feline heartworm: a threat to the travelling cat
TRANSCRIPT
Dirofilaria immitis is a filarial heartworm primarily ofcanids and is endemic in Australia, Southern Europe,all US states and many Asian and African counties. Itis a significant cause of heart disease in domestic dogsand although it is not endemic in the UK, increasingnumbers of dogs from the UK are being exposed toinfection through travel to endemic countries on thepet passport scheme. This has increased awareness ofthe disease among UK veterinarians when dealingwith heart disease in dogs which have travelledabroad but what is much less well recognised is thatcats travelling to these countries are also at risk ofserious disease from heartworm infection.
LIFE CYCLE AND EPIDEMIOLOGY
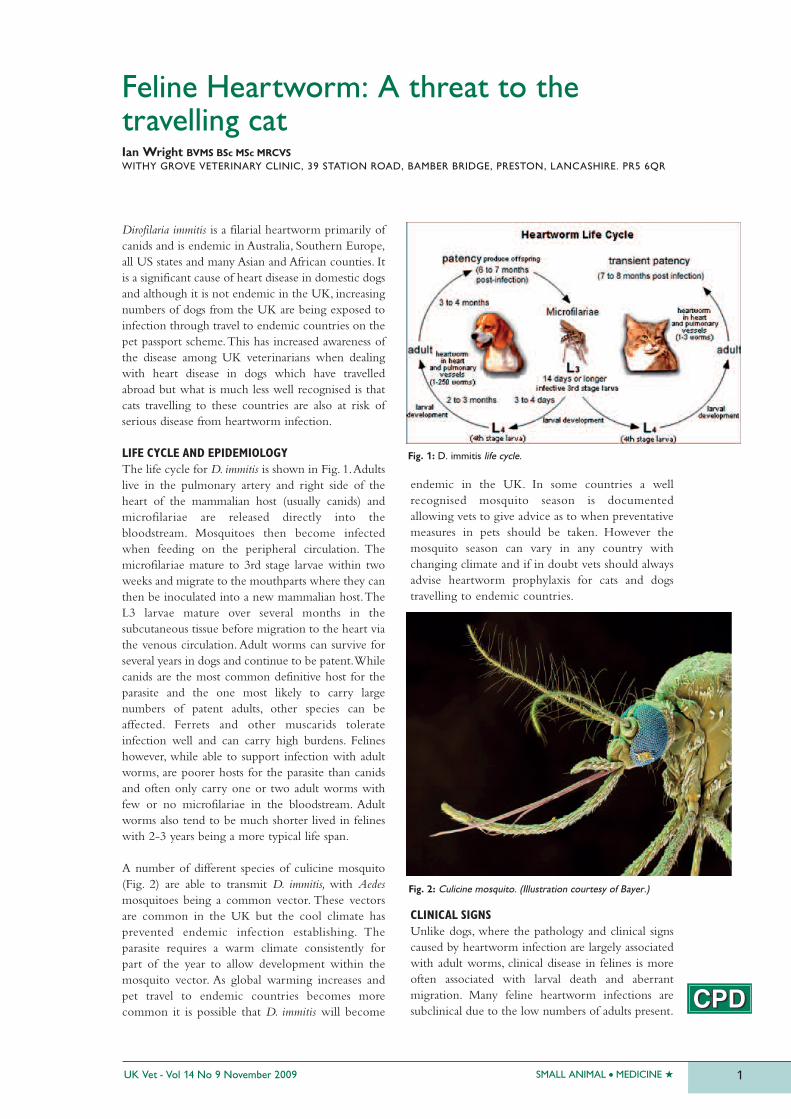
The life cycle for D. immitis is shown in Fig. 1. Adultslive in the pulmonary artery and right side of theheart of the mammalian host (usually canids) andmicrofilariae are released directly into thebloodstream. Mosquitoes then become infectedwhen feeding on the peripheral circulation. Themicrofilariae mature to 3rd stage larvae within twoweeks and migrate to the mouthparts where they canthen be inoculated into a new mammalian host. TheL3 larvae mature over several months in thesubcutaneous tissue before migration to the heart viathe venous circulation. Adult worms can survive forseveral years in dogs and continue to be patent. Whilecanids are the most common definitive host for theparasite and the one most likely to carry largenumbers of patent adults, other species can beaffected. Ferrets and other muscarids tolerateinfection well and can carry high burdens. Felineshowever, while able to support infection with adultworms, are poorer hosts for the parasite than canidsand often only carry one or two adult worms withfew or no microfilariae in the bloodstream. Adultworms also tend to be much shorter lived in felineswith 2-3 years being a more typical life span.
