failure to thrive
DESCRIPTION
S. U. S. FAILURE TO THRIVE. By William Bithoney Patrick Casey Robert Karp. Failure to Thrive. Abnormal weight status during infant-toddler years and/or Abnormal weight gain (weight growth velocity ). Abnormal weight status Referenced against:. - PowerPoint PPT PresentationTRANSCRIPT

SUS
ByWilliam Bithoney
Patrick CaseyRobert Karp
FAILURE TO THRIVE
SUS

SUS
Failure to Thrive
Abnormal weight status during infant-toddler years
and/or
Abnormal weight gain (weight growth velocity)

SUS
Abnormal weight status Referenced against:
• Genetic growth expectations for family• Children of same gender and gestation
adjusted age – <5% on NCHS curves
• Child's own length – <10-25% on NCHS curves

SUS
Abnormal weight gain (Growth Velocity)
• Falling across two standard deviation percentile lines on NCHS curves over 6 month period
• For at least one to two months

SUS
FTT Definition includes:
"light""thin"
atypical weight gain

SUS
Cautions Regarding Definition of Failure-to-Thrive
• Genetically small due to parents size • Children born small for gestational
age (SGA) may never catch up• If born larger than long-term genetic
potential demonstrate decreased growth rate in first 2 years

SUS
FTT Definition: Growth Only
• Not necessarily associated with developmental/emotional problems in child
• Not necessarily environmental causation
SUS
What's in a name?
Growth DelayGrowth FailureFailure to Grow
Growth DeficiencyFailure to Gain Weight

SUS
FTT of long duration (Grown Older)
STUNTED:• Abnormal length and head
circumference• Psychosocial Dwarf?

SUS
Failure-to -thrive Cause:
All children with Failure-To Thrive
are Undernourished

SUS
Three Methods to Categorize Undernutrition in Children
Degree of Under-Nutrition
NoneMildModerateSevere
Gomez:% medianweight-for age
>9075-9060-74<60
Waterlow:% medianweight-for-height
>9080-9070-79<70
McLaren,Read:% median wt/htfor age ratios
>9085-9075-84<75

SUS
Categorization of Undernutrition in 258 Children Referred for "Failure to Thrive"
Degree of Under-Nutrition
NoneMildModerateSevere
Gomez
No.
51321129
%
251434
Waterlow
No.
64149423
%
2558161
McLaren,Read
No.
183815646
%
7156018

SUS
Clinical Subtypes
I. Medical Cause– Organic vs. Non-organic vs. Mixed
II. Clinical Presentation – Age of onset– Severity– Chronicity

SUS
• Organic Etiology:– medical disease present and clinically judged to be sole
cause of FTT
• Non-organic Etiology:– problems in the child's environment judged to be the
primary cause of FTT, in the presense or absence of medical disease
• MIXED Etiology:– medical problem and problems in environment in
combination are judged to be cause of FTT

SUS
Problems with Organic/Non-Organic Dichotomy
1. It is often difficult to place a child in either category
2. The dichotomy fails to account for the compounding effect of problems in both the child and the environment

SUS
Problems with Organic/Non-Organic Dichotomy (Cont'd)
• 3. Children with either may have symptoms like diarrhea or vomiting
• 4. Children with either may gain weight while in the hospital
• 5. Global terminology is not specific enough to develop an individualized management plan

SUS
Clinical Subtypes (Cont'd)
III. Socioemotional
0-3 months
4-10 months
11-36 months
Homeostasis
Attachment disorder
Separation individuation disorder

SUS
Clinical Subtypes (Cont'd)
IV. Psychiatric DiagnosesFeeding DisorderDepressionReactive Attachment Disorder
V. Mechanical Feeding DisorderFood Avesion
SUS
Transactional FTT
Multiple aspects (overt or subtle) of child, parents, and the proximal and distal environments interact across time to result in FTT.
SUS
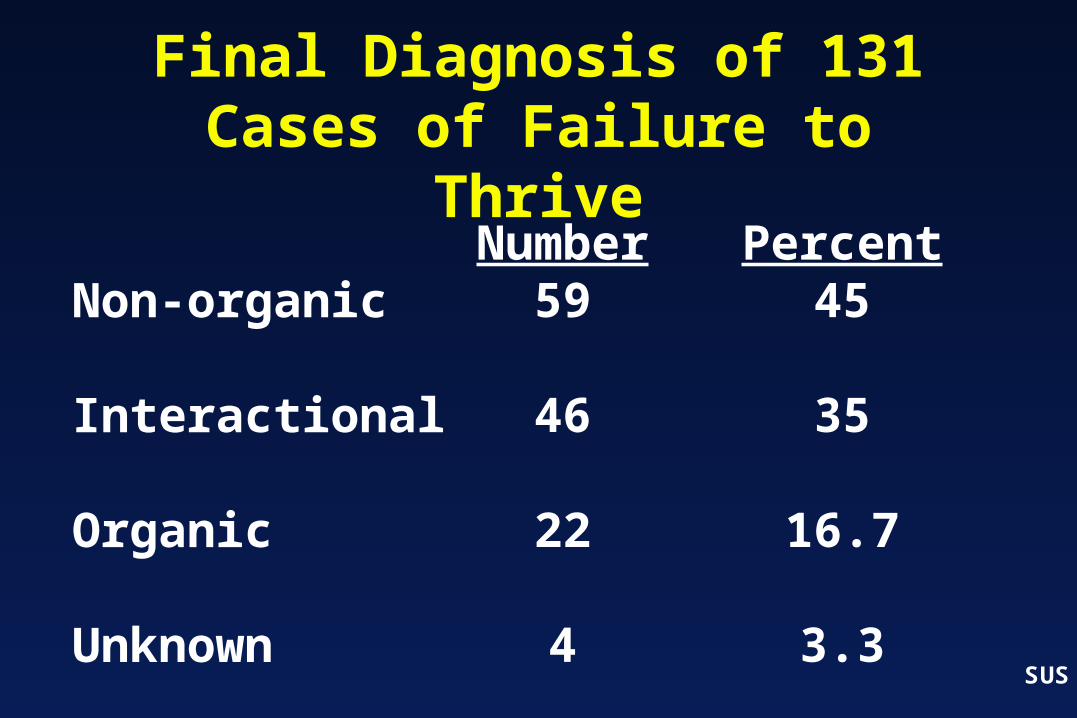
Final Diagnosis of 131 Cases of Failure to Thrive
Non-organic
Interactional
Organic
Unknown
Number59
46
22
4
Percent45
35
16.7
3.3

