feeding method and rehospitalization in newborns less than 1 month of age
TRANSCRIPT

PDFlib PLOP: PDF Linearization, Optimization, Protection
Page inserted by evaluation versionwww.pdflib.com – [email protected]

70 JOGNN Volume 34, Number 1
CLINICAL RESEARCH
Feeding Method and Rehospitalization in Newborns Less Than 1 Month of AgeMarybeth Tyler and Pam Hellings
Objective: To examine the relationship betweenfeeding method and hospitalization in a group ofnewborns under 1 month of age.
Design: Retrospective chart review based onadmission diagnoses.
Setting: Academic Medical Center and TertiaryChildren’s Hospital in the same northwest city.
Patients: 143 newborns divided into threegroups based on feeding method at hospital admis-sion: breastfed, bottle-fed, and breastfed with supple-ments.
Results: A nearly equal number of males andfemales who were just as likely to be first born as laterborn experienced a mean weight loss of 8.5% andwere hospitalized an average of 4.4 days. The breast-fed and supplemented newborns were younger andexperienced greater weight loss, and the majority hadno positive findings with the diagnostic workups. Theyresponded quickly to increased caloric intake. Thebottle-fed newborns had a higher incidence of posi-tive diagnostic results and a longer hospital stay.
Conclusions: The results of this study support theobservation that many healthy but hungry breastfednewborns are being hospitalized. Other than breast-feeding difficulties, most newborns had few problemsbeyond hyperbilirubinemia, which may be exacerbat-ed by inadequate feeding. The monetary and psycho-logical costs of unnecessary hospitalizations and thepotential for early discontinuation of breastfeedingmay be preventable. JOGNN, 34, 70-79; 2005.DOI: 10.1177/0884217504272813
Keywords: Bottle feeding—Breastfeeding—Dehydration—Failure to thrive
Accepted: September 2003
Clinical experience as lactation specialists provid-ing care for families at all stages of breastfeeding hasgenerated some interesting observations regardingnewborns who required rehospitalization for failureto thrive or dehydration. It seems that many of thesebreastfed newborns were not physiologically ill.Their problems appeared to be related to conditionsof inadequate milk intake due either to decreasedmaternal milk supply or poor breastfeeding tech-nique. The newborns lost weight, became dehydrat-ed, developed exaggerated hyperbilirubinemia, ordisplayed sepsis-like symptoms. They respondedquickly to receiving adequate calories through acombination of improved breastfeeding technique,stimulation of mother’s milk supply, supplementalfeeds, and support and education for the mother.The formula-fed newborns appeared to have otherdiagnoses that were not as easily resolved byincreased caloric intake. More data about these new-borns are required to examine the relationshipbetween method of feeding and failure to thrive.
The purpose of this study was to explore the rela-tionship between feeding method (bottle or breast)and failure to thrive, requiring hospitalization in agroup of term newborns under 1 month of age.Reviewing the records of newborns admitted forfailure to thrive, may provide additional under-standing of the relationship between feeding issuesand the health status of the newborn for both breast-fed and formula-fed babies. Knowledge of feedingmethod and outcomes may demonstrate that somehospitalizations and diagnostic evaluations areunnecessary or yield no additionally helpful infor-mation. The results may also provide additional evi-dence supporting comprehensive postpartum fol-

January/February 2005 JOGNN 71
low-up for new mothers and newborns, especially forthose who initiate breastfeeding.
Review of the Literature
Breast milk is the ideal food for the human infant. Ben-efits of breast milk feedings include the biological speci-ficity of human milk, which changes and evolves as theinfant grows; the immunological benefits of breast milk;decreased risk of allergy; decreased incidence of suddeninfant death syndrome; and decreased frequency andseverity of many illnesses in the infant period (AmericanAcademy of Pediatrics, Work Group on Breastfeeding,1997; Dewey, Heinig, & Nommsen-Rivers, 1995;Lawrence, 1999; Neifert, 2001). In addition to reports onhealth care costs associated with not breastfeeding, Rior-dan (1997) and Walker (1993) reported on some of therisks of formula feeding, including increased incidence ofotitis media, increased incidence of lower respiratory tractinfection, increased incidence of diarrheal illness,decreased bioavailability of nutrients in formula, andincreased cost.
Breastfeeding is a learned skill for both mother andinfant. When it is not going well, the infant may receiveinadequate calories and fail to gain or even lose weight.This weight loss may be severe enough to require hospi-talization. In addition to increased health care costs asso-ciated with a potentially preventable hospitalization, anadditional negative outcome may be the early discontinu-ation of breastfeeding.
Several researchers have examined the rehospitaliza-tion of breastfed infants. Hall, Simon, and Smith (2000)reviewed the charts of 125 breastfed term neonates, lessthan 2 weeks of age, who were admitted to a children’shospital over a 2-year period with diagnoses of hyper-bilirubinemia, dehydration, or feeding problems. Themajority of the newborns were readmitted between 4 and6 days of age. Forty-three percent of the newborns wereadmitted with hyperbilirubinemia only. Thirty-nine per-cent of the newborns had weight loss ≥ 12% or a serumsodium ≥ 145 mmol/L. They also noted that 18% of thenewborns had hypernatremia and weight loss withouthyperbilirubinemia, and 21% had all three conditions.The mean parity was 1.7, reflecting that these problemswere not limited to first-time mothers. Ninety-six percentof the newborns were still breastfeeding at the time of dis-charge from the hospital.
