factors which can influence the quality related to cell viability of the umbilical cord blood units
TRANSCRIPT

Factors which can influence the quality related to cell viabilityof the umbilical cord blood unitsMagda Dulugiac a,b, Ionela Horeanga a, Andrei Torcatoru a, Alexandru Bardas a,Georgiana Matei a, Otilia Zarnescu b,*a Regina Maria Central Stem Cells Bank, 5B Ion Ionescu de la Brad, 13811, Bucharest, Romaniab Faculty of Biology, University of Bucharest, Splaiul Independentei 91-95, R-050095, Bucharest, Romania
A R T I C L E I N F O
Article history:Received 9 March 2014Received in revised form 22 August 2014Accepted 25 August 2014
A B S T R A C T
Cell viability is an important indicator for the quality of umbilical cord blood (UCB) unitsthat can influence the transplant final outcome. Thus, it is particularly important to iden-tify the factors that may affect the cell quality during the banking process. The present studyis a first attempt to correlate the impact of exogenous factors (time from collection to pro-cessing, collected UCB volume) and endogenous factors (TNCC – total nucleated cell count,CD34+cell count) on cell viability assessed before UCB units cryopreservation within a bankingstandardized process. Three thousand UCB units collected in 35 ml CPDA containing bagswere processed by HES sedimentation within 48 h. TNCC, CD34+ cell counts and total cellviability were determined after processing. Cell viability of 94.37 ± 4.67%, TNCC of73.17 ± 36.73 × 107 and CD34+cell count of 2.61 ± 2.29 × 106 was obtained after processingof units with UCB collected volume of 80.23 ± 28.52 ml. A significant negative correlationwas found between cell viability and the time from collection to processing (r = –0.7228;P < 0.0001). The cell viability decreasing rate of 20.54%, 15.18% and 3–10% were achievedfor units with collected UCB volume <40 ml, (40–80 ml) and >80 ml, to 48 h versus 12 h.There were no differences considering cell viability for the UCB units with similar collect-ed UCB volume that had various CD34+cell count or TNCC (P > 0.05). The extension of thetime from collection to processing of UCB units can reduce the quality by decreasing cellviability. The cell viability decreasing rate owing to the time influence is determined bythe collected UCB volume being inversely proportional to it. Endogenous factors do not affectthe cell viability.
© 2014 Elsevier Ltd. All rights reserved.
Keywords:Umbilical cord bloodStem cellsCell viability
1. Introduction
Umbilical cord blood banks are aimed to provide highquality units needed for clinical therapies, for hematopoi-etic and immune system reconstitution in order to treatmalignant and non-malignant hematological disorders [1].Because the cord blood stem cell number is limited, main-taining cell viability becomes a critical issue. Cell viabilityis an important indicator for the quality of umbilical cord
blood units (UCB units) that can influence the final outcomeof a transplant. It seems that extensive manipulation withsignificant variables could determine unexpected viabilityproblems [2]. In this situation it is particularly importantto identify the factors that may affect the cell quality duringthe banking process. It is essential to retain viability andfunctional integrity for the cells obtained by umbilical cordblood processing [3]. Studies accomplished to date show thatthe cell viability is influenced by storage conditions of UCBunits before processing and cryopreservation. Thus, thestorage temperature of UCB units from collection tocryopreservation seems to be an essential factor that in-fluences the cell viability and contributes to maintaining the
* Corresponding author. Tel.: + 213102843; Fax: +40-21-313 17 60.E-mail address: [email protected] (O. Zarnescu).
http://dx.doi.org/10.1016/j.transci.2014.08.0191473-0502/© 2014 Elsevier Ltd. All rights reserved.
Transfusion and Apheresis Science ■■ (2014) ■■–■■
ARTICLE IN PRESS
Please cite this article in press as: Magda Dulugiac, et al., Factors which can influence the quality related to cell viability of the umbilical cord blood units, Trans-fusion and Apheresis Science (2014), doi: 10.1016/j.transci.2014.08.019
Contents lists available at ScienceDirect
Transfusion and Apheresis Science
journal homepage: www.elsevier.com/ locate / t ransci

final product quality. The controversial results show that UCBunits must be stored before processing at 4 °C [4–7] or atroom temperature [8–10]. Other authors consider that thereare no differences reflected in the quality of transplant unitsdepending on the storage temperature [11–13].
The time from collection to processing andcryopreservation is another controversial factor, exten-sively studied, which seems to exert an important impacton cell viability. If some authors consider that significantloss of nucleated cells and CD34+cells has occurred after 24 hof storage from collection [14], other authors consider thatumbilical cord blood cells maintain their viability for a sig-nificantly longer period of 24 h [15], while other authorsassume that the cells remain viable even after 48 h [9] orup to 72 h after collection [8,16]. Other studies show thatumbilical cord blood storage for 72 h induces a high degreeof cellular damage [17,18]. Although most authors recom-mend that processing and cryopreservation must beperformed as soon as possible after umbilical cord blood col-lection to maintain the characteristics of immature cells,other authors [10] suggest that a storage time for 48 h shouldbe preferred to 24 h for maintenance of progenitor cells withhigh capacity of proliferation, transmigration, with a lowrate of apoptosis. In the issue, the maximum storage timefor umbilical cord blood from collection to processing andcryopreservation may be 48 or 72 h [2,12].
