fda 7.00 cardiovascular drugs that prolong the qt interval douglas c. throckmorton, m.d. u.s. food...
TRANSCRIPT

FDA 7.00
Cardiovascular Drugs That Prolong The QT Interval
Douglas C. Throckmorton, M.D.
U.S. Food & Drug Administration
Division of Cardio-Renal Drug Products
FDA 7.00
Issues• Approval of anti-arrhythmic drugs that prolong
the QT interval– Sotalol and Dofetilide
• Approval of cardiac drugs that prolong the QT interval, excluding the anti-arrhythmics– Bepridil
• Relationship between QT prolongation, Torsade de Pointes (TdP), and Clinical Events– Sotalol and Dofetilide

FDA 7.00
I. Approval for Atrial Arrhythmias• Sotalol and Dofetilide have a dose-
dependent effect on QTc and cause TdP
• Effect on QT intrinsic to their effect as an anti-arrythmic
• Approval was based on – Demonstration of symptomatic benefit – Obtaining sufficient information to adequately
describe the nature of the arrhythmic risk

FDA 7.00
d, l,-Sotalol• Class III anti-arrhythmic
– Approved for • Treatment of life-threatening ventricular
arrhythmias • Maintenance of Normal Sinus Rhythmn in
patients with atrial arrhythmias
• Mean effect on QTc– 10 to 40 msecs at doses from 160 to 640
mg/ day
• Dose-dependent effect on QTc prolongation and TdP
FDA 7.00
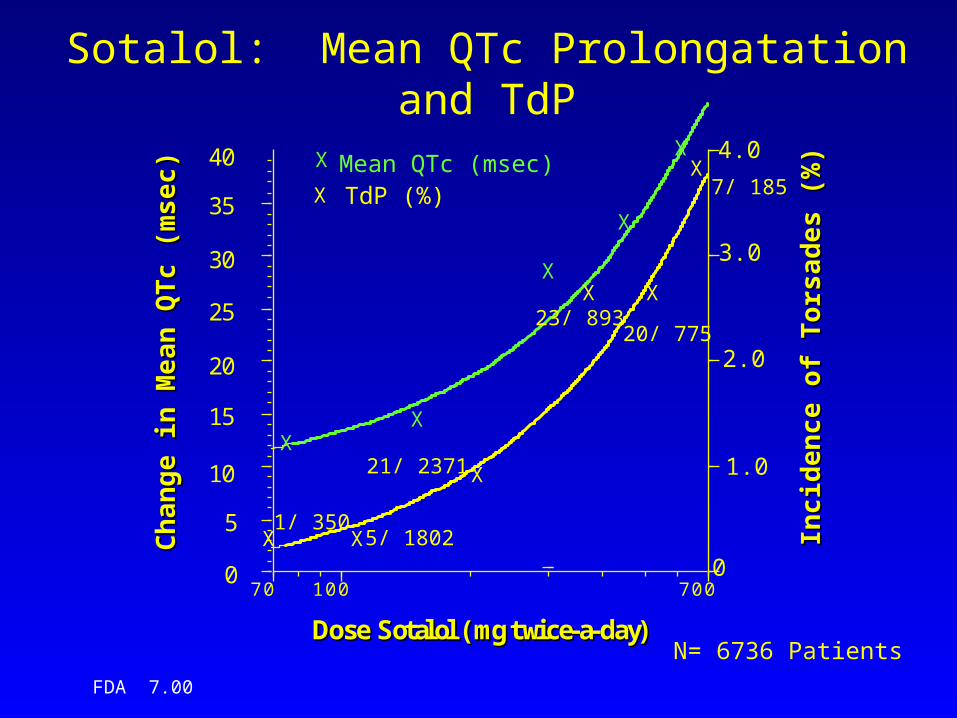
Sotalol: Mean QTc Prolongatation and TdP
XX
X
X
X
X X
X
X X
X
0
5
10
15
20
25
30
35
40
0
1.0
2.0
3.0
4.0
70 100 700
Ch
an
ge
in M
ea
n Q
Tc
(mse
c)
Ch
an
ge
in M
ea
n Q
Tc
(mse
c)
Inci
den
ce
of
To
rsa
de
s (%
)In
cid
enc
e o
f T
ors
ad
es
(%)
DDoossee SSoottaallooll ((mmgg ttwwiiccee--aa--ddaayy))
X
N= 6736 Patients
X
Mean QTc (msec)TdP (%)
21/ 2371
5/ 18021/ 350
23/ 89320/ 775
7/ 185

FDA 7.00
Sotalol: Effect on Mortality
• Post-Myocardial Infarction Trial (Julian Study); n=1,456– Early (<10 Days) Excess Mortality with
Sotalol
– Mortality on Sotalol at one year 7.3%– Mortality on Placebo at one year 8.9%