Livingstone, Willis, Abdel-Wareth, Thiessen, andLockitch (2000) reviewed a group of 21 breastfed new-borns less than 14 days of age with hypernatremic dehy-dration. Serum sodium levels ranged from 146 to 207mmol/L, and newborn weight loss ranged from 8% to30% (mean 18.2%). In each case, maternal or newbornfactors contributing to ineffective breastfeeding wereidentified: failure of lactogenesis, failure of galactopoiesis,
and inefficient milk transfer. The authors noted that manyof these situations could have been prevented with in-hos-pital screening for maternal and newborn risk factors andwith early postpartum follow-up.
Lukefar (1990) reviewed the records of 38 breastfedneonates who experienced failure to thrive. He concludedthat 26 of 28 newborns less than 1 month of age had nounderlying illness. However, 5 of the 10 infants between1 and 6 months of age who did not thrive at the breastwere experiencing other organic illnesses.
Pascale, Brittian, Lenfesty, and Jarrett-Pulliam (1996)reviewed the cases of 8 neonates readmitted to an inten-sive care nursery over a 5-month period. All had been dis-charged from the hospital as healthy breastfeeding new-borns but were readmitted within 48 hours with adiagnosis of either hyperbilirubinemia or possible sepsis.A primary diagnosis at subsequent discharge was milddehydration related to inadequate intake. Six of the new-borns were exclusively breastfeeding at discharge, 1 new-born was receiving pumped milk via a bottle, and 1 new-born was formula fed.
Kini, Zahn, and Werlin (1995) presented 3 term infantsadmitted with serum sodium levels ranging from 173 to180 mmol/L. Weight loss from birth weight ranged from25% to 29%. All 3 infants had negative septic workupsand were successfully rehydrated. All of the mothers dis-continued breastfeeding.
Cooper, Atherton, Kahana, and Kotagal (1995) dis-cussed a group of 5 breastfeeding infants with severe mal-nutrition and hypernatremia who were admitted to theirtertiary care center over a 5-month period. The meanweight loss on readmission was 23%, and the mean ini-tial sodium was 185 mmol/L. Three of these infants suf-fered significant complications. Two developed multiplecerebral infarctions, and 1 infant required amputation ofa leg due to an iliac artery thrombus. These sequelae weredetermined to be related to severe dehydration and hyper-natremia, not preexisting pathology. Follow-up neurolog-ical examinations were normal on 4 infants, but 1 demon-strated unilateral decreased tone at 9 months of age.
Numerous case reviews (Chilton, 1995; Gorman,1994; Helliker, 1994; Kaplan, Siegler, & Schmunk, 1998;Newman, 1996) detailed the events associated with sig-nificant weight loss and hypernatremia in a total of 8breastfed infants. Three infants recovered well, with 1returning to full breastfeeding. However, the other 5included two deaths from severe hypernatremic dehydra-tion, one stroke, one dehydration-induced brain damage,and one with significant truncal hypotonia and grossmotor delays at 8 months.
Escobar et al. (2002) reported on 110 infants admittedwithin 15 days of discharge with ≥ 12% weight loss orserum sodium of ≥ 150 MEq/L. These infants were allcared for by a health maintenance organization, whichprovides newborn follow-up care according to the Amer-

72 JOGNN Volume 34, Number 1
ican Academy of Pediatrics guidelines (American Acade-my of Pediatrics, Committee on Fetus and Newborn,1995). The care includes uncomplicated antepartum,intrapartum, and postpartum courses for both motherand baby; minimum 48-hour hospital stay after vaginaldelivery; and family contact with a health care provider48 to 72 hours after hospital discharge. The study foundthat although the incidence of hospitalization for dehy-dration may not have decreased, the incidence of serioussequelae was rare. Only 1 of these infants showed evi-dence of possible neurological problems at 24 to 36months after discharge. They concluded that the timelyfollow-up available to these HMO patients was essentialto preventing severe dehydration in these infants.
There was no similar literature describing the course ofevents for formula-fed infants hospitalized for failure tothrive, hyperbilirubinemia, or poor feeding.
In summary, the literature reveals numerous descrip-tions of cases with diagnoses resulting in the rehospital-ization of breastfed infants. In some cases, the outcomewas good both for the infants and for breastfeeding.However, there were several notable exceptions.
Methods
Data were collected via a retrospective chart review ofrecords of newborns less than 1 month of age who werereadmitted to two different facilities—an academic med-ical center (AMC) and a private tertiary children’s hospi-tal (TCH) in the same northwestern city. The institution-al review boards of both facilities approved the studyproposal. Data were gathered first at the AMC and laterat the TCH. Admission diagnoses used to identify chartsincluded failure to thrive, poor feeding, slow weight gain,hyperbilirubinemia, hypernatremia, and rule-out sepsis.The Health Information Services departments pulled thecharts of neonates who met the study criteria. Charts con-tinued to be identified until a sample size of approxi-mately 140 was identified with a plan to have 70 in eachof the two groups—breastfeeding and bottle feeding.Newborns with known underlying conditions such ascongenital heart disease, surgical conditions, or congeni-tal anomalies were eliminated from the study, in additionto those with a hospital stay of less than 12 hours onreadmission, gestational age less than 37 weeks, or a sin-gle diagnosis of hyperbilirubinemia.
Data were recorded on the following: newborn age;gender; diagnoses at admission and discharge; birthweight; birth order; method of feeding at admission, dur-ing hospitalization, and at discharge; admission and dis-charge weight; and length of hospital stay. Frequenciesand results of laboratory tests including lumbar puncture,blood chemistries, hematologies, blood cultures, anddiagnostic procedures, were recorded. Subspecialty con-sults and lactation consults were noted. Confidentiality
was maintained by number coding the data collectionforms.