The present study is a first attempt to correlate the impactof exogenous and endogenous factors on cell viability as-sessed before UCB units cryopreservation within a bankingstandardized process.
2. Materials and methods
2.1. UCB collection, transport and storage
A total of 3000 UCB units were collected by trainedmedical personnel at Obstetrics and Gynecology Hospitalsin Romania. UCB samples were obtained by puncture of theumbilical vein, after normal or cesarean delivery, and col-lected into blood collection bags (Baxter, Fenwal), 250 mlcapacity, containing 35 ml anticoagulant CPDA (citrate phos-phate dextrose adenine). After collection, each UCB collectionbag was folded into gel wrap (Therapak), inserted into in-sulated envelope foil (Therapak) and placed into a box fortransport. Because of insulation system, the transport canbe done in ambient temperature, between 15 and 30 °C,without affecting the temperature of UCB units. At themoment of reception, UCB collection bags revealed tem-peratures between 20 and 26 °C, measurements being donewith Testo 830-T2 thermometer. After reception, the UCBbags were maintained at room temperature (22 ± 2 °C) untilprocessing.
2.2. UCB processing
UCB units were deemed to comply if they have been pro-cessed within 48 h post collection. UCB units with collectedUCB volume (excluding the amount of anticoagulant) lessthan 15 ml were not accepted for processing. Processing wasachieved through volume reduction using hidroxietilamidon(10% HES Fresenius Pharma, Graz, Austria) sedimentation
method as has been previously described [19,20]. Aftererythrocytes and partial plasma removal UCB units with astandard volume of 25 ml designed for cryopreservationwere obtained and tested.
2.3. Total nucleated cell count
Quantification of nucleated cell number was performedby using Act Diff 5 Beckman Hematology Analyzer Coulter.The total nucleated cells count (TNCC) was established bytesting a sample of the UCB units, using a calculation formula:WBC × 103/μl × 25 × 103 μl, where 25 × 103 μl represents thefinal volume of the UCB units obtained after processing.
2.4. Flow cytometry analysis: CD34+ assay and cell viabilityassay
The flow cytometric analysis was performed after pro-cessing and before freezing on a flow cytometer BeckmanCoulter FC500 equipped with CXP System Software (Version2.0), using an automated method. We used Beckman CoulterStem-Kit Reagents intended for “In vitro diagnostic use”,including 7-aminoactinomycin D (7-AAD) – a cell viabilityreagent, CD34-phycoerythrin (PE; 580 clones)/CD45-fluorescein isothiocyanate (FITC; J33 clone) antibody, CD45-fluorescein isothiocyanate (FITC; J33 clone)/IsoClonicControl-phycoerythrin antibody, Stem Count Fluorospheres,NH4Cl Lysis solution. Two identical tests and anisomorphologic control to check the nonspecific binding ofthe CD34-PE were run for each sample. The software allowedthe evaluation of the total cell viability percentage, the si-multaneous identification and enumeration of viableCD45+cells and the dual positive CD45+/CD34+cell popula-tion percentage or absolute counts and the CD34+ total cellscounts per UCB units.
2.5. Statistical analysis
The data were expressed as the arithmetic meanvalues ± standard deviation, median and intervals(minimum-maximum). Software Graph Pad Prism 5 (GraphPad Software Inc, San Diego, CA) was used for data inter-pretation. Comparisons of quantitative variables were doneby the t test, Mann–Whitney test, one way ANOVA Kruskal–Wallis test with Dunn’s multiple comparison post test andtwo way ANOVA test with Bonferroni post tests. The Spear-man’s correlation coefficient was used to estimate thecorrelation between quantitative variables. All the re-ported P values represent two-tailed tests, with values of0.05 or less considered statistically significant. All the sta-tistical analyses were made with nonparametric tests.
3. Results
3.1. Cell viability of UCB units
Pre freeze cell viability of UCB units obtained after um-bilical cord blood (n = 3000) processing was ranged from61.86% to 99.5% with a mean value of 94.37 ± 4.67% andmedian of 95.62%. 95.14% of the UCB units had cell viabil-ity higher than 85%.
ARTICLE IN PRESS
Please cite this article in press as: Magda Dulugiac, et al., Factors which can influence the quality related to cell viability of the umbilical cord blood units, Trans-fusion and Apheresis Science (2014), doi: 10.1016/j.transci.2014.08.019
2 M. Dulugiac et al./Transfusion and Apheresis Science ■■ (2014) ■■–■■

3.2. Influence of time on cell viability
99.86% of the units were processed within 48 h fromcollection and only 0.13% of the units have been pro-cessed within 48–75 h from collection. The mean timebefore processing was 19.79 ± 8.71 h. The cell viability ofthe units exposed to different storage time between
collection and processing (results summarized in Table 1)varies inversely proportional with the time, the resultsbeing significantly different (P < 0.0001) (Fig. 1A). Also, wenoticed a significant negative correlation between cell vi-ability and the time (r = –0.7228; P < 0.0001; n = 3000)(Fig. 1B), cell viability declining with the increasing timerange.
Table 1Cell viability of the UCB units ranked by time ranges from collection to processing.
