on
ECMO are subject to prior or chronic heparin therapy and have conditions that
induce stress on the body, this is clinically significant. If levels are low to begin with,
prophylactic treatment may be indicated.
There is universal acceptance that ATIII levels fall upon initiation of ECMO,
up to 50% 9, and also, that anticoagulation should be monitored using a combination
of measurement techniques in order to understand the complete coagulation profile
for each individual patient.
Complications Related to ECMO Unfortunately, there are various complications related to ECMO. Most
complications are due to the need for systemic anticoagulation. There is a fine

15
balance to be maintained between excessive anticoagulation resulting in bleeding,
and under dosing resulting in excessive clot formation seen in the circuit tubing or
oxygenator.
Bleeding or hemolysis can occur resulting in the need for replacement and
transfusion of red blood cells. Bleeding can occur at the surgical sites from recent
surgery or at the cannula insertion sites. Unfortunately, this is exacerbated by the
use of heparin as a systemic anticoagulant. For that reason, if a patient is put on
ECMO post-‐operatively, heparin is often withheld until bleeding is controlled.
Hemolysis is another negative side effect of ECMO blood replacement that
may require red blood cell replacement. Fortunately, with further advances in
technology such as low resistance gas exchange devices and second generation
centrifugal pumps, hemolysis is not as common. Hemolysis occurs mainly from
anything resulting in excessive negative pressures and turbulance10. Cavitation can
occur when a fluid such as blood is exposed to an extreme negative pressure in
excess of 650 mmHg. Centrifugal pumps operate at high rpms can cause in excess of
700mmHg negative pressure. This can occur when blood in the pump head is
ejected, but nothing fills the void, therefore a vacuum is created resulting in
cavitation and further hemolysis. Causes of this volume issue can be due to low
blood volume, patient position, cannula size, cannula position, coughing and
others10. This can be a common problem, especially in those post-‐operative patients
16
with excessive bleeding as measured in chest tube output. Volume replacement and
maintaining safe flow parameters are the easiest solutions to avoiding hemolysis.
Other causes of hemolysis are related to shear stress, physical properties of
the ECMO circuit, as well as sub-‐lethal damage to erythrocytes11. As proof of this
hemolysis, the level of plasma free hemoglobin can increase by as much as 10 to 25
fold after just 24 hours of ECMO. Continuous renal replacement therapy, a common
addition to the circuit for those patients in renal failure, is also known to cause
hemolysis, therefore RBC transfusion due to excessive blood loss has a direct
relationship with RBC hemolysis.
Various coagulopathy problems can occur with the use of ECMO as well. Due
to the continuous contact of the patient’s blood volume with the non-‐biologic
surface of the circuit, there is activation of both contact and fibrinolytic systems.
Also, within minutes of initiation of ECMO, there is consumption and dilution of all
factors. Consumption of factors can result in with fewer factors available for
coagulation resulting in bleeding. In a study by Arnold et al., it was found that there
was both evidence of reduction in coagulation factors and activation of the
coagulation cascade12. For this reason, factor replacement is a necessity.
Another complication related to ECMO is clot formation within the circuit.
Clot formation is the most common mechanical complication resulting in potential
thrombus1. This frequently at locations where there is high turbulence such as at

17
tubing connection points as well as in the membrane oxygenator. Severe
consequences to clot formation include passing of clots into to systemic circulation
or oxygenator failure.
Coagulation Management The key to effective anticoagulation in these patients is the utilization of a
variety of monitoring techniques. It is important to create a coagulation profile for
each patient on a daily basis. This includes a combination of laboratory tests such as
measurement of platelet count, antithrombin, aPTT, TEG, as well as hemoglobin
requirements.
The easiest and most popular technique to use is the bedside measurement,
termed activated clotting time (ACT). This measures the integrity of the intrinsic
coagulation and common pathways using a whole blood sample. The acceptable
range for ACT values is between 180-‐220 seconds for patients supported on ECMO.
Despite its continued widespread use due to ease and instant results, ACT has a
limited range of accuracy. Results may be affected by many factors related to
patient characteristics, such as coagulopathy, immature coagulation system (such as
in infants), platelet dysfunction, hypothermia, ATIII levels, age, and hemodilution
from the circuit prime volume5. For this reason, it is important to consult other
monitoring techniques as well.

18
Another common test for anticoagulation management is the
thromboelastogram (TEG). The TEG is useful in that it accurately measures the
viscoelastic properties of a blood sample in order to better understand a patient’s
whole clotting system as opposed to individual components. It describes clot
formation and clot dissolution as part of fibrin breakdown, which is equally
important. The ability to also characterize hypercoagulability is necessary in order
to know if patients have the sufficient clotting factors available or if they need factor
replacement.
Specifically related to the clotting cascade, we are also interested in
measuring activated partial thromboplastin times (aPTT). This is the universal
standard for monitoring heparin therapy, in addition to congenital and acquired
factor deficiencies13. Measuring aPTT alone, however, is not the best indicator of
heparin therapy, as aPTT can be prolonged for many reasons such as factor
deficiencies, vitamin K deficiencies, as well as disseminated intravascular
coagulation. It should be used in combination with the other techniques mentioned
previously.
Despite improvements in the management of ECMO patients, complications
remain high related to bleeding and thrombosis. These patients present a unique
challenge with complicated disease states often involving pre-‐existing clotting
disorders, that are exacerbated by heparin. Therefore, the best approach to reduce