The data were analyzed with the CRUNCH statisticalpackage (Crunch Software Corporation, Oakland, CA).Frequency distributions, percentages, and means werecalculated.
Results
General Description of SampleChart reviews were completed for 143 newborns who
met selection criteria, 73 from the AMC and 70 from theTCH. Complete newborn admission information wasavailable on 45 of the charts, as these newborns had beenborn at the study hospitals or faxed newborn recordswere available for review. The newborn history on theremaining 98 neonates was obtained from the historytaken at readmission. The total sample consisted of anearly equal number of male and female newborns whowere just as likely to be first born as later born. Theyexperienced a mean weight loss of 8.5% (range 1% to24%) below birth weight and were hospitalized an aver-age of 4.4 days (range 1–67 days).
There were some notable differences between the indi-viduals from the two facilities. The mean birth weight ofthe newborns was 3288 g for the AMC and 3606 g for theTCH. The mean weight loss on readmission was 8% forthe AMC and 10% for the TCH. The average length ofhospital stay was 6.5 days (AMC) compared to 2.2 days(TCH). These differences may be partially explained bythe larger number of newborns receiving bottle feeds fromthe AMC, who experienced longer hospitalization andweighed less at admission.
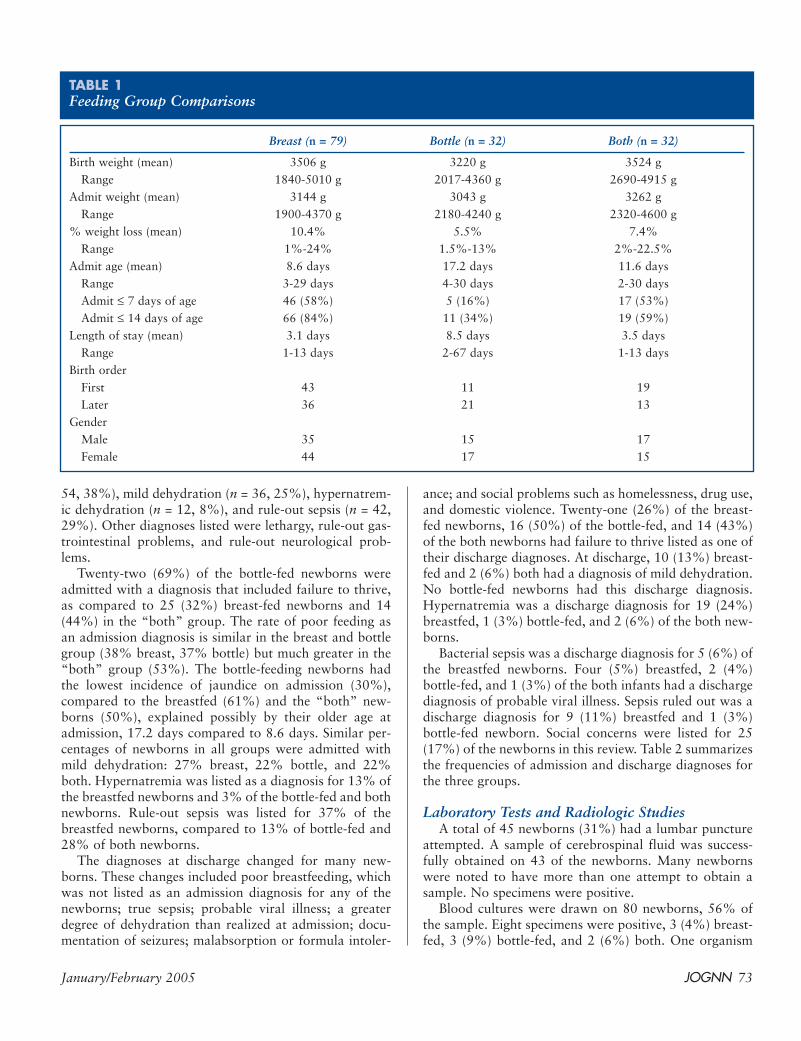
The remainder of the analysis will focus on the new-borns divided into three groups based on method of feed-ing at hospital admission: breastfed newborns, bottle-fednewborns, and those newborns receiving both breast andsupplemental formula feedings. On admission, 79 new-borns were exclusively breastfeeding, 32 newborns wereexclusively bottle-feeding, and 32 newborns were receiv-ing both breast- and bottle-feedings. The “both” new-borns ranged from those who had received supplementssince birth to those who received minimal supplementalfeeds in the hours prior to admission. It should also benoted that 4 of the 10 now exclusively bottle-fed new-borns from the TCH had started out as breastfeedingnewborns. Data describing the birth weights, admissionweights, and other variables for each of the three groupsare summarized in Table 1.
Admission and Discharge DiagnosesEach newborn had one to four diagnoses listed at
admission. Admission diagnoses included failure to thrive(n = 61, 43%), poor feeding (n = 59, 42%), jaundice (n =
January/February 2005 JOGNN 73
54, 38%), mild dehydration (n = 36, 25%), hypernatrem-ic dehydration (n = 12, 8%), and rule-out sepsis (n = 42,29%). Other diagnoses listed were lethargy, rule-out gas-trointestinal problems, and rule-out neurological prob-lems.