[0–12 h) [12–24 h) [24–36 h) [36–48 h) [48–75 h)
No. of UCB units 548 1535 808 105 4Minimum 81.77 67.58 61.86 66.46 63.44Median 98.66 95.79 93.24 86.11 73.11Maximum 99.50 99.23 99.49 95.28 91.61Mean 98.12 94.97 92.06 84.54 75.32Std. deviation 1.87 3.18 4.76 6.87 13.79Std. error 0.08 0.08 0.16 0.67 6.89Coefficient of variation 1.91% 3.35% 5.18% 8.13% 18.30%
Fig. 1. Cell viability of the UCB units (mean + min/max) grouped by ranges of time from collection to processing (A). Correlation between cell viabilityand time from collection to processing (B). Cell viability (Whiskers: Min to Max) of the UCB units grouped by collected UCB volume ranges (C). correla-tion between cell viability and collected UCB volume (D).
ARTICLE IN PRESS
Please cite this article in press as: Magda Dulugiac, et al., Factors which can influence the quality related to cell viability of the umbilical cord blood units, Trans-fusion and Apheresis Science (2014), doi: 10.1016/j.transci.2014.08.019
3M. Dulugiac et al./Transfusion and Apheresis Science ■■ (2014) ■■–■■

3.3. Influence of collected UCB volume on cell viability
The collected UCB volume was ranged from 15.2 to202 ml with a mean value of 80.23 ± 28.52 ml and medianof 78.5 ml. Evaluating cell viability for the units grouped bycollected UCB volume ranges (results summarized in Table 2)we noticed significant differences between groups(P < 0.0001). Units with collected UCB volume <80 ml hadcell viability lower compared with units with higher volumes(P < 0.0001). There were no highlight differences regard-ing cell viability between the units with collected UCBvolume higher than 80 ml (P = 0.327) (Fig. 1C). There wasa positive correlation between these parameters (r = 0.209;P < 0.0001) (Fig 1D).
Comparing units grouped by collected UCB volume rangesand time from collection to processing we have obtainedsignificantly different results (results summarized in Table 3).Both the time and collected UCB volume influence cell vi-ability (P = 0.0004 respectively P = 0.0204) (Fig. 2). The unitsprocessed in the first 12 h had similar cell viability, regard-less of the collected UCB volume (P = 0.406). Increasing ofthe time determined decreasing of the cell viability. The de-creasing of the cell viability was more remarkable for lowcollected UCB volume (<80 ml) compared with units withhigher collected UCB volume. Thus, the decreasing rate of
the cell viability increased to 48 h compared with 12 h with20.54% for units with collected UCB volume < 40 ml; with15.18% for units with a volume between (40 and 80 ml) andwith only 3–10% for units with higher volume of 80 ml. Theunits with collected UCB volumes higher than 80 ml hadsimilar cell viability when they had been processed at thesame time range (P = 0.5806). The decreasing rate of the cellviability varied directly proportional with the time from col-lection to processing and inversely proportional with thecollected UCB volume.
3.4. Influence of TNCC on cell viability
After processing were obtained UCB units with TNCCranged from 4.72 to 538.7 × 107 with a mean value of73.17 ± 36.73 × 107 and median of 67.27 × 107. TNCC was cor-related directly proportional with both the collected UCBvolume (r = 0.7576, P < 0.0001) and the number of nucle-ated cells per milliliter UCB (r = 0.613, P < 0.0001). There wasno correlation between the time from collection to pro-cessing and TNCC (r = 0.0132, P = 0.4697).
Cell viability of the units grouped by TNCC ranges (resultssummarized in Table 4) was significantly different(P < 0.0001) when all groups were compared, but there wereno significant differences between the units with TNCC
Table 2Cell viability of the UCB units ranked by UCB volume ranges.
<40 ml [40–80 ml) [80–120 ml) [120–160 ml) [160–202 ml]
No. of UCB units 172 1400 1155 246 27Minimum 66.46 61.86 67.58 77.72 84.12Median 90.96 95.27 96.10 96.27 95.45Maximum 99.14 99.47 99.50 99.31 98.16Mean 89.26 94.04 95.31 95.32 94.81Std. deviation 7.810 4.782 3.526 3.213 3.044Std. error 0.5955 0.1278 0.1038 0.2049 0.5859Coefficient of variation 8.75% 5.09% 3.70% 3.37% 3.21%
Table 3Summarizing of the results: Cell viability, TNCC, CD34+ cell of the UCB units grouped by the time fromcollection to processing and the collected UCB volume.