19
incidence of adverse events is multidisciplinary among surgeons, physicians,
perfusionists, nurses and ECMO specialists. To benefit the advancement of patient
care, we present a unique study assessing anticoagulation parameters and outcomes
related to the use of antithrombin III.
Previous Research Currently, there is very little research supporting the topic of anticoagulation
on ECMO specially related to ATIII. Previous studies have explored multiple
coagulation parameters while patients are on ECMO. One particular study
specifically looked at ATIII levels and tested two dosing mechanisms, comparing
bolus versus continuous infusion. They found continuous infusion to show better
overall outcomes by reducing activation of heparin more than bolus infusion14.
They maintained ATIII levels at >100% and showed reduced surgical revision for
bleeding within the first 48 hours. Other studies test for all coagulation factors at
set time points and compare how they relate to patient outcomes14,15. The choice of
using multiple coagulation tests in order to obtain a more accurate picture is that at
times the ACT level alone can be limited due to issues such as consumptive
coagulopathies, clotting factor deficiencies, platelet dysfunction, as well as
fibrinolysis15. Another study measured antithrombin replacement during ECMO

20
and only hemorrhagic complications16, finding that upon administration, there were
no significant differences in bleeding and ATIII levels.

21
OBJECTIVES
This study will be the first to provide a detailed analysis of ATIII and how it
relates to patient outcomes. It will enable us to more effectively manage ECMO
patients and aid in the prevention of adverse events. Hemorrhage will be measured
as packed red blood cell administration and thrombosis will be measured by circuit
change outs or any other evidence of major clotting. At this time, it is uncertain at
what minimum level patients should receive replacement prior to ECMO initiation.
Secondarily, in the long term this project has the possibiility of helping reduce the
costs of ECMO for these patients by preventing circuit change outs caused by
clotting, educing the length of time spent on the assist device, as well as reduce
expensive blood product transfusions.
It is important to monitor ATIII due to the hemodilution and activation of
other factors upon initiation of ECMO. Currently, we measure ATIII levels
throughout the ECMO run. The subsequent drop following initiation can be a
potential hazard towards maintaining optimal anticoagulation. Low levels of ATIII
may produce ACT levels below standard and the administration of more heparin
without sufficient ATIII levels can lead to increased bleeding17. It is also important
to take into consideration preexisting conditions that many patients recommended
for ECMO have that may cause them to have reduced levels of ATIII initially.

22
PATIENTS AND METHODS
An institutional review board-‐approved retrospective chart review was
performed on all adult ECMO patients supported at the University of Arizona
Medical Center between the years of 2008 and 2011.
Indications for ECMO ECMO is indicated for patients that suffer from severe acute cardiac and
respiratory failure. Indications for those that suffer from respiratory failure in this
specific population of patients include syndromes that result in the inability of the
lungs to provide sufficient oxygenation, such as Acute Respiratory Distress
Syndrome (ARDS), H1N1, sepsis, post lung transplantation, and others. Indications
for cardiac failure include syndromes that result in the heart being unable to
provide enough cardiac output or blood supply to the rest of the body, such as,
failure to wean from cardiopulmonary bypass, post myocardial infarction, and
cardiogenic shock. ECMO is used for those patients that have exhausted all other
options for treatment and have an 80% mortality risk2.
The ECMO circuit used at the University of Arizona Medical Center for all
patients includes a Maquet Rotaflow centrifugal pump with the Quadrox heparin
coated hollow fiber membrane oxygenator. Cannulation varied among patients and

23
included (i) intrathoracic, (ii) right internal jugular vein and common carotid artery,
or (iii) femoral vein and artery.
Anticoagulation and Transfusion Protocols Unfractionated heparin was used for anticoagulation purposes for all
patients. Dosing was titrated at drip rates sufficient to maintain an activated
clotting time between 160-‐200 seconds depending on bleeding issues. Packed red
blood cells (pRBCs) were transfused to maintain a hematocrit of greater than 30%.
Platelets and fresh frozen plasma were transfused as needed as well to maintain
normal clotting factor levels.
ATIII levels were measured on all patients to maintain percentage activity
between 80 and 120%. ATIII dosing to maintain normal levels was determined at
the discretion of the physician in combination with manufacturer recommendations.
Data Collection and Analysis Various demographics were collected from patient charts, such as age,
gender, height, weight, and BSA. Indication for ECMO, length of time on ECMO,
survival, and cannulation technique were also collected. Laboratory values included
ACTs, heparin drip rates, ATIII levels, ATIII dosing, as well as blood product use.

24
Adverse events were recorded as bleeding, evidence of clots in the circuit, and
cerebral vascular accidents (CVAs).
In order to determine the effect of ATIII on product use, packed red blood
cells (pRBC), platelets, and fresh frozen plasma transfusions were measured. The
amount of pRBCs transfused was used as a measure of bleeding requiring red blood
cell replacement.
In order to determine the effect that ATIII had on heparin drip rates we
measured heparin infusion at the time of the first dose of ATIII and subsequently 24
hours later. The first dose was used as to avoid potential confounding effects of
multiple doses of ATIII.