Twenty-two (69%) of the bottle-fed newborns wereadmitted with a diagnosis that included failure to thrive,as compared to 25 (32%) breast-fed newborns and 14(44%) in the “both” group. The rate of poor feeding asan admission diagnosis is similar in the breast and bottlegroup (38% breast, 37% bottle) but much greater in the“both” group (53%). The bottle-feeding newborns hadthe lowest incidence of jaundice on admission (30%),compared to the breastfed (61%) and the “both” new-borns (50%), explained possibly by their older age atadmission, 17.2 days compared to 8.6 days. Similar per-centages of newborns in all groups were admitted withmild dehydration: 27% breast, 22% bottle, and 22%both. Hypernatremia was listed as a diagnosis for 13% ofthe breastfed newborns and 3% of the bottle-fed and bothnewborns. Rule-out sepsis was listed for 37% of thebreastfed newborns, compared to 13% of bottle-fed and28% of both newborns.
The diagnoses at discharge changed for many new-borns. These changes included poor breastfeeding, whichwas not listed as an admission diagnosis for any of thenewborns; true sepsis; probable viral illness; a greaterdegree of dehydration than realized at admission; docu-mentation of seizures; malabsorption or formula intoler-
ance; and social problems such as homelessness, drug use,and domestic violence. Twenty-one (26%) of the breast-fed newborns, 16 (50%) of the bottle-fed, and 14 (43%)of the both newborns had failure to thrive listed as one oftheir discharge diagnoses. At discharge, 10 (13%) breast-fed and 2 (6%) both had a diagnosis of mild dehydration.No bottle-fed newborns had this discharge diagnosis.Hypernatremia was a discharge diagnosis for 19 (24%)breastfed, 1 (3%) bottle-fed, and 2 (6%) of the both new-borns.
Bacterial sepsis was a discharge diagnosis for 5 (6%) ofthe breastfed newborns. Four (5%) breastfed, 2 (4%)bottle-fed, and 1 (3%) of the both infants had a dischargediagnosis of probable viral illness. Sepsis ruled out was adischarge diagnosis for 9 (11%) breastfed and 1 (3%)bottle-fed newborn. Social concerns were listed for 25(17%) of the newborns in this review. Table 2 summarizesthe frequencies of admission and discharge diagnoses forthe three groups.
Laboratory Tests and Radiologic StudiesA total of 45 newborns (31%) had a lumbar puncture
attempted. A sample of cerebrospinal fluid was success-fully obtained on 43 of the newborns. Many newbornswere noted to have more than one attempt to obtain asample. No specimens were positive.
Blood cultures were drawn on 80 newborns, 56% ofthe sample. Eight specimens were positive, 3 (4%) breast-fed, 3 (9%) bottle-fed, and 2 (6%) both. One organism
TABLE 1Feeding Group Comparisons
Breast (n = 79) Bottle (n = 32) Both (n = 32)
Birth weight (mean) 3506 g 3220 g 3524 gRange 1840-5010 g 2017-4360 g 2690-4915 g
Admit weight (mean) 3144 g 3043 g 3262 gRange 1900-4370 g 2180-4240 g 2320-4600 g
% weight loss (mean) 10.4% 5.5% 7.4%Range 1%-24% 1.5%-13% 2%-22.5%
Admit age (mean) 8.6 days 17.2 days 11.6 daysRange 3-29 days 4-30 days 2-30 daysAdmit ≤ 7 days of age 46 (58%) 5 (16%) 17 (53%)Admit ≤ 14 days of age 66 (84%) 11 (34%) 19 (59%)
Length of stay (mean) 3.1 days 8.5 days 3.5 daysRange 1-13 days 2-67 days 1-13 days
Birth orderFirst 43 11 19Later 36 21 13
GenderMale 35 15 17Female 44 17 15

74 JOGNN Volume 34, Number 1
cultured from the breastfed group was felt to be due to ahospital-acquired infection.
Blood chemistries were obtained on 139 newborns,97% of the sample. Seventy-two (50%) of these sampleswere positive, defined for the purposes of this study asserum bilirubin ≥ 20 mg/dL, serum sodium ≥ 145 mEq/L,or other minor deviations. Sixty-two (42%) newbornshad positive specimens. Several other laboratory testswere performed, most commonly, urine culture, type andscreen, Coombs, viral workup, and blood gas. Of these,one urine culture was documented positive withEscherichia coli in a breastfed newborn. None of the viralworkups yielded a positive viral culture. However, 7 new-borns were still discharged with a diagnosis of probableviral illness.
One hundred thirty-three newborns (93%) had hema-tologic studies drawn. Fifteen samples (10%) were posi-tive due to either an abnormal white cell differential or alow platelet count. Five (6%) of the breastfed newbornsand 8 (25%) of the bottle-fed newborns had positive spec-imens.
Other diagnostic studies were performed, most com-monly radiography. Forty-three (30%) of the newbornshad a chest x-ray. Seven studies were positive, 1 (0.1%)breastfed, 5 (16%) bottle-fed, and 1 (3%) of the both
newborns. These findings are summarized in Table 3.Eight newborns had additional studies: ultrasoundsand/or CT scans of the head, renal or abdominal ultra-sounds, echocardiogram, and electroencephalogram(EEG). Of these tests, the only positive result was an EEGon a known drug-affected bottle-fed newborn. Two renalultrasounds showed transient renal pathology related tothe severity of dehydration experienced by the newborns.
Specialty Consults During HospitalizationAdditional consults were ordered on 62 newborns
(43%). Twenty-nine (37%) breastfed newborns, 16(50%) bottle-fed newborns, and 13 (40%) both new-borns had consults. The breast-fed and both newbornsaveraged 1 to 3 consults (mean 1.4), and the bottle-fednewborns had 1 to 7 consults (mean 3.3). The most com-mon consults were for specialists in pediatric infectiousdisease, lactation services, speech therapy for assistancewith feeding difficulties, and social services.