Time Volume No. UCB units Cell viability (%) TNCC (×107) CD34+ (×106)
12 h <40 ml 29 97.03 ± 2.46 25.33 ± 12.49 0.79 ± 0.54[40–80 ml) 261 98.22 ± 1.91 51.87 ± 20.49 1.71 ± 1.37[80–120 ml) 217 98.21 ± 1.56 88.81 ± 29.62 3.20 ± 2.04[120–160 ml) 39 97.73 ± 2.44 113.3 ± 24.76 4.61 ± 2.61[160–202 ml) 2 97.62 ± 0.76 182.5 ± 27.37 3.67 ± 4.06
12–24 h <40 ml 73 90.96 ± 5.59 26.66 ± 11.46 0.72 ± 0.47[40–80 ml) 726 94.67 ± 2.84 56.6 ± 21.71 1.81 ± 1.38[80–120 ml) 603 95.61 ± 2.87 89.06 ± 33.67 3.31 ± 2.51[120–160 ml) 121 95.87 ± 2.57 115 ± 40.64 4.82 ± 2.70[160–202 ml) 12 96.2 ± 1.49 143.6 ± 46.5 7.73 ± 3.10
24–36 h <40 ml 57 86.03 ± 7.04 28.73 ± 14.63 0.82 ± 0.59[40–80 ml) 361 91.46 ± 4.77 57.88 ± 21.33 1.81 ± 1.25[80–120 ml) 303 93.3 ± 93.4 88.92 ± 28.85 3.29 ± 2.14[120–160 ml) 75 93.96 ± 3.05 129.2 ± 50.06 5.71 ± 4.46[160–202 ml) 12 92.97 ± 3.52 132.8 ± 50.32 5.99 ± 2.925
36–48 h <40 ml 13 76.49 ± 6.73 29.06 ± 10.17 0.99 ± 0.64[40–80 ml) 15 83.04 ± 6.12 60.59 ± 28.57 1.75 ± 1.39[80–120 ml) 30 88.21 ± 4.67 90.33 ± 26.05 2.56 ± 1.29[120–160 ml) 11 90.01 ± 3.26 131.1 ± 41.51 4.65 ± 3.22[160–202 ml) 1 94.50 166.70 7.880
ARTICLE IN PRESS
Please cite this article in press as: Magda Dulugiac, et al., Factors which can influence the quality related to cell viability of the umbilical cord blood units, Trans-fusion and Apheresis Science (2014), doi: 10.1016/j.transci.2014.08.019
4 M. Dulugiac et al./Transfusion and Apheresis Science ■■ (2014) ■■–■■

higher 50 × 107 (P = 0.4646) (Fig. 3A). There was a very lowpositive correlation between TNCC and cell viability(r = 0.1167; P < 0.0001) (Fig. 3B).
Assessing cell viability of the units grouped by TNCCranges according to the time, we demonstrated that timeinfluences inversely proportional cell viability, but the ex-tending time affected units with TNCC < 50 × 107 moresignificantly compared with the other units (P < 0.05), cellviability being lower after 24 h. (Fig. 3C).
Assessing cell viability of the units grouped in TNCCranges according to the collected UCB volume, we pointedout that collected UCB volume significantly affected cell vi-ability (P < 0.05) regardless of the TNCC. The units withcollected UCB volume <40 ml had cell viability lower com-pared with the other units. We identified no differenceregarding cell viability between units with similar collect-ed UCB volume that had various TNCC (P > 0.05) (Fig. 3D).
3.5. Influence of CD34+cell count on cell viability
The units had CD34+ cell count ranged from 0.09 to35.89 × 106, with a mean value of 2.61 ± 2.29 × 106 andmedian 1.96 × 106. The percentage of CD34+cell count withinTNCC may vary between 0.1% and 3.43%; mean of0.34 ± 0.21%, median of 0.3%. The CD34+ cell count was di-rectly correlated with collected UCB volume (r = 0.6162;P < 0.0001), with TNCC (r = 0.7351; P < 0.0001) and concen-tration of CD34+ cells within TNCC (r = 0.763; P < 0.0001).There was no correlation between the time from
collection to processing and the CD34+ cell count (r = 0.003;P = 0.8946).
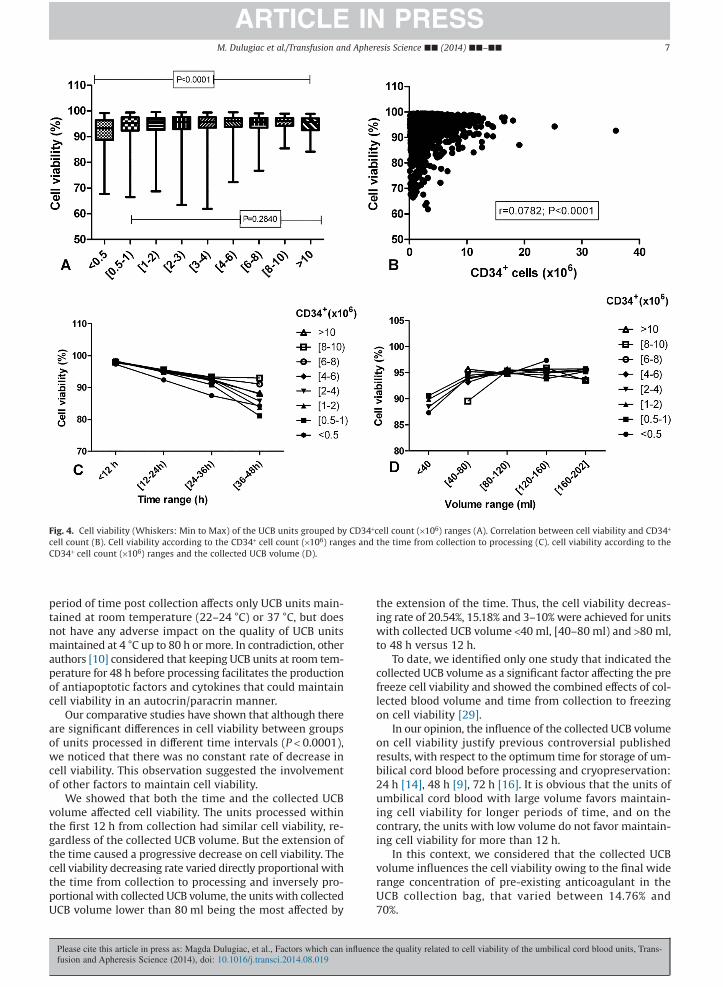
Assessing cell viability of the units grouped by CD34+ cellcount (× 106) ranges (results summarized in Table 5), we ob-served there were significant differences between these(P < 0.0001). Units that have the CD34+ cell count <0.5 × 106
had cell viability lower compared with other units. Cell vi-ability of the units with the number of CD34+ > 0.5 × 106 didnot differ significantly (P = 0.2840) (Fig. 4A). There was a verylow positive correlation between CD34+ cell count and cellviability (r = 0.0782; P < 0.0001) (Fig. 4B).