25
RESULTS
Throughout the study period, 41 patients were supported on ECMO. One patient
was excluded due to an ECMO duration of only three hours. The patients were
divided into cardiac and respiratory due to the extreme differences in underlying
pathology. The cardiac group (n=21) and respiratory group (n=20), had a
significant difference in ages with a mean age of 57.7 ± 2.7 (mean ± SD) years, and a
mean age of 39.4 ± 3.3 (Table 1) respectively. The cardiac group had a mean weight
of 92 ± 4 kg, and the respiratory group had a mean weight of 84 ± 6 kg. The cardiac
group had a statistically significant shorter length of stay at a mean of 7.4 days,
while the respiratory group had a mean of 14.1 days. Survival differences were also
statistically significant in that the cardiac group had a mean survival rate of 58%,
and the respiratory group had a rate of 35%.
Indications for ECMO in these patients include both cardiac and respiratory
failure disorders. Of the cardiac failure patients (n=21), indications include failure
to wean, idiopathic cardiomyopathy, cardiogenic shock, post cardiac surgery (valve
replacements, root replacements, CABG), post MI, post partum, etc. Of the
respiratory failure patients, a majority of indications for ECMO include ARDS,
respiratory failure, drug overdose, H1N1, sickle cell, pulmonary edema, pulmonary
fibrosis, post lung transplant, etc.