Lactation consults were completed for 72 (50%) of thenewborns. The lactation services department saw 43(54%) of the breastfed, 11 (34%) of the bottle-fed, and18 (56%) of the both newborns. The other half of themothers and newborns received no help with feedingissues beyond basic nursing care.
TABLE 2Admission Diagnoses and Discharge Diagnosis by Feeding Method on Admission
Breast Bottle Both Total
Failure to thriveAdmission 25 22 14 61Discharge 21 16 14 51
Poor feedingAdmission 30 12 17 59Discharge 7 6 8 21Poor BF at discharge 13 1 14
HyperbilirubinemiaAdmission 39 4 11 54Discharge 23 3 7 33
Mild dehydrationAdmission 22 7 7 36Discharge 10 2 12
HypernatremiaAdmission 10 1 1 12Discharge 19 1 2 22
Ruled-out sepsisAdmission 29 7 9 45Discharge sepsis 5 (bacterial) 2 (viral) 1 (viral) 4 (viral)Sepsis ruled out 9 1 10

January/February 2005 JOGNN 75
Feeding Method on Admission, During, and After Hospitalization
Of the 79 newborns who were breastfeeding at hospi-tal admission, 19 (24%) were exclusively breastfed duringthe hospitalization, 47 (59%) received both breast andsupplemental feedings, 12 (15%) were exclusively bottle-fed, and 1 received both oral and gastrostomy tube feed-ings. At discharge, only 30 (38%) of the newborns werestill exclusively breastfeeding, 22 (28%) of the newbornswere bottle-feeding, and 27 (34%) were doing both. Onenewborn continued to require a feeding tube.
Of the 32 newborns who were exclusively bottle-fed atadmission, 1 (3%) attempted exclusive breastfeeding, 22(69%) continued bottle-feeding, and 9 (28%) did a com-bination of feedings while in the hospital. At discharge,no newborns were breastfeeding, 26 (81%) were bottle-feeding, and 6 (19%) were doing both breast and bottle-feeds.
Of the 32 newborns who were admitted receiving bothbreast and supplemental feedings, 2 (6%) were exclusive-ly breastfed in the hospital, 12 (38%) were bottle-fed, and18 (56%) continued with both types of feedings. At dis-charge, 5 (16%) newborns were breastfeeding, 16 (50%)were bottle-feeding, and 11 (34%) were breast- and bottle-feeding. These findings are summarized in Table 4.
Summary
In summary, the results describing the three groups ofnewborns show many similarities, as well as some impor-tant differences. The breast and “both” newborns wereyounger at readmission and experienced a greater degreeof weight loss than the bottle-fed newborns. The majori-
ty of the breastfed and both newborns had no positiveresults with any of the diagnostic workups performed.They responded quickly to increased caloric intake andwere hospitalized an average of 3.1 days (breast) to 3.5days (both). The bottle-fed newborns were older atadmission and hospitalized for a longer time, 8.5 days.They experienced a greater frequency of diagnostic testsand consults than did the breastfed newborns.
Finally, in addition to these differences, all of the new-borns and families experienced exposure to intravenousstarts, antibiotics, phototherapy, and the disruption offamily routines. It appears that many of the hospitaliza-tions in this sample related primarily to feeding issues. It
TABLE 3Summary of Laboratory Tests and Diagnostic Studies Performed During Hospitalization
Breast Bottle Both Total
Lumbar puncture 29 8 8 45Positive result 0 0 0 0
Blood cultures 48 16 16 80Positive result 3 3 2 8
Blood chemistries 78 32 (all) 29 139Positive resulta 44 14 13 71
Hematologies 74 31 28 133Positive resultb 5 13 0 18
Diagnostic studiesChest x-ray 17 19 7 43Positive result 1 5 1 7
aBilirubin ≥ 20 mg/dL, Na+ ≥ 145mEq/L, elevated LFTs, low K+.
bAbnormal CBC, low platelets.
TABLE 4Feeding Method
Breast Bottle Both
Feeding method at admission 79 32 32Feedings during hospitalization
Breast 19 1 2Bottle 12 22 12Both 47 9 18G-tube 1
Feedings at dischargeBreast 30 0 5Bottle 22 26 16Both 26 6 11G-tube 1
Note. G-tube = gastrostomy tube.

76 JOGNN Volume 34, Number 1
is possible that some hospitalizations could have beenprevented by early assessment of the potential for prob-lems and early follow-up and management of breastfeed-ing challenges encountered in the early days postpartum.
Discussion
Discussion of ResultsThe results in this small sample regarding both the
breastfed and “both” newborns support the originalobservation that the majority of these newborns are hun-gry, not ill. The breast and both newborns appear to bemore like one another than either group compared withbottle-fed newborns in the following characteristics: birthweight (greater for breast and both), age at readmission(younger for breast and both), length of stay (shorter forbreast and both), degree of weight loss prior to admission(greater for breast and both), and frequency of diagnostictests and abnormal results (less for breast and both).
Forty-three (54%) of the newborns in the breastfedgroup, 19 (59%) of those in the both group, and 11(34%) of the bottle-fed newborns were first born. Itwould have been logical to hypothesize that a greater per-centage of breastfed newborns needing hospitalizationwould have been firstborns—due to lack of maternalknowledge regarding breastfeeding and normal newborncare. However, nothing was known about the previousbreastfeeding experience(s) of the mothers. It is possiblethat this hospitalized newborn could be her first breastfednewborn, that she had difficulties breastfeeding a previ-ous newborn, or that this newborn was her first to havebreastfeeding problems. Others have shown that bothprimiparous women and multiparous women share a sim-ilar degree of knowledge deficit in all areas during thepostpartum period. Brown and Johnson (1998) conduct-ed a pilot study regarding the benefits of postpartumhome visits for low-risk mothers and infants. Sixty-sixpercent of their study population was multiparouswomen. One of their surprise findings was an equal levelof knowledge deficit regarding self-care, newborn care,and feeding issues in the postpartum period reported byboth primiparous and multiparous women.