Evaluating cell viability of the units grouped by CD34+
cell count ranges according to the time from collection toprocessing, we proved that time affected inversely propor-tional cell viability (P < 0.0001). We observed that units withCD34+ cell count <0.5x106 were more affected (P = 0.0364)by extension of the time from collection to processing cellviability being significantly lower. We had not noticed dif-ferences in terms of cell viability of the units with CD34+cellcount >0.5 × 106 (P > 0.05) processed in different periods oftime (Fig. 4C).
Assessing cell viability of the units grouped by numberof CD34+ cell ranges according with collected UCB volumewe pointed out that collected UCB volume significantly af-fected cell viability (P < 0.05) regardless of the number ofCD34+ cell, the units with collected UCB volume <40 mlhaving lower cell viability compared with the other units(Fig. 4D). We identified no difference considering cell via-bility for the units with similar collected UCB volume thathad various CD34+ cell count (P = 0.2118).
4. Discussion
In this study, we attempt to correlate the impact of ex-ogenous factors such as the time from collection toprocessing of UCB and the collected UCB volume, as wellas the impact of endogenous factors such as the total nucle-ated cell count and CD34+ cell count on total cell viabilitybefore cryopreservation. Moreover, we studied possible as-sociation between these factors and conditions which mightinfluence them in terms of quantity, the engraftment ratebeing directly dependent on both cell amount and cellquality related to viability.
Although previously it was demonstrated that there wasno significant correlation between total cell viability (nucle-ated cell viability) and CD34+ cell viability, implying that thetotal cell viability might not be related to the functional stateof progenitors cells [21,22], according to the US Food and
Fig. 2. Cell viability of the UCB units grouped by collected UCB volumeduring increasing of time from collection to processing.
Table 4Cell viability of the UCB units grouped by TNCC ranges.
TNCC (×107) <50 50–100 100–150 150–200 >200
No. of UCB units 832 1591 471 88 18Minimum 66.46 63.44 61.86 83.48 84.12Median 94.85 95.75 96.10 95.84 94.88Maximum 99.38 99.50 99.48 99.31 98.88Mean 93.29 94.76 94.86 94.93 94.12Std. deviation 5.716 4.164 4.213 2.977 3.942Std. error 0.1982 0.1044 0.1941 0.3173 0.9292Coefficient of variation 6.13% 4.39% 4.44% 3.14% 4.19%
ARTICLE IN PRESS
Please cite this article in press as: Magda Dulugiac, et al., Factors which can influence the quality related to cell viability of the umbilical cord blood units, Trans-fusion and Apheresis Science (2014), doi: 10.1016/j.transci.2014.08.019
5M. Dulugiac et al./Transfusion and Apheresis Science ■■ (2014) ■■–■■

Drug Administration recommendations, pre freezing nucle-ated cell viability is a quality control parameter and mustbe greater than 85% [23].
Our total cell viability assessment method by flowcytometry, using standardized protocol dedicated to clin-ical use, is the most effective method with highreproducibility between laboratories that follows ISHAGE(International Society of Hematotherapy and Graft Engi-neering) recommendations [24].
The pre freeze cell viability mean value of 94.37 ± 4.67%obtained by evaluation of 3000 UCB shows that our bankingprocedures allowed maintaining optimal cell viability.
Our results were similar to the results of other studies,which reported a cell viability mean value of 94.8 ± 4.8% [21],92 ± 4% [25], 94.9% [26]. Although 87.56% of the units in-cluded in our study had cell viability higher than 90%,(99.86% of the units being processed within 48 h), we noticedthat cell viability was influenced by the time from collec-tion to processing, between these two parameter existinga negative correlation. The extension of the time from col-lection to processing was associated with a decrease of cellviability. These findings are in accord with the results fromother studies [5,6,13,21,26,27]. Some authors [28] consid-ered that temperature is a key parameter and extended
Fig. 3. Cell viability (Whiskers: Min to Max) of the UCB units grouped by TNCC (×107) ranges (A). correlation between cell viability and TNCC (B). Cellviability according to the TNCC (×107) ranges and the time from collection to processing (C). Cell viability according to the TNCC (×107) ranges and thecollected UCB volume (D).
Table 5Cell viability of the UCB units grouped by CD34+ cell count ranges.