26
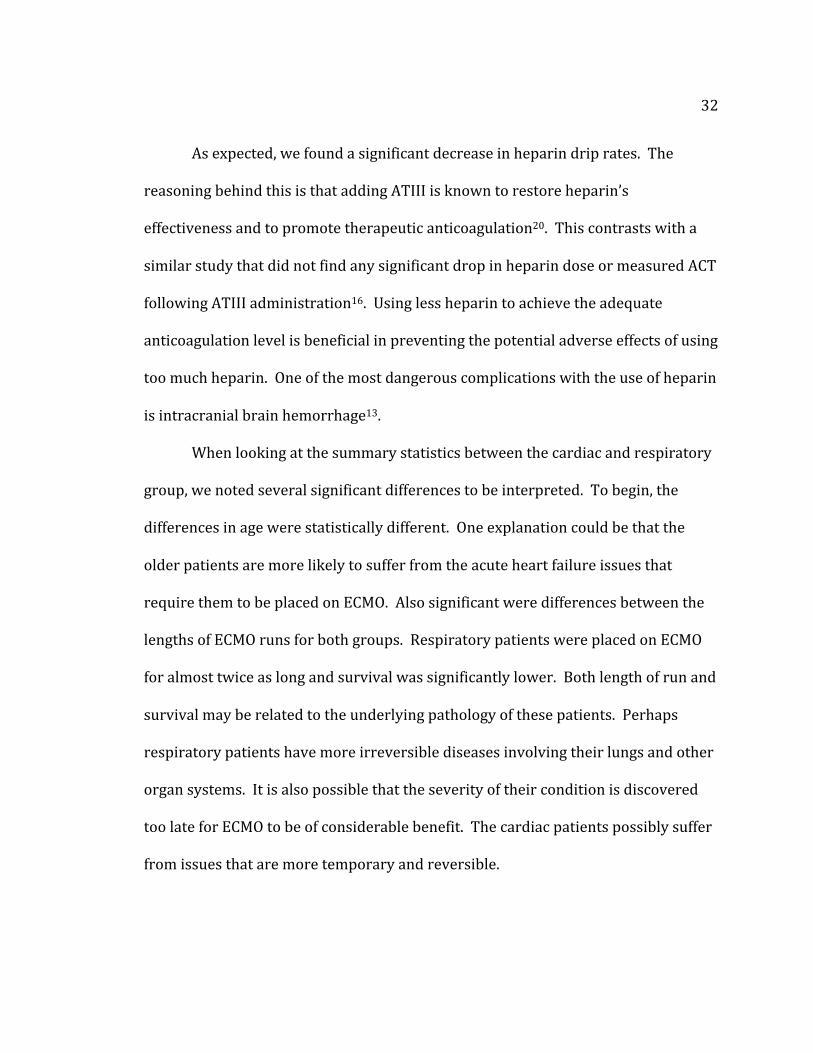
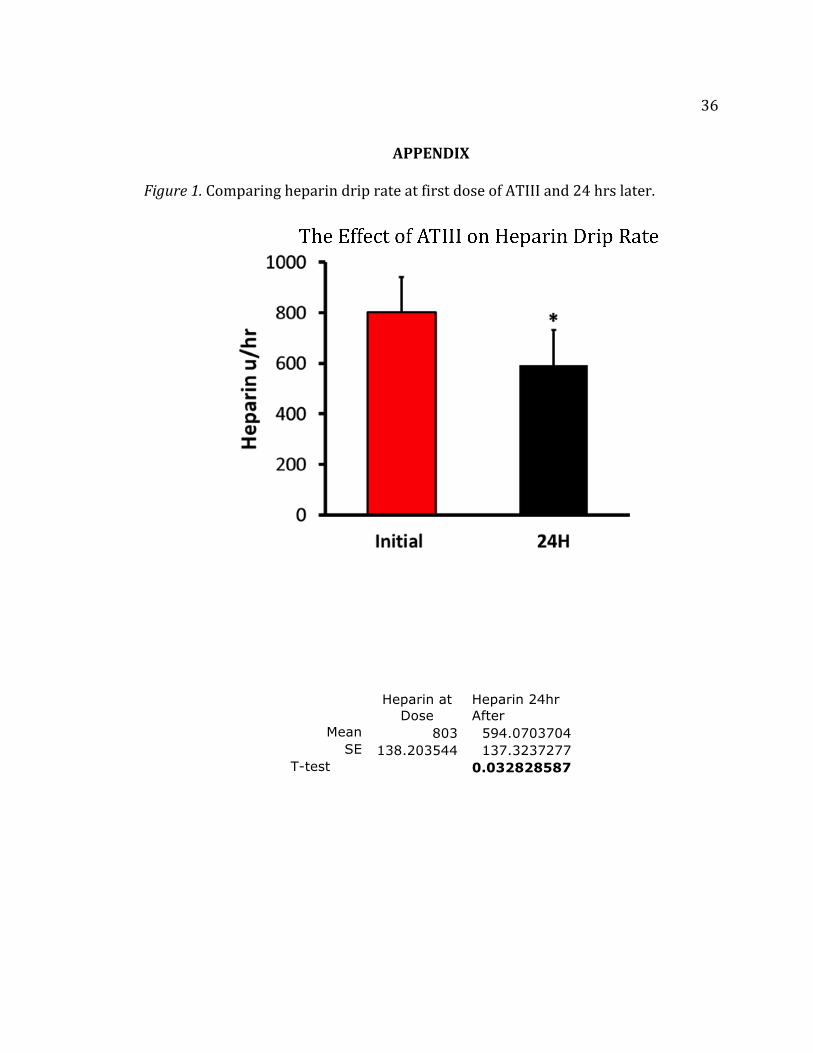
When comparing the effect of ATIII on heparin drip rate at first dose and 24h
later, the results show that there is a statistically significant (p< .05) decrease in the
heparin drip rate 24 hours after ATIII was administered (Figure 1). The mean dose
at heparin at ATIII administration was 803 units per hour, which decreased to an
average of 594 units per hour after 24 hours. Six patients were not on heparin
infusions at the time of the first dose of ATIII possibly due to uncontrolled bleeding
post-‐operatively. One of the patients not on heparin infusion had a heparin allergy,
so that patient was excluded as well. For those reasons, analysis was limited to 35
cases.
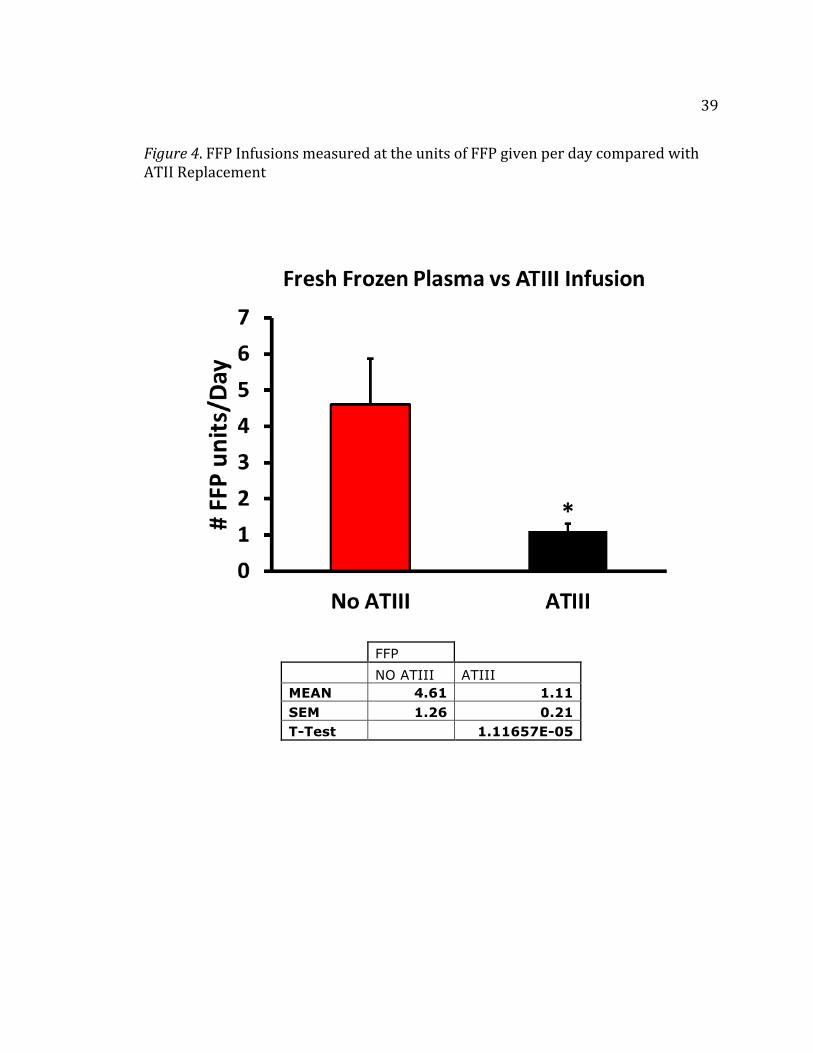
In comparing those patients who did receive ATIII replacement (n=35) to
those that did not receive ATIII replacement (n=6), there was a significant
difference for all blood products used between those that did not receive any ATIII
and those that did receive ATIII (Figure 2-‐4). Those that did not receive ATIII were
given a mean of 7.02 ± 1.25 units of pRBCs per day, 2.93 ± 0.37 units of platelets per
day, and 4.61 ±1.36 units of FFP per day. This is compared with those who were not
dosed with ATIII that were given 2.81 ± 0.30 units of pRBC per day, 0.77 ± 0.17 units
of platelets per day, and 1.11 ± 0.21 units of FFP per day. The non-‐ATIII group used
significantly more blood products on average per day compared with those who did
receive ATIII.
27
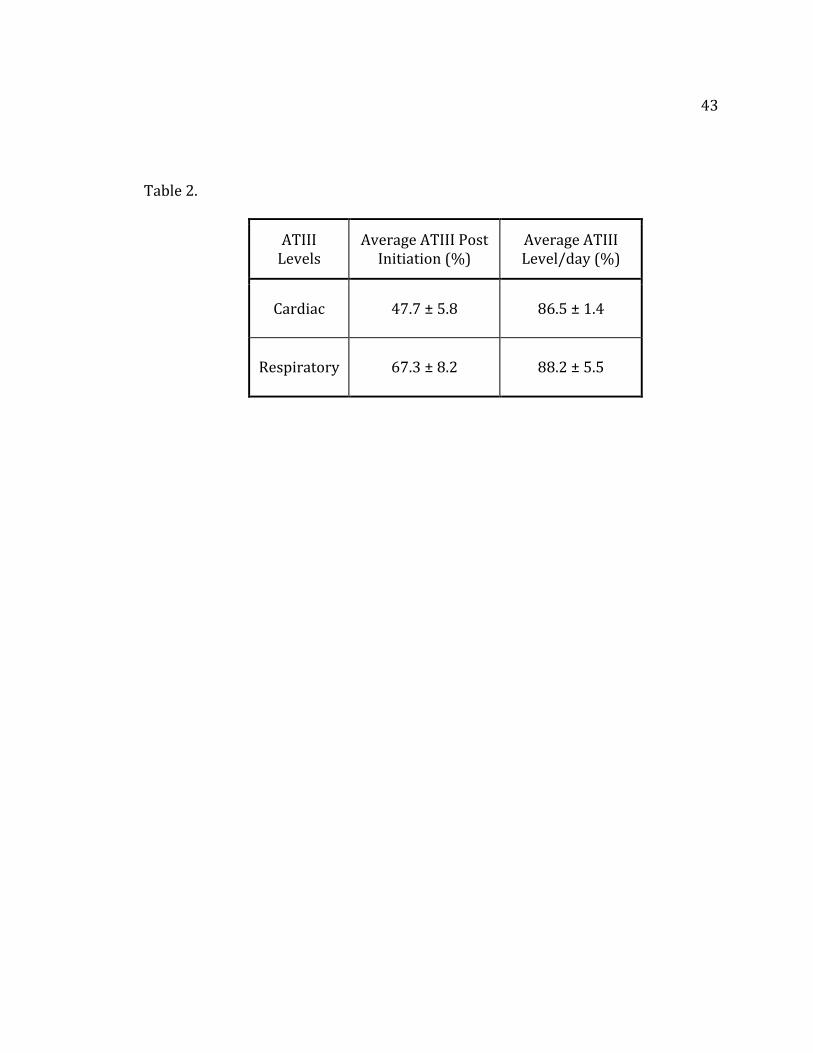