A number of different species of culicine mosquito(Fig. 2) are able to transmit D. immitis, with Aedesmosquitoes being a common vector. These vectorsare common in the UK but the cool climate hasprevented endemic infection establishing. Theparasite requires a warm climate consistently forpart of the year to allow development within themosquito vector. As global warming increases andpet travel to endemic countries becomes morecommon it is possible that D. immitis will become
endemic in the UK. In some countries a wellrecognised mosquito season is documentedallowing vets to give advice as to when preventativemeasures in pets should be taken. However themosquito season can vary in any country withchanging climate and if in doubt vets should alwaysadvise heartworm prophylaxis for cats and dogstravelling to endemic countries.
CLINICAL SIGNS
Unlike dogs, where the pathology and clinical signscaused by heartworm infection are largely associatedwith adult worms, clinical disease in felines is moreoften associated with larval death and aberrantmigration. Many feline heartworm infections aresubclinical due to the low numbers of adults present.
SMALL ANIMAL � MEDICINE �UK Vet - Vol 14 No 9 November 2009 1
Ian Wright BVMS BSc MSc MRCVSWITHY GROVE VETERINARY CLINIC, 39 STATION ROAD, BAMBER BRIDGE, PRESTON, LANCASHIRE. PR5 6QR
Feline Heartworm: A threat to thetravelling cat
Fig. 1: D. immitis life cycle.
Fig. 2: Culicine mosquito. (Illustration courtesy of Bayer.)
However, in clinical cases many different clinicalsigns can occur, making recognition of the diseasedifficult. Common clinical signs include:� Sudden death: This is most commonly caused
by pulmonary embolism when the death of anadult worm occurs. Adult worm death is morecommon in cats and often results in acutecomplications
� Caval syndrome: This occurs less commonly incats than in dogs as fewer adult worms arepresent. The syndrome is caused by groups ofadult worms suddenly moving from thepulmonary artery into the right ventricle andatrium. Repeated migrations cause a tricuspidvalve incompetence leading to acute right-sidedheart failure. A right-sided systolic heart murmuris accompanied by anorexia, weakness, dyspnoea,a jugular pulse and a weak femoral pulse,anaemia, haemoglobinuria and vomiting
� Acute dirofilariosis: Acute disease other thancaval syndrome is caused by inflammatoryreaction to migrating larvae, aberrant migrationof larvae to the central nervous system and spineor pulmonary embolism. Typical acute signsinclude collapse, dyspnoea, tachycardia, syncope,diarrhoea, vomiting and seizures
� Chronic dirofilariosis: Chronic disease can alsooccur due to inflammatory responses tomigrating larvae and aberrant migration. Thesetend to be respiratory in nature and includecoughing, dyspnoea, lethargy, anorexia andvomiting. Chylothorax has also occurred in somecases. The chronic nature of the respiratory signsoccurring sometimes months after travel caneasily be confused with feline asthma.
DIAGNOSIS
A history of travel to a heartworm endemic countryaccompanied by relevant clinical signs should provokesuspicion of clinical heartworm infection. This can beconfirmed at post mortem when adult worms arepresent in the right chambers of the heart and thepulmonary artery. The low numbers of adult wormspresent makes diagnosis in infected cats more difficultthan in the dog but several diagnostic tests are available:� Examination of blood for microfilariae: Direct
smears are an insensitive method of diagnosis soseveral techniques have been developed toconcentrate the microfilariae beforeexamination. These include filtration methods,Knott’s test (a form of sedimentation test) andexamination of the buffy coat produced bymicrohaematocrit centrifugation. These are alluseful diagnostic methods in the dog and carriedout by many labs or in house at veterinarysurgeries. Unfortunately they are extremelyinsensitive in the cat where few or nomicrofilariae are present in the bloodstream. Thisis due to the low numbers of adult worms whichcats carry. If only one adult worm is present or ifthe adult worm population is all male,microfilariae will not be present in the
SMALL ANIMAL � MEDICINE � UK Vet - Vol 14 No 9 November 20092
bloodstream. Even if microfilariae are present,microfilaraemias are transient with themicrofilariae only being present in the peripheralbloodstream when local mosquito populationswould be feeding. This adaptation by the parasitemakes repeat blood testing for microfilariaeworthwhile in the dog but not in cats, wheremicrofilaraemias may be difficult to detect or notpresent at all. If microfilariae are detected, thelarvae must be distinguished from D. repenswhich is a far more common species found incats but rarely pathogenic
� Radiology: Thoracic radiographic changes infeline heartworm patients are notpathognomonic and not always present. Diffuseinterstitial patterns are sometimes seen due tomigrating larvae. Right sided heart enlargementand enlargement of the pulmonary arteries,particularly the caudal lobar arteries may also beseen in feline cases
� Ultrasound examination: The cuticles of adultheartworms are highly echogenic and so inexperienced hands echocardiography can be avery sensitive and specific diagnostic procedure.The worms appear as short segmented parallellines. However the ultrasonographer must followthe caudal pulmonary arteries to theirbifurcation to be sure of a negative diagnosis andinexperienced operators can easily miss worms asso few are present
� Routine biochemistry: Increases in creatininekinase, urea, alanine transferase and alkalinephosphatase are all present in severe canine andfeline clinical cases and are associated withdamage to the heart and secondary damage tothe liver and kidneys
� Antigen serology: This test is considered to be the gold standard in the living caninepatient. It is highly specific in identifying thecurrent presence of adult worms and is alsohighly sensitive in dogs. Although it is still ahighly specific test in cats, it is much lesssensitive with as few as 50 – 80% of positivecases being identified. This is because the testdetects antigens in uterine secretions produced by female worms and a significantproportion of heart worm infections in cats aremale only infections. Cases in cats caused bymass or aberrant larval migration will also notbe detected. This limits its use in the felinepatient and as a result antibody testing is often used
� Antibody serology: This is the most sensitiveheartworm test available for diagnosis in theliving feline patient. Antibodies are produced inresponse to larvae and adult worms. Like mostantibody tests, a positive result only indicates pastor present exposure to infection rather thancurrent infection causing disease but a positiveresult in combination with relevant clinical signsand/or radiographic changes is stronglyindicative of heartworm disease.