CD34+ cell count (×106) <0.5 [0.5–1) [1–2) [2–3) [3–4) [4–6) [6–8) [8–10) >10
No. of UCB units 147 465 913 579 346 337 123 59 42Minimum 67.68 66.46 68.69 63.44 61.86 72.21 76.78 85.48 84.12Median 93.25 95.31 95.57 95.68 95.77 96.00 95.71 96.01 95.66Maximum 99.24 99.40 99.50 99.49 99.41 99.47 99.08 98.99 98.88Mean 91.48 93.99 94.33 94.55 94.89 95.06 95.00 95.05 94.67Std. deviation 6.99 5.21 4.47 4.65 4.25 3.68 3.47 3.21 3.59Std. error 0.57 0.24 0.14 0.19 0.22 0.20 0.31 0.41 0.55
ARTICLE IN PRESS
Please cite this article in press as: Magda Dulugiac, et al., Factors which can influence the quality related to cell viability of the umbilical cord blood units, Trans-fusion and Apheresis Science (2014), doi: 10.1016/j.transci.2014.08.019
6 M. Dulugiac et al./Transfusion and Apheresis Science ■■ (2014) ■■–■■
period of time post collection affects only UCB units main-tained at room temperature (22–24 °C) or 37 °C, but doesnot have any adverse impact on the quality of UCB unitsmaintained at 4 °C up to 80 h or more. In contradiction, otherauthors [10] considered that keeping UCB units at room tem-perature for 48 h before processing facilitates the productionof antiapoptotic factors and cytokines that could maintaincell viability in an autocrin/paracrin manner.
Our comparative studies have shown that although thereare significant differences in cell viability between groupsof units processed in different time intervals (P < 0.0001),we noticed that there was no constant rate of decrease incell viability. This observation suggested the involvementof other factors to maintain cell viability.
We showed that both the time and the collected UCBvolume affected cell viability. The units processed withinthe first 12 h from collection had similar cell viability, re-gardless of the collected UCB volume. But the extension ofthe time caused a progressive decrease on cell viability. Thecell viability decreasing rate varied directly proportional withthe time from collection to processing and inversely pro-portional with collected UCB volume, the units with collectedUCB volume lower than 80 ml being the most affected by
the extension of the time. Thus, the cell viability decreas-ing rate of 20.54%, 15.18% and 3–10% were achieved for unitswith collected UCB volume <40 ml, [40–80 ml) and >80 ml,to 48 h versus 12 h.
To date, we identified only one study that indicated thecollected UCB volume as a significant factor affecting the prefreeze cell viability and showed the combined effects of col-lected blood volume and time from collection to freezingon cell viability [29].
In our opinion, the influence of the collected UCB volumeon cell viability justify previous controversial publishedresults, with respect to the optimum time for storage of um-bilical cord blood before processing and cryopreservation:24 h [14], 48 h [9], 72 h [16]. It is obvious that the units ofumbilical cord blood with large volume favors maintain-ing cell viability for longer periods of time, and on thecontrary, the units with low volume do not favor maintain-ing cell viability for more than 12 h.
In this context, we considered that the collected UCBvolume influences the cell viability owing to the final widerange concentration of pre-existing anticoagulant in theUCB collection bag, that varied between 14.76% and70%.
Fig. 4. Cell viability (Whiskers: Min to Max) of the UCB units grouped by CD34+cell count (×106) ranges (A). Correlation between cell viability and CD34+
cell count (B). Cell viability according to the CD34+ cell count (×106) ranges and the time from collection to processing (C). cell viability according to theCD34+ cell count (×106) ranges and the collected UCB volume (D).
ARTICLE IN PRESS
Please cite this article in press as: Magda Dulugiac, et al., Factors which can influence the quality related to cell viability of the umbilical cord blood units, Trans-fusion and Apheresis Science (2014), doi: 10.1016/j.transci.2014.08.019
7M. Dulugiac et al./Transfusion and Apheresis Science ■■ (2014) ■■–■■

Our conclusion is contradictory to the results of someauthors who showed that the broad range of anticoagu-lant concentration did not affect cell viability, though agradual loss of cell viability was observed after storagefor 25–48 h and particular after 49–80 h [13]. But thereare authors that suggest that the ratio of anticoagulantcould determine low cell viability for the units with thecollected UCB volume of less than 60 ml, even if the amountof anticoagulant in collection bags was lower (29 ml)[29].
However, our observations could support the theory ofother authors that maintaining cell viability is achieved bythe presence of the growth factors and the cytokines in theumbilical cord plasma and lowering their concentrationcaused by diluting after UCB collection and mixing with an-ticoagulant would accelerate development of cellularapoptosis process [28].
Thereby, we have tried to emphasize the influence of en-dogenous factors of the units on pre freeze cell viability, suchas TNCC and CD34+ cell count.
There were remarkable variations between individualUCB units with respect to collected UCB volume, total nucle-ated cell count and CD34+ cell count. For collected volumeranged from 15.2 to 202 ml we obtained after processingUCB units with TNCC ranged from 4.72 to 538.7 × 107 meanof 73.17 ± 36.73 × 107 and CD34+ cell count ranged from 0.09to 35.89 × 106, mean of 2.61 ± 2.29 × 106. Similar studiesshowed comparable results: 90 ± 37 × 107 TNCC and2.46 ± 2.72 × 106 CD34+ cell count [30]; 94x107 TNCC and3.1 ± 2.7 × 106 CD34+cell count [31]; 2.2–2.3 × 106 CD34+ cellcount [32]. According to our data there were good and verygood positive correlations between collected UCB volume,TNCC and CD34+ cell count. Positive correlations betweencollected UCB volume and CD34+ cell count and betweenTNCC and CD34+ cell count were highlighted in other studies[13,14].
We consider that by increasing the collected UCB volumethe chance of obtaining a large number of cells increasesbut more important is the cell concentration that varies inwide range: 1.88–114 × 106 nucleated cells per milliliter UCBand 0.1–3.43% CD34+cell count within TNCC. Thus, the unitswith similar collected UCB volumes had different TNCC re-spectively CD34+ cells counts.