Given that the results suggest ATIII is important, we wanted to determine
how well our institution replacing it, in order to sustain therapeutic levels by
comparing and measuring each group’s ATIII levels post cannulation and the
average ATIII level per day (Table 2). Post cannulation, the cardiac group had an
average ATIII level of 47.7 ± 5.8%, whereas the respiratory group had an average
ATIII level of 67.3 ± 8.2%. The average ATIII level per day was 86.5 ±1.4% for the
cardiac group and 78.1 ±3.1% for the respiratory group. Subsequently, on average,
the patients are being treated to the lower threshold of therapeutic level once
replacement begins. The low levels post-‐cannulation are in support of the findings
that factors are both consumed immediately and slightly hemodiluted.
The cardiac failure group had a significant correlation between the number
of pRBCs transfused per day and the dose of ATIII given per day (p<.05) (Figure 5).
There seemed to be a cluster of patients with less ATIII and less pRBCs possibly
suggesting that there is an ideal amount of ATIII that should be given to avoid blood
product use. On the same graph, there were a few patients with significantly more
ATIII used which correlated with more pRBCs, possibly suggesting that too much
ATIII, an anticoagulant, may result in more bleeding necessitating increased blood
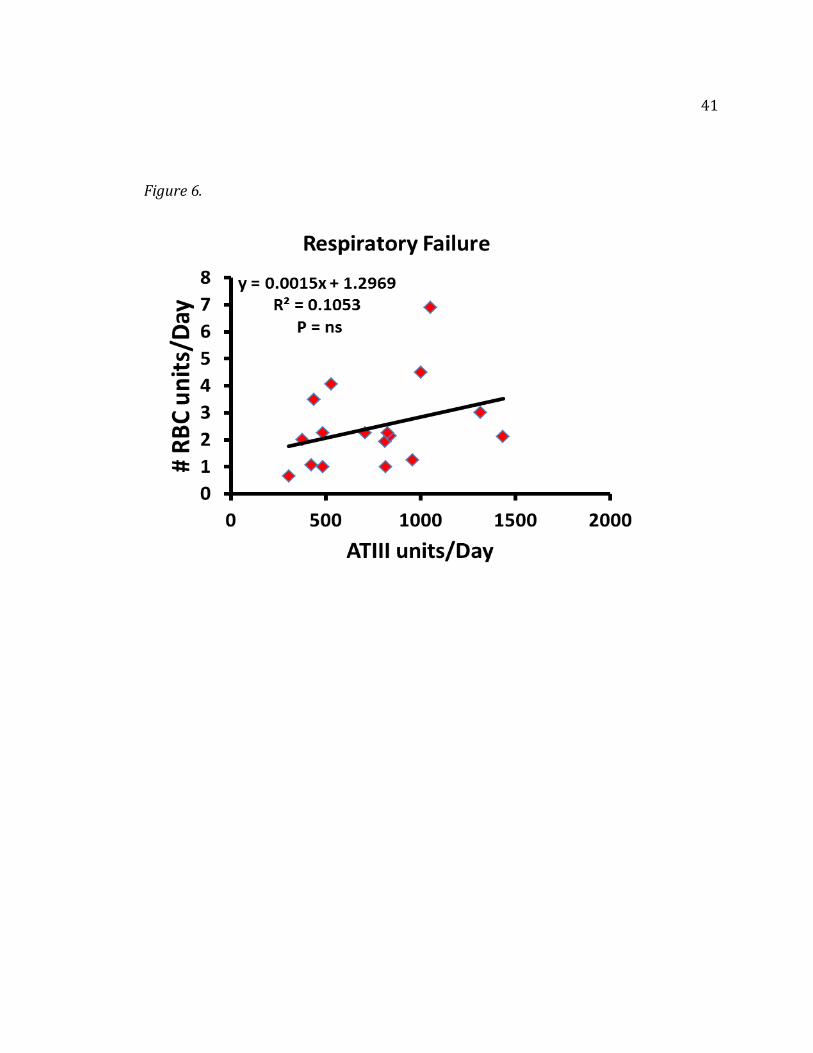
product use. The respiratory group, on the other hand, did not show any significant
correlation (Figure 6) between the amount of blood products used per day and ATIII
units given per day.