tREAtMENt
Treatment of clinical heartworm disease in catsvaries from treatment in dogs in that the use ofadulticide anthelmintics does not significantlyincrease survival rate or increase the resolution timeof clinical signs. Surgical removal of the adults hasbeen performed in cats but would only beconsidered where obstruction was occurring, such asin caval syndrome. Treatment in cats consists ofcontrolling inflammation and supportive treatment.Typical treatments are:� Corticosteroids: Prednisolone at 1-2 mg/kg q
24h to control inflammation generated inresponse to migrating larvae. If the clinicalresponse to treatment is favourable the dose canbe reduced weekly and the patient weaned offover a 4 week period. In some cases, signsfrequently reoccur and these patients need to bemaintained on prednisolone at the lowesteffective dose. In cases of severe acute dyspnoeathen shock levels of dexamethasone may need tobe administered (2 mg/kg iv or im) beforemaintenance on prednisolone
� Supportive treatment: Oxygen, IV fluids andbronchodilators are all useful in helping tostabilise acute patients, particularly those withacute dyspnoea
� Antibiotics: These are indicated in cases wheresecondary bacterial infection is suspected.
PREvENtION OF HEARtWORM INFECtION
IN CAtS IN CAtS
The mosquito vector is most active at dawn and duskso avoiding pets being outside at these times can helpto limit exposure. However, the vector will enterbuildings and can breed in small bodies of water suchas ponds, discarded rubbish, tyres filled withrainwater or hotel water features. Large populationscan therefore build up in urban areas withoutinvasion from surrounding rural areas. As a result theonly reliable method of preventing infection ischemical prophylaxis. Fortunately larvae areextremely sensitive to the macrocyclic lactoneproducts and die rapidly upon contact in thebloodstream before a microfilaraemia can beestablished. This makes monthly administration of amacrocylic lactone an almost 100% effectiveprophylactic measure and should be recommendedto any client taking a cat to an endemic area.Treatment should be started before travel andcontinued while in the endemic country. Unlikedogs, should treatment be interrupted, it is safe andadvisable to restart prophylactic treatment withouttesting for the presence of microfilariae in thebloodstream first. This is because even if microfilariae
are present then numbers are rarely high enough tocause pathology associated with worm death. Thethree macrocyclic lactone products that are licensedand safe for prophylactic use in UK cats are:� Stronghold® – containing selamectin � Advocate® – containing moxidectin � Milbemax® – containing milbemycin oxime.
All of these agents are equally effective individuallyand should not be used in combination. Usedmonthly they will prevent clinical heartworm diseasein the travelling cat but for returning unprotectedcats and with an increasing risk of D. immitisbecoming endemic in the UK, veterinarians in thiscountry will need to become increasingly vigilant inregard to feline heartworm disease.
SMALL ANIMAL � MEDICINE �UK Vet - Vol 14 No 9 November 2009 3
C O N t I N U I N G P RO F E S S I O N A LD E v E L O P M E N t S P O N S O R E D B YB AY E R A N I M A L H E A Lt H
1. Which arthropod acts as a vector of feline
heartworm disease:
a. Ixodes ticks
b. Sand flies
c. Culicoides midges
d. Mosquitoes
e. Fleas
2. How long do adult heartworms commonly live for
in feline hosts:
a. 2-3 weeks
b. 2-3 months
c. 2-3 years
d. 5-7 months
e. 5-7 years
3. Which of the following anthelmintics is not
effective as a monthly prophylactic against
D. immitis in cats?
a. Fenbendazole
b. Selamectin
c. Moxidectin
d. Milbemycin oxime
These multiple choice questions are based on the abovetext. Answers appear on page 67.