FDA 7.00
Sotalol: Effect on Mortality• Patients with Atrial Fibrillation and Atrial
Flutter*; n=1191– Sotalol: 3/747 (0.44%)
• 2 sudden deaths
– Quinidine: 1/86 (0.12%)• 0 sudden deaths
– Placebo: 2/358 (0.56%)• 1 sudden death
* Double-Blind portion of the trials only.
FDA 7.00
Dofetilide• Class III anti-arrhythmic
– Approved for • Maintenance of normal sinus rhythmn (NSR) • Conversion of atrial fibrillation/flutter to NSR
• Mean effect on QTc– 34 msec placebo-subtracted QTc
prolongation in phase II/III trials (n=976)
• Dose-dependent effect on mean QTc– 5 to 20 msecs QTc prolongation at doses
of 125 to 500 mcg BID

FDA 7.00
Dofetilide: Dose-Effect on TdP and VF*
0 0.3 0.9
10.5
0
4
8
12
<250mcgBID
250mcgBID
500mcgBID
>500mcgBID
Dofetilide Dose
Inci
de
nce
of T
dP
or
VF
TdP (%)
VF (%)
*NDA SVA PopulationN=1,346

FDA 7.00
Dofetilide: Mortality Effect in High-Risk Population
• DIAMOND CHF and MI– Patients with structural heart disease
and CHF• Dofetilide: 541/1511 (36%)• Placebo: 560/1517 (37%)

FDA 7.00
Dofetilide: Mortality in Supraventricular Arrhythmia Trials
DofetilideMortality
PlaceboMortality
Hazard Ratio(95% CI)
AF/AFl +pSVT
12/1346(0.9%)
3/677(0.4%)
1.1 (0.3, 4.3)
AF/AFl 11/1270(0.9%)
2/614(0.3%)
1.4 (0.3, 6.9)
FDA 7.00
Dofetilide: Dose-Adjustment to Minimize Cardiac Toxicity
• Measure baseline ECG, determine appropriateness of use
• Calculate creatinine clearance, choose appropriate starting dose
• Start Dofetilide under continuous ECG monitoring, dose-adjust as needed

FDA 7.00
Dofetilide: Effect of Dose-Adjusting for Renal Fxn
0
2.5
5
SVA DIAMONDCHF
DIAMONDMI
To
rsad
e d
e P
oin
tes
(%)
TdP Before
TdP After

FDA 7.00
Dofetilide/ Sotalol Summary• Dose-dependent effect on QT, QTc, TdP and
Ventricular Fibrillation– Effects on QTc and TdP rate expected
• Overall mortality in high-risk and target populations not adverse
• Characterization of factors affecting risk of TdP– Exploration of broad dose-range– Exploration of other risk factors (e.g., Dofetilide and
Renal Fxn)

FDA 7.00
II. Approval As Second-Line Therapy
• Bepridil prolongs QT and causes TdP
• Not seen with other anti-anginals
• Approval based on demonstration of symptomatic benefit in a population resistant to available therapy

FDA 7.00
Bepridil• Calcium Channel Blocker
– Approved for treatment of chronic stable angina in patients intolerant or resistant to other anti-anginals
• Mean Effect on QTc– 30 to 70 msec– 5% of patients on Bepridil >25% increase
(appr. 100 msec)
• TdP: 7 cases in 840 angina patients in the U.S. population (0.8%), with 3 fatalities

FDA 7.00
Bepridil
• Effective in Resistant Populations– 86 patients with angina, refractory to Diltiazem,
randomized to Diltizem or Bepridil– Bepridil more effective anti-anginal in this
population, measured by exercise stress testing:• time to onset of angina• time to 1 mm ST-segment depression• total exercise time

FDA 7.00
Bepridil: Summary
• Dose-dependent effect on QT, QTc and clear association with TdP
• Effective in resistant patient population

FDA 7.00
Division of Cardio-Renal Drug Products Summary/Conclusions
• Use of cardiovascular drugs that prolong the mean QT in a dose-dependent fashion is associated with an increased risk for Torsade de Pointes and Sudden Death

FDA 7.00
Division of Cardio-Renal Drug Products Summary/Conclusions
• Cardiac drugs treating symptoms (e.g., atrial arrhythmias) have been approved with the following– Demonstration of symptomatic benefit – Sufficient information to adequately describe the
nature of the arrhythmic risk • Description of the drug-effect over a broad
dose-range• Exploration of potential factors that modify the
arrhythmic risk• Point estimates of total mortality in high-risk
population and in target population

FDA 7.00
Division of Cardio-Renal Drug Products Summary/Conclusions
• Cardiac drugs that cause QT prolongation can also be approved as second-line therapy by demonstrating a symptomatic benefit in a resistant population