Consequent to comparative studies, we have not iden-tified significant differences regarding TNCC and CD34+ cellcount between the units processed within different rangesof time from collection. There was no correlation betweenthe time from collection to processing and the number ofcells. Similar results have been reported by other authors[13,26]. However, some authors [33] have identified areduced negative correlation between CD34+ cell count andthe time from collection to processing.
In a different approach some authors considered thatthe time from collection to processing influenced vari-ously the viability of different cell types. According to thesestudies, the extending of the time from collection to pro-cessing determined a decrease in cell viability mainly forgranulocyte, while the viability of CD34+ cells seems to notto be affected [7,21,22,28,34]. Thus, interested in knowingif a larger number of CD34+ cells ensure maintaining a highercell viability, we noticed that there was a very reduced
positive correlation (r = 0.0782; P < 0.0001) between theseparameters.
According to our data the units with CD34+ cell countless than 0.5 × 106 or the units with TNCC less than 50 × 107
had pre freeze cell viability lower compared with other unitswith a larger number of cells. These units are more affect-ed by the extension of time from collection to processing,the decreasing rate of cell viability being much higher.However, we have not noticed significant differences in termsof cell viability for units that have a similar volume and havevery different TNCC or CD34+ cell count. In this way, we con-sider that the TNCC and CD34+ cell count do not affect cellviability. The reduced viability of the units with TNCC lessthan 50 × 107 or with CD34+cell count less than 0.5 × 106 weredue to their common association with low collected UCBvolumes.
Even if total cell viability before cryopreservation is oneof quality control parameters for cord blood banks, its rel-ative biological value should be permanently taken intoaccount as previously demonstrated [35,36]. Only stem andprogenitors cells which could be detected by in vivo assaysand in vitro tests in thawed UCB unit, before release for trans-plantation, are relevant for hematopoietic reconstitutionpotential.
In conclusion, the extension of the time from collec-tion to processing of UCB units can reduce the quality relatedto cell viability. The cell viability decreasing rate owing tothe time influence is determined by the collected UCBvolume, being inversely proportional to it. Endogenousfactors do not affect the cell viability.
References
[1] Gluckman E, Ruggeri A, Volt F, Cunha R, Boudjedir K, Rocha V.Milestones in umbilical cord blood transplantation. BJH2011;154:441–7.
[2] Querol S, Gomez SG, Pagliuca A, Torrabadella M, Madrigal JA. Qualityrather than quantity: the cord blood bank dilemma. Bone MarrowTransplant 2010;45:970–8.
[3] McCullough J, McKenna D, Kadidlo D, Schierman T, Wagner J. Issuesin the quality of umbilical cord blood stem cells for transplantation.Transfusion 2005;45:832–41.
[4] Tron de Bouchony E, Pelletier D, Alcalay D, Bruneau J, Predeau M,Brizard A, et al. Hematopoietic progenitor content of fetal cord bloodcollected using citrate-phosphate-dextrose: influence of holdingtemperature and delays. J Hematother 1993;2:271–3.
[5] Tsagias N, Kouzi-Koliakos K, Karagiannis V, Alamdari DH, Koliakos G.Time and temperature before processing influence the recovery ofumbilical cord blood hematopoietic progenitors. Transfusion2007;47:1550–2.
[6] Fry JL, Ginger SQ, Gomez SG, Green M, Anderson S, Horder J, et al.Avoiding room temperature storage and delayed cryopreservationprovide better postthaw potency in hematopoietic progenitor cellgrafts. Transfusion 2013;53:1834–42.
[7] Radke TF, Barbosa D, Duggleby RC, Saccardi R, Querol S, Kögler G. Theassessment of parameters affecting the quality of cord blood by theappliance of the annexin V staining method and correlation with CFUassays. Stem Cells Int 2013;2013:823912.
[8] Broxmeyer HE, Douglas GW, Hangoc G, Cooper S, Bard J, English D,et al. Human umbilical cord blood as a potential source oftransplantable hematopoietic stem/progenitor cells. Proc Natl AcadSci USA 1989;86:3828–32.
[9] Campos L, Roubi N, Guyotat D. Definition of optimal conditions forcollection and cryopreservation of umbilical cord hematopoietic cells.Cryobiology 1995;32:511–5.
[10] Moledenhauer A, Wolf J, Habermann G, Genter G, Kiesewetter H,Salama A. Optimum storage conditions for cord blood-derivedhematopoietic progenitor cells prior isolation. Bone MarrowTransplant 2007;40:837–42.
ARTICLE IN PRESS
Please cite this article in press as: Magda Dulugiac, et al., Factors which can influence the quality related to cell viability of the umbilical cord blood units, Trans-fusion and Apheresis Science (2014), doi: 10.1016/j.transci.2014.08.019
8 M. Dulugiac et al./Transfusion and Apheresis Science ■■ (2014) ■■–■■

[11] Bertolini F, Gibelli N, Lanza A, Cuomo A, delia Cuna GR, Nelson EJ.Effects of storage temperature and time on cord blood progenitor cells.Transfusion 1998;38:615–7.
[12] Koenigbauer UF, Burger SR, McCullough J. Non-frozen preservationof umbilical cord blood. Transfusion 2002;42:1383–4.
[13] Salge-Bartels U, Huber HM, Kleiner K, Volkers P, Seitz R, Heiden M.Evaluation of quality parameters for cord blood donations. TransfusMed Hemother 2009;36:317–24.