SUS
Frequency of Organic Systems Causing Failure to Thrive
GastrointestinalNeurologicalRespiratory-PulmonaryCardiovascularEndocrineOther
Most Common
Least Common

SUS
Prevalence of Failure to Thrive
• 3.5% of admissions to children's hospitals
• 10% of clinic visists in urban and rural outpatient settings
• up to 16% 0-4 year olds in low income populations are "stunted"

SUS
Failure to Thrive
• Weight is abnormally 2 standard deviations below the mean for gestation corrected age -- and/or
• weight crossess percentile curves by two standard deviations
• weight to height ratio is depressed

SUS
"My baby is just small for her age"
-Parent

SUS
Failure to Thrive: Spectrum of Causes
Problem in the Child
ORGANIC
Problem in theEnvironment
NON-ORGANIC
Interactive
Effects

SUS
Parent Functioning
Child Outcomes•Development•Learning•Behavior•Growth•Health

SUS
Goals of Clinical EvaluationIdentify conditions which:1. Negatively affect growth potential (disease)2. Increase basic caloric needs (e.g. chronic
infection)3. Decrease availability/utilization of calories
(e.g., malabsorption)4. Negatively affect parents ability to meet
nutritional needs (can't/won't eat)

SUS
Diagnostic Evaluation
1. Growth assessment – confirm the diagnosis with weight and
height, present and past
2. History– predisposing factors
3. Physical examination– significant findings other than
malnutrition

SUS
Diagnostic Evaluation (Cont'd)
• 4. Development-Behavioral Assessment– Assess delays in cognitive, language, or
motor functioning– Identify any behavioral abnormalities
• 5. Laboratory Evaluation– Varies for each child– Stepwise approach is recommended
SUS
Laboratory Evaluation
• Should be directed by findings from the history and physical examination
• Document nutritional status:– albumin, iron, zinc
• Child may have endemic problem: – Tbc, AIDS, giardia

SUS
Diagnostic Evaluation (Cont'd)
• 6. Nutritional and Feeding Evaluation– Content and structure of mealtimes – Feeding techniques
• 7. Social History– Identify parental/family strengths and
weaknesses

SUS
• 8. Parent/Child Interaction– Especially as it relates to feeding
• 9. Psychiatric Evaluation– Important if the caregivers emotional
state is adversely affecting parent-child interaction
Diagnostic Evaluation (Cont'd)

SUS
Hospitalization vs. Outpatient Care
• Advantages of hospitalization:– Able to observe and control feeding– Able to observe the parent-child interaction– Medical evaluation can be done easily
• Disadvantages of hospitalization:– Cost– Child (and parent) are away from their
normal environment
SUS
Indications for Hospitalization of Children with Failure-to-Thrive
1. Evidence of physical abuse2. Extreme failure to thrive (starvation)3. Extremely dysfunctional parent-child
relationship or family4. When distance and transportation issues
mean outpatient management is not practical
5. When outpatient management has failed

SUS
Management of the Child with Failure-to-Thrive
1. Nutritional asessment and intervention2. Improved parent-child interaction3. Developmental stimulation4. Treatment/management of medical
conditions5. Support and intervention for social and
family problems6. Mental health referrals where indicated7. Regular follow-up care

SUS
Best Predictors of Prognosis
• Age of onset, chronicity• Ongoing quality of the home
environment

SUS
Interactional Model of Failure-to-Thrive
PARENT•Economic Status•Health•Knowledge•Emotional State•Past Experience
CHILD•Appearance•Health•Neuro developmental maturity•Ease of Caregiving
Parent-Child Interaction
Failure-to-Thrive
Endocrine-CellularDysfunction
Nutritional Deficiency

SUS
Environmental Characteristics: Supports and Stressors
• Home– -Marital Relationship– -Physical Quality– -Organization– -Stability– -Economic Resources
• Family• Neighborhood and Work