It is interesting to note the differences in age at admis-sion. Forty-six (58%) of the breastfed newborns were
admitted at ≤ 7 days of age, compared to 5 (16%) bottle-fed and 17 (53%) in the both group. By ≤ 14 days of age,66 (84%) of the breast-fed newborns had been readmit-ted, compared to 11 (34%) bottle-fed and 19 (59%) inthe both group. The large group of breastfed newbornsadmitted within the first 2 weeks lends support to theneed for early follow-up in order to identify and assistthose mothers and newborns experiencing feeding diffi-culties. The majority of the bottle-fed newborns (66%)were not admitted until after 2 weeks of age. These dif-ferences may again relate to the underlying hypothesisthat the bottle-fed newborns are more likely to have otherdiagnoses that impact feeding.
Feeding Group ComparisonsThe degree of weight loss experienced by the breast
and both newborns indicates a greater caloric deficit thanthe bottle-fed newborns. Many newborns were >10%below birth weight at admission, including 2 breastfednewborns who were 21% and 24% below birth weight,and 1 newborn from the both group who was 22.5%below birth weight. The greatest amount of weight loss inthe bottle-fed group was 13%. This difference might beexplained by the greater ability to regulate volume intakein the bottle-fed newborns.
Admission and Discharge DiagnosesIt is difficult to draw conclusions about similarities and
differences between the three groups of newborns basedon admission and discharge diagnoses. However, 69% ofthe bottle newborns had failure to thrive as an admissiondiagnosis, compared to 32% in the breastfed group and44% in the both group, potentially indicating that despitebeing offered adequate nutrition, the bottle-fed newbornswere unable to gain weight. It is interesting to note thatthe both newborns had an admission diagnosis of poorfeeding (53%) more often than the breastfed (38%) andbottle fed (37%) newborns. It is possible that the new-borns in the both group had earlier contact with a med-ical professional who had recommended supplementationand/or the family was aware that things were not goingwell. Both poor feeding and poor breastfeeding were list-ed as discharge diagnoses. The acknowledgement of poorbreastfeeding as a discharge diagnosis occurred with thesample collected at a later date (TCH) and may indicateincreased awareness of the need for improved breastfeed-ing support for mothers and newborns.
The admission diagnosis of mild dehydration had afairly similar distribution among the three groups, 22%to 28%. At discharge, these frequencies decreased to 13%breastfed, 6% of the both, and no bottle-fed newborns.Twelve newborns were admitted with a diagnosis ofhypernatremic dehydration, 10 breastfed (13%), 1 bottle(3%), and 1 both (3%). This number increased to 22(15%) newborns after laboratory determination of a
The breastfed and supplemented newbornswere more alike in almost all categories,
compared to bottle-fed newborns.

January/February 2005 JOGNN 77
serum sodium > 150 mEq/L. This included 9 more breast-fed newborns (24%) and 1 more of the both newborns(6%). It makes sense that the breastfed newborns experi-enced a greater degree of both mild and hypernatremicdehydration than either the bottle-fed or both infantsbecause presumably the latter two groups had beenoffered a greater amount of fluid prior to admission—even if only short term for the both group.
Although 45 newborns were admitted with a diagnosisof rule-out sepsis, only 8 blood cultures and 1 urine cul-ture were positive. Five breastfed newborns had a dis-charge diagnosis of bacterial sepsis. This included the 3breastfed newborns with positive blood cultures, 1 ofwhich was felt to be a hospital-acquired infection, thenewborn with a positive urine culture, and another new-born with a negative culture. The other 5 newborns withpositive blood cultures, 3 bottle-fed and 2 from the bothgroup, did not have a discharge diagnosis of sepsis. Thereasoning for these discrepancies was unclear from themedical records. Seven newborns were discharged with adiagnosis of probable viral illness, although they were allculture negative.
Laboratory Tests and Radiologic Studies
The newborns experienced multiple invasive proce-dures during hospitalization. Forty-five spinal taps wereperformed. Results were negative on the 43 successfullyobtained samples. Eighty newborns had venipuncture forblood culture. There were 8 positive samples. Concerns inthe perinatal period that could have indicated illness inthese newborns were not apparent from the records. Oneof these newborns was readmitted to the hospital the dayafter the newborn discharge.
Ninety-seven percent of the total sample had eithervenipuncture or heel stick phlebotomy for hematologicand/or chemical analysis. Seventy-one (51%) of thechemistries were abnormal (mostly elevated serum sodi-um or bilirubin), and 18 (13.5%) CBCs were abnormal.The slightly higher rate of positive blood chemistries inthe breastfed group (56%) compared to 44% bottle and40% both may be explained by a slightly higher degree of
dehydration and hyperbilirubinemia secondary to poorfeeding. The low degree of positive CBCs in the breastfedgroup (7%) and absence of positive CBCs in the bothgroup support the position that most of these newbornswere not ill. The bottle-fed newborns had 42% positiveCBC results.
Radiographic studies were performed more than twiceas often in the bottle-fed newborns. The higher rate of x-ray and the higher incidence of a positive result may indi-cate a higher level of pathology in these newborns.