28
Adverse events were measured on a nominal scale as yes or no, indicating
whether they were observed throughout the entire ECMO run. There was
suggestive evidence of clotting in 33 (80%) patients. Clotting was visualized on the
circuit itself as dark or white areas most often at the oxygenator or tubing
connection sites. Despite the presence of clotting in many of the circuits, only 13
patients required one or more circuit changeouts throughout the ECMO run.

29
DISCUSSION
The results suggest that antithrombin is, in fact, an important component in
the treatment of ECMO patients. Both high doses and lack of antithrombin III
replacement are correlated with excessive blood product use. There appears to be
a therapeutic range to dose ATIII to prevent bleeding. With this insightful
information, we can continue advance and improve anticoagulation therapy in
ECMO patients.
Other studies have measured the effect of preoperatively treating patients
with ATIII for cardiopulmonary bypass during cardiac surgery. One study by
Avidan, et al., found that treatment with antithrombin III was effective in restoring
heparin effectiveness, in addition to promoting anticoagulation at therapeutic levels
for cardiopulmonary bypass18. Few studies, however, have specifically looked at
ATIII replacement in adult ECMO patients as it correlates with outcomes and blood
product usage. It is recognized that ATIII will continue to be consumed in the
presence of heparin, and there is both hemodilution and activation of clotting
factors from the ECMO circuit. Based on these reasons and the evidence from
previous studies, patients may truly benefit from the maintenance of normal ATIII
activity levels.
As antithrombin is an anticoagulant, it is possible that it can contribute to
increased bleeding in these patients. Our correlation results in the cardiac group (r2

30
= .49) suggested the possibility that too much ATIII may lead to increased RBC
replacement. Other studies have not found that bleeding or the need for pRBC
transfusion increases significantly with ATIII administration16. Further research
with more patients must be conducted to increase the significance of this data.
Our data shows that patients receiving no supplemental ATIII necessitated
significantly more blood products. When trying to understand why this might be
true, we looked at the individual patients. One possible explanation could be that
patient’s heparin dose continued to increase to maintain anticoagulation standards
based on ACTs and the non-‐ATIII dependent anticoagulant effects of heparin
resulted in bleeding. ECMO runs ranged between 2 and 9 days, therefore it was not
a short length of stay that resulted in not receiving ATIII. One patient had a heparin
allergy, which would explain why ATIII was not given to him. That patient was
given argatroban, which is a direct thrombin inhibitor, therefore its use is not
dependent on the presence of ATIII . Almost all patients were placed on ECMO after
extensive heart or lung surgery, such as post lung transplant (two patients), mitral
valve replacement, aortic arch and root replacement (two patients). One patient
was seen post trauma with pulmonary edema.
Further analysis collecting d-‐dimer levels did show elevated levels above the
threshold criteria of <0.5 μg/ml in 5 out of the 6 patients throughout the run. D-‐
dimers are fibrin degradation products that arise from the breakdown of clots
31
degraded by fibrinolysis. Positive d-‐dimer results maybe be suggestive that the
coagulation system has been activated, and a patient is in disseminated
intravascular coagulation (DIC). This is also known as consumptive coagulopathy.
It occurs when the body is rapidly and pathologically activating the coagulation
mechanisms that result in small blood clots in the vessels of the body. The clots
consume all of the clotting factors, which can lead to abnormal bleeding from
locations such as surgical wounds, cannulation sites, etc. Excessive bleeding may
explain why the patients did not receive antithrombin, a natural anticoagulant. It
could be suggested that the traumatic surgery resulted in activation and further
consumption of the clotting factors, leading to increased d-‐dimers as well. When
comparing d-‐dimer levels of patients that did receive ATIII, they had positive levels
as well. This is not surprising as other studies have found elevated d-‐dimer levels at
all times during ECMO despite adequate anticoagulation19.
We also investigated fibrinogen levels. Low levels of fibrinogen can
indicate DIC when fibrinogen is consumed faster than synthesized. It was found that
only 3 of the 6 patients had below threshold fibrinogen levels. Despite the fact that
the presence of d-‐dimers and low fibrinogen levels suggest DIC, more research
would have to be completed to correctly identify these patients as having this
diagnosis that is difficult to identify in general.
32
As expected, we found a significant decrease in heparin drip rates. The
reasoning behind this is that adding ATIII is known to restore heparin’s
effectiveness and to promote therapeutic anticoagulation20. This contrasts with a
similar study that did not find any significant drop in heparin dose or measured ACT
following ATIII administration16. Using less heparin to achieve the adequate
anticoagulation level is beneficial in preventing the potential adverse effects of using
too much heparin. One of the most dangerous complications with the use of heparin
is intracranial brain hemorrhage13.
When looking at the summary statistics between the cardiac and respiratory
group, we noted several significant differences to be interpreted. To begin, the
differences in age were statistically different. One explanation could be that the
older patients are more likely to suffer from the acute heart failure issues that
require them to be placed on ECMO. Also significant were differences between the
lengths of ECMO runs for both groups. Respiratory patients were placed on ECMO
for almost twice as long and survival was significantly lower. Both length of run and
survival may be related to the underlying pathology of these patients. Perhaps
respiratory patients have more irreversible diseases involving their lungs and other
organ systems. It is also possible that the severity of their condition is discovered
too late for ECMO to be of considerable benefit. The cardiac patients possibly suffer
from issues that are more temporary and reversible.