[14] Rogers I, Sutherland DR, Holt D, Macpate F, Lains A, Hollowell S, et al.Human UC-blood banking: impact of blood volume, cell separationand cryopreservation on leukocyte and CD34+ cell recovery.Cytotherapy 2001;3:269–76.
[15] Isoyama K, Yamada K, Hirota Y, Ishikawa K, Imai M, Notake Y. Studyof the collection and separation of umbilical cord blood for use inhematopoietic progenitor cell transplantation. Int J Hematol1996;63:95–102.
[16] Kurtzberg J, Cairo MS, Fraser JK, Baxter-Lowe L, Cohen G, Carter SL,et al. Results of the Cord Blood Transplantation (COBLT) Studyunrelated donor banking program. Transfusion 2005;45:842–55.
[17] Hubel A, Carlquist D, Clay M, McCullough J. Short-term liquid storageof umbilical cord blood. Transfusion 2003;43:626–32.
[18] Xiao M, Dooley DC. Assessment of cell viability and apoptosis inhuman umbilical cord blood following storage. J Hematother StemCell Res 2003;12:115–22.
[19] Rubinstein P, Dobrila L, Rosenfield RE, Adamson JW, Migliaccio G,Migliaccio A, et al. Processing and cryopreservation of placental/umbilical cord blood for unrelated bone marrow reconstitution. ProcNatl Acad Sci USA 1995;92:10119–22.
[20] Rubinstein P. Cord blood banking for clinical transplantation. BoneMarrow Transplant 2009;44:635–42.
[21] Yang H, Loutfy MR, Mayerhofer S, Shuen P. Factors affecting bankingquality of umbilical cord blood for transplantation. Transfusion2011;51:284–92.
[22] Pereira-Cunha FG, Duarte AS, Costa FF, Saad ST, Lorand-Metze I, LuzoAC. Viability of umbilical cord blood mononuclear cell subsets until96 hours after collection. Transfusion 2013;53:2034–42.
[23] Guidance for Industry Minimally manipulated, unrelated allogeneicplacental/umbilical cord blood intended for hematopoieticreconstitution for specified indications. 2009.
[24] Keeney M, Chin-Yee I, Weir K, Popma J, Nayar R, Sutherland DR. Singleplatform flow cytometric absolute CD34+ cell counts based on the
ISHAGE guidelines. International Society of Hematotherapy and GraftEngineering. Cytometry 1998;34:61–70.
[25] Solves P, Mirabet V, Planelles D, Blasco I, Roig R. Red blood celldepletion with semiautomated system or hydroxyethyl starchsedimentation for routine cord blood banking: a comparative study.Transfusion 2005;45:867–73.
[26] Prat-Arrojo I, Ponce-Verdugo L, Hernández-Lamas MC, Rodríguez-PenaR, Antúnez C, Sánchez-Gordo F, et al. Influence on time tocryopreservation in umbilical cord blood units. IJCM 2011;2:399–403.
[27] Rubinstein P, Adamson JW, Stevens EC. The placental/ umbilical cordblood program of the New York blood center. A progress report. AnnN Y Acad Sci 1999;872:328–35.
[28] Solomon M, Wofford J, Johnson C, Regan D. Factors influencing cordblood viability assessment before cryopreservation. Transfusion2010;50:820–30.
[29] Pope B, Mitsakos K, Bilgin A, Hokin B, Grant R. Predicting overallviability of cord blood harvests. Transfusion 2012;52:1079–85.
[30] Reboredo NM, Díaz A, Castro A, Villaescusa RG. Collection, processingand cryopreservation of umbilical cord blood for unrelatedtransplantation. Bone Marrow Transplant 2000;26:1263–70.
[31] Ballen KK, Wilson M, Wuu J, Ceredona AM, Hsieh C, Stewart FM, et al.Bigger is better: maternal and neonatal predictors of hematopoieticpotential of umbilical cord blood units. Bone Marrow Transplant2001;2:7–14.
[32] Armitage S. Cord blood processing: volume reduction. Cell PreservTechnol 2004;4:9–16.
[33] Nakagawa R, Wanatabe T, Kawano Y, Kanai S, Suzuya H, Kaneko M,et al. Analysis of maternal and neonatal factors that influence thenucleated and CD34+ cell yield for cord blood banking. Transfusion2004;44:26–67.
[34] Guttridge MG, Soh TG, Belfield H, Sidders C, Watt SM. Storage timeaffects umbilical cord blood viability. Transfusion 2014;54:1278–85.
[35] Brand A, Eichler H, Sczepiorkowski ZM, Hess JR, Kekomaki R, McKennaDH, et al. Viability does not necessarily reflect the hematopoieticprogenitor cell potency of a cord blood unit: results of aninterlaboratory exercise. Transfusion 2008;48:546–9.
[36] Louis I, Wagner E, Dieng MM, Morin H, Champagne MA, Haddad E.Impact of storage temperature and processing delays on cord bloodquality: discrepancy between functional in vitro and in vivo assays.Transfusion 2012;52:2401–5.
ARTICLE IN PRESS
Please cite this article in press as: Magda Dulugiac, et al., Factors which can influence the quality related to cell viability of the umbilical cord blood units, Trans-fusion and Apheresis Science (2014), doi: 10.1016/j.transci.2014.08.019
9M. Dulugiac et al./Transfusion and Apheresis Science ■■ (2014) ■■–■■