At least 25% of the newborns had urine cultures. Ofthese, only 1 culture was positive in a breastfed newbornwho was 18 days of age at admission. It is interesting thatthis newborn was not blood culture positive. Regardlessof the urine culture, this baby warranted attention longbefore the hospital admission. The newborn was 8%below birth weight at the 2-week checkup and 19%below birth weight at a 3-week weight check. The new-born was admitted to the hospital with a diagnosis of fail-ure to thrive. It is not clear if the newborn was more sus-ceptible to infection because of its compromisednutritional status or if the newborn was not feeding wellbecause of the urinary tract infection.
Specialty ConsultsThe higher percentage of bottle-fed newborns receiving
specialty consults and the fact that they received moreconsults per newborn may indicate potential problemsbeyond simple feeding issues. However, the severity of thenonfeeding diagnoses is not clear.
Feeding Method on Admission, During, and After Hospitalization
Overall, 55% of the sample were exclusively breast-feeding (not always adequately) at hospital admission, yetonly 24% were doing so at discharge. The duration ofbreastfeeding after hospitalization for these newbornscannot be determined from this study.
Only 72 patients (50%) were seen by the lactationservices department. Intervention by a lactation specialistduring hospitalization may have improved breastfeedingsuccess during hospitalization or may have prolonged theduration of breastfeeding after discharge. It is interestingto note that 11 of the lactation consults initiated were forbottle-feeding newborns, indicating that their mothersdesired breastfeeding support and information. Thisintervention contributed to 1 bottle-fed newborn attempt-ing exclusive breastfeeding and 9 bottle-fed newbornsreceiving breast and bottle feeds while in the hospital. Atdischarge, none of the bottle-fed on admission newbornswere exclusively breastfeeding. However, 6 of the 32 bot-tle-fed on admission newborns were receiving at least par-tial breast milk feedings at the time of discharge.
Only 51% of the sample were first born,validating that all mothers and newborns face
feeding challenges in the early postpartumperiod regardless of parity.

78 JOGNN Volume 34, Number 1
Implications for Nursing PracticeThe results of this study support the need for more
comprehensive care regarding feeding issues in the peri-natal period. Feeding a newborn, whether by breast orbottle, is a learned art. Many mothers do not receive theinformation and support they need to nourish their new-borns adequately. Good support for a breastfeedingmother begins, at the very latest, during her prenatal care.Nurses in the prenatal settings are in a unique position toprovide feeding information and support to pregnantwomen. Feeding information needs to be thoroughly dis-cussed so that families can make a truly informed feedingchoice. Families need encouragement to take classes dis-cussing care of their newborn, in addition to their child-birth preparation classes. A history and physical exami-nation for breastfeeding success need to be done in the3rd trimester of pregnancy. Risk factors for inadequatemilk supply need to be addressed at this time and com-municated to the newborn’s care provider. It is possiblethat some hospitalizations in this study could have been pre-vented by early identification of risk factors for breastfeed-ing success and by early follow-up according to the Ameri-can Academy of Pediatrics guidelines (American Academy ofPediatrics, Committee on Fetus and Newborn, 1995).
Education of all levels of health professionals mustcontinue on topics including the benefits of breastfeeding,identification of risk factors that may impact successfulbreastfeeding, methods of assisting a breastfeeding moth-er and newborn, the risks of formula feeding, and ways tosupport a mother who is unable or unwilling to breast-feed. Health care providers and third-party payers mustlook at the economics of hospitalizing 1 newborn versusproviding preventive follow-up care to a large number ofmothers and newborns.
Limitations of This StudyThis convenience sample was collected at two sites in a
geographic area that historically has a high incidence ofbreastfeeding initiation (Ryan, 2002). Data were limitedto those found in the chart review process. There may beinaccurate information obtained from the family mem-bers. Comprehensive feeding histories were not well doc-umented in many charts. It is difficult to quantify the dif-ferences between breastfed newborns supplemented frombirth and those receiving supplements in the hours or daysprior to rehospitalization. The population studied did notprovide the number of bottle-fed newborns planned in theoriginal study design. Conclusions about hospitalizedbottle-fed newborns are difficult to establish becausethere were only 32 bottle-fed newborns in the sample, andsome of these began as breastfeeding newborns. Addi-tionally, organic failure to thrive may be more likely toappear later than 1 month of age. This study shows that35 newborns were exclusively breastfeeding at hospital
discharge but cannot address the duration of breastfeed-ing for these families or the adequacy of follow-up withfeeding-related issues. In addition, this study did notmeasure the degree of family disruption caused by hospi-talization of a newborn nor factors associated with thedevelopment of a vulnerable child syndrome.
Suggestions for Future ResearchTo fully understand the causes and effects of failure to
thrive and/or dehydration severe enough to warrant hos-pitalization in breastfeeding newborns would require aprospective study of many breastfeeding mothers—evaluating all aspects of the feeding process: anatomy(maternal and newborn); physiology; social support; per-tinent aspects of antepartum, intrapartum, and postpar-tum events; and detailed, intense follow-up of the motherand newborn for the 1st month of life. Another potentialstudy would be to follow a cohort of patients randomizedinto two groups. One group would receive the traditional“call if you have problems, make an appointment for thebaby in 2 weeks” care that exists for many mothers andnewborns, and the other group would receive an evalua-tion by a lactation specialist while in the hospital, a follow-up phone call within 24 hours of hospital discharge, andan outpatient visit at 48 to 72 hours postdischarge. Dif-ferences in the rate of hospitalization and type of feedingbetween the two groups at 1 month postpartum could bedocumented.