33
The other variables measured did not show statistically significant
differences. There was no significance measured between antithrombin
replacement and ACTs, length of stay, circuit change outs, or the presence of clots in
the circuit. ACTs can be affected by a number of variables which might explain the
wide variability and lack of correlation. More patients would need to be studied in
order to determine any significant results.
This study has various limitations. Being retrospective, it is not possible to
control factors such as whether or not patients receive ATIII, timing and quantity of
dose, and timing of ATIII activity level measurements. ATIII dose was subject to the
attending physician, therefore timing and dose were not necessarily standardized or
consistent. Due to the fact that not all patients were given ATIII on a daily basis, we
had to standardize dosing by dividing the total amount of ATIII given by how many
days the patients were on ECMO. Also, at times the physician recommended dose
would be rounded up to a full vial to reduce waste of an expensive product. In
future use of antithrombin III, it would be beneficial to standardize dosing based on
weight of the patient (kg). Given these patients are very sick, other comorbidities
may be confounding to the results. Obviously, we cannot control the unlimited
number of potential differences between the patient’s etiologies.
34
CONCLUSION
Summary
The management of anticoagulation and bleeding together is a complex issue.
Without sufficient anticoagulation, there can be consumption of coagulation factors
and platelets that can eventually lead to worsening of bleeding16. The present study
suggests that ATIII replacement is necessary while patients are placed on an extra-‐
corporeal membrane oxygenation device. We know that ATIII will consistently be
utilized in the presence of heparin and also that there will be a drop in ATIII due to
hemodilution and factor activation from the circuit. In addition, as the results
suggest, blood product use increases significantly without ATIII administration.
Also, the cardiac group data show that it is possible that excessive ATIII is
associated with blood loss as well as measured by pRBC replacement. For this
reason, we can conclude that there is an ideal therapeutic range for ATIII
administration.
The benefits of this study are widespread. Most importantly, the ability to
reduce bleeding would be beneficial. Reduction in the use of blood products via
reduction in the amount of bleeding is advantageous to the patient by preventing
the potential for transfusion reactions. Finally, reducing blood product use may be a
financial incentive, despite the relatively high cost of antithrombin III.
35
Future Directions
There is great potential for future research to be performed in support of this
data. It would be beneficial to require measurement of ATIII levels pre-‐cannulation
to know what level patients have initially, in order to prevent excessive drops for
reasons discussed previously, in patients that are dependent on heparin. This will
benefit patients that have heparin resistance due to prior heparin therapy, and most
importantly, those with decreased ATIII availability due to liver dysfunction as a
result of sepsis or other disorders. In this way, we can also understand the average
percentage drop in ATIII levels that can be expected from the initiation of ECMO.
Also, establishing a protocol to standardize dosing would be beneficial to evaluate
the effect of ATIII in a prospective manner. To date, no study has been performed to
measure ATIII in ECMO patients, as it has been done successful in cardiopulmonary
bypass patients. Eventually, we can extrapolate our findings to other patients such
as those that are on total artificial heart and ventricular assist devices.
36
APPENDIX
Figure 1. Comparing heparin drip rate at first dose of ATIII and 24 hrs later.
Heparin at Dose
Heparin 24hr After
Mean 803 594.0703704 SE 138.203544 137.3237277
T-test 0.032828587

37
Figure 2. RBC Infusions measured at the units of RBCs given per day compared with ATII Replacement
RBC
NO ATIII ATIII MEAN 7.02 2.81 SEM 1.25 0.30 T-Test 2.20617E-05

38
Figure 3. Platelet Infusions measured at the units of Platelets given per day compared with ATII Replacement
Platelets
NO ATIII ATIII MEAN 2.93 0.77 SEM 0.37 0.17 T-Test 3.18491E-05
39
Figure 4. FFP Infusions measured at the units of FFP given per day compared with ATII Replacement
FFP
NO ATIII ATIII MEAN 4.61 1.11 SEM 1.26 0.21 T-Test 1.11657E-05

40
Figure 5.
41
Figure 6.

42
Table 1. Summary statistics for cardiac and respiratory
Parameter Units Respiratory Cardiac P value n 20 21 ns
Age years 39.4 ± 3.3 57.7 ± 2.7 0.04 Weight Kg 84 ± 6 92 ± 4 ns
BSA M2 1.9 ± 2.0 2.0 ± 0.1 ns Gender % males 50 68 ns Length days 14.1 7.4 0.0383
Survival % 35 58 0.0002
43
Table 2.
ATIII Levels
Average ATIII Post Initiation (%)
Average ATIII Level/day (%)
Cardiac 47.7 ± 5.8 86.5 ± 1.4
Respiratory 67.3 ± 8.2 88.2 ± 5.5
44
REFERENCES
1. Allen, S., Holena, D., McCunn, M., et al. (2009). A review of the fundamental
principles and evidence base in the use of extracorporeal membrane oxygenation (ECMO) in critically ill adult patients. Journal of Intensive Care Medicine, (26)1, 13-‐26.
2. Bartlett, R.H. & Gattinoni, L. (2010). Current status of extracorporeal life support
(ECMO) for cardiopulmonary failure. Minerva Anesthesiologica, (76), 534-‐540.
3. Linhardt, R.J. Heparin: An important drug enters its seventh decade. Chemistry &
Industry, (2), 45-‐50. 4. Chesterman, C.N., Chong, B.H. (1993).Uses of heparin. British Medical Journal,
306:871. 5. Oliver, W.C. (2009). Anticoagulation and Coagulation Management for ECMO.
Semin Cardiothoracic Vasc Anesth, 13, 154-‐174. 6. Hensley, F.A., Martin, D.E., & Gravlee, G.P. (2008). Coagulation management
during and after bypass. A Practical Approach to Cardiac Anesthesia (Fourth Ed., pp. 494). Philadelphia, PA: Lippincott Williams & Wilkins, a Wolters Kluwer Business.
7. Lefkovitz, J & Topol, EJ. (1994). Direct thrombin inhbitors in cardiovascular
medicine. Circulation, 90, 1522-‐1536. 8. Levy, J.H., Montes, F., Szlam, F. & Hillyer, C.D. (2000). The In Vitro effects of
antithrombin III on the activated coagulation time in patients on heparin therapy. Anesthesia & Analgesia, 90 (5), 1076-‐1079.

45
9. Hustead, V. & Kurth, M.H. (2006). Clinical Guideline: Antithrombin III. ECMO Neonatal Clinical Management. Minnesota Neonatal Physicians PA.
10. Toomasian, JM. & Bartlett, RH. (2011). Hemolysis and ECMO pumps in the 21st
century. Perfusion, 26(1), 5-‐6. 11. Betrus, C., Remenapp, R., Charpie, J., et al. (2007). Extracorporeal Membrane
Oxygenation and Continuous Renal Replacement Therapy. Ann Thorac Cardiovasc Surg, 13(6), 378-‐383.
12. Arnold PA, Jackson, S., Wallis, J., et al. (2001). Coagulation factor activity during
neonatal extra-‐corporeal membrane oxygenation. Intensive Care Med, (27), 1395-‐1400.
13. Khaja, W.A., Bilen, O., Lukner, R.B., et al. (2010). Evaluation of Heparin Assay for
Anticoagulation Management in Newborns undergoing ECMO. American Journal of Clinical Pathology, 134, 950-‐954.
14. Agati, S., Ciccarello, G., Salvo, D, et al. (2006). Use of a Novel Anticoagulation
Strategy During ECMO in a Pediatric Population: Single Center Experience. ASAIO Journal, (52), 513-‐516.
15. Sievert, Alicia. Improvement in long-‐term ECMO by detailed monitoring of
anticoagulation: a case report.
16. Neibler, R.A., Christenson, M., Berens, R., et al. (2011). Antithrombin Replacement During Extracorporeal Membrane Oxygenation. Artificial Organs, (35)11, 1024-‐1028.
17. Nankervis, C.A., Preston, T.J., Dysart, K.C., et al. (2007). Assessing Heparin Dosing
in Neonates on Venoarterial Extracorporeal Membrane Oxygenation. ASAIO Journal, (53), 111-‐114.

46
18. Avidan, M.S., Levy, J.H. (2005). Recombinant human antithrombin III restores heparin responsiveness and decreses activation of coagulation in heparin-‐resistant patients during cardiopulmonary bypass. The Journal of Thoracic and Cardiovascular Surgery, (130), 107-‐113.
19. A.H., Willett, L.W., Fristoe, L., et al. (1995). Coagulation Monitoring during Extracorporeal Membrane Oxygenation: The Role of Thromboelastography. The Journal of Extra-Corporeal Technology, 27, 137-‐145.
19. Avidan, M.S., Levy, J.H., Scholz, J., et al. (2005). A Phase III, Double-‐blind, Placebo-‐
controlled, Multicenter Study on the Efficacy of Recombinany Human Antithrombin in Heparin-‐resistant Patients Scheduled to Undergo Cardiac Surgery Neccesitating Cardiopulmonary Bypass. Anesthesiology, 102, 276-‐284.
20. Koster, A., Chew, D., Kuebler, W., et al. (2003). High antithrombin III levels
attenuate hemostatis activation and leukocyte activation during cardiopulmonary bypass. The Journal of Thoracic and Cardiovascular SurgeryI, (126), 906-‐7.