Conclusions
This study confirms the original observation that forthe most part, healthy but hungry breastfed newborns arebeing admitted to the hospital. Other than breastfeedingdifficulties, most of these newborns had few problemsother than hyperbilirubinemia, which may have beenexacerbated by the breastfeeding difficulties. The fact thatonly half of the newborns were born to primiparouswomen confirms the observation that all mothers needsupport and information in establishing a feeding rela-tionship with their newborns. Many of these hospitaliza-tions might have been prevented by early contact with ahealth care provider knowledgeable in the area of breast-feeding.
The monetary and psychological costs of unnecessaryhospitalizations and the potential for early discontinua-tion of breastfeeding—all undesirable outcomes—may be
Most breastfed newborns in this study werechallenged primarily by feeding.

January/February 2005 JOGNN 79
preventable. It is well documented that breastfed babiessave health care dollars, both in the short term and longterm (Riordan, 1997; Walker, 1993). The money spent onthese hospitalizations would have been better utilizedproviding early follow-up programs for mothers and new-borns.
Acknowledgments
Partially funded by the NAPNAP Foundation and BetaPsi chapter, Sigma Theta Tau. Special thanks to Teri Woo,RN, MS, CPNP, and Pat Scheans, RN, NNP.
REFERENCES
American Academy of Pediatrics, Committee on Fetus and New-born. (1995). Hospital stay for healthy term newborns.Pediatrics, 96(4), 788-790.
American Academy of Pediatrics, Work Group on Breastfeed-ing. (1997). Breastfeeding and the use of human milk.Pediatrics, 100(6), 1035-1039.
Brown, S., & Johnson, B. (1998). Enhancing early dischargewith home follow-up: A pilot project. Journal of Obstet-ric, Gynecologic, and Neonatal Nursing, 27(1), 33-38.
Chilton, L. A. (1995). Prevention and management of hyperna-tremic dehydration in breastfed infants. Western Journalof Medicine, 163(1), 74-76.
Cooper, W. O., Atherton, H. D., Kahana, J., & Kotagal, U. W.(1995). Increased incidence of severe breastfeeding mal-nutrition and hypernatremia in a metropolitan area. Pedi-atrics, 96, 957-960.
Dewey, K. D., Heinig, J., & Nommsen-Rivers, L. A. (1995). Dif-ferences in morbidity between breast-fed and formula-fedinfants. Journal of Pediatrics, 125(5), 696-702.
Escobar, G. J., Gonzales, V. M., Armstrong, M. A., Folck, B. F.,Xiong, B., & Newman, T. B. (2002). Rehospitalization forneonatal dehydration: A nested case-control study.Archives of Pediatric Adolescent Medicine, 156, 155-161.
Gorman, C. (1994, August 22). When breast-feeding fails. Time,63.
Hall, R. T., Simon, S., & Smith, M. T. (2000). Readmission ofbreastfed infants in the first 2 weeks of life. Journal ofPerinatology, 20, 432-437.
Helliker, K. (1994, July 22). Some mothers, trying in vain tobreast-feed, starve their infants. Wall Street Journal.
Kaplan, J. A., Siegler, R. W., & Schmunk, G. A. (1998). Fatalhypernatremic dehydration in exclusively breast-fed new-born infants due to maternal lactation failure. The Amer-ican Journal of Forensic Medicine and Pathology, 19(1),19-22.
Kini, N., Zahn, S., & Werlin, S. L. (1995). Hypernatremic dehy-dration in breast-fed infants. Wisconsin Medical Journal,94(3), 143-145.
Lawrence, R. A. (1999). Breastfeeding: A guide for the medicalprofessional. St. Louis, MO: C. V. Mosby.
Livingstone, V. H., Willis, C. E., Abdel-Wareth, L. O., Thiessen,P., & Lockitch, G. (2000). Neonatal hypernatremic dehy-dration associated with breast-feeding malnutrition: Aretrospective survey. Canadian Medical Association Jour-nal, 162(5), 647-652.
Lukefar, J. L. (1990). Underlying illness associated with failureto thrive in breastfed infants. Clinical Pediatrics, 29(8),468-470.
Neifert, M. R. (2001). Prevention of breastfeeding tragedies.Pediatric Clinics of North America, 48(2), 273-297.
Newman, J. (1996). Decision tree and postpartum managementfor preventing dehydration in the “breastfed” baby. Jour-nal of Human Lactation, 12(2), 129-135.
Pascale, J. A., Brittian, L., Lenfesty, C. C., & Jarrett-Pulliam, C.(1996). Breastfeeding, dehydration, and shorter maternitystays. Neonatal Network, 15(7), 37-43.
Riordan, J. (1997). The cost of not breastfeeding: A commen-tary. Journal of Human Lactation, 13(2), 93-97.
Ryan, A. S. (2002). Breastfeeding continues to increase into thenew millennium. Pediatrics, 110(6), 1103-1109.
Walker, M. (1993). A fresh look at the risks of artificial feeding.Journal of Human Lactation, 9(2), 97-107.
Marybeth Tyler, RN, MS, NNP, IBCLC, is neonatal practioner,Legacy Emanuel Hospital & Health Center, Portland, OR, andan instructor, Oregon Health & Science University School ofNursing, Portland, OR.
Pam Hellings, RN, PhD, CPNP, is a professor emerita, OregonHealth & Science University School of Nursing, Portland, OR.
Address for correspondence: Marybeth Tyler, RN, MS, NNP,IBCLC, Legacy Emanuel Hospital & Health Center, OregonHealth & Science University School of Nursing, Portland, OR.E-mail: [email protected].